Acute Abdominal Pain In Children Hai Ho, M.D. Department of Family Practice.
53
Acute Abdominal Acute Abdominal Pain In Children Pain In Children Hai Ho, M.D. Hai Ho, M.D. Department of Family Department of Family Practice Practice
-
Upload
winston-richley -
Category
Documents
-
view
216 -
download
2
Transcript of Acute Abdominal Pain In Children Hai Ho, M.D. Department of Family Practice.

Acute Abdominal Pain Acute Abdominal Pain In ChildrenIn Children
Acute Abdominal Pain Acute Abdominal Pain In ChildrenIn Children
Hai Ho, M.D.Hai Ho, M.D.Department of Family PracticeDepartment of Family Practice

Pathophysiology of pain
• Visceral pain– Mechanical – stretching– Chemical – mucosa– Aching and dull, poorly localized
• Parietal pain– Sharp, well-localized

Pathophysiology of pain
• Referred pain– Somatic and visceral afferent fibers
enter the spinal close to each other
• Localization of pain– Bilateral – most GI tract, midline pain– Unilateral – kidney, ureter, ovary,
somatic

History• Usual: quality, location, severity,
associated symptoms, aggravating/alleviating factors
• Kids cannot give a history• Dangerous signs given by parents

My history: the red flags
• Duration – acute vs. chronic• Fever – inflammation, infection• Vomiting – stasis, obstruction,
dehydration• Urine output – volume depletion• Diarrhea - bloody

Examination• Usual: inspection, auscultation,
percussion, palpitation• Rectal – rectocecal appendicitis,
occult blood• Pelvic – PID• Scrotal - torsion

Tests?• Chemistry – electrolyte abnormality,
BUN/creatinine, liver function test• CBC – infection, bleeding• Plain abdominal x-ray – free air,
obstruction• Urinalysis – pyuria, hematuria• Pregnancy test
Pyloric stenosisPyloric stenosisPyloric stenosisPyloric stenosis
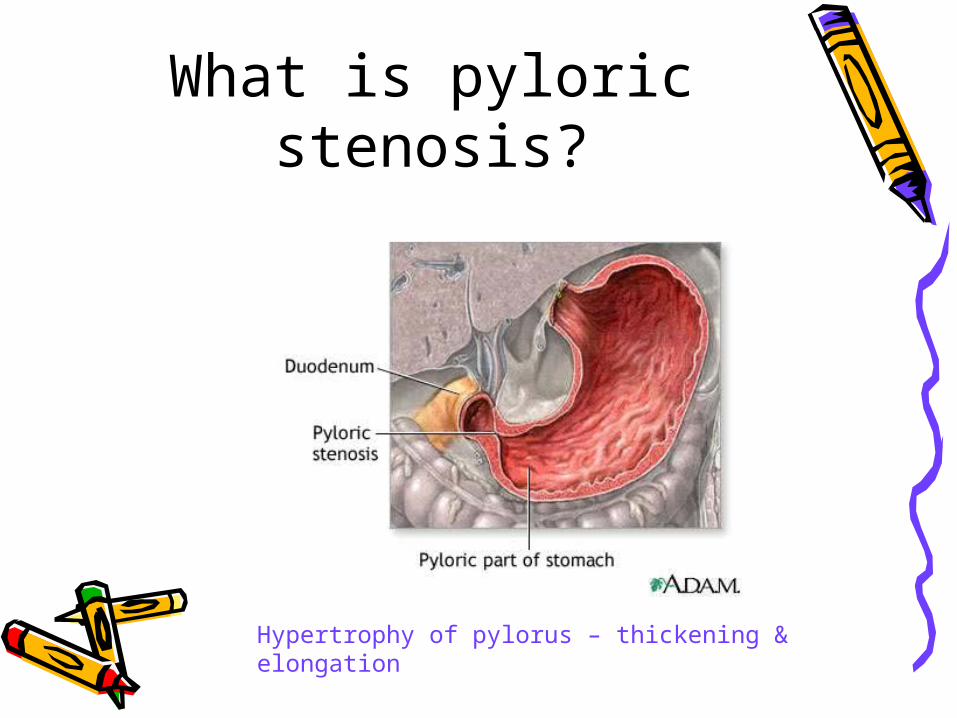
What is pyloric stenosis?
Hypertrophy of pylorus – thickening & elongation

Cause of pyloric stenosis?
• Unknown• Associations
– Abnormal muscle innervations– Erythromycin in neonates for
pertussis postexposure prophylaxis– Infant hypergastrinemia

Epidemiology• Prevelance – 3/1000• More common in white northern
European descents• Male:female = 4:1 to 6:1• Age – 1 week – 5 months but
usually 3 to 6 weeks

Clinical presentation?• Abdominal pain• Nonbilious vomiting after feeding
and with 91% having projectile emesisDistinguish pyloric stenosis from GER?

Clinical presentation?• Abdominal pain• Nonbilious vomiting after feeding
and with 91% having projectile emesis– Hungry after feeding– Weight loss– Progressive symptoms

Clinical presentations• Jaundice
– 5% of affected patients– Indirect hyperbilirubinemia due to
decreased level of glucuronyl transferase

Examination?• Abdominal
distension• Olive mass –
RUQ, after feeding

Examination• Gastric peristaltic
wave from left to right after feeding

Tests?• Chemistry• Plain abdominal x-ray• Ultrasound• UGI

Chemistry?• Decreased chloride• Elevated bicarbonate – metabolic
alkalosis• ± Hypokalemia• Elevated BUN and creatinine• ±Elevated indirect bilirubin

Abdominal x-ray
Increased gastric air or fluid suggestive gastric outlet obstruction
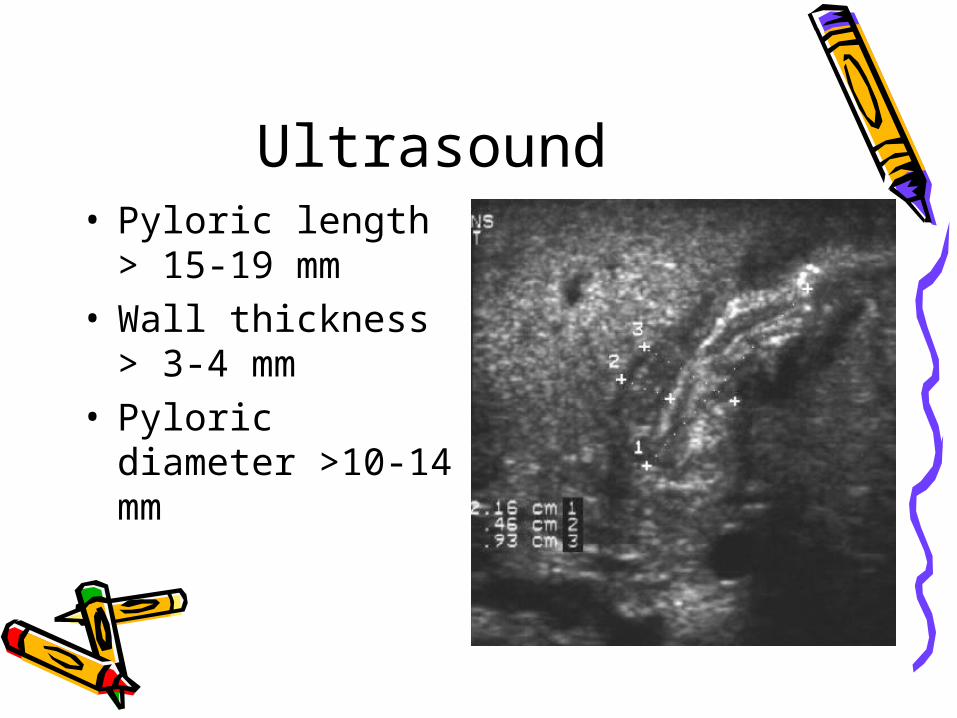
Ultrasound• Pyloric length >
15-19 mm• Wall thickness >
3-4 mm• Pyloric diameter
>10-14 mm
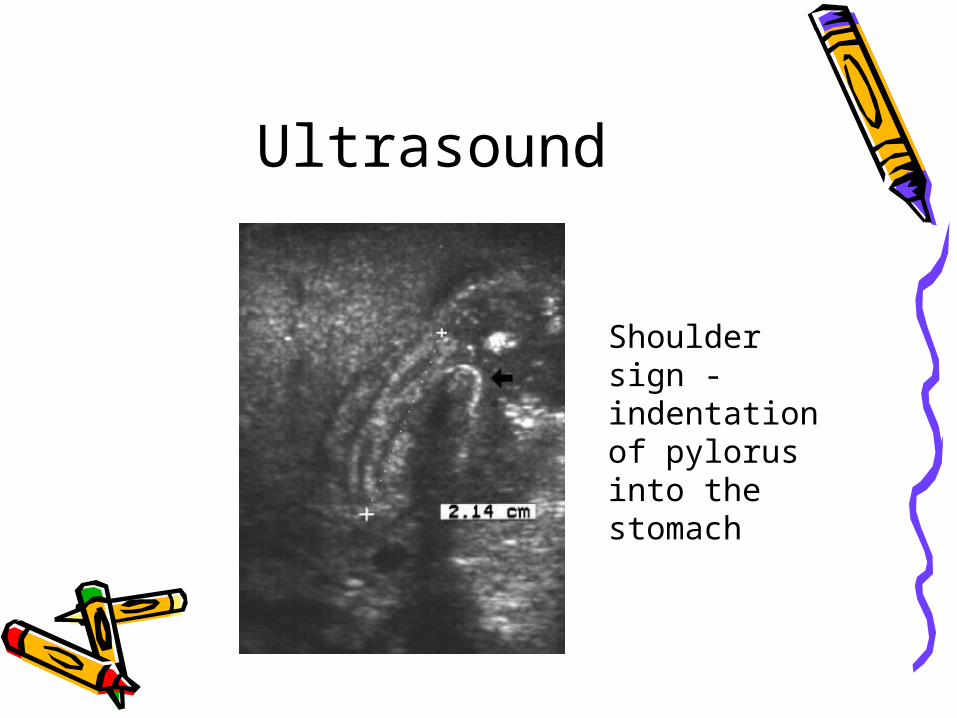
Ultrasound
Shoulder sign - indentation of pylorus into the stomach

UGI• String sign• Pyloric spasm
may mimic the string sign

Treatment?• Medical resuscitation first
– IVF hydration with potassium– Correction of alkalosis because of
postoperative apnea associated with general anesthesia
• Pyloromyotomy• Endoscopically-guided balloon dilation –
surgery is contraindicated or incomplete pyloromyotomy

Pyloromyotomy

Pyloromyotomy

Pyloromyotomy: laparoscopy

Postoperative management
• May be fed within 12-24 hours, early as 4 hours post-op in one study
• Vomiting– Not a reason to delay feeding– GER – up to 80% post-op– Consider UGI if vomiting persists > 5
days
IntussusceptionIntussusceptionIntussusceptionIntussusception

What is What is intussusception?intussusception?
What is What is intussusception?intussusception?
Invagination of intestine into itselfInvagination of intestine into itself

Pathophysiology• Proximal bowel
telescopes into distal segment, dragging along mesentery
• Compression of mesenteric vessels & lymphatics leads to edema, ischemia, mucosal bleeding, perforation, and peritonitis

Ileocolic intussusception

Causes of intussusception?
• Idiopathic – – 75% of ileocolic intussusception– More likely in children < 5

Causes of intussusception
• Leading point– Hyperplasia of Peyer patches in
terminal ileum– Structural: small bowel lymphoma,
Meckel diverticulum– Systemic: cystic fibrosis, Henoch-
Schönlein, Crohn disease

Epidemiology• Male:female – 3:2• Age –
– 3 months to 6 years with 80% < age 2
– Peak at 6-12 months
• Most common - ileocolic

Clinical manifestations?• Intermittent, severe, crampy
abdominal pain with loud cry and in curled up position
• Vomiting• Appear normal between attack• Currant-jelly stool

Currant-jelly stool
Mixture of blood and mucusFoul smelling

Tests?• Chemistry – dehydration, electrolyte
imbalance• CBC – infection• X-ray: plain film & contrast or air enema• Ultrasound• CT scan – only if other tests are negative

X-ray : plain film

X-ray• Contrast material
between the intussusceptum and the intussuscipiens is responsible for the coil-spring appearance
• Use water-soluble agent prior to barium if high risk of perforation suspected

Ultrasound
Could detect ileoileal intussusception

Treatment?• Air or contrast reduction
– Air is better than barium reduction – less perforation <1%
– Not very successful if symptoms > 24 – 48 hours or with bowel obstruction
– Successful rate – 75-90% with ileocolic intussusception
• Surgery

Reduction

Surgery• Manual reduction and end-to-end
anastomosis• Indications
– Persistent filling defects– Failed nonoperative reduction– Prolonged intussusception
Recurrence• 10%• Not necessary an indication for
surgery

Malrotation & Malrotation & VolvulusVolvulus
Malrotation & Malrotation & VolvulusVolvulus

Normal development

Midgut volvulus

Volvulus
Cecal volvulus Sigmoid volvulus

Clinical presentation?• Bilious emesis• Abdominal distension

Tests?• UGI- duodenum not crossing the
midline• Barium enema – malposition of
cecum
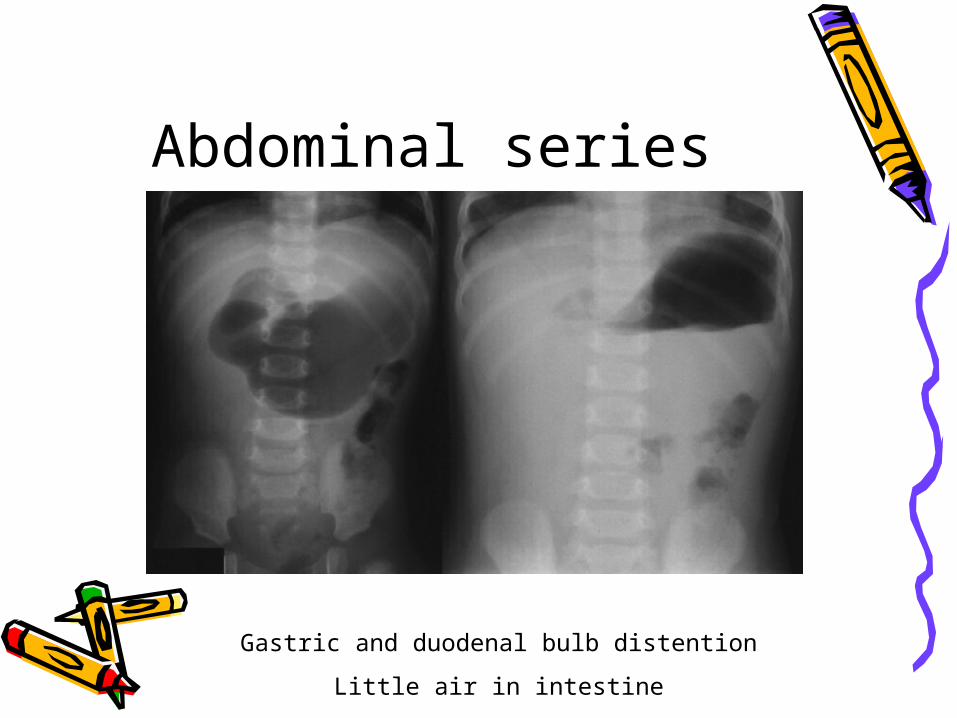
Abdominal series
Gastric and duodenal bulb distention
Little air in intestine

UGI with SBFT
Cork-screw pattern – barium flowing through restricted bowel lumen
Treatment: surgery