Acute Management of Stable Narrow Complex Tachycardia Mini Lecture 2013.
20
Acute Management of Stable Narrow Complex Tachycardia Mini Lecture 2013
Transcript of Acute Management of Stable Narrow Complex Tachycardia Mini Lecture 2013.

Acute Management of Stable
Narrow Complex Tachycardia
Mini Lecture
2013

Objectives
• Review the initial approach to diagnose and treat narrow complex tachycardia
• Review examples of AVNRT, AVRT, Atrial Tachycardia
• This is not a comprehensive review of all the narrow complex tachycardias
• You are not expected to manage these patients on your own, always ask for back up

Case
• Nurse calls to inform you that bed 10’s heart rate just went up to 200s on telemetry. Which of the following information should you obtain asap?A. Blood pressureB. Mental statusC. EKGD. Focused Physical ExamE. All of the above

Case
• Nurse calls to inform you that bed 10’s heart rate just went up to 200s on telemetry. Which of the following information should you obtain asap?A. Blood pressureB. Mental statusC. EKGD. Focused Physical ExamE. All of the above

Narrow Complex Tachycardia • Rate >100 (often 150-250)• QRS <120 msec
– Regular• Sinus tachycardia (usually <150)• AVNRT• AVRT• Atrial Tachycardia• Atrial Flutter with regular block (150, 100, 75)
– Irregular• Atrial Fibrillation• MAT

Initial Assessment for Tachycardia
Questions
• Symptomatic?
• Hypotensive?
• 12 lead EKG
• IV access
Stable or Unstable?
• Altered Mental Status
• Hypotension
• Chest Pain
• Acute SOB
• Hypoxia

Unstable?
• Crash Cart• ACLS• Call for backup
– Senior resident– Cardiology fellow– Nocturnist– Code blue

Stable?Initial Assessment
• Focused H&P– Talk to the patient to assess mental status– Reason for admission (sepsis, ACS)– Cardiac Hx (CAD, HF, Afib, SVT)– Recent electrolytes– Medications (AV nodal agents, digoxin)– Listen to heart and lungs– Volume status– JVD

EKG shows..

Too fast to interpret rhythm?
• Vagal Maneuvers and Adenosine – Slow down the rhythm– Terminate certain SVTs which conduct
through the AV node– If possible obtain 12 lead EKG recording
during intervention

• Vagal maneuvers– Bearing down– Face in ice cold water– Carotid Massage– Blowing into a folded straw– Cough
• Adenosine– May avoid if bronchospasm/asthma/COPD?– Caution if history of pre-exitation/ WPW?*– Warn them about the symptoms
• 6mg IV push followed by NS flush followed by• 12mg IV push followed by NS flush

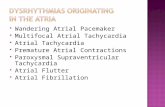
AVNRT
Cause• Dual AV nodal pathways
with differing refractory periods
• Often initiated by a PAC• 60% SVT
DX• Rate 150-250• Inverted p or “psuedo S”
Tx• Vagal • Adenosine• BB: Metoprolol 5mg q5min x3 • CCB: Diltiazem 10mg IV,
repeat 10-30mg IV in 5-10 min

AVNRT
PSUEDO S WAVES

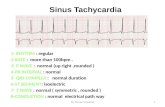
AVRT
Cause• Re-entrant tachycardic
circuit with conduction down AV node and back up a bypass tract (i.e. WPW)
• 30% SVT
Dx:• Rate 150-250 • Retrograde P inferior leads
Tx:• Vagal • Adenosine• BB: Metoprolol 5mg min q5 x 3• CCB: Diltiazem 10mg IV, repeat
10-30mg IV in 5-10 min

AVRT

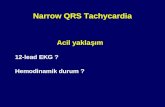
Atrial TachycardiaCause• Enhanced Automaticity of atrial
tissue or ectopic atrial pacemaker
• 10% SVT
Dx• P wave precedes each
QRS• Unusual p wave axis• Adenosine may show
continued atrial beats, without AV conduction
Tx:• BB: metoprolol 5mg q5 x 3• CCB: Diltiazem 10mg IV,
repeat 10-30mg IV in 5-10 min

QuickTime™ and a decompressor
are needed to see this picture.
ADENOSINE
Atrial Tachycardia
Unusual p wave axis Continued atrial automaticity

General Principles
• Note the common theme: Vagal Maneuvers, Adenosine, Beta Blockers, Calcium Channel Blockers, caution in WPW
• Check vitals (BP) frequently during acute setting to make sure a stable situation does not become unstable
• Again, this is meant to be a review of the initial management of SVT you are not expected to independently manage these patients- Call for backup!

Case Follow Up
• Nurse calls: “ Bed 10’s heart rate just went up to 200s”
• You reply:– What is his blood pressure?– Is his arousable and oriented?– Please get a 12 lead EKG now– Does he have IV access?– I’ll be right there..

References
• UpToDate
• Med Res UCLA http://medres.med.ucla.edu/
• FP Notebook http://www.fpnotebook.com/
• Images sited previously