Acute Pancreatitis due to Ischaemia-reperfusion Injury After Mesenteric Revascularisation
3
EJVES Extra 4, 43–45 (2002) doi:10.1053/ejvx.2002.0122, available online at http://www.idealibrary.com on SHORT REPORT Acute Pancreatitis due to Ischaemia-reperfusion Injury After Mesenteric Revascularisation A. Mahmood 1 , M. Sintler 1 , M. Duddy 2 and R. K. Vohra∗ 1 Departments of 1 Vascular Surgery and 2 Radiology, University Hospital Birmingham NHS Trust, Selly Oak Hospital, Birmingham B29 6JD, U.K. Introduction We present a rare case of acute pancreatitis due to ischaemia-reperfusion injury after mesenteric re- vascularisation for chronic mesenteric ischaemia. This patient had undergone various interventions for ab- dominal pain before a vascular pathology was con- sidered. Case Report A 66-year-old female presented to the surgical clinic with a history of worsening postprandial epigastric pain and a loss of 3 kg in weight over the preceding 8 months. For these symptoms, she had previously had Helicobacter pylori eradication and a chole- cystectomy for a non-functioning gall bladder 6 months prior to presentation. She had undergone a vagotomy and pyloroplasty 22 years previously for a duodenal ulcer. She was a smoker and had a left iliac angioplasty in the past for intermittent claudication. General examination revealed an emaciated patient. There were renal bruits on abdominal examination Fig. 1a. Occluded origins of IMA and SMA. The thick arrow shows but little else. A diagnosis of mesenteric angina was the superior haemorhoidal anastomosis. The thin arrow shows the made and an aortogram (Fig. 1a) revealed occluded occluded IMA origin. origins of the coeliac axis, superior and inferior mes- enteric arteries (SMA and IMA). The SMA re- was perfused by the superior haemorhoidal ana- constituted via the wandering artery (Fig. 1b), which stomosis. It was decided that she would require mes- enteric revascularisation, with an iliac to SMA graft. The patient presented before planned surgery as an ∗ Please address all correspondence to: R. K. Vohra, Consultant emergency with acute abdominal pain and unable to Vascular Surgeon University, Hospital Birmingham NHS Trust, Selly Oak Hospital, Birmingham B29 6JD, U.K. drink water, which would exacerbate the pain. She was 1533–3167/02/040122+03 $35.00/0 2002 Published by Elsevier Science Ltd
Transcript of Acute Pancreatitis due to Ischaemia-reperfusion Injury After Mesenteric Revascularisation

EJVES Extra 4, 43–45 (2002)doi:10.1053/ejvx.2002.0122, available online at http://www.idealibrary.com on
SHORT REPORT
Acute Pancreatitis due to Ischaemia-reperfusion Injury After MesentericRevascularisation
A. Mahmood1, M. Sintler1, M. Duddy2 and R. K. Vohra∗1
Departments of 1Vascular Surgery and 2Radiology, University Hospital Birmingham NHS Trust, Selly Oak Hospital,Birmingham B29 6JD, U.K.
Introduction
We present a rare case of acute pancreatitis due toischaemia-reperfusion injury after mesenteric re-vascularisation for chronic mesenteric ischaemia. Thispatient had undergone various interventions for ab-dominal pain before a vascular pathology was con-sidered.
Case Report
A 66-year-old female presented to the surgical clinicwith a history of worsening postprandial epigastricpain and a loss of 3 kg in weight over the preceding8 months. For these symptoms, she had previouslyhad Helicobacter pylori eradication and a chole-cystectomy for a non-functioning gall bladder 6months prior to presentation. She had undergone avagotomy and pyloroplasty 22 years previously for aduodenal ulcer. She was a smoker and had a left iliacangioplasty in the past for intermittent claudication.
General examination revealed an emaciated patient.There were renal bruits on abdominal examination
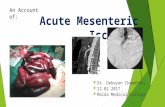
Fig. 1a. Occluded origins of IMA and SMA. The thick arrow showsbut little else. A diagnosis of mesenteric angina wasthe superior haemorhoidal anastomosis. The thin arrow shows themade and an aortogram (Fig. 1a) revealed occluded occluded IMA origin.
origins of the coeliac axis, superior and inferior mes-enteric arteries (SMA and IMA). The SMA re-
was perfused by the superior haemorhoidal ana-constituted via the wandering artery (Fig. 1b), whichstomosis. It was decided that she would require mes-enteric revascularisation, with an iliac to SMA graft.
The patient presented before planned surgery as an∗ Please address all correspondence to: R. K. Vohra, Consultant emergency with acute abdominal pain and unable toVascular Surgeon University, Hospital Birmingham NHS Trust, SellyOak Hospital, Birmingham B29 6JD, U.K. drink water, which would exacerbate the pain. She was
1533–3167/02/040122+03 $35.00/0 2002 Published by Elsevier Science Ltd

A. Mahmood et al.44
Fig. 1b. Wandering artery perfused by IMA (arrow to right). Superiormesenteric artery (oblique arrow) reconstitutes via the wandering Fig. 2a. Right iliac to superior mesenteric artery graft stenoses.artery (arrow to left). Arrows show these in proximal segment and midpoint of the graft.
midpoint of the graft (Fig. 2a). These stenoses weredehydrated and tachycardic. Abdominal examination successfully angioplastied to 6 mm (Fig. 2b). However,revealed a tender abdomen without peritonism. The graft occlusion at 18 months necessitated further sur-serum amylase was 138 mg/dl without a leucocytosis. gery and graft revision.A diagnosis of an acute exacerbation of chronic mes- This graft has remained patent up to over 3 yearsenteric ischaemia was made with a decision to proceed of follow-up on 6-monthly Duplex ultrasound sur-to immediate operation. Laparotomy did not reveal veillance. She has, however, required angioplasty forsigns of acutely ischaemic bowel and a right iliac to a right common iliac artery stenosis below the ana-SMA bypass was carried out using reversed long stomosis.saphenous vein from the right leg.
On the second postoperative day the patient becamehaemodynamically unstable and acidotic withoutsigns of hypovolaemia. The serum amylase was found Discussionto be 1872 mg/dl. A contrast-enhanced computerisedtomography (CT) scan revealed pancreatic oedema Chronic mesenteric ischaemia may present with symp-
toms similar to peptic ulcer disease and cholelithiasis.without signs of necrosis while angiography revealeda functioning graft. A diagnosis of severe acute pan- This case highlights the fact that patients with athero-
sclerosis and normal gastrointestinal investigationscreatitis was made. She required 12 days of intensivecardiorespiratory support having developed the com- warrant vascular investigation.
Chronic mesenteric ischaemia can be managed byplications of the systemic inflammatory response syn-drome (SIRS) and the acute respiratory distress complete revascularisation to the coeliac axis, superior
and inferior mesenteric arteries or selectively to in-syndrome (ARDS).Five months later, a colour flow Duplex Doppler dividual arteries.1–3 Endovascular techniques have also
been employed successfully.4 However, no randomisedscan revealed stenoses at the iliac origin and the
EJVES Extra, 2002

Acute Pancreatitis due to Ischaemia-reperfusion Injury 45
In this case, an ischaemic pancreas was re-vascularised. The diagnosis of ischaemia reperfusion-induced pancreatitis in this case is supported by theabsence of other causes of pancreatitis. A non-func-tioning gall bladder had been removed previously andthere was no evidence of pancreatitis preoperatively.In addition the operative dissection was remote fromthe pancreas during the operation. Furthermore, thehyperamylasemia could not have been due to isch-aemic small bowel as the angiogram showed a patentgraft. The diagnosis of acute pancreatitis was con-firmed by the presence of pancreatic oedema on theCT scan.
The patient in this case was obviously very unwelland there was a definite risk of mortality from SIRSand ARDS. Endotoxaemia associated with these mayhave been due to pancreatitis although ischaemia-reperfusion injury to the small bowel causing thesecomplications cannot be excluded.
This case highlights the fact that one should be alertto the risk of acute pancreatitis and possibly SIRS whenconsidering mesenteric revascularisation especially incases with occlusion of the coeliac axis, superior andinferior mesenteric arteries.
References
Fig. 2b. Angioplasty for right iliac to superior mesenteric artery 1 Foley MI, Moneta GL, Abou-Zamzam AM Jr et al. Re-graft stenoses. vascularisation of the superior mesenteric artery alone for treat-
ment of intestinal ischaemia. J Vasc Surg 2000; 32: 37–47.2 Schneider DB, Nelken NA, Messina LM, Ehrenfeld WK. Isol-
ated inferior mesenteric artery revascularization for chronic vis-controlled trial exists to compare the various pro-ceral ischaemia. J Vasc Surg 1999; 30: 51–58.cedures.
3 Cappeller WA, Hubner GH, Kettmann R, Behrmann C. Sur-Microvascular ischaemia-reperfusion injury has gical therapy of chronic visceral arterial ischaemia with aorto-coeliac mesenteric patch bypass. Chirurg 1998; 69: 642–647.been implicated in the pathogenesis of acute pan-
4 Nyman U, Ivancev K, Lindh M, Uher P. Endovascular treatmentcreatitis5 secondary to the common aetiologies of al-of chronic mesenteric ischaemia. Cardiovasc Intervent Radiol 1998;cohol and gallstones. Ischaemia reperfusion injury 21: 305–313.
5 Toyama MT, Lewis MP, Kusske AM et al. Ischaemia-reperfusionleading to acute pancreatitis following thoraco-ab-mechanisms in acute pancreatitis. Scan J Gastro 1996; 219 (Suppl.):dominal aortic aneurysm repair6 has been documented20–23.but not in the setting of mesenteric revascularisation 6 Gullo L, Cavicchi L, Tomasetti P et al. Effects of ischaemia onthe human pancreas. Gastroenterology 1996; 111: 1033–1038.procedures.
EJVES Extra, 2002