Actinomycosis of Distal Phalanx Twenty Years after Flap ...actinomycosis of distal phalanx of finger...
3
48 Malaysian Orthopaedic Journal 2018 Vol 12 No 1 Prashant N, et al ABSTRACT Actinomycosis is a chronic granulomatous suppurative infection caused by anaerobic bacteria from genus Actinomyces which are normal flora of mouth, colon and vagina. Actinomycosis of upper extremity is rare. We report a case of actinomycosis of the distal phalanx of finger many years after flap reconstruction. The patient presented with two months’ history of chronic discharging sinus from the tip of his right index finger, which had sustained a degloving injury 20 years previously. It had been treated with an anterior chest wall flap which had healed uneventfully but was bulky due to excess tissue from the donor site. Radiograph revealed osetomyelitis changes of distal phalanx. Debulking surgery with curettage of the distal phalanx was done. Wound healing was uneventful. He was treated with six weeks of metronidazole and ciprofloxacin. The discharge from the distal phalanx cultured actinomycosis odontolyticus. Histopathology of the debrided tissue showed chronic inflammation. As far as we are aware, there are no reports of actinomycosis in a flap involving the finger treated previously with a chest wall skin flap. The infection was probably dormant for many years before manifesting as a discharging sinus. Although the finger flap was bulky, it was not problematic until it started to have serous discharge. With a thorough debridement of all infected tissue, six weeks of antibiotic was adequate. Ciprofloxacin was prescribed based on discharge culture sensitivity. Metronidazole was added as actinomycosis is anaerobic. Response was prompt as patient was not immunocompromised. At follow-up six months post-surgery the finger had recovered with good function. If not for the discharging sinus, patient would probably have tolerated his bulky finger for the rest of his life. Key Words: actinomycosis, flap surgery, chronic hand infections, osteomyelitis phalanx INTRODUCTION Actinomycosis is a chronic granulomatous suppurative infection caused by anaerobic bacteria from genus Actinomyces which is a normal flora of mouth, colon and vagina 1 . Actinomycosis of the extremity is rare, even more so in the upper extremity 2 . We report an interesting case of actinomycosis of distal phalanx of finger many years after flap reconstruction (Fig. 1a, b). CASE REPORT Our patient presented with a chronic discharging sinus from the tip of his right index finger (Fig. 1c). Interestingly, this finger had sustained a degloving injury 20 years earlier and had been treated with an anterior chest wall flap. After two weeks, the flap was detached from the chest wall and the wound over the right index finger healed uneventfully; however, the finger was bulky due to excess tissue from the donor site. A month prior to presentation, the index finger started discharging serous fluid from the tip. There was no significant history of trauma at this time which preceeded the sinus formation. Radiograph of hand revealed osetomyelitis changes over the distal phalanx of the index finger (Fig. 1d). ESR was 78 mm/hr, suggestive of chronic inflammation. He underwent a debulking surgery with curettage of the distal phalanx (Fig. 2). Intraoperatively, we noted the osteomyelitic changes in the bone surrounded by dense inflamed tissue which was further surrounded by relatively normal looking fatty tissue, probably form the donor flap. The fingertip was debulked to give it a more acceptable appearance. The wound healed within two weeks as expected and he was treated with six weeks of oral antibiotics. Actinomycosis odontolyticu was cultured from the tissue from the distal phalanx. The histopathology of the debrided tissue showed non-specific chronic inflammatory process. At six months, the index finger had completely healed with no Actinomycosis of Distal Phalanx Twenty Years after Flap Reconstruction of Index Finger: A Case Report Prashant N, MMed Orth (USM), Azuhairy A, MMed Orth (USM) Orthopaedic Oncology Unit, Hospital Pulau Pinang, Georgetown, Malaysia This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited Date of submission: 30th April 2017 Date of acceptance: 25th February 2018 Corresponding Author: Prashant Narhari, Orthopaedic Oncology Unit, Hospital Pulau Pinang, Georgetown, Penang, Malaysia Email: [email protected] doi: http://dx.doi.org/10.5704/MOJ.1803.011
Transcript of Actinomycosis of Distal Phalanx Twenty Years after Flap ...actinomycosis of distal phalanx of finger...

48
Malaysian Orthopaedic Journal 2018 Vol 12 No 1 Prashant N, et al
ABSTRACTActinomycosis is a chronic granulomatous suppurativeinfection caused by anaerobic bacteria from genusActinomyces which are normal flora of mouth, colon andvagina. Actinomycosis of upper extremity is rare. We reporta case of actinomycosis of the distal phalanx of finger manyyears after flap reconstruction. The patient presented withtwo months’ history of chronic discharging sinus from the tipof his right index finger, which had sustained a deglovinginjury 20 years previously. It had been treated with ananterior chest wall flap which had healed uneventfully butwas bulky due to excess tissue from the donor site.Radiograph revealed osetomyelitis changes of distalphalanx. Debulking surgery with curettage of the distalphalanx was done. Wound healing was uneventful. He wastreated with six weeks of metronidazole and ciprofloxacin.The discharge from the distal phalanx culturedactinomycosis odontolyticus. Histopathology of the debridedtissue showed chronic inflammation. As far as we are aware,there are no reports of actinomycosis in a flap involving thefinger treated previously with a chest wall skin flap. Theinfection was probably dormant for many years beforemanifesting as a discharging sinus. Although the finger flapwas bulky, it was not problematic until it started to haveserous discharge. With a thorough debridement of allinfected tissue, six weeks of antibiotic was adequate.Ciprofloxacin was prescribed based on discharge culturesensitivity. Metronidazole was added as actinomycosis isanaerobic. Response was prompt as patient was notimmunocompromised. At follow-up six months post-surgerythe finger had recovered with good function. If not for thedischarging sinus, patient would probably have tolerated hisbulky finger for the rest of his life.
Key Words: actinomycosis, flap surgery, chronic hand infections,osteomyelitis phalanx
INTRODUCTIONActinomycosis is a chronic granulomatous suppurativeinfection caused by anaerobic bacteria from genusActinomyces which is a normal flora of mouth, colon andvagina1. Actinomycosis of the extremity is rare, even more soin the upper extremity2. We report an interesting case ofactinomycosis of distal phalanx of finger many years afterflap reconstruction (Fig. 1a, b).
CASE REPORTOur patient presented with a chronic discharging sinus fromthe tip of his right index finger (Fig. 1c). Interestingly, thisfinger had sustained a degloving injury 20 years earlier andhad been treated with an anterior chest wall flap. After twoweeks, the flap was detached from the chest wall and thewound over the right index finger healed uneventfully;however, the finger was bulky due to excess tissue from thedonor site. A month prior to presentation, the index fingerstarted discharging serous fluid from the tip. There was nosignificant history of trauma at this time which preceeded thesinus formation. Radiograph of hand revealed osetomyelitischanges over the distal phalanx of the index finger (Fig. 1d).ESR was 78 mm/hr, suggestive of chronic inflammation.
He underwent a debulking surgery with curettage of thedistal phalanx (Fig. 2). Intraoperatively, we noted theosteomyelitic changes in the bone surrounded by denseinflamed tissue which was further surrounded by relativelynormal looking fatty tissue, probably form the donor flap.The fingertip was debulked to give it a more acceptableappearance. The wound healed within two weeks as expectedand he was treated with six weeks of oral antibiotics.Actinomycosis odontolyticu was cultured from the tissuefrom the distal phalanx. The histopathology of the debridedtissue showed non-specific chronic inflammatory process. Atsix months, the index finger had completely healed with no
Actinomycosis of Distal Phalanx Twenty Years after FlapReconstruction of Index Finger: A Case Report
Prashant N, MMed Orth (USM), Azuhairy A, MMed Orth (USM)
Orthopaedic Oncology Unit, Hospital Pulau Pinang, Georgetown, Malaysia
This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited
Date of submission: 30th April 2017Date of acceptance: 25th February 2018
Corresponding Author: Prashant Narhari, Orthopaedic Oncology Unit, Hospital Pulau Pinang, Georgetown, Penang, MalaysiaEmail: [email protected]
doi: http://dx.doi.org/10.5704/MOJ.1803.011
11-CR3-078_OA1 3/28/18 12:19 AM Page 48

Actinomycosis of Distal Phalanx
49
sign of residual infection and with improved functioncompared to before surgery (Fig. 3).
DISCUSSIONInfection due to actinomycosis is rare and involvement of theupper limb is even more rare2. As far as we are aware, thereis no report of actinomycosis in a previous skin flapreconstruction involving the finger. We believe the infectionhas been indolent for some time and manifested as a sinusmany years later. As our patient was using his finger for mostdaily activities with very little limitation of function, webelieve he would have contracted the infection during hisdaily use of the finger. Although the finger was bulky, ourpatient did not find it to be a problem until it started to haveserous discharge from the tip of the finger. As the radiographsuggested osteomyelitis changes over the tip of distalphalanx, debridement and curettage of the bone becamenecessary and the opportunity was taken to debulk the excesstissue covering the index finger at the same time. Mostliterature on the infection propose antibiotics for a prolongedperiod of three months to a year1,2; however we instituted theantibiotic therapy for six weeks only. We believed with athrough debridement of all infected tissue the six weeksduration was adequate. The choice of antibiotic wasciprofloxacin based on culture sensitivity result.Metronidazole was added as actinomycosis is an anaerobicbacterial infection. Response was prompt as our patient washealthy and most importantly not immunocompromised. Webelieved the longer antibiotic therapy of at least three monthswas probably appropriate for immunocompromised patients
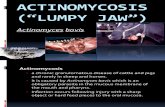
Fig. 1: Preoperative images of (a) Dorsal, (b) Volar, (c) Fingertipand (d) Radiograph of the index finger with bulky softtissue from previous skin flap.
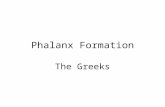
Fig. 3: Volar view of index finger a year after surgery showingsignificantly less bulky soft tissue as a result of debulking.
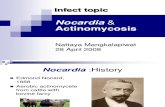
Fig. 2: Intraoperative findings of dense fibrous tissuesurrounding the osteomyelitic phalanx.
(a) (b)
(c) (d)
11-CR3-078_OA1 3/28/18 12:19 AM Page 49

Malaysian Orthopaedic Journal 2018 Vol 12 No 1 Prashant N, et al
50
and in cases where the debridement was not done or therewas a possibility of residual infection post-debridement.
On our follow-up a year post-surgery the finger wound hadhealed completely with improvement in the functioncompared to before debridement, with almost full range ofmotion. If not for the actinomycosis infection presenting
with the discharging sinus, this patient probably would havejust tolerated his bulky finger for the rest of his life.
CONFLICT OF INTERESTThe authors declare no conflicts of interest.
REFERENCES
1. Fayman M, Schein M, Braun S. A foreign body related actinomycosis of finger. J Hand Surg Am. 1985; 10(3): 411-2.2. Altman D, Lubahn JD, Kuhn PJ. A case report and review of mycetoma of the hand: a diagnostic and therapeutic challenge. J
Hand Surg Am. 1994; 19(6): 998-1002.
11-CR3-078_OA1 3/28/18 12:19 AM Page 50