Acute Respiratory Distress Syndrome · 2019-10-14 · Acute Respiratory Distress Syndrome Although...
45
Courtesy of Drs. Faraaz Shah and Bryan McVerry Acute Respiratory Distress Syndrome Although not included in the Berlin Definition, the underlying pathophysiology is important to remember in the management of ARDS ARDS is under-recognized, how can we better identify patients at risk for ARDS? Lung Injury Prediction Score (LIPS) Predisposing Conditions Points Risk Modifiers Points Sepsis 1.5 Alcohol use 1 Shock 1.5 Tobacco use 0.5 Trauma 0.5 Hypoalbuminemia 2 Pneumonia 0.5 Diabetes -1.5 Aspiration 1.5 Chemotherapy 2 Pancreatitis 1.5 FiO2 > 0.35 1 Elective Surgery 1.5 Tachypnea 1 Emergency Surgery 2 LIPS < 4 has a high negative predictive value, odds of ARDS increase with higher scores Trigger Inflammatory and Chemical Mediators Alveolar Injury • Epithelial • Endothelial Surfactant dysfunction Capillary leak Capillary thrombi Vasoconstriction Shunt- Hypoxemia Decreased compliance Increased dead space Decreased aerated lung Berlin Definition Timing Within 1 week of a known clinical insult, or new or worsening respiratory symptoms Chest Imaging Bilateral opacities not fully explained by effusions, lobar collapse, or lung nodules Origin of Edema Respiratory failure not fully explained by cardiac failure or fluid overload (an objective assessment [ex- TTE] to exclude hydrostatic edema is warranted if no trigger is identified) Oxygenation Mild: 200 < P/F ratio ≤ 300 with PEEP ≥ 5 or CPAP ≥ 5 Moderate: 100 < P/F ratio ≤ 200 with PEEP ≥ 5 Severe: P/F ratio ≤ 100 with PEEP ≥ 5
Transcript of Acute Respiratory Distress Syndrome · 2019-10-14 · Acute Respiratory Distress Syndrome Although...

Courtesy of Drs. Faraaz Shah and Bryan McVerry Acute Respiratory Distress Syndrome
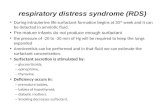
Although not included in the Berlin Definition, the underlying pathophysiology is important to remember in the management of ARDS
ARDS is under-recognized, how can we better identify patients at risk for ARDS?
Lung Injury Prediction Score (LIPS)
Predisposing Conditions Points Risk Modifiers Points Sepsis 1.5 Alcohol use 1 Shock 1.5 Tobacco use 0.5 Trauma 0.5 Hypoalbuminemia 2 Pneumonia 0.5 Diabetes -1.5 Aspiration 1.5 Chemotherapy 2 Pancreatitis 1.5 FiO2 > 0.35 1 Elective Surgery 1.5 Tachypnea 1 Emergency Surgery 2 LIPS < 4 has a high negative predictive value, odds of ARDS increase with higher scores
Trigger Inflammatory and Chemical Mediators
Alveolar Injury• Epithelial• Endothelial
Surfactant dysfunction
Capillary leakCapillary thrombiVasoconstriction
Shunt- HypoxemiaDecreased complianceIncreased dead space
Decreased aerated lung
Berlin Definition
Timing Within 1 week of a known clinical insult, or new or worsening respiratory symptoms
Chest Imaging Bilateral opacities not fully explained by effusions, lobar collapse, or lung nodules
Origin of Edema Respiratory failure not fully explained by cardiac failure or fluid overload (an objective assessment [ex- TTE] to exclude hydrostatic edema is warranted if no trigger is identified)
Oxygenation Mild: 200 < P/F ratio ≤ 300 with PEEP ≥ 5 or CPAP ≥ 5
Moderate: 100 < P/F ratio ≤ 200 with PEEP ≥ 5
Severe: P/F ratio ≤ 100 with PEEP ≥ 5

Courtesy of Drs. Faraaz Shah and Bryan McVerry ARDS is under-treated, start appropriate treatments early instead of as salvage therapies
Effects of ARDS last long after the inciting event, start thinking of your patients as survivors when they enter the ICU
Mortality In-hospital mortality globally ~ 40%
1 year mortality in survivors is 20-25%
Lung function Spirometry and DLCO recover to normal levels at 1 year
Survivors will still report dyspnea and difficulty with exertion
Cognitive deficits Discharge- 70-100% of survivors report some cognitive impairment
1 year: 45-80%
5 year: 20%
Psychiatric disease New or worsened psychiatric disease including depression, PTSD, and anxiety is reported in 40-60% of survivors and persists 2+ years in many studies
Physical function Musculoskeletal weakness has been observed in 35-70% of survivors at hospital discharge and is associated with worse 1 and 5 year survival.

CourtesyofDr.IanBarbashCoreConference:Anaphylaxis
ByMikaelHäggström-Ownwork,CC0,https://commons.wikimedia.org/w/index.php?curid=17700404
SpickettandSproud.ClinicalMedicine2011;11(4):390-96
KempandLockey.JAllergyClinImmunology.2002;110:341-8

Approach to Difficult Asthma Step 1: Confirm an asthma diagnosis and identify difficult to treat asthma • Obtain pre and post bronchodilator spirometry- need at least 12% and 200mL improvement in FEV1 Asthma Mimicker with normal spirometry: Vocal Cord dysfunction • Think about - symptoms out of proportion to FEV1, atypical spirometry, poor response to meds • Symptoms: cannot get air in, dry cough, chest tightness below the neck • Long history of “asthma exacerbations” on high doses of medications and poor response • Episodic cough and dyspnea around irritants- perfumes, etc.. • Flat inspiratory loop on spirometry • Diagnose with laryngoscopy Asthma Mimickers with abnormal spirometry Obstructive Restrictive COPD Obesity ABPA Mixed Constrictive bronchiolitis Hypersensitivity Eosinophilic granulomatosis (Churg-Strauss) Eosinophilic granulomatosis (Churg-Strauss) Asthmatic Granulomatosis Step 2: Differentiate severe asthma from milder asthma • Requires treatment with high dose ICS plus a second controller
Compliance is complicated- don’t like taking inhalers, expensive, sign of weakness, forgetfulness, they don’t work. Watch the patient use their inhaler to ensure they are doing it right! Comorbidities that make asthma worse: • obesity • GERD • Chronic sinusitis Step 3: Determine whether severe asthma is controlled or uncontrolled Any one of the following qualifies as uncontrolled: • Symptom control: ACQ >1.5 or ACT <20 over 3 months • Exacerbations: 2 or more steroid bursts OR 1 hospitalization in the last year • Airflow limitation: FEV1 <80% predicted with reduced ratio
Consider biomarkers to identify presence of Type-2 cytokine signature Th2-Hi Type 2-Lo Atopy, high eosinophils, high exhaled NO Absence of atopy, eos, NO Respond to inhaled corticosteroid Associated with poor corticosteroid response late onset, obesity- responds to weight loss
Maximize corticosteroids for type-2 Hi (atopic, high eos, high FeNO). For those who remain uncontrolled, consider alternatives such as T2 targeted therapies (anti IL-4 dupilumab, anti-IL-5 mepolizumab and resilizumab) and diagnostic biopsy if needed.


Chronic Obstructive Pulmonary Disease Management Based on 2017 GOLD criteria Symptoms Risk Therapy A CAT<10, MRC 0-1 ratio <0.7 and FEV1 ≥50% (GOLD I, II) AND 0-1
exacerbations/yr LAMA or LABA
B CAT ≥10, MRC ≥2 ratio <0.7 and FEV1 ≥50% (GOLD I, II) AND 0-1 exacerbations/yr
1. LABA or LAMA 2. LAMA + LABA Pulmonary rehab
C CAT <10, MRC 0-1 ratio <0.7 and FEV1 ≤50% (GOLD III, IV) AND ≥ 2 exacerbations/yr or 1 hospitalization
1. LABA+ICS or LAMA 2. LAMA + LABA Pulmonary rehab Consider PDE-4 inhibitor
D CAT ≥10, MRC ≥2 ratio <0.7 and FEV1 ≤50% (GOLD III, IV) AND ≥ 2 exacerbations/yr or 1 hospitalization
1. LABA+ICS and/or LAMA 2. ICS+LABA+PDE4 Pulmonary rehab Consider surgery
* COPD Assessment Test (CAT): http://www.catestonline.org Ratio <70 over-diagnoses patients the older they get! So, when reading PFTs, don’t overcall obstruction for older patients. Comorbidities in COPD are higher compared to an age adjusted population: CAD Osteoporosis depression Cancer ** 50% of COPD discharges have CHF and/or CAD and COPD is an independent predictor of CVD mortality.
Risks for exacerbation: • Any exacerbation in the last year • Chronic wheezing and asthma • Every 100cc decrease in FEV1 • Plasma fibrinogen and eosinophils are possible biomarkers
The BODE index Variable Points on BODE index 0 1 2 3 FEV1 % >65 50-65 35-50 <35 6 min walk distance >350 250-350 150-250 <150 MMRC dyspnea scale 0-1 2 3 4 BMI >21 <21 For a BODE score of 7-10, survival is 50% at 3 years- think about transplant survival (~50% at 5 years) Exacerbation reduction: • Fluticasone/salmeterol 250/50 – 30% reduction • Roflumilast – 25% reduction • Tiotropium – 14% reduction • Daily azithromycin – 27% reduction 5 days of corticosteroid is non-inferior to 14 day course in terms of re-exacerbations. The greatness of pulmonary rehabilitation: Efficacious and cost effective Improves functional performance Less than 2% with COPD participate Improves quality of life It is exercise, education, psychosocial support Decreases healthcare utilization Lung Volume Reduction Surgery • Most benefit: upper lobe emphysema with low exercise capacity- 30% reduction in exacerbations • High risk group: FEV <20% predicted, homogenous emphysema, DLCO <20% predicted

Diagnostic Approach to Cough
Take a history, but note: character and timing of the cough and presence or absence of sputum has been shown in one study to not help with the diagnosis. More importantly, look for symptoms suggesting an underlying diagnosis: asthma, GERD, bronchiectasis, etc…
90% of chronic cough cases are upper airway cough syndrome (post-nasal drip), asthma, and GERD. One study showed it was 99.4% in nonsmokers, not using an ACEi, and with normal CXR.
One approach: 1. postnasal drip is really common so start with empiric antihistamine-decongestant therapy. In one study this
was all that was needed in 36% and 87% got at least some benefit. 2. They smoke? Yep, that’s why they are coughing- tell them to stop. 3. Stop that ACE inhibitor 4. Infectious signs/symptoms- try some antibiotics (pertussis! Common and under-recognized) 5. Treat that GERD 6. Asthma can make you cough! Try some bronchodilators/ICS 7. If none of that is working- get a CXR
So what to do when there’s no obvious cause and CXR is normal? Some less conventional testing Diagnosis Test GERD Esophageal pH monitoring (BRAVO testing) Asthma not apparent on PFTs Methacholine test, exhaled NO Non-asthmatic eosinophilic bronchitis Sputum eosinophils, exhaled NO Upper airway cough syndrome Allergy skin testing and sinus CT And what if the cough still persists? Now you’re looking for weird stuff Diagnosis Test Lesions compressing upper airway- AVM, retrotracheal masses
HRCT scan
Esophagoscopy Tracheobronchomalacia, airway lesion, tracheal diverticuli Bronchoscopy PVCs EP study Laryngeal sensory neuropathy (these people clear their throat all the time)
Laryngeal EMG, videostroboscopy
“ear-cough”- cerumen or foreign body impaction (vagus nerve)
Look in their ears!
Holmes-Adie syndrome- autonomic dysfunction of the vagus nerve
Anisocoria, hyperhidrosis, abnormal DTRs
Psychogenic cough Sigh.. Post-infectious cough can last 3-8 weeks. So tell your patients (and yourself) to expect a cough for 2 months after something like pneumonia.

ChronicThromboembolicPulmonaryHypertensionAsareminder:pulmonaryhypertensiondiagnosisrequiresPAP>25andPCWP<15ItisunknownwhysomepatientswithpulmonaryembolismdevelopCTEPHandothersdonot.Someconsiderations:• CTEPHpatientsseemtohaveahigherlevelofFactorVIIIcomparedwithcontrols• Antiphospholipidantibodiesarepresentin10-20%ofCTEPHpatients• ActivatedproteinCresistanceandlevelsofantithrombin,proteinC&SdonotseemtoplayaroleinCTEPH
OneuniquephysicalexamfindinginCTEPHisaflowmurmuroverthelungfields.Theseareahigh-pitched,blowingbruitheardduringinspiration.Havethepatientinhaleandthenholdtheirbreath.NotdescribedinotherformsofPH.
DiagnosisVQscanistheinitialimagingprocedureofchoice RightHeartCatheterization• Differentiatesproximalissues(CTEPH)fromdistal
smallvesseltypes(PAH)• ThepearlhereisthatPApressuresmayonlybe
modestlyelevatedatrestanddisproportionatelyelevatedwithexercise.
• CTEPHhasoneorseveralsegmentalorlargermismatches.PAHhasmottledsubsegmentaldefects
• PHwithexercisebutnotatrestmayindicateCTEPH
• GreatersensitivitycomparedwithCTA(96vs51%) CT-angiography• Canunderestimatecentralvascularobstruction • Similarperformancetoangiographyforcentral
diseasebutlesssoforsegmentaldiseaseOtherPHdisordersthatshowlargersegmentaldefectsonVQ:PAsarcoma,PVOD,fibrosingmediastinitis,largevesselvasculitisTreatmentAnticoagulationisthemainstayoftherapy.~65–90%willresolvein12monthswithanticoagulation.Therearenodataatthistimeregardingchoiceofagentorduration.Risksforincompleteresolutiondespiteanticoagulationinclude:• Largethrombus • Longertimebetweensymptomsanddiagnosis • Olderage• Centrallocation • PriorhistoryofVTEPulmonaryThromboendarterectomyistheonlydefinitivetreatment.Surgicaloutcomesarerelatedtodecreasingthepulmonaryvascularresistance.IfthePVRdoesnotcomedownduetodistalthrombus,thenpooroutcomes-inabilitytoweanfrombypass,postophemodynamicinstability,anddeath.ThereshouldbehemodynamicabnormalitiesatrestonRCH,butifnot:• StillconsidersurgeryiftheyhavePHwithminimalexercise–thethoughtisthatthiswillprogresstoatrest• PatientswithonemainPAinvolvedhaveincreaseddeadspaceandhighminuteventilationrequirementwith
poorexercisecapacitywithouthemodynamicimpairmentThereare2mainpostoperativecomplicationsthatwillbeonyourboards!1. Pulmonaryarterysteal–incidenceis70%-referstoredirectionofbloodflowfromwell-erfusedsegmentstonely
endarterectomizedsegmentswithsubsequentVQmismatchingandhypoxemia.2. Reperfusionpulmonaryedema–30%incidence–non-cardiogenicedemaoccurringinlungwhereproximal
thrombuswasremoved.Occurs72hourspostop.Canbesevere,hemorrhagicandmayrequireVVECMO.MedicalTherapyisfor:InoperableCTEPH AsabridgetodefinitivesurgicalinterventionSuboptimalhemodynamicandfunctionaloutcomeaftersurgery–calledpersistentCTEPHSmallrandomizedstudiesshowthatmedicaltherapyforinoperableCTEPHhassomehemodynamicandsymptomaticbenefits;particularlybosentanandriociguatwhichispreferredforfunctionalclassIItoIIwithinoperableandpersistentCTEPH.Forsickerpatients,classIV,considerIVprostanoidtherapy.

Cystic Fibrosis People with cystic fibrosis are living longer! Median predicted survival is 41-42 years. So you will be seeing them in your practice as a pulmonologist. The Basic Defects in Cystic Fibrosis Cystic Fibrosis is an autosomal recessive disorder. CFTR gene is located on chromosome 7 Normal CFTR is made, reaches the cell surface, and functions properly- transfer of chloride and water Class I No functional CFTR created Class II CFTR is misfolded and cannot reach the cell surface- F508del Class III CFTR reaches the cell surface but does not function properly- G551D Class IV CFTR channel opening is faulty Class V CFTR is created in insufficient quantities Diagnostic Testing Sweat test: >60 abnormal Nasal potential difference (salt measure) CFTR mutation analysis Semen analysis Phenotypic Features Chronic Sinopulmonary Disease GI and nutritional abnormalities • Colonization of typical pathogens (staph) • Intestinal: DIOS, rectal prolapse • Chronic cough and sputum production • Pancreatic: insufficiency, recurrent pancreatitis • CXR changes, i.e., bronchiectasis • Hepatic: focal biliary cirrhosis, multinodular cirrhosis • Wheezing and air trapping • Nutritional: protein-calorie malnutrition, AEDK deficiency • Nasal polyps, digital clubbing Salt Loss Syndromes Male urogenital- obstructive azoospermia • Acute salt depletion, chronic met alkalosis Chronic Respiratory Regimen Airway clearance- exercise, chest vest, flutter DNAse or pulmozyme Bronchodilators- albuterol Inhaled hypertonic saline 3-7% Inhaled antibiotics- tobi, colistin CTFR modulators:
Ivacaftor- G551D; ivacaftor/lumacaftor- dF508 Macrolides (avoid with NTM colonization) Chronic Nutritional Regimen Pancreatic enzyme supplements Monitor for CF-related diabetes (OGTT) Proton pump inhibitor Monitor for CF-related bone disease (DEXA) AEDK, iron, zinc supplementation Monitor for liver disease (LFTs +/- RUQ US) So you’ve got an exacerbation… • Ddx: exacerbation of chronic microbes, new bacterial growth, ABPA, non-Tb mycobacterium,
pneumothorax, sinus disease, GERD • Mild-mod: oral fluoroquinolone • May try continuous infusion of beta lactam • Mod-severe: 2 anti-pseudomonals IV • May try short course of oral steroid • Aminoglycoside: tobra daily at 10 mg/kg/day • Airway clearance! NIV if needed Treat those complications Pneumothorax- try to avoid VATS, pleurodesis NTM- check AFB sputum annually, consider treating Hemoptysis- bronchial embolization with IR DIOS- gastrograffin enema ABPA- check IgE; treat with steroid, itraconazole Consider: pancreatitis, intusseception, colon cancer CTFR modulators • Ivacaftor (at least one G551D mutation) - improved lung function at 2 weeks and sustained through 48
weeks. Also improvements in risk of exacerbations, patient-reported respiratory symptoms, weight. • Lumacaftor-Ivacaftor (homozygous 508del) – improved FEV1, nearly 40% lower exacerbation rate, lower
use of IV antibiotics

CourtesyofDrs.PhilLambertyandStephanieMaximous
Difficult Airway Algorithm Initial Considerations Take the time to get resources together: personnel, meds, equipment, lines IO access AIRWAY ANATOMY ease to visualize glottis/deliver tube limitations on positioning consideration of secretions
SECRETIONS DL vs. video suction ready, forceps
BAGGING/VENTILATION/OXYGENATION ability to BVM consider Bilevel/DSI (ketamine) FIND LMA
BLOOD PRESSURE (SHOCK) will they crash? pre-intubation cardiac US IO access may be needed push dose pressors
Fiberoptic Intubation ketamine .5 to 1 mg/kg IBW- repeat for effect Precedex load and infusion LOAD: mix 2mL vial in 48 mL saline give 1mcg/kg over 10 mins drip at run at .7mcg/kg/hr (.01 mcg/kg/min) Topical Anesthesia— max LIDOCAINE ~ 400mg-600mg bottle of 2%- 10mL— load onto ATOMIZER tongue, post pharynx, then down the hatch lidocaine gel on back of tongue depressor- suck bottle of 1% - lidocaine via scope (1-2mL)
RSI: Ketamine 1.5-2 mg/kg IBW Etomidate 0.3-0.4 mg/kg TBW Propofol (10mg/mL) 1-2.5 mg/kg IBW + (0.4 x TBW) OR 1.5 mg/ kg x TBW = 100mg=10mL!!! Succ 1-2 mg/kg TBW, 4mg/kg for SHOCK Rocuronium 0.6-1.2 mg/kg IBW
PUSH DOSE PRESSORS EPINEPHRINE iono-pressor take 9mL of saline (from saline stick) 1mL of cardiac EPI (100mcg/mL) now have 10mcg/mL Onset-1 minute Duration-5-10 minutes Dose: 0.5-2 ml every 2-5 minutes (5-20 mcg) PHENYLEPHRINE vasoconstrictor nurse makes 100mcg/mL bag (100ml) from a 1:100 dilation of the vial Onset-1 minute Duration- 10-20 minutes Dose-0.5-2 ml every 2-5 minutes (50-200 mcg

CourtesyofDr.RachelGivelber
5. Effectofdutyhoursrulesonmedicalerrorsormortalityhasbeendifficulttodemonstrate.[Volpp,JAMA2007,FIRSTtrial;iCOMPAREnotyetreported]
6. Whatcanyoudotoimprovesleepandfatigueduringshiftwork?a. Sleephygiene:setaroutine,lowerthermostat
i. Avoidnaturalandartificiallight1-2hoursbeforebedtime(TV,laptops,cellphones),blackoutcurtains,whitenoise(forlightsleepers).
ii. Nohotbaths/strenuousexercisebeforebed,nofood/alcoholb. Roleofmelatonin:Brightlightsuppressesendogenousproduction,and
exogenousdosingcanhelpentraincircadianrhythm:1mgimmediaterelease1hourbeforebedtime.

Endocrine Emergencies Adrenal Crisis
• Making the Diagnosis o Take a detailed steroid hx, include topical/intra-articular steroids, ICS + HAART o Risk factors to consider: anticoagulation (Waterhouse Friedrich’s) o Primary (adrenal failure) much more common than secondary (anterior pituitary)
• Lab Testing o Cortisol testing may be misleading à measuring total not free cortisol
§ Less than 3 ug/dL diagnostic, random > 12 rules out in HEALTHY adults § Unclear what the appropriate cortisol level is in critical illness § Cosyntropin stim tests can be helpful in acute settings
o Free cortisol influenced by albumin and cortisol binding globulin (CBG) § CBG high (false neg)– high estrogen (OCPs), hypergammaglobulinemia § CBG low (false positive)—nephrotic syndrome, cirrhosis
• Treatment o IV corticosteroids preferred early in the acute setting
Thyroid Storm • Making the Diagnosis
o Possible causes: Graves, medications (amiodarone, PD-1 therapies), iodine o Often precipitated by a stressor (surgery, pregnancy, infection, anesthesia) o Clinical suspicion important as lab findings may be misleading
• Systemic Effects o Fevers, tachycardias, AMS, abd pain common (may mimic acute abdomen)
§ Sinus tach and afib are most common arrhythmias, but VT also possible o Hypercoagulability (increased fibrinogen and clotting factors) o Encephalitis, status epilepticus, cerebral sinus thrombosis
• Treatment – Goal is decreasing T3/T4 production and conversion of T4 to T3 o Beta blockers (propranolol), corticosteroids, cholestyramine, PTU/methimazole
§ PTU may help reduce peripheral conversion but has liver toxicities o Potassium iodide or Lugol’s solution (must be used with methimazole or PTU) o ICU options: plasmapheresis, surgery o AVOID salicylates (may increase free T4) o Pheresis and iodides may not be as effective in setting of amiodarone toxicity
Myxedema Coma • Keys to Diagnosis à don’t need to be comatose for myxedema coma
o Most common cause is withdrawal of therapy, need detailed thyroid hx o Helpful PE findings: hyporeflexia, bradycardia, obtundation, goiter, myxedema
• Critical care considerations o Commonly incited by infection/sepsis, also by CVA, GI bleed, sedatives (opiates) o Systemic effects include bradycardia/heart block, pericardial effusions, coagulation
abnormalities, seizures, respiratory depression, hyponatremia o Prognostic factors: hypotension, bradycardia, resp failure, refractory hypothermia
• Treatment- cover for concomitant adrenal insufficiency while awaiting lab results o Start with IV thyroxine repletion until sure that bowels are working o T3 is more potent than T4 but may worsen heart disease, arrhythmias o Early T3 may stave off need for mechanical ventilation o Judicious fluid management, early antibiotics o Opiates will linger, avoid whenever possible

ICU delirium
Diagnosis Confusion assessment method (CAM) 1. Acute onset Is there acute behavior change from baseline and does it fluctuate during
the day? 2. Inattention Does the patient have difficulty focusing, easily distractible 3. Disorganized thinking Does the patient ramble, unclear or illogical flor of words 4. Altered consciousness For example, vigilant, lethargic, stupor, or coma Diagnosis requires presence of 1 AND 2 plus either 3 OR 4 The Intensive Care Delirium Screening Checklist (ICDSC) has high agreement with CAM
Management • Treatment of medical conditions:
o Fluids and electrolytes o Organ failure – uremia, hypoxemia, etc
o Infections o Hypoglycemia
• Drug toxicity – thought to contribute to 30% of all cases of delirium, even when levels are “therapeutic” o Classic examples are lithium and digoxin
• Withdrawal- namely alcohol and sedatives • Thiamine deficiency and Wernicke encephalopathy- older patients with nutritional deficiency • Managing agitation
o Nonpharmacologic interventiosn such as addressing noise, light, windows, and restraints have been shown to improve clinical outcomes of frail patients.
o Physical restraints should be a last resort. o Neuroleptics to treat severe agitation – data support reduces severity and duration, not incidence
§ Best data is for quetiapine as add-on treatment to as-needed haloperidol o When pain is an issue: data supports more rapid improvement with morphine versus haloperidol
• Hypoactive delirium- similar management to the above; some data for low dose methylphenidate improving alertness
Hyperactive delirium is less common in older patients and usually alternates with periods of hypoactive delirium which is less obvious to providers.
Prognosis Mortality – one and six month mortality is 14 and 22%, respectively, even after adjusting for confounders Persistent cognitive dysfunction- after 2 years, only 1/3 of patients live independently Course of Alzheimer disease – deterioration proceeds at twice the rate compared with pre-hospitalization
Delirium Prevention • Nothing has been shown to reliably prevent delirium, but you can reduce the incidence: Orientation protocol- clocks, calendars, windows, etc Cognitive stimulation Physiologic sleep- data supports ear plugs, noise reduction Early mobilization, limited restraints Visual and hearing aides Avoid problematic medications Manage medical issues – volume depletion, hypoxemia Treat pain • Current evidence does not support using medications to prevent delirium in ICU or postoperative settings

CourtesyofDrs.PhilLambertyandBryanMcVerry
Approach to ICU Sedation Key Principles
• Focusonminimaldrugnecessarytoachievecomforto Reducetimeonvento ReduceICULOSo Promotefunctionalityo Reducedelirium
• Startminimizationprocessassoonafterintubationaspossible/safe• Goaldirected
o Riker4default§ Recognizethatwillnotnecessarilyworkforallcomers
• EtOHwithdrawal• Needforparalytic
• Startwithpainreliefbasedfocuso Fentanyldrugofchoiceo Supplementwithlongeractingtominimizeinfusion
• Benzodiazepineuseo Usefulwhenindicatedo Boluswhenneededo Supplementwithlongeractingenteralagentifneeded/effectiveo Avoidinfusion
• Utilizeshortactingnon-benzodiazepinemedsforcontinuousinfusionwhenpossibleo Propofolo Dexmedetomidineo Ketamineo Benzodiazepinelastresort
• Dailyinterruptionwhencontinuousdripsrequiredtoassessongoingneedo Regularattemptsatde-escalationifpatientdoesnotmeetautomaticsedation
interruptioncriteria• Implementasbundleintervention
o Cannotdoinisolationthoughsedationminimizationiskeycomponentofbundleasallelseflowsfromwakefulness
o ABCDE§ Awakening§ BreathingCoordination
• SBT§ DeliriumMonitoring/Management§ EarlyMobilization
• doesnotnecessarilyequatetoearlyambulation• ASSESSYOURPATIENT’SNEEDSBEFOREDOSEADJUSTMENT
o Attempttodiscernandfixunderlyingreasonforagitationo Don’tforgetaboutdeliriumprevention/treatment
• Frequentreassessmento Patientresponseo Bedsidenursesupport

CourtesyofDr.RachelGivelber
FatigueMitigation1. Fatigue:tiredness,reducedmotivation,needtoexpendincreasedefforttoperforma
taskeffectivelyandwithouterrora. Accumulateswithincreasingworkdurationandintensityb. Affectedbyquantityandqualityofsleepc. Affectedbytimeofdaythatworkoccurs(relativetocircadiantime)
2. Cognitivedomainsaffectedbysleepiness:attention,workingmemory,mood,executivefunctioning.FatiguedpeoplehavePOORINSIGHTintoimpairment
3. Individualvariability
4. Multipleadverseeffectsonresidentsassociatedwithprolongedshiftwork:needle
sticks,carcrashes,self-reportedmedicalerrors;objectivelyobservedmedicalerrors.

HEMATOLOGICEMERGENCIESBenignHemeEmergencies MalignantHemeEmergenciesAutoimmunehemolyticanemia HypercalcemiaTTP HyperleukocytosisSicklecellcrisis Hyperviscosity Acutetumorlysissyndrome Acutecordcompression SuperiorvenacavaesyndromeAcutecordcompression
• Lungca>Breastca>Prostateca• Thoracicspine>Cervicalspine>Lumbarspine• 90%pain;75%weakness;50%lossofbladder/bowelfunction• Treatment:XRT+IVDex+surgery(ifable)bestoutcomes
Tumorlysissyndrome
• Morecommon:high-gradelymphoma(Burkits)oracuteleukemia(ALL)• TumorlysisLabs:↑uricacid,↑K,↑Phos,↓Ca• Clinicaltumorlysis=Tumorlysislabs+oneofthefollowing:
o Cr>1.5,Arrythmia,Seizure,orDeath• ProphylaxisandTreatment:
o IVFo Allopurinolo Rasbirucase
Hypercalcemia
• Etiologieso PTH-rP(80%):SqcellCA(lung,Head&Neck),RCC,Bladder,Breast,Ovariano Osteolysisfrombonemets(20%):Multiplemyeloma,Breast,Lungo ExcessVitDproductionfrommalignantcells:leastcommon
• Sx:lethargy,confusion,nausea,constipation,polyuria,polydipsia,arrhythmias(bradycardia,shortQT,cardiacarrest)• Treatment(forCa>12-14):
o IVFo Calcitonino Pamidronateo Zolendronicacido Steroidso Furosemide(onlyuseoneuvolemicpatients)
Superiorvenacavaesyndrome
• Etiologieso Non-malignancy:thrombosis,fibrosingmediastinitis,post-radiationfibrosiso Malignancy:lungca,lymphoma(diffuselargeB-cell)
• Initialtreatment:Airwaymanagement• Definitivetreatment:XRT,chemo,endovascularstenting
HEMATOLOGICURGENCIESNeutropenicfever
Transfusionreaction
DIC
AMLw/ohyperleukocytosis
Bleedingdiathesis

Hemoptysis
MassiveHemoptysis-rangingfrom100mLto600mLover24hours.Lifethreateningbleeding-usually>500mLofbloodover24hoursorarateof>100mL/hour.
CausesofHemoptysisAirway ParenchymalBronchitisand*bronchiectasis Almostanyinfection–*Tb,fungal,bacterial,viralBronchovascularfistula(aorticaneurysm,trauma,surgery,stentcomplication)
Exoticinfections–anthrax,Y.pestis,tularemia,*Pwestermani
*Bronchogeniccarcinoma Rheumatic–amyloid,Goodpasture,Bechet,GPA,SLE,APLA
Dieulafoy–subepithelialbronchialartery IdiopathicpulmonaryhemisiderosisMetastaticcancer CoagulationDisordersForeignbody Medications–anticoagulantandantiplateletTracherosionintoinnominateartery(lowplacement) DICPulmonaryVascular ThrombocytopeniaHeartfailure,mitralregurgitation,congenitaldisease VonWillebranddiseasePulmonaryembolism LeptospirosisPVOD Onecaseseriesofembolizationforhemoptysis:40%CF/bronchiectasis,14%metastaticdisease,12%lungcancer,7%fungalinfection.Mostcommonetiologies*bolded
RememberthatbloodfromtheupperGItractcanbeexpectoratedandmimichemoptysis-called“pseudohemoptysis”Diagnosis1. CXRrevealsthesiteofhemoptysisisalmosthalfofcasesandthecasein~35%.2. CTispreferableforbronchiectasisandcarcinomas.Bronchoscopyisbetterformucosalabnormalitiessuchas
bronchitis,Kaposi,smallpapillomas,etc• Studyof50patientswithhemoptysis,normalCXR:CTdiagnosticin30%andbronchoscopyin10%.
3. RecurrenthemoptysiswithnormalCTandbronchoscopy–mostcommonetiologyhereisupperairwaysourceoruseofanticoagulants.Recurrenceintheremainderhappensinabout20%.
ManagementofMassiveHemoptysisFirstpositionthepatientbadlungdown,establishanairway,ensurehemodynamicstability,andthentrytocontrolthebleeding.
• Identificationofsideofbleedingcanbedifficult–patientscanoftentellyouwhichsideit’scomingfromandphysicalexamandCXRmayhelp.
• Trytoplacean8.0ETT.Youcanplaceinthemainstemofthenonbleedinglungtoprotectthisgoodlung.Combinethiswithballoontamponadeorbronchialblockerplacement.
• Doublelumentubesareanotheroption–trytogetaleft-sideddouble-lumentube-longlumenterminatesintheleftmainbronchusandshorterlumenterminatesinthedistaltrachea.ThisavoidsRULocclusion.
BronchoscopyisoftengoingtobeyourfirstchoiceintheICU
• Endobronchialblocker.Seevideo<https://www.youtube.com/watch?v=Tru-vVO6s3w>• Icedsalinelavage–cool1Lofsalineaheadoftime(putinabunchof50-60ccsyringes).Lavagebleedingsource
with50ccaliquotsofcoldsaline.Averagevolumeinonecaseserieswas500mLperpatient.• Topicalepinephrine[1:20,000]
ArteriographyandEmbolization
• Usewhenthereispersistenthemoptysisdespitebronchoscopyandcorrectionofcoagulopathy.• Anteriorspinalarteryarisesfromabronchialarteryin5%-embolizationmayresultinparaplegia(1%)

IdiopathicPulmonaryFibrosis
ThemainthingyouhavetodowhenconsideringIPFistoruleoutothercausesofinterstitiallungdisease.
History PhysicalExam50-60yearsold Coarsebibasilarcracklesatendinspiration
• CanbeunilateralespeciallyearlyMosthaveasmokinghistorySeveralmonthsofdyspneaandcough EndinspiratorysqueaksaretractionbronchiectasisSystemicsymptomsarerare(fever,myalgias,etc) Clubbingin50-75%RadiologyIftheH&PisasaboveandtheCTchesthasthesethreefeatures,thenitislikelyIPF1. Peripheral,bibasilarpredominantreticularopacities2. Honeycombing3. TractionbronchiectasisHowever,thereareafewexceptionstotheabove-asexpertsyoushouldbeaware:
• HoneycombingisessentialtomakingaUIPdiagnosis,butissometimesabsent• Upto30%ofUIPdiagnosedbybiopsyhaveotherfeaturesonCTchestthanlistedabove• GroundglassopacitiescanbepresentinIPF!Butshouldnotbethepredominantfeature
So,ifI’mprettysureit’sIPF,doIneedlabs?Usuallytheanswerisno.SeetheILDhandoutfordetailsonserologies.Afewthingstokeepinmind:1. ANA>1:40ispresentinupto25%ofbiopsyprovenUIP2. Positiverheumatoidfactorispresentinabout15%3. Upto70%apeoplewithanti-synthetasesyndromecanpresentwithaUIPpatternoffibrosisWhendoIrecommendabiopsy?Ifwiththeabove,youarenotconfidentinanIPFdiagnosisthengetabiopsy.It’simportanttogetthisrightbecauseIPFhasaprognosisworsethanmostcancers.Butusuallyyoucansparethemthemorbidityofabiopsy.Ok.SotheyhaveIPF.WhatcanItellthemtoexpect?• FVCdeclinesabout150–200ccperyear–thismeans
theycanexpectaslowdeclineinfunctioning• Acuteexacerbationsareunpredictable–this
meansconsiderearlytransplantreferral• “IfItake100peoplewithIPF,about20ofthemwillbedeadin5years”
Andthentheysay,“aren’ttheresomemedicinesorsomething?”FormildtomoderateIPF,meaningDLCO45-65%predicted,Iwouldhaveadiscussionabouttheprosandconsofmedication.Here’swhatyouneedtoknow:• Nintedanibisamultipletyrosinekinaseblockerandmediateselaborationoffibrogenicgrowthfactors(PDGF,VEGF,
FGF).Itslowstherateofdeclineinlungfunction.Don’tgivetocirrhotics.AnditinterfereswithCYP3A4andincreasesriskofbleedingonanticoagulation.
• PirfenidoneisanantifibroticthatinhibitsTGF-betastimulatedcollagensynthesis;blocksfibroblastproliferationinvitro.Alsoslowstherateofdeclineinlungfunctionandpossiblyasurvivalbenefitinapooledanalysis.
NowtheyareinthehospitalwithanacuteexacerbationofIPF.Sonowwhat?Knowthatmortalityisabout50%andprobablyhigheriftheyenduponmechanicalventilation–approaching100%insomestudies.Cantrythefollowing:• Ruleoutinfectionandgive1-2gramsofsolumedroldailyfor3-5days-knowthatevidenceforthisislacking• VerylimiteddataonprotocolwithpheresisandIVIg-patientsthatrespondtothis(andtheabovemeds)probably
haveanunderlying,undiagnosedconnectivetissuedisease

Approach to Interstitial Lung Disease History Physical Exam Allergic rhinitis and asthma – eosinophilic pneumonia Fibrosis sounds like coarse, velcro-like crackles Nasal polyps – EGPA (churg-strauss) High pitched inspiratory squawk – bronchiolitis (HSP) Medications – amiodarone, anti-TNFα, nitrofurantoin Clubbing is nonspecific, usually in advanced fibrosis Smoking – RBILD, DIP, EG PAH, cor pulmonale (edema, loud P2, RV heave) Exposures – asbestos, silica, birds, etc Extrapulmonary – rashes, Raynauds, arthritis,
muscle weakness/pain, nailfold capillary ILD that may have obstructive PFTs • Sarcoidosis • LAM/tuberous sclerosis • Hypersensitivity pneumonitis • Eosinophilic granuloma • Combined pulmonary fibrosis emphysema Clinical Pearl: Look at old imaging and PFTs to determine the time course and progression of disease! Radiology Classic UIP pattern that indicates IPF and requires no further workup:
1. Bilateral, subpleural reticular opacities in a basilar predominance 2. Traction bronchiectasis 3. Honeycombing
Other typical radiographic patterns of ILD • Balanced hilar adenopathy- sarcoidosis • Pleural plaques and septal lines – asbestosis • Centrilobular nodules – hypersensitivity pneumonitis, eosinophilic granuloma, sarcoidosis • “Atoll sign” – airspace disease at the end of an airway with central clearing – COP • Cysts – EG, LAM, Sjogren Clinical Pearl: If you have a classic UIP pattern and no inkling of autoimmune disease, you can call it IPF. We still recommend some screening serologies to help with prognosis and rule out myositis. Serologies Screening serologies that I get on almost everyone ANA – get excited with titer >1:80; pattern matters, i.e., nucleolar important, homogenous not so much RF- pretty nonspecific but can clue you in that something is afoot CK, aldolase, myositis panel, Jo-1: 70% of anti-synthetase syndrome presents with ILD and negative ANA ESR and CRP- these are not helpful and I do not get them Disease specific serologies that I only get if pretest probability is high ccp- specific marker for RA, get hand XR as well if suspicion is high ssA/ssB, immunoglobulins: Sjogren, IgG f seronegative Sjogrens, IgG subclasses for IgG4 disease Scl 70, centromere, PM-1: scleroderma and the scleroderma/myositis overlap syndrome ANCA- order with suspicion of vasculitis: GPA, EGPA, MPA; interpretation can be difficult dsDNA, smith, RNP- SLE and its overlap syndromes, RNP is helpful if dsDNA and smith are negative Clinical Pearl: If the CT is not classic UIP fibrosis and/or you suspect autoimmune disease based on history, exam, serologies- try to biopsy something to get an actual diagnosis. VATS TBBx NSIP Sarcoidosis COP Hypersensitivity pneumonitis Eosinophiic pneumonia Lymphangitic carcinomatosis

Liver Failure Differential Diagnosis A Acetaminophen, hepatitis A, autoimmune, Amanita phallodes, adenovirus B Hepatitis B, Budd-Chiari C Hepatitis C, CMV, cryptogenic D Hepatitis D, drugs E Hepatitis E, EBV F Fatty infiltration, acute fatty liver of pregnancy, Reye’s syndrome G Genetic – Wilson disease, hemochromatosis H Hypoperfusion, HELLP, HSV, heat stroke, hemophagocytic lymphohistiocytosis I Infiltration by tumor Physical Exam Hepatic encephalopathy is the hallmark of acute liver failure and has four grades: • Grade I – mild confusion, slurred speech, disordered sleep; mild asterixis • Grade II – lethargy, moderate confusion • Grade III – stupor, incoherent speech, sleeping; asterixis is the most prominent • Grade IV – coma, unresponsive to pain; cerebral edema in 75%; posturing present
Subclinical seizures are thought to occur in ~30% and are difficult to detect clinically Laboratory Pearls • Elevated INR is part of the definition of acute liver failure and must be present (INR >1.5) • Aminotransferases should be markedly elevated (acutely) • Decreasing aminotransferases may indicate recovery or worsening with loss of hepatocyte mass – don’t be fooled! • Bilirubin and INR are the most important to monitor, only give FFP if really needed
Despite elevated INR – 20% are hypocoaguable, 45% normal, 35% hypercoaguable! (via thromboelastography)
Management • Have a low threshold to send patients to a liver transplant center. Only 40% of patients with acute liver failure will
spontaneously recover. • Use hepatic encephalopathy for triage: Grade I on the floor, Grade II – IV in the ICU Some disease- specific treatments N-acetylcysteine Obvious role in acetaminophen toxicity; there may be some role in non-acetaminophen
liver failure as well; low threshold to administer, risks are minimal Hepatitis B Consider lamivudine; give to transplant candidates to prevent post-transplant
recurrence Amanita phalloides Early charcoal improves survival; consider silibinin (milk thistle extract) and penicillin G Budd-Chiai TIPS, surgical decompression, thrombolysis HSV Acyclovir for 7 days Wilson disease Will generally require transplant; plasma exchange with FFP to remover copper as a
temporizing measure Autoimmune hepatitis Trial of steroid not unreasonable (prednisone 40-60 mg daily); be weary of infection Acute fatty liver of pregnancy Emergent delivery

1-page TICU tips David T. Huang, MD, MPH
May 2018 Neuro
1. Hepatic encephalopathy is like ileus – something caused it! 2. Cirrhotics get NMS too 3. Golytely a good hepatic enceph tool
Cardiovascular
1. Know “usual” blood pressure 2. Investigate “normal” CI 3. Watch for the crump – even w/ minor stress 4. Love, fear, + respect lactate!
Pulm
1. OK to tap belly/chest w mild-mod coagulopathy 2. Check more ABGs when Bili > 20 3. Drain ascites/hydrothoraces slowly, then speed up
GIB
1. Intubate suspected variceal bleeding pre-EGD 2. Transfuse to ~8 3. Tell GI + IR to talk directly to each other, while you stabilize pt 4. Hey GI, what’s rebleed plan? 5. Balloon tamponade? – remember 50/50! (50 cm in, 50 cc air – take Xray!)
Renal
1. Cirrhotics get drug/sepsis/etc-induced AKI too 2. Carefully err on side of more volume 3. Dialysis may not be a good idea…
Infection
1. Infection likely worsens liver function, and portal HTN, per se 2. TICU handshake = ascites tap 3. Treat ~ as if transplant pt! 4. Intubation a 2-step procedure (Tube, then lung specimen)

Approach to Lung Cancer I - Screening
Some Lung Cancer Fun Facts • There are more lung cancer deaths than breast, prostate, and colon combined • 80% are nonresectable on presentation and 50% are dead within 1 year • It takes about 10 years of smoking cessation to get your cancer risk down to ~5%
Causes of Lung Cancer Smoking Second hand smoke Occupational exposures Air pollution Radiation Diet and nutrition Occupational Agents Associated with Lung Cancer- it’s on the boards! Arsenic Asbestos (multiplicative risk for cancer with smoking) Chromium Nickel Radon Vinyl Chloride
Most common genetic abnormalities Cancer Mutation Incidence Squamous cell p53 60-70% Adenocarcinoma KRAS in smokers
EGFR kinase domain in nonsmokers 10-30% 10-40%
Small cell c-MET overexpression 13% The best evidence of effective screening is a reduction in mortality, not prolonged survival. Higher survival rates in the screened population is due to earlier detection- the classic “lead time bias”. Bias in Screening Lead time bias Disease detected earlier but death is not delayed Length bias Screening preferentially detects slowly progressive disease Overdiagnosis bias Screening detects disease that would not otherwise be clinically evident National Lung Screening Trial (NSLT) of low dose CT scan • 53,000 participants, 148,000 exams, 59 sites in 28 US states • 20% reduction in mortality; 3 fewer deaths per 1,000 people over an average of 6.5 years of follow up • 24% with abnormal result and 96% of those were false positives • 2.5% had an invasive test, 1.9% had a biopsy, and 0.4% had an adverse outcome
Whom do I screen? Age 55-75 Smoking history of at least 30 pack years Asymptomatic Current smoker or has quit within the last 15 years Check out the very awesome Solitary Pulmonary Nodule Risk Calculator: https://www.uptodate.com/contents/calculator-solitary-pulmonary-nodule-malignancy-risk-brock-university-cancer-prediction-equation

Lung Cancer II – Staging and Treatment
Fleischner Society Guidelines 2017 Nodule Type Size (mm) Follow up (months) Solid <6 No follow up, optional CT at 12 months for high risk
6-8 CT at 6-12 months then 18-24 >8 CT, PET, or biopsy at 3 months
Ground glass <6 No routine follow up ≥6 CT at 6-12 months, then every 2 years until 5 years
Mixed <6 No routine follow up ≥6 CT at 3-6 months, then annually until 5 years
Multiple Solid ≥6 CT at 3-6 months, then 18-24 months for high risk Multiple Ground glass ≥6 CT at 3-6 months, if stable repeat at 2 & 4 years PET scanning • Avoids futile thoracotomies in ~20% (detects non-resectable disease) • False Positives: granulomatous disease (sarcoid), rheumatoid nodules, pneumoconiosis • False Negatives: tumors <1cm, low-grade BAC, carcinoid When performing bronchoscopy, EBUS, Navigational, whatever... you really need to get enough tissue to do molecular studies. Survival is better for targeted therapy vs non-targeted therapy. Lung Cancer Paraneoplastic Phenomena Syndrome Marker Cancer Hypercalcemia Bony mets (usually), PTHrP squamous SIADH Hyponatremia, urine and serum osm Small cell Lambert-eaton Voltage gated calcium channel Ab Small cell Limbic encephalitis/nonconvulsive status Anti-Hu Small cell Hypertrophic osteoarthropathy Clubbing, PET with diffuse uptake Dermatomyositis and Polymyositis Muscle weakness, CK, aldolase
There are many online sites to help with learning this, such as http://www.radiologyassistant.nl/en/p42459cff38f02/lung-cancer-new-tnm.html

CourtesyofDr.MattMorrell
Diseasespecificcriteriaforlistingforlungtransplantation
ChronicobstructivepulmonarydiseaseBODEindexofatleast7oratleast1ofthefollowing:
• FEV1<20%predictedandeitherDLCO<20%predictedorhomogenousdistributionofemphysema
• Historyofrecurrentexacerbationswithassociatedhypercapnia(pCO2>50mmHg)despiteaggressivemedicalmanagement
• Pulmonaryhypertensionorcorpulmonale,orboth,despiteoxygentherapyIdiopathicpulmonaryfibrosis HistologicorradiographicevidenceofUIPandanyofthefollowing:
• A10%orgreaterdecrementinFVCduring6monthsoffollow-up• Adecreaseinpulseoximetry<88%duringa6-minutewalktest• Honeycombingonhigh-resolutionCTofthechest• ADLCO<39%predicted
Cysticfibrosis• FEV1<30%predictedorrapidlydeclininglungfunction• Pulmonaryhypertension• Increasingoxygenrequirements• Baselinehypercapnia(pCO2>50mmHg)
PulmonaryHypertension• PersistentNYHAclassIIIorIVsymptomsonmaximalmedicaltherapy• Lowordeclining6-minutewalk• Failingtherapywithintravenousepoprostenolorequivalent• Cardiacindex<2L/min/m2• Rightatrialpressure>15mmHg
Contraindicationsfortransplantation:
Relative AbsoluteHistoryofHIV,HepCorB RecentoractivemalignancyBMI>35or<18 Activedruguse,cigaretteoralcoholabuseAge>70 SevereneurologicorpsychiatricdiseasePresenceofendorgandamage(dualorgantransplant?)
Non-compliance
Priorthoracicsurgeryorpleurodesis AbsentsocialsupportMechanicalsupport(ventilation/ECMO) SeveredeconditioningHighlevelofHLAantibodies
Studiesrequiredfortransplantworkup:
CXR PFTs ECHO V/Qscan BariumSwallow
CTchest 6minutewalk R/LHC Serologies HLAAntibodies

Neurocritical care – Acute Traumatic Brain Injury
Glasgow Coma Sale Eye opening Verbal response Motor response 1 No eye opening None None 2 Painful stimuli Incomprehensible sounds Extension to central pain 3 Verbal command Inappropriate words Withdrawal to central pain 4 Spontaneous Confused Withdrawal to pain 5 Oriented Localizing pain 6 Obeys commands *Give the best score for each category. 8 or less is severe brain injury * severe injury is GCS <8 and carries a 30% risk of death Guidelines recommend CT head in TBI patients with GCS 14 or lower. Evolution of CT findings is common and often does change management. Don’t hesitate to repeat CT if things change or even routinely
General Management Issues in the ICU Blood pressure management • Avoid SBP <90
• For ischemia target SBP 140-180 Intracranial pressure management
ICP monitoring indications: • GCS ≤ 8 AND abnormal CT with mass effect • Consider if age > 40, posturing, SBP <90
General management: • Elevated head of bed to 30 degrees • Optimize neck vein drainage (loosen
neck brace!) • Avoid hypervolemia, reasonable to
track CVP
Advanced management • First- consider CSF drainage if ICP >20 • Mannitol 1g/kg q4-6h- monitor serum osmolality • Hyperventilation – can reduce ICP but also leads to
vasoconstriction- goal pCO2 30-40 • Sedation – Propofol is first line both for ICP reduction and
neuroprotective effects Seizures • Incidence is ~10%, up to 30% with severe TBI
• Short term ppx to reduce early seizures- 7 days of phenytoin, valproate, orkeppra
Temperature management • Maintain normothermia – fever worsens outcomes • Therapeutic hypothermia (32-35 C) is not recommended
outside of clinical trials Glucose management • Hyper- and hypoglycemia are bad
• Hemostasis • Coagulopathy common, up to 30%
• Correct medication associated coagulopathy – antiplatelet, warfarin
Hypoxia (PaO2 <60) and hypotension (SBP <90) have been found in 50 and 30% of patients, respectively, and associated with poorer neurologic outcomes (OR ~2 for both).

Non-CFBronchiectasisClinicalFeaturesChronicproductivecough RecurrentpulmonaryinfectionsHemoptysis RecurrentrhinosinusitisDyspnea WheezingWeightloss fatigueDifferentialDiagnosisPostinfectious Congenital ImmunodeficiencyPseudomonas,haemophilus Primaryciliarydyskinesia HypogammaglobulinemiaTuberculosis Alpha1antitrypsin HIVAspergillus(ABPA) Trocheobronchomegaly(MounierKuhn) JobsyndromeVirus(HIV,measles,flu) Cartilagedeficiency(Williams-Campbell) Chronicgranulomatousdisease Sequestration Cancer/chemotherapyToxicinhalation/aspiration Rheumatic OtherChlorine RA IBD:UC&Crohn’sSmoke/fire SLE Young’ssyndromeHeroinoverdose Sjogren’s YellownailsyndromeForeignbody/obstruction Relapsingpolychondritis ConstrictivebronchiolitisEtiologybylocationfocal Broncholithiasis Congenitalbronchialatresia
Endobronchialneoplasm/foreignbody MucouspluggingUpperlung Cysticfibrosis Post-tuberculosis
Sarcoidosis Central/upper ABPARML MAI Immotileciliasyndrome
RMLsyndrome Lowerlung Aspiration hypogammaglobulinemia
UIPwithtraction Alpha1antitrypsin(rarely)Makethatdiagnosis• Bacterialandmycobacterialsputumculture • ExcludeCFwithsweattest(<40isnormal)• Immunoglobulins o CanalsodonasalPD,semenanalysis• ANA,RF,ssA/ssB • Primaryciliarydyskinesia–screenwithnasalNO(low)• Bronchoscopy,GIevaluation o CarinalornasalbiopsywithelectronmicroManagementPearls• DNAse-notusedbecausetrialdatashowedincreasedexacerbationsandFEV1decline• Corticosteroids-useonlyforABPA• Antibioticsforexacerbation-trytobaseonpriorculturedata,coverpseudomonas,1-2weekduration

Core Conference Series: Numerical Concepts in Clinical Study Interpretation Type I and Type II error in Clinical Trials
“Truth” Clinical Benefit No Benefit
Trial Result
“Positive” “Correct” Type I error
“Negative” Type II error “Correct” The “p-value” = probability of type I error—the probability of finding benefit where there is no benefit. “α” The power = 1 - probability of type II error—the probability of finding no benefit when there is benefit. “1-β” The sample size a function of the study design, effect size, and acceptable type I and type II error. Sensitivity, Specificity, PPV, NPV, and Likelihood Ratios in Diagnostic Testing
“Truth” Disease + Disease -
Test Result
“Positive” True Positive
False Positive
“Negative” False Negative
True Negative
Sensitivity, specificity, and likelihood ratios are inherent to the test; PPV and NPV depend on specificity, sensitivity, and disease prevalence Relative Risk Difference vs. Absolute Risk Difference
N Alive
N Dead Mortality
Absolute Risk
Reduction
Relative Risk Reduction
Number Needed to
Treat Study 1 Treatment 80 20 0.20 0.05 1-(0.20/0.25)=0.20 1/ARR=20
N=200 Control 75 25 0.25
Study 2 Treatment 980 20 0.02 0.01 1-(0.02/0.03)=0.33 1/ARR=100
N=2000 Control 975 30 0.03 Greater relative risk reduction ≠ “better” treatment!
𝑆𝑒𝑛𝑠 =𝑇𝑃
𝑇𝑃 + 𝐹𝑁 𝑆𝑝𝑒𝑐 =𝑇𝑁
𝑇𝑁 + 𝐹𝑃
𝑃𝑃𝑉 =𝑇𝑃
𝑇𝑃 + 𝐹𝑃 𝑁𝑃𝑉 =𝑇𝑁
𝑇𝑁 + 𝐹𝑁
𝐿𝑅+=𝑠𝑒𝑛𝑠
1− 𝑠𝑝𝑒𝑐 𝐿𝑅−=1− 𝑠𝑒𝑛𝑠𝑠𝑝𝑒𝑐

Diagnostic Testing Example: DDimer for VTE—low risk population 1000 pts VTE
Yes No DDimer Positive 56 536 592
Negative 4 404 408 60 940 1000
Example: DDimer for VTE—high risk population 1000 pts VTE
Yes No
DDimer Positive 263 410 673 Negative 17 310 327
280 720 2000
Relative vs. Absolute Risk
N Total N Dead Mortality Absolute
Risk Reduction
Relative Risk Reduction
Number Needed to
Treat Prostate Cancer
Screening Screen 72,952 214 0.0030
Control 89,435 326 0.0036
Low VT for ARDS Low VT 432 134 0.31
Control 429 171 0.40
𝑆𝑒𝑛𝑠 =𝑇𝑃
𝑇𝑃 + 𝐹𝑁 = 𝑆𝑝𝑒𝑐 =𝑇𝑁
𝑇𝑁 + 𝐹𝑃 =
𝑃𝑃𝑉 =𝑇𝑃
𝑇𝑃 + 𝐹𝑃 = 𝑁𝑃𝑉 =𝑇𝑁
𝑇𝑁 + 𝐹𝑁 =
𝐿𝑅+=𝑠𝑒𝑛𝑠
1− 𝑠𝑝𝑒𝑐 = 𝐿𝑅−=1− 𝑠𝑒𝑛𝑠𝑠𝑝𝑒𝑐 =
𝑆𝑒𝑛𝑠 =𝑇𝑃
𝑇𝑃 + 𝐹𝑁 = 𝑆𝑝𝑒𝑐 =𝑇𝑁
𝑇𝑁 + 𝐹𝑃 =
𝑃𝑃𝑉 =𝑇𝑃
𝑇𝑃 + 𝐹𝑃 = 𝑁𝑃𝑉 =𝑇𝑁
𝑇𝑁 + 𝐹𝑁 =
𝐿𝑅+=𝑠𝑒𝑛𝑠
1− 𝑠𝑝𝑒𝑐 = 𝐿𝑅−=1− 𝑠𝑒𝑛𝑠𝑠𝑝𝑒𝑐 =

Diagnostic Testing Example: DDimer for VTE—low risk population 1000 pts VTE
Yes No DDimer Positive 56 536 592
Negative 4 404 408 60 940 1000
Example: DDimer for VTE—high risk population 1000 pts VTE
Yes No
DDimer Positive 263 410 673 Negative 17 310 327
280 720 2000
Relative vs. Absolute Risk
N Total N Dead Mortality Absolute
Risk Reduction
Relative Risk Reduction
Number Needed to
Treat Prostate Cancer
Screening Screen 72,952 214 0.0030 0.0006 1-(0.0030/0.0036)
=0.17 1/ARR=
1667
Control 89,435 326 0.0036
Low VT for ARDS Low VT 432 134 0.31 0.09 1-(0.31/0.40)=0.23 1/ARR=11
Control 429 171 0.40
𝑆𝑒𝑛𝑠 =𝑇𝑃
𝑇𝑃 + 𝐹𝑁 =5660 = 0.93 𝑆𝑝𝑒𝑐 =
𝑇𝑁𝑇𝑁 + 𝐹𝑃 =
404940 = 0.43
𝑃𝑃𝑉 =𝑇𝑃
𝑇𝑃 + 𝐹𝑃 =56592 = 0.09 𝑁𝑃𝑉 =
𝑇𝑁𝑇𝑁 + 𝐹𝑁 =
404408 = 0.99
𝐿𝑅+=𝑠𝑒𝑛𝑠
1− 𝑠𝑝𝑒𝑐 =0.93
1− 0.43 = 1.63 𝐿𝑅−=1− 𝑠𝑒𝑛𝑠𝑠𝑝𝑒𝑐 =
1− 0.930.43 = 0.16
𝑆𝑒𝑛𝑠 =𝑇𝑃
𝑇𝑃 + 𝐹𝑁 =263280 = ~0.93 𝑆𝑝𝑒𝑐 =
𝑇𝑁𝑇𝑁 + 𝐹𝑃 =
310720 = 0.43
𝑃𝑃𝑉 =𝑇𝑃
𝑇𝑃 + 𝐹𝑃 =263673 = 0.39 𝑁𝑃𝑉 =
𝑇𝑁𝑇𝑁 + 𝐹𝑁 =
310327 = 0.95
𝐿𝑅+=𝑠𝑒𝑛𝑠
1− 𝑠𝑝𝑒𝑐 =0.93
1− 0.43 = 1.63 𝐿𝑅−=1− 𝑠𝑒𝑛𝑠𝑠𝑝𝑒𝑐 =
1− 0.930.43 = 0.16

Obstructive Sleep Apnea Complications of Sleep Apnea (aka: why this is important) Daytime function and cognition Daytime sleepiness, inattention, exacerbation of cognitive deficits,
increased errors and accidents Motor vehicle crashes 2-3 times more common in OSA Cardiovascular HTN, PAH, CAD, heart failure, CVA
• Unclear whether treatment improved mortality; see SAVE study in NEJM 2016
Metabolic syndrome Independent of obesity, OSA is a risk for incident diabetes Nonalcoholic fatty liver Again seems to be independent of obesity; 2-3 fold increase in risk Perioperative complications Respiratory failure, cardiac arrest, and ICU transfer All-cause mortality AHI >30 has a 2-3x increase; more in women; not present in untreated mild
OSA Risk factors for OSA Age Plateaus around the sixth to seventh decade Gender 2-3x more common in males; gap narrows in menopausal women Obesity This is the strongest risk; 10% increase in weight confers a 6x OSA risk Craniofacial, upper airway Short mandible, wide craniofacial base, tonsillar/adenoid hypertrophy Medical Conditions Associated with Increased OSA Prevalence Pregnancy Asthma, COPD, IPF CHF CVA and TIA ESRD Acromegaly Hypothyroidism Polycystic ovary syndrome A note on screening questionnaires: not adequately tested as a screening tool for asymptomatic patients and are not recommended for diagnosis. They tend to have a high false positive rate and thus are more useful to rule out OSA when the score is low. For example, the STOP-Bang questionnaire has a sensitivity and specificity of 84 and 56% for AHI >5 and a sensitivity and specificity of 93 and 43 for AHI >15. So for whom should I perform diagnostic testing? • Basically anyone with excessive daytime sleepiness • In the absence of excessive daytime sleepiness, if the patient snores and works in a “mission-critical”
profession (airline pilots, bus drivers, truck drivers) or has two additional features of OSA • For patients who do not snore and do not have daytime sleepiness, consider testing high risk groups like
PAH, resistant HTN, secondary polycythemia. Diagnosis – need one of the following two conditions: 1. Five or more obstructive events (apneas, hypopneas, or respiratory effort related arousals) per hour of
sleep with one or more of: sleepiness, gasping or choking, snoring, comorbidity (HTN, mood, CAD, CVA, CHF, AFib, DM II)
2. 15 of more obstructive events per hour of sleep regardless of symptoms or comorbidities Differential –These are other conditions that cause excessive daytime sleepiness Periodic limb movements Jerks in arms and legs fragment sleep Shift workers These workers get 7 hours per week less sleep than non-shift workers Narcolepsy Daytime sleepiness, cataplexy, hypnagogic hallucinations, sleep paralysis Upper airway resistance syndrome
Considered a type of OSA, not many apneas of hypopneas, rather respiratory effort related arousals; common in thin women with craniofacial abnormalities
Central sleep apnea No respiratory effort Primary snoring Most patients who snore do not have OSA GERD Can causes choking and dyspnea and may actually improve with NIV!

Occupational Lung Disease Silicosis – inhalation of crystalline silica in quartz, granite, sandstone – the most widespread pneumoconiosis in the US – occupations include mining, quarrying, drilling, sandblasting • Simple Silicosis – upper lobe, small rounded opacities, centrilobular and perilymphatic nodules • Complicated Silicosis – confluence of silicotic nodules into large opacities – this evolves into
progressive massive fibrosis – “angel wing” appearance • 10% of silicosis will have UIP fibrosis • Hilar and mediastinal adenopathy is common -
Calcium salt deposits lead to eggshell calcification • Tuberculosis is found in 25% due to toxic effect of silica on alveolar macrophages • Acute silicosis – usually in sandblasters – looks like alveolar proteinosis on imaging with ground glass
and crazy paving • Erasmus syndrome – association of occupational silica exposure with development of scleroderma Coal worker’s pneumoconiosis – silica free coal dust particles that reach the alveoli – looks similar to silicosis but the pathology is distinct. • Upper lobe small, rounded, opacities, that can develop into progressive massive fibrosis • 10-40% with UIP fibrosis and honeycombing – associated with bronchogenic carcinoma • Caplan syndrome – coal worker pneumoconiosis with rheumatoid arthritis Talcosis– exposure to ceramic, paper, plastics, rubber, paint, cosmetics • Similar appearance to silicosis – upper lobe opacities, bases are spared • Often contaminated with amphibole asbestos fibers – will get pleural plaques • Don’t confuse with talc granulomatosis which is from crushing and injecting pills Hard Metal Pneumoconiosis – produced by compacting tungsten carbide with cobalt called sintering. • Manifested by interstitial fibrosis and asthma, sometimes obliterative bronchiolitis • Pathology is alveolar macrophages and multinucleated giant cells – giant cell pneumonia Asbestos-related diseases – primary exposure in mining and milling, secondary exposure with insulation, brakes, shipbuilding, construction, textiles • Pleural plaques – most common manifestation, usually on parietal and diaphragmatic pleura; rarely
associated with restrictive physiology • Benign asbestos pleural effusion – 10-12 years after exposure, exudative and unilateral • Diffuse pleural thickening – starts unilateral in the base and progresses to bilateral; can lead to
pleurogenic fibrosis or retractile pleuritic with restrictive physiology • Malignant mesothelioma- latent period of 30-45 years; pleural thickening > 1cm • Asbestosis – lower lobe fibrosis, think septal lines; seen in up to 1/3 of exposed patients • Bronchogenic carcinoma – usually lower lobe adenocarcinoma, also consider rounded atelectasis Berylliosis – granulomatous lung disease; beryllium is a lightweight metal used in dental, computer, nuclear weapons, nuclear reactor , and aerospace industries • Imaging: early is ground glass, later is perilymphatic small nodules, mediastinal adenopathy in 25% • Pathology looks like sarcoidosis with noncaseating granuloma • Acute berylliosis looks like noncardiogenic pulmonary edema Hypersensitivity pneumonitis – inhalation and sensitization to agricultural dusts, bioaerosols, microorganisms, or reactive chemicals • 34% birds; 21% hot tub (mycobacteria); 11% farmer lung (actinomycetes); 25% no cause identified • Imaging hallmark is centrilobular ground glass nodules; mosaic attenuation, bases usually spared • Chronic hypersensitivity – fibrosis tends to start lower and progress to upper regions, endstage is severe
upper lobe scarring and distortion. Noxious Fumes – nitric acid, sulfur dioxide, chlorine gas, ammonia, phosgene • Acute lung injury, noncardiogenic pulmonary edema, asthma, delayed-onset obliterative bronchiolitis

PalliativeCareintheIntensiveCareUnit
FourPartstoaFamilyMeeting Wordsandphrasestotry1. Getwhattheyfamilyknows• Getsyouonthesamepage• letsyouknowwhetherornottheyalreadyknowthe
badnews
• “Whathaveyouheard?Whathaveotherdoctorsandnursesbeentellingyou?”
• “Whathaveyoutalkedaboutwithyourfamily?”• “Whathaveyoureadonline?”• Followupwith“Hasanyonetalkedwithyouabout
whatthefuturemaylooklike?”2. Delivertheheadline• Theheadlineisasuccinct,clearmessage-usuallythis
isthebadnews• Whenthereisuncertainty,acknowledgeitandthen
saywhatyoucan-putintermsofADLs
• “I’mworriedthat…”• “Shewillalwaysrequiresomeonetotakecareofher-
tobathher,feedher.Shewillnotbeabletowalk,willspendmostofhertimeinthebed”
• “Hewilllikelyrequiremachinesfortherestofhislife”
3. Expectandattendtoemotion• Emotionisgood,itletsyouknowthefamilyheard
yourheadline.• RememberyourNURSEstatements
• Name-“I’llbetyouarefeelingscaredandhelplessrightnow.Thisisallsosudden.”
• Understand-“Ican’timaginewhatitlikeseeingyourdadlikethis.”
• Respect-“Youhavedonesuchagreatjobcaringforyourmom.”
• Support-“Wewillbeherewithyouthroughthewholeprocess”
• Explore–“Tellmemoreaboutthat.”4. Makearecommendation• Thefamilyistheexpertinthepatient,theirlived
experience,andtheirvalues• Youarethemedicalexpertandthefamilywantsyour
medicalrecommendationonwhatmakessense
• “Ifyourdadcouldsitherewithus,whatdoyouthinkhewouldsayaboutallthis?”
• “Hasheeverthoughtaboutbeingreallysickorfilledoutalivingwill.”
• “Giveneverythingyou’vetoldmeaboutyourmom,Ithinkweshould…”
CommunicatingPrognosticUncertainty• Evenwhensurrogatesratecommunicationhighly,theyareofteninaccurateaboutprognosis• Familieshaveaperceivedneedtoremainoptimisticandthat’sok• Uncertaintyisbetdealtwithbyacknowledgingtheuncertaintyandstillgivingwhatyouthinkthefuturewilllooklike• “Hopeforthebestandplanfortheworst”Conflict• Conflictoverlife-sustainingtherapiesintheICUisexceedinglycommon–over50%inmoststudies• Recognizeconflictearlyandthenaskyourself3questions:
1. Whatistheirstory–Whyisthislovingfamilymembersayingsomethingthatdoesnotmakesense2. Whatisourcommonground–Thisisusuallythepatient.Refocustheconversationonthepatient3. Howcanweworktogether
• Givethemsometime–morethanhalfthetimewithdrawaltakesmorethanadayand“stuttered”withdrawalisassociatedwithincreasedsatisfaction
• Proposeatimelimitedtrial–beclearonhowlongandhowweknowifitisworking
Ifconflictpersists,considerapalliativecareconsult–itcanbeveryhelpfultohaveaskilled,impartialthirdparty

PleuralDiseaseDiagnostics
Light’sCriteria Two-testrule Three-testrulePleuralprotein:serumprotein>0.5 Pleuralcholesterol>45 Pleuralfluidprotein>2.9PleuralLDH:serumLDH>0.6 PleuralLDH>0.45upperlimit Pleuralcholesterol>45PleuralLDH>2/3upperlimit PleuralLDH>0.45upperlimit SomebasiccutoffsTuberculouseffusionproteinis>4.0 Cholesterol>250ischyliform,
longstandingeffusionLDH>1000–empyema,rheumatoid
Protein>7–thinkmultiplemyeloma TAG>110isachylothorax PJPhasLDHratio>1;verylowprotein Verylowglucose(lessthan60)rheumatoid Esophagealrupture EmpyemaMalignant Lupus TuberculousSomemoreobscurepleuralfluidtestsUrinothorax–pleural:serumcreatinine>1(usually1.7) Peritonealdialysis–pleural:serumglucose>1Hemothorax–pleural:bloodhematocrit>0.5 CSF–beta-2transferrinPleuraleosinophiliaPneumothorax(includingcatamenial) HemothoraxPulmonaryinfarction BenignasbestoseffusionParasiticdisease Fungal–coccidio,crypto,histoMalignancy(absenceofeosdoesnotruleout) DrugsAlwaysTransudatesAtelectasis DuetoincreasednegativeintrapleuralpressureCSFleak Surgery,trauma,ventriculopleuralshuntsHeartfailure DiuresismaymakethisappearexudativeHepatichydrothorax Ontheright,shouldhaveascitesaswellHypoalbuminemia RareNephrotic BilateralandsubpulmonicPeritonealdialysis Acuteandlarge48hoursafterinitiatingdialysisUrinothorax Ipsilateralobstructiveuropathy,i.e.,astoneSomeselectedexudates(therearealot…)Infectious Pneumonia,Tb,hepaticandsplenicabscess/infarction,hepatitis,esophagealruptureIatrogenic CVCmigration(s/pFontain),drug-related,RFAoflungnodulesMalignancy Carcinoma,Mesthelioma,Leukemia,Mult.MyelomaandWaldenstrom’sCTD SLE,RA,MCTD,EGPA,GPA,FMFEndocrine Hypothyroidism,ovarianhyperstimulationLymphatic Malignancy,chylothorax,yellownailsyndrome,LAM,lymphangiectasiaAbdominal Pancreatitis,Meigs’syndrome,Malignantascites,Subphrenicabscess,Other Trappedlung,benignasbestoseffusion,PE,Radiationtherapy,Sarcoidosis,postcardiacinjury
Whenyoustilldonothaveadiagnosis:1. Revisitthehistorywithspecialattentiontodrugs,exposures,PE,Tb,andcomorbidities2. Timecoursehelps–somelastforweekstomonths(parapneumonia,Tb,postcardiacinjurt)andotherslastforyears
orforever(yellownail,lymphangectasia,trappedlung,malignancy)3. Considertrappedlungwithhistoryofpneumonia,pneumothorax,surgery,hemothorax,RA,Tb,malignancy4. Ifstillunsure-getaCT(PEThasanemergingrolehere)andconsiderpleuralbiopsy

Pneumonia
Pneumonia is a clinical diagnosis: fever, dyspnea, sputum production. Airspace opacities on CXR can be a lot of things (as you know) and some studies say CXR has a 30% false negative rate compared with CT. Some fun facts on culture data in pneumonia: • Sputum cultures positive in ~60% (as long as sputum
is adequate. 60% of these are strep • Blood cultures positive in only 16%
• Urine strep antigen positive in 50% of those with confirmed Strep pneumoniae
• Bronchoscopy helpful in about 50% of patient who do not make sputum.
Again… pneumonia is a clinical diagnosis. So what’s up with procalcitonin? You will probably get a question about this on your boards. Know that in a Cochrane meta-analysis use of procalcitonin decreased antibiotic exposure from 8 to 4 days without increase in mortality. Low level supports viral or non-bacterial etiology. Use is not guideline supported however.. Risk Stratification. There are a number of tools out there. You should know the PSI and CURB-65. PSI is the gold standard however it’s complicated and needs a calculator. CURB 65 30 day Mortality C - Confusion 1 = 0.7% U – Urea (BUN >20) 2 = 2% R – respiratory rate >30 3 = 9% B – blood pressure, systolic <90, diastolic <60 4 = 15% Age > 65 years 5 = 40% Score of 3 or higher usually merits ICU admission. Treatment. Note here that treatments are highly influenced by local resistance patterns and the dementia of local antibiotic stewardship programs. In general go for: Ceftriaxone P Azithromcyin O Levofloxacin Cefotaxime L clarithromycin R moxifloxacin Ceftaroline U Ertapenem S Amp-Sulbactam A note on tigecycline because it may be on your boards. Tigecycline has a black box warning for increased mortality with hospital acquired pneumonia, in particular ventilator associated pneumonia. So only use it if fluoroquinolone or beta-lactam is not an option. Concern for multidrug resistant Pseudomonas or other MDR GNRs – like CF, bronchiectasis, severe COPD- it is not unreasonable to double up with something like pip/tazo + levofloxacin. Just know that there is absolutely no data to support this practice. What about steroids? It’s kind of controversial but a recent meta-analysis showed a modest mortality benefit in hospitalized patients with more severe pneumonia. If you’re going to do it, pick more severely ill patients, be wary of those that may have influenza or Aspergillus, and make a note of risks for adverse events like GI bleeding, neuropsychiatric illness, immunocompromised patients, and pregnant women. And finally, a note about treatment duration. A meta-analysis of 15 RCTs showed no difference in less than 7 days versus more than 7 days. In fact, in the more than 7 days group there was a signal of harm with increased antibiotic side effects. So, less is more people. Give patients 72 hours to respond to your therapy and if they do, you can stop after another couple of days. HCAP does not exist anymore because there is no data that nursing home residence, hemodialysis, etc increases the risk for MRSA and Pseudomonas pneumonia. The 2016 HAP/VAP guidelines are on your website for you but are mostly expert consensus-type recommendations.

Preoperative Pulmonary Evaluation Postoperative pulmonary complications are the most costly of major postoperative medical complications and result in the longest length of stay. Significant complications that adversely affect the clinical outcome Atelectasis Hypoxemia Infection Exacerbation of COPD or asthma Respiratory failure (mechanical ventilation >48 hours after surgery or unplanned reintubation) The rate of postop pulmonary complications across all surgery was 6.8 % in one systematic review Patient-related risk factors • Age – independent risk factor for every decade over 50; even healthy older adults have post-op pulmonary
risk (unlike cardiac surgery) • COPD – OR 2.4 for all complications; no absolutely prohibitive level of pulmonary function, most severe
obstruction surgical mortality is 5-6%; must weigh against risks and benefits of surgery • Smoking – RR 1.7, risk is greater with more than 20 pack years, risk decreases with at least 4 weeks of
smoking cessation • OSA – many patients preparing for surgery have undiagnosed sleep apnea and should be screened • Pulmonary hypertension – even mild and moderate and regardless of etiology; i.e., hip replacement
mortality OR is 3.7 • Heart Failure – OR is about 3 • ASA class >2 has OR of 4.8 for pulmonary complications (that’s “severe systemic disease” or worse) Asthma and obesity are not risk factors for post-op pulmonary complications Procedure-related risk factors • Surgical site is most important and inversely related to distance from diaphragm – upper abdominal OR is
20 and lower abdominal OR is 8. (An exception is laparoscopic cholecystectomy.) • Duration – less than 2 hours has 8% complication rate while greater than 4 hours has a 40% rate • Anesthesia – this is controversial but existing data suggests lower risk with regional anesthesia compared
with general. One large systematic review showed 40% decrease in pneumonia and 60% decrease in post-op respiratory depression with epidural or spinal vs general
Preoperative risk assessment • Most important is a history and physical with particular attention to the above factors • If concerned for sleep apnea, administer the 4 question STOP questionnaire • Candidates for lung resection should have preoperative PFTs; sometimes a quantitative VQ scan Pulmonary Function Testing should not be part of routine preoperative testing, including abdominal and other high risk surgery with the exception of lung resection. Get PFTs if it will change preoperative management. For example, if the patient has COPD and you are not sure if they are at baseline. If the patient has unexplained dyspnea and could have heart or lung disease or deconditioning. Other routine testing that does not help • ABG – the exception is a pCO2 >45, but this risk is not prohibitive and you should already know about it • CXR – very unlikely you will find anything that will change preoperative management CPET is helpful in two settings: 1. Patients with abnormal PFTs to assess the safety of lung resection 2. Unexplained dyspnea in non-cardiopulmonary surgery – can predict survival and overall complication rate. Distance
on a 6 minute walk gives comparable numbers. There are several postoperative pulmonary risk calculators out there. I like the Arozullah respiratory failure index because it predicts the incidence of postoperative respiratory failure, which is what we mostly care about. (Arozulla AM, et al. Ann Surg 2000; 232:242 – This article among others is on your website) Here is a different calculator that is online and easier to use (this is from the CHEST paper on the website): https://www.qxmd.com/calculate/calculator_261/postoperative-respiratory-failure-risk-calculator

CourtesyofDr.Rivera-Lebron
PULMONARYEMBOLISMEpidemiology
• 90%achievecompleteresolution• 30%recurrencewithin10yrs• 4-5%ofacutePEdevelopCTEPH
Diagnosis
• Useclinicaldecisionrues(WellsorGeneva)tocategorizepatientsintoapre-testprobability:PELikelyorPEUnlikely.PElikelygetsatCTA.PEunlikelythengetsPEruleoutcriteria(PERCrule).IfPERCneg,nothingelsetodo.IfPERCpositive,thendoD-dimer.
• CTAisgoldstandardfordiagnosis• Echoiscomplementaryandprovidesprognosticinfo• BNPandTropareusefulforprognosticinfo
ClassificationHighrisk(Massive)=hemodynamiccompromise(SBP<90for>15min)Intermediaterisk(Submassive)=HDstablebutsignsofRVstrainbyCT,EchoorbiomarkersLowrisk=noHDcompromiseorRVstrainTreatment
• NOACisACofchoiceforVTEw/ocancer• LovenoxifACofchoiceforVTEwcancer• DurationofACforProvokedPEis3mo• DurationofACforUnprovokedPEisindefinite(untilriskofbleedingis>riskof
recurrence)• LowriskPE,withnomajorcomorbiditiesorcontraindicationstoAC,goodcompliance
canbetreatedoutofthehospital• SingleSubsegmentalPE,withoutDVT,asymptomaticandlowriskofrecurrencedoes
notneedtobeAC• SystemictpaonlyindicatedinHighrisk(massive)• Catheter-directedtpareversesRVstrainquickly,butnomortalitybenefitreportedyet• IVCFilteronlyindicatedinpatientsunabletotolerateAC

PulmonaryFunctionTestingInterpretation
ClinicalPresentation RecommendedTestingDyspnea • Spirometrybefore/afterbronchodilator,volumes,DLCO
• AmbulatorypulseoximetryCough • Spirometrybefore/afterbronchodilator
• ConsiderMethacholinechallengeAsthma • Spirometrybefore/afterbronchodilator
• ConsiderMethacholinechallengeCOPD • Spirometrybefore/afterbronchodilator,oximetry
• ConsiderlungvolumesandDLCOininitialevaluationSuspectedILD • Spirometry,volumes,DLCO,oximetryNeuromusculardisease,diaphragmaticweakness • Uprightspirometry,volumes
• MaxinspiratoryandexpiratoryforceForinitial,diagnosticPFTS,askthepatienttoholdtheirbronchodilatorssothatbronchodilatorresponsecanbeassessed.Holdshortactingfor4hoursandlongactingfor12hours.LungVolumesandCapacities
Spirometry:forcedvitalcapacity(FVC),forcedexpiratoryvolumeinonesecond(FEV1),andtheirration(FEV1/FVC).• Normalratiois>70;othernormalare>80%ofpredictedingeneral• Supinespirometrytoevaluatediaphragmdysfunction:supinedecreaseinVCby25%unilateraland50%bilateralPost-Bronchodilator:significantwithincreaseinFEV1morethan12%and0.2litersLungVolumes:vitalcapacity(VC),functionalresidualcapacity(FRC)-thisistheendofatidalbreath,residualvolume(RV),expiratoryreservevolume(ERV),inspiratorycapacity(IC),totallungcapacity(TLC)• Decreasedvitalcapacityalonemaybeduetoairtrappinginsevereobstruction.Youcanseeairtrappingwhenthe
FRCorRVisincreased>120%DLCO: Restriction,ReducedDLCO
Intrinsicdisease:ILD,fibrosisExtrinsicrestriction,i.e.,obesity,DLCOisnormalorslightlyreduced
Obstruction,ReducedDLCOEmphysemaNormalinotherobstructivedisease
IsolateddecreaseinDLCOPulmonaryvasculardisease,PAH,CTEPH
MaximalInspiratoryPressures:MIPandMEP-usedtofollowpatientswithneuromusculardisease• Neuromusculardiseasepattern:increasedRV,normalFRC,lowMIPandMEP,lowMVV

ObstructiveandRestrictiveFlowVolumeLoops
UpperAirwayObstructionFlowVolumeLoops
B:intra-andextra-thoracicmasses,adenopathy,fixedairwaystenosisC:laryngomalacia,tracheomalacia,vocalcordabnormalities,i.e.,paradoxicalvocalfoldmotionD:introthoracictracheomalacia,bronchogeniccysts,trachealmasses,i.e.,malignancyApproachtopulmonaryfunctiontestinterpretation
Inobstructivedisease,forcedexpiratoryvolumeinthefirstsecondisdecreased(FEV1).Expiratoryflowinthelattertwo-thirdsofexpirationareeffortindependentandvarydirectlywithelasticrecoilofthelungandinverselywithairwayresistance.InCOPDelasticrecoilisdecreasedduetolossoflungparenchymaandairwayresistanceisincreasedduetosecretions,bronchospasm,orlossofsmallairways.
Normalratio
Spirometry
Lowratio:Obstruction
Bronchodilator
Negative: COPD vs asthma
Positive: asthma
DLCO
Normal: asthma/COPD
Low: emphysema
Clinicalasthma/chroniccough?
CheckforreducedFEF25-75%Methacholinechallenge
NormalratioLowFVC:Restriction
IsolatedDLCOdecrease:pulmvasculardisease
Confirmwithlungvolumes
DLCO
Low:ILD
Normal:extrinsic–
obesity,NMD

Pulmonary Hypertension
Pretest Probability Assessment via Echocardiography (some numbers are rounded for ease of use) Probability of PH
ESC/ERS 2015 guidelines recommend TRV Older 2009 guidelines and ISHLT use PASP
Low TRV < 2.8 m/s PASP <35 and TRV <2.8 Medium TRV ~ 3 – 3.5 m/s PASP and TRV and in-between low and high +
other PH signs on echo High TRV~3 – 3.5 with other PH signs on echo PASP > 50 and TRV > 3.5
TRV > 3.5 m/s What are “other signs of PH on echo” ?
• RV:LV basal diameter ratio > 1.0, flattening of the septum • PA diameter > 25 • IVC > 21 mm with decreased inspiratory collapse
Who to screen for pulmonary hypertension – high risk groups Systemic sclerosis Congenital heart disease HIV HHT, family history of HHT, other heritable etiologies Portopulmonary hypertension Sickle cell disease
If you have a medium to high risk of pulmonary hypertension on echocardiography 1. Determine if there is left heart disease sufficient to explain the pulmonary hypertension 2. If there is no left heart disease or insufficient left heart disease, consider the following work up:
• Chronic lung disease evaluation with PFTs, CT chest, 6 minute walk; overnight oximetry/PSG if needed • Venous thromboembolism evaluation with VQ scan; rare cases may require angiography
3. Consider HIV and serologic testing 4. If one of these etiologies is identified, you do not necessarily need a RHC but it may be indicated, especially in mixed
disease or to assess for treatment effect
Primary Therapy for Pulmonary Hypertension (AKA – treat the underlying disease) • In all patients, consider the following: diuretics, oxygen, anticoagulation, digoxin (particularly in group 3 with
COPD and biventricular failure), exercise • Anticoagulation seems beneficial in idiopathic PAH, not in CTD-associated PAH (Khan MS, et al. Circulation. 2018; 11) A special note on oxygen in Group 3 PH – the only modality with proved mortality benefit • PaO2 < 60 on oxygen for 15 hrs/day - decreased 5 year mortality but only after 500 days of therapy (lancet 1981) • NOTT showed improved 3 year mortality in continuous oxygen vs nocturnal oxygen (Ann Int Med 1980)
Broad Review of Drug Therapies – This is mostly for Group 1 PAH Calcium channel blockers – use for those who are vasoreactive on RHC (mean PAP decreases at least 10 and to a value less than 40 mmHg). Nifedipine has been shown to increase 5 year survival (Rich S, et al. NEJM 1992) Prostacyclin agonists – epoprostenol, treprostinil, selexipag • Epoprostenol improves hemodynamics, functional capacity and survival in idiopathic PAH, but no known survival
benefit in other types of Group 1 - Consider for idiopathic, CTD, portal hypertension, HIV, congenital heart disease Endothelin receptor antagonists – bosentan, macitentan, ambrisentan - improved exercise capacity, dyspnea, and hemodynamics (not survival); adverse effects are hepatotoxicity and peripheral edema • Note: ambrisentan is associated with disease progression and hospitalizations in patients with IPF PDE5 inhibitors – sildenafil, tadalafil, vardenafil – improves functional class for group 1, no role in lung disease, benefit in left heart disease “unclear” according to Cochrane review 2019 Guanylate cyclase stimulant – riociguat – benefit in inoperable CTEPH, maybe benefit in group 1 (Ghofrani HA. NEM 2013)
Combination therapy with tadalafil plus ambristentan shows decreased hospitalizations and increased exercise capacity (Galie N. NEJM 2015)

Pulmonary Rehabilitation
Benefits – What you can tell your patients they will get out of pulmonary rehabilitation: Mortality- meta-analysis suggests decreased mortality in patients receiving rehab after COPD exacerbation Exercise capacity- meta-analysis 65 RCTs shows improved capacity compared with community-based care Quality of life – same meta-analysis shows improvement based on chronic respiratory questionnaire Health care utilization- uncontrolled studies suggest decrease in hospital stay by 23 days/year/patient; other controlled studies are less clear, showing little to no decrease Comorbidities – preexisting functional disability and osteoporosis result in poorer outcomes from rehab; CAD did not adversely affect likelihood of improved exercise tolerance and quality of life Frailty. In one study, those who met criteria for frailty found that pulmonary rehabilitation experienced reduced dyspnea, improved exercise performance, and most no longer met frailty criteria. **These benefits decline over time and the degree of improvement tends to decrease with successive programs. Main indication for pulmonary rehabilitation is COPD with GOLD category B (FEV1 >50%), C (FEV1 <50%), and D (more symptoms with COPD assessment test score >10). What about other lung diseases? Interstitial lung disease- increased exercise tolerance, decreased dyspnea, improved QOL, but less than in COPD Bronchiectasis- improved walk distance and fewer exacerbations Cystic fibrosis – consider infection control issues Asthma- pre-exercise bronchodilators may reduce exercise-induced bronchoconstriction Pulmonary hypertension- concern for syncope and sudden death; submaximal exercise appears safe Exercise capacity measurements • 6 minute walk – mean improvement in 6 min walk after pulmonary rehab is 107 meters. • Shuttle walk (patient walks back and forth between two cones) – mean improvement is 81 meters • CPET- when dyspnea etiology is unclear- can determine intensity of training workload to target Components of Pulmonary Rehabilitation Endurance training- the most common- benefits thought to be due to true training effect with skeletal muscle adaptation, reduction in lactic acidosis and ventilation • Arm or leg ergometer for 20-30 min at 60% of max work rate; usually associated with Borg score of 4-6 • Most evidence is for lower extremity exercise; upper extremity exercise is derived from leg training data Interval training- better tolerated than continuous with greater adherence to the program and similar improvements Strength training- lower oxygen consumption and MV with less dyspnea; seems additive to endurance training Benefits of breathing retraining such as yoga and diaphragmatic breathing, ventilator muscle training, transcutaneous neuromuscular electrical stimulation, Tai Chi, flexibility training are being studied and have less clear benefits Education – smoking cessation, oxygen therapy, nutrition, physical activity, medications, health maintenance (vaccines) • Education is not an effective substitute for exercise training- in multiple trials education alone is same as
control Advance care planning is an accepted component of pulmonary rehabilitation Psychological Support- one trial showed improved depression scores independent of changes in QOL and dyspnea Maintenance Programs- one multicenter trial of 143 patients with COPD showed marginal but significant differences between the maintenance and control groups in BODE index and six-minute walk distance up to two years, but the benefit vanished after that time. No mortality difference over 3 years.

Pulmonary Vasculitis A number of vasculitic processes can involve the lungs, we are mostly dealing with GPA/Wegner’s, microscopic polyangitis (MPA), and eosinophilic granulomatosis with polyangiitis (EGPA/Churg-Strauss). Granulomatous with Polyangiitis (GPA, Wegner’s) – small vessel vasculitis Extra-Pulmonary Organ Involvement Joints- myalgias, arthralgias, arthritis Nervous system – mononeuritis, cranial neuropathies,
hearing loss, tinnitus, opthalmoplegia Eyes – conjunctivitis, episcleritis, uveitis Cardiac – pericarditis, myocarditis, conduction system Skin – vesicular, purpura; subcutaneous nodules Also- GI, GU, parotid, thyroid, liver, breast Pulmonary Manifestations Chronic rhinosinusitis – pain; purulent, bloody discharge; hearing loss, nasal perforation • May be present without other manifestations for weeks, months before progressing to vasculitic disease • Key difference vs EGPA is that EGPA has nasal polyposis and is less likely to have nasal perforation Tracheobronchial disease –stenosis, inflammatory pseudotumors, malacia, TE fistula • Subglottic stenosis in up to 50%- may be the sole manifestation and require tracheostomy Pulmonary nodules – cavitation in 25-50% Interstitial disease – fibrosis and honeycombing – commonly a UIP pattern; ILD most common with MPA Alveolar hemorrhage – presenting ~25%, commonly associated skin, renal, and neurologic involvement Pulmonary artery stenosis – rarely, seen on CTA, PA pressures may not be elevated Over 90% of GPA or MPA with lung and renal involvement are cANCA (PR3) positive. Minority will have pANCA (MPO). Persistently elevated ANCA is associated with relapse. Biopsy is important because need to exclude infection and metastatic disease affecting the lung • In general you want a surgical lung biopsy – not recommended in DAH or ILD. • Nasal and sinus biopsies are very low yield- usually do not show vasculitis Treatment Induction: usually cyclophosphamide (more experience) or rituximab (less toxicity); for mild disease without renal involvement- may try MTX
Maintenance: usually azathioprine or rituximab, again- if no renal disease may try MTX
Eosinophilic Granulomatosis with Polyangitis (EGPA, Churg-Strauss) Three Phases of disease: • Prodromal – atopy, allergic rhinitis, asthma • Eosinophilic – peripheral eosinophilia, eosinophilic infiltration of lung and GI tract in particular; this is the
triad of pulmonary opacities, asthma, and eosinophilia that presents prior to systemic vasculitis (true ~40%) • Vasculitic – medium and small vessels; associated with constitutional symptoms EGPA Clinical Manifestations Asthma – in 90% and precedes vasculitis by 8-10 years Neurologic – usually mononeuritis – up to 75% Upper Airway – nasal polyposis; looks like aspirin exacerbated respiratory disease
Renal – common, biopsy shows necrotizing glomerulonephritis
Skin –subcutaneous nodules on extensor surfaces, biopsy shows granulomas
GI – abdominal pain, bleeding, diarrhea- may precede vasculitis
Cardiac – due to high eosinophilic infiltration Myalgias and arthritis are less common Increased thromboembolic risk Eosinophilic lymphadenopathy in ~40% EGPA Diagnostic Criteria: need 4 or more of the following (sensitivity 85%, specificity 99%) Asthma Migratory or transient pulmonary opacities >10% eosinophils Paranasal sinus abnormality Mononeuropathy or polyneuropathy Biopsy showing extravascular accumulation of eosinophils

Sarcoidosis
There are three forms of sarcoidosis to consider: 1. Spontaneous remission- clinically inactive and usually requires no treatment 2. Transiently or chronically active disease- treatment to prevent granulomas and organ damage 3. Relapsing and remitting- treatment to prevent disease relapses. We often fail to recognize this form and it
is this form that often insidiously progresses and leads to end organ damage.
Sarcoidosis organ involvement (can affect any organ) Lung 95% Erythema nodosum 8% Skin 16% Spleen 6% Lymph node 15% Neurologic 5% Eye & liver 11% Cardiac 2% (prob underestimated) A word about ACE level: ACE level is useful for following disease activity. However, it has poor sensitivity and insufficient specific (almost 10% false positives; diabetes has a high ACE), thus is not used for diagnosis.
I need a biopsy I don’t need a biopsy Biopsy the most accessible lesions- skin, nodes, certain ocular lesions
Stage I asymptomatic disease, just monitor
Next choice is lung parenchyma (transbronchial yield ~75%%) and/or intrathoracic nodes (EBUS)
Classic Lofgren’s- fever, EN, arthralgias, bilateral hilar adenopathy
Exclude other noncaseating granulomatous disease, i.e. fungal and mycobacterial, before calling sarcoidosis and treating as such. Don’t be the guy who gives steroids to histoplasmosis. Triad of CD4:CD8 >4, lymphs >16%, TBBx with noncaseating granuloma has 100% PPV for sarcoid vs other ILD and 80% PPV for sarcoid vs all other disease Corticosteroids for Sarcoidosis Pros Cons Rapid improvement in symptoms Toxicity limits long term dosing Short term radiographic improvement Dose required for chronic disease is too high Effective in most organs Dose too high to prevent relapsing-remitting disease
Methotrexate for sarcoidosis Pros Cons Clinical trial data showing efficacy as a steroid-sparing agent
Slow onset of action- may take 2-6 months for full effect
Relatively low doses control inflammation and prevent relapses
Variable oral bioavailability
Well-tolerated Very rare side effect of hypersensitivity pneumonitis within 6 weeks on starting
Effective in most organ systems (?CNS and liver)
Liver toxicity rarely develops after cumulative dose of 3 grams (which is about 2-3 years)
Antimetabolite, steroid-sparing therapy for sarcoidosis Level of evidence Common toxicity Rare toxicity Methotrexate Double blind, placebo
controlled trials Nausea, leukopenia, hepatotoxicity, “washed out” feeling
Pneumonitis, teratogenic
Azathioprine Case series and reports
Leukopenia, nausea Hepatotoxicity, pancreatitis, skin cancer
Leuflunomide Double blind, placebo controlled trials
Leukopenia, hepatotoxic, alopecia
Pneumonitis, teratogenic, neuropathy
Mycophenolate Case series Nausea, diarrhea Skin cancer

CoreConference:SepsisUpdate
ListoftheStrongRecommendationsbasedonModerate/HighQualityEvidenceinSSCGuidelines2016Antibiotics AntibioticsASAPandwithin1hourforsepsisandsepticshock
Empiricbroad-spectrumantimicrobialstocoveralllikelypathogensAGAINSTroutinecombinationtherapy(i.e.2GNRagents)inneutropenicsepsis/bacteremia
VolumeExpansion
Crystalloidsasresuscitationfluidofchoice(ratherthancolloids)AGAINSTuseofhydroxyethylstarchesUsetransfusionthresholdofHgb<7.0inabsenceofAMI,severehypoxemia,hemorrhageAGAINSTuseofEPOforanemiaAGAINSTuseofAT-III
Vasopressors TargetMAP>65withvasopressorsifneededNorepinephrineasvasopressorofchoiceAGAINSTlowdosedopamineforrenalprotection
MechanicalVentilationandSepsis-inducedARDS
Lungprotectiveventilation:Vt6cc/kg,Pplat<30PronepositioningforP:F<150AGAINSThigh-frequencyoscillatoryventilationConservativefluidmanagementinabsenceoftissuehypoperfusionAGAINSTB-agonistsinabsenceofbronchospasmAGAINSTroutineuseofPAcathetersUseaweaningprotocolincludingdailySBTs
GlucoseControl
Protocolwithtarget<=180
DVTPPX Usesomething,andLMWH>UFHunlesscontraindicatedNutrition AGAINSTearlyTPNwhereenteralfeedingpossibleorbefore7days AGAINSTIVseleniumorglutamineGoalsofCare Incorporategoalsofcareintotreatmentandend-of-lifecareplanning,utilizingpalliativecare
principleswhereappropriateBeyondtheGuidelinesDiagnosis-What’sinaname?:Sepsis-3vs.“goodoldSIRS”;whatdowedowithoutagoldstandard?Treatment-Protocolizedsepsisresuscitation:
-Thetrials:PROCESS,PROMISE,ARISE:“failure”ofthebundleorimprovementinusualcare?-Themeta-analysis:PRISM:protocolizedcareincreasedcostswithoutimprovingoutcomes
-Real-worldimpactofcareprotocols:Rory’sRegulationsinNYState:antibioticshelp,butwhataboutfluids?-TheFederalGovernmententersthefray:TheSEP-1Bundle-HowmuchfluidshouldIgive?:Enoughbutnottoomuch!-TheMagicBullet?:Hydrocortisone/VitaminC/ThiamineEpidemiology-Long-termoutcomes:amongpreviouslyindependentpatientswithseveresepsis,1/3die;ofthesurvivors,1/3arenotindependentat6months-Majordriverofreadmissions

ApproachtoShock1. Airway,breathing,circulation–establishairway,IVaccess,sendsomelabs,startwithanIVFbolus2. Performtargetedhistory,physical,bedsideUS3. Performlife-savinginterventionifneeded4. SupporthemodynamicswithcontinuedIVFand/orvasopressors
ClassificationofShockCardiogenicCardiomyopathy• MI• CHFexacerbation• Cardiomyopathyofsepsis• Myocarditis• Drugs(BB)
Arrthythmogenic• Atrialandventricular
tachyarrhythmias• Bradyarrhythmias–heartblock
Mechanical• Valvularinsufficiency(severe)• Valve/chordaerupture• Septalwalldefect• Atrialmyxoma• Freewallrupture
ObstructivePulmonaryVascular• PEwithRVstrain• SeverePAH• Pulmonicortricuspidvalveobstruction• Airembolism
Mechanical• Tensionpneumothorax• Hemothorax• Tamponade• Constrictivepericarditis• Restrictivecardiomyopathy• IntrinsicPEEP• Abdominalcompartmentsyndrome
Distributive–Septicvsnon-septicNon-septic
• Inflammatory–burns,pancreatitis,post-bypass,post-arrest,amnioticandfatembolism• Neurogenic–braininjury,spinalcordinjury,neuro-axialanesthesia• Anaphylactic–allergicreaction(food,meds,insectbite),exerciseorheatinduced• Other–adrenalinsufficiency,thyrotoxicosis,myxedemacoma,heavymetalpoisoning,toxicshocksyndrome
Hypovolemic–hemorrhagicvsnon-hemorrhagicNon-hemorrhagic
• GIlosses–vomiting,diarrhea• Skinlosses–heatstroke,burns• Renallosses–diuretics,salt-wastingnephropathy,hypoaldosteronism• Thirdspacelosses–postop,intestinalobstruction,pancreatitis,cirrhosis
ShockType Cardiacoutput PCWPHypovolemic ↓ ↓Cardiogenic ↓ ↑Obstructive ↓ Normalor↑Distributive ↑ ↓ornormal
FluidsandPressors
• Agoodfluidbolusisabout30cc/kg–thencheckforresponse(examandhemodynamicchanges)• Firstlinepressor=norepinephrine(alpha1>beta1)• Secondline:Epinephrine(beta1>beta2>alpha1)-God’sowncatecholamine!• AddtoNE:Vasopressin(AVPanalog;mayupregulatebeta1receptors)• PhenylephrineAKAwater(alpha1)-usewhentachyarrhythmiasareaproblem• Dopamine(dosedependenteffects:5mg=dopa,10mg=beta1,15mg=alpha1)• Dobutamine(beta2thenbeta1)-probablywillneedNEunderneathtooffsetfallinperipheralvascularresistance

Toxicology
Airway Tips • When intubating- use rocuronium. Do not use succinylcholine in case of cholinergic toxicity • In salicylate poisoning, avoid intubation. The hyperventilation is beneficial and difficulty to replicate. • If a patient is compensating for a metabolic acidosis, i.e., toxic alcohol, and begin to tire or have a seemingly normal
pCO2, then intubate.
Toxidrome Exam Pupils Discerning Features
Examples
Sympathomimetic Hyperalert, hallucinations, hyperthermia, tachycardia
Dilated Wide pulse pressure, hyperreflexia, seiure
Cocaine, amphetamines, ephedrine, caffeine, theophylline
Anticholinergic Agitation, hallucinations, delirium, fever, tachycardia, hypertension
Dilated Dry skin and mucous membranes, flushing, urinary retention, picking
Antihistamines, TCA, Parkinson meds, phenothiazines (chlorpromazine, Compazine)
Hallucinogenic Hallucinations, agitation, synesthesia, fever, tachycardia
Dilated Nystagmus PCP, LSD, psilocybin, MDMA
Opioid CNS depression, apnea, bradycardia
Constricted Pulmonary edema, track marks
Heroin, fentanyl, methadone
Sedative Confusion, stupor, coma
Varies BZD, barbiturates, alcohols, zolpidem
Cholinergic Confusion, coma, bradycardia, hypothermia
Constricted Salivation, diaphoresis, incontinence, diarrhea, fasciculations
Pesticides (organophosphates), nicotine, physostigmine, bethanechol
Serotonin syndrome
Confusion, agitation, hyperthermia, tachycardia
Dilated Tremor, myoclonus, clonus, diaphoresis, trismus, rigidity
SSRIs, meperidine, dextromethorphan, TCAs, MAOIs
Testing Tips • Always check for acetaminophen and salicylates- difficult to diagnosis and treatments should be implemented early • Rapid drugs of abuse screens are immunoassays that have some false positives and negatives • Comprehensive screening is mass spectrometry and takes longer- this rarely leads to management changes
Toxin Antidote Cyanide (nitroprusside) Hydroxocobalamin (vit B12) IV 5 grams (or thiosulfate) Methemoglobinemia Methylene blue IV 2mL/kg Digoxin Digoxin Fab IV 2-5 vials Calcium channel blocker 10% Calcium chloride IV 20mL
Insulin IV 0.5-1 units /kg with dextrose Local anesthetic 20% Intralipid bolus IV 1.5 mL/kg Sodium channel blocker (anti-arrhythmic, TCA, antihistamines, cocaine)
Sodium bicarbonate IV 100 mL
Cholinergic Atropine IV 2 mg- double every 3-5 min as needed