Acute Uncomplicated Type B Aortic Dissection: The UT …€¦ · Department of Cardiothoracic &...
37
Department of Cardiothoracic & Vascular Surgery McGovern Medical School / The University of Texas Health Science Center at Houston Acute Uncomplicated Type B Aortic Dissection: Type B Aortic Dissection: The UT Houston Experience Ali Azizzadeh, MD Professor & Chief Professor & Chief Program Director in Vascular Surgery Department of Cardiothoracic and Vascular Surgery McGovern Medical School The University of Texas Science Center at Houston The University of Texas Science Center at Houston Memorial Hermann Heart & Vascular Institute
-
Upload
phamnguyet -
Category
Documents
-
view
217 -
download
4
Transcript of Acute Uncomplicated Type B Aortic Dissection: The UT …€¦ · Department of Cardiothoracic &...
Department of Cardiothoracic & Vascular SurgeryMcGovern Medical School / The University of Texas Health Science Center at Houston
Acute UncomplicatedType B Aortic Dissection:Type B Aortic Dissection:The UT HoustonExperience
Ali Azizzadeh, MDProfessor & ChiefProfessor & ChiefProgram Director in Vascular Surgery
Department of Cardiothoracic and Vascular SurgeryMcGovern Medical SchoolThe University of Texas Science Center at HoustonThe University of Texas Science Center at HoustonMemorial Hermann Heart & Vascular Institute

Disclosures
Consultant
WL Gore WL Gore
Medtronic

Epidemiology
10-15 cases/100,000adults/yearadults/year
2/3 type A
1/3 type B 1/3 type B
Acute Type B
30% Cx 30% Cx
70% UnCx 70% UnCx
Male: Female 2-5:1

Classifications of Dissection:Stanford and DeBakeyStanford and DeBakey

Treatment of ATBAD
3° Referral Center
Multi-specialty team: Multi-specialty team: CT, Vasc Surg
Critical care
Consultants Consultants
Advanced imaging: CT, MR, IVUS, TEE CT, MR, IVUS, TEE
Hybrid OR’s
Monitoring MEP, SSEP
Full spectrum of Full spectrum ofopen/endovascularproceduresprocedures

Protocol
Admit CVICUCVC, arterial line, UOP
Admit CVICUCVC, arterial line, UOPCVC, arterial line, UOPCVC, arterial line, UOP
B -BlockerB -BlockerAnti-impulse Therapy
SBP<120, HR<60Control pain
Anti-impulse TherapySBP<120, HR<60
Control pain
B -Blocker
Ca+2 Blocker
Nitroglycerin
B -Blocker
Ca+2 Blocker
Nitroglycerin
Respiratory
DVT prevent
Nutrition
Respiratory
DVT prevent
NutritionControl painControl painNitroprussideNitroprusside
Nutrition
Mobilization
Nutrition
Mobilization
Reassessment
Blood pressure
Pain
Reassessment
Blood pressure
PainPainPain

Protocol
Percutaneous InterventionSurgical Intervention
Percutaneous InterventionSurgical Intervention
Rupture/ LeakRupture/ LeakRupture/ LeakMalperfusion (renal, visceral, peripheral)
Acute ExpansionRefractory Symptoms
Rupture/ LeakMalperfusion (renal, visceral, peripheral)
Acute ExpansionRefractory SymptomsRefractory SymptomsRefractory Symptoms

Acute Type B Aortic Dissection
2000 to 2014
1079 pts AD
532 ATBAD 532 ATBAD
60% Male
Mean age 60.6 ± 13.6 yrs Mean age 60.6 ± 13.6 yrs
Median age = 60.5 yrs
Range 16 –98 yrs Range 16 –98 yrs
Average Follow up: 3.7 yrs

Aortic Dissection
1079 DISSECTIONS

Aortic Dissection
535 532535TYPE A
532TYPE B
1079 DISSECTIONS

Aortic Dissection
294
535
294UNCOMPLICATED
535TYPE A
238COMPLICATED
1079 DISSECTIONS
COMPLICATED

Complicated ATBAD
Rupture
Malperfusion: Malperfusion:
Neurologic
Spinal Cord Spinal Cord
Visceral (Celiac, SMA)
Renal Renal
Lower Limb
Refractory Pain & HTN Refractory Pain & HTN

Goals of TEVAR for cATBAD
Seal off proximal entry tear
Alleviate malperfusion
Expand compressed true Expand compressed truelumen
Induce false lumen thrombosis Induce false lumen thrombosis
Prevent/treat rupture
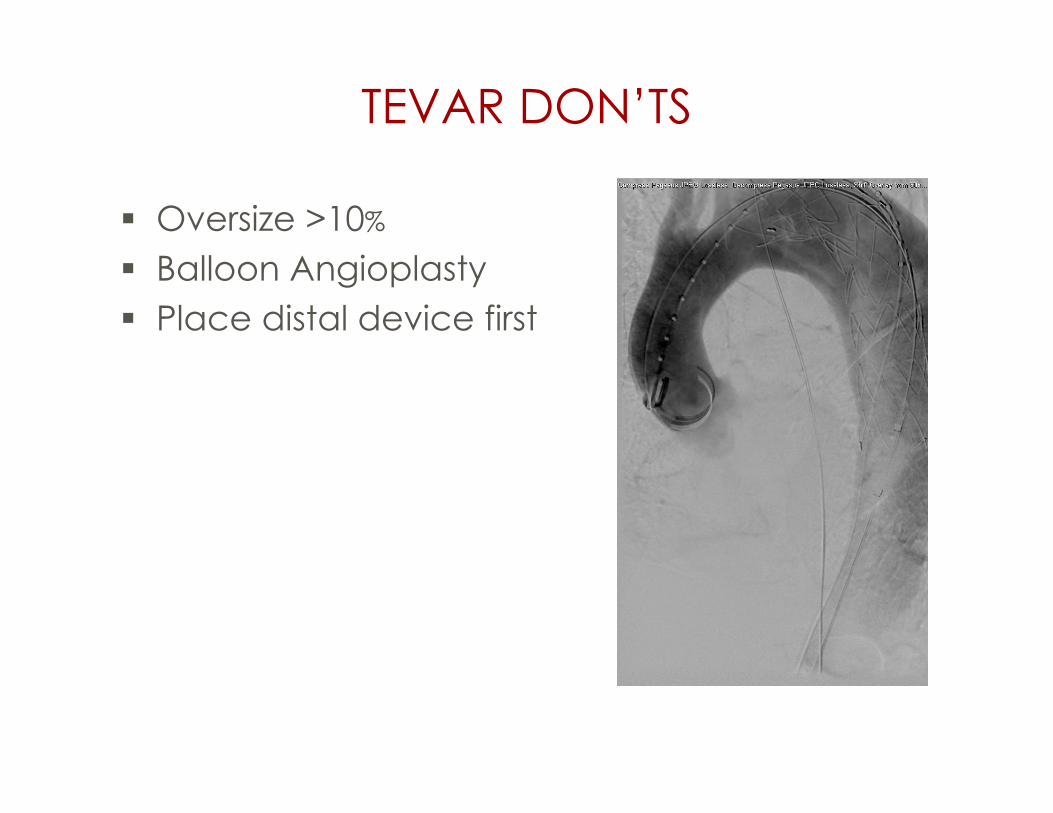
TEVAR DON’TS
Oversize >10%
Balloon Angioplasty Balloon Angioplasty
Place distal device first

IVUS
Adjunct to CTA,angiogram and TEEangiogram and TEE
Wire placement intrue lumen
Assesses adequacyof treatment
Guide additional Guide additionaltherapy
Diagnose Diagnosecomplications

Mortality by Management Strategy
Total = 444Uncomplicated
C o m p l i c a t e d ( N = 1 7 3 )OR,
Total = 444Uncomplicated
N=271OR,
p-valueMedN=69
OpenN=52
TEVARN=37
Other CVN=15
Mortality5 13 6 5 3
* 8.8, 0.0001Mortality5
1.9%13
18.8%6
11.5%5
13.5%3
20%* 8.8, 0.0001
* Uncomplicated compared to complicated type b aortic dissection

Survival at 5 yrs forSurvival at 5 yrs foruATBAD was 76.6%

Uncomplicated ATBAD
Early intervention appears reasonable in following scenarios:
• Initial aortic diameter ≥ 4.0cm with patent false lumen• Initial aortic diameter ≥ 4.0cm with patent false lumen
• ≥ 22mm false lumen in proximal DTA
• Proximal entry tear size >10mm• Proximal entry tear size >10mm
• Recurrent/refractory pain or HTN
• Well-designed, prospective, randomized trial needed• Well-designed, prospective, randomized trial needed

Purpose
To determine which factors predisposepatients with uncomplicated acute type Bpatients with uncomplicated acute type B
aortic dissections to worse outcomes,including mortality and need for intervention.including mortality and need for intervention.

Acute Type B Aortic Dissections
PATIENTS WITH ACUTE TYPE B DISSECTION532532
294 238UNCOMPLICATED294 COMPLICATED238
Inadequate120
InadequateImaging120
Abdominal11
156
IMH / PAU7
WITH ADEQUATE IMAGING DATA ANALYSIS156

Methods Measurement: Measurement: TeraRecon(Foster City, CA) Multi-planar reconstruction Multi-planar reconstruction Double orthogonal oblique
measures
Proximal descending aorta FL Proximal descending aorta FLdiameter and area: level ofmain pulmonary artery
Maximum aortic diameter on Maximum aortic diameter onadmission
Measurements by specializedcardiovascular radiologistcardiovascular radiologist

Overall Survival: Max AorticDiameterDiameter

Overall Survival: False LumenDiameterDiameter

Overall Survival: Age

Intervention-free Survival:Max Aortic DiameterMax Aortic Diameter

Intervention-free Survival:False Lumen DiameterFalse Lumen Diameter

Intervention-free Survival:Max Aortic Diameter (Quartiles)Max Aortic Diameter (Quartiles)

Intervention Rates
Overall Intervention rate:
>44mm: 34.4%
≤44mm: 11.3%
(OR 4.12, p=0.02) (OR 4.12, p=0.02)
The 1,5,and 10 year intervention rates
Intervention Rate (%)
Admission Aortic Diameter (mm) 1 year 5 years 10 years
>44 18.8 29.5 50.3
≤44 4.8 13.3 13.3≤44 4.8 13.3 13.3

Intervention Rates
Intervention Rate (%)
Admission Aortic 1 5 10Admission AorticDiameter (mm)
1year
5years
10years
>44 18.8 29.5 50.3>44 18.8 29.5 50.3
≤44 4.8 13.3 13.3
Overall Intervention rate:
>44mm: 34.4% >44mm: 34.4%
≤44mm: 11.3%
(OR 4.12, p=0.02)
The 1,5,and 10 year intervention rates

Incidence of Risk Factors in AUTBAD
Risk FactorsRisk Factors
TAD >44mm / FLD >22 / Age >60
1 Risk Factor 44%1 Risk Factor 44%
2 Risk Factors 19%
3 Risk Factors 6%
Total 69%

Conclusions
Aortic diameter >44mm is a predictor ofmortality after adjustment for significantmortality after adjustment for significantrisk factors.
Age >60 years is a risk factor for mortality.
Decreased intervention-free survival in Decreased intervention-free survival inthose with FL>22mm and/or max aorticdiameter >44mm on admission.diameter >44mm on admission.
Patients with Aortic diameter >44mm,FL>22mm, and/or age>60 should beFL>22mm, and/or age>60 should beconsidered for TEVAR.

Department of Cardiothoracic & Vascular SurgeryMcGovern Medical School / The University of Texas Health Science Center at Houston
The Impact of Arch Involvement in AcuteType B Aortic Dissection
Hunter M. Ray, Kristofer M. Charlton-Ouw, Anthony L. Estrera,Charles C. Miller, Hazim J. Safi, Ali Azizzadeh
Type B Aortic Dissection
Charles C. Miller, Hazim J. Safi, Ali Azizzadeh
Department of Cardiothoracic and Vascular SurgeryMcGovern Medical School / The University of Texas Science Center at HoustonMemorial Hermann Heart & Vascular Institute

Department of Cardiothoracic & Vascular SurgeryMcGovern Medical School / The University of Texas Health Science Center at Houston
Ascending Aortic Size is a Predictor ofOutcomes in Patients with Uncomplicated
Hunter M. Ray, Joseph M. Besho, Jason Au, Kristofer M.Charlton-Ouw, Anthony L. Estrera, Charles C. Miller, Hazim J.
Outcomes in Patients with UncomplicatedAcute Type B Aortic Dissection
Charlton-Ouw, Anthony L. Estrera, Charles C. Miller, Hazim J.Safi, Ali Azizzadeh
Department of Cardiothoracic and Vascular SurgeryMcGovern Medical School / The University of Texas Science Center at HoustonMcGovern Medical School / The University of Texas Science Center at HoustonMemorial Hermann Heart & Vascular Institute

Thank You