Active placebos versus antidepressants for depression
29
Active placebos versus antidepressants for depression (Review) Moncrieff J, Wessely S, Hardy R This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library 2009, Issue 1 http://www.thecochranelibrary.com Active placebos versus antidepressants for depression (Review) Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
Transcript of Active placebos versus antidepressants for depression

Active placebos versus antidepressants for depression(Review)
Moncrieff J, Wessely S, Hardy R
This is a reprint of a Cochrane review, prepared and maintained by The Cochrane Collaboration and published in The Cochrane Library2009, Issue 1
http://www.thecochranelibrary.com
Active placebos versus antidepressants for depression (Review)Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

T A B L E O F C O N T E N T S
1HEADER . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .1ABSTRACT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .2PLAIN LANGUAGE SUMMARY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3BACKGROUND . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3OBJECTIVES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .3METHODS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .5RESULTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .7DISCUSSION . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .9AUTHORS’ CONCLUSIONS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .9ACKNOWLEDGEMENTS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .9REFERENCES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
11CHARACTERISTICS OF STUDIES . . . . . . . . . . . . . . . . . . . . . . . . . . . . .17DATA AND ANALYSES . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Analysis 1.1. Comparison 1 antidepressant versus active placebo (all trials), Outcome 1 change in mood after treatmentperiod. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 19
Analysis 2.1. Comparison 2 subgroup analysis: in patients, Outcome 1 change in mood after treatment. . . . . . 20Analysis 3.1. Comparison 3 subgroup analysis: out patients, Outcome 1 change in mood after treatment. . . . . 20Analysis 4.1. Comparison 4 sensitivity analysis (excluding Daneman 1961), Outcome 1 change in mood after treatment. 21Analysis 5.1. Comparison 5 sensitivity analysis (excluding Daneman 1961 and Murphy et al 1984), Outcome 1 change in
mood after treatment. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 22Analysis 6.1. Comparison 6 sensitivity analysis (excluding Daneman 1961 and using higher effect size from Weintraub &
Aronson, 1963), Outcome 1 change in mood after treatment. . . . . . . . . . . . . . . . . . 23Analysis 7.1. Comparison 7 sensitivity analysis, inpatients (using higher effect size from Weintraub & Aronson, 1963),
Outcome 1 change in mood after treatment. . . . . . . . . . . . . . . . . . . . . . . . 24Analysis 8.1. Comparison 8 sensitivity analysis, outpatients (excluding Daneman 1961), Outcome 1 change in mood after
treatment. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 24Analysis 9.1. Comparison 9 sensitivty analysis (excluding trials with categorical outcomes), Outcome 1 change in mood
after treatment. . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . 25Analysis 10.1. Comparison 10 sensitivity analysis (excluding trials with estimated s.d.’s), Outcome 1 change in mood. 26
26WHAT’S NEW . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .26HISTORY . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .26CONTRIBUTIONS OF AUTHORS . . . . . . . . . . . . . . . . . . . . . . . . . . . . .27DECLARATIONS OF INTEREST . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .27SOURCES OF SUPPORT . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .27INDEX TERMS . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . . .
iActive placebos versus antidepressants for depression (Review)Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

[Intervention Review]
Active placebos versus antidepressants for depression
Joanna Moncrieff1, Simon Wessely2, Rebecca Hardy3
1University College London, Warley Hospital, Essex, UK. 2Academic Dept of Psychological Medicine, Guy’s, King’s, & St Thomas,School of Medicine & Institute of Psychiatry, 103 Denmark Hill, London, UK. 3Department of Epidemiology and Public Health,MRC National Survey of Health and Development, London, UK
Contact address: Joanna Moncrieff, University College London, Warley Hospital, Mascalls Lane, Brentwood, Essex, CM14 4TU, [email protected]. (Editorial group: Cochrane Depression, Anxiety and Neurosis Group.)
Cochrane Database of Systematic Reviews, Issue 1, 2009 (Status in this issue: Edited)Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.DOI: 10.1002/14651858.CD003012.pub2This version first published online: 26 January 2004 in Issue 1, 2004. Re-published online with edits: 21 January 2009 in Issue 1,2009.Last assessed as up-to-date: 11 February 2008. (Help document - Dates and Statuses explained)
This record should be cited as: Moncrieff J, Wessely S, Hardy R. Active placebos versus antidepressants for depression. CochraneDatabase of Systematic Reviews 2004, Issue 1. Art. No.: CD003012. DOI: 10.1002/14651858.CD003012.pub2.
A B S T R A C T
Background
Although there is a consensus that antidepressants are effective in depression, placebo effects are also thought to be substantial. Side effectsof antidepressants may reveal the identity of medication to participants or investigators and thus may bias the results of conventionaltrials using inert placebos. Using an ’active’ placebo which mimics some of the side effects of antidepressants may help to counteractthis potential bias.
Objectives
To investigate the efficacy of antidepressants when compared with ’active’ placebos.
Search strategy
CCDANCTR-Studies and CCDANCTR-References were searched on 12/2/2008. Reference lists from relavant articles and textbookswere searched.
Selection criteria
Randomised and quasi randomised controlled trials comparing antidepressants with active placebos in people with depression.
Data collection and analysis
Since many different outcome measures were used a standard measure of effect was calculated for each trial. A subgroup analysis ofinpatient and outpatient trials was conducted. Two reviewers independently assessed whether each trial met inclusion criteria.
Main results
Nine studies involving 751 partcipants were included. Two of them produced effect sizes which showed a consistent and statisticallysignificant difference in favour of the active drug. Combining all studies produced a pooled estimate of effect of 0.39 standard deviations(confidence interval, 0.24 to 0.54) in favour of the antidepressant measured by improvement in mood. There was high heterogeneitydue to one strongly positive trial. Sensitivity analysis omitting this trial reduced the pooled effect to 0.17 (0.00 to 0.34). The pooledeffect for inpatient and outpatient trials was highly sensitive to decisions about which combination of data was included but inpatienttrials produced the lowest effects.
1Active placebos versus antidepressants for depression (Review)Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Authors’ conclusions
The more conservative estimates from the present analysis found that differences between antidepressants and active placebos weresmall. This suggests that unblinding effects may inflate the efficacy of antidepressants in trials using inert placebos. Further researchinto unblinding is warranted.
P L A I N L A N G U A G E S U M M A R Y
Tricyclic antidepressants compared with active placebos for depression
This review examined trials which compared antidepressants with ’active’ placebos, that is placebos containing active substances whichmimic side effects of antidepressants. Small differences were found in favour of antidepressants in terms of improvements in mood.This suggests that the effects of antidepressants may generally be overestimated and their placebo effects may be underestimated.
2Active placebos versus antidepressants for depression (Review)Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

B A C K G R O U N D
Since the 1970’s there has been a consensus, based predominantlyon the results of clinical trials, that tricyclic antidepressants (TCAs)have a specific therapeutic effect in depression. However, an ex-amination of the literature reveals that the evidence from suchtrials is not consistent. Although most reviews find that the drugis significantly superior to a placebo in a majority cases, the de-gree of superiority is generally not large and between 22% and73% of studies or comparisons fail to find a significant difference(Cole 1964; Davis 1965; Klerman 1967; McNair 1974; Morris1974; Rogers 1975). In addition, comprehensive analyses of earlyantidepressant research revealed that the methodology employedinfluenced the result. In particular, the absence of random alloca-tion or blinding increased the apparent effect size (Smith 1969,Wechsler 1965), a finding which has been noted more recently inother areas of medicine (Schulz 1995, Schulz 1996).
A further methodological concern is the possibility of bias due tounblinding effects. Greenberg 1994a have pointed out that thedifferent physiological experiences resulting from the ingestion ofan active drug and an inert placebo may lead patients and assessorsto suspect the identify of medication. This may introduce bias dueto different expectations of treatment. Several studies have foundthat drugs, including antidepressants, can be distinguished fromplacebo more readily than would be predicted by chance (White1992). There are various possible explanations for this unblind-ing effect and its possible association with outcome. Unblindingmay occur due to the therapeutic effect of the medication or mayoccur due to side effects but correlate with therapeutic effect. Inboth these circumstances the therapeutic effect would determinethe outcome and how it was measured. However, another sugges-tion is that side effects may enhance the placebo effect in patientstaking active medication (Thomson 1982). A further possibility isthat the occurrence of side effects may unblind raters which mayproduce biased ratings. In these latter situations, outcome may bedetermined by factors other than the specific effect of the medi-cation, that is results may be biased.
There is some evidence that unblinding effects may be associatedwith outcome ratings in the absence of evidence that the drugis effective. A drug trial with problem drinkers found that per-ception of medication group predicted outcome rating, althoughthere was no evidence the drug was effective (Toneatto 1992) andsimilar findings were reported in a trial of antipsychotic drugs (Engelhardt 1969). In addition side effects have been shown to cor-relate significantly with patient and clinician outcome depressionratings in a meta-analysis of placebo controlled trials of fluoxetine(Greenberg 1994b).
Some investigators have addressed this difficulty by using place-bos containing active substances. Small doses of drugs with an-ticholinergic actions have typically been employed to mimic sideeffects of TCAs in placebo preparations. Thomson 1982 reviewed
some of these studies and found that they were more likely to havea negative outcome than studies using inert placebos. It would bedifficult to conduct a trial using an active placebo at present be-cause many clinicians would feel it was unethical. Meta-analysis ofprevious active placebo controlled trials therefore provides an op-portunity to investigate the efficacy of antidepressants under con-ditions of greater “blindness”. In addition, by combining results ofseveral small trials with various groups of depressed patients meta-analysis should increase the power to detect an effect and balancethe idiosyncracies of individual trials.
Depression is the commonest psychiatric condition and antide-pressant drug treatment accounted for 1.9% of all NHS drug costsin the early 1990s (Henry 1993). This proportion is likely to haveincreased since then due to the escalation in prescribing of thenew SSRI drugs (Donoghue 1996). Antidepressants are lucrativeproducts for the pharmaceutical industry which therefore devotesmuch research to the development of new agents. These new drugsare frequently expensive and represent a potentially significant andescalating drain on health service resources unless properly evalu-ated. Since new drugs have been evaluated by comparison with thegold standard of TCAs the results of this review also have implica-tions for evaluation of the role of newer drugs such as the SSRIs.
O B J E C T I V E S
To investigate the efficacy of antidepressants when compared with’active’ placebos for treating people with depression. An activeplacebo is a placebo tablet which contains a drug which is notthought to have a specific effect in the disorder being treated andwhich is employed to mimic the effect of taking an active sub-stance.
M E T H O D S
Criteria for considering studies for this review
Types of studies
Randomised and quasi randomised trials which were conducteddouble blind.
Types of participants
Participants of either sex of all age groups whose primary diagnosiswas of a depressive disorder. A concurrent diagnosis of anotherpsychiatric or medical disorder was not an exclusion criteria.
Types of interventions
Interventions included any currently used antidepressant drug orantidepressants which have been withdrawn for reasons other thanlack of efficacy. To be considered trials also had to use a placebocontaining some active substance employed to mimic the nonspecific effects of taking an active drug.
3Active placebos versus antidepressants for depression (Review)Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Types of outcome measures
Trials were included if they used some measurement of depressionas an outcome variable. Any type of measure was admissable (sincemost of the trials found were conducted before the developmentof outcome measures in current use).
Search methods for identification of studies
1. The following databases were searched with the following strate-giesCCDANCTR-Studies (searched on 12/2/2008)Intervention = “Active Placebo”.CCDANCTR-References (searched on 12/2/2008)Free text = “active placebo*”
2. Reference lists of relevant papers were scanned for publishedreports and citations of unpublished research.3. Book chapters on treatment of depression were scanned fordescriptions of trials.
Data collection and analysis
Two reviewers (JM & RH) assessed studies independently to de-cide whether they met inclusion criteria.
Data extractionMany different outcomes measures were used, and it was assumedthat they all measured an underlying construct which we havecalled mood. Standardised mean differences (the difference be-tween the group means divided by the combined standard devia-tion) were used to calculate a standard measure of effect for eachtrial. Change in mood at the end of treatment was defined as theoutcome of interest. In some studies this information was pre-sented directly for the outcome scale used. In one study (Murphy1984) it was calculated by subtracting pre-treatment scores frompost-treatment scores. In this case the standard deviation was es-timated from another study using the same outcome measure (Rush 1977). In other cases direct measures of improvement orchange were used, such as categorical ratings of improvement oruse of measures such as the Global Clinical Improvement Scale (Friedman 1975). Observer rated measures were selected in pref-erence to patient rated ones as these were employed most consis-tently. Where there was a choice, the measure indicated by theauthors as the one of principle importance was selected. If no prin-ciple measure was specified, priority was given to instruments thathave been widely used and subject to reliability testing, if avail-able data permitted. Where different measures or ratings withinthe same study disagreed substantially, as occurred in one trial (Weintraub 1963) separate effect sizes were calculated and used inthe analysis. Intention to treat data were used where possible andin one trial, with a large number of early withdrawals, this wascalculated by assigning the poorest possible outcome to dropouts(Daneman 1961). Results consisting only of categorical ratings
of degree of improvement were weighted (e.g. much improved=3, moderate improvement=2, no change=1, worse=0) and meanscores and standard deviations obtained as described in a previousmeta-analysis in this area (QAP 1983).Requests were sent to authors of studies for more complete dataand statistics such as standard deviations. However, unsurprisinglynone of the data was still available since studies were too old.Since the number of studies was small, and estimation and ap-proximation was required to produce compatible outcomes, nofurther analyses were attempted.Statistical proceduresStandardised mean differences, or ’effect sizes’ for the individualtrials were calculated by subtracting the mean score in the placebogroup from that of the group allocated to antidepressants and di-viding the result by the pooled standard deviation. A number ofpapers did not report standard deviations and so estimates wereobtained from other trials using the same outcome measures andsimilar patient groups. In one study (Uhlenhuth 1964) patientsallocated to the antidepressant were more severely depressed atbaseline than the placebo group. An effect size adjusted for base-line values was therefore computed using analysis of variance. Thisadjusted value could not be used in the MetaView analyses but wasused for the purpose of correlation analysis with quality scores.Results from individual trials were combined using the MetaView(version 4.0) procedure for standardised mean differences. A fixedeffects model was used, because this is the simplest model andthere is no consensus as to whether fixed or random effects modelsare preferable in given situations. In addition, it was felt that het-erogeneity between studies should be identified and explored andnot incorporated into the effect estimate as would be the case witha random effects model. Heterogeneity was examined visually andstatistically.A subgroup analysis of inpatients and outpatients was planned apriori. Sensitivity analyses were conducted to explore the assump-tions made and the consistency of the data. In addition wheretwo or more measures in one trial yielded substantially differentoutcomes, sensitivity analyses were done using the different effectsizes calculated for each measure.Quality assessmentThere is no consensus on what constitutes quality in randomisedcontrolled trials in psychiatry. Two assessments were conducted forthis review. Firstly a qualitative evaluation of the quality of studieswas undertaken focusing on allocation, blinding and inclusion ofsubjects in the analysis. These three aspects of trial design havebeen found to be the principle determinants of quality in one in-vestigation of trial quality (Jadad 1996). Secondly a more detailedand quantitative examination of trial quality was conducted usingan instrument for the assessment of the quality of interventiontrials in psychiatry (Moncrieff 2001). This consists of ratings of23 aspects of trial quality encompassing issues relating to both in-ternal validity or the control of bias, and external validity or gen-eralisability. Each item was scored between zero and two for each
4Active placebos versus antidepressants for depression (Review)Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
trial giving a maximum score of 46.
R E S U L T S
Description of studies
See: Characteristics of included studies; Characteristics of excludedstudies.The following studies were identified that satisfied all inclusioncriteria. Further details are provided in the Table of Characteristics.Daneman 1961A parallel group trial of outpatients comparing imipramine withan atropine placebo. It was of variable duration with assessmentsmade at one and two months.Weintraub 1963A parallel group study with inpatients comparing imipramine andan atropine placebo over 4 weeks.Wilson 1963A factorial study evaluating ECT and imipramine compared withsimulated ECT and an atropine placebo with inpatients lasting 5weeks.Uhlenhuth 1964Crossover trial of 4 weeks duration with outpatients for whichdata is reported as for a parallel group trial at 2 weeks. Comparedimipramine with an atropine placebo.Hollister 1964Parallel three group trial comparing amitiptyline, imipramine andan atropine placebo in inpatient veterans over 3 weeks.Friedman 1966A parallel group trial with inpatients lasting 3 weeks comparingimipramine and an atropine placebo.Hussain 1970A parallel three group study of patients from “psychiatric prac-tice” comparing amitriptyline, an amitryptiline and perphenazinecombination tablet and an atropine placebo.Friedman 1975A parallel group factorial study with married outpatients evaluat-ing marital therapy and amitriptyline using an atropine placeboover 12 weeks.Murphy, 1984Murphy, 1984Parallel group trial of cognitive therapy and nortriptylene in out-patients with 12 weeks of treatment. Groups allocated to nor-triptylene plus cognitive therapy and cognitive therapy plus activeplacebo containing atropine and phenobarbital sodium were usedin the current analysis.Three other RCTs comparing antidepressants with active placeboswere found. These were not included in the analysis because thesubjects were not suffereing from a depressive disorder. Furtherdetails are given in the table of characteristics of excluded studies.Outcome measures:
(See also table of Included studies).Only two of the trials used the Hamilton Rating Scale for De-pression (HRSD) (Wilson 1963, Murphy 1984). Murphy 1984also used the Beck Depression Inventory. Another study used amodified version but did not report its overall ratings (Friedman1975). Hollister 1964 used a Manifest Depression scale appendedto the Inpatient Multidimensional Psychiatric Inventory (IMPS)which was constructed using ratings of a panel of experts and sub-jected to factor analysis to explore internal validity (Overall 1962).The authors had used this scale in several previous studies. Theyalso used various scales derived from the Minnesota Multipha-sic Personality Inventory (MMPI). Two studies (Friedman 1966,Friedman 1975) used a Global Clinical Improvement Scale whichthe authors say was described by DiMascio, but no reference wasgiven or could be traced. However, this scale appears to be similarto the much used Clinical Global Impressions Scale which wascertainly in widespread use before it was officially described byGuy 1976. Both these studies used several other outcome mea-sures but did not report them fully. Uhlenhuth 1964 describe thedevelopment of a scale called the Total Distress Score. This wasconstructed by rating symptoms from a commonly used symptomchecklist (Frank 1957) according to the degree of distress the pa-tient was suffering. Forty two symptoms relevant to the evaluationof depression were then selected via the agreement of a panel ofeight senior psychiatrists acting independently. They also used ascale called the Morale Loss Scale derived from the MMPI. Otherstudies only used or reported ratings of improvement in variousnumbers of categories.
Risk of bias in included studies
Quality of studiesThe simple overview of trial quality revealed some strengths de-spite the age of most of the studies. Inclusion criteria ensuredthat they were conducted double blind and had taken measures tostrengthen this procedure by using an active placebo. They all usedrandom allocation and although only two did an explicit intentionto treat analysis (Friedman 1975; Murphy 1984), all but one (Daneman 1961) of the others documented only small numbers ofearly withdrawals. Two studies tested the integrity of the blind inassessors by asking for guesses of medication group and althoughguesses were more accurate than would be predicted by chance,the effect was not statistically significant in either trial (Uhlenhuth1964; Weintraub 1963). However, in the Weintraub 1963 trial itwas found that both raters assessed those they guessed to be on theactive drug as more improved. One other trial reported that sideeffects had been more prominent in patients on antidepressants (Hollister 1964), indicating the possibility that residual unblindingeffects may have occurred despite the use of active placebos.In the more extensive procedure using the quality rating instru-ment the mean score of the nine studies was 20 (maximum possiblescore 46, s.d. 6.71). Correlation analysis demonstrated an inverseassociation between quality score and effect size with a correlation
5Active placebos versus antidepressants for depression (Review)Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

coefficient of -0.605 (p=0.09) and a positive association betweenquality score and later year of publication (r=0.414, p=0.3). How-ever, the power of correlation analysis was limited by the smallnumber of studies and hence neither of these associations reachedstatistical significance. Graphical inspection of the relationship be-tween effect size and quality revealed an approximately linear re-lationship with one outlying study (Daneman 1961). Excludingthis study resulted in a correlation coefficient of -0.775 for theassociation in the eight remaining studies which was statisticallysignificant at the 5% level (p=0.02).
Effects of interventions
Individual studiesNine trials, involving 751 participants were included. All com-pared TCAs with active placebos containing atropine. A mini-mum dose of 100mg of amitriptyline or equivalent was used in allstudies except one where the dose used was not stated (Hussain1970). The effect sizes (SMDs) calculated for each study in unitsof standard deviation are listed below according to a fixed effectsmodel.Daneman 1961This trial showed a positive and significant difference favouringimipramine over active placebo.SMD = 1.1 (95% confidence interval, C. I., 0.8 to 1.4). Calculatedfrom scored categories of response to treatment. Based on 101patients allocated to imipramine and 94 to placebo.Uhlenhuth 1964This trial showed no difference between imipramine and placebowhen the results were adjusted for substantial differences in base-line levels of depression.Unadjusted SMD = 0.60 (95% C.I. 0.02, 1.2). Calculated onTotal Distress Score pre minus post treatment scores (individualpatient data was provided and so exact scores could be computed).Based on 22 patients allocated to imipramine and 20 to placebo.SMD adjusted for baseline values = 0.35 (95% C.I. -0.25 to 0.96).(Not shown in metaview. Calculated using multiple regressionanalysis).Weintraub 1963Results for two different raters were inconsistent with one findinga significant advantage for imipramine over placebo and the otherfinding no significant difference.SMD for hospital director = 0.14 (95% C.I. -0.34 to 0.62). Basedon 36 patients allocated to imipramine and 31 to placebo.SMD for ward doctor = 0.63 (95% C.I. 0.15 to 1.11). Based on36 patients allocated to imipramine and 32 to placebo.Calculated from scored categories of “improvement”Wilson 1963No difference between imipramine and placebo.Effect size = -0.26 (95% C.I. -1.10 to 0.58). Calculated fromchange in Hamilton Rating Scale for Depression (HRSD) scoresbetween pre and post treatment measurements. Based on 10 pa-tients allocated to imipramine and 12 to placebo.
Hollister 1964No difference between two tricyclic antidepressants (imipramineand amitriptyline) and placebo.SMD = 0.19 (95% C.I. -0.24 to 0.63). Calculated from changein Inpatient Multi-dimensional Psychiatric Scale (IMPS) betweenpre and post treatment measures. Based on 62 patients allocated toone of the antidepressants and 31 to placebo. Standard deviationestimated from Hollister 1963.Friedman 1966No difference between imipramine and placebo.SMD = 0.13 (95% C.I. -0.37 to 0.64)Calculated from Global Clinical Improvement scale. Based on36 patients allocated to imipramine and 26 to placebo. Standarddeviation estimated from results at 4 weeks in trial by Friedman1975.Hussain 1970The effect size in this trial indicated that antidepressants weresuperior to placebo, although the authors found no significantdifference using a categorical analysis.SMD = 0.79 (95% C.I. 0.09 to 1.5)Calculated from scored categories of improvement.Based on 15 patients allocated to imipramine and 17 to placebo.Friedman 1975No difference between amitriptyline and placebo.SMD = 0.14 (95% C.I. -0.14 to 0.42).Calculated from Global Clinical Improvement scale. Based on 98patients in each group.Murphy 1984No difference between nortriptyline and placebo.Effect size = -0.36 (95% C.I. -1.0 to 0.28)Calculated from change in HRSD score between pre and posttreatment.Based on 22 patients allocated to nortriptyline and 17 to placebo.Standard deviation estimated from Rush 1977.Ratings by the two observers in the trial of Weintraub 1963yielded discrepant estimates of effect size, and pooled meta-anal-ysis was conducted separately using both estimates. In three trials(Friedman 1966; Hollister 1964; Murphy 1984) standard devia-tions for the relevant measures were not reported and estimateswere taken from studies by the same authors or, in one case, fromthe study that the authors referenced as their blueprint (Rush1977). Effect sizes calculated in this way were consistent with theresults of individual measures reported in the studies and withthe authors interpretations of their findings. Two trials showed aconsistent and statistically significant difference favouring the an-tidepressant drug over placebo (Daneman 1961; Hussain 1970),although only one of these authors (Daneman 1961) concludedthat an effect had been demonstrated. Adjustment for baseline dis-crepancies in the severity of depressive symptoms made a markeddifference in the trial by Uhlenhuth 1964. Post treatment scoresin this study were virtually identical for the intervention and con-trol group, implying that the greater change score in the group
6Active placebos versus antidepressants for depression (Review)Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

allocated to antidepressants may partly represent regression to themean.
Combined analysisThe distribution of the effect sizes calculated fitted a normal distri-bution. Tests of skewness and kurtosis were not significant (skew-ness=0.39, p=0.50; kurtosis 2.19, p=0.89) (Stata). Therefore para-metric methods for combining trial statistics could be used.Combining effect sizes from all nine trials, using the more conser-vative estimate from Weintraub 1963 (rating by hospital director),yielded a pooled estimate of 0.39 (95% C.I. 0.24 to 0.54). This in-dicates a highly significant difference between antidepressants andplacebos. However, a high degree of heterogeneity was revealed(X2 = 36.3, degrees of freedom, d.f. 8, p<0.001) . Inspection of theresults indicated that the source of heterogeneity was likely to beone trial by Daneman 1961, with other results being reasonablyconsistent. This trial produced a large positive effect size of 1.1(95% C.I. 0.8 to 1.4) despite assuming a poor outcome in subjectslost to follow up. It yielded an even larger estimate of 2.80 (95%C.I. 2.41 to 3.19) when these assumptions were not made and theimprovement rate in the placebo group was unusually poor (9% ateight weeks). Closer inspection revealed the possibility that ratingof response was not blind and that selective reporting of outcomeshad occurred. It was therefore decided to repeat the analysis ex-cluding this study. This reduced heterogeneity to a non significantlevel (X2= 8.51, d.f. 7, p=0.29). The pooled effect size for the eightremaining trials was 0.17 (95% C.I. 0.00 to 0.34).Repeating these analyses with the higher estimate from the trialby Weintraub 1963 marginally increased the size of the overallestimates. In particular it increased the pooled effect for the eighttrials excluding Daneman 1961 to 0.23 (95% C.I. 0.06 to 0.40).It did not influence heterogeneity findings.Excluding the study by Murphy 1984, on the grounds that all par-ticipants received cognitive therapy as well as medication, also in-creased pooled effects a little without affecting heterogeneity. Thecombined effect size for seven trials excluding Daneman 1961andMurphy 1984 was 0.21 (95% C.I. 0.03, 0.38).Sensitivity analysis was performed excluding trials in which cat-egorical data was transformed into continuous data. This analy-sis revealed a low and non signifcant estimate of effect (SMD=0.13, 95% C.I. -0.06 to 0.31), but it was little different fromthe estimate of effect obtained by excluding the Daneman 1961trial alone. Sensitivity analysis was also performed excluding trialsin which estimated standard deviations had been used. This pro-duced a higher estimate of effect of 0.51 (0.33, 0.68) based on thesix remaining trials and 0.22 (95% C.I. 0.02, 0.43) on the fiveother trials excluding Daneman 1961.Inpatient trials predominantly involved patients with endogenousor severe depression. The majority of subjects in outpatient trialswere diagnosed as having neurotic or moderate depression. Sub-group analysis in inpatients produced a small and non significantpooled effect size of 0.12 (95% C.I. -0.14 to 0.38) using the lower
of the two estimates from Weintraub 1963. Heterogeneity waslow and non significant. Using the higher estimate from this trialincreased the combined effect to 0.25 (95% C.I. 0.00, 0.51) withno discernable effect on heterogeneity.Combined analysis with all five outpatient trials produced an effectsize of 0.52 (95% C.I. 0.34, 0.70). Again heterogeneity was high(X2=29.1, p<0.001). Excluding Daneman 1961reduced the het-erogeneity to a non statistically significant level (X2=7.38, p=0.06)and reduced the effect size to 0.20 (95% C.I. -0.02, 0.43).
D I S C U S S I O N
Limitations of review.
This study demonstrates the difficulty of performing meta-anal-ysis with small numbers of trials because of the sensitivity of theresults to the inclusion or exclusion of individual studies. For thisreason, decisions about which studies to include in the analysisand which estimates of effect to use should be explicit, and resultsof sensitivity analyses should be presented. The exclusion of thelarge trial by Daneman 1961, which was the source of significantheterogeneity, had the most substantial impact on this meta-anal-ysis. It is generally recommended that the source of heterogeneityshould be investigated rather than proceeding with a combinedanalysis of discrepant results (Abramson 1990). In this case it wasapparent that the results of this study were inconsistent with theother studies in this review as well as with well known trials usinginert placebos (MRC 1965).
In addition, calculating effect size was rarely straight forward, in-volving conversion of categorical ratings to continuous data andthe use of estimated standard deviations in some cases. Sensitivityanalysis excluding trials in which categorical data was transformedinto continuous data, was little different from the estimate of effectobtained by excluding the Daneman 1961 trial alone. Sensitivityanalysis excluding trials in which estimated standard deviationshad been used produced slightly higher estimates of effect, sinceit involved excluding two trials in which antidepressants did notperform better than placebo.
A further problem is that data on change may be skewed and thecalculation of effect size is based on parametric statistics. Thereis no research into how robust these methods are to skewed data.In the trial by Uhlenhuth 1964 in which individual data wereavailable the data did not deviate significantly from the normaldistribution (X2 for combined skewness and kurtosis was 3.65,p=0.16) (Stata). However it was apparent that data which had beentransformed from categorical ratings were skewed but sensitivityanalysis ommitting these trials did not change the results.
Such problems are endemic to meta-analysis in the absence of stan-dard forms of measurement and reporting and are especially preva-lent in older trials. They limit the accuracy of the results. How-
7Active placebos versus antidepressants for depression (Review)Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

ever, the general interpretation of the results should be consistentwith a more qualitative review of the individual studies included.The effect sizes computed were all consistent with indivudal studyresults and authors’ conclusions.
However, the results of a meta-analysis are only as good as the trialson which it is based. Most trials in this review were conductedbefore operationalised diagnostic criteria were available and whenstandardised outcome measures were still being developed. Theoutcome measures used were a mixture which included unvali-dated categorical ratings of improvement as well as standardisedinstruments such as the HRSD and measures developed by theauthors of various trials using methods they describe. A globalimprovement scale similar to the widely used CGI was used in 2papers. It was necessary to use this mixture of outcome measuresin order to use data from all the trials. However, the use of stan-dardised measures is not a panacea. Establishing validity in a con-dition such as depression is a complex task and existing measureshave only been shown to correlate with each other and not withany objective measure of depression. In addition research into thereliability and comparative validity of current measures such asthe HRSD has been criticised for using concurrent interviews andinappropriate statistics. When these latter issues are addressed es-timates of reliability and validity are much lower (Cicchetti 1983).
The short duration of most of the studies should also be noted,which may make differences between drugs and placebos moredifficult to detect. However, all studies used random allocationand by virtue of the inclusion criteria they had all taken measuresto strengthen the double blind by use of an active placebo. Also,numbers of exclusions after allocation were small in all but onestudy. Thus, the studies had all addressed some of the most im-portant aspects of quality whose influence has only recently beenwidely publicised.
An alternative explanation of the present findings is that atropineitself has antidepressant properties and hence acts not as a placeboin these trials, but as a specific therapeutic agent. Although someopen studies have suggested that this may be the case (Kasper1981), this was not confirmed in a randomised controlled trialcomparing centrally and peripherally acting anticholinergic agentswhich found no difference in their effect on mood (Gillin 1995).
Summary of results.
The limitations of the quantitative analysis and of the individualtrials themselves mean that interpretation of results must remaintentative.
All except one of the individual studies were fairly consistent infinding a small, and in most cases non significant, difference be-tween antidepressant drugs and an active atropine placebo. Thepooled estimates of effect varied according to which combinationof studies was used. The most conservative estimate was 0.17 stan-dard deviations and the least conservative was 0.39. Assuming a
normal response to treatment, these estimates indicate that theaverage score of people taking antidepressant drugs exceeds thatof between 57% and 65% of people taking placebo. Alternatively,using the standard deviations reported by Friedman 1975, the es-timates would translate into a difference of between 0.4 and 0.8on the 6 point Clinical Global Improvement Scale. The more con-servative estimates might be preferred because of the reasons givenfor the exclusion of the trial by Daneman 1961, and because thefindings about unblinding and rating bias in the trial by Weintraub1963. In addition, results will have been inflated somewhat be-cause it was not possible to use a measure of effect adjusted for thediscrepancy in baseline values in the trial by Uhlenhuth 1964 inthe pooled analysis. The large unadjusted effect in this trial mayrepresent partly a regression to the mean effect, since both groupsended the trial with the same levels of depression. There was alsoevidence of residual unblinding in some of the trials in this review,and the possibility of publication bias may also suggest a moreconservative interpretation of results is appropriate. However, thelarger estimates of effect are more consistent with other estimates(see below) of the effects of antidepressant drugs.
Subgroup analyses, based on place of care, which was associatedwith severity of depression, were highly sensitive to decisions aboutwhich trials and outcomes to include. The small numbers involvedalso limited power and accuracy. Conservative estimates showedsmall and non significant effects in both subgroups.
Quality analysis is in line with previous findings which suggest thatpoor methodology may inflate the apparent effects of treatmentin antidepressant trials (Smith 1969; Wechsler 1965).
Comparisons with other meta-analyses.
Previous meta-analyses of drug treatment of depression have pro-duced diverse estimates of effect size. The largest estimates of 0.81(95% C.I. 0.65 to 0.97) for endogenous depression and 0.55 (95%C.I. 0.43 to 0.67) for neurotic depression were found in the QAP1983. Other general samples of trials produced effect sizes of 0.4 (Smith 1980) and 0.67 (Steinbrueck 1983). The smallest estimatecame from a review of trials comparing a new antidepressant withboth a standard drug and a placebo. It was hypothesised that thisdesign would reduce the influence of expectation on the perfor-mance of the standard drug. “Older” antidepressants yielded acombined effect size of 0.25 (p<0.001) using observer rated mea-sures and 0.06 (not statistically significant) with patient ratings (Greenberg 1992).
The more conservative estimates from the present study are similarin magnitude to the pooled observer rated outcomes in the reviewby Greenberg 1992, which would be consistent with the hypoth-esis that effect sizes in antidepressant trials are inflated by expecta-tions of participants, including researchers. However, confidenceintervals were wide and the less conservative estimates, which in-cluded the Daneman 1961 trial, were closer to combined resultsobtained from unselected analyses of antidepressant trials.
8Active placebos versus antidepressants for depression (Review)Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

A U T H O R S ’ C O N C L U S I O N S
Implications for practice
It is difficult to draw firm conclusions from this review because ofthe small number of trials and the sensitivity of the pooled analysisto inclusion and exclusion of trials with discrepant results.
However, inspection of effect sizes from individual trials revealedthat the majority of trials found only small differences betweenantidepressants and active placebos. Excluding the trial which wasthe source of heterogeneity resulted in a relatively small pooledeffect. It may therefore be the case that unblinding effects have animpact on the results of antidepressant trials using inert placebosand help to inflate the results of other unselective meta-analyses.The specific effects of antidepressants may therefore be smallerthan is generally believed, with the placebo effect accounting formore of the clinical improvement observed than is already knownto be the case. This would imply that the risks of antidepressanttherapy are less likely to be outweighed by their benefits than iscurrently held to be the case. It might therefore be appropriateto reassess the current pattern of widespread prescribing of an-tidepressants. However, the age and quality of the studies and the
problems of meta-analysis in this situation should not be disre-garded and mean that these conclusions must remain tentative.
Implications for research
Further research into unblinding and its impact on antidepressanttrials is desirable to clarify this area of concern. Research into safeactive placebos may enable further trials with active placebos to beconducted. Given the extent of their current use, it would be par-ticularly interesting to be able to compare the new generation ofantidepressants such as the SSRIs to active placbos. In the mean-time, testing the integrity of the double-blind in trials using inertplacebos provides some idea of the extent to which unblindingoccurs. This procedure is recommended for future clinical trials.
A C K N O W L E D G E M E N T S
South Thames NHS executive for funding the review as part of aresearch training fellowship.
Hugh McGuire, CCDAN trials search co-ordinator, for perform-ing the electronic searches.
R E F E R E N C E S
References to studies included in this review
Daneman 1961 {published data only}Daneman EA. Imipramine in office management of depressive reac-tions. Diseases of the Nervous System 1961;22:213–7.
Friedman 1966 {published data only}Friedman AS, Granick S, Cohen HW, Cowitz B. Imipramine(tofranil) vs. placebo in hospitalised psychotic depressives. Journalof Psychiatric Research 1966;4(1):13–36.
Friedman 1975 {published data only}Friedman AS. Interaction of drug therapy with marital therapy indepressive patients. Archives of General Psychiatry 1975;32(5):619–37.
Hollister 1964 {published data only}Hollister LE, Overall JE, Johnson M, Pennington V, Katz G, SheltonJ. Controlled comparison of imipramine, amitriptyline and placeboin hospitalised depressed patients. Journal of Nervous and MentalDisease 1964;139(4):370–5.
Hussain 1970 {published data only}Hussain Z. Drugs in depressive illness. BMJ 1970;1(707):482.
Murphy 1984 {published data only}Murphy GE, Simons AD, Wetzel RD, Lustman PJ. Cognitive therapyand pharmacotherapy. Archives of General Psychiatry 1984;41(1):33–41.
Uhlenhuth 1964 {published data only}Uhlenhuth EH, Park LC. The influence of medication (imipramine)and doctor in relieving depressed psychoneurotic outpatients. Journalof Psychiatric Research 1964;2(2):101–22.
Weintraub 1963 {published data only}Weintraub W, Aronson H. Clinical judgement in psychopharmaco-logical research. Journal of Neuropsychiatry 1963;5(1):65–70.
Wilson 1963 {published data only}Wilson IC, Vernon JT, Guin T, Sandifer MG. A controlled study oftreatments of depression. Journal of Neuropsychiatry 1963;4:331–7.
References to studies excluded from this review
Azima 1962a {published data only}Azima H, Arthurs D, Silver A, Azima F. The effect of MP-809 indepressive states: a multi-blind study.. American Journal of Psychiatry1962;119:573–74.
Azima 1962b {published data only}Azima H, Silver A, Arthurs D. The effects of G-33040 in depressivestates: a multi-blind study.. American Journal of Psychiatry 1962;119:465–6.
Giannini 1986 {published data only}Giannini AJ, Malone DA, Giannini MC, Price WA, Loiselle RH.Treatment of depression in chronic cocaine and phencyclidine abusewith desipramine.. J Clin Pharmaco 1986;26(3):211–214.
9Active placebos versus antidepressants for depression (Review)Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Max 1987 {published data only}Max MB, Culnane M, Schafer SC, Gracely RH, Walther DJ, SmollerB, Dubner R. Amitriptyline relieves diabetic neuropathy pain in pa-tients with normal or depressed mood.. Neurology 1989;37(4):589–96.
Max 1991 {published data only}Max MB, Kishore Kumar R, Schafer SC, Meister B, Gracely RH,Smoller B, Dubner R. Efficacy of desipramine in painful diabeticneuropathy: a placebo-controlled trial. Pain 1991;45(1):3–9.
Additional references
Abramson 1990Abramson JH. Meta-analysis: a review of the pros and cons. PublicHealth Review 1990;18(1):1–47.
Cicchetti 1983Cicchetti DV, Prusoff BA. Reliability of depression and associatedclinical symptoms.. Archives of General Psychiatry 1983;40(9):987–90.
Cole 1964Cole J. Therapeutic efficacy of antidepressant drugs. JAMA 1964;190:448–55.
Davis 1965Davis JM. Efficacy of tranquilising and antidepressant drugs. Archivesof General psychiatry 1965;13(6):552–72.
Donoghue 1996Donoghue J, Tylee A, Wildgust H. Cross sectional database analysisof antidepressant prescribing in general practice in the United King-dom, 1993-5. BMJ 1996;313(7061):861–2.
Engelhardt 1969Engelhardt DM, Margolis RA, Rudorfer L, Paley HM. Physicianbias and the double-blind. Archives of General Psychiatry 1969;20(3):315–20.
Frank 1957Frank JD, Gleidman LH, Imber SD, Nash EH, Stone AR. Whypatients leave psychotherapy. Archives of Neurology and Psychiatry1957;77:283–95.
Gillin 1995Gillin JC, Laurellio J, Kelsoe JR, Rapaport M, Golshan S, KennyWM, et al.No antidepressant effect of biperiden compared withplacebo in depression: A double-blind 6-week clinical trial. Psychi-atric Research 1995;58(2):99–105.
Greenberg 1992Greenberg RP, Bornstein RF, Greenberg MD, Fisher S. A meta-anal-ysis of antidepressant outcome under “blinder” conditions. Journalof Consulting and Clinical Psychology 1992;60(5):664–9.
Greenberg 1994aGreenberg RP, Fisher S. Suspended judgement. Seeing through thedouble-masked design: a commentary. Controlled Clinical Trials1994;15(4):244–6.
Greenberg 1994bGreenberg RP, Bornstein RF, Zborowski MJ, Fisher S, GreenbergMD. A meta-analysis of fluoxetine outcome in the treatment of de-pression. Journal of Nervous and Mental Disease 1994;182(10):547–51.
Guy 1976Guy W. ECDEU Assessments Manual for Psychopharmacology.Rockville, MD: National Institute for Mental Health, 1976.
Henry 1993Henry JA. Debits and credits in the management of depression.British Journal of Psychiatry Supplementum 1993;20:33–39.
Hollister 1963Hollister LE, Overall JE, Johnson M, Katz G, Kimbell I, HonigfeldG. Evaluation of desipramine in depressive states. Journal of NewDrugs 1963;3:161–6.
Jadad 1996Jadad AR, Moore RA, Carroll D, Jenkinson C, Reynolds DJ, Gav-aghan DJ, et al.Assessing the quality of reports of randomised clinicaltrials: is blinding necessary?. Controlled Clinical Trials 1996;17(1):1–12.
Kasper 1981Kasper S, Moises HW, Beckman H. The anticholinergic biperidenin depressive disorders. Pharmacopsychiatria 1981;14(6):195–8.
Klerman 1967Klerman GL, Cole J. Clinical pharmacology of imipramine and re-lated compounds. International Journal of Psychiatry 1967;3(4):267–304.
McNair 1974McNair DM. Self-evaluations of antidepressants. Psychopharmacolo-gia 1974;37(4):281–302.
Moncrieff 2001Moncrieff J, Churchill R, Drummond DC, McGuire H. Develop-ment of a quality assessment instrument for trials of treatments fordepression and neurosis. International Journal of Methods in Psychi-atric Research 2001;10(3):126–33.
Morris 1974Morris JB, Beck AT. The efficacy of antidepressant drugs. A reviewof reaearch (1958-1972). Archives of General Psychiatry 1974;30(5):667–74.
MRC 1965Medical Research Council. Clinical trial of the treatment of depres-sive illness. BMJ 1965;1:881–6.
Murray 1989Murray EJ. Measurement issues in the evaluation of psychopharma-cological therapy. In: Fisher S, Greenberg RP editor(s). The limits ofbiological treatments for psychological distress. Hillsdale, NJ: LawrenceErlbaum Associates, 1989:39–68.
Overall 1962Overall JE. Dimensions of manifest depression. Journal of PsychiatricResearch 1962;1:239–47.
QAP 1983The Quality Assurance Project. A treatment outline for depressivedisorder. Australia and New Zealand Journal of Psychiatry 1983;17:129–46.
Rogers 1975Rogers SC, Clay PM. A statistical review of controlled trials ofimipramine and placebo in the treatment of depressive illness. BritishJournal of Psychiatry 1975;127:599–603.
10Active placebos versus antidepressants for depression (Review)Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Rush 1977Rush AJ, Beck AT, Kovacs M, Hollon S. Comparative effects ofcognitive therapy and pharmacotherapy in the treatment of depressedoutpatients. Cognitive Research and Therapy 1977;1(1):17–37.
Schulz 1995Schulz KF, Chalmers I, Hayes RJ, Altman DG. Empirical evidence ofbias. Dimensions of methodological quality associated with estimatesof treatment effects in controlled trials. JAMA 1995;273(5):408–412.
Schulz 1996Schulz KF, Grimes DA, Altman DG, Hayes RJ. Blinding and ex-clusions after allocation in randomised controlled trials: survey ofparallel group trials in obstetrics and gynaecology.. BMJ 1996;312(7033):742–4.
Smith 1969Smith A, Traganza E, Harrison G. Studies on the effectiveness ofantidepressants drugs. Psychopharmacology 1969;Suppl:1–53.
Smith 1980Smith MC, Glass GV, Miller TI. Reviews of research on the effects ofdrug therapy on psychological disorders. In: Smith MC, Glass GV,Miller TI editor(s). The benefits of psychotherapy. Baltimore, MD:John Hopkins University Press, 1980:127–261.
StataStata Press. Stata. 5. College Station, TX: Stata Press, 1997.
Steinbrueck 1983Steinbrueck SM, Maxwell SE, Howard GS. A meta-analysis of psy-chotherapy and drug therapy in the treatment of unipolar depression
with adults. Journal of Consulting and Clinical Psychology 1983;51(6):856–63.
Thomson 1982Thomson R. Side effects and placebo amplification. British Journalof Psychiatry 1982;140:64–68.
Toneatto 1992Toneatto T, Sellers EM. Perception of whether drug or placebo hasbeen administered is a determinant of drinking reduction. In: SellersEM, Naranjo CA editor(s). Novel pharmacological interventions foralcoholism. New York, NY: Springer Verlag, 1992.
Wechsler 1965Wechsler H, Grosser GH, Greenblatt M. Research evaluating antide-pressants in hospitalised mental patients: a survey of published re-ports during a five year period. Journal of Nervous and Mental Disease1965;141(2):231–9.
White 1992White K, Kando J, Park T, Waternaux C, Brown WA. Side effectsand the “blindability” of clinical drug trials. American Journal ofPsychiatry 1992;149(12):1730–61.
References to other published versions of this review
Moncrieff 1998Moncrieff J, Wessely S, Hardy R. Meta-analysis of trials comparingantidepressants with active placebos. British Journal of Psychiatry1998;172:227–31.
∗ Indicates the major publication for the study
C H A R A C T E R I S T I C S O F S T U D I E S
Characteristics of included studies [ordered by study ID]
Daneman 1961
Methods parallel group trial. Variable duration with evaultions done at 1 month and 2 months.
Participants 195 outpatients, age range 17-75, 69% women
Interventions imipramine mean dose 133mg and atropine 1.25 mg
Outcomes 4 “response to treatment” categories
Notes not clear if response to treatment, which was based on ratings of a list of symptoms, was rated blind.
Risk of bias
11Active placebos versus antidepressants for depression (Review)Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Daneman 1961 (Continued)
Item Authors’ judgement Description
Allocation concealment? Yes A - Adequate
Friedman 1966
Methods parallel group trial. Duration 3 weeks.
Participants 78 inpatients
Interventions imipramine 150-200mgplacebo contained atropine (dose not reported)
Outcomes Global Clinical Improvement on 6 point scale rated by project psychiatrist and ward doctor, PhiladelphiaPsychiatric Centre Psychatric Rating Scale (30 items), Philadelphia Psychiatric Center Depression ProgressTest, Clyde Mood Scale plus psychometric tests.
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear B - Unclear
Friedman 1975
Methods parallel group factorial trial evaluating marital therapy and amitriptyline. Duration 12 weeks.
Participants 196 married outpatients, mean age 36, range 21-67; 79% women
Interventions amitriptyline 100mgplacebo contained atropine 0.4mg
Outcomes Global Clinical Improvement Scale (score 1-6), Psychiatric Rating Scale (based on HRSD), Patient SelfReport Inventory of Psychic and Somatic Complaints, family role, marital relations
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear B - Unclear
12Active placebos versus antidepressants for depression (Review)Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Hollister 1964
Methods parallel group trial comparing imipramine, amitriptyline and placebo.Duration 3 weeks
Participants 110 inpatient in veterans hospitals, median age 43, range 26-72; all men
Interventions imipramine mean dose 171mg, amitriptyline mean dose 157mgplacebo contained atropine 1mg
Outcomes 5 subscales from Inpateint Multidimensional Psychiatric Scale: manifest depression, anxious intropuni-tiveness, retardation, conceptual disorganisation, excitement; 2 subscales from Minnesota MultiphasicPersonality Inventory: manifest depression scale and “D” scale
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear B - Unclear
Hussain 1970
Methods parallel group trial comparing amitriptyline, amitiptyline + perphenazine and placebo. Duration notreported.
Participants 34 patients from psychiatric practice, no details reported
Interventions doses not reportedplacebo contained atropine (dose not reported)
Outcomes 5 categories of improvement
Notes This is a brief communication about preliminary results in a letter. No final report of this trial could betraced.
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear B - Unclear
13Active placebos versus antidepressants for depression (Review)Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Murphy 1984
Methods parallel group cognitive therapy trial. Groups had adjunctive cognitive therapy. Duration 12 weeks treat-ment followed by 4 weeks follow up.
Participants 39 outpatients involved in this comparison, age range of completers 19-59, 66% completers women
Interventions nortriptyline 100-150mgplacebo contained atropine 0.1-0.15mg and phenobarbital sodium 10-15mg
Outcomes Hamilton Rating Scale for Depression, Beck Depression Inventory, Scale for Suicidal Ideation, Hopeless-ness Scale, Raskin, Three-Area Severity of Depression Scale, Visual Analogue Scale, Zung Anxiety Scale,Social Adjustment Scale, MMPI, Self Control Scale, Cognitive Response Test, Dsysfunctional AttitudeScale, Automatic Thoughts Questionnaire
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Yes A - Adequate
Uhlenhuth 1964
Methods crossover trial of 4 weeks with results of first period of 2 weeks reported as for parallel groups.
Participants 50 outpatients, mean age 42 (range 22-71); 76% women
Interventions imipramine 150mgatropine 0.6mg
Outcomes Total Distress Score, Morale Loss Scale, doctors and patients overall estimate of condition as better, same,worse.
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear B - Unclear
14Active placebos versus antidepressants for depression (Review)Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
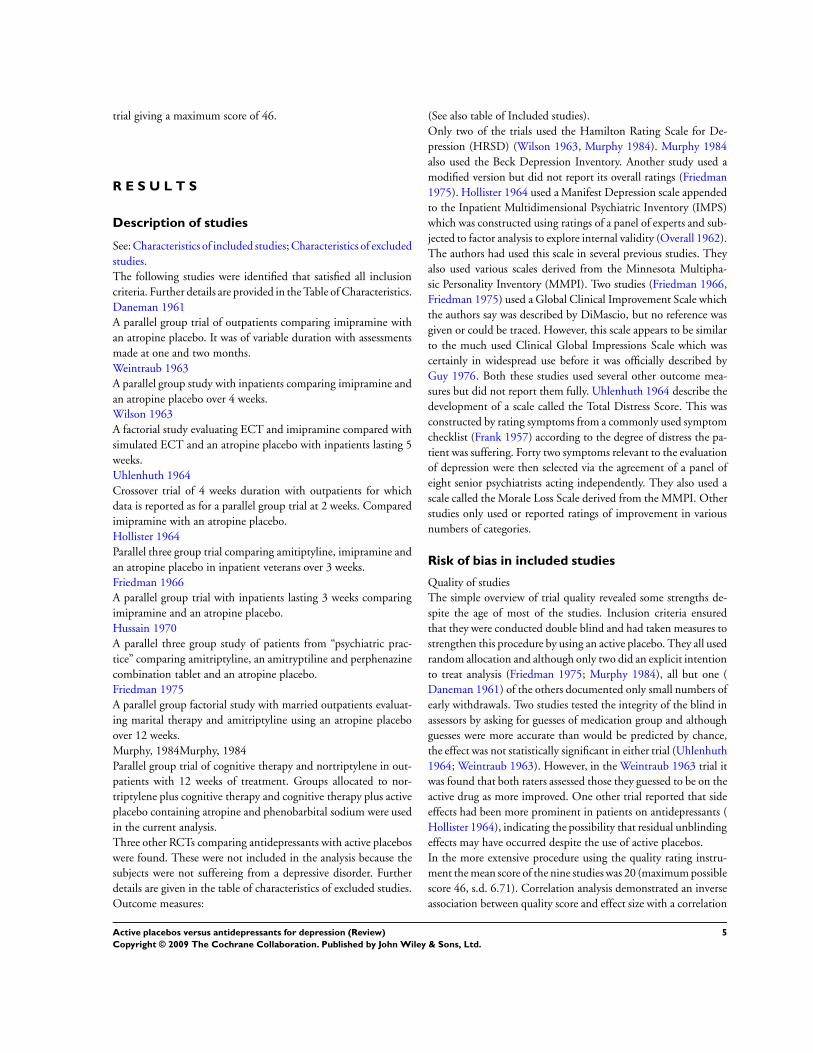
Weintraub 1963
Methods parallel group study. Duration 4 weeks.
Participants 89 inpatients, 60% women, mean age 51 (range 19-73)
Interventions imipramine 150 mgatropine 0.6mg
Outcomes improvement rated in three catgeories by ward doctor and hospital director
Notes discrepant ratings with ward doctor rating drug group as more improved and finding greater drug placebodifference.Blind tested. Neither rater guessed medication group better than chance but both raters rated those theyguessed to be on the drug as significantly more improved (p<0.1).
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear B - Unclear
Wilson 1963
Methods factorial design testing ECT vs simulated ECT and drug vs placeboDuration 5 weeks.
Participants 24 inpatients, all women, age range 40-59
Interventions imipramine 150-220 mgatropine (dose not reported)
Outcomes Hamilton Rating Scale for Depression, MMPI “D” scale
Notes
Risk of bias
Item Authors’ judgement Description
Allocation concealment? Unclear B - Unclear
15Active placebos versus antidepressants for depression (Review)Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Characteristics of excluded studies [ordered by study ID]
Azima 1962a Did not use a recognised antidepressant. Not all observers were blind to treatment allocation.
Azima 1962b Did not use a recognised antidepressant. Not all observers were blind to treatment allocation.
Giannini 1986 Subjects did not have a diagnosed depressive disorder. (Trial of desipramine for depressive symptoms associatedwith cocaine and PCP withdrawal.)
Max 1987 Subjects did not have a diagnosed depressive disorder. (Crossover trial of amitiptyline in diabetic neuropathy)
Max 1991 Subjects did not have a diagnosed depressive disorder. (Crossover trial of amitiptyline in diabetic neuropathy)
16Active placebos versus antidepressants for depression (Review)Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

D A T A A N D A N A L Y S E S
Comparison 1. antidepressant versus active placebo (all trials)
Outcome or subgroup titleNo. ofstudies
No. ofparticipants Statistical method Effect size
1 change in mood after treatmentperiod
9 750 Std. Mean Difference (IV, Fixed, 95% CI) 0.39 [0.24, 0.54]
Comparison 2. subgroup analysis: in patients
Outcome or subgroup titleNo. ofstudies
No. ofparticipants Statistical method Effect size
1 change in mood after treatment 4 244 Std. Mean Difference (IV, Fixed, 95% CI) 0.12 [-0.14, 0.38]
Comparison 3. subgroup analysis: out patients
Outcome or subgroup titleNo. ofstudies
No. ofparticipants Statistical method Effect size
1 change in mood after treatment 5 506 Std. Mean Difference (IV, Fixed, 95% CI) 0.52 [0.34, 0.70]
Comparison 4. sensitivity analysis (excluding Daneman 1961)
Outcome or subgroup titleNo. ofstudies
No. ofparticipants Statistical method Effect size
1 change in mood after treatment 8 555 Std. Mean Difference (IV, Fixed, 95% CI) 0.17 [-0.00, 0.34]
17Active placebos versus antidepressants for depression (Review)Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Comparison 5. sensitivity analysis (excluding Daneman 1961 and Murphy et al 1984)
Outcome or subgroup titleNo. ofstudies
No. ofparticipants Statistical method Effect size
1 change in mood after treatment 7 516 Std. Mean Difference (IV, Fixed, 95% CI) 0.21 [0.03, 0.38]
Comparison 6. sensitivity analysis (excluding Daneman 1961 and using higher effect size from Weintraub &Aronson, 1963)
Outcome or subgroup titleNo. ofstudies
No. ofparticipants Statistical method Effect size
1 change in mood after treatment 8 556 Std. Mean Difference (IV, Fixed, 95% CI) 0.23 [0.06, 0.40]
Comparison 7. sensitivity analysis, inpatients (using higher effect size from Weintraub & Aronson, 1963)
Outcome or subgroup titleNo. ofstudies
No. ofparticipants Statistical method Effect size
1 change in mood after treatment 4 245 Std. Mean Difference (IV, Fixed, 95% CI) 0.25 [-0.00, 0.51]
Comparison 8. sensitivity analysis, outpatients (excluding Daneman 1961)
Outcome or subgroup titleNo. ofstudies
No. ofparticipants Statistical method Effect size
1 change in mood after treatment 4 311 Std. Mean Difference (IV, Fixed, 95% CI) 0.20 [-0.02, 0.43]
Comparison 9. sensitivty analysis (excluding trials with categorical outcomes)
Outcome or subgroup titleNo. ofstudies
No. ofparticipants Statistical method Effect size
1 change in mood after treatment 6 454 Std. Mean Difference (IV, Fixed, 95% CI) 0.13 [-0.06, 0.31]
18Active placebos versus antidepressants for depression (Review)Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Comparison 10. sensitivity analysis (excluding trials with estimated s.d.’s)
Outcome or subgroup titleNo. ofstudies
No. ofparticipants Statistical method Effect size
1 change in mood 6 556 Std. Mean Difference (IV, Fixed, 95% CI) 0.51 [0.33, 0.68]
Analysis 1.1. Comparison 1 antidepressant versus active placebo (all trials), Outcome 1 change in moodafter treatment period.
Review: Active placebos versus antidepressants for depression
Comparison: 1 antidepressant versus active placebo (all trials)
Outcome: 1 change in mood after treatment period
Study or subgroup Treatment Control Std. Mean Difference Weight Std. Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
Daneman 1961 94 1.64 (1.45) 101 0.37 (0.78) 24.0 % 1.10 [ 0.80, 1.40 ]
Friedman 1966 36 2.9 (1.9) 26 2.65 (1.84) 8.6 % 0.13 [ -0.37, 0.64 ]
Friedman 1975 98 1.85 (2.17) 98 1.54 (2.27) 27.8 % 0.14 [ -0.14, 0.42 ]
Hollister 1964 62 50.17 (57.4) 31 39 (57.4) 11.7 % 0.19 [ -0.24, 0.63 ]
Hussain 1970 15 3 (1.6) 19 1.79 (1.4) 4.4 % 0.79 [ 0.09, 1.50 ]
Murphy 1984 22 12.22 (9.22) 17 15.59 (9.22) 5.4 % -0.36 [ -1.00, 0.28 ]
Uhlenhuth 1964 22 28.36 (29.05) 20 12.35 (23.06) 5.7 % 0.60 [ -0.02, 1.22 ]
Weintraub 1963 36 1.17 (0.7) 31 1.07 (0.68) 9.4 % 0.14 [ -0.34, 0.62 ]
Wilson 1963 10 15.3 (3.74) 12 16.4 (4.32) 3.1 % -0.26 [ -1.10, 0.58 ]
Total (95% CI) 395 355 100.0 % 0.39 [ 0.24, 0.54 ]Heterogeneity: Chi2 = 36.26, df = 8 (P = 0.00002); I2 =78%
Test for overall effect: Z = 5.18 (P < 0.00001)
-10 -5 0 5 10
Favours control Favours treatment
19Active placebos versus antidepressants for depression (Review)Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 2.1. Comparison 2 subgroup analysis: in patients, Outcome 1 change in mood after treatment.
Review: Active placebos versus antidepressants for depression
Comparison: 2 subgroup analysis: in patients
Outcome: 1 change in mood after treatment
Study or subgroup Treatment Control Std. Mean Difference Weight Std. Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
Friedman 1966 36 2.9 (1.9) 26 2.65 (1.84) 26.1 % 0.13 [ -0.37, 0.64 ]
Hollister 1964 62 50.17 (57.4) 31 39 (57.4) 35.7 % 0.19 [ -0.24, 0.63 ]
Weintraub 1963 36 1.17 (0.7) 31 1.07 (0.68) 28.8 % 0.14 [ -0.34, 0.62 ]
Wilson 1963 10 15.3 (3.74) 12 16.4 (4.32) 9.4 % -0.26 [ -1.10, 0.58 ]
Total (95% CI) 144 100 100.0 % 0.12 [ -0.14, 0.38 ]Heterogeneity: Chi2 = 0.90, df = 3 (P = 0.83); I2 =0.0%
Test for overall effect: Z = 0.91 (P = 0.36)
-10 -5 0 5 10
Favours control Favours treatment
Analysis 3.1. Comparison 3 subgroup analysis: out patients, Outcome 1 change in mood after treatment.
Review: Active placebos versus antidepressants for depression
Comparison: 3 subgroup analysis: out patients
Outcome: 1 change in mood after treatment
Study or subgroup Treatment Control Std. Mean Difference Weight Std. Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
Daneman 1961 94 1.64 (1.45) 101 0.37 (0.78) 35.7 % 1.10 [ 0.80, 1.40 ]
Friedman 1975 98 1.85 (2.17) 98 1.54 (2.27) 41.4 % 0.14 [ -0.14, 0.42 ]
Hussain 1970 15 3 (1.6) 19 1.79 (1.4) 6.5 % 0.79 [ 0.09, 1.50 ]
Murphy 1984 22 12.22 (9.22) 17 15.59 (9.22) 8.0 % -0.36 [ -1.00, 0.28 ]
Uhlenhuth 1964 22 28.36 (29.05) 20 12.35 (23.06) 8.5 % 0.60 [ -0.02, 1.22 ]
Total (95% CI) 251 255 100.0 % 0.52 [ 0.34, 0.70 ]Heterogeneity: Chi2 = 29.07, df = 4 (P<0.00001); I2 =86%
Test for overall effect: Z = 5.68 (P < 0.00001)
-10 -5 0 5 10
Favours control Favours treatment
20Active placebos versus antidepressants for depression (Review)Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
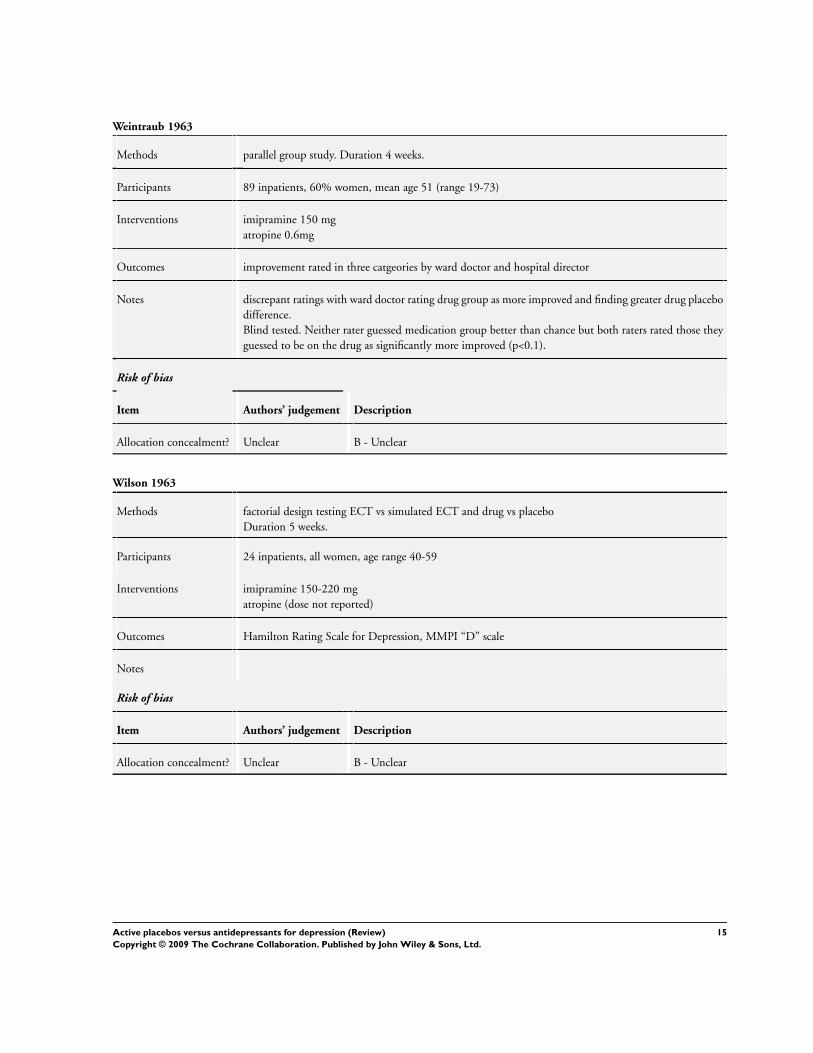
Analysis 4.1. Comparison 4 sensitivity analysis (excluding Daneman 1961), Outcome 1 change in moodafter treatment.
Review: Active placebos versus antidepressants for depression
Comparison: 4 sensitivity analysis (excluding Daneman 1961)
Outcome: 1 change in mood after treatment
Study or subgroup Treatment Control Std. Mean Difference Weight Std. Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
Friedman 1966 36 2.9 (1.9) 26 2.65 (1.84) 11.3 % 0.13 [ -0.37, 0.64 ]
Friedman 1975 98 1.85 (2.17) 98 1.54 (2.27) 36.6 % 0.14 [ -0.14, 0.42 ]
Hollister 1964 62 50.17 (57.4) 31 39 (57.4) 15.4 % 0.19 [ -0.24, 0.63 ]
Hussain 1970 15 3 (1.6) 19 1.79 (1.4) 5.8 % 0.79 [ 0.09, 1.50 ]
Murphy 1984 22 12.22 (9.22) 17 15.59 (9.22) 7.1 % -0.36 [ -1.00, 0.28 ]
Uhlenhuth 1964 22 28.36 (29.05) 20 12.35 (23.06) 7.5 % 0.60 [ -0.02, 1.22 ]
Weintraub 1963 36 1.17 (0.7) 31 1.07 (0.68) 12.4 % 0.14 [ -0.34, 0.62 ]
Wilson 1963 10 15.3 (3.74) 12 16.4 (4.32) 4.0 % -0.26 [ -1.10, 0.58 ]
Total (95% CI) 301 254 100.0 % 0.17 [ 0.00, 0.34 ]Heterogeneity: Chi2 = 8.51, df = 7 (P = 0.29); I2 =18%
Test for overall effect: Z = 1.94 (P = 0.053)
-10 -5 0 5 10
Favours control Favours treatment
21Active placebos versus antidepressants for depression (Review)Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 5.1. Comparison 5 sensitivity analysis (excluding Daneman 1961 and Murphy et al 1984), Outcome1 change in mood after treatment.
Review: Active placebos versus antidepressants for depression
Comparison: 5 sensitivity analysis (excluding Daneman 1961 and Murphy et al 1984)
Outcome: 1 change in mood after treatment
Study or subgroup Treatment Control Std. Mean Difference Weight Std. Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
Friedman 1966 36 2.9 (1.9) 26 2.65 (1.84) 12.1 % 0.13 [ -0.37, 0.64 ]
Friedman 1975 98 1.85 (2.17) 98 1.54 (2.27) 39.3 % 0.14 [ -0.14, 0.42 ]
Hollister 1964 62 50.17 (57.4) 31 39 (57.4) 16.6 % 0.19 [ -0.24, 0.63 ]
Hussain 1970 15 3 (1.6) 19 1.79 (1.4) 6.2 % 0.79 [ 0.09, 1.50 ]
Uhlenhuth 1964 22 28.36 (29.05) 20 12.35 (23.06) 8.0 % 0.60 [ -0.02, 1.22 ]
Weintraub 1963 36 1.17 (0.7) 31 1.07 (0.68) 13.4 % 0.14 [ -0.34, 0.62 ]
Wilson 1963 10 15.3 (3.74) 12 16.4 (4.32) 4.3 % -0.26 [ -1.10, 0.58 ]
Total (95% CI) 279 237 100.0 % 0.21 [ 0.03, 0.38 ]Heterogeneity: Chi2 = 5.71, df = 6 (P = 0.46); I2 =0.0%
Test for overall effect: Z = 2.31 (P = 0.021)
-10 -5 0 5 10
Favours control Favours treatment
22Active placebos versus antidepressants for depression (Review)Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
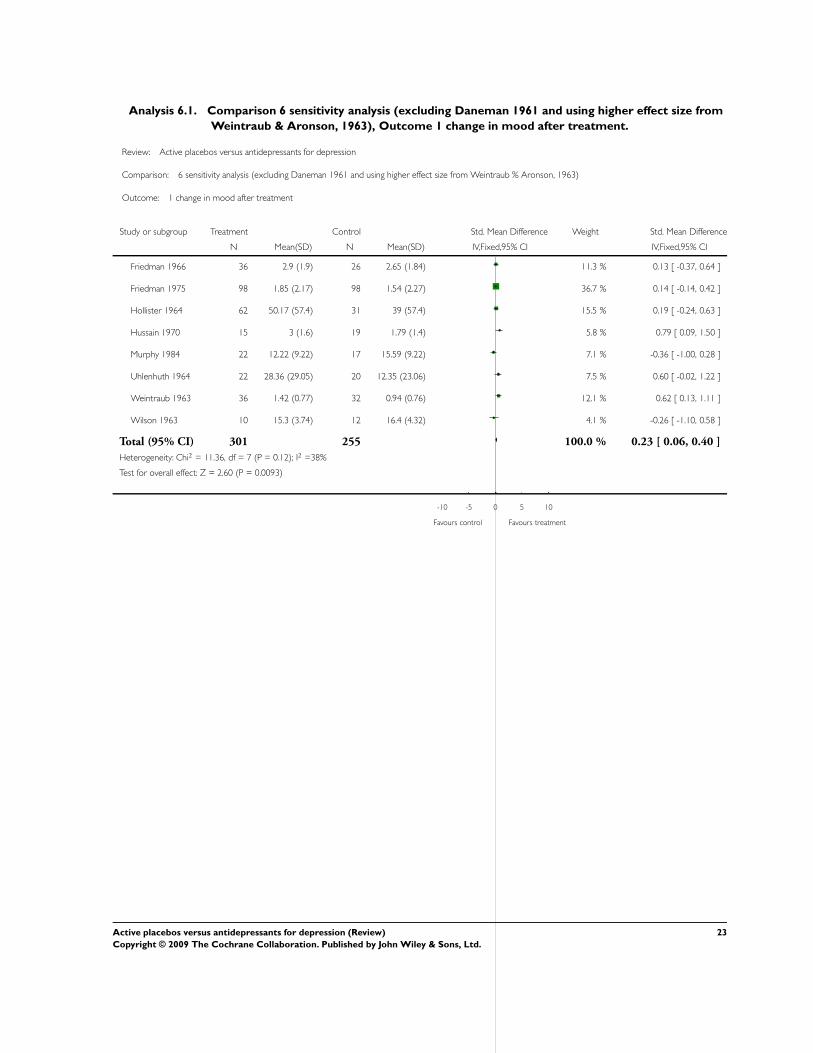
Analysis 6.1. Comparison 6 sensitivity analysis (excluding Daneman 1961 and using higher effect size fromWeintraub & Aronson, 1963), Outcome 1 change in mood after treatment.
Review: Active placebos versus antidepressants for depression
Comparison: 6 sensitivity analysis (excluding Daneman 1961 and using higher effect size from Weintraub % Aronson, 1963)
Outcome: 1 change in mood after treatment
Study or subgroup Treatment Control Std. Mean Difference Weight Std. Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
Friedman 1966 36 2.9 (1.9) 26 2.65 (1.84) 11.3 % 0.13 [ -0.37, 0.64 ]
Friedman 1975 98 1.85 (2.17) 98 1.54 (2.27) 36.7 % 0.14 [ -0.14, 0.42 ]
Hollister 1964 62 50.17 (57.4) 31 39 (57.4) 15.5 % 0.19 [ -0.24, 0.63 ]
Hussain 1970 15 3 (1.6) 19 1.79 (1.4) 5.8 % 0.79 [ 0.09, 1.50 ]
Murphy 1984 22 12.22 (9.22) 17 15.59 (9.22) 7.1 % -0.36 [ -1.00, 0.28 ]
Uhlenhuth 1964 22 28.36 (29.05) 20 12.35 (23.06) 7.5 % 0.60 [ -0.02, 1.22 ]
Weintraub 1963 36 1.42 (0.77) 32 0.94 (0.76) 12.1 % 0.62 [ 0.13, 1.11 ]
Wilson 1963 10 15.3 (3.74) 12 16.4 (4.32) 4.1 % -0.26 [ -1.10, 0.58 ]
Total (95% CI) 301 255 100.0 % 0.23 [ 0.06, 0.40 ]Heterogeneity: Chi2 = 11.36, df = 7 (P = 0.12); I2 =38%
Test for overall effect: Z = 2.60 (P = 0.0093)
-10 -5 0 5 10
Favours control Favours treatment
23Active placebos versus antidepressants for depression (Review)Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 7.1. Comparison 7 sensitivity analysis, inpatients (using higher effect size from Weintraub &Aronson, 1963), Outcome 1 change in mood after treatment.
Review: Active placebos versus antidepressants for depression
Comparison: 7 sensitivity analysis, inpatients (using higher effect size from Weintraub % Aronson, 1963)
Outcome: 1 change in mood after treatment
Study or subgroup Treatment Control Std. Mean Difference Weight Std. Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
Friedman 1966 36 2.9 (1.9) 26 2.65 (1.84) 26.4 % 0.13 [ -0.37, 0.64 ]
Hollister 1964 62 50.17 (57.4) 31 39 (57.4) 36.0 % 0.19 [ -0.24, 0.63 ]
Weintraub 1963 36 1.42 (0.77) 32 0.94 (0.76) 28.2 % 0.62 [ 0.13, 1.11 ]
Wilson 1963 10 15.3 (3.74) 12 16.4 (4.32) 9.4 % -0.26 [ -1.10, 0.58 ]
Total (95% CI) 144 101 100.0 % 0.25 [ 0.00, 0.51 ]Heterogeneity: Chi2 = 3.89, df = 3 (P = 0.27); I2 =23%
Test for overall effect: Z = 1.92 (P = 0.054)
-10 -5 0 5 10
Favours control Favours treatment
Analysis 8.1. Comparison 8 sensitivity analysis, outpatients (excluding Daneman 1961), Outcome 1 changein mood after treatment.
Review: Active placebos versus antidepressants for depression
Comparison: 8 sensitivity analysis, outpatients (excluding Daneman 1961)
Outcome: 1 change in mood after treatment
Study or subgroup Treatment Control Std. Mean Difference Weight Std. Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
Friedman 1975 98 1.85 (2.17) 98 1.54 (2.27) 64.3 % 0.14 [ -0.14, 0.42 ]
Hussain 1970 15 3 (1.6) 19 1.79 (1.4) 10.1 % 0.79 [ 0.09, 1.50 ]
Murphy 1984 22 12.22 (9.22) 17 15.59 (9.22) 12.4 % -0.36 [ -1.00, 0.28 ]
Uhlenhuth 1964 22 28.36 (29.05) 20 12.35 (23.06) 13.1 % 0.60 [ -0.02, 1.22 ]
Total (95% CI) 157 154 100.0 % 0.20 [ -0.02, 0.43 ]Heterogeneity: Chi2 = 7.38, df = 3 (P = 0.06); I2 =59%
Test for overall effect: Z = 1.78 (P = 0.076)
-10 -5 0 5 10
Favours control Favours treatment
24Active placebos versus antidepressants for depression (Review)Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.
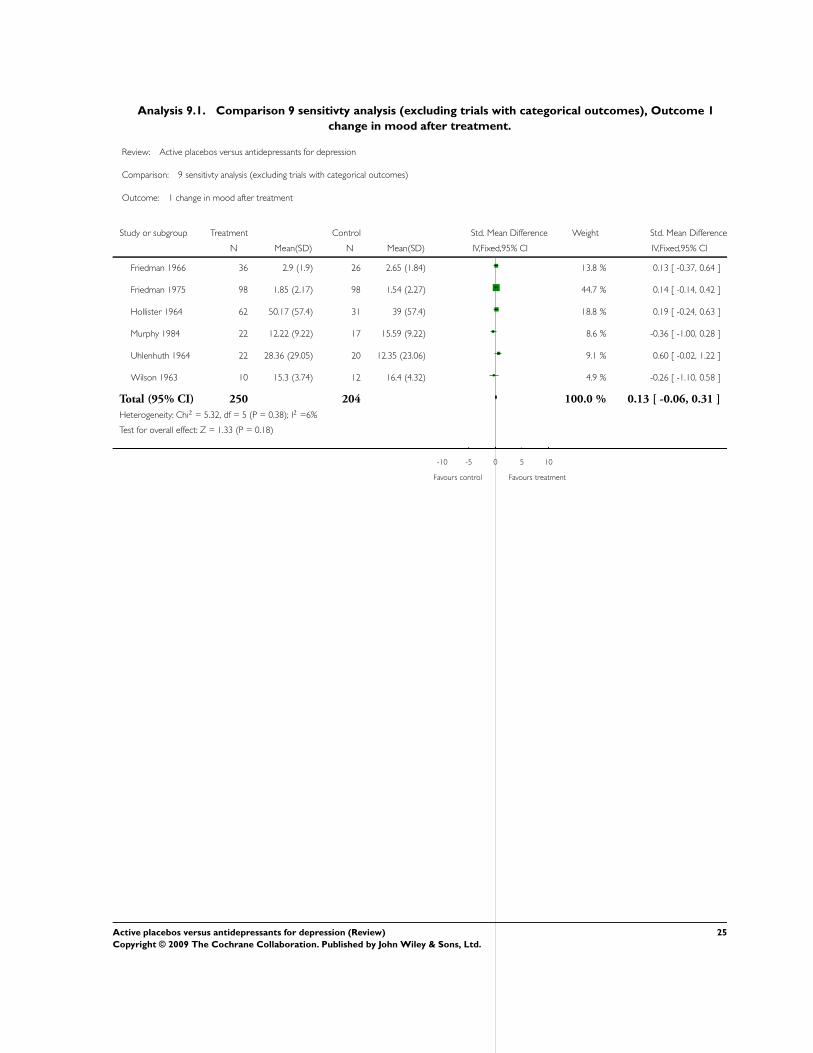
Analysis 9.1. Comparison 9 sensitivty analysis (excluding trials with categorical outcomes), Outcome 1change in mood after treatment.
Review: Active placebos versus antidepressants for depression
Comparison: 9 sensitivty analysis (excluding trials with categorical outcomes)
Outcome: 1 change in mood after treatment
Study or subgroup Treatment Control Std. Mean Difference Weight Std. Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
Friedman 1966 36 2.9 (1.9) 26 2.65 (1.84) 13.8 % 0.13 [ -0.37, 0.64 ]
Friedman 1975 98 1.85 (2.17) 98 1.54 (2.27) 44.7 % 0.14 [ -0.14, 0.42 ]
Hollister 1964 62 50.17 (57.4) 31 39 (57.4) 18.8 % 0.19 [ -0.24, 0.63 ]
Murphy 1984 22 12.22 (9.22) 17 15.59 (9.22) 8.6 % -0.36 [ -1.00, 0.28 ]
Uhlenhuth 1964 22 28.36 (29.05) 20 12.35 (23.06) 9.1 % 0.60 [ -0.02, 1.22 ]
Wilson 1963 10 15.3 (3.74) 12 16.4 (4.32) 4.9 % -0.26 [ -1.10, 0.58 ]
Total (95% CI) 250 204 100.0 % 0.13 [ -0.06, 0.31 ]Heterogeneity: Chi2 = 5.32, df = 5 (P = 0.38); I2 =6%
Test for overall effect: Z = 1.33 (P = 0.18)
-10 -5 0 5 10
Favours control Favours treatment
25Active placebos versus antidepressants for depression (Review)Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

Analysis 10.1. Comparison 10 sensitivity analysis (excluding trials with estimated s.d.’s), Outcome 1 changein mood.
Review: Active placebos versus antidepressants for depression
Comparison: 10 sensitivity analysis (excluding trials with estimated s.d.’s)
Outcome: 1 change in mood
Study or subgroup Treatment Control Std. Mean Difference Weight Std. Mean Difference
N Mean(SD) N Mean(SD) IV,Fixed,95% CI IV,Fixed,95% CI
Daneman 1961 94 1.64 (1.45) 101 0.37 (0.78) 32.3 % 1.10 [ 0.80, 1.40 ]
Friedman 1975 98 1.85 (2.17) 98 1.54 (2.27) 37.4 % 0.14 [ -0.14, 0.42 ]
Hussain 1970 15 3 (1.6) 19 1.79 (1.4) 5.9 % 0.79 [ 0.09, 1.50 ]
Uhlenhuth 1964 22 28.36 (29.05) 20 12.35 (23.06) 7.6 % 0.60 [ -0.02, 1.22 ]
Weintraub 1963 36 1.17 (0.7) 31 1.07 (0.68) 12.7 % 0.14 [ -0.34, 0.62 ]
Wilson 1963 10 15.3 (3.74) 12 16.4 (4.32) 4.1 % -0.26 [ -1.10, 0.58 ]
Total (95% CI) 275 281 100.0 % 0.51 [ 0.33, 0.68 ]Heterogeneity: Chi2 = 27.42, df = 5 (P = 0.00005); I2 =82%
Test for overall effect: Z = 5.78 (P < 0.00001)
-10 -5 0 5 10
Favours control Favours treatment
W H A T ’ S N E W
Last assessed as up-to-date: 11 February 2008.
31 October 2008 Amended Converted to new review format.
H I S T O R Y
Protocol first published: Issue 2, 1998
Review first published: Issue 2, 2001
6 October 2003 New citation required and conclusions have changed Substantive amendment
26Active placebos versus antidepressants for depression (Review)Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.

C O N T R I B U T I O N S O F A U T H O R S
JM devised protocol, conducted review, wrote review.
RH helped devise protocol, applied inclusion criteria and provided statistical advice.
SW helped devise protocol and provided general supervision for the review project.
D E C L A R A T I O N S O F I N T E R E S T
none
S O U R C E S O F S U P P O R T
Internal sources
• South Thames Regional Health Authority, UK.
External sources
• No sources of support supplied
I N D E X T E R M S
Medical Subject Headings (MeSH)
Antidepressive Agents [∗therapeutic use]; Bias (Epidemiology); Depression [∗drug therapy]; Placebo Effect; Randomized ControlledTrials as Topic; Treatment Outcome
MeSH check words
Humans
27Active placebos versus antidepressants for depression (Review)Copyright © 2009 The Cochrane Collaboration. Published by John Wiley & Sons, Ltd.