
Acute Coronary Syndromes Disclosures · NSTEMI STEMI ~90% 100% Constant pain NSTEMI vs STEMI...
28
Jon Tardiff, BS, PA-C OHSU Clinical Assistant Professor Acute Coronary Syndromes Disclosures • I work for Virginia Garcia Memorial Health Center, Beaverton, OR. • And I am a medical editor for Jones & Bartlett Publishing. Arabic, Somali, Mai Mai, Pashtu, Urdu, ASL, and more! 4 Goals of this session • Identify Acute Coronary Syndromes (STEMI vs NSTEMI) • Identify old myocardial infarction • Distinguish between Right and Left BBB
Transcript of Acute Coronary Syndromes Disclosures · NSTEMI STEMI ~90% 100% Constant pain NSTEMI vs STEMI...
Jon Tardiff, BS, PA-C�OHSU Clinical Assistant Professor�
Acute Coronary Syndromes� Disclosures�
• I work for Virginia Garcia� Memorial Health Center,� Beaverton, OR.�
• And I am a medical editor for Jones & Bartlett Publishing.�
Arabic, Somali, Mai Mai, Pashtu, Urdu, ASL, and more!�4�
Goals of this session�
• Identify Acute Coronary Syndromes �
(STEMI vs NSTEMI)�
• Identify old myocardial infarction�
• Distinguish between Right and Left BBB�

What a 12-Lead ECG can help you do�
• Diagnose ACS / AMI�• Interpret arrhythmias�• Identify life-threatening syndromes (WPW,
LGL, Long QT synd., Wellens synd., etc)�• Infer electrolyte imbalances�• Infer hypertrophy of any chamber�• Infer COPD, pericarditis, drug effects, and
more!�6�6666666666666666666666666666666666666666666666666666666666666666666666666666666666666666666
For example:�73 y.o. male with nausea, syncope�
7�777777777777777777777777777777777777777777777777777777777777777777777777777777777777777777777
Acute Inferior MI�
ST elevation�
8�88888888888888888888888888888888
What rhythm? (look at V1 for P waves)�

9�9999999999999999999999999999999
P waves� Limitations of a 12-Lead ECG�
• Truly useful only ~40% of the time�• Each ECG is only a 10 sec. snapshot�• Serial ECGs are necessary, especially for ACS�• Other labs help corroborate ECG findings
(cardiac markers, Cx X-ray)�• Confounders must be ruled out (LBBB, LVH,
WPW, digoxin, RVH, pericarditis, dissecting aneurysm)�
11�1111111111111111111111111111111111111111111111
Confounder: Left Bundle Branch Block�
12�1212121111112121212121111121112112212111211112111111111111111121111121111111
Impending AMI with normal ECG!�

13�1313131313131313131331313111311313111111131313131313131111113131313333333333333333333333333333313
13 hrs later — Acute Anterior MI�
Elevated ST segments�
14�
ECG Lead Placement�&�
Electrophysiology Review�
15�
� I � II � III
Limb Leads�
(standard leads)
-� ±�
+� 16�
Rapid Interpretation Tips�
1616116161161616161616161116666161666666666666
RRaapid Interpreettatttttiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiioooooooooooooooooooooooooooooooooooooooooooooooonnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnn TTTiipss
Dr. Willem Einthoven�

17�
Leads I, II, III�
I
II III
Normal 12-Lead ECG�
SA Node AV Node His Bundle BBs Purkinje Fibers�
P�
Q�
R�
S�
T�
II�
U�
Conduction System�
20�Q�
R�
S�
P wave axis�
R wave axis�
…upright in L II�
…upright in L II�
Lead II�

21�21�
PR�
II�
Intervals�
PR Interval: 120 – 200 mSec (3 – 5 boxes) �QRS width: 60 – 120 mSec (1 ½ – 3 boxes) �QT/QTc interval: 400 mSec (10 boxes)�
QT�QRS�
22�
� I � II � III � aVR � aVL � aVF
Limb (frontal plane) Leads�
(augmented leads)
(standard leads)
23�
Augmented Leads�
aVR
aVL
aVF
Normal 12-Lead ECG�

25�
6 Frontal Plane Leads (limb leads)�
I
II III
R
L
F
Axis�
26�
Leads � I� II� III� aVR*� aVL� aVF�
-�
27�
QRS Morphology in Lead II�
II�
Axis Determination�

29�
Why We Care About Axis Deviations�
The axis shifts towards hypertrophy�& away from infarction�
The axis also shifts for ectopic rhythms, such as V-Tach�
Normal axis is -20° to +110°�
30�
Axis Deviation�
Horizontal heart (0°): obesity, � 3rd trimester pregnancy. Ascites�
Vertical heart (90°): slender build�
Left Axis Deviation: LBBB,� Anterior MI, Inferior MI, Left� anterior hemiblock, LVH�
Right Axis Deviation: Anterior MI,� Lateral MI, RBBB, COPD, RVH,� Left posterior hemiblock�
Extreme RAD: Ectopic rhythm� (VT), MI�
31�
How to determine Axis�
Easiest: the computer does it for you!�
Pretty Easy: Thumbs up / Thumbs down�
A Little Harder: find the tallest R wave � (if tallest is Lead II = normal axis)�
32�
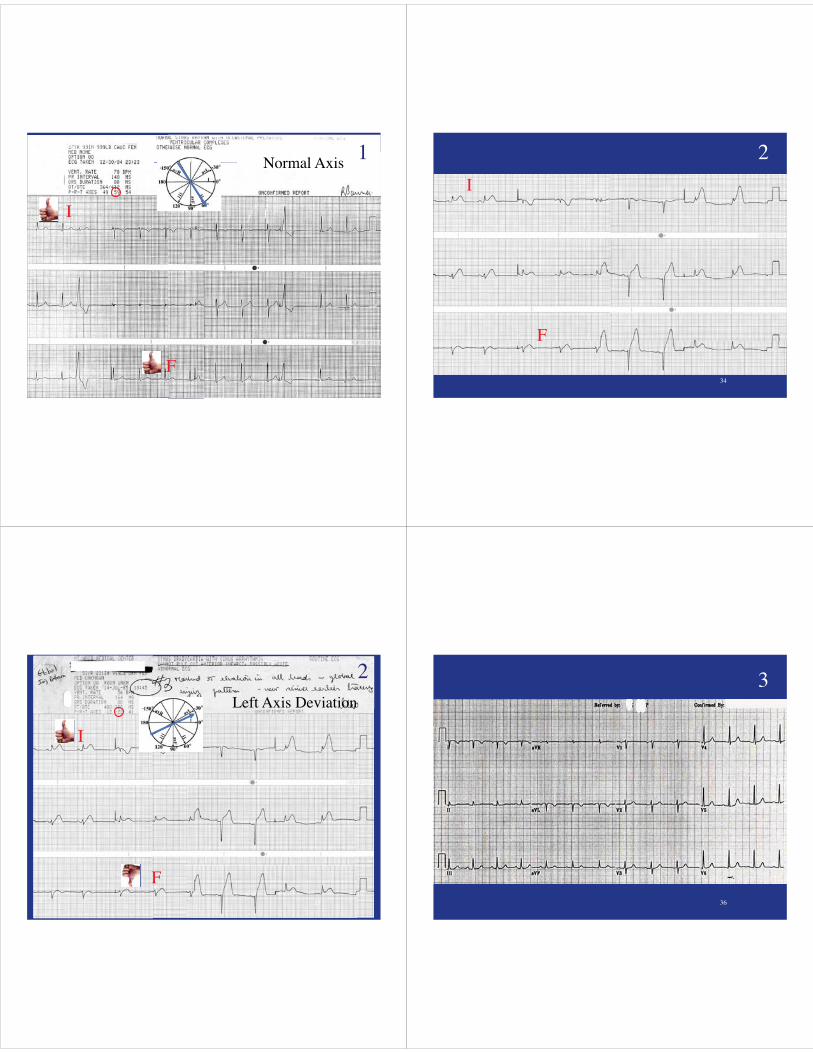
Practice: Axis� 1�
I�
F�
33�
Axis Practice� 1�
333333333333333333333333333333333333333333333333333333333333333333333333333333333333333333333333333333333333333333333333333333333333333333333333333333333333333333333333333333333333333333333333333333333333333333
Normal Axis�
I�
F�
1�
34�
2�
I�
F�
35�
2�Left Axis Deviation�
I�
F�36�
3�
37�
3�
37373737377777737373777377777777777777777737777373777377737373377737773333333333377773333333333733333377777333373737333333333333373333
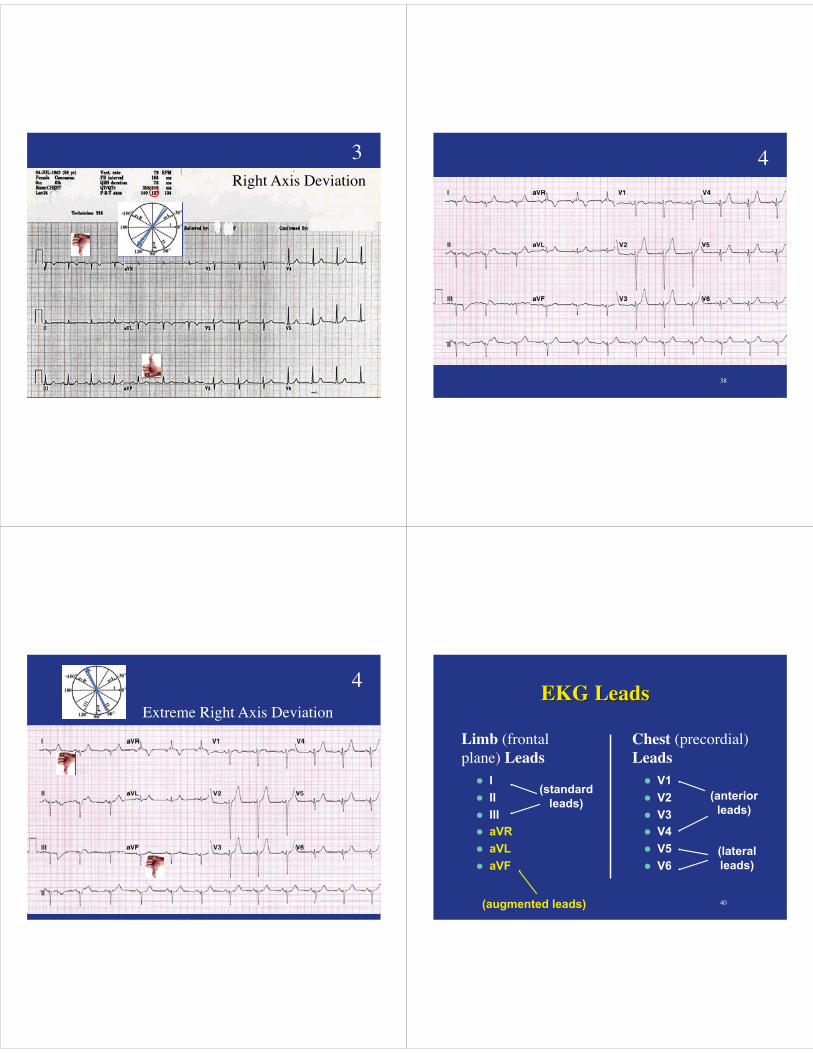
Right Axis Deviation�
38�
4�
39�393933939939333333933333333939993933339999393993333393333333333333333933333333
4�
Extreme Right Axis Deviation�
40�
� I � II � III � aVR � aVL � aVF
� V1 � V2 � V3 � V4 � V5 � V6
Limb (frontal plane) Leads�
(augmented leads)
(standard leads) (anterior
leads)
(lateral leads)
Chest (precordial) Leads�

41�
V Lead Cutaway�
V Lead Progression�
Normal 12-Lead ECG�

45�45 46�
Step-by-step method for reading a 12-Lead�
Rapid Interpretation Tips�
Rapid Interpretation Tips�• Identify the rhythm. If supraventricular*, �
If no LBBB,�
�If present, �
• Rule out other confounders: WPW, pericarditis, LVH, digoxin effect�
• Identify location of infarct, and consider appropriate treatments: MONA, PCI [or fibrinolytic], nitrate infusion, heparin infusion, GP IIb, IIIa inhibitor, beta-blocker, clopidogrel, statin, etc. �
Supraventricular rhythms�
• Sinus rhythm�
• Atrial fibrillation�
• Junctional rhythm�
• PSVT�
• Atrial tachycardia�
• Atrial flutter�
• Wandering atrial pacemaker�
• Multifocal Atrial Tachycardia�

Normal 12-Lead ECG�Rapid Interpretation Tips�
Rapid Interpretation Tips�• Identify the rhythm. If supraventricular, �
If no LBBB,�
�If present, �
• Rule out other confounders: WPW, pericarditis, LVH, digoxin effect�
• Identify location of infarct, and consider appropriate treatments: MONA, PCI [or fibrinolytic], nitrate infusion, heparin infusion, GP IIb, IIIa inhibitor, beta-blocker, clopidogrel, statin, etc. �
The Problem with Bundle Branch Blocks�
• Dyssynchronized contraction of the ventricles�• Reduced cardiac output�• Worsened heart failure�• LBBB confounds the EKG interpretation� —LBBB makes it harder to find ACS�
52�
Bundle Branch Blocks (QRS > 0.12 sec.)
Left BBB (L I, V5, V6: upright QRS with a notch)
Right BBB (V1, V2, MCL1: rsR’ pattern)
R’
S
r
notch I V1
(left-sided lead) (right-sided lead)

53�
Bundle Branch Blocks Two QRSs
5353553535353535535355555553535553353553553535553335
notch I
Healthy ventricle�
Blocked bundle�
R’
S
r V1 slur I
V1 & V2�
RBBB�
V5 V6�
(& I, aVL)�
LBBB�
56�
Practice: Bundle Branch Block�

RBBB�
Which Bundle Branch is Blocked?� 5�
RBBB�
Right Bundle Branch Block (Lead V1)� 5�
LBBB 12-Lead�
Which Bundle Branch is Blocked?� 6�LBBB 12-Lead�Left Bundle Branch Block�
(L I, V5, V6)�
6�

Where is the Pathology?� Right Bundle Branch Block�
63�
64�
Left Bundle Branch Block�

65�
New 12-Lead ECG Format�
aVL�
I�
-aVR�
II�
aVF�
III�
New 12-Lead ECG Format�
aVL�
I�
-aVR�
II�
aVF�
III�
New �
Old�
Rapid Interpretation Tips�
Rapid Interpretation Tips�• Identify the rhythm. If supraventricular, �
• Rule out left bundle branch block. If no LBBB,�
• Check for: ST elevation, or ST depression with T wave inversion, and/or pathologic Q waves. �
�If present, �
• Rule out other confounders: WPW, pericarditis, LVH, digoxin effect�
• Identify location of infarct, and consider appropriate treatments: MONA, PCI [or fibrinolytic], nitrate infusion, heparin infusion, GP IIb, IIIa inhibitor, beta-blocker, clopidogrel, statin, etc. �
Ischemia� Injury� Infarction�Normal�
STEMI�
ST elevation, ST depression, T wave inversion, pathologic Q waves�
NSTEMI?�

Percutaneous Coronary Intervention�
71�
RCA before and after stenting�
Before stenting� After stenting�
The Spectrum of Acute Coronary Syndromes�
Healthy� CAD� Angina� Unstable Angina� NSTEMI� STEMI� Shock /� Death�
Patent�artery�
~50%� ~70%� >70%� or 100%� ~90%� 100%� 100%�(or vasospasm)�
No symptoms� Pain on� exertion�
Pain at rest;�relieved by NTG� Constant pain�

NSTEMI� STEMI�
~90%�100%�
Constant pain�
NSTEMI vs STEMI�
Constant pain�
STEMI: ECG Changes�A. Normal ECG�B. Hyperacute T wave changes - increased T wave amplitude and width; may also see ST elevation�C. Marked ST elevation with hyperacute T wave changes (transmural injury)�D. Pathologic Q waves, less ST elevation, terminal T wave inversion (necrosis)�E. Pathologic Q waves, T wave inversion (necrosis and fibrosis) �F. Pathologic Q waves, loss of R waves (fibrosis)�
(w/onset cx pn)�
(20 minutes)� (1 hour)�
(1 week – years)�(>1 hr)�
(normal)�
75�
Why Pathologic Q Waves Form�
Normal q� Pathologic Q�
MI ECG Patterns�MMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIII EEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEEECCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCCGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGGG PPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaattttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttttteeeeeeeeeeeeeeeeeeeeeeeeeeeeerrrrrrrrrrrnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnssssssssssssssssssssssssssssssssssssssssssssssssssssssss
NSTEMI�(non Q wave MI)�

77�
STEMI — Typical Progression� Acute Inferior MI#1�
Acute Inferior MI�
ST elevation�
Qs� Qs�
Axis is shifting leftward…�
Acute Inferior MI #2�
Same Patient~2 hrs later�
Worsened ST elevation�
Qs� Qs�
New ST elevation�
Acute Inferior MI #3�Same Patient 9 days later�
Permanent Q waves�(inferior wall scar)�
But NO anterior infarct (no Qs)�
Permanent left axis deviation�

Acute Anterior MI Page�AAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAccccccccccccccccccccccccccccccccccccccccccccccuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuuutttteeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeee AAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnnttttttttttttttttttttttttttttttttteeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeerrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrriiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiioooooooooooooooooooooorrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrrr MMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMIIIIIIIIIIIIIIIIIIIIIIIIIIIIIIII PPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaggggggggggggggggggggggggggggggggggggggggggggggggggggggeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeeee
45% of MIs�
Acute Inferior MI Page�AAAAAAAAAAAAAAAAAAAAAAAAAAAAcccccccccccccuuuuuuuuuuuuuuteeeeeeeeeeeeeeeee IIIIIIIIIIIIIIIIIIInnnnnnnnnnnnnnnnnnfffffffffffffffffffffffffffffffffffffffffffffffffffffffffffffeeeeeeeeeeeeeerrrrrrrrrrrrrrrrrriiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiooorrrrrrrrrrrrrrrrrrrrrr MMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMIIIIIIIIIIIIIIIIIIIIIII PPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPaaaaaaaaaaggggggggggggggggggggggggggggeee
40% of MIs�
Acute R Ventricle MI Page�AAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAcccccccccccccccccccccccccccuuuuuuuuuutttttttttttttttttttttttttteeeeeee RRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRRR VVVVVVVVVVVVVVVVVVVVVVVVVVVVVVVVVVVVVVVVVVVVVVVVVVVVVVVVVVVVVVVVVVVVVVVVeeeeeeeeeeeeeeennnnnnnnnntrrrrrrriiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiiccccccccccccccccccccccccccccccclllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllllleeeeeeee MMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMIIIIIIIIIIIIIIIIIIIIIIIIIIII PPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPaaaaaaaaaaaaaaaaaaaaaaaaaaaaaaggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggggeeeeeeeeeeeeeeee
1/3 of Inferior MIs�
Acute Lateral MI Page�AAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAcutttttttttttttttttttttttttttte LLLLLLLLLLLLLLLLLLLLLLLLLLLLatttttttttttttterallllllllllllllllllllllllllllllllllll MMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMI PPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPaggggggggggggggggggggggggggggggggggggggggggeeeeeeeeeeeeeeeee
15% of MIs�
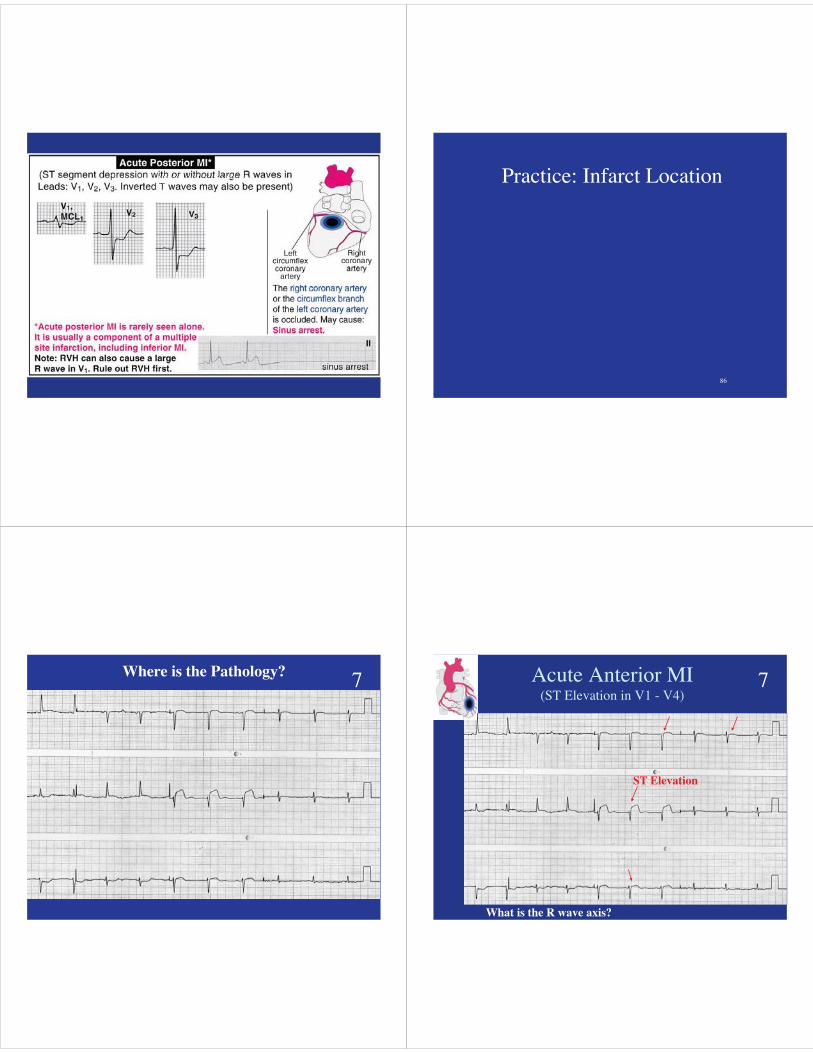
Acute Posterior MI Page�AAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAAcccccuuuuuuutttttttttttttttttttteeeeeee PPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPooooooossssssssssttttttttttttttteeeeeerrrrrrrrrrrrrriiiiiiiiiiiiiiiiiiiiooooooooooooooooorrrrrrrrrr MMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMMIIIIIIIIIIIIIIIII PPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPPaaaaaaaaaaaaggggggggggggggggggggggeeeeee
86�
Practice: Infarct Location�
Acute Anterior MI�
Where is the Pathology?� 7� Acute Anterior MI�(ST Elevation in V1 - V4)�
ST Elevation�
What is the R wave axis?�
7�

Acute Inferior MI�
Where is the Pathology?� 8�Acute Inferior MI�
Acute Inferior MI�(ST elevation in II, III, F)�
8�
Acute Inferolateral MI�
Where is the Pathology?� 9�Acute Inferolateral MI�Acute Inferolateral MI �
(ST elevation in II, III, F, V5, V6)�
Note the axis has not shifted and there are no loss of R waves yet, because it is early in the AMI,. �
9�
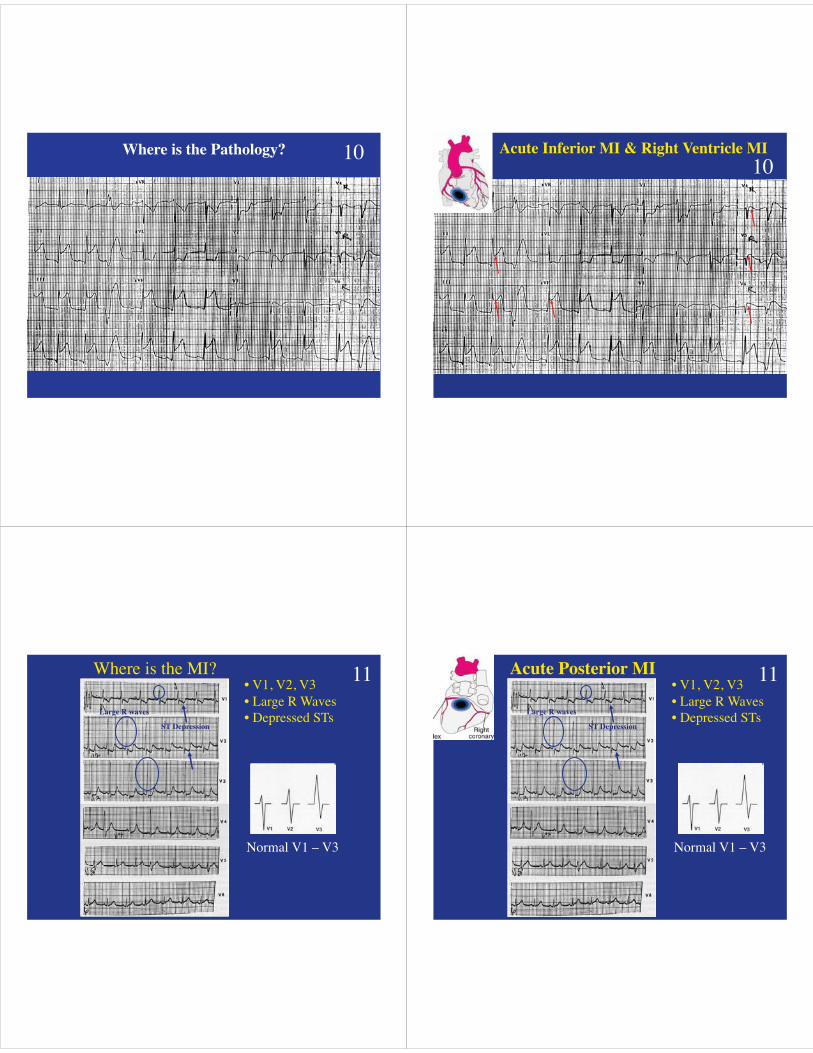
Where is the Pathology?� 10� Acute Inferior MI & Right Ventricle MI�10�
Where is the MI?�
Normal V1 – V3�
• V1, V2, V3�• Large R Waves�• Depressed STs�
ST Depression�
Large R waves�
11� Acute Posterior MI�
Normal V1 – V3�
• V1, V2, V3�• Large R Waves�• Depressed STs�
ST Depression�
Large R waves�
11�

Where is the Pathology?�
LAE�
LBBB�
LBBB�
Left Bundle Branch Block�
Anterior MI�
MI? What rhythm is this?�
Anterior MI�
Sinus Tach� Acute Anteroseptal MI�
Elevated ST segments�

Rhythm? Pathology?�Acute Inferolateral MI�
Elevated STs II, III, aVF, V5, V6�
MI? Rhythm?�AF? Acute Anterolateral MI�
Hyperacute T waves V3–V6�(early sign of AMI)�
Elevated STs�
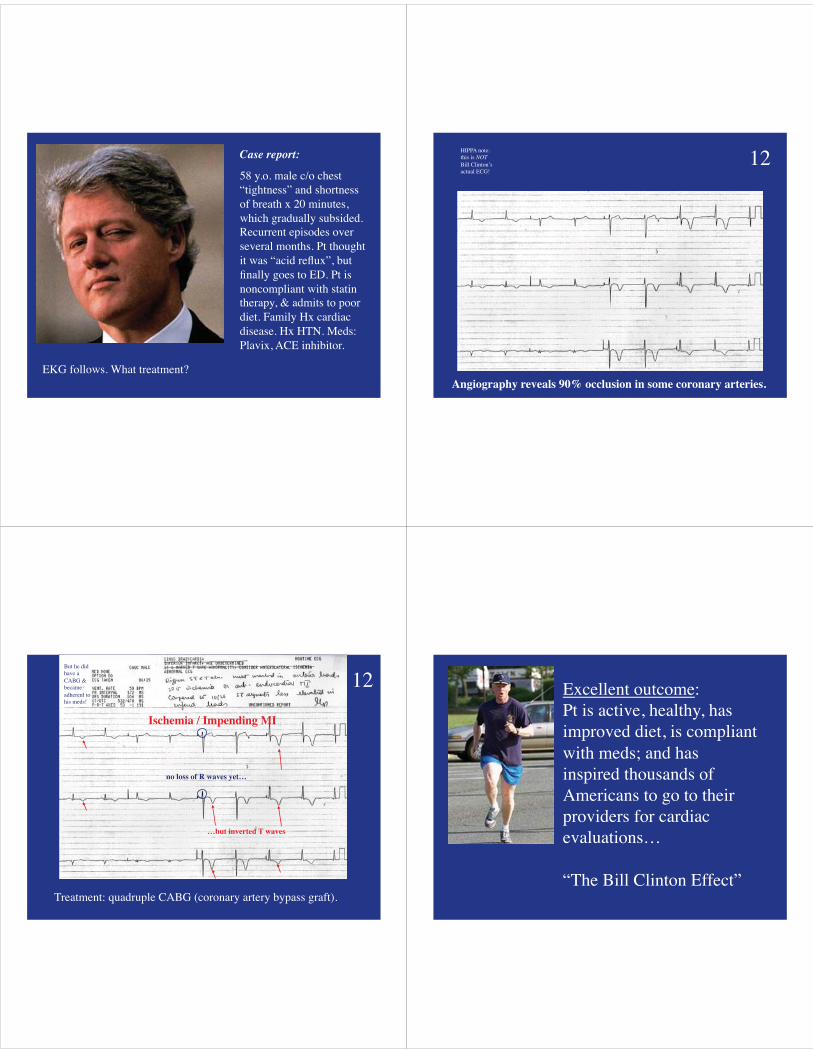
Case report:�
58 y.o. male c/o chest “tightness” and shortness of breath x 20 minutes, which gradually subsided. Recurrent episodes over several months. Pt thought it was “acid reflux”, but finally goes to ED. Pt is noncompliant with statin therapy, & admits to poor diet. Family Hx cardiac disease. Hx HTN. Meds: Plavix, ACE inhibitor. �
EKG follows. What treatment?�Angiography reveals 90% occlusion in some coronary arteries. �
HIPPA note: �this is NOT�Bill Clinton’s�actual ECG!�
12�
Treatment: quadruple CABG (coronary artery bypass graft).�
Ischemia / Impending MI�
no loss of R waves yet…�
…but inverted T waves�
But he did have a CABG & became adherent to his meds!�
12� Excellent outcome:�Pt is active, healthy, has improved diet, is compliant with meds; and has inspired thousands of Americans to go to their providers for cardiac evaluations… �
“The Bill Clinton Effect”�
109�01010101011101010101010101111111110111111011010100010101000100010000999999999999999999999999999999999999999
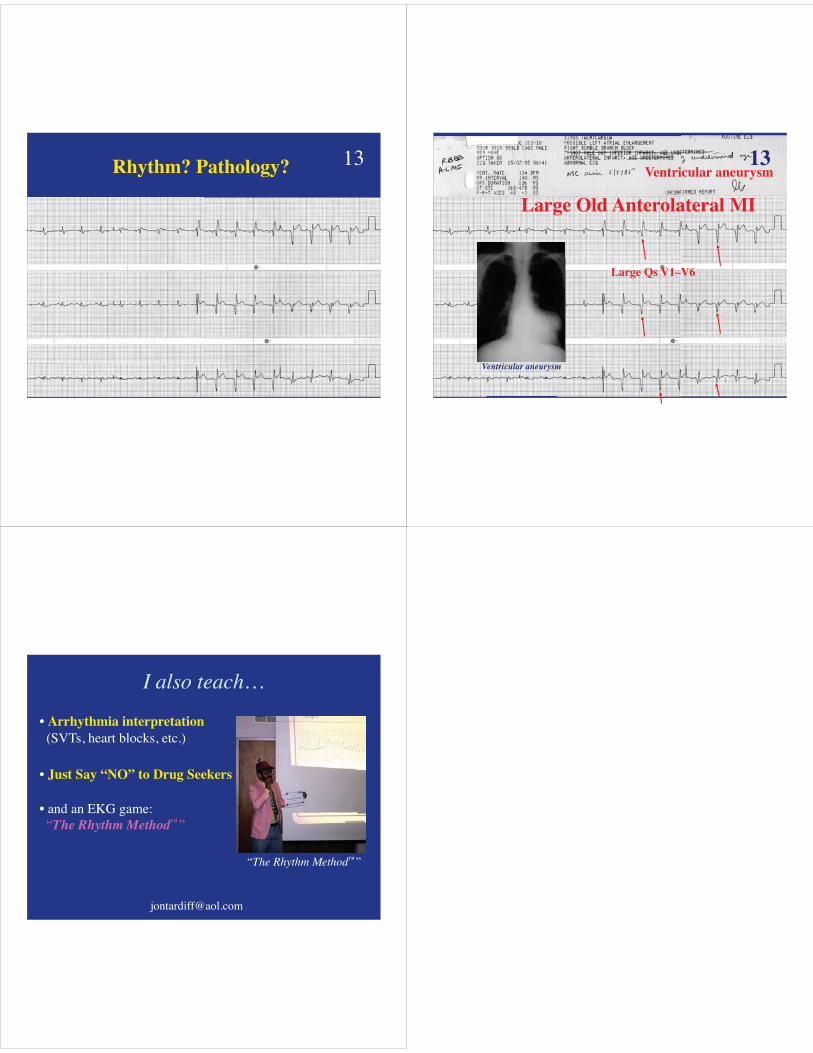
Rhythm? Pathology?� 13�
110�1111111111111111111111111111111111111111111111111111111111111111111111110000000000000000000000000000000000000
Large Old Anterolateral MI�
Large Qs V1–V6�
Ventricular aneurysm�
Ventricular aneurysm�
13�
I also teach…�
• Arrhythmia interpretation� (SVTs, heart blocks, etc.)�
• Just Say “NO” to Drug Seekers�
• and an EKG game:� “The Rhythm Method™”�
“The Rhythm Method™”�


















