Acute Coronary Syndromes - Illinois College of Emergency ......Acute Coronary Syndromes Page 3 iii....
24
Acute Coronary Syndromes Henry Pitzele, MD, FACEP Associate Director, Section of Emergency Medicine, Jesse Brown VA Medical Center, Chicago; Clinical Assistant Professor, Department of Emergency Medicine, University of Illinois at Chicago
Transcript of Acute Coronary Syndromes - Illinois College of Emergency ......Acute Coronary Syndromes Page 3 iii....

Acute Coronary Syndromes
Henry Pitzele, MD, FACEP
Associate Director, Section of Emergency Medicine, Jesse Brown VA Medical Center, Chicago; Clinical Assistant Professor, Department
of Emergency Medicine, University of Illinois at Chicago


Notes
Acute Coronary Syndromes Page 1
ACUTE CORONARY SYNDROMES
I. INTRODUCTION
A. Epidemiology
1. 5 million annual ED visits for CP a. 15% AMI b. 25-30% UA
2. IHD leading cause of death in US a. 500,000 annual deaths b. MI still 35% mortality
3. Released MI = malpractice payouts
B. History
1. Early 1900s: advent of arrhythmia control 2. Revolution in the ’60s
a. Catheterization b. CPR c. CCU d. EMS
3. Active reperfusion begun in 1980s
C. Definitions
1. All definitions necessarily retrospective 2. Stable angina
a. Chest pain (or ischemic angina variant) b. Transient c. Episodic d. Reproducible e. Extinguishable f. Unchanged from previous g. Canadian Cardiovascular Society
i. Class I Strenuous activity ii. Class II Slight limitation iii. Class III Severe limitation (1 block/flight) iv. Class IV Any activity/pain at rest
3. ACS a. Unstable angina: any change from previous
i. New onset angina ii. Any change in provocation iii. Increased duration iv. Increased severity

Notes
Acute Coronary Syndromes Page 2
v. Resistance to previous treatment vi. Synonyms
• Preinfarction angina • Accelerating angina • Crescendo angina • Intermediate coronary syndrome • Preocclusive syndrome
v. Evolution • 40% progress to AMI • 17% mortality without diagnosis
b. Variant angina i. AKA Prinzmetal’s Angina ii. Nonocclusive coronary vasospasm iii. STE with clinical features of AMI
c. Acute MI (WHO definition from 1960s): two of three i. Chest pain > 15-20 mins ii. No relief with NTG or rest iii. EKG changes +/- enzyme bump
d. Acute MI (2000 ACC definition) = troponin elevation plus one of the following: i. Ischemic symptoms ii. Q waves iii. ST deviation iv. PCI
II. PATHOPHYSIOLOGY
A. Mechanism: Tissue ischemia
1. Lack of oxygen delivery to tissue/muscle 2. Usually secondary to lack of blood flow 3. Continuum of hypoxia to cell death 4. Occlusion of coronary arteries 5. Usually by thrombus
B. Anatomy
1. Coronary vasculature review a. Left
i. LAD ii. Circumflex
b. Right 2. Two types of thrombi
a. White i. Platelet rich ii. Gradual onset

Notes
Acute Coronary Syndromes Page 3
iii. Only partially occlusive iv. Like rings of tree v. Thought to be cause of UA/NSTEMI
b. Red i. Caused by plaque rupture
• Change in intraluminal pressure • Mechanical shearing forces • Size/thickness of fibrous cap • Lipid content • Statins: possible plaque stabilizer?
ii. Clotting factors involved iii. Not more likely with larger lesions iv. Causes complete occlusion v. Sudden vi. Thought to be responsible for STEMI
C. Tissue Damage
1. Three steps of damage a. Acute ischemia b. Vasospasm c. Reperfusion injury
2. Two main complications a. Dysrhythmias b. Pump failure
i. No CHF 5% mortality ii. Mild CHF 15-20% mortality iii. Pulm edema 40% mortality iv. Cardiogenic shock 80% mortality
c. Rarer: papillary muscle/valvular rupture
III. DIAGNOSIS
A. History
1. Risk factors a. Age / sex b. Traditional coronary risk factors
i. HTN ii. DM iii. HL iv. Smoking v. FMH vi. Obesity
c. Known CAD 2. Pain Quality

Notes
Acute Coronary Syndromes Page 4
a. Angina ≠ ‘Chest Pain’ i. Choking / Strangulation / Constriction ii. Pressure iii. Squeezing iv. Fullness v. Burning vi. Heaviness
b. If described as ‘pain’ i. Dull / Aching ii. Less likely sharp / stabbing
c. Location i. Sternal ii. Left chest
d. Radiation i. Shoulder ii. Neck iii. Mandible iv. Arm
e. ‘Atypical’ isn’t so atypical i. Above are suggestive; 24% of patients presenting this
way have MI; 30% have UA ii. However, of all presenting with sharp / stabbing chest
pain, 5% have MI / 17% have UA iii. Up to 20% ACS for “burning” type pain iv. 19% MI’s describe as stabbing
f. Duration guidelines i. Angina < 15 min ii. MI > 15 min iii. Generally not ACS when < 1 second iv. Hours of pain = large differential
g. Provocation i. Exertion ii. Cold iii. Food
h. Relief i. Rest ii. NTG iii. (reperfusion)
i. Associated symptoms i. Diaphoresis ii. N/V iii. Dizziness iv. Anxiety v. Dyspnea
j. Anginal Equivalents i. Dyspnea (30% AMIs!)

Notes
Acute Coronary Syndromes Page 5
ii. Radiation pain alone iii. Dizziness iv. Weakness v. Diaphoresis
3. Special populations a. Elderly
i. Pain sensory mechanisms decreased • Nerve damage • Cortical damage • High pain thresholds • Baseline MS decrease
ii. Silent / variant ischemic syndromes more common as age increases
iii. Often present to evaluate complication, not original event b. Young
i. Symptoms often typical ii. No age immune
c. DM i. More MIs ii. Earlier MIs iii. Asymptomatic MIs iv. Polyneuropathy v. Altered perception cardiac pain vi. Extensive comorbidities
4. Prior exams a. ‘Negative’ cath
i. Good for 6-12 mos ii. Negative must be truly negative; subcritical 40% lesion
could rupture at any time b. Negative stress
i. Reliable for less than 6 mos ii. And only 60-70% sensitive for CAD at time of test!
c. In either case, no result is gold
B. Physical
1. Differential a. Pleuritic / positional / palpable b. Signs
i. DVT ii. AAA
2. Complications i. CHF ii. Dysrhythmia iii. New murmur

Notes
Acute Coronary Syndromes Page 6
C. Tests
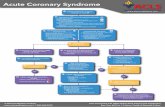
1. EKG a. Electrophysiology
i. Anatomic correlations
Anatomic Location EKG Location Coronary Artery
Septal V1-2 LAD lesion
Anterior V3-4 LAD lesion
Lateral V4-6, I, aVL Circumflex branch of LAD
Inferior II, III, aVF RCA (90%)
Posterior V8-9 Circumflex or dominant branch of RCA
Right Ventricular V4R RCA
ii. Evolution of ischemia
• ST Depression • T wave inversion • Biphasic T waves / nonspecific changes • Hyperacute T wave • ST Elevation / reciprocal depression • T wave inversion • Q waves
b. EKG’s of typical localizations of AMI i. Anteroseptal STEMI

Notes
Acute Coronary Syndromes Page 7
ii. Anterior STEMI
iii. Anterolateral STEMI
iv. Inferior STEMI

Notes
Acute Coronary Syndromes Page 8
v. Right Ventricular STEMI
vi. Posterior MI
• STD in V1, STE in V8, V9 • pathologic R’s • R/S ratio > 1 in V1-V2
c. Limitations i. Totally normal EKG: 5% have ACS ii. Nonspecific: 25% have ACS iii. 50% AMI had nondiagnostic initial EKGs iv. Immediate risk stratification: low
• Totally normal • Nonspecific ST/T wave changes • No change
i. Immediate risk stratification: higher • ST deviation • Pathologic Q • T-wave changes • LBBB • Pace • LVH
d. Confounds and Mimics

Notes
Acute Coronary Syndromes Page 9
i. LBBB • Difficult to read EKG for ischemia due to baseline ST
changes • Sgarbossa criteria for diagnosing acute ischemia in
face of LBBB → STE > 1mm concordant with QRS = 5 pts → STD > 1mm V1, V2, or V3 = 3 pts → STE > 5mm discordant with QRS = 2 pts → Score > 3 suggests MI → Score < 3 not so clear
• Presumably new LBBB with clinical MI → Acute reperfusion therapy → Historically, LBBB and AMI get less therapy
ii. Paced rhythm • Similar to LBBB
→ Reverse depolarization → Mimics and masks
• Sgarbossa criteria also predict suggest ischemia in paced rhythm—same criteria apply
iii. LVH: Features less suggestive of ischemia • Precordial leads V1-V3 should be mirror image of
V4-V4 • Concave ST • Asymmetric TWI
iv. Mimics • Benign early repolarization • Pericarditis • Left ventricular aneurysm
2. Biomarkers a. Creatine Kinase: specifically, CK-MB
i. MB fraction specific for myocardium ii. Earlier rise iii. Earlier fall iv. False positives
• Trauma • Muscular dystrophies • Rhabdomyolysis • Vigorous exercise
v. Still need serial testing b. Troponin
i. Highly sensitive and specific (definitionally) ii. Last longer in the serum iii. Predict mortality for all comers
c. Markers out of favor i. Myoglobin

Notes
Acute Coronary Syndromes Page 10
• Very early rise • Specificity too low • Does not rule out UA
ii. New markers—as yet unproven or disproven • ST2 • CRP
3. CXR a. Useful to rule out diagnoses in differential
i. Pneumonia ii. Pneumothorax iii. Rib fracture iv. Dissection
b. Seek out complications i. Pulmonary edema ii. Cardiomegaly
4. ECHO a. Ischemia begins with hypokinesis b. Progresses to paradoxic akinesis c. Relatively cheap and safe d. Disadvantages
i. Not always readily available ii. Highly operator dependent iii. Cannot differentiate AMI from
• Noninfarctional ischemia • Nontransmural infarction • Old infarct
D. Schemata / Protocols
1. Accepted standard: “Rule-out MI” a. ED enzymes triage bed type for admit b. One to two more sets at q6-8h c. Rule out UA with provocative stress vs. cath
i. Provocative factor • Exercise • Chemical
→ Persantine → Dobutamine
ii. Sensing factor • EKG • ECHO • Nuclear scintography
2. Current Trend: The Chest Pain Unit a. Goals
i. Sensitively and specifically Dx

Notes
Acute Coronary Syndromes Page 11
ii. Decrease utilization by decreasing hospital stays b. Procedure
i. Initial risk stratification ii. Rapid protocol ROMI iii. Stress before D/C
c. Prototype: The Erlanger Protocol i. Two hour rule-out ii. Initial 5-level risk stratification iii. Serial ECG’s q15 minutes iv. Comparative delta CK-MB v. Re-stratification at 2h vi. Stress almost all groups vii. Still miss a few ACS
3. Future Goal: Magic Bullet? a. Sensitivity approaching 100% b. Noninvasive c. Cheap d. Plentiful e. Fast
IV. TREATMENT
A. Management—Goals
1. Reperfuse a. Goal of TIMI-3 flow (equal flow before and after lesion) b. Outcome data obtained by bench research / tPA c. ‘Open Artery Theory’: Time = Muscle
i. Limit infarct size ii. Decreased CHF iii. Decreased mortality iv. 2 hours is watershed time—large benefit if reperfuse <
2h • Prehospital delays significant • ED delays less so
→ EKG in 10 minutes → Decision time minimization → Action time minimization
• Door to drug / balloon • 90 minutes
2. Halt clot formation / progression 3. Decrease current ischemia
a. Dilate vasculature b. Decrease myocardial demand
4. Prevent / treat complications

Notes
Acute Coronary Syndromes Page 12
B. Reperfusion Therapies
1. Thrombolysis a. Mechanism
i. Binds to fibrin-bound plasminogen ii. Turns to plasmin iii. Plasmin breaks fibrin strands iv. Clot busted
b. Drug Choice i. tPA (alteplase, Genentech 1984)
• Recombinant version of naturally occurring endothelial enzyme
• Highly fibrin specific • ‘Front-load’ 1.5h supplanted old 3h protocol
→ Bolus 15mg → .75 mg/kg over next 30 min → .5 mg/kg over subsequent 60 minutes → Max of 100mg
• Circulating half-life of 5 minutes • Always coadminister IV heparin
ii. rPA (reteplase, Boeringer 1996) • Mutant recombinant tPA • Less fibrin-specific
→ Faster → Diffuses through entire clot
• Less bleeding • Easier administration
→ ‘Double bolus’ of 10 Units, 30 minutes apart • Only inferior to tPA in presentation > 4h
iii. TNKase (tenecteplase, Genentech 2000) • Third-generation mutant (2000) • Longer half life: single 30-50mg bolus • Extremely fibrin-specific (14x tPA) • Outcomes ≥ tPA
iv. No longer commonly used for ACS • Streptokinase
→ Antigenic; allergic reaction common with recent strep infection
→ Inferior outcome data compared to tPA products • Urokinase • APSAC
c. Indications: STEMI with EKG showing i. STE ≥ 1mm in ≥ 2 contiguous standard limb leads OR ii. STE ≥ 2mm in ≥ 2 contiguous precordial leads

Notes
Acute Coronary Syndromes Page 13
OR iii. (presumed) New LBBB
• Left bundle outcomes worse • Treated less frequently • Concern for lytic side effects in face of uncertain Dx
d. Absolute contraindications i. Active internal bleeding ii. CVA history
• Previous hemorrhagic CVA • Ischemic CVA < 1y ago
iii. Known intracranial mass • Neoplasm • AVM • Aneurysm
iv. Suspected • Aortic dissection • Suspected pericarditis
e. Relative contraindications i. HTN
• Acutely > 180/100 • Chronically uncontrolled
ii. Old CVA due to intracranial pathology iii. INR > 3 iv. Known bleeding diathesis v. Trauma < 2 wks vi. CPR > 10 min vii. Major surgery < 3 wks viii. Noncompressible vascular puncture ix. Internal bleed < 4 wks x. Pregnancy xi. Active PUD
f. Complications i. Bleeding ii. Allergy (streptokinase)
2. PCI / PTCA a. Background
i. Mechanical revascularization ii. Balloon expansion of arterial lumen iii. Greater dilatation gives
• Less restenosis • More complications: dissection, thrombus, rupture
iv. Often leave fenestrated stent as scaffold b. Has become industry standard
i. Primary PTCA: outcomes better than lytics, IF • Performed within time window (90-120 min)

Notes
Acute Coronary Syndromes Page 14
• Performed by experienced operator ii. Need to have staffing / backup iii. Less bleeding complications iv. Hard indication for cardiogenic shock
3. Combinations a. Rescue angioplasty
i. Diagnostic: check flow after lytics (rarely used) ii. Therapeutic: mechanically dilate artery if not resolved
after lytics b. Facilitated PCI
i. Half-dose front-load tPA or other lytic followed by cath ii. Used if PCI imminent, but expecting delay past 90 min iii. Shown to be both safe and effective
4. Emergent CABG a. Last resort b. Failed PCI with continued symptoms / instability
C. Anticoagulants / Antiplatelets
1. Aspirin a. Features
i. Potent irreversible antiplatelet ii. Cheap iii. Extremely effective
• Alone decreases mortality 23% • Synergizes with lytics (42% mortality reduction)
b. Dosages i. 160mg - 325mg ii. Chewed preferable (faster onset)
c. Contraindications i. Acute GI bleed ii. Allergy to ASA (use Plavix)
2. Plavix (clopidogrel) a. Inhibits GP IIb/IIIa transformation to high-affinity state b. Routine ED use not proven c. Credible antiplatelet backup in ASA allergy (300mg load)
3. GPIIb/IIIa inhibitors a. Mechanism
i. Inhibits receptor on surface of platelet ii. Prevents crosslinking of fibrinogen / vWf iii. Therefore decreases platelet adhesion
b. Drug choices i. Eptifibatide (Integrillin) ii. Tirofiban (Aggrastat) iii. Abciximab (try saying several times in a row) (ReoPro)
c. Indications

Notes
Acute Coronary Syndromes Page 15
i. Improves outcome if PCI performed ii. Some centers using routinely for all MI
4. Heparins a. Mechanism
i. Binds antithrombin III, eventually preventing fibrin formation
ii. Stops new clot formation • Keeps newly revascularized arteries patent (a
necessity when using lytics) • Prevents mural thrombus formation in anterior MI • Prevents formation and dissemination of clots to CNS • Does nothing to break up existing clot • Indicated in UA and MI
b. Unfractionated heparin i. Load at 60 U/kg, infuse at 12 U/kg/hr ii. Max of 5000 U bolus / 1000 U/hr iii. Goal of PTT 1.5 to 2.5 times control
c. Low molecular weight heparins i. Inactivates factor Xa ii. Equal or greater efficacy to UFH
• Not all LMWH are the same • Literature supports Lovenox (enoxaparin) over others
iii. Easier to administer, less frequent checks, fewer complications: overall cheaper
iv. Indicated in UA, used often. v. Not routinely used in AMI: many interventionalists loath
subsequent cath (long half-life, unclear reversal characteristics)
D. Maximize oxygen delivery / minimize oxygen consumption
1. Nitrates: nitroglycerin a. Decrease preload and dilate coronary vasculature
i. Contraindicated in hypotension below 90mm syst ii. Seriously consider holding in inferior/RV infarct, as
decreasing preload may induce severe hypotension b. Historically shows some mortality benefit in AMI c. Three SL’s followed by IV
i. Start at 10 ug/min ii. Titrate until pain free, max 200
2. Beta adrenergic blockade a. Decrease myocardial oxygen demand
i. Decrease catechol-induced tachycardia ii. Decrease contractility
b. Contraindications i. Severe COPD / asthma

Notes
Acute Coronary Syndromes Page 16
ii. CHF iii. Bradycardia / AV nodal blockade iv. Hypotension v. Contraindications may explain why this proven
therapy is often not given in clinical situations c. Any β-Blocker will do
i. Most commonly metoprolol 5mg IV ii. Esmolol gtt is ultra-short acting, consider in presence of
contraindications 3. Opioid analgesia
a. Theoretically decreased myocardial O2 consumption by decreasing pain and anxiety
b. Some vasodilatory effects c. Never proven in trials d. Why not?
4. Oxygen a. Goal is to maximize O2 delivery b. Attempt to maximize PaO2
E. Treat complications 1. Antiarrhythmics: routine administration not indicated 2. Pressors
a. Begin with fluids, especially in RV infarct syndromes b. Each vasoactive has its indications and side effects c. Norepinephrine
i. Increases SVR ii. Indicated in hypotension below 80mm systolic iii. Increased myocardial O2 demand iv. Switch to dopamine when you hit 80
d. Dopamine i. Vasoactive of choice above 80mm systolic ii. Increases HR, but overall best profile of the vasoactives in
face of MI e. Dobutamine
i. Can consider coadministration with DA above 90mm systolic to decrease amount of DA needed
ii. Dilates coronary vasculature iii. Less myocardial O2 demand than others
3. Mechanical intervention a. Endotracheal intubation b. Intraaortic balloon pump
i. Used in refractory cardiogenic shock ii. Inflates in diastole, deflates for systole iii. Vacuum assists LV iv. Overall improves CO and EF, increases coronary
perfusion pressure, and decreases myocardial O2 demand

Notes
Acute Coronary Syndromes Page 17
ACUTE CORONARY SYNDROMES
PEARLS
1. ACS is common, and the cause of large amounts of morbidity,
mortality, and litigation. 2. UA is any change in symptoms from that patient’s previous baseline. 3. Acute MI is now defined mainly by an increase in serum troponin. 4. Incompletely occlusive white thrombus is thought to cause UA,
completely occlusive red thrombus is thought to case AMI. 5. Typical anginal symptoms include exertional squeezing/choking and shortness of breath. 6. ‘Atypical’ anginal equivalents are extremely common, especially in
the old and diabetic. 7. Prior stress / cath results are of limited use in ‘ruling out’ ACS in the
ED. 8. EKG is the foremost risk-stratification and diagnostic tool for ACS, but
alone cannot ‘rule out’ MI/UA. 9. Consider concordance and the Sgarbossa criteria in evaluation for
ischemia in the face of LBBB or paced rhythm. 10. Cardiac enzymes are the standard for ruling-in MI, but one set never
rules it out. 11. The goal for reperfusion of AMI is 90 minutes, whether by balloon or
chemical. 12. Don’t forget ASA, heparin, and β-blocker unless they are
contraindicated—all have a significant mortality benefit in AMI.


Notes
Acute Coronary Syndromes Page 19
REFERENCES 1. The Global Use of Strategies to Open Occluded Coronary Arteris
(GUSTO IIb) Investigators. A Clinical Trial Comparing Primary Coronary Angioplasty with Tissue Plasminogen Activator for Acute Myocardial infarction. N Engl J Med 1997;336:1621-8.
2. Zalenski R J, MA, MD, McCarren, Madeline, PhD et al. An Evaluation
of Chest Pain Diagnostic Protocol to Exclude Acute Cardiac Ischemia in the Emergency Department. Arch Intern Med Vol 1997;157:1085-1091.
3. Antman E M, MD, Grudzien Christine MS, MT, et al. Detection of
Unsuspected Myocardial Necrosis by Rapid Bedside Assay for Cardiac Troponin T. Am Heart J 1997;133:596-8.
4. Collins Rory, MB, BS, Peto Richard, FRS, et al. Aspirin, Heparin and
Fibrinolytic Therapy in Suspected Acute Myocardial Infarction. N Engl J Med 1997:336 847-860.
5. Tatum James L, MD, Jesse Robert L, MD, PhD, et al. Comprehensive
Strategy for the Evaluation and Triage of the Chest Pain Patient. Annals of EM 1997;29:116-125.
6. Zalenski R J, Rydman R J, et al. Feasibility of a Rapid Diagnostic
Protocol for an Emergency Department Chest Pain Unit. Annals of EM 1997;29:99-108.
7. Tintinalli, J E, MD, MS. Emergency Medicine, A Comprehensive Study
Guide 6th Edition. Mc Graw Hill 2004. Pp.343-351. 8. Myocardial Infarction Triage and Intervention Investigators (MITI). A
Comparison of Thrombolytic Therapy with Primary Coronary Angioplasty for Acute Myocardial Infarction. N Engl J Med 1996;335:1253-60.
9. GUSTO IIa Investigators. Cardiac Troponin T Levels for Risk
Stratification in Acute Myocardial Ischemia. N Engl J Med 1996;335:1333-41.
10. Sullivan Daniel J., MD, JD, FACEP, Zalenski Robert, MD.
Thrombolysis: Evolving Standards of Care. ED Legal Letter 1996;7\7. 11. Sullivan Daniel J., MD, JD, FACEP and Zalenski Robert, MD. Missed Myocardial Infarction: Minimizing the Risk. ED Legal Letter 1996;7\6.

Notes
Acute Coronary Syndromes Page 20
12. Howel John M., MD, FACEP. Acute Myocardial Infarction and Congestive Heart Failure. EM Clinics of NA 1996:14;83-91.
13. Mair Johannes, MD, Smidt Jorn, MD, et al. A Decision Tree for the
Early Diagnosis of Acute Myocardial Infarction in Nontraumatic Chest Pain Patients at Hospital Admission. CHEST 1995;108:1502-09.
14. McLaughlin Mary Ann, MD, Fuster Valentin, MD, PhD. The Three
Mechanisms for Coronary Artery Disease Progression. The Mount Sinai J of Med 1995;62:165-274.
15. Antman Elliot M, MD, Grudzien Christine, MS, MD, Sacks David B,
MB, ChB. Evaluation of a Rapid Bedside Assay for Detection of Serum Cardiac Troponin T. JAMA 1995;273:1279-1282.
16. International Society and Federation of Cardiology and World Health
Organization Task Force on Myocardial Reperfusion. Reperfusion in Acute Myocardial Infarction. Circulation 1994;90:2091-2102.
17. Tucker John F, MD, Collins Richard A, MD, et al. Value of Serial
Myoglobin Levels in Early Diagnosis of Patients Admitted for Acute Myocardial Infarction. Annals of EM 1994;24:704-708.
18. The GUSTO Investigators. An International Randomized Trial
Comparing Four Thrombolytic Strategies for Acute Myocardial Infarction. N Engl J Med 1993;329:673-82.
19. The Primary Angioplasty in Myocardial Infarction Study Group
(PAMI). A Comparison of Immediate Angioplasty with Thrombolytic Therapy for Acute Myocardial Infarction. N Engl J Med 1993;328:673.
20. Marx, J. Rosen’s Emergency Medicine Concepts and Clinical Practice
Vol II. 5h Edition. Mosby Year Book Inc. 2002; pps1011-10522. 21. Hamm Christian W, MD, et al. Emergency Room Triage of Pateitnets
with Acute Chest Pain by Means of Rapid Testing for Cardiac Troponin T or Troponin I. N Engl J Med 1997;337:1648-53.
22. The Third International Study of Infarct Survival (ISIS3) Collaborative
Group. ISIS-3: A Randomised Comparison of Streptokinase vs Tissue Plasminogen Activator vs Anistreplase and of Aspirin plus Heparin vs Aspirin alone among 41,299 cases of Suspected Acute Myocardial Infarction. Lancet 1992;339:753-70.
23. Gene Kenneth MD, Anderson Vernon, MD. Thrombolytic Therapy in
Acute MI. Postgraduate Medicine 1990;88:79-93.

Notes
Acute Coronary Syndromes Page 21
24. Gruppo Italiano Per Lo Studio Della Sopravvivenza Nell=Infarto
Miocardico (GISSI). GISSI-2: A Factorial Randomised Trial of Alteplase vs Streptokinase and Heparin vs no Heparin among 12,490 patients with Acute Myocardial Infarction. Lancet 1990;336:65-71.
25. The TIMI Study Group. Comparison of Invasive and Conservative
Strategies after Treatment with Intravenous Tissue Plasminogen Activator in Acute Myocardial Infarction. N Engl J Med 1989;320:618-27.
26. Second International Study of Infarct Survival(ISIS-2) Collaborative
Group. Randomised Trial of IV Streptokinase, Oral Aspirin, Both or Neither among 17,187 cases of Suspected Acute Myocardial Infarction. Lancet 1988; 349-360.
27. The TIMI Investigators. Thrombolysis in Myocardial Infarction:
Comparative Studies of Coronary Reperfusion and Systemic Fibrinogenolysis with two forms of Recombinant Tissue-Type Plasminogen Activator. J Am Coll Cardiol 1987;10:479-90.
28. GISSI. Effectiveness of IV Thrombolytic Treatment in Acute
Myocardial Infarction. The Lancet 1986;397-410. 29. Special Report: The TIMI Trial. Phase I Findings N Engl J Med
1985:932-936. 30. Abdulla AM, MD, Watkins LA, MD, MPH, FRCP. Bedside Evaluation
in Cardiac Emergencies. Postgraduate Medicine 1984;75:203-210. 31. Dadkhah S, Fisch C, Zonia C. Accelerated coronary reperfusion through the use of rapid bedside cardiac markers. Angiology Jan 1999: 50(1)55-62. 32. Cannon C, Gibson C, Lambrew C, et al. Relationship of symptom- onset-to-balloon time and door-to-balloon time with mortality in patients undergoing angioplasty for acute myocardial infarction. JAMA June 2000: 283(22)2941-2989. 33. Cannon C, et al. TNK-tissue plasminogen activator in acute myocardial infarction. Circualtion Jan 1997: 95(2)351-356. 34. ASSENT Investigators. Single-bolus tenecteplase compared with front- loaded alteplase in acute myocardial infarction: the ASSENT-2 double- blind randomised trial. Lancet Aug 1999: 354(9180)716-722.

Notes
Acute Coronary Syndromes Page 22
35. Vorchheimer D, Badimon J, Fuster V. Platelet glycoprotein IIb/IIIa receptor antagonists in cardiovascular disease. JAMA April 1999:281(15)1407-1414. 36. Lincoff A, et al. Management of patients with acute coronary syndromes in the United States by platelet glycoprotein IIb/IIIa inhibition. Circulation Mar 2000: (102)1093-1100. 37. Cohen M, et al. A comparison of low-molecular-weight heparin with unfractionated heparin for unstable coronary artery disease. N Eng J Med Aug 1997(337)447-452. 38. Ewy G, Ornato J. 31st Bethesda Conference. Emergency Cardiac Care. J Am Coll Cardiol Mar 2000: 35(4)825-880. 39. Young J, et al. Superiority of “triple” drug therapy in heart failure: insights from the PROVED and RADIANCE trials. J Amer Coll Cardiol Sep 1998: 32(3)686-692. 40. Joseph J, Taylor D. Beta-blockade in chronic heart failure: science and practice. Res & Staff Phys Mar 2000: 46(3)11-14, 57-61. 41. Califf R, O’Connor C. Beta-blocker therapy for heart failure. JAMA Mar 2000: 283(10)1335-1337. 42. Antman et al., Management of Patients With STEMI: Executive
Summary. J Am Coll Cardiol 2004;44:671-719. 43. Braunwald E, Antman EM, Beasley JW, Califf RM, Cheitlin MD,
Hochman JS, Jones RH, Kereiakes D, Kupersmith J, Levin TN, Pepine CJ, Schaeffer JW, Smith EE III, Steward DE, Théroux P. ACC/AHA 2002 guideline update for the management of patients with unstable angina and non–ST-segment elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines.
44. Fesmire, F., et al. The Erlanger Chest Pain Evaluation Protocol: A One-
Year Experience With Serial 12-Lead ECG Monitoring, Two-Hour Delta Serum Marker Measurements, and Selective Nuclear Stress Testing to Identify and Exclude Acute Coronary Syndromes. Ann Emerg Med. 2002;40:584-594.
8/10