Acute Ischaemic Stroke Mx SCGH - ED Update
52
ED Stroke Update DAVID BLACKER Neurologist & stroke physician, Sir Charles Gairdner Hospital Clinical Professor of Neurology University of WA Medical Director WA Neuroscience Research Institute No disclosures
-
Upload
scgh-ed-cme -
Category
Health & Medicine
-
view
135 -
download
3
Transcript of Acute Ischaemic Stroke Mx SCGH - ED Update

ED Stroke Update
DAVID BLACKER
Neurologist & stroke
physician,
Sir Charles Gairdner
Hospital
Clinical Professor of
Neurology
University of WA
Medical Director
WA Neuroscience Research
InstituteNo disclosures

?Best Rx for large clots


Logistic regression curve representing an estimate of the probability for successful
recanalization of occluded vessels by intravenous thrombolysis (IVT) depending on thrombus
length.
Riedel C H et al. Stroke 2011;42:1775-1777
Copyright © American Heart Association

Solitaire FR Stentriever
possibly the preferred option

Basilar thrombosis- SCGH case
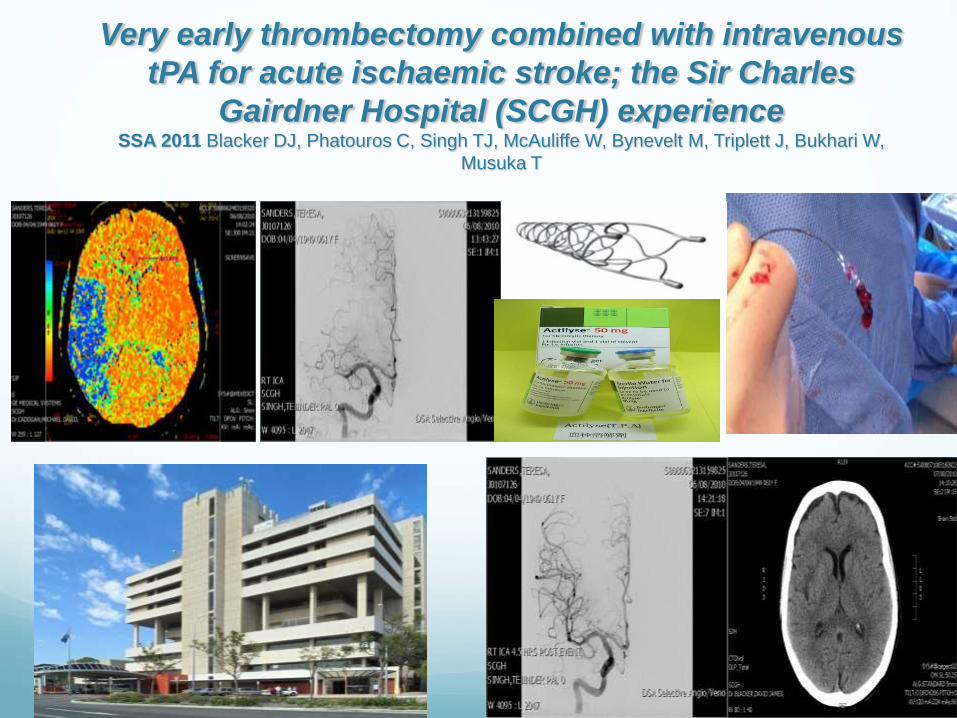
Very early thrombectomy combined with intravenous
tPA for acute ischaemic stroke; the Sir Charles
Gairdner Hospital (SCGH) experienceSSA 2011 Blacker DJ, Phatouros C, Singh TJ, McAuliffe W, Bynevelt M, Triplett J, Bukhari W,
Musuka T






Recent transfer to SCGH Initially registrar to registrar contact
Wrong hospital
NOT a stroke
Distress to patient
Delays on return
$$$$$$
How do we do better?

Is transfer required For stroke?
For neurological evaluation
Who is to benefit from the transfer?
Patient?
Family?
Doctors?

Stroke Units In Utopia
All patients should be managed in a stroke unit, since
the evidence suggests better outcomes.

Stroke UnitsStroke Unit benefits
Benefit 5.6/100
reduced mortality (22% v 26%)
reduced dependency (56% v 62%)
reduced cost of care ($10-16 000 savings)
LOS reduced 2-11 days

Stroke UnitsStroke unit features
geographically distinct
comprehensive assessment
co-ordinated MDT
early mobilisation (avoid bed rest)
staff with interest; ongoing training and education
team meetings (DC planning)
encourage patient participation in rehab

Stroke UnitsReasons for benefit
application of proven treatments
?more intense monitoring of physiology
anticipation, early recognition, and treatment of complications
volume of practice
audit, review, QA, research
enthusiastic, expert staff

Stroke Unit- Physician role Knowledge of stroke and TIA
Accurate determination of mechanism
Institution of appropriate Rx;
eg anti-coagulation for AF
CEA -symptomatic high grade stenosis
Correct Dx of mimics

Patients to transfer to teritary or
“quaternary” centres
1. Acute therapy for ischaemic stroke; depends on system of care
2. Most cases of ICH (if active treatment planned)
3. Young massive MCA, candidates for decompression.
4. Cerebellar infarct > 3cm, candidate for decompression.
5. Carotid revascularization.
6. Dx unclear, advanced workup required (neuro opinion, MRI, TOE, LP)

Consultant to consultant
discussion Early advice on Dx
Early advice on interventions
In the future; IV tPA
“Big picture” discussion on goals of transfer
Chance for education

ACUTE STROKE- EVERY MINUTE COUNTS
1 minute= 1.9 million neurons
14 billion synapses
7.5 miles of myelinated fibres

IV tPA meta-analysis – level 1 evidence
Lees et al Lancet 2010
NNT
4.5 9 14.1
Time is BRAIN!
Treatment effect
p<0.001
Interaction with
time p=0.03
4.5 hours

Future strategies Can thrombectomy be expanded to more patients?

Slowing the clock
Expanding the time window

Neuroprotective agents in the field

Figure 1 The stroke emergency mobile unit with CT scanner on boardNote the CT scanner in
the back of the cabin and the separated shielded workstation on the right behind the door.
Weber J E et al. Neurology 2013;80:163-168
© 2013 American Academy of Neurology

Pre-hospital therapies
Jeff Saver California
Unique pre-hospital stroke trial
Ethics considerations
Magnesium IV
1700 patients

72% enrolled < 60 mins post Sx onset
>150 enrolled < 30 mins
62% ischaemic stroke
22% haemorrhage
13% TIAs
3% mimics
Neutral results
Model for the future

Neuroprotective agents in the
field Peptides
Hypothermia
Minocycline
Combinations
Physical methods- TCD
Head positioning

NeuroprotectionPoly-arginine and arginine rich peptides are
neuroprotective in stroke models
Bruno Meloni et al
J Cerebral Blood Flow and Metabolism 2015 Feb 11th

The Perth Intravenous Minocyline
Stroke Study PIMSS
David Blacker
David Prentice
Edith Kohler
Tim Bates
Graeme Hankey
RPH, SCGH,
Swan Districts Hospital, UWA

van Heerden and David BlackerEdith Kohler, David A. Prentice, Timothy R. Bates, Graeme J. Hankey, Anne Claxton, Jolandi
Meta-AnalysisIntravenous Minocycline in Acute Stroke : A Randomized, Controlled Pilot Study and
Print ISSN: 0039-2499. Online ISSN: 1524-4628 Copyright © 2013 American Heart Association, Inc. All rights reserved.
is published by the American Heart Association, 7272 Greenville Avenue, Dallas, TX 75231Stroke published online July 18, 2013;Stroke.
http://stroke.ahajournals.org/content/early/2013/07/18/STROKEAHA.113.000780
World Wide Web at: The online version of this article, along with updated information and services, is located on the
http://stroke.ahajournals.org//subscriptions/
is online at: Stroke Information about subscribing to Subscriptions:
http://www.lww.com/reprints Information about reprints can be found online at: Reprints:
document. Permissions and Rights Question and Answer process is available in the
Request Permissions in the middle column of the Web page under Services. Further information about thisOnce the online version of the published article for which permission is being requested is located, click
can be obtained via RightsLink, a service of the Copyright Clearance Center, not the Editorial Office.Strokein Requests for permissions to reproduce figures, tables, or portions of articles originally publishedPermissions:
by GRAEME HANKEY on July 23, 2013http://stroke.ahajournals.org/Downloaded from

The West Australian Intravenous
Minocycline and tPA Stroke Study
(WAIMATSS)
A pilot study of a strategy to reduce
haemorrhagic transformation
David Blacker
Mike Bynevelt
David Prentice
Graeme Hankey
Tim Bates
Andrew Kelly
Tony Alvaro

20% STROKE: ICH
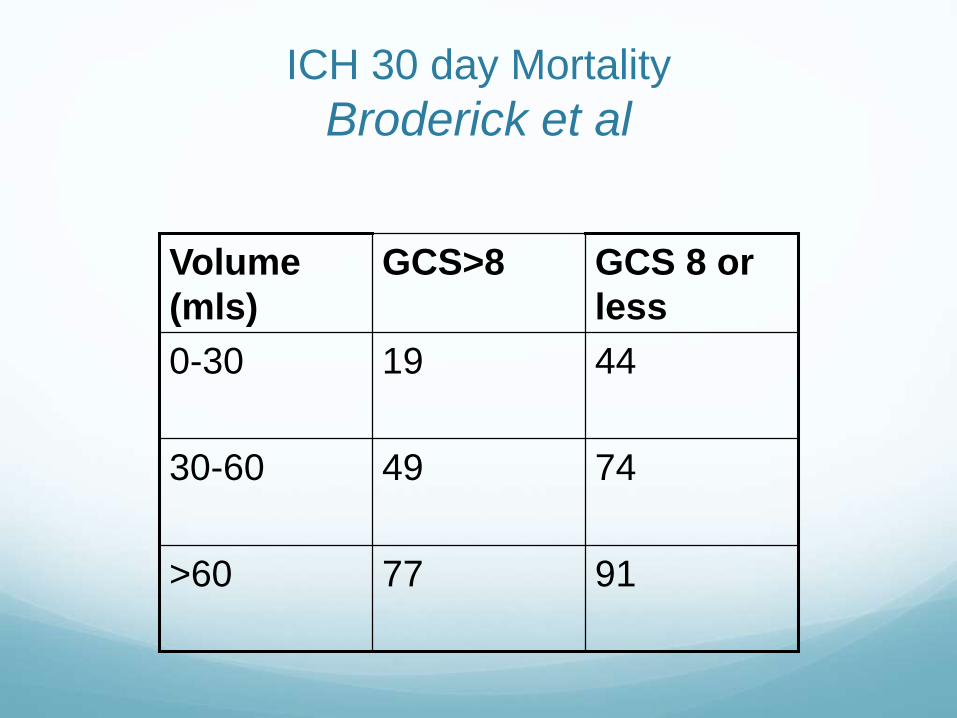
ICH 30 day Mortality
Broderick et al
9177>60
744930-60
44190-30
GCS 8 or
less
GCS>8Volume
(mls)

Stereotactic ICH Aspiration

ICH is Dynamic

Figure CT scans Baseline noncontrast CT shows heterogeneous right deep parenchymal
hemorrhage (A).
Bermejo P G et al. Neurology 2010;75:834-834
©2010 by Lippincott Williams & Wilkins
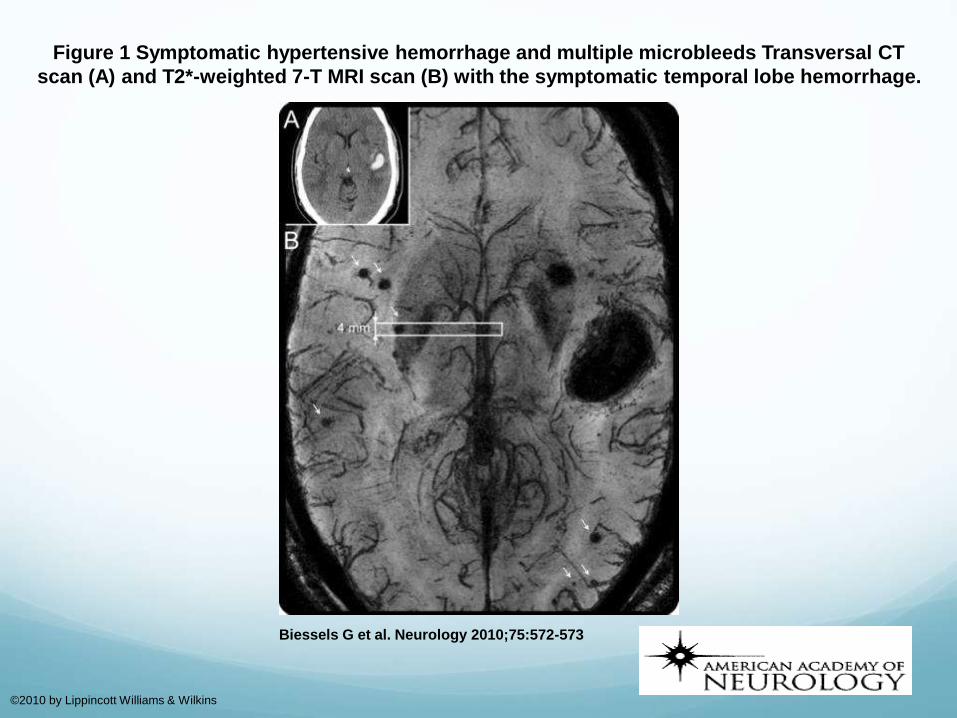
Figure 1 Symptomatic hypertensive hemorrhage and multiple microbleeds Transversal CT
scan (A) and T2*-weighted 7-T MRI scan (B) with the symptomatic temporal lobe hemorrhage.
Biessels G et al. Neurology 2010;75:572-573
©2010 by Lippincott Williams & Wilkins


? An endovascular approach
to ICHPerforator stroke following intracranial stenting. A
sacrifice for the greater good?
Levy E, Chaturvedi S.
Neuology 2006;66:1803-4. Editorial





Instead of ...

“Star Trek” approach
Stereotactic DXRT, or US to “cauterise” the
bleeder; activated microbubbles+ haemostatic
drug?

Other issues Secondary prevention strategies
Novel rehabilitation techniques
Organisation of services
Basic sciences
Psychology