
Active FOIUS surveillance: Shrinking the grey zone Sommerakademi … · 2016. 7. 31. · Klotz et...
18
Active surveillance: Shrinking the grey zone Sommerakademi e Munich, June 30 2016 Active surveillance: Shrinking the grey zone 3 rd FOIUS Tel Aviv, July 2016
Transcript of Active FOIUS surveillance: Shrinking the grey zone Sommerakademi … · 2016. 7. 31. · Klotz et...
-
Active
surveillance:
Shrinking the
grey zone
Sommerakademi
e
Munich, June 30
2016
Active surveillance:
Shrinking the grey zone
3rd FOIUS
Tel Aviv, July 2016
-
Active Surveillance for low risk PCa
What has changed?
(since Klotz, Choo J Urol 167: 1664, 2002)
• Greater recognition of overtreatment problem, acceptance of concept
• Nature of occult high grade disease
• Predictive value of baseline parameters
• Flaws of PSA kinetics as trigger
• Multiparametric MRI
• New modelling studies
• Randomized data on role of 5 ARIs
• Longer follow up,, ~2000 publications
-
• Molecular genetics of Gleason pattern 3 resembles normal cells in most cases; pattern 4
has many molecular hallmarks of cancer
• Metastatic potential of Gleason 3 ~ zero.
• The major limitation of current active surveillance strategies relates to pathologic miss of co-
existent higher grade cancer
• True biological grade progression occurs, but is uncommon
• Pre-histologic adverse genetic alterations exist
• MRI and molecular biomarkers enhance diagnostic accuracy (complementary)
2016: What we know
-
Gleason 3 lacks hallmarks of cancer
Characteristic/Pathway Gleason 3 Gleason 4
Expression of pro-proliferation embryonic, neuronal,
hematopoietic stem cell genes, EGF, EGFR
No Overexpressed
AKT pathway: MAP2K4, RALA, PHLPP, PML No Aberrant
HER2/neu No Amplified
Antigrowth signal insensitivity (Cyclin D2, CKDN1β) Expressed Absent
Resisting apoptosis: DAD1 Negative Strong Exp
BCL2 Mostly Neg. Upregulated
Absence of senescence: TMPRSS2-ERG ERG normal Increased
Sustained angiogenesis: VEGF Low Increased
Expression of other pro-angiogenic factors Normal Increased
Tissue invasion/metastasis markers (CXCR4, others) Normal Overexpressed
PTEN loss 10% > 90%
Clinical evidence of metastasis/mortality Absent Present
-
The clonal origin
of lethal prostate cancer Haffner M, Yegasubramanian et al, JCI, epub Oct 29 2913
-
In Vivo Imaging Reveals Extracellular Vesicle-Mediated
Phenocopying of Metastatic Behavior
Zomer A, Cell 2015, 161, 1046–1057
• Extra-cellular vesicles released by malignant tumor cells
taken up by less malignant cells located within the same and
within distant tumors
• These EVs carry mRNAs involved in migration and
metastasis.
• The RNA from more aggressive cells is incorporated and
induces aggressive behavior in the indolent cells
-
Toronto Surveillance Cohort
• 993 patients, median f/u of 8.9 years (0.5 – 19.8 years)
• Serial PSA, biopsy (no MRI until 2012)
• 78% low risk
• 22% patients intermediate risk (G7 or PSA > 10)
• 38% of these < 70 years
• Intervention for PSA DT < 3 years (until 2010), upgrading to Gleason 3 + ‘significant’ 4
• 30 patients have developed metastases
• 15 died of prostate cancer
• 4 died other causes, 11 alive with mets
-
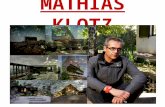
Intervention free survival in active
surveillance Klotz et al JCO 33(3):272-7 2015
-
Survival with AS Klotz et al JCO 33(3):272-7 2015 OS
CSS
-
OS and CSS: Low vs Intermediate risk
(Gleason 3+4, PSA >10) 67%
51% HR 2.13
HR 3.75 89%
97%
Overall Survival
Cause Specific Survival
-
Intermediate risk group: Baseline Gleason
score, not PSA, predicted for mets
Baseline PSA >10 vs GS 7, Met free survival
77%
93%
-
Recursive partitioning analysis: Metastasis
free survival by risk group
-
Hopkins AS long term outcome: Overall mortality and Pca
mortality Tosoian J, Carter B et al. JCO.2015
©
Pca
mortality
0.5% at
15 years
-
Sunnybrook Johns Hopkins
Eligibility All Gleason 6, PSA
-
Active surveillance
• Initial Bx and risk categorization
• Comorbidity and life expectancy
• Patient preference
• Re—biopsy to improve accuracy of risk classification
• Periodic re-evaluation for change in risk
• Intervention:
• Change in risk category
• PSA anxiety
• Patient preference
• Reduce uncertainty of eligibility determination
• MRI/biomarker instead of 2nd biopsy
• Improved patient selection:
• MRI negative/favorable score : The new very low risk
• MRI target/high score: greater acceptance of treatment
• Serial imaging/molecular monitoring with modulated interval
• More rational decision for intervention
Current Paradigm Image based/
Molecular paradigm
-
PCa: Traditional large grey zone
Gleason 6, PSA < 10 Everything else
T1a
-
The new black, white, and grey zones
Gleason >= 7 with
> 10% Gleason 4
The ‘grey zone’:
• Extensive Gleason 6
• Gleason 6 in men < 50 yrs
• Gleason 7 with < 10% Gleason 4
AS: Gleason 6,
non-extensive
disease, non-
suspicious MRI, low
PSA density
• PiRADS 4-5 with low
grade cancer on targeted
biopsy,
• high PSAD
-
• Gleason pattern 3 is a non-metastasizing lesion lacking most hallmarks of cancer
• Presence of any Gleason 4 at baseline confers significant increased risk of metastasis at 15
years
• The ‘grey zone’ has shifted and shrunk
• Small volume Gleason 6 no longer grey zone
• Today:
• High volume Gleason 6 in young patient
• Gleason 3+ pattern 4 < 10%
• Small volume Gleason 3+4 with negative MRI or genomic assay
• Most Gleason 7 should be treated
Conclusions:








![Bapi jco[1]](https://static.fdocuments.net/doc/165x107/55587609d8b42aaa7e8b5447/bapi-jco1.jpg)







