ACUTE OTITIS MEDIA AOM, Bacterial Otitis Media · Early acute bacterial otitis media (AOM)....
26
ACUTE OTITIS MEDIA AOM, Bacterial Otitis Media © Bruce Black MD
Transcript of ACUTE OTITIS MEDIA AOM, Bacterial Otitis Media · Early acute bacterial otitis media (AOM)....

ACUTE OTITIS MEDIA AOM, Bacterial Otitis Media
© Bruce Black MD

Early acute bacterial otitis media (AOM). Bacterial infection secondary to a URTI has soiled the middle ear.
Inflammation and a purulent effusion are developing. © Bruce Black MD

Developing inflammation with progressive AOM. Substantial moist cerumen in the EAC.
© Bruce Black MD

Pus under pressure distending the drum. Pneumococcus, H. influenzea and moraxella are the main culprits.
© Bruce Black MD
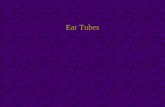
Advanced drum distension due to purulent middle ear effusion under pressure.
© Bruce Black MD

Grossly distended pars tensa, characteristic radial inflammation. Deafness, pain and malaise likely.
© Bruce Black MD
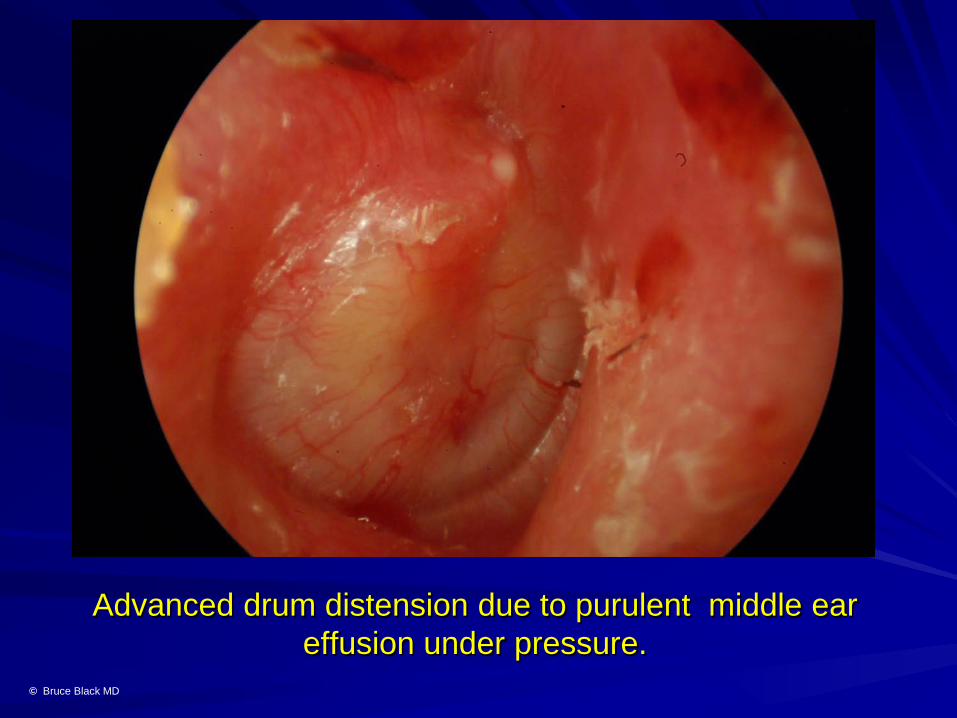
Extreme drum distension, pain, distress. In an adult, consider an acute myringotomy to relieve pain.
© Bruce Black MD

Early bleb formation on the posterior left pars tensa. Serous fluid is forced through the collagenous layer of the drum ,
raising small blisters on same. © Bruce Black MD
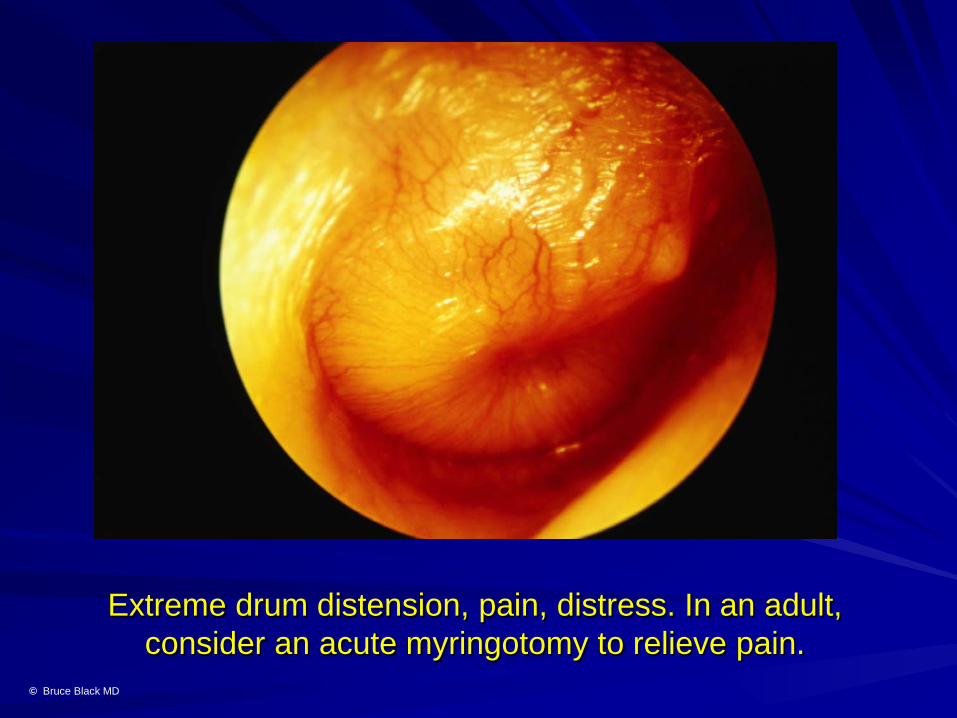
Advanced bleb formation on the drum causing maceration of the lateral, squamous epithelial layer of the pars tensa.
© Bruce Black MD
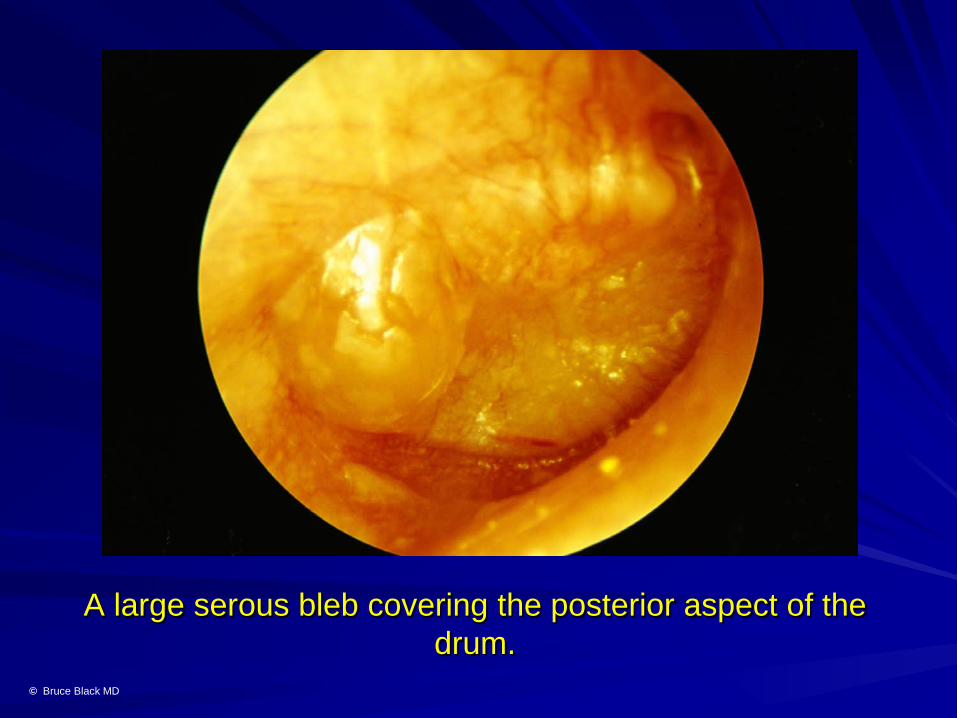
A large serous bleb covering the posterior aspect of the drum.
© Bruce Black MD
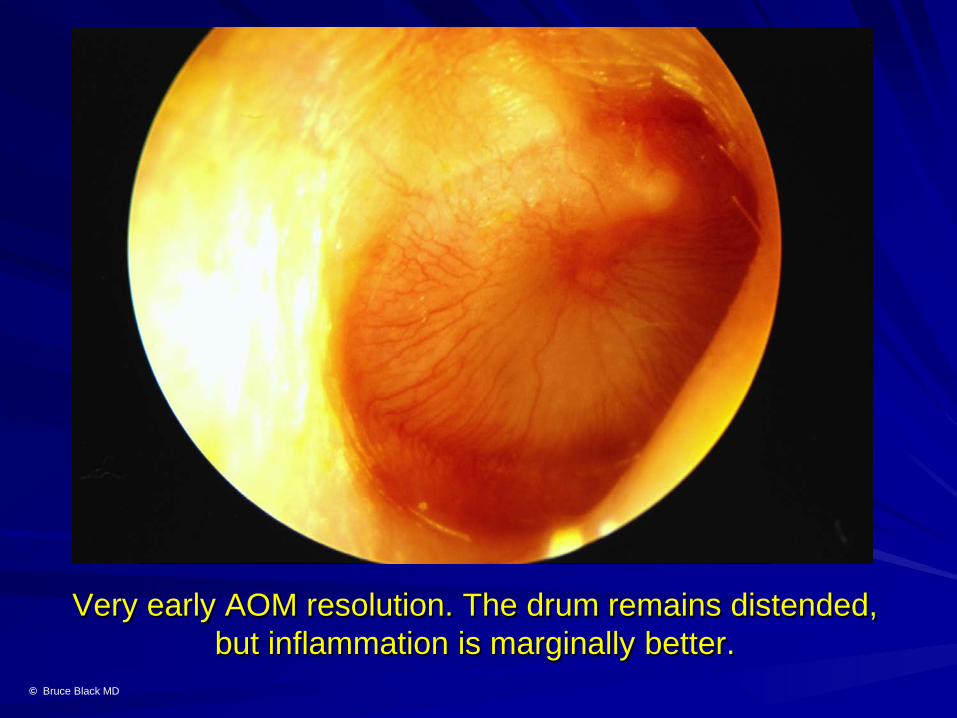
Very early AOM resolution. The drum remains distended, but inflammation is marginally better.
© Bruce Black MD
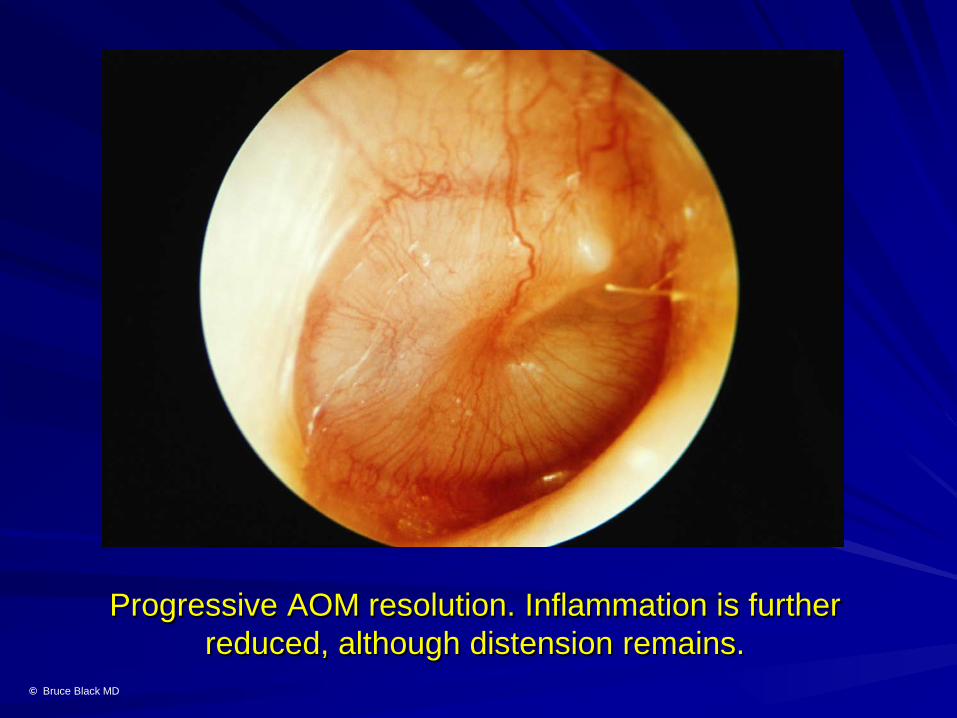
Progressive AOM resolution. Inflammation is further reduced, although distension remains.
© Bruce Black MD

Early AOM resolution phase. Successful treatment with amoxycillin/clavulanic acid has diminished drum distension
and inflammation. © Bruce Black MD

Perforation subsequent to AOM. The pinhole at 8 o’clock relieves pressure and promotes a more rapid resolution of symptoms. Permanent perforation is uncommon, if treated. © Bruce Black MD

Perforated AOM. Generally a tiny pinhole defect is present, healing rapidly over a few days.
© Bruce Black MD

Perforated AOM. Profuse discharge of mucopurulent effusion from the EAC. Clean thoroughly, treat with
amoxycillin/clavulanic acid plus antibiotic drops. © Bruce Black MD
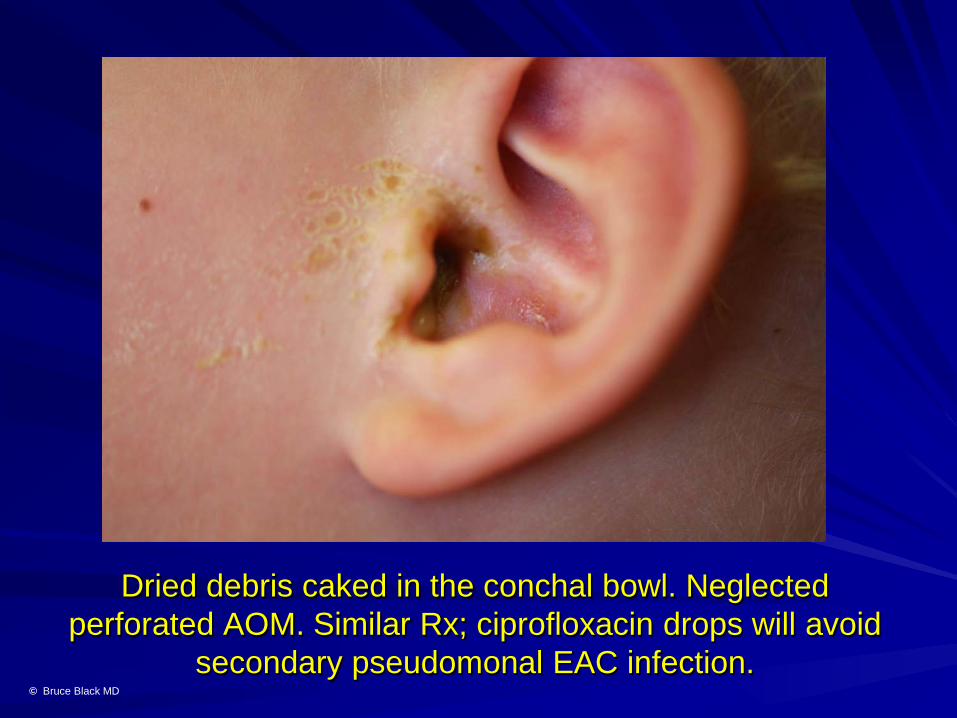
Dried debris caked in the conchal bowl. Neglected perforated AOM. Similar Rx; ciprofloxacin drops will avoid
secondary pseudomonal EAC infection. © Bruce Black MD
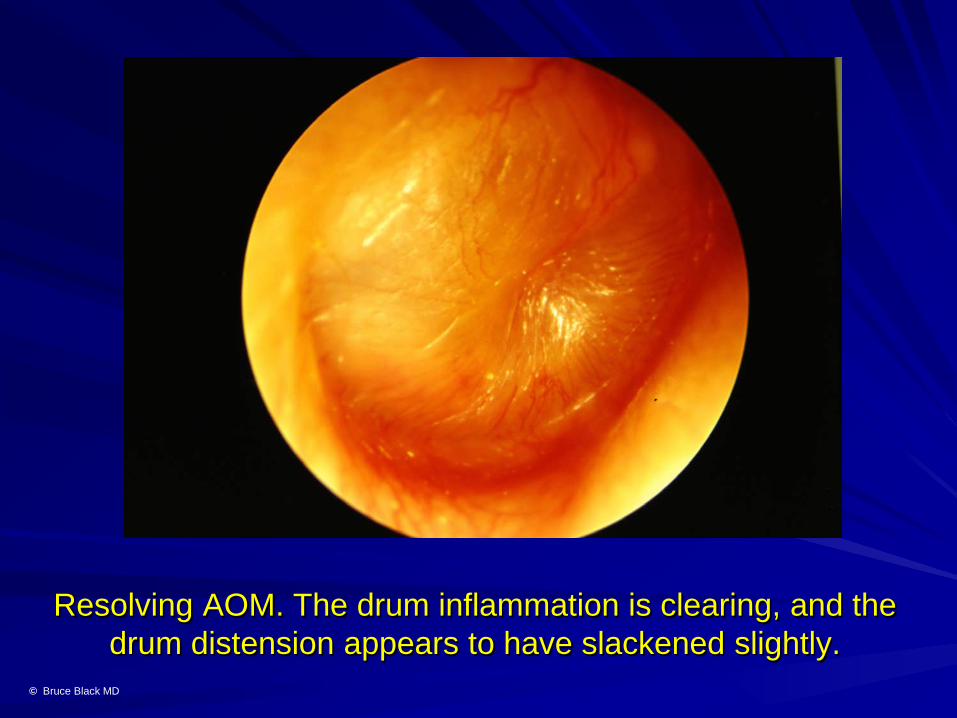
Resolving AOM. The drum inflammation is clearing, and the drum distension appears to have slackened slightly.
© Bruce Black MD

Resolving AOM. The inflammatory reaction has largely settled, although the drum remains distended by sterile
effusions. © Bruce Black MD
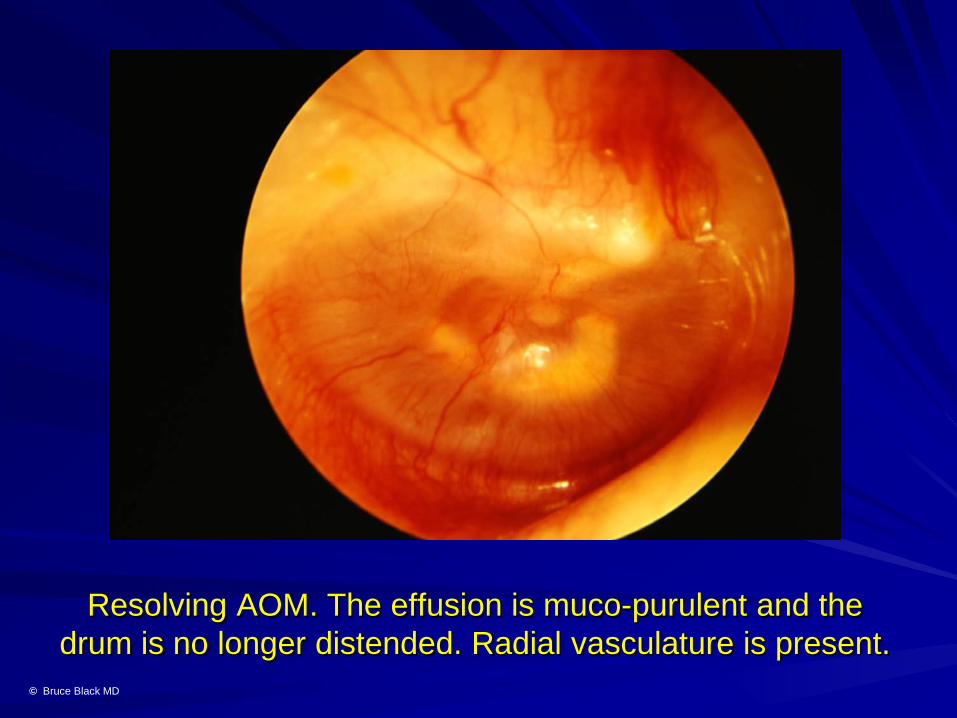
Resolving AOM. The effusion is muco-purulent and the drum is no longer distended. Radial vasculature is present.
© Bruce Black MD

Early re-aeration during resolution of AOM. A fluid level is seen anterosuperiorly behind the right pars tensa. Mild
inflammation persists. © Bruce Black MD

Bubbles are evident in the purulent effusion as the AOM resolves. Inflammation is absent.
© Bruce Black MD

Advancing re-aeration. Multiple bubbles are evident; inflammation has cleared and the effusion is now mucoid
rather than purulent. © Bruce Black MD

Advanced AOM resolution phase. Inflammation has cleared, the drum has regained transparency, and a fluid
level over sterile effusion is evident. © Bruce Black MD
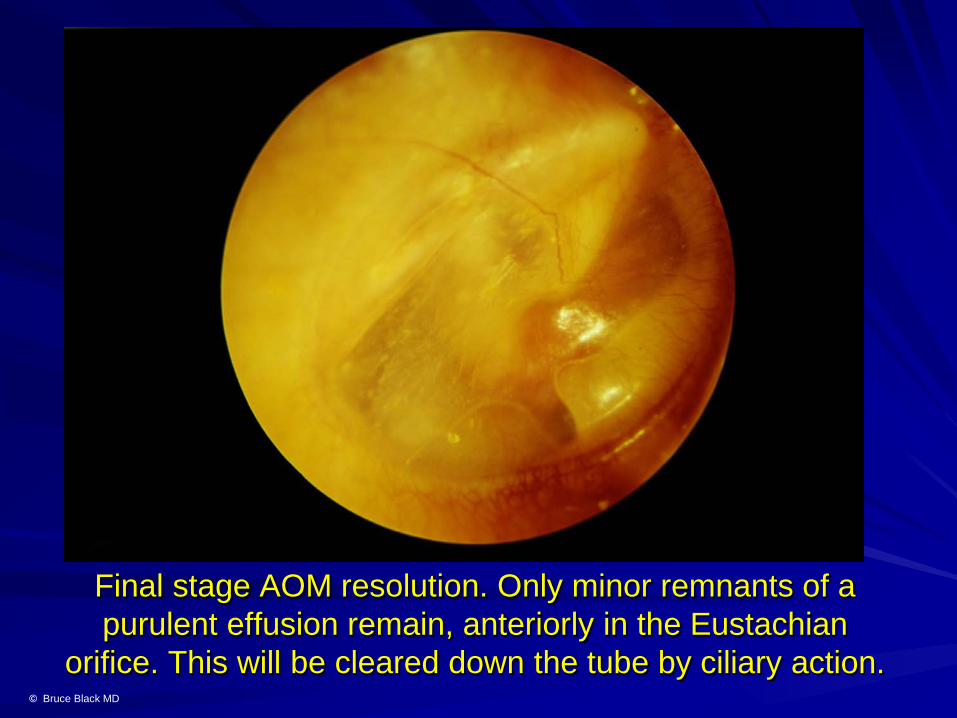
Final stage AOM resolution. Only minor remnants of a purulent effusion remain, anteriorly in the Eustachian
orifice. This will be cleared down the tube by ciliary action. © Bruce Black MD
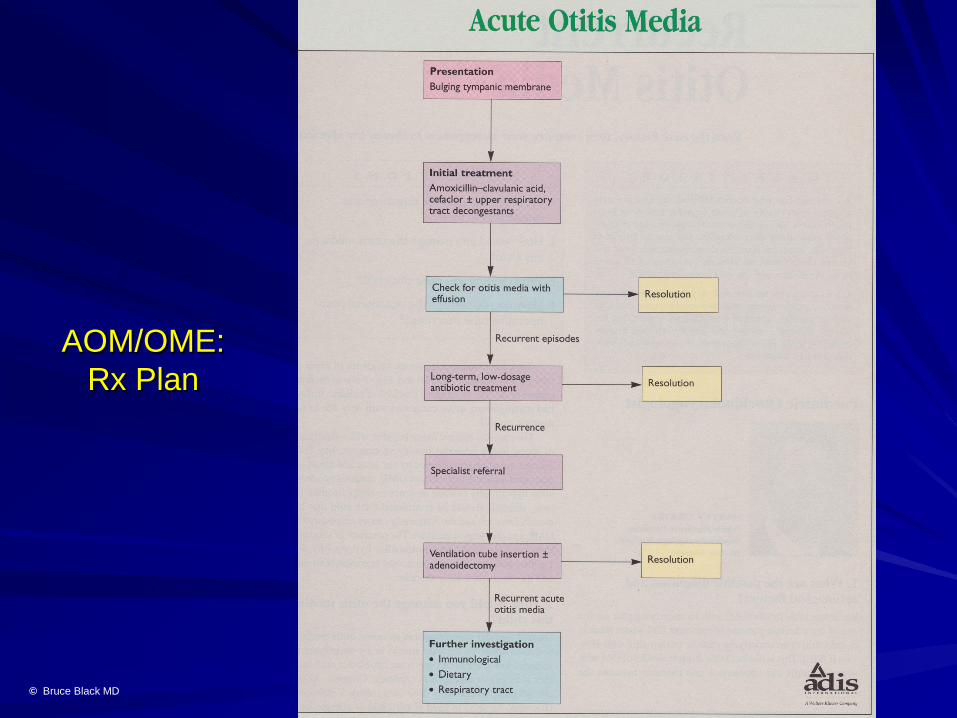
AOM/OME: Rx Plan
© Bruce Black MD