
Acute cholecystitis: Pathogenesis, clinical features, and ... · extensive chronic inflammatory...
38
Acute cholecystitis: Pathogenesis, clinical features, and diagnosis Authors Salam F Zakko, MD, FACP Nezam H Afdhal, MD, FRCPI Section Editor Sanjiv Chopra, MD, MACP Deputy Editor Anne C Travis, MD, MSc, FACG, AGAF All topics are updated as new evidence becomes available and our peer review process is complete. Literature review current through: Mar 2015. | This topic last updated: Nov 19, 2013. INTRODUCTION — Acute cholecystitis predominantly occurs as a complication of gallstone disease and typically develops in patients with a history of symptomatic gallstones. In a systematic review, it was seen in 6 to 11 percent of patients with symptomatic gallstones over a median follow-up of 7 to 11 years [ 1 ]. (See"Uncomplicated gallstone disease in adults", section on 'Natural history' .) This topic will review the pathogenesis, clinical manifestations, and diagnosis of acute cholecystitis. The management of uncomplicated gallstone disease, acalculous cholecystitis, and the treatment of acute cholecystitis are discussed separately. (See "Uncomplicated gallstone disease in adults" and "Acalculous cholecystitis" and"Treatment of acute calculous cholecystitis" .) DEFINITIONS — The term cholecystitis refers to inflammation of the gallbladder. It may develop acutely in association with gallstones (acute cholecystitis) or, less often, without gallstones (acalculous cholecystitis). It may also develop over time and be discovered histologically following cholecystectomy (chronic cholecystitis). Acute cholecystitis — Acute cholecystitis refers to a syndrome of right upper quadrant pain, fever, and leukocytosis associated with gallbladder inflammation that is usually related to gallstone disease. Acalculous cholecystitis — Acalculous cholecystitis is clinically identical to acute cholecystitis but is not associated with gallstones and usually occurs in critically ill patients. It accounts for approximately 10 percent of cases of acute cholecystitis and is associated with high morbidity and mortality rates [ 2 ]. (See "Acalculous cholecystitis" .) Chronic cholecystitis — Chronic cholecystitis is the term used to describe chronic inflammatory cell infiltration of the gallbladder seen on histopathology. It is almost invariably associated with the presence of gallstones and is thought to be the result of mechanical irritation or recurrent attacks of acute cholecystitis leading to fibrosis and thickening of the gallbladder [3-5 ]. Its presence does not correlate with symptoms since patients with
Transcript of Acute cholecystitis: Pathogenesis, clinical features, and ... · extensive chronic inflammatory...

Acute cholecystitis: Pathogenesis, clinical features, and diagnosis
Authors
Salam F Zakko, MD, FACP
Nezam H Afdhal, MD, FRCPI
Section Editor
Sanjiv Chopra, MD, MACP
Deputy Editor
Anne C Travis, MD, MSc, FACG, AGAF
All topics are updated as new evidence becomes available and our peer review process is
complete.
Literature review current through: Mar 2015. | This topic last updated: Nov 19, 2013.
INTRODUCTION — Acute cholecystitis predominantly occurs as a complication of gallstone
disease and typically develops in patients with a history of symptomatic gallstones. In a
systematic review, it was seen in 6 to 11 percent of patients with symptomatic gallstones
over a median follow-up of 7 to 11 years [1]. (See"Uncomplicated gallstone disease in
adults", section on 'Natural history'.)
This topic will review the pathogenesis, clinical manifestations, and diagnosis of acute
cholecystitis. The management of uncomplicated gallstone disease, acalculous cholecystitis,
and the treatment of acute cholecystitis are discussed separately. (See "Uncomplicated
gallstone disease in adults" and "Acalculous cholecystitis" and"Treatment of acute calculous
cholecystitis".)
DEFINITIONS — The term cholecystitis refers to inflammation of the gallbladder. It may
develop acutely in association with gallstones (acute cholecystitis) or, less often, without
gallstones (acalculous cholecystitis). It may also develop over time and be discovered
histologically following cholecystectomy (chronic cholecystitis).
Acute cholecystitis — Acute cholecystitis refers to a syndrome of right upper quadrant
pain, fever, and leukocytosis associated with gallbladder inflammation that is usually related
to gallstone disease.
Acalculous cholecystitis — Acalculous cholecystitis is clinically identical to acute
cholecystitis but is not associated with gallstones and usually occurs in critically ill patients. It
accounts for approximately 10 percent of cases of acute cholecystitis and is associated with
high morbidity and mortality rates [2]. (See "Acalculous cholecystitis".)
Chronic cholecystitis — Chronic cholecystitis is the term used to describe chronic
inflammatory cell infiltration of the gallbladder seen on histopathology. It is almost invariably
associated with the presence of gallstones and is thought to be the result of mechanical
irritation or recurrent attacks of acute cholecystitis leading to fibrosis and thickening of the
gallbladder [3-5]. Its presence does not correlate with symptoms since patients with

extensive chronic inflammatory cell inflammation may have only minimal symptoms, and
there is no evidence that chronic cholecystitis increases the risk for future morbidity [6].
Hence, the clinical significance of this entity is questionable. (See "Uncomplicated gallstone
disease in adults".)
Some authors use the phrase "chronic cholecystitis" when referring to gallbladder
dysfunction as a cause of abdominal pain [7]. It is more appropriate in this instance to refer
to the condition based on the disorder present, such as pain due to gallstone disease, pain
due to biliary dyskinesia (which is attributed to sphincter of Oddi dysfunction), or pain due to
functional gallbladder disorder (also called gallbladder dyskinesia). (See "Clinical
manifestations and diagnosis of sphincter of Oddi dysfunction" and "Functional gallbladder
disorder in adults".)
PATHOGENESIS — Acute cholecystitis occurs in the setting of cystic duct obstruction.
However, in contrast to biliary colic, the development of acute cholecystitis is not fully
explained by cystic duct obstruction alone. Studies suggest that an additional irritant
(possibly lysolecithin) is required to develop gallbladder inflammation. Once inflammation of
the gallbladder begins, additional inflammatory mediators are released, further propagating
gallbladder inflammation. In many patients, infection of the biliary system is also involved in
the development of acute cholecystitis.
Studies in animals have demonstrated that ligation of the cystic duct alone does not result in
acute cholecystitis [8,9]. However, acute cholecystitis can be produced by blocking the cystic
duct, followed by deliberate irritation of the gallbladder mucosa (either mechanically with an
indwelling catheter or by infusion of an irritant).
One such irritant used in experimental models, lysolecithin, is produced from lecithin, a
normal constituent of bile. The production of lysolecithin from lecithin is catalyzed by
phospholipase A, which is present in gallbladder mucosa. This enzyme may be released into
the gallbladder following trauma to the gallbladder wall from an impacted gallstone [9].
Supporting this hypothesis is the observation that lysolecithin (normally absent in bile) is
detectable in gallbladder bile in patients with acute cholecystitis [10].
Inflammatory mediators are released in response to gallbladder inflammation and further
propagate the inflammation [11]. Prostaglandins, which are involved in gallbladder
contraction and fluid absorption, probably play a central role in this process. In experimental
models using human gallbladder tissue, the main prostaglandins synthesized by inflamed
human gallbladder microsomes were prostaglandin E2 and 6-keto-prostaglandin F1 alpha,
the concentrations of which were increased four times above normal [12]. The prostaglandin
hypothesis is supported by the observation that prostaglandin inhibitors relieve biliary colic
and can reduce intraluminal cystic pressure [13-15].

Infection of bile within the biliary system probably has a role in the development of
cholecystitis; however, not all patients with cholecystitis have infected bile. This observation
was illustrated in a study of 467 subjects in whom bile samples were obtained from the
gallbladder and common bile duct for aerobic and anaerobic culture [16]. Patients with a
variety of hepatobiliary diseases and a healthy control group were included. Patients with
gallstones, acute cholecystitis, and hydropic gallbladder had similar rates of positive cultures
in the gallbladder and common bile duct, ranging from 22 to 46 percent; cultures were
generally sterile in healthy subjects. The main species isolated were Escherichia coli,
Enterococcus, Klebsiella, and Enterobacter.
Histologic changes of the gallbladder in acute cholecystitis can range from mild edema and
acute inflammation to necrosis and gangrene. Occasionally, prolonged impaction of a stone
in the cystic duct can lead to a distended gallbladder that is filled with colorless, mucoid fluid.
This condition, known as a mucocele with white bile (hydrops), is due to the absence of bile
entry into the gallbladder and absorption of all the bilirubin within the gallbladder.
CLINICAL MANIFESTATIONS — The clinical manifestations of acute cholecystitis include
prolonged (more than four to six hours), steady, severe right upper quadrant or epigastric
pain, fever, abdominal guarding, a positive Murphy's sign, and leukocytosis.
History — Patients with acute cholecystitis typically complain of abdominal pain, most
commonly in the right upper quadrant or epigastrium. The pain may radiate to the right
shoulder or back. Characteristically, acute cholecystitis pain is steady and severe.
Associated complaints may include fever, nausea, vomiting, and anorexia. There is often a
history of fatty food ingestion one hour or more before the initial onset of pain. The episode
of pain is typically prolonged (greater than four to six hours).
Physical examination — Patients with acute cholecystitis are usually ill appearing, febrile,
and tachycardic, and lie still on the examining table because cholecystitis is associated with
true local parietal peritoneal inflammation that is aggravated by movement. Abdominal
examination usually demonstrates voluntary and involuntary guarding. Patients frequently
will have a positive Murphy's sign. (See 'Murphy's sign' below.)
Patients with complications may have signs of sepsis (gangrene), generalized peritonitis
(perforation), abdominal crepitus (emphysematous cholecystitis), or bowel obstruction
(gallstone ileus). (See 'Complications' below and "Sepsis and the systemic inflammatory
response syndrome: Definitions, epidemiology, and prognosis", section on
'Sepsis' and "Diagnostic approach to abdominal pain in adults", section on
'Peritonitis' and "Epidemiology, clinical features, and diagnosis of mechanical small bowel
obstruction in adults", section on 'Gallstones or foreign body' and "Epidemiology, clinical
features, and diagnosis of mechanical small bowel obstruction in adults", section on 'Clinical
presentations'.)

Laboratory evaluation — Patients typically have a leukocytosis with an increased number
of band forms (ie, a left shift). Elevation in the serum total bilirubin and alkaline phosphatase
concentrations are not common in uncomplicated acute cholecystitis since biliary obstruction
is limited to the gallbladder; if present, they should raise concerns about complicating
conditions such as cholangitis, choledocholithiasis, or Mirizzi syndrome (a gallstone
impacted in the distal cystic duct causing extrinsic compression of the common bile duct)
(image 1). (See "Mirizzi syndrome".)
However, there have been reports of mild elevations in serum aminotransferases and
amylase, along with hyperbilirubinemia and jaundice, even in the absence of these
complications [17]. These abnormalities may be due to the passage of small stones, sludge,
or pus.
In patients with emphysematous cholecystitis, mild to moderate unconjugated
hyperbilirubinemia may be present because of hemolysis induced by clostridial infection.
(See 'Emphysematous cholecystitis' below.)
DIAGNOSIS — Acute cholecystitis should be suspected in a patient presenting with right
upper quadrant or epigastric pain, fever, and a leukocytosis. A positive Murphy's sign
supports the diagnosis [18]. However, history, physical examination, and laboratory test
findings are not sufficient to establish the diagnosis. Confirmation of the diagnosis requires
demonstration of gallbladder wall thickening or edema, a sonographic Murphy's sign, or
failure of the gallbladder to fill during cholescintigraphy (algorithm 1). In most cases, the
diagnosis can be confirmed with an abdominal ultrasound. If the diagnosis remains unclear,
cholescintigraphy can be obtained.
Murphy's sign — Patients with acute cholecystitis frequently have a positive "Murphy's
sign". To check for a Murphy's sign, the patient is asked to inspire deeply while the examiner
palpates the area of the gallbladder fossa just beneath the liver edge. Deep inspiration
causes the gallbladder to descend toward and press against the examining fingers, which in
patients with acute cholecystitis commonly leads to increased discomfort and the patient
catching his or her breath.
In one study, using cholescintigraphy as the gold standard, the sensitivity and specificity of a
positive Murphy's sign were 97 and 48 percent, respectively [19]. However, the sensitivity
may be diminished in the elderly [20].
Imaging studies — Physical examination alone cannot determine which abdominal viscera
is the source of inflammation and pain. Thus, patients presenting with clinical features
suggestive of acute cholecystitis should undergo abdominal imaging to confirm the
diagnosis. Ultrasonography is usually the first test obtained and can often establish the

diagnosis. Nuclear cholescintigraphy may be useful in cases in which the diagnosis remains
uncertain after ultrasonography.
Ultrasonography — The presence of stones in the gallbladder in the clinical setting of right
upper quadrant abdominal pain and fever supports the diagnosis of acute cholecystitis but is
not diagnostic. Additional sonographic features include:
●Gallbladder wall thickening (greater than 4 to 5 mm) or edema (double wall sign)
(image 2).
●A "sonographic Murphy's sign" is similar to the Murphy's sign elicited during
abdominal palpation, except that the positive response is observed during palpation
with the ultrasound transducer. This is more accurate than hand palpation because it
can confirm that it is indeed the gallbladder that is being pressed by the imaging
transducer when the patient catches his or her breath.
Several studies have evaluated the accuracy of ultrasonography in the diagnosis of acute
cholecystitis [18,21-26]. A particularly informative systematic review summarized the results
of 30 studies of ultrasonography for gallstones and acute cholecystitis [23]. Adjusted
sensitivity and specificity for diagnosis of acute cholecystitis were 88 percent (95%
confidence interval [CI] 0.74 to 1.00) and 80 percent (95% CI 0.62 to 0.98), respectively.
The sensitivity and specificity of ultrasonography for detection of gallstones are
approximately 84 (95% CI 0.76 to 0.92) and 99 percent (95% CI 0.97 to 1.00), respectively
[23]. Ultrasonography may not detect small stones or sludge as illustrated by a study that
compared ultrasonography with direct percutaneous mini-endoscopy in patients who had
undergone topical gallstone dissolution [27]. Ultrasonography was negative in 12 of 13
patients in whom endoscopy demonstrated 1 to 3 mm stones or fragments (picture 1) [27].
In patients with emphysematous cholecystitis, the ultrasound report may erroneously note
the presence of "overlying bowel gas making adequate visualization of the gallbladder
difficult", when in reality, this reflects air in the wall of the gallbladder. (See 'Emphysematous
cholecystitis' below.)
Cholescintigraphy (HIDA scan) — Cholescintigraphy using 99mTc-hepatic iminodiacetic
acid (generically referred to as a HIDA scan) is indicated if the diagnosis remains uncertain
following ultrasonography. Technetium labeled hepatic iminodiacetic acid (HIDA) is injected
intravenously and is then taken up selectively by hepatocytes and excreted into bile. If the
cystic duct is patent, the tracer will enter the gallbladder, leading to its visualization without
the need for concentration. The HIDA scan is also useful for demonstrating patency of the
common bile duct and ampulla. Normally, visualization of contrast within the common bile
duct, gallbladder, and small bowel occurs within 30 to 60 minutes (image 3). The test is

positive if the gallbladder does not visualize. This occurs because of cystic duct obstruction,
usually from edema associated with acute cholecystitis or an obstructing stone (image 4).
Cholescintigraphy has a sensitivity and specificity for acute cholecystitis of approximately 97
and 90 percent, respectively [23,26,28]. Cystic duct obstruction with a stone or tumor in the
absence of acute cholecystitis can cause a false positive test. Conditions that can cause
false positive results despite a non-obstructed cystic duct include:
●Severe liver disease, which may lead to abnormal uptake and excretion of the tracer.
●Fasting patients receiving total parenteral nutrition, in whom the gallbladder is already
maximally full due to prolonged lack of stimulation.
●Biliary sphincterotomy, which may result in low resistance to bile flow, leading to
preferential excretion of the tracer into the duodenum without filling of the gallbladder.
●Hyperbilirubinemia, which may be associated with impaired hepatic clearance of
iminodiacetic acid compounds. Newer agents commonly used in cholescintigraphy
(diisopropyl and m-bromotrimethyl iminodiacetic acid) have generally overcome this
limitation [29].
False negative results are uncommon since most patients with acute cholecystitis have
obstruction of the cystic duct. When they occur, they may be due to incomplete cystic duct
obstruction.
Morphine cholescintigraphy — A modified version of the HIDA scan has been described in
which patients are given intravenous morphine during the examination. Morphine increases
sphincter of Oddi pressure, thereby causing a more favorable pressure gradient for the
radioactive tracer to enter the cystic duct. This modification is thought to be particularly
useful in critically ill patients, in whom standard HIDA scanning may be associated with false
positive results [30,31]. However, the test has not been well standardized and has not
gained wide acceptance.
Magnetic resonance cholangiography — Magnetic resonance cholangiopancreatography
(MRCP) is a noninvasive technique for evaluating the intrahepatic and extrahepatic bile
ducts (image 5). Its role in the diagnosis of acute cholecystitis was evaluated in a series that
included 35 patients with symptoms of acute cholecystitis who underwent both ultrasound
and MRCP prior to cholecystectomy [7]. MRCP was superior to ultrasound for detecting
stones in the cystic duct (sensitivity 100 versus 14 percent) but was less sensitive than
ultrasound for detecting gallbladder wall thickening (sensitivity 69 versus 96 percent). At the
present time, its role in the diagnosis of acute cholecystitis should remain within clinical
trials. However, MRCP may be appropriate if there is concern that the patient may have a
stone in the common bile duct. (See "Magnetic resonance cholangiopancreatography".)

Computed tomography — Abdominal computed tomography (CT) is usually unnecessary
in the diagnosis of acute cholecystitis, although it can easily demonstrate gallbladder wall
edema associated with acute cholecystitis (image 6). Other CT findings include
pericholecystic stranding and fluid, and high-attenuation bile [32,33]. However, CT may fail
to detect gallstones because many stones are isodense with bile (image 7) [34,35]. CT can
be useful when complications of acute cholecystitis (such as emphysematous cholecystitis
or gallbladder perforation) are suspected or when other diagnoses are being considered.
(See 'Complications' below.)
Oral cholecystography — Oral cholecystography has no role in the diagnosis of acute
cholecystitis since it cannot show gallbladder wall edema and requires days to complete.
(See "Uncomplicated gallstone disease in adults", section on 'Oral cholecystography'.)
DIFFERENTIAL DIAGNOSIS — The greatest initial challenge in the diagnosis of acute
cholecystitis is distinguishing it from the more benign condition of biliary colic. Biliary colic is
usually caused by the gallbladder contracting in response to a fatty meal, pressing a stone
against the gallbladder outlet or cystic duct opening. This then results in increased intra-
gallbladder pressure and pain. As in acute cholecystitis, biliary colic causes pain in the right
upper quadrant. However, unlike acute cholecystitis, the pain is entirely visceral in origin,
without true gallbladder wall inflammation, so peritoneal signs are absent. In addition,
patients with biliary colic are afebrile with normal laboratory studies. As the gallbladder
relaxes, the stones often fall back from the cystic duct. As a result, the attack reaches a
crescendo over a number of hours and then resolves completely. (See "Uncomplicated
gallstone disease in adults", section on 'Biliary colic'.)
Most patients who develop acute cholecystitis have had previous attacks of biliary colic,
which may further confuse the diagnosis or lead patients to delay seeking medical attention.
The following features may help to distinguish an attack of biliary colic from acute
cholecystitis. However, such patients usually require imaging studies to help establish the
diagnosis:
●The pain of biliary colic typically reaches a crescendo, and then resolves completely.
Pain resolution occurs when the gallbladder relaxes, permitting stones to fall back from
the cystic duct. An episode of right upper quadrant pain lasting for more than four to six
hours should raise suspicion for acute cholecystitis.
●Patients with constitutional symptoms such as malaise or fever are more likely to
have acute cholecystitis.
Symptoms that are not suggestive of a biliary etiology include fatty food intolerance not in
the form of pain, nausea not in association with pain, pain only a few minutes after a meal,
irregular bowel habits, or belching [36,37].

A variety of other conditions can give rise to symptoms in the upper abdomen, which may be
confused with biliary colic or acute cholecystitis. These include:
●Acute pancreatitis.
●Appendicitis.
●Acute hepatitis.
●Peptic ulcer disease.
●Nonulcer dyspepsia.
●Irritable bowel disease.
●Functional gallbladder disorder.
●Sphincter of Oddi dysfunction.
●Diseases of the right kidney.
●Right-sided pneumonia.
●Fitz-Hugh-Curtis syndrome (perihepatitis caused by gonococcal infection). Right
upper quadrant pain with fever and even a possible positive Murphy's sign in patients
at high risk for sexually transmitted diseases should raise this possibility. The HIDA
scan is usually negative, but pericholecystic fluid may be confused with acute
cholecystitis (image 8).
●Subhepatic or intraabdominal abscess.
●Perforated viscus.
●Cardiac ischemia.
●Black widow spider envenomation [38].
These conditions can usually be differentiated by the clinical setting in which they occur and
by obtaining the appropriate diagnostic studies. (See "Differential diagnosis of abdominal
pain in adults", section on 'Upper abdominal pain syndromes' and "Diagnostic approach to
abdominal pain in adults", section on 'Acute abdominal pain'.)
COMPLICATIONS — Left untreated, symptoms of cholecystitis may abate within 7 to 10
days. However, complications are common, so patients with suspected acute cholecystitis
require definitive treatment (eg, cholecystectomy). The most common complication is the
development of gallbladder gangrene (up to 20 percent of cases) (image 9) with subsequent
perforation (2 percent of cases) [39]. (See "Treatment of acute calculous cholecystitis".)
Gangrene — Gangrenous cholecystitis is the most common complication of cholecystitis,
particularly in older patients, patients with diabetes, or those who delay seeking therapy [39].
The presence of a sepsis-like picture in addition to the other symptoms of cholecystitis
suggests the diagnosis, but gangrene may not be suspected preoperatively. (See "Sepsis
and the systemic inflammatory response syndrome: Definitions, epidemiology, and
prognosis", section on 'Sepsis'.)

Perforation — Perforation of the gallbladder usually occurs after the development of
gangrene. It is often localized, resulting in a pericholecystic abscess (image 10). Less
commonly, perforation is free into the peritoneum, leading to generalized peritonitis (image
11). Such cases are associated with a high mortality rate. (See"Diagnostic approach to
abdominal pain in adults", section on 'Peritonitis'.)
Cholecystoenteric fistula — A cholecystoenteric fistula may result from perforation of the
gallbladder directly into the duodenum or jejunum. Fistula formation is more often due to
long standing pressure necrosis from stones than to acute cholecystitis [40].
Gallstone ileus — Passage of a gallstone through a cholecystoenteric fistula may lead to
the development of mechanical bowel obstruction, usually in the terminal ileum (gallstone
ileus) (image 12) [41]. (See "Gallstone ileus" and "Epidemiology, clinical features, and
diagnosis of mechanical small bowel obstruction in adults", section on 'Clinical
presentations' and "Epidemiology, clinical features, and diagnosis of mechanical small bowel
obstruction in adults", section on 'Gallstones or foreign body'.)
Emphysematous cholecystitis — Emphysematous cholecystitis is caused by secondary
infection of the gallbladder wall with gas-forming organisms (such as Clostridium welchii)
(image 13) [42,43]. Other organisms that may be isolated include Escherichia coli (15
percent), staphylococci, streptococci, Pseudomonas, and Klebsiella [43].
Affected patients are often men in their fifth to seventh decade [43], and approximately one-
third to one-half have diabetes [43-45]. Gallstones are present in about one-half of patients.
Like other patients with acute cholecystitis, patients with emphysematous cholecystitis
usually present with right upper quadrant pain, nausea, vomiting, and low-grade fever.
Peritoneal signs are usually absent, but crepitus in the abdominal wall adjacent to the gall
bladder may rarely be detected. When such crepitus is present, it is an important clue to the
diagnosis. Mild to moderate unconjugated hyperbilirubinemia may be present (caused by
hemolysis induced by clostridial infection). The ultrasound report may erroneously note the
presence of "overlying bowel gas making adequate visualization of the gallbladder difficult",
when in reality, this reflects air in the wall of the gallbladder.
Emphysematous cholecystitis often heralds the development of gangrene, perforation, and
other complications [43-45]. In a review of 20 patients with emphysematous cholecystitis,
gallbladder perforation occurred in seven, pericholecystic abscess in nine, and bile peritonitis
in three [45].
INFORMATION FOR PATIENTS — UpToDate offers two types of patient education
materials, "The Basics" and "Beyond the Basics." The Basics patient education pieces are
written in plain language, at the 5th to 6
th grade reading level, and they answer the four or five
key questions a patient might have about a given condition. These articles are best for

patients who want a general overview and who prefer short, easy-to-read materials. Beyond
the Basics patient education pieces are longer, more sophisticated, and more detailed.
These articles are written at the 10th to 12
th grade reading level and are best for patients who
want in-depth information and are comfortable with some medical jargon.
Here are the patient education articles that are relevant to this topic. We encourage you to
print or e-mail these topics to your patients. (You can also locate patient education articles
on a variety of subjects by searching on "patient info" and the keyword(s) of interest.)
●Basics topics (see "Patient information: Gallstones (The Basics)" and "Patient
information: Gallbladder removal (cholecystectomy) (The Basics)")
●Beyond the Basics topics (see "Patient information: Gallstones (Beyond the Basics)")
SUMMARY AND RECOMMENDATIONS
●Acute cholecystitis refers to a syndrome of right upper quadrant pain, fever, and
leukocytosis associated with gallbladder inflammation and is usually related to
gallstone disease. (See 'Definitions' above.)
●Patients with acute cholecystitis typically complain of abdominal pain, most commonly
in the right upper quadrant or epigastrium. The pain may radiate to the right shoulder or
back. Characteristically, acute cholecystitis pain is prolonged (more than four to six
hours), steady, and severe. Associated complaints may include nausea, vomiting, and
anorexia. (See 'Clinical manifestations' above.)
●Acute cholecystitis should be suspected in a patient presenting with right upper
quadrant or epigastric pain, fever, and a leukocytosis. A positive Murphy's sign
supports the diagnosis. However, history, physical examination, and laboratory test
findings are not sufficient to make the diagnosis. Confirmation of the diagnosis requires
demonstration of gallbladder wall thickening or edema, a sonographic Murphy's sign, or
failure of the gallbladder to fill during cholescintigraphy (algorithm 1).
(See 'Diagnosis' above.)
●Acute cholecystitis must be distinguished from the more benign condition of biliary
colic, which presents with the same type of pain. Most patients who develop acute
cholecystitis have had previous attacks of biliary colic. The following features may help
to distinguish an attack of biliary colic from acute cholecystitis, though such patients
usually require imaging studies to help establish the diagnosis (see 'Differential
diagnosis' above and "Uncomplicated gallstone disease in adults", section on 'Biliary
colic'):
•The pain of biliary colic typically reaches a crescendo and then resolves
completely. Pain resolution occurs when the gallbladder relaxes, permitting
stones to fall back from the cystic duct. An episode of right upper quadrant pain

lasting for more than four to six hours should raise suspicion for acute
cholecystitis.
•Patients with constitutional symptoms such as malaise or fever are more likely to
have acute cholecystitis.
•Patients with biliary colic do not have signs of peritonitis on examination and
have normal laboratory tests.
●Left untreated, symptoms of cholecystitis may abate within 7 to 10 days. However,
complications are common, so patients with suspected acute cholecystitis require
definitive treatment (eg, cholecystectomy). The most common complication of acute
cholecystitis is the development of gallbladder gangrene (up to 20 percent of cases)
with subsequent perforation (2 percent of cases). (See 'Complications' above
and "Treatment of acute calculous cholecystitis".)
Use of UpToDate is subject to the Subscription and License Agreement.
REFERENCES
1. Friedman GD. Natural history of asymptomatic and symptomatic gallstones. Am J Surg 1993; 165:399.
2. Barie PS, Fischer E. Acute acalculous cholecystitis. J Am Coll Surg 1995; 180:232. 3. Ziessman HA. Cholecystokinin cholescintigraphy: clinical indications and proper
methodology. Radiol Clin North Am 2001; 39:997. 4. Kalloo AN, Kantsevoy SV. Gallstones and biliary disease. Prim Care 2001; 28:591. 5. Ahmed A, Cheung RC, Keeffe EB. Management of gallstones and their complications. Am
Fam Physician 2000; 61:1673. 6. Nahrwold DL, Rose RC, Ward SP. Abnormalities in gallbladder morphology and function in
patients with cholelithiasis. Ann Surg 1976; 184:415. 7. Park MS, Yu JS, Kim YH, et al. Acute cholecystitis: comparison of MR cholangiography and
US. Radiology 1998; 209:781. 8. MORRIS CR, HOHF RP, IVY AC. An experimental study of the role of stasis in the etiology
of cholecystitis. Surgery 1952; 32:673. 9. Roslyn JJ, DenBesten L, Thompson JE Jr, Silverman BF. Roles of lithogenic bile and cystic
duct occlusion in the pathogenesis of acute cholecystitis. Am J Surg 1980; 140:126. 10. Kaminski DL. Arachidonic acid metabolites in hepatobiliary physiology and disease.
Gastroenterology 1989; 97:781. 11. Jivegård L, Thornell E, Svanvik J. Pathophysiology of acute obstructive cholecystitis:
implications for non-operative management. Br J Surg 1987; 74:1084. 12. Myers SI, Bartula L. Human cholecystitis is associated with increased gallbladder
prostaglandin I2 and prostaglandin E2 synthesis. Hepatology 1992; 16:1176. 13. Thornell E, Jansson R, Svanvik J. Indomethacin reduces raised intraluminal gallbladder
pressure in acute cholecystitis. Acta Chir Scand 1985; 151:261. 14. Thornell E, Jansson R, Svanvik J. Indomethacin intravenously--a new way for effective relief
of biliary pain: a double-blind study in man. Surgery 1981; 90:468. 15. Akriviadis EA, Hatzigavriel M, Kapnias D, et al. Treatment of biliary colic with diclofenac: a
randomized, double-blind, placebo-controlled study. Gastroenterology 1997; 113:225.

16. Csendes A, Burdiles P, Maluenda F, et al. Simultaneous bacteriologic assessment of bile from gallbladder and common bile duct in control subjects and patients with gallstones and common duct stones. Arch Surg 1996; 131:389.
17. Kurzweil SM, Shapiro MJ, Andrus CH, et al. Hyperbilirubinemia without common bile duct abnormalities and hyperamylasemia without pancreatitis in patients with gallbladder disease. Arch Surg 1994; 129:829.
18. Trowbridge RL, Rutkowski NK, Shojania KG. Does this patient have acute cholecystitis? JAMA 2003; 289:80.
19. Singer AJ, McCracken G, Henry MC, et al. Correlation among clinical, laboratory, and hepatobiliary scanning findings in patients with suspected acute cholecystitis. Ann Emerg Med 1996; 28:267.
20. Adedeji OA, McAdam WA. Murphy's sign, acute cholecystitis and elderly people. J R Coll Surg Edinb 1996; 41:88.
21. Ralls PW, Colletti PM, Lapin SA, et al. Real-time sonography in suspected acute cholecystitis. Prospective evaluation of primary and secondary signs. Radiology 1985; 155:767.
22. Cooperberg PL, Burhenne HJ. Real-time ultrasonography. Diagnostic technique of choice in calculous gallbladder disease. N Engl J Med 1980; 302:1277.
23. Shea JA, Berlin JA, Escarce JJ, et al. Revised estimates of diagnostic test sensitivity and specificity in suspected biliary tract disease. Arch Intern Med 1994; 154:2573.
24. Kalimi R, Gecelter GR, Caplin D, et al. Diagnosis of acute cholecystitis: sensitivity of sonography, cholescintigraphy, and combined sonography-cholescintigraphy. J Am Coll Surg 2001; 193:609.
25. Chatziioannou SN, Moore WH, Ford PV, Dhekne RD. Hepatobiliary scintigraphy is superior to abdominal ultrasonography in suspected acute cholecystitis. Surgery 2000; 127:609.
26. Kiewiet JJ, Leeuwenburgh MM, Bipat S, et al. A systematic review and meta-analysis of diagnostic performance of imaging in acute cholecystitis. Radiology 2012; 264:708.
27. Zakko SF, Srb S, Ramsby GR. Sensitivity of percutaneous endoscopy compared with ultrasonography in the detection of residue or mucosal lesions after topical gallbladder stone dissolution. Gastrointest Endosc 1995; 42:434.
28. Fink-Bennett D, Freitas JE, Ripley SD, Bree RL. The sensitivity of hepatobiliary imaging and real-time ultrasonography in the detection of acute cholecystitis. Arch Surg 1985; 120:904.
29. Kim EE, Moon TY, Delpassand ES, et al. Nuclear hepatobiliary imaging. Radiol Clin North Am 1993; 31:923.
30. Flancbaum L, Choban PS, Sinha R, Jonasson O. Morphine cholescintigraphy in the evaluation of hospitalized patients with suspected acute cholecystitis. Ann Surg 1994; 220:25.
31. Oates E, Selland DL, Chin CT, Achong DM. Gallbladder nonvisualization with pericholecystic rim sign: morphine-augmentation optimizes diagnosis of acute cholecystitis. J Nucl Med 1996; 37:267.
32. Paulson EK. Acute cholecystitis: CT findings. Semin Ultrasound CT MR 2000; 21:56. 33. Fidler J, Paulson EK, Layfield L. CT evaluation of acute cholecystitis: findings and
usefulness in diagnosis. AJR Am J Roentgenol 1996; 166:1085. 34. Barakos JA, Ralls PW, Lapin SA, et al. Cholelithiasis: evaluation with CT. Radiology 1987;
162:415. 35. Benarroch-Gampel J, Boyd CA, Sheffield KM, et al. Overuse of CT in patients with
complicated gallstone disease. J Am Coll Surg 2011; 213:524. 36. Barbara L, Sama C, Morselli Labate AM, et al. A population study on the prevalence of
gallstone disease: the Sirmione Study. Hepatology 1987; 7:913.

37. Kraag N, Thijs C, Knipschild P. Dyspepsia--how noisy are gallstones? A meta-analysis of epidemiologic studies of biliary pain, dyspeptic symptoms, and food intolerance. Scand J Gastroenterol 1995; 30:411.
38. Bush SP. Black widow spider envenomation mimicking cholecystitis. Am J Emerg Med 1999; 17:315.
39. Reiss R, Nudelman I, Gutman C, Deutsch AA. Changing trends in surgery for acute cholecystitis. World J Surg 1990; 14:567.
40. Roslyn JJ, Thompson JE Jr, Darvin H, DenBesten L. Risk factors for gallbladder perforation. Am J Gastroenterol 1987; 82:636.
41. Clavien PA, Richon J, Burgan S, Rohner A. Gallstone ileus. Br J Surg 1990; 77:737. 42. Lorenz RW, Steffen HM. Emphysematous cholecystitis: diagnostic problems and differential
diagnosis of gallbladder gas accumulations. Hepatogastroenterology 1990; 37 Suppl 2:103. 43. Sarmiento RV. Emphysematous cholecystitis. Report of four cases and review of the
literature. Arch Surg 1966; 93:1009. 44. Mentzer RM Jr, Golden GT, Chandler JG, Horsley JS 3rd. A comparative appraisal of
emphysematous cholecystitis. Am J Surg 1975; 129:10. 45. Garcia-Sancho Tellez L, Rodriguez-Montes JA, Fernandez de Lis S, Garcia-Sancho Martin
L. Acute emphysematous cholecystitis. Report of twenty cases. Hepatogastroenterology 1999; 46:2144.
Ultrasound from a patient with acute cholecystitis and Mirizzi syndrome
Transabdominal ultrasound from a patient with acute cholecystitis and Mirizzi syndrome. The
patient presented with right upper quadrant pain and jaundice. Acute cholecystitis and
Mirizzi syndrome are confirmed by the ultrasound findings of a positive sonographic
Murphy's sign (pain with compression of the gallbladder by the ultrasound probe), a large
shadowing stone impacted in the infundibulum of the gallbladder (white arrow), cholestasis
with sludge (yellow arrowhead), and a dilated common hepatic duct (white arrowheads in
B).Graphic 86878 Version 1.0

Algorithm for the diagnosis of acute cholecystitis
GB: gallbladder; U/S: ultrasound.Graphic 50032 Version 3.0
Acute cholecystitis with pericholecystic fluid seen on
ultrasound

(A) Longitudinal view of the gallbladder showing small shadowing stones in the dependent
part of the gallbladder (green arrow). The ultrasound also shows a thickened wall in both
the longitudinal projection (white arrow) and transverse projection (B). (B) A small amount
of pericholecystic fluid is noted (yellow arrow). (C) The Doppler study shows an increase in
blood flow to the wall (red arrow) reminiscent of the hyperemia of an inflammatory process.
These findings are consistent with acute calculous cholecystitis. Graphic 83042 Version 2.0
Percutaneous gallbladder endoscopy showing gallstone
Percutaneous gallbladder endoscopy shows a small gallstone that was not detected on
ultrasonography. Courtesy of Salam Zakko, MD, FACP. Graphic 65714 Version 2.0
Normal HIDA scan

This is an example of a normal 99mTc-hepatic iminodiacetic acid (HIDA) scan and shows
early filling of the gallbladder at 15 minutes (white arrow) and complete filling by 25
minutes (white arrowhead), indicating a patent cystic duct. Graphic 59241 Version 3.0
HIDA scan in a patient with acute cholecystitis
The hepatic iminodiacetic acid (HIDA) scan is abnormal and shows absence of filling of the
gallbladder, indicating obstruction of the cystic duct. The duodenum starts to fill with
radioisotope at about 20 minutes (white arrow). The radioisotope flows directly into the
duodenum (white arrow) starting at 20 minutes. The gallbladder never fills during the
course of the 60 minute examination. These findings are consistent with the diagnosis of
acute cholecystitis. Graphic 86879 Version 1.0

Magnetic resonance imaging (MRI) and magnetic resonance cholangiopancreatography (MRCP) in a patient with acute
cholecystitis
MRI and MRCP images from a patient with acute cholecystitis. Contrast enhanced (A) and fat
saturated T2-weighted imaging (B) reveal a hyperemic gallbladder wall (white arrowheads).
Multiple small stones are noted lying dependently in the base of the gallbladder (white
arrow). The MRCP in the coronal projections (C and D) reveals accumulation of
pericholecystic fluid (short yellow arrows). These findings are consistent with the diagnosis of
acute cholecystitis Graphic 86864 Version 2.0
Computed tomographic (CT) scan from a patient with acute cholecystitis

The CT scan shows a distended gallbladder with an edematous and hyperemic wall (thick
arrow) and inflammatory induration in the fat surrounding the gallbladder (arrowheads). A
calcified stone is visible lying dependently at the base of the gallbladder (thin arrow).
Graphic 77336 Version 3.0
Computed tomographic (CT) scan and ultrasound in a patient with acute
cholecystitis
The CT scan (A and B) shows a thick walled and distended gallbladder (thick white arrow)
with pericholecystic induration (yellow arrowheads). However, it does not reveal
gallstones. The radiologic differential diagnosis includes acute calculous and acalculous
cholecystitis. The ultrasound (C and D) confirms the presence of a distended gallbladder
(thick white arrow) with stones (black arrow), and the presence of tumefactive sludge
(short yellow arrow). The thin white arrow shows a small amount of fluid in the gallbladder
fossa. These findings are consistent with acute calculous cholecystitis. Graphic 86866
Version 1.0

Fitz-Hugh Curtis syndrome
A CT-scan image (left) of a young female with Fitz-Hugh Curtis Syndrome. Note the
contracted gallbladder in the very center giving the appearance of a gallstone and the large
amount of pericholecystic fluid around it. The ultrasound image (right) confirms the
contracted gallbladder with the double wall sign. Courtesy of Salam F Zakko, MD,
FACP.Graphic 65754 Version 3.0
Gallbladder gangrene on transabdominal ultrasound
Transabdominal ultrasound of a gangrenous gallbladder showing evidence of necrotic and
denuded mucosa. The longitudinal view of the base of the gallbladder (A) shows a distended
gallbladder, with multiple stones within gallbladder sludge (thin yellow arrow) casting an
acoustic shadow (thick yellow arrow). The longitudinal view of the fundus (B) demonstrates
denuded mucosa (yellow arrowhead), indicating early necrosis of the gallbladder wall.
Graphic 86863 Version 1.0

Liver abscess complicating acute cholecystitis
Computed
tomographic (CT) scan in a patient with acute cholecystitis complicated by perforation and
liver abscess formation. (A) The CT scan shows a gall stone (yellow arrow) surrounded by
an irregular accumulation of fluid with a hyperemic rim (yellow arrowhead). (B) The fluid
can be seen extending from the gallbladder fossa into the liver parenchyma (yellow
arrowhead). (C) Percutaneous aspiration of pus confirmed the presence of an abscess and a
drain was placed (yellow arrow). Following drainage of the abscess, a small amount of
contrast was injected into the decompressed cavity. Graphic 86867 Version 1.0

Contained gallbladder perforation in a patient with acute cholecystitis
Computed
tomographic (CT) scan showing a sealed perforation of the gallbladder. Transverse (A) and
reformatted coronal projections (B) of the CT scan demonstrate a focal accumulation of fluid
near the fundus of the gallbladder (white arrowhead) with significant induration in the
pericholecystic fat (yellow arrow). At surgery a necrotic and perforated gallbladder was
identified. Graphic 86865 Version 1.0
Gallstone ileus seen on computed tomography (CT) scan
CT scan in a 75-year-old woman with small bowel obstruction due to gallstone ileus. Left
panel: Free air is seen in the biliary tree and gallbladder (arrow). Right panel: Dilated loops
of small bowel with large gallstone with a calcified rim (arrow) impacted in the terminal
ileum. Courtesy of Nezam Afdhal, MD. Graphic 80522 Version 5.0

Emphysematous cholecystitis seen on computed tomographic scan
(A) An axial image of a contrast enhanced computed tomographic (CT) scan demonstrating air within the gallbladder lumen (arrows). (B) A coronal reformat of a contrast enhanced CT demonstrating air within the wall of the gallbladder (arrow).

Treatment of acute calculous cholecystitis
Authors
Charles M Vollmer, Jr, MD
Salam F Zakko, MD, FACP
Nezam H Afdhal, MD, FRCPI
Section Editor
Stanley W Ashley, MD
Deputy Editor
Kathryn A Collins, MD, PhD, FACS
All topics are updated as new evidence becomes available and our peer review process is
complete.
Literature review current through: Mar 2015. | This topic last updated: Feb 03, 2015.
INTRODUCTION — Acute cholecystitis refers to a syndrome of right upper quadrant pain,
fever, and leukocytosis associated with gallbladder inflammation, which is usually related to
gallstone disease (ie, acute calculous cholecystitis). Complications include the development
of gangrene and gallbladder perforation, which can be life-threatening.
The treatment of acute calculous cholecystitis will be reviewed here. The approach to
patients with asymptomatic gallstones, the approach to the pregnant patient with gallstones,
and the clinical manifestations and diagnosis of biliary colic, acute cholecystitis and related
conditions, such as acalculous and xanthogranulomatous cholecystitis, are discussed
separately. (See "Uncomplicated gallstone disease in adults" and "Approach to the patient
with incidental gallstones" and"Choledocholithiasis: Clinical manifestations, diagnosis, and
management" and "Gallstones in pregnancy" and "Acute cholecystitis: Pathogenesis, clinical
features, and diagnosis" and "Acalculous cholecystitis" and "Xanthogranulomatous
cholecystitis".)
OVERVIEW OF TREATMENT — Once a patient develops symptoms or complications
related to gallstones (biliary colic, acute cholecystitis, cholangitis, and/orpancreatitis),
definitive therapy (cholecystectomy, cholecystostomy, endoscopic sphincterotomy, medical
gallstone dissolution) is recommended. Without treatment to eliminate the gallstones, the
likelihood of subsequent symptoms or complications is high. Complications include the
development of gangrene and gallbladder perforation, which can be life-threatening.
(See 'Morbidity and mortality' below.)
●In the National Cooperative Gallstone Study, a trial of nonsurgical treatment with
chenodiol for biliary tract pain, demonstrated that the risk of recurrent symptoms for
untreated patients was approximately 70 percent during the two years following initial
presentation [1].

●In a cohort study of 25,397 patients from Ontario, Canada with a first episode of
uncomplicated acute cholecystitis, 10,304 did not undergo cholecystectomy on their
first admission [2]. During a median 3.4 years of follow-up, 24 percent of patients had a
gallstone-related event with the majority of events occurring within the first year (88
percent). The risk was highest among 18 to 34-year-old patients. Among the events, 30
percent were for biliary obstruction or pancreatitis.
●A review of the United States Medicare database that included 29,818 elderly patients
with acute cholecystitis, found a higher risk for mortality over the following two years in
patients who were discharged without surgery compared with patients who underwent
cholecystectomy in the initial hospitalization (hazard ratio 1.56, 95% CI 1.47-1.65) [3].
Our treatment approach is as follows (algorithm 1):
●Patients with acute cholecystitis should be admitted to the hospital for supportive
care, which includes intravenous fluid therapy, correction of electrolyte disorders, and
control of pain. Antibiotics may also be indicated. (See 'Supportive care' below.)
●The selection and timing of definitive therapy depends upon the severity of symptoms
and the patient's overall risk for cholecystectomy. (See 'Medical risk
assessment' below.)
●If gangrene or perforation are suspected, or if the patient develops progressive
symptoms and signs such as fever, hemodynamic instability, or intractable pain while
on supportive therapy, emergency cholecystectomy or gallbladder drainage may be
needed (image 1). (See 'Timing of cholecystectomy' below and 'Indications for surgery
in high-risk patients' below.)
●Low-risk patients without emergent indications for intervention generally undergo
laparoscopic cholecystectomy preferably during the same admission. (See 'Low-risk
patients' below.)
●High-risk patients without emergent indications for intervention are treated with a
gallbladder drainage procedure if symptoms do not improve with supportive care. For
patients whose medical status can be optimized to allow surgery, cholecystectomy can
be considered. (See 'High-risk patients' below.)
SUPPORTIVE CARE — Patients diagnosed with acute calculous cholecystitis should be
admitted to the hospital. Patients have often been ill for days prior to seeking medical
attention, making intravenous hydration and correction of any associated electrolyte
disorders an important initial measure.
Patients should be kept fasting, and although uncommonly needed, those who are vomiting
should have placement of a nasogastric tube. (See "Nasogastric and nasoenteric tubes".)

Pain control — Pain control in patients with acute cholecystitis can usually be achieved with
nonsteroidal antiinflammatory drugs (NSAIDs) or opioids. Progression of pain during
treatment for acute cholecystitis, despite adequate analgesia, is an indicator of a clinical
progression.
We prefer ketorolac (30 to 60 mg adjusted for age and renal function given in a single
intramuscular dose) for patients with biliary colic. Treatment usually relieves symptoms
within 20 to 30 minutes. Opioids, such as morphine, hydromorphone, or meperidine are
appropriate therapy for patients who have contraindications to NSAIDs or who do not
achieve adequate pain relief with an NSAID, which may be more common in patients with
acute cholecystitis compared with uncomplicated gallstone disease.
It was traditionally thought that meperidine was the opioid of choice in patients with gallstone
disease because it has less of an effect on sphincter of Oddi motility thanmorphine [4-6].
However, a systematic review found that all opioids increase sphincter of Oddi pressure [5].
There are insufficient data to suggest that morphine should be avoided. Morphine has an
advantage that it requires less frequent dosing than meperidine, which has a shorter half-life.
Antibiotics — Acute cholecystitis is primarily an inflammatory process, but secondary
infection of the gallbladder can occur as a result of cystic duct obstruction and bile stasis
[7,8]. The rate of empyema and pericholecystic abscess is overall low, but patients can
easily develop life-threatening gram negative sepsis from uncomplicated, acute cholecystitis.
Thus, antibiotics are commonly administered at the outset to protect against sepsis and
wound infection [9]. Studies are conflicting as to whether antibiotics are required for the
treatment of uncomplicated, acute cholecystitis [7,8,10-12]. One study of 302 patients
showed a lower rate of bacteremia and wound infection, but no difference in the
development of empyema of the gallbladder or pericholecystic abscesses with the
administration of antibiotics [13]. This is likely due to the obstruction to bile flow that
interferes with achieving adequate gallbladder bile concentrations of antibiotics.
Many clinicians routinely administer antimicrobial therapy to all patients diagnosed with
acute cholecystitis, which are continued until the gallbladder is removed or the cholecystitis
clinically resolves. Others advocate that antimicrobial therapy should only be instituted if
sepsis is suspected on the basis of laboratory (more than 12,000 white cells per cubic
millimeter) or clinical findings (temperature of more than 38.3°C, <36°C), or in patients with a
diagnosis of acute cholecystitis and radiographic findings indicative of gallbladder ischemia
or necrosis (eg, air in the gallbladder or gallbladder wall). Routine antibiotics are also
recommended in older patients or those with diabetes or immunodeficiency with a diagnosis
of acute cholecystitis regardless of these signs [10,14]. (See "Sepsis and the systemic
inflammatory response syndrome: Definitions, epidemiology, and prognosis".)

When antibiotic therapy is initiated, the duration of postoperative treatment is generally
tailored to the clinical situation. A multicenter trial randomly assigned 414 patients
hospitalized for mild or moderate calculous cholecystitis to continue their preoperative
antibiotic regimen for five days (2 g amoxicillin plus clavulanic acid, three times daily) or to
receive no antibiotics following cholecystectomy [15]. No significant differences in
postoperative infection rates (17 versus 15 percent) were found. These results support our
current practice of discontinuing antibiotics the day after the cholecystectomy for patients
with uncomplicated cholecystitis. Clinical judgement should dictate antibiotic management in
more complicated scenarios, such as in the septic postoperative patient.
The need for prophylactic antibiotics at the time of surgery in the absence of
clinical symptoms/signs of biliary infection is discussed elsewhere. (See "Open
cholecystectomy", section on 'Prophylactic antibiotics' and "Laparoscopic cholecystectomy",
section on 'Antibiotics'.)
Empiric antibiotic therapy should include activity against the most common pathogens. In a
study of 467 patients, including a control group of 42 with normal biliary trees, positive bile
cultures were found in 22 percent of patients with symptomatic gallstones and 46 percent of
patients with acute cholecystitis [16]. The most frequent isolates from the gallbladder or
common bile duct were Escherichia coli (41 percent), Enterococcus (12 percent), Klebsiella
(11 percent), and Enterobacter (9 percent). Empiric antibiotic therapy options and doses are
provided in the table (table 1). Antibiotic therapy should subsequently be tailored to culture
and susceptibility results when available [7]. Thus, broad-spectrum antibiotics should cover
gram-negative organisms and anaerobes. Commonly used regimens are piperacillin-
tazobactam, ceftriaxoneplus metronidazole, or levofloxacin plus metronidazole.
MEDICAL RISK ASSESSMENT — The American Society of Anesthesiologists (ASA)
physical status classification is commonly used to stratify the risk of surgery (table 2) [17].
Other methods to specifically assess cardiac or pulmonary risk are discussed elsewhere.
(See "Overview of anesthesia and anesthetic choices" and "Evaluation of cardiac risk prior to
noncardiac surgery" and "Evaluation of preoperative pulmonary risk".)
LOW-RISK PATIENTS
Timing of cholecystectomy — Early cholecystectomy, rather than antibiotic therapy and
delayed (>7 days after admission) may be preferred among patients who require
hospitalization for acute cholecystitis and who are good candidates for cholecystectomy. The
bulk of the evidence from large database reviews and randomized trials show that
cholecystectomy performed early during the initial hospitalization may be associated with
reduced perioperative morbidity and mortality in some patients, and reduces the length of
hospital stay and cost [3,18-30]. Early surgery is also easier to perform as local inflammation
increases 72 hours past the initial onset of symptoms making dissection less precise,
http://www.uptodate.com/contents/piperacillin-and-tazobactam-sodium-drug-information?source=see_link

increasing the severity of surgical complications, and making open conversion more likely.
Nevertheless, there are data to suggest that surgery is still safe even after 72 hours of
symptom onset [27,31,32].
An early systematic review that included predominantly open, but also laparoscopic
cholecystectomy in patients with acute calculous cholecystitis found no significant
differences in perioperative morbidity or mortality, but a significantly shorter length of hospital
stay for the early surgery group (9.6 versus 5.8 days) [26]. More than 20 percent of patients
in the delayed surgery group failed to respond to conservative management or suffered
recurrent cholecystitis in the interval period. A coincident Cochrane review (2004) that
included five trials limited to laparoscopic cholecystectomy concluded that early laparoscopic
cholecystectomy (ranging from immediate cholecystectomy to cholecystectomy within seven
days of symptoms) is safe and significantly shortens hospital stay [18]. No significant
differences were seen between the groups for the rate of bile duct injury or conversion to
open cholecystectomy. An updated Cochrane review (2013) limited to laparoscopic
cholecystectomy included two additional trials [28,30], but had similar findings [27]. The
incidence of bile duct injury in the early group was 0.4 percent, while that in the delayed
group was 0.9 percent, a difference that was not significant. Conversion rates were 19.7
versus 22.1 percent in the early versus late groups, respectively. Among four trials, the total
hospital stay was shorter in the early compared with the delayed group (mean difference -
4.12 days; 95% CI -5.22 to -3.03). It is important to note that significant complications such
as bile duct injury occur rarely, and the included trials (and likely any future clinical trials)
were not adequately powered to detect differences in the rates of bile duct injury and other
serious complications. Although the Cochrane reviews suggest similar conversion rates for
open procedures in patients operated on within seven days, they do not specify how many of
the “early surgery” patients were symptomatic for less than 72 hours. Some studies suggest
that patients who have surgery more than three days after the onset of symptoms have a
higher rate of conversion to open surgery compared with those who have had symptoms for
less than three days [33].
A later multicenter trial not included in the Cochrane metaanalyses, the Acute Cholecystitis-
early laparoscopic surgery versus antibiotic therapy and Delayed elective Cholecystectomy
(ACDC) trial (NCT00447304), randomly assigned patients to surgery within 24 hours of
hospital admission (n = 304) or initial antibiotic treatment followed by laparoscopic
cholecystectomy delayed more than seven days (n = 314 patients) [23]. The overall rate of
morbidity was significantly lower in the immediate compared with delayed cholecystectomy
group (11.8 versus 34.4 percent). The rate of conversion to open surgery and mortality did
not differ significantly between groups. Mean length of hospital stay (5.4 days versus 10.0
days) and total hospital costs were significantly lower in the immediate cholecystectomy
group.

Large database reviews have identified similar benefits for prompt surgical intervention, as
well as possible reductions in morbidity and improved late outcomes [22,25,29].
●In a large cohort study from Ontario, Canada, a significantly lower rate of major bile
duct injury (0.28 versus 0.53 percent) and shorter length of hospital stay (mean
difference -1.9 days) were seen for early compared with delayed cholecystectomy (≥7
days) among 14,220 patients with a first episode of acute cholecystitis [25].
●In a review from the American College of Surgeons National Surgical Quality
Improvement Program (NSQIP), those who underwent operation later in the course of
admission were more likely to require an open procedure [22].
Surgical approach — Laparoscopic cholecystectomy is considered the standard approach
for the surgical treatment of acute calculous cholecystitis. Compared with open
cholecystectomy, laparoscopic cholecystectomy reduces postoperative pain and significantly
shortens hospital length of stay and convalescence, and time away from work, and is
preferred by many patients from a cosmetic viewpoint [34-40]. However, the overall serious
complication rate in laparoscopic cholecystectomy remains higher than that seen with open
cholecystectomy; thus, the threshold for conversion to an open procedure should be low
[41,42]. Factors which may lead the surgeon to primarily choose, or convert to, an open
approach are discussed in detail elsewhere. (See "Open cholecystectomy", section on
'Indications for open surgery' and"Laparoscopic cholecystectomy", section on 'Intraoperative
complications'.)
For selected patients in whom the risk for injury or excessive blood loss is deemed too high
to perform cholecystectomy, a cholecystostomy or a subtotal cholecystectomy can be
performed. The latter procedure achieves control of the cystic duct at the level of the neck of
the gallbladder and leaves the dome of the gallbladder adherent to the liver fossa in situ
[43,44]. Biliary leaks can still occur, but these can generally be managed conservatively.
(See "Laparoscopic cholecystectomy" and "Complications of laparoscopic
cholecystectomy" and "Repair of common bile duct injuries".)
HIGH-RISK PATIENTS — Patients categorized as ASA classes III, IV, or V, have
perioperative mortality rates ranging from 5 to 27 percent, and are considered high risk for
cholecystectomy [17].
For these patients, the risk of cholecystectomy likely outweighs the potential benefits, and an
initial nonoperative approach should be undertaken that includes antibiotic therapy and
bowel rest. For those who fail to improve, gallbladder drainage should be implemented with
the eventual goal of performing cholecystectomy. Once cholecystitis resolves, the patient’s
risk for surgery should be reassessed. Patients who have become reasonable candidates for
surgery should undergo elective cholecystectomy [45]. Medical management with interval

cholecystectomy only for recurrent acute cholecystitis may be appropriate in some patients
[46].
Gallbladder drainage — Some form of gallbladder drainage is required for high-risk
patients managed conservatively but who show no appreciable improvement and progress
to severe symptoms. The goal of drainage is to direct purulent material away from the
obstructed gallbladder which also allows for resolution of edema, which often “opens” up the
obstructed cystic duct.
Gallbladder drainage can be accomplished via percutaneous, open surgical, or endoscopic
approaches. In one retrospective review of 185 patients, 78 percent were treated with
percutaneous cholecystostomy, and 22 percent with a tube placed surgically [47]. Over half
the patients (57 percent) subsequently underwent laparoscopic cholecystectomy.
Regardless of cholecystostomy tube approach, surgical or percutaneous, there were no
differences in the proportion of patients who underwent laparoscopic cholecystectomy as
definitive treatment.
Percutaneous and endoscopic methods are reviewed in the next sections. Open
cholecystostomy is discussed below. (See 'Indications for surgery in high-risk
patients'below.)
Percutaneous — Gallbladder drainage by percutaneous cholecystostomy in conjunction
with antibiotics may be the best initial treatment for very ill patients [48-51]. Percutaneous
cholecystostomy is often performed with the intent of delayed cholecystectomy; however,
many patients do not actually go on to receive cholecystectomy due to ongoing
contraindications [47,52].
A Cochrane review identified only two trials comparing outcomes for patients treated with
cholecystostomy for acute cholecystitis [53]. Neither of these trials found any significant
differences in mortality for the approaches studied, which included percutaneous
cholecystostomy and early laparoscopic cholecystectomy compared with delayed
laparoscopic cholecystectomy in one trial, and percutaneous cholecystostomy compared
with conservative treatment in the other trial. Although mortality differences have been found
in observational studies, in these studies, the healthiest cohort is selected by surgeons for
surgical management. As an example, in one retrospective review that included 1918
patients, 30-day mortality after percutaneous cholecystostomy was 15.4 percent, but only
4.5 percent for cholecystectomy [54]. Patients who underwent percutaneous
cholecystostomy were older, had a higher ASA classification, more comorbidities, longer
hospital stay, more complications, and more readmissions; most ultimately required
cholecystectomy. A time-cohort study had similar findings and noted that compared with
patients treated with cholecystostomy between 1989 and 1998, a significantly lower

percentage of patients treated between 1998 and 2009 had low ASA classification (zero
versus 18 percent) [55].
The technical success of percutaneous cholecystostomy ranges from 82 to 100 percent in
various series [48-51]. In a retrospective review, the outcomes of 106 patients with acute
cholecystitis (calculous and acalculous) treated by percutaneous cholecystostomy were
evaluated over a 10-year period; 67 percent presented to the emergency room and 23
percent were inpatients admitted initially for other conditions [56]. About half in each group
had gallstones. After cholecystostomy tube placement, clinical improvement was seen
overall in 68 percent, whereas 32 percent showed no improvement or clinically worsened.
More patients who presented to the emergency department primarily with acute cholecystitis
showed improvement compared with the inpatients (84 versus 34 percent).
Minor complications of percutaneous drainage include bleeding, catheter blockage and
dislodgement (10 to 15 percent), and failure to resolve the acute cholecystitis (10 percent)
[49,51,57]. In one study, major bleeding complications occurred rarely (0.4 percent) and
were no different between patients with and without coagulopathy [57]. Failure is usually
related to ineffective drainage due to thick sludge or pus. We generally irrigate the
gallbladder contents manually with normal saline through the catheter. If irrigation is
ineffective, the percutaneous pigtail catheter can be replaced over a wire with a larger one to
achieve more effective irrigation.
Patients who stabilize but continue to be high risk for surgery can be considered for
percutaneous gallstone extraction with or without mechanical lithotripsy [58].
Endoscopic — Endoscopic transpapillary gallbladder drainage has also been reported in
patients with acute cholecystitis in whom percutaneous approaches are contraindicated, or
are not anatomically feasible [59,60]. The technique can be technically challenging. In
addition, this procedure has all the inherent and occasionally serious complications
associated with endoscopic retrograde cholangiography. (See "Endoscopic retrograde
cholangiopancreatography: Indications, patient preparation, and complications".)
Indications for surgery in high-risk patients — The risk for surgery should be
reconsidered once cholecystitis resolves in patients treated conservatively with antibiotics
and gallbladder drainage. Patients who have become reasonable candidates for surgery
should undergo elective cholecystectomy.
An initial surgical approach may be preferred in some high-risk patients for whom the burden
of the ongoing systemic effects of cholecystitis is deemed to be greater than the risk of
surgery. A surgical approach may also become necessary if the less-invasive techniques
discussed above are not technically feasible, are unsuccessful at providing adequate

drainage, or if the patient does not improve following drainage, which suggests that the
gallbladder may have progressed to gangrene.
Laparoscopic cholecystectomy may be the preferred treatment in high-risk patients who
require surgery. If cholecystectomy is not feasible, a subtotal cholecystectomy can be
performed instead, but if medical risk precludes gallbladder removal, a surgical
cholecystostomy tube can be performed through a limited laparotomy in the operating room,
or at the bedside in the intensive care unit setting, if necessary. (See "Open
cholecystectomy", section on 'Open cholecystostomy tube placement'.)
MORBIDITY AND MORTALITY — The overall mortality of a single episode of acute
cholecystitis is approximately 3 percent. However, the risk in a given patient depends upon
the patient's health and surgical risk [49]. Mortality is less than 1 percent in young, otherwise
healthy patients, but approaches 10 percent in high-risk patients, or in those with
complications. Perioperative morbidity and mortality associated with specific treatments are
reviewed elsewhere. (See "Open cholecystectomy", section on 'Perioperative morbidity and
mortality' and "Laparoscopic cholecystectomy", section on 'Postoperative complications'.)
A study of the American College of Surgeons National Surgical Quality Improvement
Program (NSQIP) database evaluated outcomes following treatment of acute cholecystitis in
5460 patients with and without diabetes [61]. Mortality among 770 patients with diabetes was
significantly higher than in the 4690 patients without diabetes (4.4 versus 1.4 percent). The
risk for complications including cardiovascular events and renal failure was also significantly
increased.
Prevention of recurrent gallstones — Following cholecystectomy, or other nonsurgical
means to remove gallstones, patients who remain at high risk for developing recurrent
gallstones may benefit from certain medical therapies. These are discussed elsewhere.
(See "Patient selection for the nonsurgical treatment of gallstone disease", section on
'Prophylaxis in patients at high risk for developing symptomatic gallstone disease'.)
SUMMARY AND RECOMMENDATIONS
●Acute cholecystitis refers to a syndrome of right upper quadrant pain, fever, and
leukocytosis associated with gallbladder inflammation, which is usually related to
gallstone disease. Once a patient develops acute cholecystitis, definitive therapy aimed
at eliminating the gallstones is recommended. Without definitive therapy, the likelihood
of recurrent symptoms or complications is high. (See 'Introduction' above
and 'Overview of treatment' above.)
●Patients diagnosed with acute cholecystitis should be admitted to the hospital. Initial
supportive care includes intravenous fluid therapy, correction of electrolyte disorders,
and control of pain. Adequate pain control can usually be achieved with nonsteroidal

antiinflammatory drugs (NSAIDs) or opioids. Patients should be kept fasting and those
who are vomiting may need placement of a nasogastric tube. (See 'Supportive
care' above.)
●Acute cholecystitis is primarily an inflammatory process, but secondary infection of
the gallbladder can occur as a result of cystic duct obstruction and bile stasis. Many
clinicians routinely administer antimicrobial therapy to all patients diagnosed with acute
cholecystitis, which are continued until the gallbladder is removed or the cholecystitis
clinically resolves. If sepsis is suspected (laboratory or clinical findings), or radiographic
findings are indicative of gallbladder ischemia or necrosis, we suggest empiric antibiotic
therapy (Grade 2C). Antibiotic options and doses are provided in the table (table 1).
For patients with uncomplicated cholecystitis, we discontinue antibiotics the day after
the cholecystectomy. (See 'Antibiotics' above.)
●The choice and timing of intervention for acute cholecystitis (cholecystectomy,
gallbladder drainage) depends upon the severity of symptoms and the patient's overall
risk of surgery. Drainage options include percutaneous or open cholecystostomy and
endoscopic sphincterotomy.
•Emergent intervention is indicated for patients with:
-Progressive symptoms and signs such as high fever, hemodynamic
instability, or intractable pain in spite of adequate pain medication.
-Suspicion of gallbladder gangrene or gallbladder perforation
•For patients without emergent indications for definitive therapy who are low risk
for surgery, we recommend cholecystectomy during the initial hospitalization
(Grade 1A). Cholecystectomy performed early rather than later in the
hospitalization may be associated with reduced perioperative morbidity and
mortality. Low-risk patients generally undergo laparoscopic cholecystectomy.
Compared with open cholecystectomy, laparoscopic cholecystectomy reduces
postoperative pain and significantly shortens the length of hospital stay and
convalescence. (See 'Timing of cholecystectomy' above and 'Low-risk
patients'above.)
•For patients without emergent indications for definitive therapy, and in whom the
risk of cholecystectomy outweighs the potential benefits, gallbladder drainage
(percutaneous cholecystostomy, endoscopic sphincterotomy, open
cholecystostomy) is indicated if symptoms do not improve with supportive care.
Once cholecystitis resolves, the patient’s risk for surgery should be reassessed.
Patients who have become reasonable candidates for surgery should undergo
elective cholecystectomy. Patients who stabilize with a cholecystostomy tube but
continue to be at high-risk for surgery can be considered for percutaneous
gallstone extraction with or without mechanical lithotripsy. (See 'Gallbladder
drainage' above.)

●Mortality associated with a single episode of acute cholecystitis depends upon the
patient's health and surgical risk. Overall mortality is approximately 3 percent, but is
less than 1 percent in young, otherwise healthy patients, and approaches 10 percent in
high-risk patients, or in those with complications.
Use of UpToDate is subject to the Subscription and License Agreement.
REFERENCES
1. Thistle JL, Cleary PA, Lachin JM, et al. The natural history of cholelithiasis: the National Cooperative Gallstone Study. Ann Intern Med 1984; 101:171.
2. de Mestral C, Rotstein OD, Laupacis A, et al. A population-based analysis of the clinical course of 10,304 patients with acute cholecystitis, discharged without cholecystectomy. J Trauma Acute Care Surg 2013; 74:26.
3. Riall TS, Zhang D, Townsend CM Jr, et al. Failure to perform cholecystectomy for acute cholecystitis in elderly patients is associated with increased morbidity, mortality, and cost. J Am Coll Surg 2010; 210:668.
4. Elta GH, Barnett JL. Meperidine need not be proscribed during sphincter of Oddi manometry. Gastrointest Endosc 1994; 40:7.
5. Thompson DR. Narcotic analgesic effects on the sphincter of Oddi: a review of the data and therapeutic implications in treating pancreatitis. Am J Gastroenterol 2001; 96:1266.
6. Thune A, Baker RA, Saccone GT, et al. Differing effects of pethidine and morphine on human sphincter of Oddi motility. Br J Surg 1990; 77:992.
7. Fuks D, Cossé C, Régimbeau JM. Antibiotic therapy in acute calculous cholecystitis. J Visc Surg 2013; 150:3.
8. Strasberg SM. Clinical practice. Acute calculous cholecystitis. N Engl J Med 2008; 358:2804. 9. Järvinen H, Renkonen OV, Palmu A. Antibiotics in acute cholecystitis. Ann Clin Res 1978;
10:247. 10. Solomkin JS, Mazuski JE, Bradley JS, et al. Diagnosis and management of complicated
intra-abdominal infection in adults and children: guidelines by the Surgical Infection Society and the Infectious Diseases Society of America. Clin Infect Dis 2010; 50:133.
11. Kanafani ZA, Khalifé N, Kanj SS, et al. Antibiotic use in acute cholecystitis: practice patterns in the absence of evidence-based guidelines. J Infect 2005; 51:128.
12. Mazeh H, Mizrahi I, Dior U, et al. Role of antibiotic therapy in mild acute calculus cholecystitis: a prospective randomized controlled trial. World J Surg 2012; 36:1750.
13. Kune GA, Burdon JG. Are antibiotics necessary in acute cholecystitis? Med J Aust 1975; 2:627.
14. Landau O, Kott I, Deutsch AA, et al. Multifactorial analysis of septic bile and septic complications in biliary surgery. World J Surg 1992; 16:962.
15. Regimbeau JM, Fuks D, Pautrat K, et al. Effect of postoperative antibiotic administration on postoperative infection following cholecystectomy for acute calculous cholecystitis: a randomized clinical trial. JAMA 2014; 312:145.
16. Csendes A, Burdiles P, Maluenda F, et al. Simultaneous bacteriologic assessment of bile from gallbladder and common bile duct in control subjects and patients with gallstones and common duct stones. Arch Surg 1996; 131:389.
17. Feigal DW, Blaisdell FW. The estimation of surgical risk. Med Clin North Am 1979; 63:1131. 18. Gurusamy KS, Samraj K. Early versus delayed laparoscopic cholecystectomy for acute
cholecystitis. Cochrane Database Syst Rev 2006; :CD005440.

19. Norrby S, Herlin P, Holmin T, et al. Early or delayed cholecystectomy in acute cholecystitis? A clinical trial. Br J Surg 1983; 70:163.
20. Lahtinen J, Alhava EM, Aukee S. Acute cholecystitis treated by early and delayed surgery. A controlled clinical trial. Scand J Gastroenterol 1978; 13:673.
21. McArthur P, Cuschieri A, Sells RA, Shields R. Controlled clinical trial comparing early with interval cholecystectomy for acute cholecystitis. Br J Surg 1975; 62:850.
22. Brooks KR, Scarborough JE, Vaslef SN, Shapiro ML. No need to wait: an analysis of the timing of cholecystectomy during admission for acute cholecystitis using the American College of Surgeons National Surgical Quality Improvement Program database. J Trauma Acute Care Surg 2013; 74:167.
23. Gutt CN, Encke J, Köninger J, et al. Acute cholecystitis: early versus delayed cholecystectomy, a multicenter randomized trial (ACDC study, NCT00447304). Ann Surg 2013; 258:385.
24. Banz V, Gsponer T, Candinas D, Güller U. Population-based analysis of 4113 patients with acute cholecystitis: defining the optimal time-point for laparoscopic cholecystectomy. Ann Surg 2011; 254:964.
25. de Mestral C, Rotstein OD, Laupacis A, et al. Comparative operative outcomes of early and delayed cholecystectomy for acute cholecystitis: a population-based propensity score analysis. Ann Surg 2014; 259:10.
26. Papi C, Catarci M, D'Ambrosio L, et al. Timing of cholecystectomy for acute calculous cholecystitis: a meta-analysis. Am J Gastroenterol 2004; 99:147.
27. Gurusamy KS, Davidson C, Gluud C, Davidson BR. Early versus delayed laparoscopic cholecystectomy for people with acute cholecystitis. Cochrane Database Syst Rev 2013; 6:CD005440.
28. Macafee DA, Humes DJ, Bouliotis G, et al. Prospective randomized trial using cost-utility analysis of early versus delayed laparoscopic cholecystectomy for acute gallbladder disease. Br J Surg 2009; 96:1031.
29. Dua A, Dua A, Desai SS, et al. Gender based differences in management and outcomes of cholecystitis. Am J Surg 2013; 206:641.
30. Yadav RP, Adhikary S, Agrawal CS, et al. A comparative study of early vs. delayed laparoscopic cholecystectomy in acute cholecystitis. Kathmandu Univ Med J (KUMJ) 2009; 7:16.
31. Farooq T, Buchanan G, Manda V, et al. Is early laparoscopic cholecystectomy safe after the "safe period"? J Laparoendosc Adv Surg Tech A 2009; 19:471.
32. Litwin DE, Cahan MA. Laparoscopic cholecystectomy. Surg Clin North Am 2008; 88:1295. 33. Pessaux P, Tuech JJ, Regenet N, et al. [Laparoscopic cholecystectomy in the treatment of
acute cholecystitis. Prospective non-randomized study]. Gastroenterol Clin Biol 2000; 24:400.
34. Soper NJ, Stockmann PT, Dunnegan DL, Ashley SW. Laparoscopic cholecystectomy. The new 'gold standard'? Arch Surg 1992; 127:917.
35. Wiesen SM, Unger SW, Barkin JS, et al. Laparoscopic cholecystectomy: the procedure of choice for acute cholecystitis. Am J Gastroenterol 1993; 88:334.
36. Wilson RG, Macintyre IM, Nixon SJ, et al. Laparoscopic cholecystectomy as a safe and effective treatment for severe acute cholecystitis. BMJ 1992; 305:394.
37. Johansson M, Thune A, Nelvin L, et al. Randomized clinical trial of open versus laparoscopic cholecystectomy in the treatment of acute cholecystitis. Br J Surg 2005; 92:44.
38. Yamashita Y, Takada T, Kawarada Y, et al. Surgical treatment of patients with acute cholecystitis: Tokyo Guidelines. J Hepatobiliary Pancreat Surg 2007; 14:91.

39. Overby DW, Apelgren KN, Richardson W, et al. SAGES guidelines for the clinical application of laparoscopic biliary tract surgery. Surg Endosc 2010; 24:2368.
40. NIH releases consensus statement on gallstones, bile duct stones and laparoscopic cholecystectomy. Am Fam Physician 1992; 46:1571.
41. Vollmer CM Jr, Callery MP. Biliary injury following laparoscopic cholecystectomy: why still a problem? Gastroenterology 2007; 133:1039.
42. Khan MH, Howard TJ, Fogel EL, et al. Frequency of biliary complications after laparoscopic cholecystectomy detected by ERCP: experience at a large tertiary referral center. Gastrointest Endosc 2007; 65:247.
43. Bernard HR, Hartman TW. Complications after laparoscopic cholecystectomy. Am J Surg 1993; 165:533.
44. National Institutes of Health Consensus Development Conference Statement on Gallstones and Laparoscopic Cholecystectomy. Am J Surg 1993; 165:390.
45. Morse BC, Smith JB, Lawdahl RB, Roettger RH. Management of acute cholecystitis in critically ill patients: contemporary role for cholecystostomy and subsequent cholecystectomy. Am Surg 2010; 76:708.
46. McGillicuddy EA, Schuster KM, Barre K, et al. Non-operative management of acute cholecystitis in the elderly. Br J Surg 2012; 99:1254.
47. Cherng N, Witkowski ET, Sneider EB, et al. Use of cholecystostomy tubes in the management of patients with primary diagnosis of acute cholecystitis. J Am Coll Surg 2012; 214:196.
48. Melin MM, Sarr MG, Bender CE, van Heerden JA. Percutaneous cholecystostomy: a valuable technique in high-risk patients with presumed acute cholecystitis. Br J Surg 1995; 82:1274.
49. Ito K, Fujita N, Noda Y, et al. Percutaneous cholecystostomy versus gallbladder aspiration for acute cholecystitis: a prospective randomized controlled trial. AJR Am J Roentgenol 2004; 183:193.
50. Davis CA, Landercasper J, Gundersen LH, Lambert PJ. Effective use of percutaneous cholecystostomy in high-risk surgical patients: techniques, tube management, and results. Arch Surg 1999; 134:727.
51. Byrne MF, Suhocki P, Mitchell RM, et al. Percutaneous cholecystostomy in patients with acute cholecystitis: experience of 45 patients at a US referral center. J Am Coll Surg 2003; 197:206.
52. de Mestral C, Gomez D, Haas B, et al. Cholecystostomy: a bridge to hospital discharge but not delayed cholecystectomy. J Trauma Acute Care Surg 2013; 74:175.
53. Gurusamy KS, Rossi M, Davidson BR. Percutaneous cholecystostomy for high-risk surgical patients with acute calculous cholecystitis. Cochrane Database Syst Rev 2013; 8:CD007088.
54. Abi-Haidar Y, Sanchez V, Williams SA, Itani KM. Revisiting percutaneous cholecystostomy for acute cholecystitis based on a 10-year experience. Arch Surg 2012; 147:416.
55. Smith TJ, Manske JG, Mathiason MA, et al. Changing trends and outcomes in the use of percutaneous cholecystostomy tubes for acute cholecystitis. Ann Surg 2013; 257:1112.
56. Joseph T, Unver K, Hwang GL, et al. Percutaneous cholecystostomy for acute cholecystitis: ten-year experience. J Vasc Interv Radiol 2012; 23:83.
57. Dewhurst C, Kane RA, Mhuircheartaigh JN, et al. Complication rate of ultrasound-guided percutaneous cholecystostomy in patients with coagulopathy. AJR Am J Roentgenol 2012; 199:W753.
58. Burhenne HJ, Stoller JL. Minicholecystostomy and radiologic stone extraction in high-risk cholelithiasis patients. Preliminary experience. Am J Surg 1985; 149:632.

59. Itoi T, Sofuni A, Itokawa F, et al. Endoscopic transpapillary gallbladder drainage in patients with acute cholecystitis in whom percutaneous transhepatic approach is contraindicated or anatomically impossible (with video). Gastrointest Endosc 2008; 68:455.
60. Kjaer DW, Kruse A, Funch-Jensen P. Endoscopic gallbladder drainage of patients with acute cholecystitis. Endoscopy 2007; 39:304.
61. Karamanos E, Sivrikoz E, Beale E, et al. Effect of diabetes on outcomes in patients undergoing emergent cholecystectomy for acute cholecystitis. World J Surg 2013; 37:2257.
Treatment of acute cholecystitis
Ruptured gallbladder with biloma

Axial CT scan of the upper abdomen without intravenous but with oral contrast
demonstrates a ruptured gallbladder with a collection of bile (biloma) in the
gallbladder fossa. Note that there are multiple gallstones that are located outside of
the gallbladder. There is also a small amount of fluid around the liver.
Courtesy of J Pierre Sasson, MD. Graphic 74614 Version 3.0
Empiric antibiotic therapy for gram-negative and anaerobic pathogens
Regimen Dose (adult)*
First choice
Monotherapy with a beta-lactam/beta-lactamase inhibitor:
Ampicillin-sulbactam• 3 g IV every six hours
Piperacillin-tazobactamΔ 3.375 or 4.5 g IV every six hours
Ticarcillin-clavulanate 3.1 g IV every four hours
Combination third generation cephalosporin PLUS metronidazole:
Ceftriaxone plus 1 g IV every 24 hours or 2 g IV every 12 hours for CNS infections
Metronidazole 500 mg IV every eight hours
Alternative empiric regimens
Combination fluoroquinolone◊ PLUS metronidazole:
Ciprofloxacin or 400 mg IV every 12 hours
Levofloxacin plus 500 or 750 mg IV once daily
Metronidazole 500 mg IV every eight hours
Monotherapy with a carbapenem§:
Imipenem-cilastatin 500 mg IV every six hours
Meropenem 1 g IV every eight hours
Doripenem 500 mg IV every eight hours
Ertapenem¥ 1 g IV once daily
* Antibiotic doses should be adjusted appropriately for patients with renal insufficiency
or other dose-related consideration. • E coli resistance to Ampicillin-sulbactam is
merging in some areas; check local susceptibility data.

Δ Some clinicians use 4.5 g every eight hours for empiric therapy since the percent
time above the MIC is similar between the regimens for most pathogens; however, this
regimen is NOT recommended for nosocomial pneumonia or Pseudomonas coverage.
Please refer to UpToDate topics on the "Treatment of hospital-acquired, ventilator-
associated, and healthcare-associated pneumonia in adults" and "Treatment
of Pseudomonas aeruginosainfections". ◊ Fluoroquinolones are generally avoided in
pregnant women due to potential fetal toxicity. § Use carbapenems cautiously in
patients with immediate-type hypersensitivity to beta-lactams. ¥ Ertapenem lacks
activity against Acinetobacter and Pseudomonas and is not an appropriate choice for
severe or nosocomial infection.
American Society of Anesthesiologists (ASA) Physical Status Classification System
ASA 1 A normal healthy patient
ASA 2 A patient with mild systemic disease
ASA 3 A patient with severe systemic disease
ASA 4 A patient with severe systemic disease that is a constant threat to life
ASA 5 A moribund patient who is not expected to survive without the operation
ASA 6 A declared brain-dead patient whose organs are being removed for donor purposes
ASA Physical Status Classification System is reprinted with permission of the American
Society of Anesthesiologists, 520 N. Northwest Highway, Park Ridge, Illinois 60068-
2573.





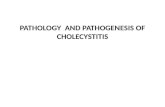









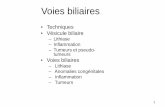
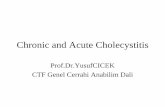
![Chronic Cholecystitis which Mimics Gallbladder Cancer: a ......malignant gallbladder disorders from benign ones [1-3]. We describe a case of chronic cholecystitis that showed focal](https://static.fdocuments.net/doc/165x107/5e9edb35d364e168286b9adc/chronic-cholecystitis-which-mimics-gallbladder-cancer-a-malignant-gallbladder.jpg)
