Adaptive Dose-Finding Based on Efficacy-Toxicity Trade-Offs
7
PLEASE SCROLL DOWN FOR ARTICLE This article was downloaded by: [University of Alberta] On: 7 January 2009 Access details: Access Details: [subscription number 713587337] Publisher Informa Healthcare Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House, 37-41 Mortimer Street, London W1T 3JH, UK Encyclopedi a of Biopharmaceutical Statistics Publication details, including instructions for authors and subscription information: http://www.informaworld. com/smpp/title~c ontent=t713172960 Adaptive Dose Finding Based on Efficacy Toxicity Trade Offs Peter F. Thall a ; John D. Cook a a Department of Biostatistics and Applied Mathematics, Universit y of Texas, M.D. Anderson Cancer Center, Houston, Texas, U.S.A. Online Publication Date: 15 August 2006 To cite this Section Thall, Peter F. and Cook, John D.(2006)'Adaptive Dose-Finding Based on Efficacy-Toxicity Trade- Offs',Encyclopedia of Biopharmaceutical Statistics,1:1,1 — 5 Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf This article may be used for research, teaching and private study purposes. Any substantial or systematic reproduction, re-distribution, re-selling, loan or sub-licensing, systematic supply or distribution in any form to anyone is expressly forbidden. The publisher does not give any warranty express or implied or make any representation that the contents will be complete or accurate or up to date. The accuracy of any instructions, formulae and drug doses should be independently verified with primary sources. The publisher shall not be liable for any loss, actions, claims, proceedings, demand or costs or damages whatsoever or howsoever caused arising directly or indirectly in connection with or arising out of the use of this material.
-
Upload
ecaterina-adascalitei -
Category
Documents
-
view
215 -
download
0
Transcript of Adaptive Dose-Finding Based on Efficacy-Toxicity Trade-Offs

8/13/2019 Adaptive Dose-Finding Based on Efficacy-Toxicity Trade-Offs
http://slidepdf.com/reader/full/adaptive-dose-finding-based-on-efficacy-toxicity-trade-offs 1/7
PLEASE SCROLL DOWN FOR ARTICLE
This article was downloaded by: [University of Alberta] On: 7 January 2009 Access details: Access Details: [subscription number 713587337] Publisher Informa Healthcare Informa Ltd Registered in England and Wales Registered Number: 1072954 Registered office: Mortimer House,37-41 Mortimer Street, London W1T 3JH, UK
Encyclopedia of Biopharmaceutical StatisticsPublication details, including instructions for authors and subscription information:http://www.informaworld.com/smpp/title~content=t713172960
Adaptive Dose Finding Based on Efficacy Toxicity Trade OffsPeter F. Thall a; John D. Cook a
a Department of Biostatistics and Applied Mathematics, University of Texas, M.D. Anderson Cancer Center,Houston, Texas, U.S.A.
Online Publication Date: 15 August 2006
To cite this Section Thall, Peter F. and Cook, John D.(2006)'Adaptive Dose-Finding Based on Efficacy-Toxicity Trade-Offs',Encyclopedia of Biopharmaceutical Statistics,1:1,1 — 5
Full terms and conditions of use: http://www.informaworld.com/terms-and-conditions-of-access.pdf
This article may be used for research, teaching and private study purposes. Any substantial orsystematic reproduction, re-distribution, re-selling, loan or sub-licensing, systematic supply ordistribution in any form to anyone is expressly forbidden.
The publisher does not give any warranty express or implied or make any representation that the contentswill be complete or accurate or up to date. The accuracy of any instructions, formulae and drug dosesshould be independently verified with primary sources. The publisher shall not be liable for any loss,actions, claims, proceedings, demand or costs or damages whatsoever or howsoever caused arising directlyor indirectly in connection with or arising out of the use of this material.

8/13/2019 Adaptive Dose-Finding Based on Efficacy-Toxicity Trade-Offs
http://slidepdf.com/reader/full/adaptive-dose-finding-based-on-efficacy-toxicity-trade-offs 2/7
Adaptive Dose-Finding Based onEfficacy-Toxicity Trade-Offs
Peter F. ThallJohn D. CookDepartment of Biostatistics and Applied Mathematics, University of Texas,M.D. Anderson Cancer Center, Houston, Texas, U.S.A.
AbstractClinical trials in which both efficacy (E ) and toxicity (T ) are used to choose doses adaptively for suc-cessive cohorts of patients based on the accumulating dose-outcome data are commonly called‘‘phase I-II’’ trials. We describe a Bayesian method[1,2] for the design and conduct of such trials thatutilizes two types of decision criteria, each defined in terms of the probabilities pE (x, h ) and pT (x, h )of E and T for a patient given dose x, where h denotes the model parameter vector. The first criterionconsists of a fixed lower limit ppT p on pE (x, h ) and a fixed upper limit p on pT (x, h ), which are usedtogether to determine whether x is acceptable. The second criterion is a set of elicited target prob-ability pairs p ¼ (pE ,pT ) that embody equally desirable trade-offs between E and T . These elicitedtarget trade-offs pairs are used to construct a function giving the distance between a given (pE ,pT )pair and the ideal point (1, 0) corresponding to certain efficacy without toxicity. Pairs closer to
the ideal are more desirable. The function is constructed so that the elicited pairs are equally distantfrom the ideal. Each time a dose must be chosen based on the current interim data, D, the desirabilityof each acceptable dose x is defined to be the desirability of the contour containing the pair of poster-ior means Eðpðx; yÞ jDÞ ¼ ðEfpE ðx; yÞ jDg; EfpT ðx; yÞ jDgÞ. The next cohort is then given the mostdesirable dose, and this criterion also is used to select a best dose at the end of the trial.
INTRODUCTION
Clinical trials in which both efficacy (E ) and toxicity (T )are used to choose doses adaptively for successivecohorts of patients based on the accumulating dose-outcome data are commonly called ‘‘phase I–II’’ trials.
We describe a Bayesian method[1,2]
for the design andconduct of such trials that utilizes two types of decisioncriteria, each defined in terms of the probabilitiespE (x, y)andpT (x, y) of E and T for a patient given dose x, where ydenotes the model parameter vector. The first criterionconsists of a fixed lower limit pE on pE (x,y) and a fixedupper limit ppT on pT (x, y), which are used together todetermine whether x is acceptable. The second criterionis a set of elicited target probability pairs p ¼ (pE ,pT )that embody equally desirable trade-offs between E
and T . These elicited target trade-offs pairs are used toconstruct a function giving the distance between a given(pE ,pT ) pair and the ideal point (1, 0) corresponding to
certain efficacy without toxicity. Pairs closer to the idealare more desirable. The function is constructed so thatthe elicited pairs are equally distant from the ideal. Eachtime a dose must be chosen based on the current interimdata, D, the desirability of each acceptable dose x isdefined to be the desirability of the contour containingthe pair of posterior means E ðpðx; yÞ jDÞ ¼ðE fpE ðx; yÞ jDg; E fpT ðx; yÞ jDgÞ. The next cohort isthen given the most desirable dose, and this criterion alsois used to select a best dose at the end of the trial.
DOSE–OUTCOME MODELS
Let Y ¼ (Y E , Y T ) be the binary indicators of E and T .The bivariate probabilities pa;bðx; yÞ ¼ PrðY E ¼ a;Y T ¼ b j x; yÞ for a; b 2 f0; 1g are formulatedin terms of the marginal probabilities pT ðx; yÞ ¼
p1;1ðx;yÞ þp0;1ðx;yÞ ¼ logit1
fZT ðx;yÞg and pE ðx; yÞ ¼p1;1ðx; yÞ þ p1;0ðx; yÞ ¼ logit1 fZE ðx; yÞg, and anassociation parameter, c. For toxicity, ZT ðx; yÞ ¼mT þ xbT . For efficacy ZE ðx; yÞ ¼ mE þ xbE ;1 þx2bE ;2,a flexible form allowing pE (x, y) to be non-monotonein x, which is particularly important in trials of bio-logic agents. Thus, y ¼ ðmT ; bT ; mE ; bE ;1; bE ;2; cÞ.
Suppressing x and y, the bivariate model[3,4] is
pa;b ¼ ðpE Það1 pE Þ
1aðpT Þbð1 pT Þ
1b
þ ð1ÞaþbpE ð1 pE ÞpT ð1 pT Þ
ec 1
ec þ 1
ð1Þ
and the likelihood for a patient treated at dose x is
LðY; x jyÞ ¼ p1;1ðx; yÞY E Y T p1;0ðx; yÞY E ð1Y T Þ
p0;1ðx; yÞð1Y E ÞY T p0;0ðx; yÞð1Y E Þð1Y T Þ
ð2Þ
where p0,0 ¼ 1 (p1,1 þ p1,0 þ p0,1). Given dose–outcome data Dn ¼ fðY 1; xð1ÞÞ; : : :; ðY n; xðnÞÞg from
Encyclopedia of Biopharmaceutical Statistics DOI: 10.1081/E-EBS-120041935Copyright # 2006 by Taylor & Francis. All rights reserved. 1

8/13/2019 Adaptive Dose-Finding Based on Efficacy-Toxicity Trade-Offs
http://slidepdf.com/reader/full/adaptive-dose-finding-based-on-efficacy-toxicity-trade-offs 3/7
the first n patients in the trial, the likelihood isLnðDn jyÞ ¼ P
ni¼1LðYi; xðiÞ jyÞ. The method also
accommodates the case of trinary outcomes when E
and T are disjoint, so that (Y E , Y T ) ¼ (1, 1) cannotoccur. The reader is referred to Thall and Cook [1] fordetails of the model dealing with this case.
ESTABLISHING PRIORS
The prior must represent the physician’s uncertainty,provide a reliable basis for decision-making, and besufficiently uninformative to allow the accumulatingdata to dominate the posteriors and hence the deci-sions. We assume that each component yl of y isnormally distributed with mean ml and standard devia-tion (sd) sl. For each dose xj , j ¼ 1, . . . , K , and out-come y ¼ E,T , let my,j (x) and sy,j (x) denote the priormean and sd of py(xj , y). To obtain the 2p-vector of hyperparameters, x ¼ (m1,s1,m2,s2, . . . ,mp,sp) for each
xj we elicit the means mðeÞ
E ;j and m
ðeÞ
T ;j of pE (xj , y) andpT (xj , y) that the physician expects a priori at thatdose. One may also elicit prior credible intervalsaround pE (xj , y) and pT (xj , y) to obtain values of
sðeÞE ;j and s
ðeÞT ;j , restricted to be in the range 0.29–0.50,
corresponding to beta distributions with parametershaving sum at most 2. We then treat the m
ðeÞy;j and
sðeÞT ;j values like data with means my,j (x) and sy,j (x), and
solve for the value of x that minimizes the sums of squares
Xy¼E ;T
Xk
j ¼1
mðeÞy;j my;j ðxÞn o2
þ sðeÞy;j sy;j ðxÞn o2
þ cX
1r <lp
ðsr slÞ2
The last sum is included as a penalty term, with c
approximately .10–.20, to ensure that the sr ’s do nothave different orders of magnitude, which tends todestabilize computation of posteriors. Details are givenin Thall and Cook.[1]
DECISION CRITERIA
Dose Acceptability
The dose-finding algorithm utilizes two different typesof criteria, both based on the current posteriorf (y j Dn). The first criterion is a pair of probabilitylimits used to determine the set of acceptable doses,to control the risks of unacceptably high toxicity orunacceptably low efficacy. The second is a geometricmethod for choosing a best acceptable dose. Let pE
and ppT be fixed lower and upper limits on the probabil-ities of E and T , specified by the physician, and let pE
and pT be fixed probability cut-offs. A dose xj hasacceptable efficacy if
Pr pE ðxj ; yÞ > pE jDn
> pE ð3Þ
and xj has acceptable toxicity if Pr pT ðxj ; yÞ < ppT jDn
> pT ð4Þ
A dose is acceptable if it satisfies both (3) and (4),or if it is the lowest untried dose and satisfies (4).The set of acceptable doses based on current data Dn
is denoted by A(Dn).
Efficacy–Toxicity Trade-Offs
If no dose is acceptable, then the trial is terminated.This is a substantive departure from rules for conduct-
ing conventional phase I trials, as it ends a trial if alldoses are safe but none have acceptable efficacy. Inthe non-problematic case, where A(Dn) consists of asingle dose, it is assigned to the next cohort of patients.When A(Dn) contains two or more doses, however,an additional criterion for choosing among them isrequired. As ðpE ðxj ; yÞ; pT ðxj ; yÞÞ is two-dimensional,to compare doses in terms of these pairs of probabil-ities, each pair must somehow be represented by aone-dimensional object. The following geometric
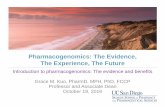
Fig. 1 Trade-off contours for the breast cancer trial design.The elicited target probability pairs (0.05,0), (0.20, 0.20), and(1.0,0.50) are given as points, the resulting efficacy–toxicitytrade-off contour C is given as a thick curve, and the remain-ing curves are trade-off contours generated from C.
2 Adaptive Dose-Finding Based on Efficacy-Toxicity Trade-Offs

8/13/2019 Adaptive Dose-Finding Based on Efficacy-Toxicity Trade-Offs
http://slidepdf.com/reader/full/adaptive-dose-finding-based-on-efficacy-toxicity-trade-offs 4/7
construction provides a basis doing this, and thusfor choosing the best among several acceptable doses.This construction is shown in Fig. 1 in the case of the breast cancer trial, described below, that we willuse to illustrate the method.
The trade-off between efficacy and toxicity is quan-tified by constructing a function based on the distancebetween a p ¼ (pE , pT ) pair and the ideal pair (1, 0).The basic idea is that the closer p is to the ideal point,the greater its desirability. The distance function isdetermined by three elicited target probability pairs,p
1;p2; p
3
, which the physician considers to be
equally desirable. The first point is p1 ¼ ðp
1;E ; 0Þ,where p
1;E is the smallest response that the physicianwould consider acceptable if toxicity were impossible.Next, p
2 ¼ ð1;p2;T Þ is obtained by asking the
physician for the largest value of pT that would beacceptable if efficacy were certain. For any q > 0,we may define the distance r of a (pE , pT ) pair to theideal pair (1, 0) by
r ¼ pE 1
p1;E 1
!q
þ pT
p2;T
!q( )1=q
This is the usual Lq distance with the pE and pT axesscaled, so that p
1 and p2 have unit distance to the ideal,
which causes the final elicited pair p3 to also have unit
distance to the ideal. We then define the desirability of
a (pE ,pT ) pair to be d ¼ 1 r . For additional details,see Ref.[5]. In Ref.[1], a distance function based on pT asan inverse quadratic function of pE was used. How-ever, the Lq approach provides greater flexibility, andit is straightforward to implement.
To utilize this structure for choosing the best accept-able dose from A(Dn), one first computes E fp(xj , y) jDng for each xj . The desirability of xj is then definedto be the d of the contour where E fp(xj , y) jDng falls.The use of an elicited trade-off contour as a device toreduce a two-dimensional parameter to a one-dimen-sional object for use as a decision criterion is not new.Thall, Sung, and Estey[6] employ a similar construct inthe context of a trial to compare two-stage treatmentstrategies in terms of the probabilities of response anddeath. More generally, such a contour is an example of an ‘‘indifference region’’[7] as all doses having the abovepair of posterior means falling on the same contour areequally desirable.
RULES FOR TRIAL CONDUCT
To use the above decision criteria to design andconduct a dose-finding a trial, one first establishesthe disease and trial entry criteria, the definitions of E and T , the treatment regime and the set of dosesx1, . . . , xK to be studied, a starting dose, a maximumsample size N , and a cohort size. Then, one elicits
Table 1 Selection percentages and sample sizes of the trade-off-based method for the biologic agent trial under each
of four dose-outcome scenariosDose (mg/kg)
Scenario 0.5 1.0 2.0 5.0 None
1 True (pE , pT ) (.02, .05) (.10, .08) (.15, .12) (.27, .15)
d 0.048 0.016 0.035 0.124
No. Patients 10.2 5.7 7.0 12.3
% Selected 7.8 13.7 20.6 53.7 4.8
2 True (pE , pT ) (.05, .05) (.12, .07) (.30, .10) (.10, .12)
d 0.017 0.044 0.204 0.016
No. Patients 14.2 4.1 10.5 5.4
% Selected 22.0 8.4 42.9 16.5 10.2
3 True (pE , pT ) (.25, .20) (.26, .45) (.28, .50) (.30, .52)
d 0.047 0.307 0.373 0.392
No. Patients 31.5 1.6 1.0 1.2
% Selected 90.6 2.5 0.8 1.3 4.8
4 True (pE , pT ) (.01, .30) (.03, .40) (.08, .55) (.12, .65)
d 0.302 0.421 0.609 0.743
No. Patients 7.9 4.5 4.1 4.1
% Selected 3.3 5.7 1.5 1.6 87.9
Adaptive Dose-Finding Based on Efficacy-Toxicity Trade-Offs 3

8/13/2019 Adaptive Dose-Finding Based on Efficacy-Toxicity Trade-Offs
http://slidepdf.com/reader/full/adaptive-dose-finding-based-on-efficacy-toxicity-trade-offs 5/7
the two limits pE ; ppT and the trade-off targetsp
1;p2; p
3
. The trial is conducted as follows:
1. Treat the first cohort at the starting dose.2. No untried dose may be skipped when escalating.3. If AðDnÞ 6¼ f, then treat the next cohort at the
x 2 AðDnÞ have largest d.
4. If AðDnÞ ¼ f, then stop the trial and do notselect any dose.5. If the trial is not stopped early andAðDN Þ 6¼ f,
then select the dose in AðDN Þ that maximizes d.
ILLUSTRATIVE TRIAL
We illustrate the method with a trial of a biologicagent for the treatment of metastatic breast cancerthat is resistant to conventional chemotherapy. Eachpatient receives a dose of 0.5, 1.0, 2.0, or 5.0 mg/kg
of the agent, given by intravenous infusion. Toxicityis defined as death or NCI grade 3 or 4 hematologicaltoxicity, flu-like symptoms, skin rash, or other unex-pected toxicities occurring within 28 days of thestart of therapy. Efficacy is defined as less than fivecirculating tumor cells per 7.5 cubic centimeters of blood at day 21. A maximum of 36 patients will betreated in cohorts of size three, with the first cohorttreated at the lowest dose, 0.5. The elicited means of p used to construct a prior are (0.01, 0.05) for dose0.5, (.03, 0.15) for dose 1.0, (.05,0.20) for dose 2.0,and (0.10, 0.25) for dose 5.0. The fixed acceptabilitylimits are ppT ¼ 0:30 and pE ¼ 0:10, with decisioncut-off probabilities pE ¼ 0.05 and pT ¼ 0.10. Thethree elicited targets for defining C are (0.05,0),(0.20, 0.20), and (1.00, 0.50), and Lq norm trade-off con-tours were used. The upper limit of 0.30 on pT ðxj ; yÞisa very commonly used value in phase I trials based ontoxicity alone. The very low limit on pE ðxj ; yÞ was estab-lished toensurea minimal level ofantidisease effect, andin
Fig. 2 Dose-outcome curves of the four scenarios used in the simulation study of the design for the breast cancer trial. Toxicityprobabilities pT (x) are given as triangles connected by dashed lines, efficacy probabilities pE (x) are given as round dots connectedby dotted lines, and the fixed limits pE ¼ :10 and ppT ¼ :30 are given as solid horizontal lines.
4 Adaptive Dose-Finding Based on Efficacy-Toxicity Trade-Offs

8/13/2019 Adaptive Dose-Finding Based on Efficacy-Toxicity Trade-Offs
http://slidepdf.com/reader/full/adaptive-dose-finding-based-on-efficacy-toxicity-trade-offs 6/7
this sense the goal in terms of efficacy is that of a conven-tional phase IIA or ‘‘activity’’ trial.[8,9] Taken together,these two limits illustrate the manner in which the designcombines conventional phase I and phase II goals.
Computer simulation results summarizing thisdesign’s average behavior under four dose-outcomescenarios are summarized in Table 1. The simulationscenarios are shown graphically in Fig. 2. The trialwas simulated 1000 times under each scenario. In Sce-nario I, toxicity is acceptable for all four doses, and thethree highest doses all have acceptable efficacy, with pE
increasing monotonically in xj , so that the highest doseis most desirable. The selection probabilities and sam-ple sizes show that the method detects this pattern,making a correct decision 88% of the time and selectingthe best dose 54% of the time. Scenario 2 differs fromScenario 1 in that pE is not monotone in dose, firstincreasing to 0.30 at dose 2.0, but then decreasing to0.10 at dose 5.0. The algorithm detects this pattern,selecting an acceptable dose 68% of the time and select-
ing the best dose 43%
of the time. In Scenario 3, only thelowest dose is acceptable, as the three highest doses areall unacceptably toxic. Themethod selects theone accept-able dose 90.6% of the time in this case. In Scenario 4,no dose is acceptable, and the method correctly con-cludes that this is the case 88% of the time after treatingon average only 12 of the maximum 36 patients.
Although we have given the design’s operatingcharacteristics under each of four hypothetical dose–outcome scenarios for the purpose of illustration, inpractice there are many possibilities, and examiningas many as eight different scenarios is common whenimplementing this design. Moreover, while we have
reported the operating characteristics under the partic-ular design parameterization actually used in the trial,a much larger number of parameterizations wereexamined in preliminary simulations as a basis forchoosing a design. This process should be a standardpractice when applying this method, as a given design’sproperties vary substantially with the choice of designparameters.
CONCLUSIONS
A variety of other methods for dose finding using
efficacy and toxicity have been proposed.[10–14] Thetrade-off-based method described here is considerablymore structured than most other methods, and apply-ing it requires a substantial effort from both thestatistician and the physician. However, the methodis both scientifically and ethically attractive as itaccounts for both efficacy and toxicity, it uses a quan-tification of the trade-offs between these two outcomesto choose doses, and the design parameters may becalibrated quite easily using computer simulation to
obtain good operating characteristics. An essentialaspect of the method is that various numerical valueselicited from the physician play a critical role inconstructing the design. Consequently, the design clos-ely reflects the physician’s beliefs and goals rather thansome arbitrary statistical criterion.
The method is computationally intensive, both inthe design stage and during trial conduct, as one mustrepeatedly compute the posteriors each time new databecome available. Moreover, many computationsbased on each posterior must be carried out, includingthe evaluation of E fpy(xj , y) j Dg for each xj andy ¼ E,T and the acceptability criteria. The repeateduse of computer simulations when designing the trialrequires all of these computations be carried out thou-sands of times so establishing a design’s operatingcharacteristics is extremely computationally intensive.Consequently, specialized computer software isrequired to implement the method. This software,‘‘EffTox,’’ is freely available at http://biostatistics.
mdanderson.org/SoftwareDownload.
ACKNOWLEDGMENT
Peter Thall’s research was partially supported by NIHgrant R01 CA 83932.
ARTICLES OF FURTHER INTEREST
Adaptive Designs, p. 001.
Bayesian Statistics, p. 072.Cancer Trials, p. 152.Clinical Endpoint, p. 189.Clinical Trial Simulation, p. 200.Clinical Trials, p. 202.Dose Response Study Design, p. 304.Maximum Tolerable Dose for Cancer
Chemotherapy, p. 554.Multiple Endpoints, p. 656.Phase I Cancer Clinical Trials, p. 001.
REFERENCES
1. Thall, P.F.; Cook, J.D. Dose-finding based on efficacy-toxicity trade-offs. Biometrics 2004, 60, 684–693.
2. Thall, P.F.; Russell, K.T. A strategy for dose-findingand safety monitoring based on efficacy and adverseoutcomes in phase I/II clinical trials. Biometrics 1998,54, 251–264.
3. Prentice, R.L. Correlated binary regression with covari-ates specific to each binary observation. Biometrics1988, 44, 1033–1048.
Adaptive Dose-Finding Based on Efficacy-Toxicity Trade-Offs 5

8/13/2019 Adaptive Dose-Finding Based on Efficacy-Toxicity Trade-Offs
http://slidepdf.com/reader/full/adaptive-dose-finding-based-on-efficacy-toxicity-trade-offs 7/7
4. Murtaugh, P.A.; Fisher, L.D. Bivariate binary modelsof efficacy and toxicity in dose-ranging trials. Commu-nic. Stat., Part A - Theory Meth. 1990, 19, 2003–2020.
5. Thall, P.F.; Cook, J.D. Adaptive dose selection usingefficacy-toxicity trade-offs: illustrations and practicalconsiderations. J. Biopharm. Stat. In press.
6. Thall, P.F.; Sung, H.-G.; Estey, E.H. Selecting therapeu-tic strategies based on efficacy and death in multi-course
clinical trials. J. Am. Stat. Assoc., 2002, 97 , 29–39.7. DeGroot, M.H. Optimal Statistical Decisions; McGraw-Hill: New York, 1970.
8. Gehan, E.A. The determination of the number of patients required in a follow-up trial of a new che-motherapeutic agent. J. Chronic Dis. 1961, 13, 346–353.
9. Thall, P.F.; Sung, H-G. Some extensions and applica-tions of a Bayesian strategy for monitoring multiple
outcomes in clinical trials. Stat. Med. 1998, 17 ,1563–1580.
10. Gooley, T.A.; Martin, P.J.; Fisher, L.D.; Pettinger, M.Simulation as a design tool for phase I/II clinical trials:an example from bone marrow transplantation. Control.Clinic. Trials 1994, 15, 450–462.
11. O’Quigley, J.; Hughes, M.D.; Fenton, T. Dose-findingdesigns for HIV studies. Biometrics 2001, 57 , 1018–1029.
12. Braun, T. The bivariate continual reassessment method:extending the CRM to phase I trials of two competingoutcomes. Control. Clinic. Trials 2002, 23, 240–256.
13. Ivanova, A. A new dose-finding design for bivariateoutcomes. Biometrics 2003, 59, 1001–1007.
14. Bekele, B.N.; Shen, Y. A Bayesian approach to jointlymodeling toxicity and biomarker expression in a phaseI/II dose-finding trial. Biometrics 2004, 60, 343–354.
6 Adaptive Dose-Finding Based on Efficacy-Toxicity Trade-Offs