Acetabulum and Pelvis
57
2777 ACETABULAR FRACTURES e treatment of acetabular fractures is a complex area of orthopaedics that is being continually refined. It involves a definite learning curve, probably best documented in a report by Matta and Merritt of the first 100 acetabular fractures treated operatively by Matta. Grouping the surgical reduc- tions chronologically in groups of 20 clearly showed that experience improved the ability to avoid unsatisfactory reductions and to perform anatomical reductions (Fig. 56-1). Kebaish, Roy, and Rennie demonstrated this same concept by comparing the reductions obtained by experienced pelvic trauma surgeons with those obtained by less experienced sur- geons, who had a much lower rate of anatomical reduction (Fig. 56-2). INITIAL TREATMENT Acetabular fractures generally are caused by high-energy trauma, and associated injuries are frequent. Management of the entire patient should follow accepted Advanced Trauma Life Support (ATLS) protocol, with orthopaedic treatment of the acetabular fracture appropriately integrated into the treatment plan. In general, operative treatment of an acetabular fracture should not be performed as an emer- gency except when it is part of open fracture management or is performed for a fracture associated with an irreducible dislocation of the hip. In the latter case, urgent open reduc- tion of the hip dislocation followed by treatment of the asso- ciated fracture is required to decrease the risk of complications of osteonecrosis and ongoing cartilaginous damage to the femoral head. Closed reduction of hip dislocations should be per- formed with sedation in the emergency department or with general anesthesia and fluoroscopy. e patient then can be placed in skeletal traction if necessary to maintain reduction and possibly slight distraction of the hip while the other acute injuries are treated and radiographic studies of the pelvis are obtained. Admittedly, not all patients require skel- etal traction if the hip is stable with the patient on an abduc- tion wedge pillow. However, we tend to place most patients with potentially operative fractures in skeletal traction of 20 to 35 pounds while they are in the resuscitation area to mini- mize further injury to the femoral head by the sharp fracture surfaces. We prefer the use of distal femoral traction pins to facilitate knee flexion during subsequent surgery if traction is used. Historically, central fracture-dislocation of the hip was used to describe any acetabular fracture with medial sublux- ation of the femoral head. Although this terminology has been replaced with more descriptive fracture classification systems, a true central fracture-dislocation, with the femoral head completely dislocated medially into the pelvis is an unusual injury that requires urgent treatment (Fig. 56-3). e femoral head can be locked between the fracture fragments, making reduction extremely difficult. Closed reduction with general anesthesia and fluoroscopic assistance should be attempted. Aſter reduction, the femoral head is extremely unstable and will easily redisplace into the pelvis if skeletal traction is not maintained. If closed reduction of a hip dislocation associated with an acetabular fracture is unsuccessful, the immediate treat- ment of the hip depends on the experience of the surgeon. A rapid CT scan of the pelvis with 3-mm cuts can demonstrate the obstruction to reduction of the hip dislocation and the acetabular fracture pattern, which will allow formulation of an operative plan for open reduction and internal fixation (ORIF) (Fig. 56-4). If indicated, transfer to a facility capable of managing such injuries should be done promptly. ANATOMY e acetabulum can be described as an incomplete hemi- spherical socket with an inverted horseshoe-shaped articular FRACTURES OF ACETABULUM AND PELVIS James L. Guyton • Edward A. Perez CHAPTER ACETABULAR FRACTURES 2777 INITIAL TREATMENT 2777 ANATOMY 2777 RADIOGRAPHIC EVALUATION 2780 CLASSIFICATION 2783 TREATMENT 2784 Indications for Nonoperative Treatment 2784 Indications for Operative Treatment 2787 Timing of Surgery 2788 Choice of Surgical Approach 2788 Specific Fracture Patterns 2789 POSTOPERATIVE CARE 2795 OUTCOME AND COMPLICATIONS 2795 TOTAL HIP ARTHROPLASTY AS TREATMENT OF ACETABULAR FRACTURE 2799 PELVIC FRACTURES 2799 INITIAL MANAGEMENT 2800 ANATOMY 2801 CLASSIFICATION 2801 RADIOGRAPHIC EVALUATION 2805 TREATMENT 2809 Initial Treatment 2809 Reconstructive Phase 2814 56
-
Upload
bipin-solanki -
Category
Documents
-
view
17 -
download
1
Transcript of Acetabulum and Pelvis
2777
ACETABULAR FRACTURES
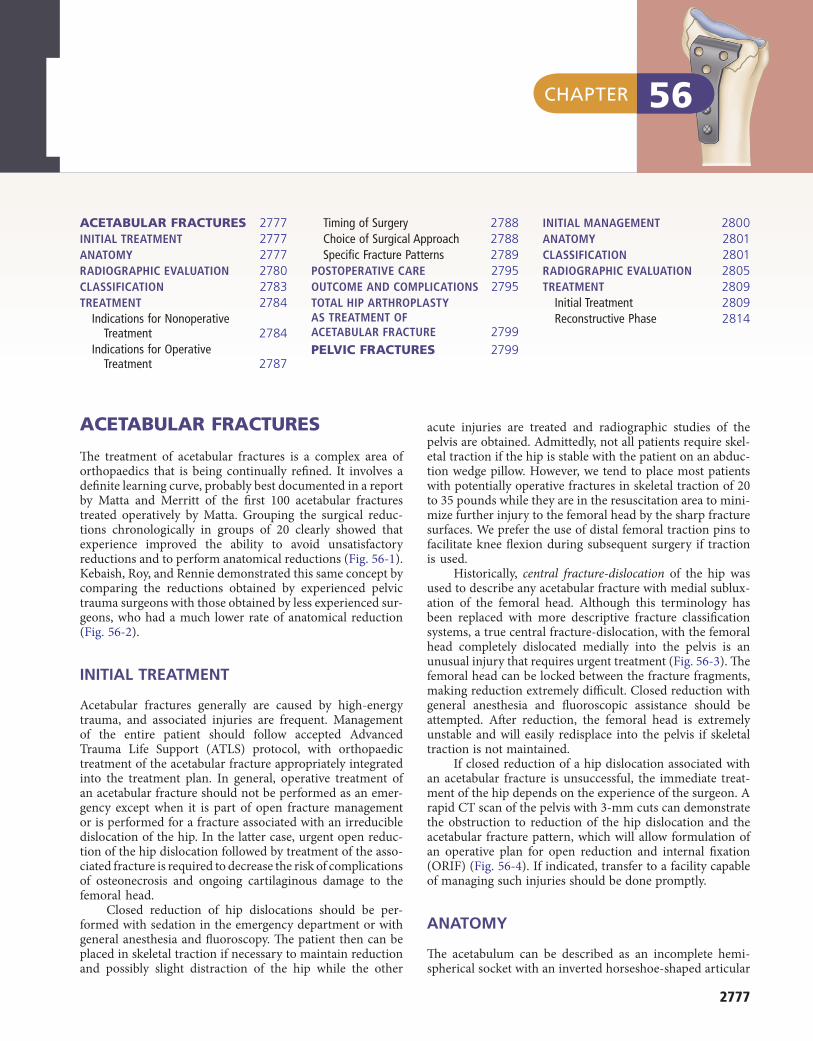
The treatment of acetabular fractures is a complex area of orthopaedics that is being continually refined. It involves a definite learning curve, probably best documented in a report by Matta and Merritt of the first 100 acetabular fractures treated operatively by Matta. Grouping the surgical reduc-tions chronologically in groups of 20 clearly showed that experience improved the ability to avoid unsatisfactory reductions and to perform anatomical reductions (Fig. 56-1). Kebaish, Roy, and Rennie demonstrated this same concept by comparing the reductions obtained by experienced pelvic trauma surgeons with those obtained by less experienced sur-geons, who had a much lower rate of anatomical reduction (Fig. 56-2).
INITIAL TREATMENT
Acetabular fractures generally are caused by high-energy trauma, and associated injuries are frequent. Management of the entire patient should follow accepted Advanced Trauma Life Support (ATLS) protocol, with orthopaedic treatment of the acetabular fracture appropriately integrated into the treatment plan. In general, operative treatment of an acetabular fracture should not be performed as an emer-gency except when it is part of open fracture management or is performed for a fracture associated with an irreducible dislocation of the hip. In the latter case, urgent open reduc-tion of the hip dislocation followed by treatment of the asso-ciated fracture is required to decrease the risk of complications of osteonecrosis and ongoing cartilaginous damage to the femoral head.
Closed reduction of hip dislocations should be per-formed with sedation in the emergency department or with general anesthesia and fluoroscopy. The patient then can be placed in skeletal traction if necessary to maintain reduction and possibly slight distraction of the hip while the other
acute injuries are treated and radiographic studies of the pelvis are obtained. Admittedly, not all patients require skel-etal traction if the hip is stable with the patient on an abduc-tion wedge pillow. However, we tend to place most patients with potentially operative fractures in skeletal traction of 20 to 35 pounds while they are in the resuscitation area to mini-mize further injury to the femoral head by the sharp fracture surfaces. We prefer the use of distal femoral traction pins to facilitate knee flexion during subsequent surgery if traction is used.
Historically, central fracture-dislocation of the hip was used to describe any acetabular fracture with medial sublux-ation of the femoral head. Although this terminology has been replaced with more descriptive fracture classification systems, a true central fracture-dislocation, with the femoral head completely dislocated medially into the pelvis is an unusual injury that requires urgent treatment (Fig. 56-3). The femoral head can be locked between the fracture fragments, making reduction extremely difficult. Closed reduction with general anesthesia and fluoroscopic assistance should be attempted. After reduction, the femoral head is extremely unstable and will easily redisplace into the pelvis if skeletal traction is not maintained.
If closed reduction of a hip dislocation associated with an acetabular fracture is unsuccessful, the immediate treat-ment of the hip depends on the experience of the surgeon. A rapid CT scan of the pelvis with 3-mm cuts can demonstrate the obstruction to reduction of the hip dislocation and the acetabular fracture pattern, which will allow formulation of an operative plan for open reduction and internal fixation (ORIF) (Fig. 56-4). If indicated, transfer to a facility capable of managing such injuries should be done promptly.
ANATOMY
The acetabulum can be described as an incomplete hemi-spherical socket with an inverted horseshoe-shaped articular
FRACTURES OF ACETABULUM AND PELVISJames L. Guyton • Edward A. Perez
CHAPTER
ACETABULAR FRACTURES 2777INITIAL TREATMENT 2777ANATOMY 2777RADIOGRAPHIC EVALUATION 2780CLASSIFICATION 2783TREATMENT 2784
Indications for Nonoperative Treatment 2784
Indications for Operative Treatment 2787
Timing of Surgery 2788Choice of Surgical Approach 2788Specific Fracture Patterns 2789
POSTOPERATIVE CARE 2795OUTCOME AND COMPLICATIONS 2795TOTAL HIP ARTHROPLASTY AS TREATMENT OF ACETABULAR FRACTURE 2799
PELVIC FRACTURES 2799
INITIAL MANAGEMENT 2800ANATOMY 2801CLASSIFICATION 2801RADIOGRAPHIC EVALUATION 2805TREATMENT 2809
Initial Treatment 2809Reconstructive Phase 2814
56
PART XV FRACTURES AND DISLOCATIONS IN ADULTS2778
FIGURE 56-1 A, Percentage of anatomical reductions per group of 20 for first 100 cases. B, Number of unsatisfactory reductions of dis-placed acetabular fractures per group of 20 for Matta’s first 100 surgical cases. (From Matta JM, Merritt PO: Displaced acetabular frac-tures, Clin Orthop Relat Res 230:83, 1988.)
1–20 20–40 40–60 60–80 80–1000
25
50
75
100
1–20 20–40 40–60 60–80 80–100
A BGroups of 20 Groups of 20
% a
nato
mic
al r
educ
tions
No.
uns
atis
fact
ory
redu
ctio
ns
4
5
3
2
1
0
FIGURE 56-2 Quality of reduction of acetabular fractures obtained by experienced pelvic trauma surgeons compared with surgeons with less experience. Mild incongruency is defined as up to 4 mm of fracture displacement; moderate incongruency, as 4 to 10 mm; and severe incongruency, as more than 10 mm. (From Kebaish AS, Roy A, Rennie W: Displaced acetabular fractures: long-term follow-up, J Trauma 31:1539, 1991.)
Anatomical Mild Moderate Severe
Experienced surgeonLess experienced surgeon
100
80
60
40
20
0
FIGURE 56-3 Transverse acetabular fracture with true central fracture-dislocation; intrapelvic femoral head can become locked between superior and inferior fracture fragments.
FIGURE 56-4 Anteroposterior pelvic radiograph (A) and CT scan (B) of irreducible hip dislocation with posterior wall acetabular fracture. Posterior wall fragment is incarcerated, blocking reduction.
BA
CHAPTER 56 FRACTURES OF ACETABULUM AND PELVIS 2779
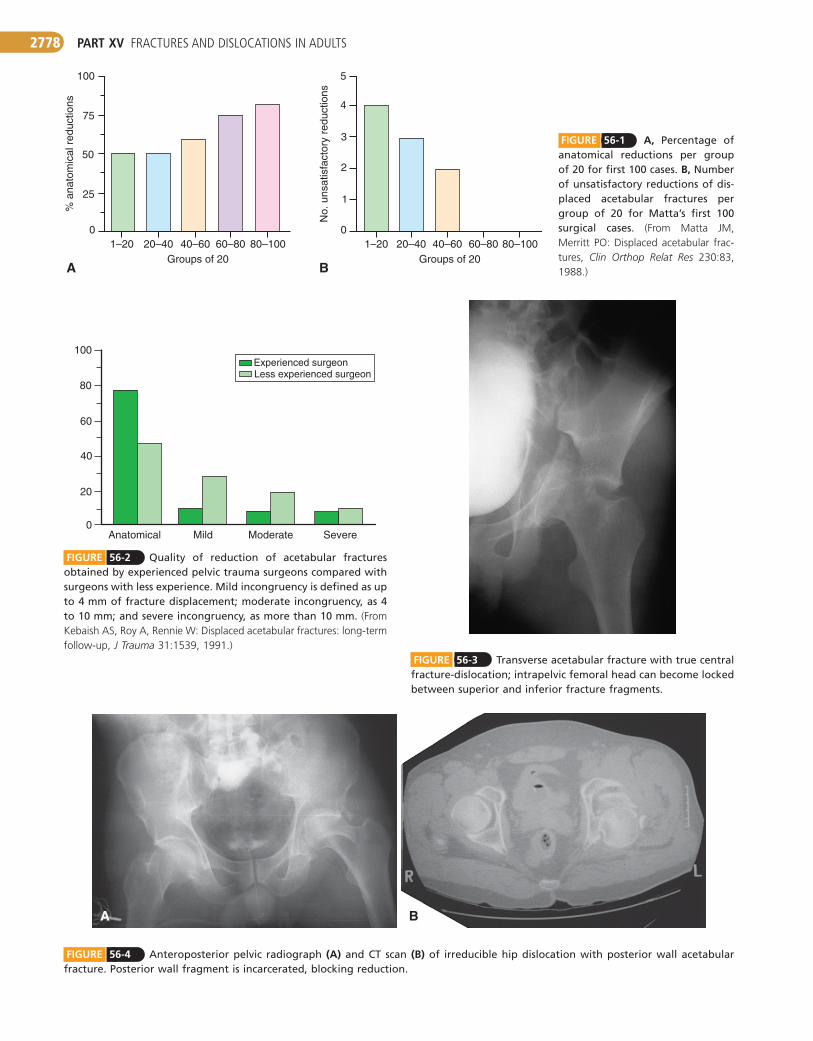
The neurovascular structures passing through the pelvis are at risk during the original injury and subsequent treat-ment, and the various surgical approaches are designed around these structures. The sciatic nerve exiting the greater sciatic notch inferior to the piriformis muscle frequently is injured with posterior fracture-dislocations of the hip and fractures with posterior displacement (Fig. 56-8). The func-tioning of both the tibial and common peroneal components of the sciatic nerve must be carefully documented in the emergency department and after subsequent interventions (including reduction of a hip dislocation and changes in trac-tion). The sciatic nerve has frequent variation in its relation-ship to the piriformis muscle as it exits the sciatic notch, with common separation of tibial and peroneal branches at this level. The superior gluteal artery and nerve exit the greater sciatic notch at its most superior aspect and can be tethered to the bone at this level by variable fascial attachments. Frac-tures that enter the superior portion of the greater sciatic notch can be associated with significant hemorrhage, possibly requiring angiography with embolization of the superior gluteal artery. Before performance of the extensile approaches that rely on a superior gluteal artery–based vascular pedicle,
surface surrounding the nonarticular cotyloid fossa. This articular socket is composed of and supported by two columns of bone, described by Letournel and Judet as an inverted Y (Fig. 56-5). The anterior column is composed of the anterior half of the iliac crest, the iliac spines, the anterior half of the acetabulum, and the pubis. The posterior column is the ischium, the ischial spine, the posterior half of the acetabu-lum, and the dense bone forming the sciatic notch. The shorter posterior column ends at its intersection with the anterior column at the top of the sciatic notch. The column concept is used in classification of these fractures and is central to the discussion of fracture patterns, operative approaches, and internal fixation.
The dome, or roof, of the acetabulum is the weight-bearing portion of the articular surface that supports the femoral head (Fig. 56-6). Anatomical restoration of the dome with concentric reduction of the femoral head beneath this dome is the goal of both operative and nonoperative treat-ment. The quadrilateral surface is the flat plate of bone forming the lateral border of the true pelvic cavity and thus lying adjacent to the medial wall of the acetabulum (Fig. 56-7). The iliopectineal eminence is the prominence in the anterior column that lies directly over the femoral head. Both the quadrilateral surface and the iliopectineal eminence are thin and adjacent to the femoral head, limiting the types of fixation that can be used in these regions.
FIGURE 56-5 Two-column concept of Letournel and Judet used in classification of acetabular fractures (see text).
Anteriorcolumn Posterior
columnPosterior
column
FIGURE 56-6 Superior dome of acetabulum.
Dome ofacetabulum
FIGURE 56-7 A, Iliopectineal eminence overlies dome of ace-tabulum. B, Quadrilateral surface lies adjacent to medial wall of acetabulum.
BA
Iliopectinealeminence
Quadrilateralsurface
FIGURE 56-8 Piriformis divides greater sciatic notch and is key to this region. Sciatic nerve is shown leaving pelvis below this muscle; superior gluteal artery, vein, and nerve are above it.
Piriformis
Sciatic nerve
Superior glutealartery and nerve
PART XV FRACTURES AND DISLOCATIONS IN ADULTS2780
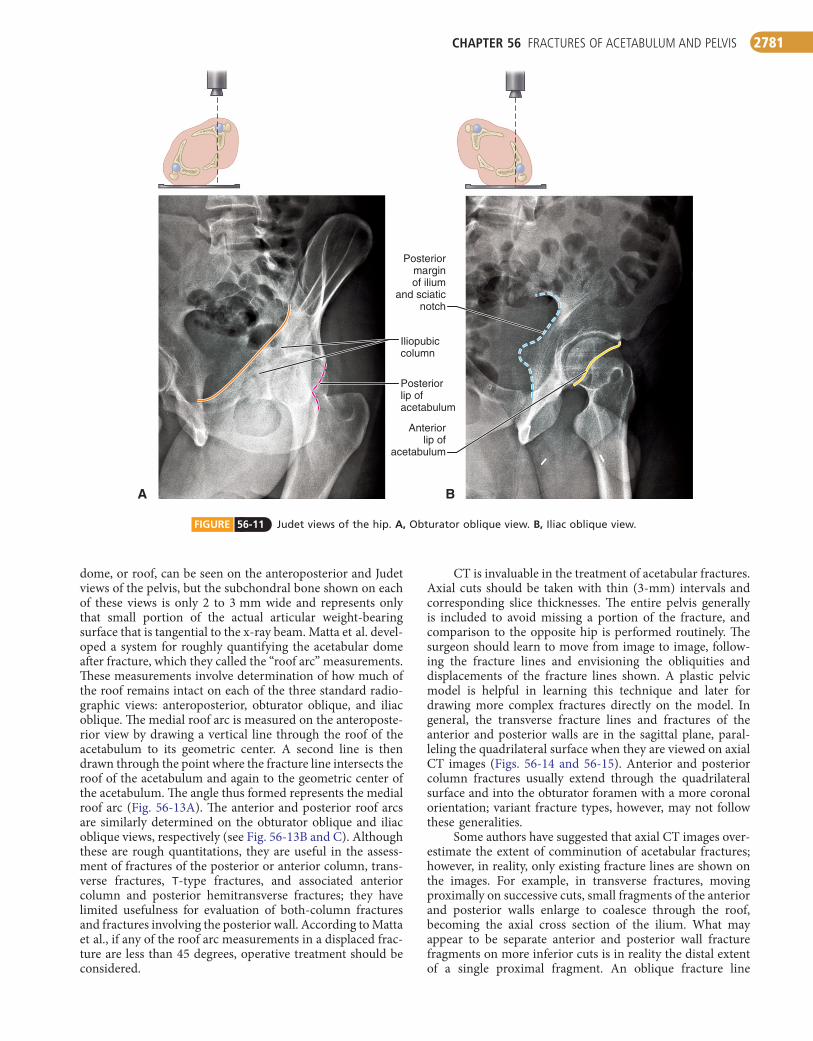
the anterior column disrupt the iliopectineal line, whereas fractures that traverse the posterior column disrupt the iliois-chial line. Each fracture pattern in the classification of Letournel and Judet has typical radiographic characteristics with respect to the disruption or intactness of the radio-graphic landmarks, as shown for a posterior column fracture in Figure 56-12. Evaluation of the various fracture patterns from the standard radiographs requires an understanding of the three-dimensional implications of the status of each of the radiographic landmarks as well as a three-dimensional grasp of pelvic bony anatomy and the possible variations of fracture lines within a given fracture pattern. In the operating room, the three standard views can be obtained with fluo-roscopy. The restoration of the radiographic landmarks is a guide to the adequacy of fracture reduction. Borrelli et al. described the use of Judet view radiographs generated from CT data that they found to be as good as or better than conventional radiographs in identifying fracture character-istics and classification.
The anatomical dome is a three-dimensional structure composed of subchondral bone and its overlying cartilage that articulates with the weight-bearing portion of the femoral head. Multiple studies have concluded that the single most important factor affecting long-term outcome in both opera-tively and nonoperatively treated acetabular fractures is maintenance of a concentric reduction of the femoral head beneath an intact or anatomically reconstructed dome. The
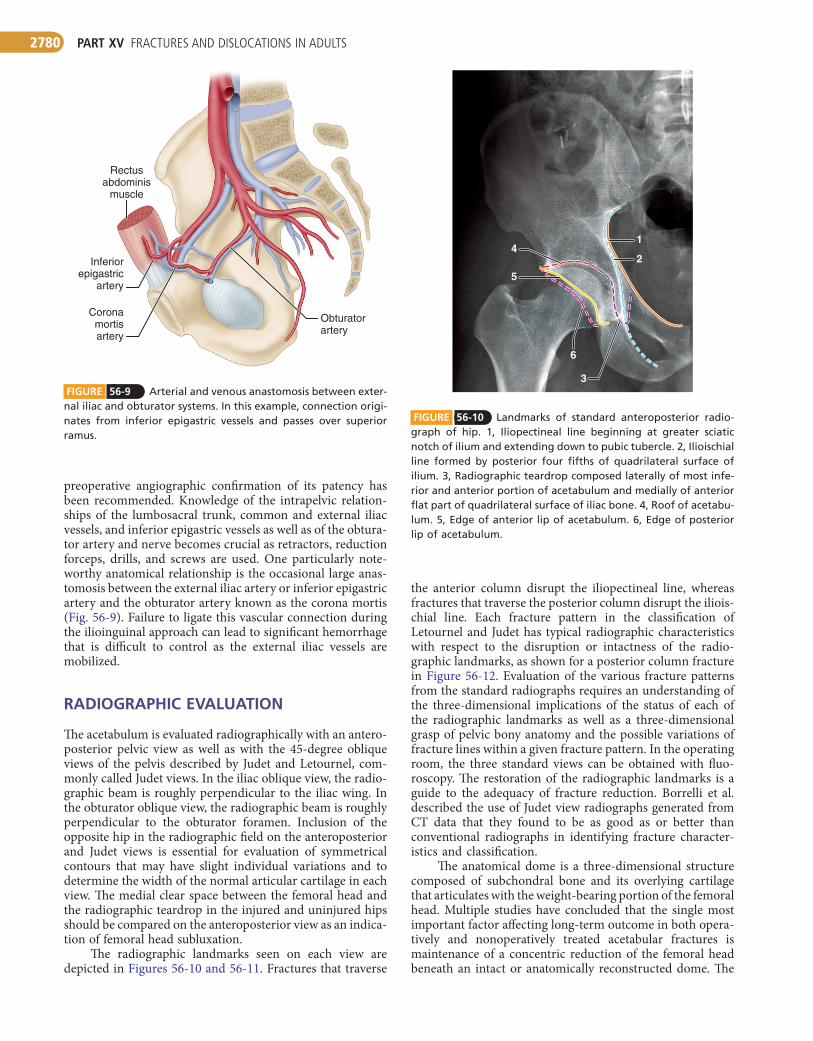
FIGURE 56-9 Arterial and venous anastomosis between exter-nal iliac and obturator systems. In this example, connection origi-nates from inferior epigastric vessels and passes over superior ramus.
Rectusabdominis
muscle
Inferiorepigastric
artery
Coronamortisartery
Obturatorartery
FIGURE 56-10 Landmarks of standard anteroposterior radio-graph of hip. 1, Iliopectineal line beginning at greater sciatic notch of ilium and extending down to pubic tubercle. 2, Ilioischial line formed by posterior four fifths of quadrilateral surface of ilium. 3, Radiographic teardrop composed laterally of most infe-rior and anterior portion of acetabulum and medially of anterior flat part of quadrilateral surface of iliac bone. 4, Roof of acetabu-lum. 5, Edge of anterior lip of acetabulum. 6, Edge of posterior lip of acetabulum.
1
2
3
4
5
6
preoperative angiographic confirmation of its patency has been recommended. Knowledge of the intrapelvic relation-ships of the lumbosacral trunk, common and external iliac vessels, and inferior epigastric vessels as well as of the obtura-tor artery and nerve becomes crucial as retractors, reduction forceps, drills, and screws are used. One particularly note-worthy anatomical relationship is the occasional large anas-tomosis between the external iliac artery or inferior epigastric artery and the obturator artery known as the corona mortis (Fig. 56-9). Failure to ligate this vascular connection during the ilioinguinal approach can lead to significant hemorrhage that is difficult to control as the external iliac vessels are mobilized.
RADIOGRAPHIC EVALUATION
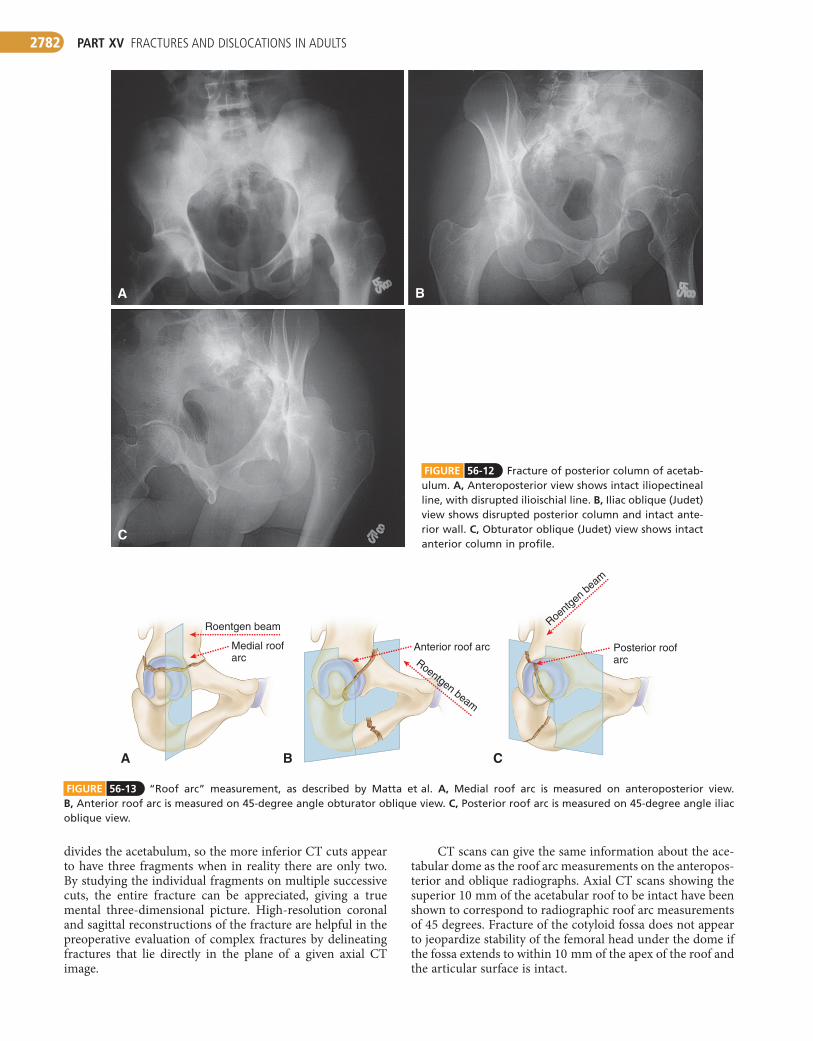
The acetabulum is evaluated radiographically with an antero-posterior pelvic view as well as with the 45-degree oblique views of the pelvis described by Judet and Letournel, com-monly called Judet views. In the iliac oblique view, the radio-graphic beam is roughly perpendicular to the iliac wing. In the obturator oblique view, the radiographic beam is roughly perpendicular to the obturator foramen. Inclusion of the opposite hip in the radiographic field on the anteroposterior and Judet views is essential for evaluation of symmetrical contours that may have slight individual variations and to determine the width of the normal articular cartilage in each view. The medial clear space between the femoral head and the radiographic teardrop in the injured and uninjured hips should be compared on the anteroposterior view as an indica-tion of femoral head subluxation.
The radiographic landmarks seen on each view are depicted in Figures 56-10 and 56-11. Fractures that traverse
CHAPTER 56 FRACTURES OF ACETABULUM AND PELVIS 2781
FIGURE 56-11 Judet views of the hip. A, Obturator oblique view. B, Iliac oblique view.
BA
Iliopubiccolumn
Posteriormarginof ilium
and sciaticnotch
Posteriorlip ofacetabulum
Anteriorlip of
acetabulum
dome, or roof, can be seen on the anteroposterior and Judet views of the pelvis, but the subchondral bone shown on each of these views is only 2 to 3 mm wide and represents only that small portion of the actual articular weight-bearing surface that is tangential to the x-ray beam. Matta et al. devel-oped a system for roughly quantifying the acetabular dome after fracture, which they called the “roof arc” measurements. These measurements involve determination of how much of the roof remains intact on each of the three standard radio-graphic views: anteroposterior, obturator oblique, and iliac oblique. The medial roof arc is measured on the anteroposte-rior view by drawing a vertical line through the roof of the acetabulum to its geometric center. A second line is then drawn through the point where the fracture line intersects the roof of the acetabulum and again to the geometric center of the acetabulum. The angle thus formed represents the medial roof arc (Fig. 56-13A). The anterior and posterior roof arcs are similarly determined on the obturator oblique and iliac oblique views, respectively (see Fig. 56-13B and C). Although these are rough quantitations, they are useful in the assess-ment of fractures of the posterior or anterior column, trans-verse fractures, T-type fractures, and associated anterior column and posterior hemitransverse fractures; they have limited usefulness for evaluation of both-column fractures and fractures involving the posterior wall. According to Matta et al., if any of the roof arc measurements in a displaced frac-ture are less than 45 degrees, operative treatment should be considered.
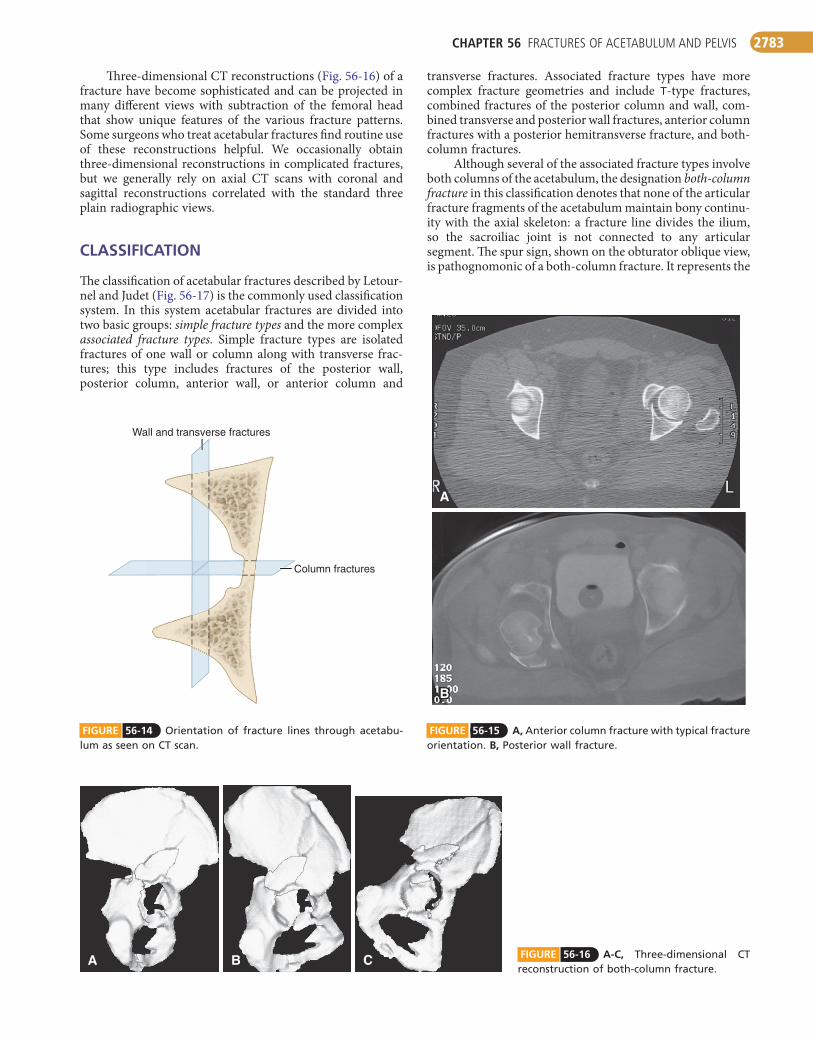
CT is invaluable in the treatment of acetabular fractures. Axial cuts should be taken with thin (3-mm) intervals and corresponding slice thicknesses. The entire pelvis generally is included to avoid missing a portion of the fracture, and comparison to the opposite hip is performed routinely. The surgeon should learn to move from image to image, follow-ing the fracture lines and envisioning the obliquities and displacements of the fracture lines shown. A plastic pelvic model is helpful in learning this technique and later for drawing more complex fractures directly on the model. In general, the transverse fracture lines and fractures of the anterior and posterior walls are in the sagittal plane, paral-leling the quadrilateral surface when they are viewed on axial CT images (Figs. 56-14 and 56-15). Anterior and posterior column fractures usually extend through the quadrilateral surface and into the obturator foramen with a more coronal orientation; variant fracture types, however, may not follow these generalities.
Some authors have suggested that axial CT images over-estimate the extent of comminution of acetabular fractures; however, in reality, only existing fracture lines are shown on the images. For example, in transverse fractures, moving proximally on successive cuts, small fragments of the anterior and posterior walls enlarge to coalesce through the roof, becoming the axial cross section of the ilium. What may appear to be separate anterior and posterior wall fracture fragments on more inferior cuts is in reality the distal extent of a single proximal fragment. An oblique fracture line
PART XV FRACTURES AND DISLOCATIONS IN ADULTS2782
CT scans can give the same information about the ace-tabular dome as the roof arc measurements on the anteropos-terior and oblique radiographs. Axial CT scans showing the superior 10 mm of the acetabular roof to be intact have been shown to correspond to radiographic roof arc measurements of 45 degrees. Fracture of the cotyloid fossa does not appear to jeopardize stability of the femoral head under the dome if the fossa extends to within 10 mm of the apex of the roof and the articular surface is intact.
divides the acetabulum, so the more inferior CT cuts appear to have three fragments when in reality there are only two. By studying the individual fragments on multiple successive cuts, the entire fracture can be appreciated, giving a true mental three-dimensional picture. High-resolution coronal and sagittal reconstructions of the fracture are helpful in the preoperative evaluation of complex fractures by delineating fractures that lie directly in the plane of a given axial CT image.
FIGURE 56-13 “Roof arc” measurement, as described by Matta et al. A, Medial roof arc is measured on anteroposterior view. B, Anterior roof arc is measured on 45-degree angle obturator oblique view. C, Posterior roof arc is measured on 45-degree angle iliac oblique view.
A B C
Roentg
en be
am
Roentgen beam
Roentgen beam
Medial roofarc
Anterior roof arc Posterior roofarc
C
BA
FIGURE 56-12 Fracture of posterior column of acetab-ulum. A, Anteroposterior view shows intact iliopectineal line, with disrupted ilioischial line. B, Iliac oblique (Judet) view shows disrupted posterior column and intact ante-rior wall. C, Obturator oblique (Judet) view shows intact anterior column in profile.
CHAPTER 56 FRACTURES OF ACETABULUM AND PELVIS 2783
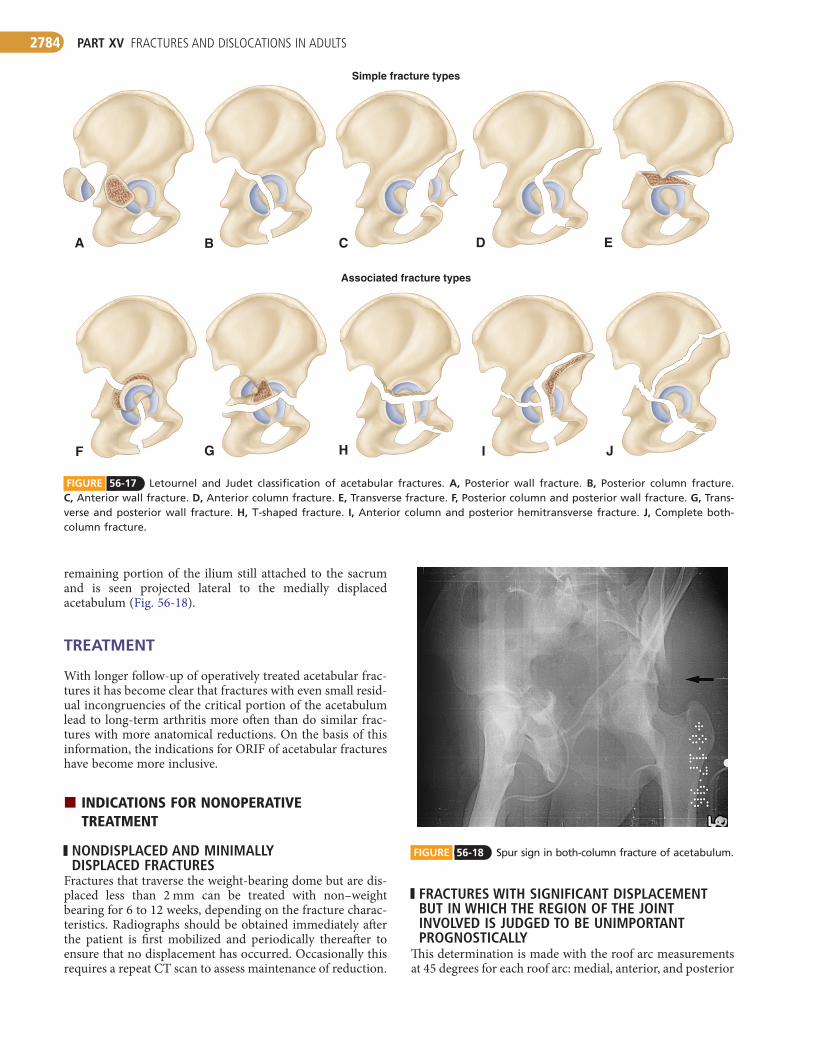
transverse fractures. Associated fracture types have more complex fracture geometries and include T-type fractures, combined fractures of the posterior column and wall, com-bined transverse and posterior wall fractures, anterior column fractures with a posterior hemitransverse fracture, and both-column fractures.
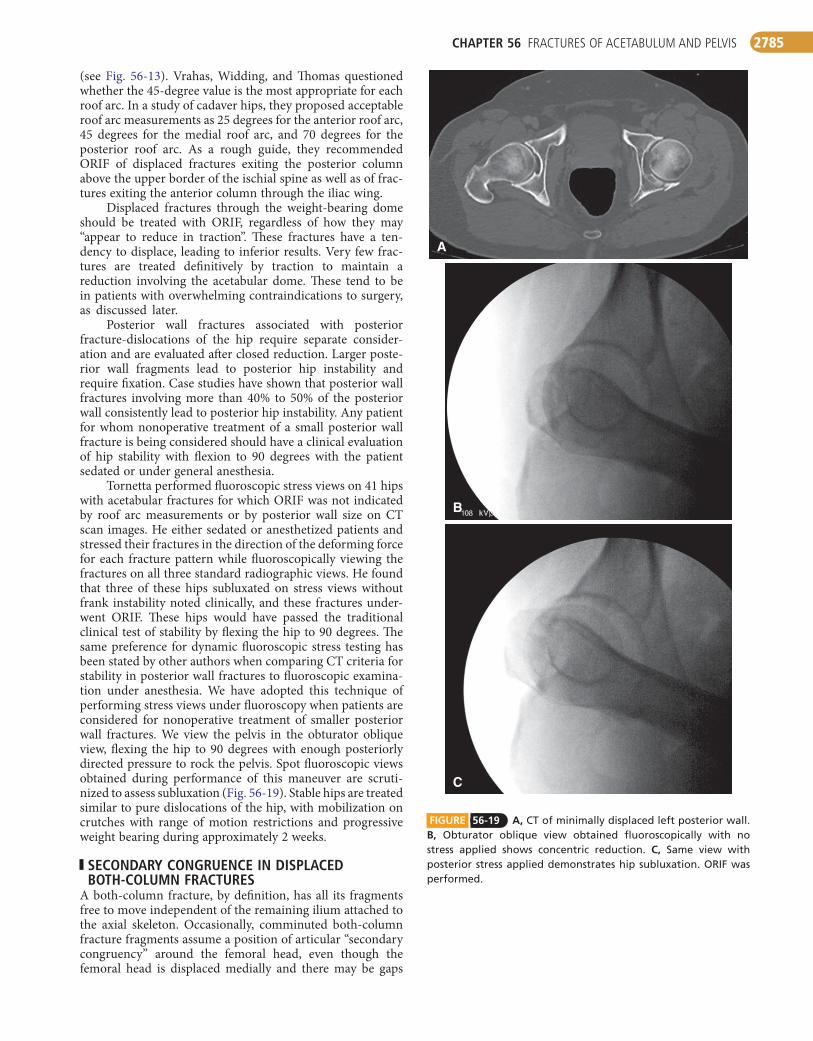
Although several of the associated fracture types involve both columns of the acetabulum, the designation both-column fracture in this classification denotes that none of the articular fracture fragments of the acetabulum maintain bony continu-ity with the axial skeleton: a fracture line divides the ilium, so the sacroiliac joint is not connected to any articular segment. The spur sign, shown on the obturator oblique view, is pathognomonic of a both-column fracture. It represents the
Three-dimensional CT reconstructions (Fig. 56-16) of a fracture have become sophisticated and can be projected in many different views with subtraction of the femoral head that show unique features of the various fracture patterns. Some surgeons who treat acetabular fractures find routine use of these reconstructions helpful. We occasionally obtain three-dimensional reconstructions in complicated fractures, but we generally rely on axial CT scans with coronal and sagittal reconstructions correlated with the standard three plain radiographic views.
CLASSIFICATION
The classification of acetabular fractures described by Letour-nel and Judet (Fig. 56-17) is the commonly used classification system. In this system acetabular fractures are divided into two basic groups: simple fracture types and the more complex associated fracture types. Simple fracture types are isolated fractures of one wall or column along with transverse frac-tures; this type includes fractures of the posterior wall, posterior column, anterior wall, or anterior column and
FIGURE 56-14 Orientation of fracture lines through acetabu-lum as seen on CT scan.
Column fractures
Wall and transverse fractures
FIGURE 56-15 A, Anterior column fracture with typical fracture orientation. B, Posterior wall fracture.
BB
A
FIGURE 56-16 A-C, Three-dimensional CT reconstruction of both-column fracture.
CBA
PART XV FRACTURES AND DISLOCATIONS IN ADULTS2784
remaining portion of the ilium still attached to the sacrum and is seen projected lateral to the medially displaced acetabulum (Fig. 56-18).
TREATMENT
With longer follow-up of operatively treated acetabular frac-tures it has become clear that fractures with even small resid-ual incongruencies of the critical portion of the acetabulum lead to long-term arthritis more often than do similar frac-tures with more anatomical reductions. On the basis of this information, the indications for ORIF of acetabular fractures have become more inclusive.
INDICATIONSFORNONOPERATIVETREATMENT
NONDISPLACED AND MINIMALLY DISPLACED FRACTURES
Fractures that traverse the weight-bearing dome but are dis-placed less than 2 mm can be treated with non–weight bearing for 6 to 12 weeks, depending on the fracture charac-teristics. Radiographs should be obtained immediately after the patient is first mobilized and periodically thereafter to ensure that no displacement has occurred. Occasionally this requires a repeat CT scan to assess maintenance of reduction.
FIGURE 56-17 Letournel and Judet classification of acetabular fractures. A, Posterior wall fracture. B, Posterior column fracture. C, Anterior wall fracture. D, Anterior column fracture. E, Transverse fracture. F, Posterior column and posterior wall fracture. G, Trans-verse and posterior wall fracture. H, T-shaped fracture. I, Anterior column and posterior hemitransverse fracture. J, Complete both-column fracture.
JIHGF
EDCBA
Simple fracture types
Associated fracture types
FIGURE 56-18 Spur sign in both-column fracture of acetabulum.
FRACTURES WITH SIGNIFICANT DISPLACEMENT BUT IN WHICH THE REGION OF THE JOINT INVOLVED IS JUDGED TO BE UNIMPORTANT PROGNOSTICALLY
This determination is made with the roof arc measurements at 45 degrees for each roof arc: medial, anterior, and posterior
CHAPTER 56 FRACTURES OF ACETABULUM AND PELVIS 2785
FIGURE 56-19 A, CT of minimally displaced left posterior wall. B, Obturator oblique view obtained fluoroscopically with no stress applied shows concentric reduction. C, Same view with posterior stress applied demonstrates hip subluxation. ORIF was performed.
A
B
C
(see Fig. 56-13). Vrahas, Widding, and Thomas questioned whether the 45-degree value is the most appropriate for each roof arc. In a study of cadaver hips, they proposed acceptable roof arc measurements as 25 degrees for the anterior roof arc, 45 degrees for the medial roof arc, and 70 degrees for the posterior roof arc. As a rough guide, they recommended ORIF of displaced fractures exiting the posterior column above the upper border of the ischial spine as well as of frac-tures exiting the anterior column through the iliac wing.
Displaced fractures through the weight-bearing dome should be treated with ORIF, regardless of how they may “appear to reduce in traction”. These fractures have a ten-dency to displace, leading to inferior results. Very few frac-tures are treated definitively by traction to maintain a reduction involving the acetabular dome. These tend to be in patients with overwhelming contraindications to surgery, as discussed later.
Posterior wall fractures associated with posterior fracture-dislocations of the hip require separate consider-ation and are evaluated after closed reduction. Larger poste-rior wall fragments lead to posterior hip instability and require fixation. Case studies have shown that posterior wall fractures involving more than 40% to 50% of the posterior wall consistently lead to posterior hip instability. Any patient for whom nonoperative treatment of a small posterior wall fracture is being considered should have a clinical evaluation of hip stability with flexion to 90 degrees with the patient sedated or under general anesthesia.
Tornetta performed fluoroscopic stress views on 41 hips with acetabular fractures for which ORIF was not indicated by roof arc measurements or by posterior wall size on CT scan images. He either sedated or anesthetized patients and stressed their fractures in the direction of the deforming force for each fracture pattern while fluoroscopically viewing the fractures on all three standard radiographic views. He found that three of these hips subluxated on stress views without frank instability noted clinically, and these fractures under-went ORIF. These hips would have passed the traditional clinical test of stability by flexing the hip to 90 degrees. The same preference for dynamic fluoroscopic stress testing has been stated by other authors when comparing CT criteria for stability in posterior wall fractures to fluoroscopic examina-tion under anesthesia. We have adopted this technique of performing stress views under fluoroscopy when patients are considered for nonoperative treatment of smaller posterior wall fractures. We view the pelvis in the obturator oblique view, flexing the hip to 90 degrees with enough posteriorly directed pressure to rock the pelvis. Spot fluoroscopic views obtained during performance of this maneuver are scruti-nized to assess subluxation (Fig. 56-19). Stable hips are treated similar to pure dislocations of the hip, with mobilization on crutches with range of motion restrictions and progressive weight bearing during approximately 2 weeks.
SECONDARY CONGRUENCE IN DISPLACED BOTH-COLUMN FRACTURES
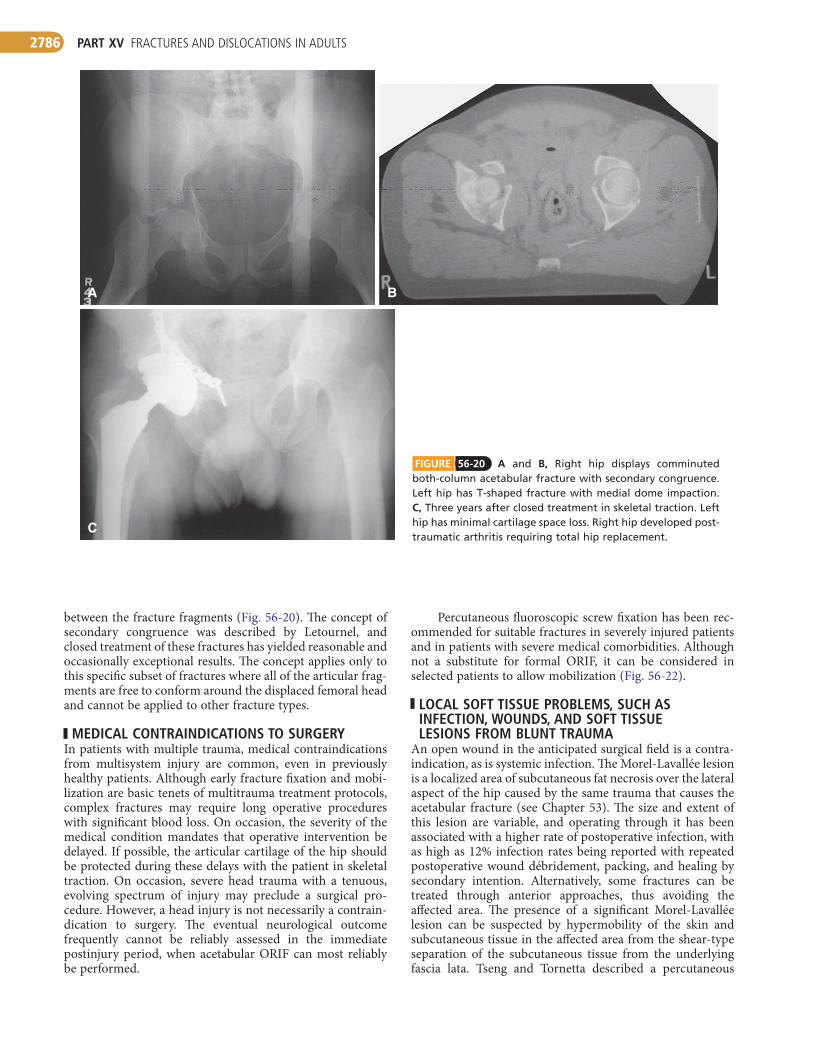
A both-column fracture, by definition, has all its fragments free to move independent of the remaining ilium attached to the axial skeleton. Occasionally, comminuted both-column fracture fragments assume a position of articular “secondary congruency” around the femoral head, even though the femoral head is displaced medially and there may be gaps
PART XV FRACTURES AND DISLOCATIONS IN ADULTS2786
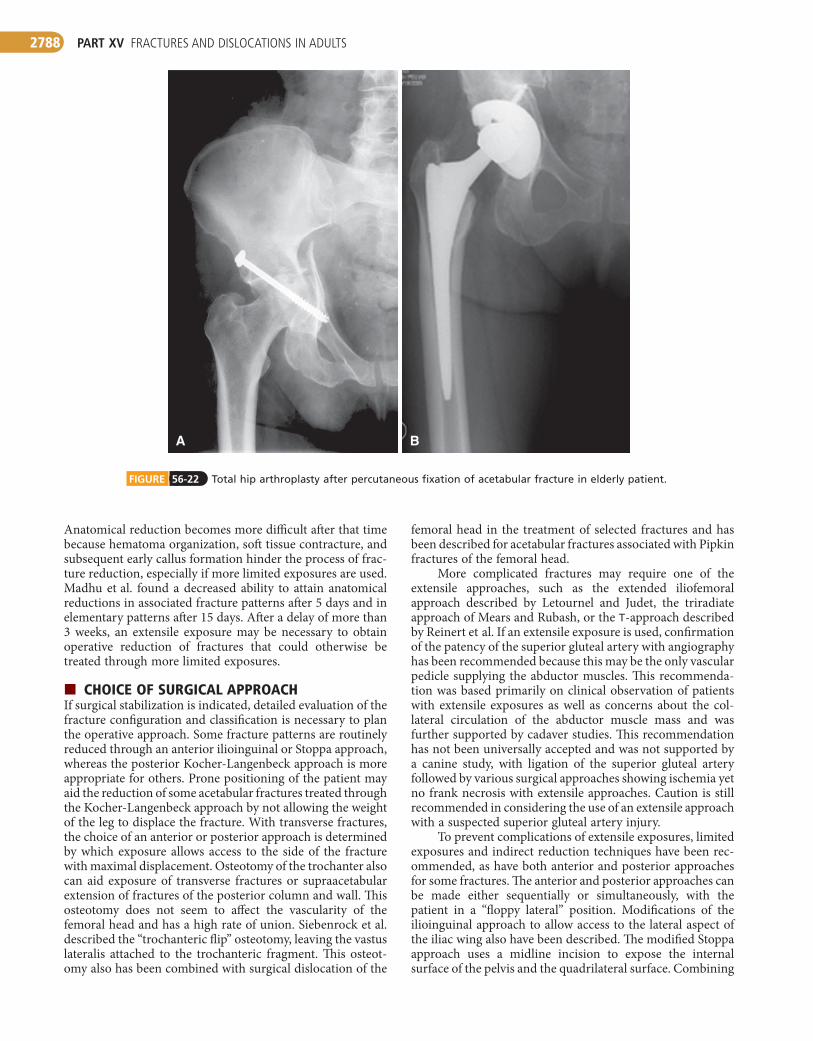
Percutaneous fluoroscopic screw fixation has been rec-ommended for suitable fractures in severely injured patients and in patients with severe medical comorbidities. Although not a substitute for formal ORIF, it can be considered in selected patients to allow mobilization (Fig. 56-22).
LOCAL SOFT TISSUE PROBLEMS, SUCH AS INFECTION, WOUNDS, AND SOFT TISSUE LESIONS FROM BLUNT TRAUMA
An open wound in the anticipated surgical field is a contra-indication, as is systemic infection. The Morel-Lavallée lesion is a localized area of subcutaneous fat necrosis over the lateral aspect of the hip caused by the same trauma that causes the acetabular fracture (see Chapter 53). The size and extent of this lesion are variable, and operating through it has been associated with a higher rate of postoperative infection, with as high as 12% infection rates being reported with repeated postoperative wound débridement, packing, and healing by secondary intention. Alternatively, some fractures can be treated through anterior approaches, thus avoiding the affected area. The presence of a significant Morel-Lavallée lesion can be suspected by hypermobility of the skin and subcutaneous tissue in the affected area from the shear-type separation of the subcutaneous tissue from the underlying fascia lata. Tseng and Tornetta described a percutaneous
between the fracture fragments (Fig. 56-20). The concept of secondary congruence was described by Letournel, and closed treatment of these fractures has yielded reasonable and occasionally exceptional results. The concept applies only to this specific subset of fractures where all of the articular frag-ments are free to conform around the displaced femoral head and cannot be applied to other fracture types.
MEDICAL CONTRAINDICATIONS TO SURGERYIn patients with multiple trauma, medical contraindications from multisystem injury are common, even in previously healthy patients. Although early fracture fixation and mobi-lization are basic tenets of multitrauma treatment protocols, complex fractures may require long operative procedures with significant blood loss. On occasion, the severity of the medical condition mandates that operative intervention be delayed. If possible, the articular cartilage of the hip should be protected during these delays with the patient in skeletal traction. On occasion, severe head trauma with a tenuous, evolving spectrum of injury may preclude a surgical pro-cedure. However, a head injury is not necessarily a contrain-dication to surgery. The eventual neurological outcome frequently cannot be reliably assessed in the immediate postinjury period, when acetabular ORIF can most reliably be performed.
B
C
A
FIGURE 56-20 A and B, Right hip displays comminuted both-column acetabular fracture with secondary congruence. Left hip has T-shaped fracture with medial dome impaction. C, Three years after closed treatment in skeletal traction. Left hip has minimal cartilage space loss. Right hip developed post-traumatic arthritis requiring total hip replacement.

CHAPTER 56 FRACTURES OF ACETABULUM AND PELVIS 2787
INDICATIONSFOROPERATIVETREATMENT
FRACTURE CHARACTERISTICSAn acetabular fracture with 2 mm or more of displacement in the dome of the acetabulum as defined by any roof arc measurements of less than 45 degrees is an indication for operative intervention, as is any subluxation of the femoral head from a displaced acetabular fracture noted on any of the three standard radiographic views. Also, operative treat-ment should be considered for posterior wall fractures with more than 50% involvement of the articular surface of the posterior wall or clinical instability with hip flexion to 90 degrees. As stated earlier, posterior wall fractures with more than 50% of the wall involved are generally considered unstable and do not require any test of stability. However, posterior wall fractures involving less than 50% of the wall may be unstable and are assessed clinically by flexing the hip to 90 degrees with the patient sedated or anesthetized as well as by stress testing of equivocal cases under anesthesia with fluoroscopy.
INCARCERATED FRAGMENTS IN THE ACETABULUM AFTER CLOSED REDUCTION OF A HIP DISLOCATION
Small avulsed fragments of the ligamentum teres that stay sequestered in the cotyloid fossa and do not affect the congru-ency of the hip probably do not require excision. Fragments noted on CT to be lodged between the articular surfaces of the femoral head and the acetabulum warrant excision.
PREVENTION OF NONUNION AND RETENTION OF SUFFICIENT BONE STOCK FOR LATER RECONSTRUCTIVE SURGERY
This last indication for ORIF is largely outdated and should be applied only in cases of extreme deformity because total hip arthroplasty after failed ORIF of an acetabular fracture may be more difficult than hip arthroplasty after nonopera-tive management. Scarring from previous surgeries, hard-ware, and heterotopic bone can complicate such secondary reconstruction. We occasionally use percutaneous fixation in older patients with comminuted fractures destined for post-traumatic arthritis. We use this technique to mobilize these patients, using limited column fixation to prevent gross dis-placement of the fracture. After fracture healing, conversion to total hip arthroplasty can be done if the patient’s symptoms warrant (Fig. 56-22). Primary total hip arthroplasty has been advocated in older patients having fractures with a poor prog-nosis. We have used this technique in appropriate patients who have fractures that can be adequately stabilized to provide immediate stability of the acetabular shell. This topic is covered in more detail later (see Total Hip Arthroplasty as Treatment of Acetabular Fracture).
TIMINGOFSURGERYAcetabular fractures associated with irreducible hip disloca-tion, open fracture, vascular compromise, or worsening neu-rologic deficit are all situations that require urgent surgical intervention. In most circumstances, acetabular fracture surgery should only be performed after the patient is medi-cally optimized and the surgeon has studied the fracture in detail with adequate preoperative planning and assembly of an experienced surgical team. Ideally, ORIF of acetabular fractures should be performed within 5 to 7 days of injury.
technique for débriding Morel-Lavallée lesions through smaller 2-inch incisions with no infections at 6-month follow-up in 19 patients (see Technique 53-1).
The presence of a suprapubic catheter generally is con-sidered a contraindication to acetabular ORIF by the ilioin-guinal approach. Bacterial colonization of the catheter has been anecdotally reported to increase the rate of infection. The best method of avoiding this situation is to discuss with the urologist the possibility of avoiding suprapubic drainage of the bladder with possible primary repair of the bladder rupture and Foley catheter drainage. We generally delay surgery through the ilioinguinal approach until a bladder rupture or repair has sealed, and occasionally we delay surgery to allow a previous suprapubic catheter track to seal before proceeding.
ELDERLY PATIENTS WITH OSTEOPOROTIC BONE IN WHOM OPEN REDUCTION MAY NOT BE FEASIBLE
A report of ORIF in a series of patients older than 60 years questioned this indication for nonoperative treatment because only one fracture lost its reduction because of fixation failure and complications were similar to those in younger patients. In another group of patients with an average age of 71 years, only 60% had good or excellent radiographic results at 3-year follow-up. Superior medial impaction of the dome, or the “gull sign,” particularly correlated with a poor outcome (see Fig. 56-21). In our practice, some comminuted and impacted fractures in elderly, osteopenic patients are not treated by standard ORIF. The options for these patients include mobi-lization without fixation, percutaneous fixation with mobili-zation, and primary total hip arthroplasty. Although each fracture and patient is unique with different considerations, we aim to avoid prolonged traction.
FIGURE 56-21 “Gull sign” on this transverse fracture indicates impaction of medial portion of weight-bearing dome.
PART XV FRACTURES AND DISLOCATIONS IN ADULTS2788
femoral head in the treatment of selected fractures and has been described for acetabular fractures associated with Pipkin fractures of the femoral head.
More complicated fractures may require one of the extensile approaches, such as the extended iliofemoral approach described by Letournel and Judet, the triradiate approach of Mears and Rubash, or the T-approach described by Reinert et al. If an extensile exposure is used, confirmation of the patency of the superior gluteal artery with angiography has been recommended because this may be the only vascular pedicle supplying the abductor muscles. This recommenda-tion was based primarily on clinical observation of patients with extensile exposures as well as concerns about the col-lateral circulation of the abductor muscle mass and was further supported by cadaver studies. This recommendation has not been universally accepted and was not supported by a canine study, with ligation of the superior gluteal artery followed by various surgical approaches showing ischemia yet no frank necrosis with extensile approaches. Caution is still recommended in considering the use of an extensile approach with a suspected superior gluteal artery injury.
To prevent complications of extensile exposures, limited exposures and indirect reduction techniques have been rec-ommended, as have both anterior and posterior approaches for some fractures. The anterior and posterior approaches can be made either sequentially or simultaneously, with the patient in a “floppy lateral” position. Modifications of the ilioinguinal approach to allow access to the lateral aspect of the iliac wing also have been described. The modified Stoppa approach uses a midline incision to expose the internal surface of the pelvis and the quadrilateral surface. Combining
Anatomical reduction becomes more difficult after that time because hematoma organization, soft tissue contracture, and subsequent early callus formation hinder the process of frac-ture reduction, especially if more limited exposures are used. Madhu et al. found a decreased ability to attain anatomical reductions in associated fracture patterns after 5 days and in elementary patterns after 15 days. After a delay of more than 3 weeks, an extensile exposure may be necessary to obtain operative reduction of fractures that could otherwise be treated through more limited exposures.
CHOICEOFSURGICALAPPROACHIf surgical stabilization is indicated, detailed evaluation of the fracture configuration and classification is necessary to plan the operative approach. Some fracture patterns are routinely reduced through an anterior ilioinguinal or Stoppa approach, whereas the posterior Kocher-Langenbeck approach is more appropriate for others. Prone positioning of the patient may aid the reduction of some acetabular fractures treated through the Kocher-Langenbeck approach by not allowing the weight of the leg to displace the fracture. With transverse fractures, the choice of an anterior or posterior approach is determined by which exposure allows access to the side of the fracture with maximal displacement. Osteotomy of the trochanter also can aid exposure of transverse fractures or supraacetabular extension of fractures of the posterior column and wall. This osteotomy does not seem to affect the vascularity of the femoral head and has a high rate of union. Siebenrock et al. described the “trochanteric flip” osteotomy, leaving the vastus lateralis attached to the trochanteric fragment. This osteot-omy also has been combined with surgical dislocation of the
FIGURE 56-22 Total hip arthroplasty after percutaneous fixation of acetabular fracture in elderly patient.
A B

CHAPTER 56 FRACTURES OF ACETABULUM AND PELVIS 2789
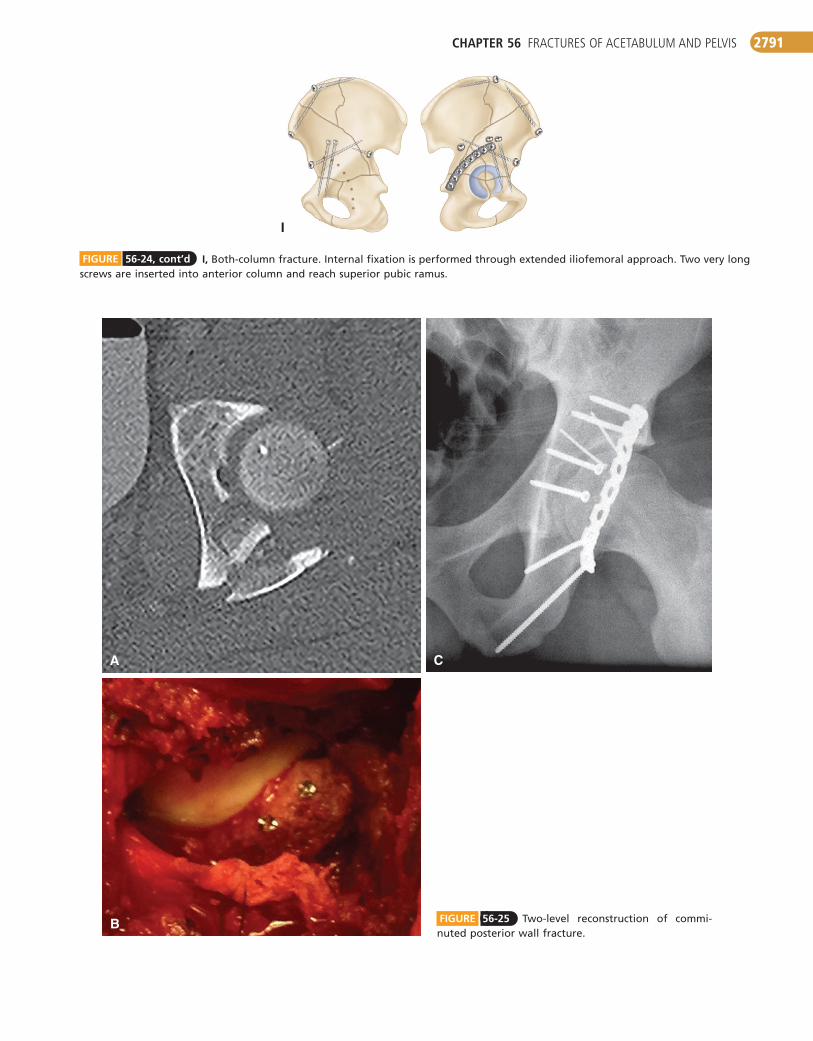
fragment in addition to the gluteus medius, can be used. The trochanteric fragment is displaced anteriorly to expose the supraacetabular surface of the ilium. The hip is distracted to clear any incarcerated fragments before reduction of the wall fragments. A close inspection is made for marginal impaction of articular fragments into the intact posterior column. Impacted segments are elevated and bone grafted. We frequently use the technique described by Giannoudis, Tzioupis, and Moed for two-level reconstruction of com-minuted posterior wall fractures with marginal fragments secured by subchondral miniscrews (Fig 56-25). After reduc-tion of the wall fragments, provisional fixation with Kirschner wires can be used while definitive fixation is performed with lag screws and a contoured reconstruction plate placed from the ischium, over the retroacetabular surface onto the lateral ilium (Fig. 56-26).
The use of spring plates has been advocated to improve stability in comminuted fractures. These can be made out of one-third tubular plates by cutting or breaking the plate through the last screw hole and bending down the remaining end as tines, which are used to capture bone fragments that cannot be easily fixed with screws. Premade spring plates are also available. The spring plate is slightly overcontoured so that when the reconstruction plate is applied over the spring plate the captured fragments are held firmly in position. We have found this technique useful in fractures with multiple fragments and fractures that extend close to the acetabular rim (Fig. 56-27).
Although a posterior wall fracture is the easiest fracture pattern to reduce, the reported long-term results after this fracture have varied. Osteonecrosis of the femoral head as a result of associated hip dislocation, marginal impaction, mul-tiple fracture fragments, and osteochondral injuries of the femoral head all adversely affect the outcome of these frac-tures. Intraarticular screw placement must be avoided. Intra-operative fluoroscopy in multiple views should be used to ensure that all screws are extraarticular.
the ilioinguinal and Stoppa approaches has been suggested to improve access and fixation of the quadrilateral surface with anterior fracture patterns.
Traditionally, most surgeons have preferred to use skeletal traction on a radiolucent fracture table for most fractures. Increasingly, some surgeons prefer to drape the limb free to allow positioning of the limb to facilitate exposure. The standard operative approaches are described in Chapter 1.
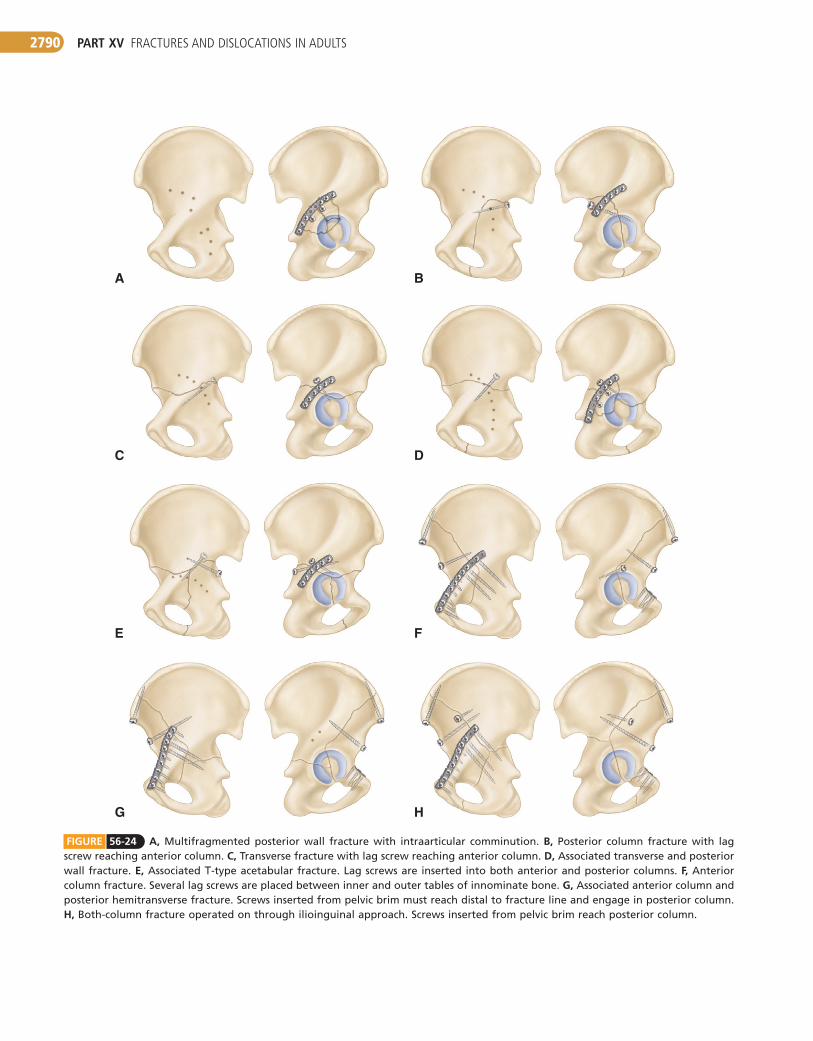
SPECIFICFRACTUREPATTERNSDetailed surgical recommendations and techniques for ace-tabular fracture stabilization are too numerous to be included here, and the reader is referred to the standard texts of Letournel and Judet and of Tile et al. Specialized pelvic equip-ment, implants, and facilities are required for optimal treat-ment of these fractures, including a radiolucent fracture table, a full array of screw sizes and lengths (up to 110 mm), and reconstruction plates that can be contoured in three dimen-sions as required by the convoluted configuration of the bony pelvis (Fig. 56-23). Pelvic clamps developed by the AO/ASIF group for reduction of fracture fragments are especially helpful. Treatment strategies for specific fractures are shown in Figure 56-24.
POSTERIOR WALL FRACTURESThe most common fracture treated by the average orthopae-dist is the posterior wall fracture. These fractures are treated through a Kocher-Langenbeck approach (see Technique 1-67) with the patient positioned either prone or in the lateral decubitus position on a fracture table or with the leg free. To avoid osteonecrosis of the posterior wall, the posterior wall fragments must not be detached from the posterior capsule during exposure. If the fracture extends superiorly into the dome, a trochanteric osteotomy may be performed to allow additional exposure. A trochanteric flip osteotomy, leaving the vastus lateralis muscle attached to the trochanteric
FIGURE 56-23 Specialized instruments and implants for treatment of acetabular fractures.
PART XV FRACTURES AND DISLOCATIONS IN ADULTS2790
FE
DC
BA
HG
FIGURE 56-24 A, Multifragmented posterior wall fracture with intraarticular comminution. B, Posterior column fracture with lag screw reaching anterior column. C, Transverse fracture with lag screw reaching anterior column. D, Associated transverse and posterior wall fracture. E, Associated T-type acetabular fracture. Lag screws are inserted into both anterior and posterior columns. F, Anterior column fracture. Several lag screws are placed between inner and outer tables of innominate bone. G, Associated anterior column and posterior hemitransverse fracture. Screws inserted from pelvic brim must reach distal to fracture line and engage in posterior column. H, Both-column fracture operated on through ilioinguinal approach. Screws inserted from pelvic brim reach posterior column.
CHAPTER 56 FRACTURES OF ACETABULUM AND PELVIS 2791
A C
B FIGURE 56-25 Two-level reconstruction of commi-nuted posterior wall fracture.
FIGURE 56-24, cont’d I, Both-column fracture. Internal fixation is performed through extended iliofemoral approach. Two very long screws are inserted into anterior column and reach superior pubic ramus.
I
PART XV FRACTURES AND DISLOCATIONS IN ADULTS2792
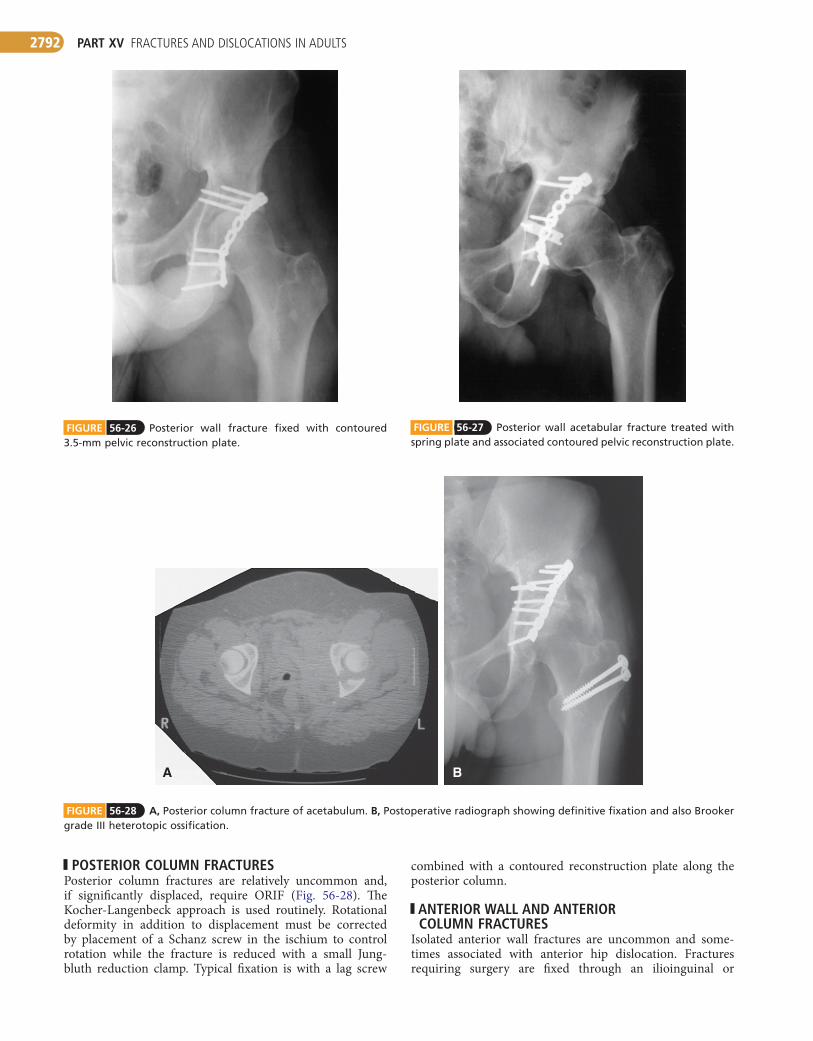
FIGURE 56-26 Posterior wall fracture fixed with contoured 3.5-mm pelvic reconstruction plate.
FIGURE 56-27 Posterior wall acetabular fracture treated with spring plate and associated contoured pelvic reconstruction plate.
FIGURE 56-28 A, Posterior column fracture of acetabulum. B, Postoperative radiograph showing definitive fixation and also Brooker grade III heterotopic ossification.
BA
POSTERIOR COLUMN FRACTURESPosterior column fractures are relatively uncommon and, if significantly displaced, require ORIF (Fig. 56-28). The Kocher-Langenbeck approach is used routinely. Rotational deformity in addition to displacement must be corrected by placement of a Schanz screw in the ischium to control rotation while the fracture is reduced with a small Jung-bluth reduction clamp. Typical fixation is with a lag screw
combined with a contoured reconstruction plate along the posterior column.
ANTERIOR WALL AND ANTERIOR COLUMN FRACTURES
Isolated anterior wall fractures are uncommon and some-times associated with anterior hip dislocation. Fractures requiring surgery are fixed through an ilioinguinal or
CHAPTER 56 FRACTURES OF ACETABULUM AND PELVIS 2793
from a position above the acetabulum. Care must be taken with placement of the anterior lag screw because of the proximity of the iliac vessels.
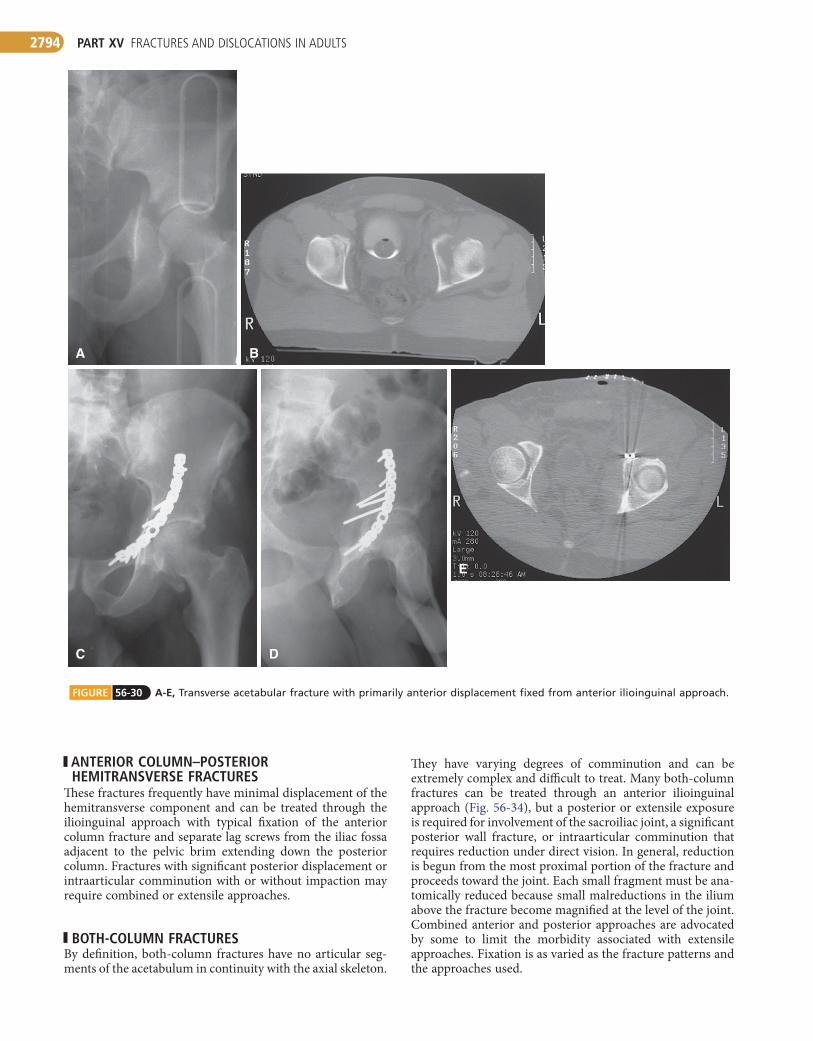
From the ilioinguinal approach, reduction is usually accomplished by using plate reduction along the anterior column to close the fracture gap; a large spiked reduction clamp placed on the quadrilateral surface and the lateral surface of the ilium in the region of the anterior inferior spine controls medial displacement and rotation of the caudal frag-ment. Typical fixation is a contoured plate along the pelvic brim with lag screws directed down the posterior column (Fig. 56-30). On occasion, extensile or combined approaches are necessary for more complex transverse fractures.
POSTERIOR COLUMN FRACTURE WITH ASSOCIATED POSTERIOR WALL FRACTURE
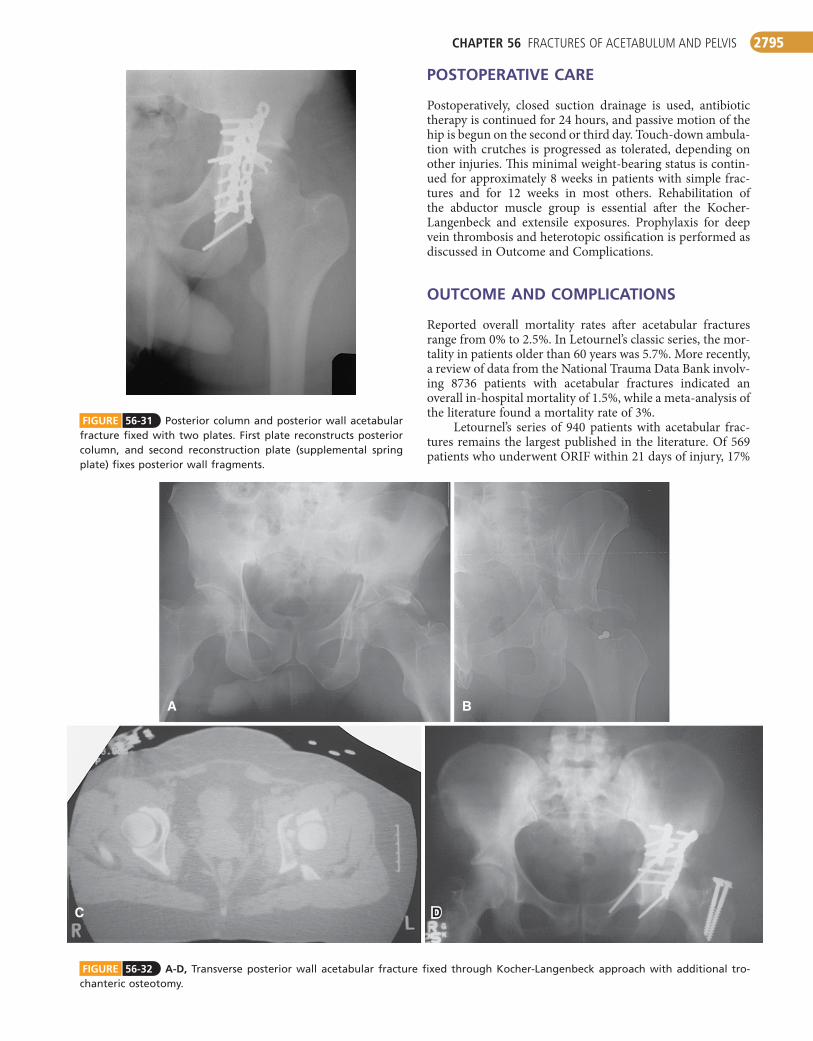
A Kocher-Langenbeck approach is used, with or without a trochanteric osteotomy. The column fracture is reduced first, and a short reconstruction plate is placed posteriorly along the posterior edge of the column. A separate plate is used for the wall fragment. When the wall fragment is small, spring plates can be used instead of a separate wall plate (Fig. 56-31).
TRANSVERSE FRACTURE WITH ASSOCIATED POSTERIOR WALL FRACTURE
This common fracture usually is treated through the Kocher-Langenbeck approach with the patient prone. Prone position-ing prevents the weight of the leg from displacing the fracture, as in the lateral position. The intraarticular portion of the transverse fracture can be seen through the defect created by the retraction of the posterior wall fragment. Care must be taken not to injure the sciatic nerve when a reduction clamp is being placed through the greater sciatic notch to reduce the transverse component of this fracture. Rotational control of the distal segment is accomplished by placing a Schanz pin in the ischium. Typically, the transverse component is fixed with lag screws into the anterior column while the posterior wall is plated, thus further stabilizing the posterior portion of the transverse fracture (Fig. 56-32).
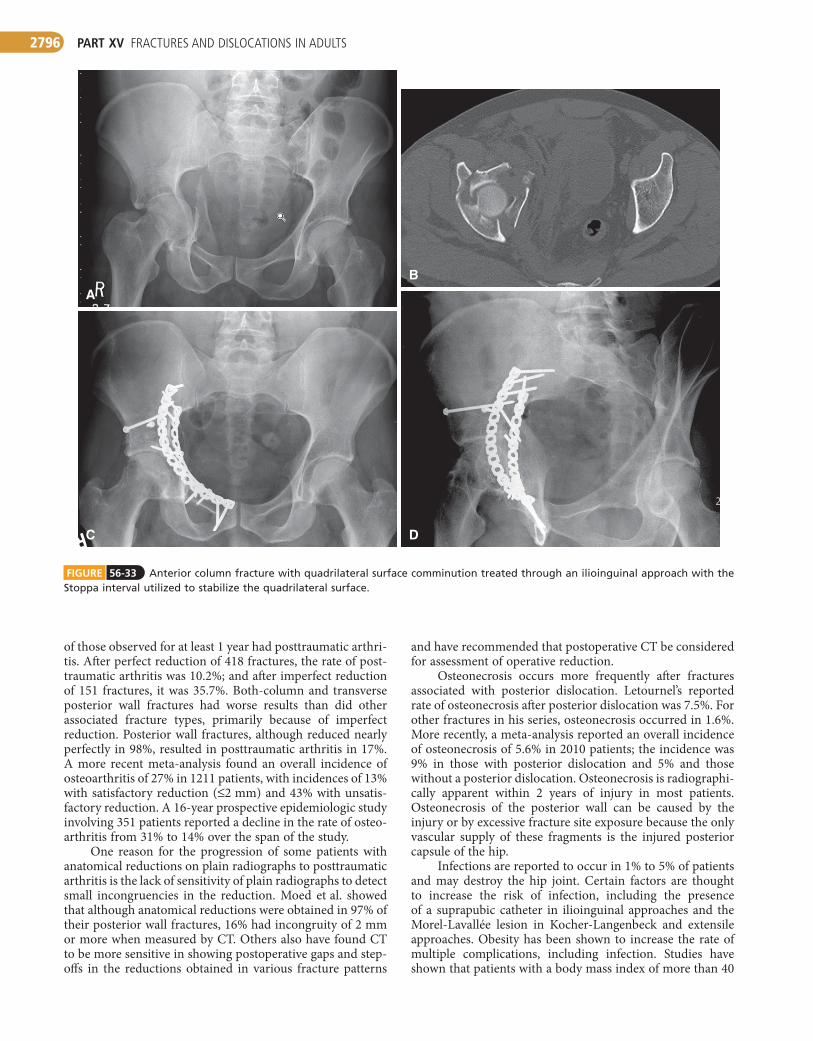
T-TYPE FRACTUREST-type fractures span a range of severity requiring different reduction and fixation methods. These fractures usually can be treated with the patient prone through a Kocher-Langenbeck approach. The anterior column fracture line can be reduced through the sciatic notch after reduction of the posterior column portion or reduced first with displacement of the posterior column, facilitating clamp placement. The anterior column is fixed with screws placed down the anterior column from a position above the acetabulum; the posterior column portion can be fixed with a lag screw and a recon-struction plate. These fractures can occasionally be treated through an ilioinguinal approach with a contoured plate placed along the pelvic brim and lag screws extending into the posterior column. If both the anterior and posterior com-ponents of the fracture are significantly displaced, extensile or combined approaches may be required to obtain a reduc-tion. On occasion, with T-type fractures as well as other asso-ciated fracture types, a separate medial fragment is present. If it is proximal enough to affect stability, a Stoppa approach can be used to place a plate along the quadrilateral surface (Fig. 56-33).
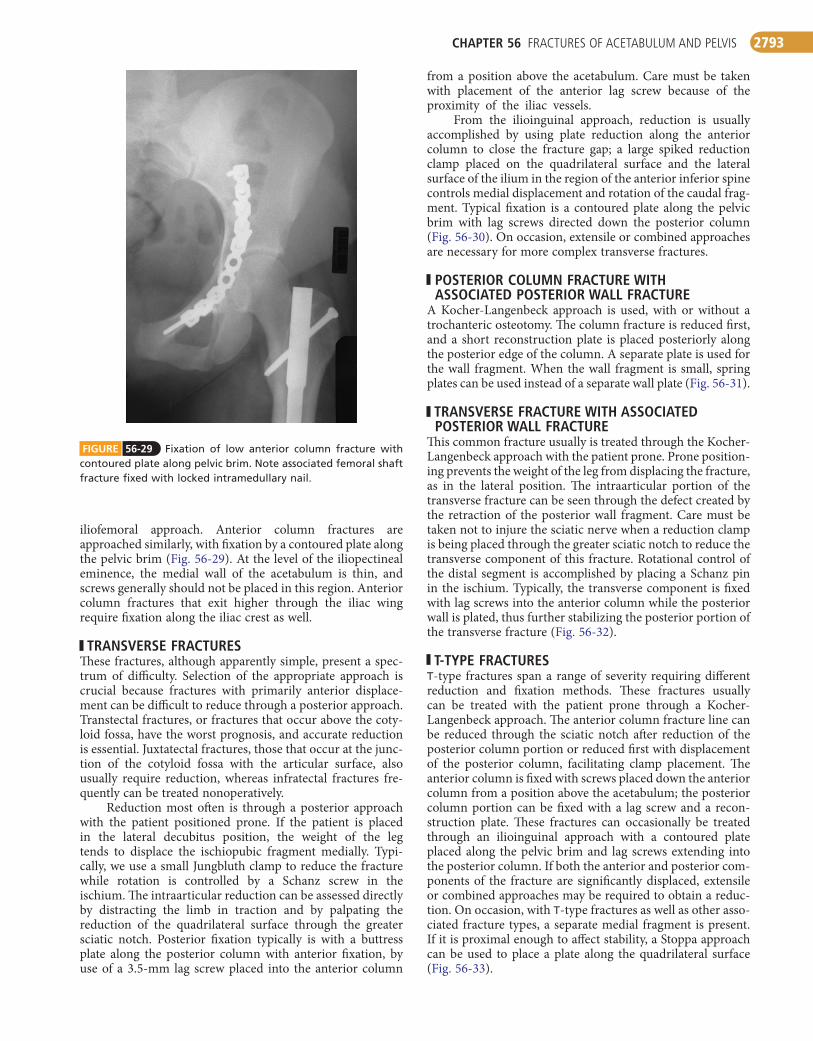
FIGURE 56-29 Fixation of low anterior column fracture with contoured plate along pelvic brim. Note associated femoral shaft fracture fixed with locked intramedullary nail.
iliofemoral approach. Anterior column fractures are approached similarly, with fixation by a contoured plate along the pelvic brim (Fig. 56-29). At the level of the iliopectineal eminence, the medial wall of the acetabulum is thin, and screws generally should not be placed in this region. Anterior column fractures that exit higher through the iliac wing require fixation along the iliac crest as well.
TRANSVERSE FRACTURESThese fractures, although apparently simple, present a spec-trum of difficulty. Selection of the appropriate approach is crucial because fractures with primarily anterior displace-ment can be difficult to reduce through a posterior approach. Transtectal fractures, or fractures that occur above the coty-loid fossa, have the worst prognosis, and accurate reduction is essential. Juxtatectal fractures, those that occur at the junc-tion of the cotyloid fossa with the articular surface, also usually require reduction, whereas infratectal fractures fre-quently can be treated nonoperatively.
Reduction most often is through a posterior approach with the patient positioned prone. If the patient is placed in the lateral decubitus position, the weight of the leg tends to displace the ischiopubic fragment medially. Typi-cally, we use a small Jungbluth clamp to reduce the fracture while rotation is controlled by a Schanz screw in the ischium. The intraarticular reduction can be assessed directly by distracting the limb in traction and by palpating the reduction of the quadrilateral surface through the greater sciatic notch. Posterior fixation typically is with a buttress plate along the posterior column with anterior fixation, by use of a 3.5-mm lag screw placed into the anterior column
PART XV FRACTURES AND DISLOCATIONS IN ADULTS2794
ANTERIOR COLUMN–POSTERIOR HEMITRANSVERSE FRACTURES
These fractures frequently have minimal displacement of the hemitransverse component and can be treated through the ilioinguinal approach with typical fixation of the anterior column fracture and separate lag screws from the iliac fossa adjacent to the pelvic brim extending down the posterior column. Fractures with significant posterior displacement or intraarticular comminution with or without impaction may require combined or extensile approaches.
BOTH-COLUMN FRACTURESBy definition, both-column fractures have no articular seg-ments of the acetabulum in continuity with the axial skeleton.
FIGURE 56-30 A-E, Transverse acetabular fracture with primarily anterior displacement fixed from anterior ilioinguinal approach.
DC
BA
E
They have varying degrees of comminution and can be extremely complex and difficult to treat. Many both-column fractures can be treated through an anterior ilioinguinal approach (Fig. 56-34), but a posterior or extensile exposure is required for involvement of the sacroiliac joint, a significant posterior wall fracture, or intraarticular comminution that requires reduction under direct vision. In general, reduction is begun from the most proximal portion of the fracture and proceeds toward the joint. Each small fragment must be ana-tomically reduced because small malreductions in the ilium above the fracture become magnified at the level of the joint. Combined anterior and posterior approaches are advocated by some to limit the morbidity associated with extensile approaches. Fixation is as varied as the fracture patterns and the approaches used.
CHAPTER 56 FRACTURES OF ACETABULUM AND PELVIS 2795
FIGURE 56-31 Posterior column and posterior wall acetabular fracture fixed with two plates. First plate reconstructs posterior column, and second reconstruction plate (supplemental spring plate) fixes posterior wall fragments.
FIGURE 56-32 A-D, Transverse posterior wall acetabular fracture fixed through Kocher-Langenbeck approach with additional tro-chanteric osteotomy.
C D
BA
POSTOPERATIVE CARE
Postoperatively, closed suction drainage is used, antibiotic therapy is continued for 24 hours, and passive motion of the hip is begun on the second or third day. Touch-down ambula-tion with crutches is progressed as tolerated, depending on other injuries. This minimal weight-bearing status is contin-ued for approximately 8 weeks in patients with simple frac-tures and for 12 weeks in most others. Rehabilitation of the abductor muscle group is essential after the Kocher-Langenbeck and extensile exposures. Prophylaxis for deep vein thrombosis and heterotopic ossification is performed as discussed in Outcome and Complications.
OUTCOME AND COMPLICATIONS
Reported overall mortality rates after acetabular fractures range from 0% to 2.5%. In Letournel’s classic series, the mor-tality in patients older than 60 years was 5.7%. More recently, a review of data from the National Trauma Data Bank involv-ing 8736 patients with acetabular fractures indicated an overall in-hospital mortality of 1.5%, while a meta-analysis of the literature found a mortality rate of 3%.
Letournel’s series of 940 patients with acetabular frac-tures remains the largest published in the literature. Of 569 patients who underwent ORIF within 21 days of injury, 17%
PART XV FRACTURES AND DISLOCATIONS IN ADULTS2796
FIGURE 56-33 Anterior column fracture with quadrilateral surface comminution treated through an ilioinguinal approach with the Stoppa interval utilized to stabilize the quadrilateral surface.
A
B
C D
of those observed for at least 1 year had posttraumatic arthri-tis. After perfect reduction of 418 fractures, the rate of post-traumatic arthritis was 10.2%; and after imperfect reduction of 151 fractures, it was 35.7%. Both-column and transverse posterior wall fractures had worse results than did other associated fracture types, primarily because of imperfect reduction. Posterior wall fractures, although reduced nearly perfectly in 98%, resulted in posttraumatic arthritis in 17%. A more recent meta-analysis found an overall incidence of osteoarthritis of 27% in 1211 patients, with incidences of 13% with satisfactory reduction (≤2 mm) and 43% with unsatis-factory reduction. A 16-year prospective epidemiologic study involving 351 patients reported a decline in the rate of osteo-arthritis from 31% to 14% over the span of the study.
One reason for the progression of some patients with anatomical reductions on plain radiographs to posttraumatic arthritis is the lack of sensitivity of plain radiographs to detect small incongruencies in the reduction. Moed et al. showed that although anatomical reductions were obtained in 97% of their posterior wall fractures, 16% had incongruity of 2 mm or more when measured by CT. Others also have found CT to be more sensitive in showing postoperative gaps and step-offs in the reductions obtained in various fracture patterns
and have recommended that postoperative CT be considered for assessment of operative reduction.
Osteonecrosis occurs more frequently after fractures associated with posterior dislocation. Letournel’s reported rate of osteonecrosis after posterior dislocation was 7.5%. For other fractures in his series, osteonecrosis occurred in 1.6%. More recently, a meta-analysis reported an overall incidence of osteonecrosis of 5.6% in 2010 patients; the incidence was 9% in those with posterior dislocation and 5% and those without a posterior dislocation. Osteonecrosis is radiographi-cally apparent within 2 years of injury in most patients. Osteonecrosis of the posterior wall can be caused by the injury or by excessive fracture site exposure because the only vascular supply of these fragments is the injured posterior capsule of the hip.
Infections are reported to occur in 1% to 5% of patients and may destroy the hip joint. Certain factors are thought to increase the risk of infection, including the presence of a suprapubic catheter in ilioinguinal approaches and the Morel-Lavallée lesion in Kocher-Langenbeck and extensile approaches. Obesity has been shown to increase the rate of multiple complications, including infection. Studies have shown that patients with a body mass index of more than 40

CHAPTER 56 FRACTURES OF ACETABULUM AND PELVIS 2797
A
F
E
D
C
B
FIGURE 56-34 A-F, Both-column acetabular fracture treated through ilioinguinal approach with indirect reduction of acetabulum and fixation placed on internal surfaces of pelvis.

PART XV FRACTURES AND DISLOCATIONS IN ADULTS2798
have a five times increased risk of infection with acetabular surgery, as well as more frequent overall wound healing com-plications (46% vs. 12% for patients with indices < 40).
Sciatic nerve palsies as a result of the initial injury occur in 10% to 15% of patients with acetabular fractures. Sciatic nerve injury as a result of surgery occurs in 2% to 6% of patients and is more often associated with posterior fracture patterns treated through the Kocher-Langenbeck and extensile exposures. Many authors have proposed intra-operative monitoring of somatosensory evoked potentials as a means of decreasing the incidence of intraoperative sciatic nerve injury, especially with posterior approaches. Other authors, however, have found that with experience their rates of iatrogenic nerve injury without monitoring were similar to the levels quoted in studies recommending routine monitoring; they did not recommend intraoperative nerve monitoring and questioned the usefulness of routine monitoring when the operating surgeon is sufficiently expe-rienced. A poll of 181 members of the Orthopaedic Trauma Association who commonly perform acetabular surgery found that only 15% routinely used nerve monitoring during acetabular surgery.
In a report of 14 patients with sciatic nerve injuries, the peroneal component of the sciatic nerve was more often involved than the tibial component and the tibial component had a greater chance of recovery; complete peroneal palsies had the worst prognosis. Functional recovery has been shown in approximately 65% of patients, and function may improve up to 3 years after injury.
Heterotopic ossification occurs after most extensile approaches, with moderate-to-severe heterotopic ossification occurring in 14% to 50% of patients when no prophylaxis is used; it occurs after the Kocher-Langenbeck approach in approximately 25% of patients in whom no prophylaxis is used (Fig. 56-35). Heterotopic ossification is rare after the ilioinguinal approach unless the external surface of the ilium is stripped. The effectiveness and choice of prophylactic mea-sures to prevent heterotopic ossification remain controversial. Multiple authors have found indomethacin to be effective in decreasing significant heterotopic ossification after acetabular
FIGURE 56-35 Brooker grade IV heterotopic ossification occ-urred despite postoperative irradiation.
fracture surgery, although this has been called into question by others who found indomethacin to be ineffective in their prospective series. Low-dose irradiation has been shown to be effective in decreasing the incidence of significant hetero-topic ossification, and an additive effect has been noted when the two regimens were combined.
For most patients treated with the Kocher-Langenbeck approach, we use indomethacin (25 mg three times a day for 4 to 6 weeks) or occasionally radiation therapy with a one-time dose of 700 cGy in patients in whom indometha-cin is contraindicated. We use radiation therapy more fre-quently in patients with extensile exposures. We tend not to use routine radiation therapy in very young patients. We débride devitalized gluteus minimus muscle as advocated by Rath et al.
Thromboembolic complications can be devastating; the reported risk of pulmonary embolism ranges from 2% to 6%. Deep vein thrombosis has been reported to occur in 8% to 61% of patients with acetabular fractures; however, this depends on the method used to detect the thrombosis. Venous Doppler ultrasound examination may underestimate the presence of significant clots because of the inability of ultrasound to detect intrapelvic vein thrombosis reliably in comparison to more invasive venographic studies.
Magnetic resonance venography (MRV) has been shown to be more sensitive than venography in detecting clots within the intrapelvic veins and contralateral extremity, detecting asymptomatic deep vein thrombosis in 34% of patients, 49% of which were above the level of the inguinal ligament. Other authors, however, found that MRV and contrast-enhanced CT both had high false-positive rates for detecting deep vein thrombosis when correlated with selective venography and recommended that if either contrast-enhanced CT or MRV is used as a screening test for asymptomatic deep vein throm-bosis, correlating selective venography should be used before opting for aggressive prophylactic treatments such as inferior vena cava filters. Slobogean et al. performed a meta-analysis of the available literature involving recommendations for thromboembolic prophylaxis in patients with pelvic and ace-tabular fractures and could not identify adequate evidence to support one regimen over another.
Our current protocol involves the use of subcutaneous heparin or enoxaparin as well as intermittent compression boots while patients are awaiting surgery. We obtain a preop-erative screening duplex Doppler scan in any patient in whom the injury is more than 4 days old and in patients who have not received prophylaxis. We use Greenfield vena cava filters in patients with abnormalities on duplex scans and also occa-sionally use them in other high-risk groups. Identified high-risk groups include patients older than 60 years, patients with contraindications to anticoagulation, and patients in whom morbid obesity, malignant disease, or a history of prior deep vein thrombosis is a factor. Postoperatively, anticoagulation with enoxaparin followed by warfarin is continued for 6 to 12 weeks unless it is medically contraindicated.
TOTAL HIP ARTHROPLASTY AS TREATMENT OF ACETABULAR FRACTURE
Total hip arthroplasty has been used for treatment of some acetabular fractures with extremely poor prognoses, using
CHAPTER 56 FRACTURES OF ACETABULUM AND PELVIS 2799
10-year loosening rate reported later in a similar population of patients.
PELVIC FRACTURES
Fractures of the adult pelvis, exclusive of the acetabulum, generally are either stable fractures resulting from low-energy trauma, such as falls in elderly patients, or fractures caused by high-energy trauma that result in significant morbidity and mortality. As is true of fractures of other bones, low-energy trauma to the pelvis generally produces stable frac-tures that can be treated symptomatically with crutch- or walker-assisted ambulation and that can be expected to heal uneventfully in most patients. High-energy pelvic fractures often are managed operatively, with the treatment method determined by the degree of pelvic stability remaining after the injury. The focus here is on these high-energy injuries, their management in both the resuscitative and reconstruc-tive phases, and their potential complications.
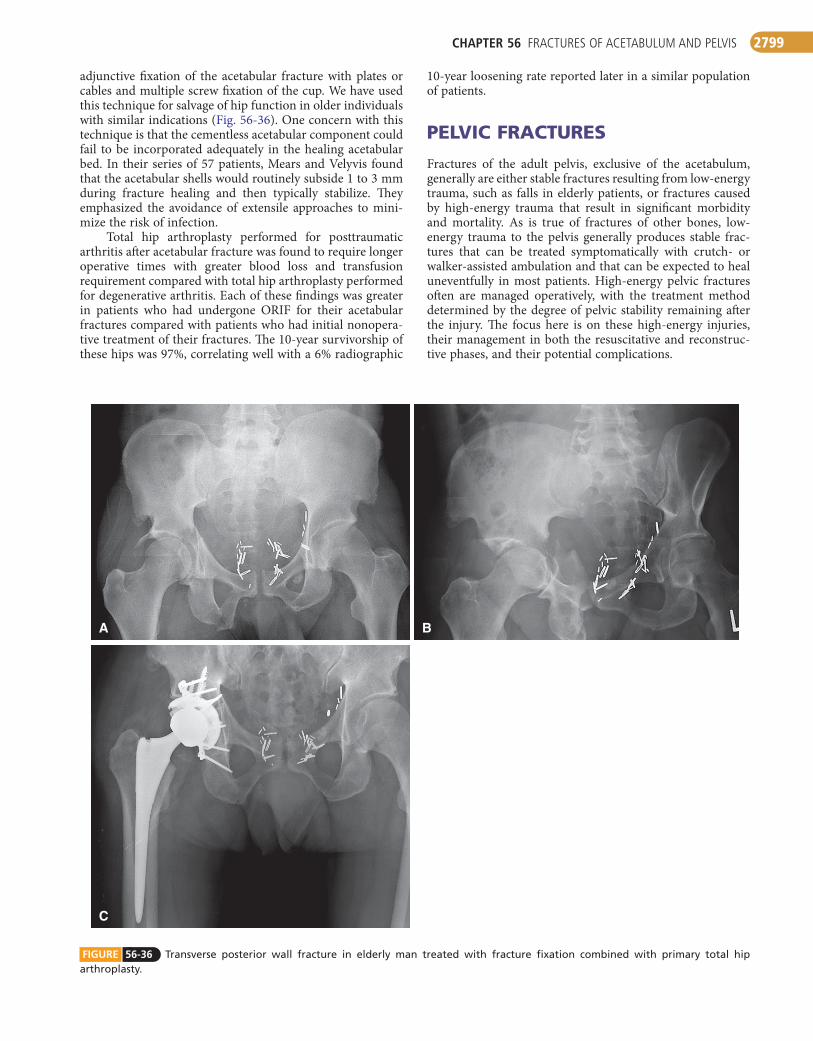
adjunctive fixation of the acetabular fracture with plates or cables and multiple screw fixation of the cup. We have used this technique for salvage of hip function in older individuals with similar indications (Fig. 56-36). One concern with this technique is that the cementless acetabular component could fail to be incorporated adequately in the healing acetabular bed. In their series of 57 patients, Mears and Velyvis found that the acetabular shells would routinely subside 1 to 3 mm during fracture healing and then typically stabilize. They emphasized the avoidance of extensile approaches to mini-mize the risk of infection.
Total hip arthroplasty performed for posttraumatic arthritis after acetabular fracture was found to require longer operative times with greater blood loss and transfusion requirement compared with total hip arthroplasty performed for degenerative arthritis. Each of these findings was greater in patients who had undergone ORIF for their acetabular fractures compared with patients who had initial nonopera-tive treatment of their fractures. The 10-year survivorship of these hips was 97%, correlating well with a 6% radiographic
FIGURE 56-36 Transverse posterior wall fracture in elderly man treated with fracture fixation combined with primary total hip arthroplasty.
A
C
B
PART XV FRACTURES AND DISLOCATIONS IN ADULTS2800
when a pelvic orthotic device was used to apply circumfer-ential pressure in patients with unstable, complex pelvic fractures, but Ghaemmaghami et al. did not find that pelvic binders reduced hemorrhage or mortality associated with pelvic fractures. One recent study noted inaccurate place-ment, above the level of the greater trochanters, to be associ-ated with inadequate fracture reduction.
Once in the controlled environment of the operating room, an external fixator can be applied to maintain stability of the pelvis while allowing access to the abdomen and perineum. A reduction in transfusion requirements has been reported in patients with unstable pelvic fractures who were treated with immediate external fixation compared with those who did not undergo immediate fixation. Injuries with significant posterior displacement may benefit from a C-clamp type of external fixator, ideally applied in the operat-ing room when the situation allows (see Technique 56-3).
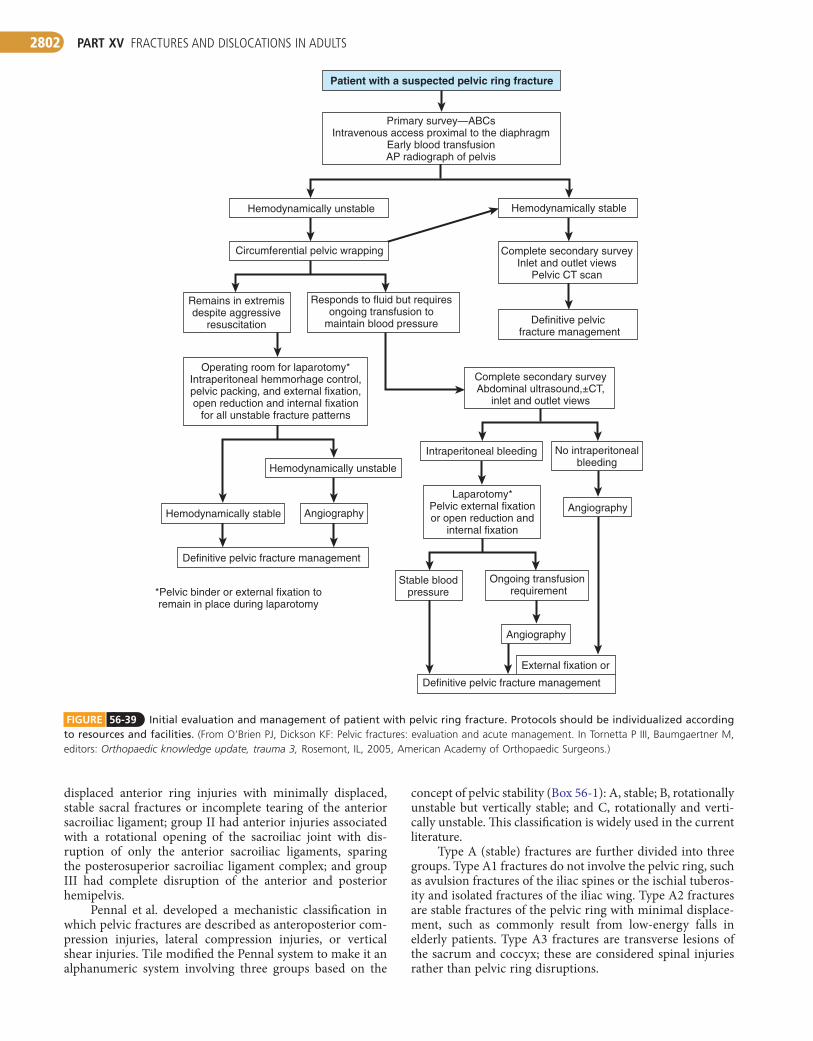
The patient with a pelvic ring injury, persistent hypoten-sion after circumferential pelvic binding, and no other source of bleeding should be considered for arteriography. Hemor-rhage frequently results from fracture surfaces and small vessels in the retroperitoneum. Only 5% to 10% of patients with pelvic fractures bleed from arterial sources identified by angiography and are treated with embolization. Higher rates of arterial bleeding in the geriatric population have been noted by Henry et al. An algorithm by O’Brien and Dickson (Fig. 56-39) has been proposed; however, the authors recom-mended that each institution develop its own protocol, depending on resources and facilities. More recently, favor-able results have been reported with retroperitoneal packing and external fixation. This technique is popular in Europe and has been used in some centers in the United States. Although the technique and algorithm are intriguing, their use requires further investigation in the United States where the imple-mentation of trauma care is very different.
Open pelvic fractures are extremely difficult injuries to manage, with reported mortality rates of up to 50%. If the retroperitoneal space is open, no tamponade effect occurs to prevent excessive bleeding. Sepsis caused by fecal contamina-tion is a major cause of mortality with this injury, and
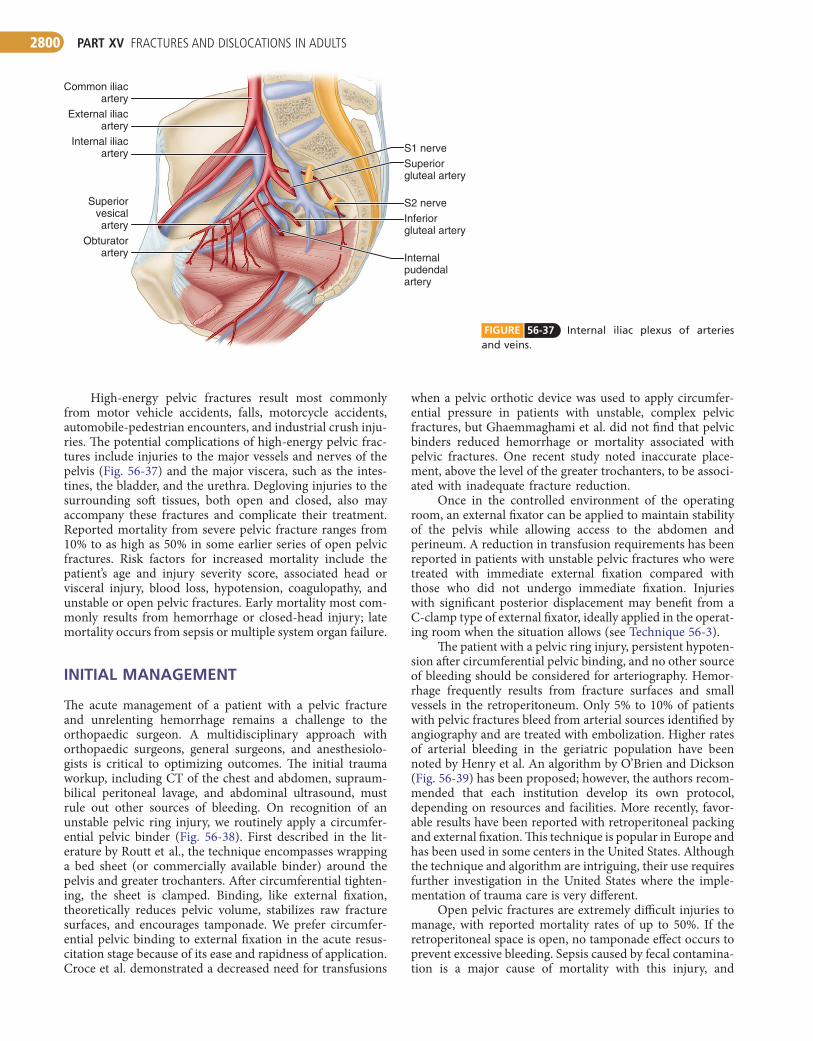
High-energy pelvic fractures result most commonly from motor vehicle accidents, falls, motorcycle accidents, automobile-pedestrian encounters, and industrial crush inju-ries. The potential complications of high-energy pelvic frac-tures include injuries to the major vessels and nerves of the pelvis (Fig. 56-37) and the major viscera, such as the intes-tines, the bladder, and the urethra. Degloving injuries to the surrounding soft tissues, both open and closed, also may accompany these fractures and complicate their treatment. Reported mortality from severe pelvic fracture ranges from 10% to as high as 50% in some earlier series of open pelvic fractures. Risk factors for increased mortality include the patient’s age and injury severity score, associated head or visceral injury, blood loss, hypotension, coagulopathy, and unstable or open pelvic fractures. Early mortality most com-monly results from hemorrhage or closed-head injury; late mortality occurs from sepsis or multiple system organ failure.
INITIAL MANAGEMENT
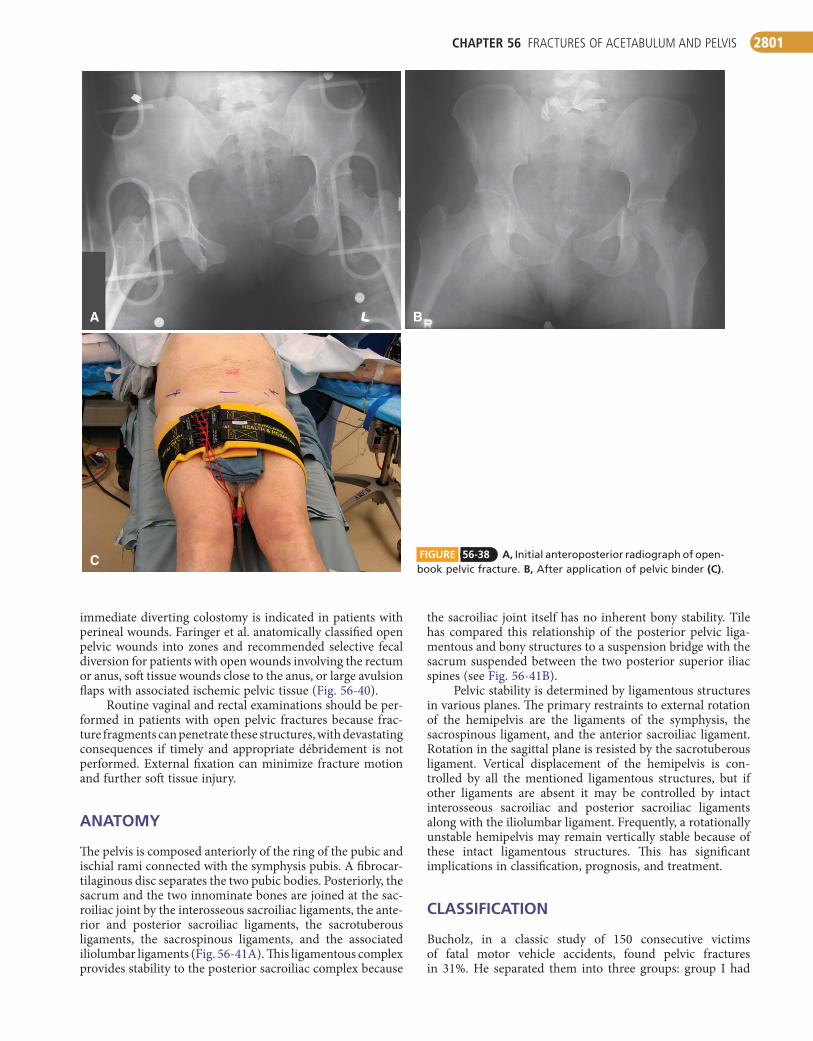
The acute management of a patient with a pelvic fracture and unrelenting hemorrhage remains a challenge to the orthopaedic surgeon. A multidisciplinary approach with orthopaedic surgeons, general surgeons, and anesthesiolo-gists is critical to optimizing outcomes. The initial trauma workup, including CT of the chest and abdomen, supraum-bilical peritoneal lavage, and abdominal ultrasound, must rule out other sources of bleeding. On recognition of an unstable pelvic ring injury, we routinely apply a circumfer-ential pelvic binder (Fig. 56-38). First described in the lit-erature by Routt et al., the technique encompasses wrapping a bed sheet (or commercially available binder) around the pelvis and greater trochanters. After circumferential tighten-ing, the sheet is clamped. Binding, like external fixation, theoretically reduces pelvic volume, stabilizes raw fracture surfaces, and encourages tamponade. We prefer circumfer-ential pelvic binding to external fixation in the acute resus-citation stage because of its ease and rapidness of application. Croce et al. demonstrated a decreased need for transfusions
FIGURE 56-37 Internal iliac plexus of arteries and veins.
Common iliacartery
External iliacartery
Internal iliacartery
Obturatorartery
Superiorvesicalartery
S1 nerve
S2 nerve
Internalpudendalartery
Superiorgluteal artery
Inferiorgluteal artery
CHAPTER 56 FRACTURES OF ACETABULUM AND PELVIS 2801
the sacroiliac joint itself has no inherent bony stability. Tile has compared this relationship of the posterior pelvic liga-mentous and bony structures to a suspension bridge with the sacrum suspended between the two posterior superior iliac spines (see Fig. 56-41B).
Pelvic stability is determined by ligamentous structures in various planes. The primary restraints to external rotation of the hemipelvis are the ligaments of the symphysis, the sacrospinous ligament, and the anterior sacroiliac ligament. Rotation in the sagittal plane is resisted by the sacrotuberous ligament. Vertical displacement of the hemipelvis is con-trolled by all the mentioned ligamentous structures, but if other ligaments are absent it may be controlled by intact interosseous sacroiliac and posterior sacroiliac ligaments along with the iliolumbar ligament. Frequently, a rotationally unstable hemipelvis may remain vertically stable because of these intact ligamentous structures. This has significant implications in classification, prognosis, and treatment.
CLASSIFICATION
Bucholz, in a classic study of 150 consecutive victims of fatal motor vehicle accidents, found pelvic fractures in 31%. He separated them into three groups: group I had
immediate diverting colostomy is indicated in patients with perineal wounds. Faringer et al. anatomically classified open pelvic wounds into zones and recommended selective fecal diversion for patients with open wounds involving the rectum or anus, soft tissue wounds close to the anus, or large avulsion flaps with associated ischemic pelvic tissue (Fig. 56-40).
Routine vaginal and rectal examinations should be per-formed in patients with open pelvic fractures because frac-ture fragments can penetrate these structures, with devastating consequences if timely and appropriate débridement is not performed. External fixation can minimize fracture motion and further soft tissue injury.
ANATOMY
The pelvis is composed anteriorly of the ring of the pubic and ischial rami connected with the symphysis pubis. A fibrocar-tilaginous disc separates the two pubic bodies. Posteriorly, the sacrum and the two innominate bones are joined at the sac-roiliac joint by the interosseous sacroiliac ligaments, the ante-rior and posterior sacroiliac ligaments, the sacrotuberous ligaments, the sacrospinous ligaments, and the associated iliolumbar ligaments (Fig. 56-41A). This ligamentous complex provides stability to the posterior sacroiliac complex because
A
C
B
FIGURE 56-38 A, Initial anteroposterior radiograph of open-book pelvic fracture. B, After application of pelvic binder (C).
PART XV FRACTURES AND DISLOCATIONS IN ADULTS2802
concept of pelvic stability (Box 56-1): A, stable; B, rotationally unstable but vertically stable; and C, rotationally and verti-cally unstable. This classification is widely used in the current literature.
Type A (stable) fractures are further divided into three groups. Type A1 fractures do not involve the pelvic ring, such as avulsion fractures of the iliac spines or the ischial tuberos-ity and isolated fractures of the iliac wing. Type A2 fractures are stable fractures of the pelvic ring with minimal displace-ment, such as commonly result from low-energy falls in elderly patients. Type A3 fractures are transverse lesions of the sacrum and coccyx; these are considered spinal injuries rather than pelvic ring disruptions.
displaced anterior ring injuries with minimally displaced, stable sacral fractures or incomplete tearing of the anterior sacroiliac ligament; group II had anterior injuries associated with a rotational opening of the sacroiliac joint with dis-ruption of only the anterior sacroiliac ligaments, sparing the posterosuperior sacroiliac ligament complex; and group III had complete disruption of the anterior and posterior hemipelvis.
Pennal et al. developed a mechanistic classification in which pelvic fractures are described as anteroposterior com-pression injuries, lateral compression injuries, or vertical shear injuries. Tile modified the Pennal system to make it an alphanumeric system involving three groups based on the
FIGURE 56-39 Initial evaluation and management of patient with pelvic ring fracture. Protocols should be individualized according to resources and facilities. (From O’Brien PJ, Dickson KF: Pelvic fractures: evaluation and acute management. In Tornetta P III, Baumgaertner M, editors: Orthopaedic knowledge update, trauma 3, Rosemont, IL, 2005, American Academy of Orthopaedic Surgeons.)
Patient with a suspected pelvic ring fracture
Primary survey—ABCsIntravenous access proximal to the diaphragm
Early blood transfusionAP radiograph of pelvis
Hemodynamically unstable Hemodynamically stable
Circumferential pelvic wrapping
Responds to fluid but requiresongoing transfusion to
maintain blood pressure
Complete secondary surveyInlet and outlet views
Pelvic CT scan
Definitive pelvic fracture management
Remains in extremisdespite aggressive
resuscitation
Operating room for laparotomy*Intraperitoneal hemmorhage control,pelvic packing, and external fixation,open reduction and internal fixation
for all unstable fracture patterns
Hemodynamically unstable
Hemodynamically stable Angiography
Definitive pelvic fracture management
Complete secondary surveyAbdominal ultrasound,±CT,
inlet and outlet views
Intraperitoneal bleeding No intraperitonealbleeding
Laparotomy*Pelvic external fixationor open reduction and
internal fixation
Angiography
Angiography
Stable bloodpressure
Ongoing transfusion requirement
External fixation or
Definitive pelvic fracture management
*Pelvic binder or external fixation toremain in place during laparotomy
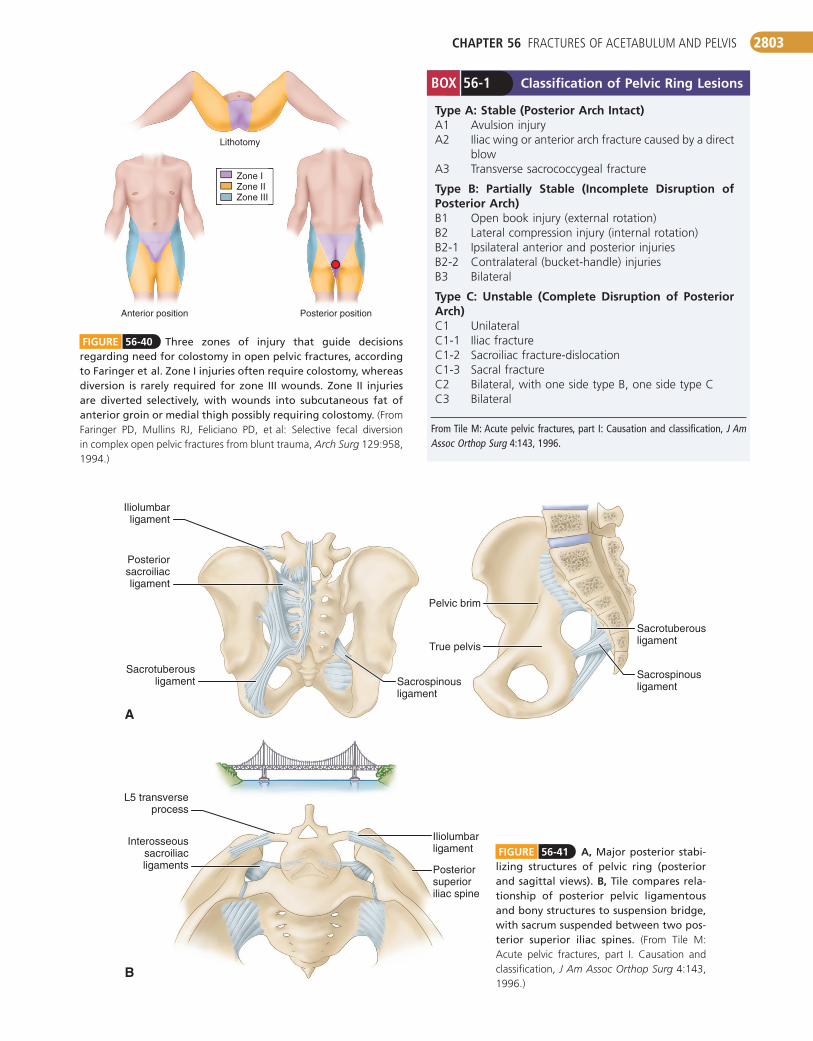
CHAPTER 56 FRACTURES OF ACETABULUM AND PELVIS 2803
FIGURE 56-40 Three zones of injury that guide decisions regarding need for colostomy in open pelvic fractures, according to Faringer et al. Zone I injuries often require colostomy, whereas diversion is rarely required for zone III wounds. Zone II injuries are diverted selectively, with wounds into subcutaneous fat of anterior groin or medial thigh possibly requiring colostomy. (From Faringer PD, Mullins RJ, Feliciano PD, et al: Selective fecal diversion in complex open pelvic fractures from blunt trauma, Arch Surg 129:958, 1994.)
Zone IZone IIZone III
Lithotomy
Anterior position Posterior position
B
A
Sacrotuberousligament
Iliolumbarligament
Posteriorsacroiliacligament
Pelvic brim
True pelvis
Sacrospinousligament
Sacrotuberousligament
Sacrospinousligament
Iliolumbarligament
L5 transverseprocess
Interosseoussacroiliacligaments Posterior
superioriliac spine
FIGURE 56-41 A, Major posterior stabi-lizing structures of pelvic ring (posterior and sagittal views). B, Tile compares rela-tionship of posterior pelvic ligamentous and bony structures to suspension bridge, with sacrum suspended between two pos-terior superior iliac spines. (From Tile M: Acute pelvic fractures, part I. Causation and classification, J Am Assoc Orthop Surg 4:143, 1996.)
Classification of Pelvic Ring LesionsBOX 56-1
Type A: Stable (Posterior Arch Intact)A1 Avulsion injuryA2 Iliac wing or anterior arch fracture caused by a direct
blowA3 Transverse sacrococcygeal fracture
Type B: Partially Stable (Incomplete Disruption of Posterior Arch)B1 Open book injury (external rotation)B2 Lateral compression injury (internal rotation)B2-1 Ipsilateral anterior and posterior injuriesB2-2 Contralateral (bucket-handle) injuriesB3 Bilateral
Type C: Unstable (Complete Disruption of Posterior Arch)C1 UnilateralC1-1 Iliac fractureC1-2 Sacroiliac fracture-dislocationC1-3 Sacral fractureC2 Bilateral, with one side type B, one side type CC3 Bilateral
From Tile M: Acute pelvic fractures, part I: Causation and classification, J Am Assoc Orthop Surg 4:143, 1996.
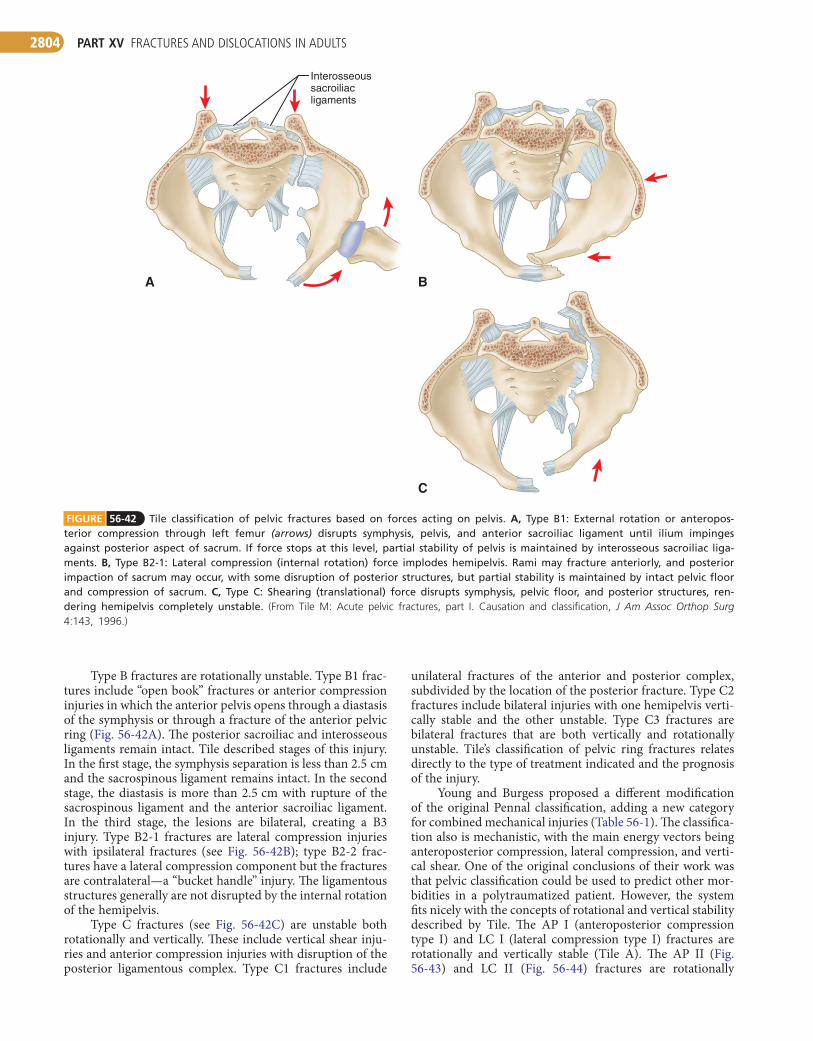
PART XV FRACTURES AND DISLOCATIONS IN ADULTS2804
unilateral fractures of the anterior and posterior complex, subdivided by the location of the posterior fracture. Type C2 fractures include bilateral injuries with one hemipelvis verti-cally stable and the other unstable. Type C3 fractures are bilateral fractures that are both vertically and rotationally unstable. Tile’s classification of pelvic ring fractures relates directly to the type of treatment indicated and the prognosis of the injury.
Young and Burgess proposed a different modification of the original Pennal classification, adding a new category for combined mechanical injuries (Table 56-1). The classifica-tion also is mechanistic, with the main energy vectors being anteroposterior compression, lateral compression, and verti-cal shear. One of the original conclusions of their work was that pelvic classification could be used to predict other mor-bidities in a polytraumatized patient. However, the system fits nicely with the concepts of rotational and vertical stability described by Tile. The AP I (anteroposterior compression type I) and LC I (lateral compression type I) fractures are rotationally and vertically stable (Tile A). The AP II (Fig. 56-43) and LC II (Fig. 56-44) fractures are rotationally
Type B fractures are rotationally unstable. Type B1 frac-tures include “open book” fractures or anterior compression injuries in which the anterior pelvis opens through a diastasis of the symphysis or through a fracture of the anterior pelvic ring (Fig. 56-42A). The posterior sacroiliac and interosseous ligaments remain intact. Tile described stages of this injury. In the first stage, the symphysis separation is less than 2.5 cm and the sacrospinous ligament remains intact. In the second stage, the diastasis is more than 2.5 cm with rupture of the sacrospinous ligament and the anterior sacroiliac ligament. In the third stage, the lesions are bilateral, creating a B3 injury. Type B2-1 fractures are lateral compression injuries with ipsilateral fractures (see Fig. 56-42B); type B2-2 frac-tures have a lateral compression component but the fractures are contralateral—a “bucket handle” injury. The ligamentous structures generally are not disrupted by the internal rotation of the hemipelvis.
Type C fractures (see Fig. 56-42C) are unstable both rotationally and vertically. These include vertical shear inju-ries and anterior compression injuries with disruption of the posterior ligamentous complex. Type C1 fractures include
FIGURE 56-42 Tile classification of pelvic fractures based on forces acting on pelvis. A, Type B1: External rotation or anteropos-terior compression through left femur (arrows) disrupts symphysis, pelvis, and anterior sacroiliac ligament until ilium impinges against posterior aspect of sacrum. If force stops at this level, partial stability of pelvis is maintained by interosseous sacroiliac liga-ments. B, Type B2-1: Lateral compression (internal rotation) force implodes hemipelvis. Rami may fracture anteriorly, and posterior impaction of sacrum may occur, with some disruption of posterior structures, but partial stability is maintained by intact pelvic floor and compression of sacrum. C, Type C: Shearing (translational) force disrupts symphysis, pelvic floor, and posterior structures, ren-dering hemipelvis completely unstable. (From Tile M: Acute pelvic fractures, part I. Causation and classification, J Am Assoc Orthop Surg 4:143, 1996.)
C
BA
Interosseous sacroiliac ligaments
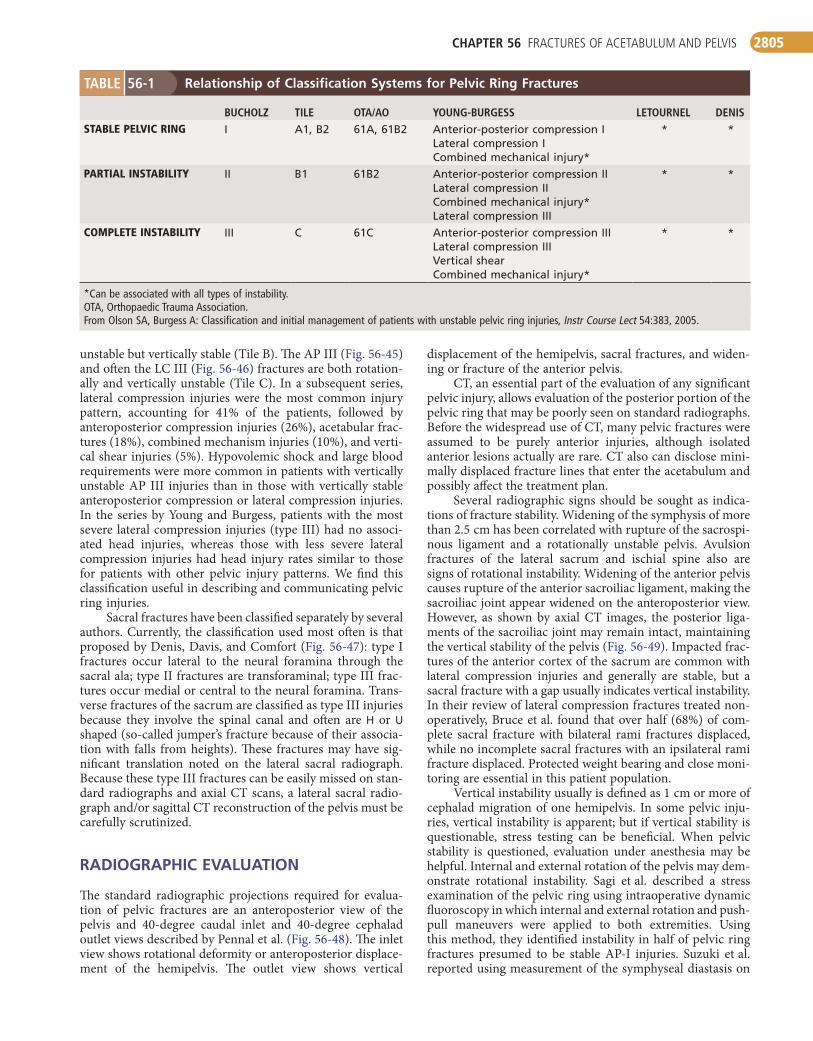
CHAPTER 56 FRACTURES OF ACETABULUM AND PELVIS 2805
displacement of the hemipelvis, sacral fractures, and widen-ing or fracture of the anterior pelvis.
CT, an essential part of the evaluation of any significant pelvic injury, allows evaluation of the posterior portion of the pelvic ring that may be poorly seen on standard radiographs. Before the widespread use of CT, many pelvic fractures were assumed to be purely anterior injuries, although isolated anterior lesions actually are rare. CT also can disclose mini-mally displaced fracture lines that enter the acetabulum and possibly affect the treatment plan.
Several radiographic signs should be sought as indica-tions of fracture stability. Widening of the symphysis of more than 2.5 cm has been correlated with rupture of the sacrospi-nous ligament and a rotationally unstable pelvis. Avulsion fractures of the lateral sacrum and ischial spine also are signs of rotational instability. Widening of the anterior pelvis causes rupture of the anterior sacroiliac ligament, making the sacroiliac joint appear widened on the anteroposterior view. However, as shown by axial CT images, the posterior liga-ments of the sacroiliac joint may remain intact, maintaining the vertical stability of the pelvis (Fig. 56-49). Impacted frac-tures of the anterior cortex of the sacrum are common with lateral compression injuries and generally are stable, but a sacral fracture with a gap usually indicates vertical instability. In their review of lateral compression fractures treated non-operatively, Bruce et al. found that over half (68%) of com-plete sacral fracture with bilateral rami fractures displaced, while no incomplete sacral fractures with an ipsilateral rami fracture displaced. Protected weight bearing and close moni-toring are essential in this patient population.
Vertical instability usually is defined as 1 cm or more of cephalad migration of one hemipelvis. In some pelvic inju-ries, vertical instability is apparent; but if vertical stability is questionable, stress testing can be beneficial. When pelvic stability is questioned, evaluation under anesthesia may be helpful. Internal and external rotation of the pelvis may dem-onstrate rotational instability. Sagi et al. described a stress examination of the pelvic ring using intraoperative dynamic fluoroscopy in which internal and external rotation and push-pull maneuvers were applied to both extremities. Using this method, they identified instability in half of pelvic ring fractures presumed to be stable AP-I injuries. Suzuki et al. reported using measurement of the symphyseal diastasis on
unstable but vertically stable (Tile B). The AP III (Fig. 56-45) and often the LC III (Fig. 56-46) fractures are both rotation-ally and vertically unstable (Tile C). In a subsequent series, lateral compression injuries were the most common injury pattern, accounting for 41% of the patients, followed by anteroposterior compression injuries (26%), acetabular frac-tures (18%), combined mechanism injuries (10%), and verti-cal shear injuries (5%). Hypovolemic shock and large blood requirements were more common in patients with vertically unstable AP III injuries than in those with vertically stable anteroposterior compression or lateral compression injuries. In the series by Young and Burgess, patients with the most severe lateral compression injuries (type III) had no associ-ated head injuries, whereas those with less severe lateral compression injuries had head injury rates similar to those for patients with other pelvic injury patterns. We find this classification useful in describing and communicating pelvic ring injuries.
Sacral fractures have been classified separately by several authors. Currently, the classification used most often is that proposed by Denis, Davis, and Comfort (Fig. 56-47): type I fractures occur lateral to the neural foramina through the sacral ala; type II fractures are transforaminal; type III frac-tures occur medial or central to the neural foramina. Trans-verse fractures of the sacrum are classified as type III injuries because they involve the spinal canal and often are H or U shaped (so-called jumper’s fracture because of their associa-tion with falls from heights). These fractures may have sig-nificant translation noted on the lateral sacral radiograph. Because these type III fractures can be easily missed on stan-dard radiographs and axial CT scans, a lateral sacral radio-graph and/or sagittal CT reconstruction of the pelvis must be carefully scrutinized.
RADIOGRAPHIC EVALUATION
The standard radiographic projections required for evalua-tion of pelvic fractures are an anteroposterior view of the pelvis and 40-degree caudal inlet and 40-degree cephalad outlet views described by Pennal et al. (Fig. 56-48). The inlet view shows rotational deformity or anteroposterior displace-ment of the hemipelvis. The outlet view shows vertical
Relationship of Classification Systems for Pelvic Ring Fractures
BUCHOLZ TILE OTA/AO YOUNG-BURGESS LETOURNEL DENISSTABLEPELVICRING I A1, B2 61A, 61B2 Anterior-posterior compression I
Lateral compression ICombined mechanical injury*
* *
PARTIALINSTABILITY II B1 61B2 Anterior-posterior compression IILateral compression IICombined mechanical injury*Lateral compression III
* *
COMPLETEINSTABILITY III C 61C Anterior-posterior compression IIILateral compression IIIVertical shearCombined mechanical injury*
* *
*Can be associated with all types of instability.OTA, Orthopaedic Trauma Association.From Olson SA, Burgess A: Classification and initial management of patients with unstable pelvic ring injuries, Instr Course Lect 54:383, 2005.
TABLE 56-1

PART XV FRACTURES AND DISLOCATIONS IN ADULTS2806
D
BA
C
E
FIGURE 56-43 Young and Burgess anteroposterior type II (AP II) pelvic ring injury with pubic diastasis treated with anterior fixation. A and B, Preoperative views. C-E, Postoperative antero-posterior, inlet, and outlet views.

CHAPTER 56 FRACTURES OF ACETABULUM AND PELVIS 2807
A
DC
B
FIGURE 56-44 Young and Burgess lateral compression type II (LC II) pelvic ring injury with posterior crescent fracture. A-D, Preopera-tive anteroposterior, oblique, inlet, and outlet views, respectively.
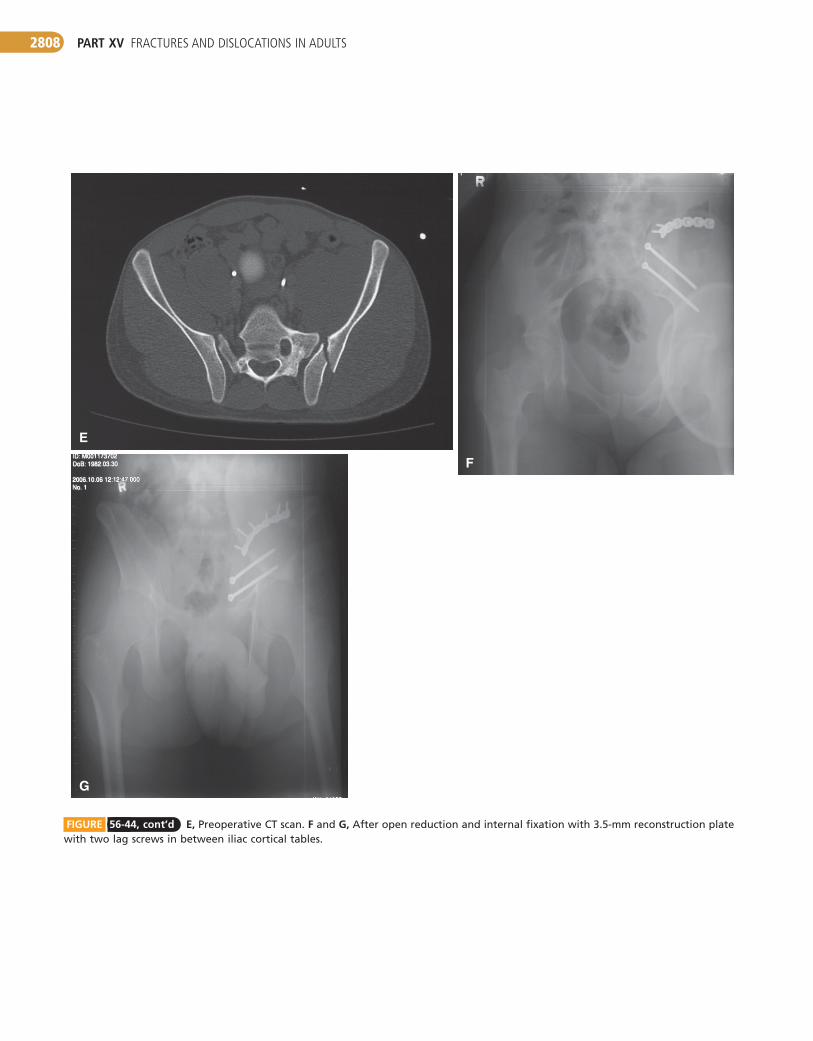
PART XV FRACTURES AND DISLOCATIONS IN ADULTS2808
F
G
E
FIGURE 56-44, cont’d E, Preoperative CT scan. F and G, After open reduction and internal fixation with 3.5-mm reconstruction plate with two lag screws in between iliac cortical tables.
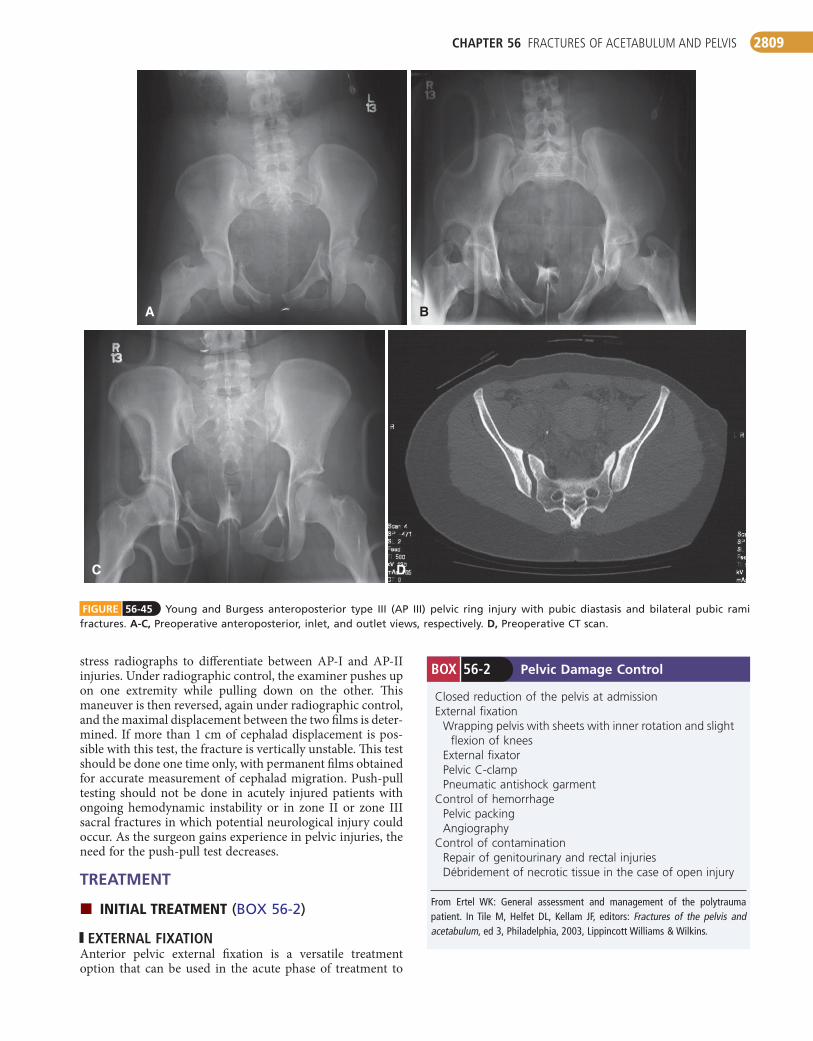
CHAPTER 56 FRACTURES OF ACETABULUM AND PELVIS 2809
DC
BA
FIGURE 56-45 Young and Burgess anteroposterior type III (AP III) pelvic ring injury with pubic diastasis and bilateral pubic rami fractures. A-C, Preoperative anteroposterior, inlet, and outlet views, respectively. D, Preoperative CT scan.
Pelvic Damage ControlBOX 56-2
Closed reduction of the pelvis at admissionExternal fixation
Wrapping pelvis with sheets with inner rotation and slight flexion of knees
External fixatorPelvic C-clampPneumatic antishock garment
Control of hemorrhagePelvic packingAngiography
Control of contaminationRepair of genitourinary and rectal injuriesDébridement of necrotic tissue in the case of open injury
From Ertel WK: General assessment and management of the polytrauma patient. In Tile M, Helfet DL, Kellam JF, editors: Fractures of the pelvis and acetabulum, ed 3, Philadelphia, 2003, Lippincott Williams & Wilkins.
stress radiographs to differentiate between AP-I and AP-II injuries. Under radiographic control, the examiner pushes up on one extremity while pulling down on the other. This maneuver is then reversed, again under radiographic control, and the maximal displacement between the two films is deter-mined. If more than 1 cm of cephalad displacement is pos-sible with this test, the fracture is vertically unstable. This test should be done one time only, with permanent films obtained for accurate measurement of cephalad migration. Push-pull testing should not be done in acutely injured patients with ongoing hemodynamic instability or in zone II or zone III sacral fractures in which potential neurological injury could occur. As the surgeon gains experience in pelvic injuries, the need for the push-pull test decreases.
TREATMENT
INITIALTREATMENT(BOX 56-2)
EXTERNAL FIXATIONAnterior pelvic external fixation is a versatile treatment option that can be used in the acute phase of treatment to
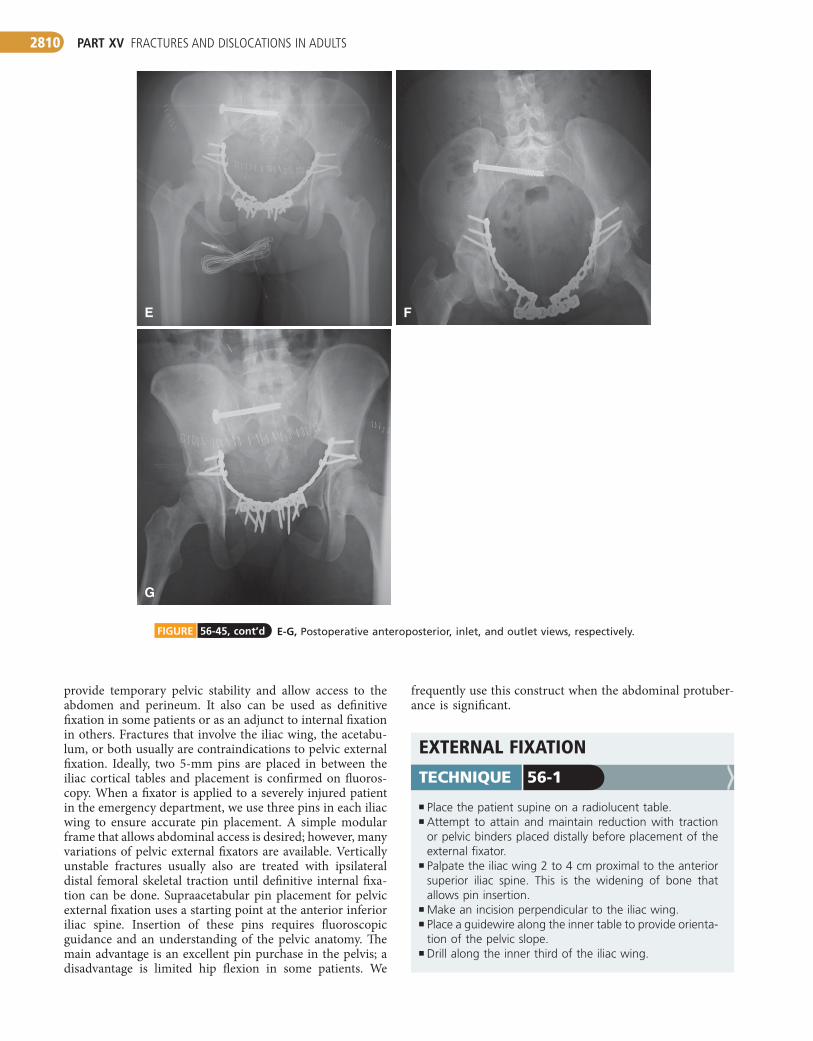
PART XV FRACTURES AND DISLOCATIONS IN ADULTS2810
E
G
F
E-G, Postoperative anteroposterior, inlet, and outlet views, respectively. FIGURE 56-45, cont’d
provide temporary pelvic stability and allow access to the abdomen and perineum. It also can be used as definitive fixation in some patients or as an adjunct to internal fixation in others. Fractures that involve the iliac wing, the acetabu-lum, or both usually are contraindications to pelvic external fixation. Ideally, two 5-mm pins are placed in between the iliac cortical tables and placement is confirmed on fluoros-copy. When a fixator is applied to a severely injured patient in the emergency department, we use three pins in each iliac wing to ensure accurate pin placement. A simple modular frame that allows abdominal access is desired; however, many variations of pelvic external fixators are available. Vertically unstable fractures usually also are treated with ipsilateral distal femoral skeletal traction until definitive internal fixa-tion can be done. Supraacetabular pin placement for pelvic external fixation uses a starting point at the anterior inferior iliac spine. Insertion of these pins requires fluoroscopic guidance and an understanding of the pelvic anatomy. The main advantage is an excellent pin purchase in the pelvis; a disadvantage is limited hip flexion in some patients. We
EXTERNALFIXATION
■ Place the patient supine on a radiolucent table.■ Attempt to attain and maintain reduction with traction
or pelvic binders placed distally before placement of the external fixator.
■ Palpate the iliac wing 2 to 4 cm proximal to the anterior superior iliac spine. This is the widening of bone that allows pin insertion.
■ Make an incision perpendicular to the iliac wing.■ Place a guidewire along the inner table to provide orienta-
tion of the pelvic slope.■ Drill along the inner third of the iliac wing.
TECHNIQUE 56-1
frequently use this construct when the abdominal protuber-ance is significant.
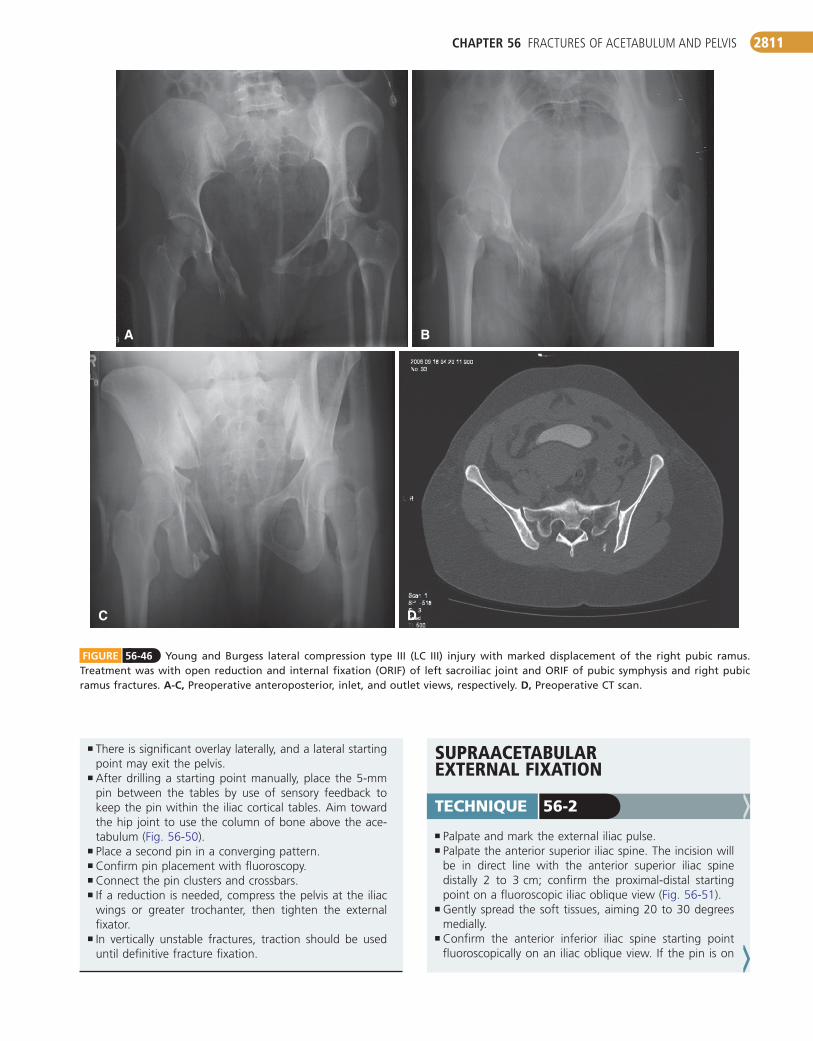
CHAPTER 56 FRACTURES OF ACETABULUM AND PELVIS 2811
DC
BA
FIGURE 56-46 Young and Burgess lateral compression type III (LC III) injury with marked displacement of the right pubic ramus. Treatment was with open reduction and internal fixation (ORIF) of left sacroiliac joint and ORIF of pubic symphysis and right pubic ramus fractures. A-C, Preoperative anteroposterior, inlet, and outlet views, respectively. D, Preoperative CT scan.
SUPRAACETABULAREXTERNALFIXATION
■ Palpate and mark the external iliac pulse.■ Palpate the anterior superior iliac spine. The incision will
be in direct line with the anterior superior iliac spine distally 2 to 3 cm; confirm the proximal-distal starting point on a fluoroscopic iliac oblique view (Fig. 56-51).
■ Gently spread the soft tissues, aiming 20 to 30 degrees medially.
■ Confirm the anterior inferior iliac spine starting point fluoroscopically on an iliac oblique view. If the pin is on
TECHNIQUE 56-2
■ There is significant overlay laterally, and a lateral starting point may exit the pelvis.
■ After drilling a starting point manually, place the 5-mm pin between the tables by use of sensory feedback to keep the pin within the iliac cortical tables. Aim toward the hip joint to use the column of bone above the ace-tabulum (Fig. 56-50).
■ Place a second pin in a converging pattern.■ Confirm pin placement with fluoroscopy.■ Connect the pin clusters and crossbars.■ If a reduction is needed, compress the pelvis at the iliac
wings or greater trochanter, then tighten the external fixator.
■ In vertically unstable fractures, traction should be used until definitive fracture fixation.
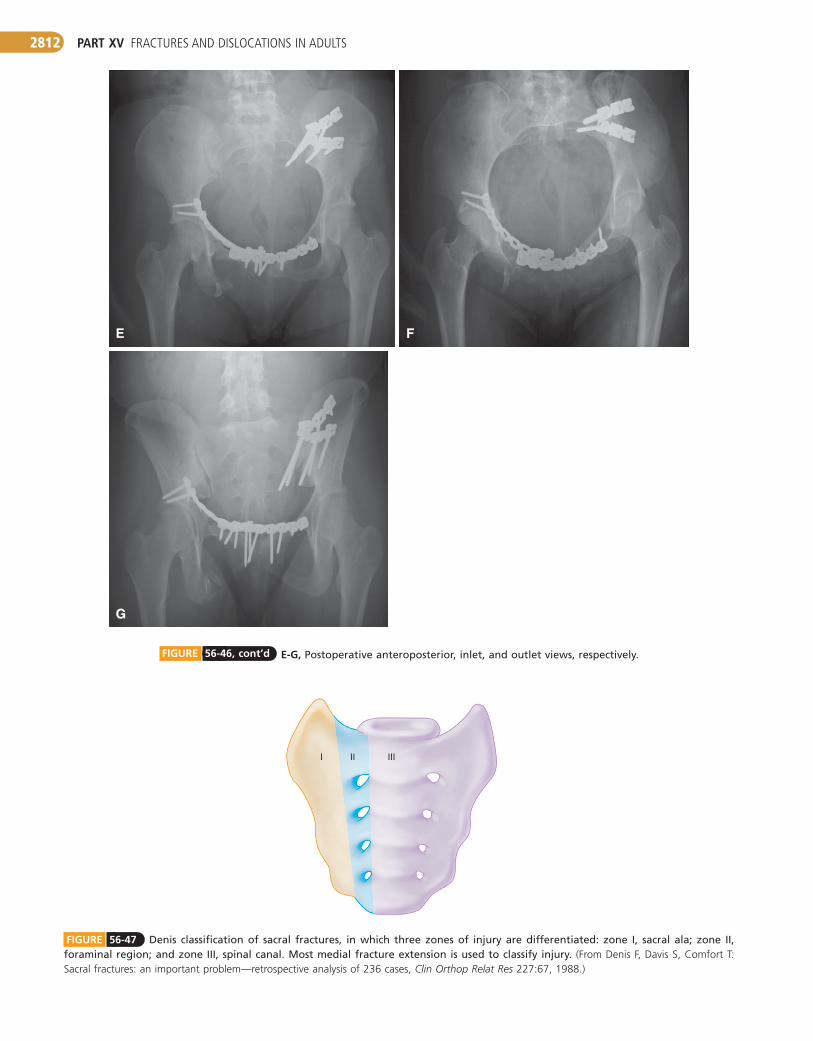
PART XV FRACTURES AND DISLOCATIONS IN ADULTS2812
E
G
F
E-G, Postoperative anteroposterior, inlet, and outlet views, respectively. FIGURE 56-46, cont’d
FIGURE 56-47 Denis classification of sacral fractures, in which three zones of injury are differentiated: zone I, sacral ala; zone II, foraminal region; and zone III, spinal canal. Most medial fracture extension is used to classify injury. (From Denis F, Davis S, Comfort T: Sacral fractures: an important problem—retrospective analysis of 236 cases, Clin Orthop Relat Res 227:67, 1988.)
II IIII
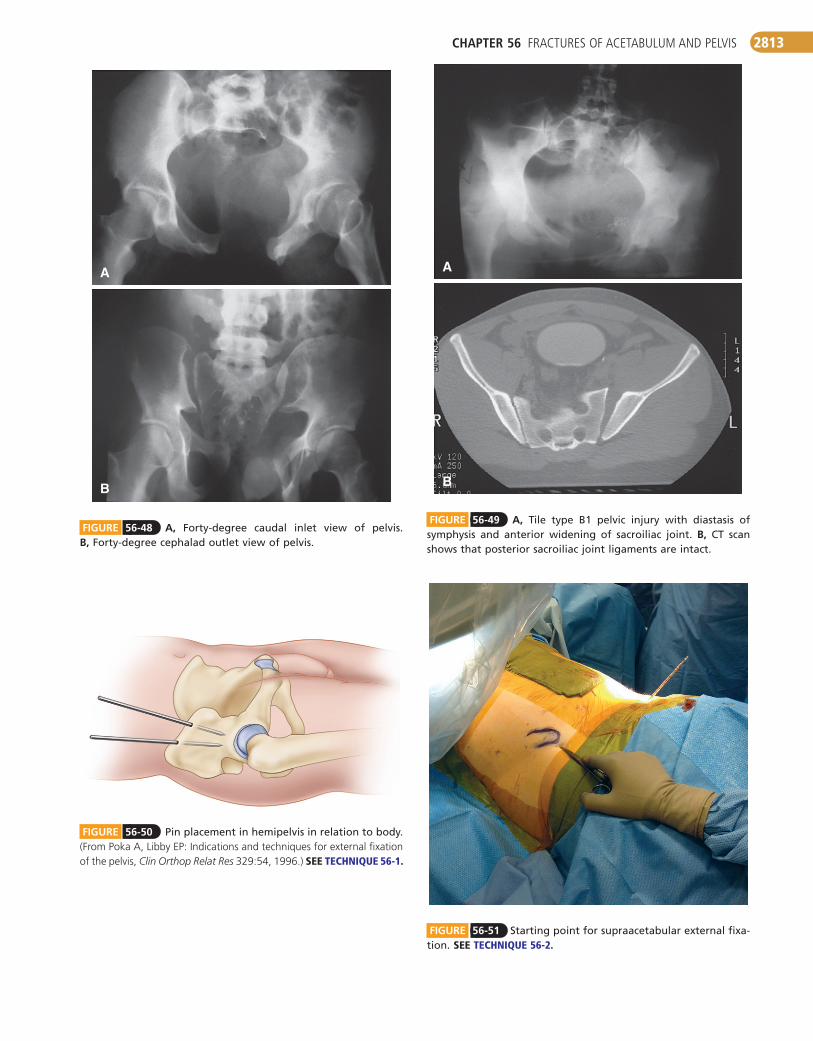
CHAPTER 56 FRACTURES OF ACETABULUM AND PELVIS 2813
FIGURE 56-48 A, Forty-degree caudal inlet view of pelvis. B, Forty-degree cephalad outlet view of pelvis.
B
A
FIGURE 56-49 A, Tile type B1 pelvic injury with diastasis of symphysis and anterior widening of sacroiliac joint. B, CT scan shows that posterior sacroiliac joint ligaments are intact.
B
A
FIGURE 56-51 Starting point for supraacetabular external fixa-tion. SEETECHNIQUE56-2.
FIGURE 56-50 Pin placement in hemipelvis in relation to body. (From Poka A, Libby EP: Indications and techniques for external fixation of the pelvis, Clin Orthop Relat Res 329:54, 1996.) SEE TECHNIQUE56-1.
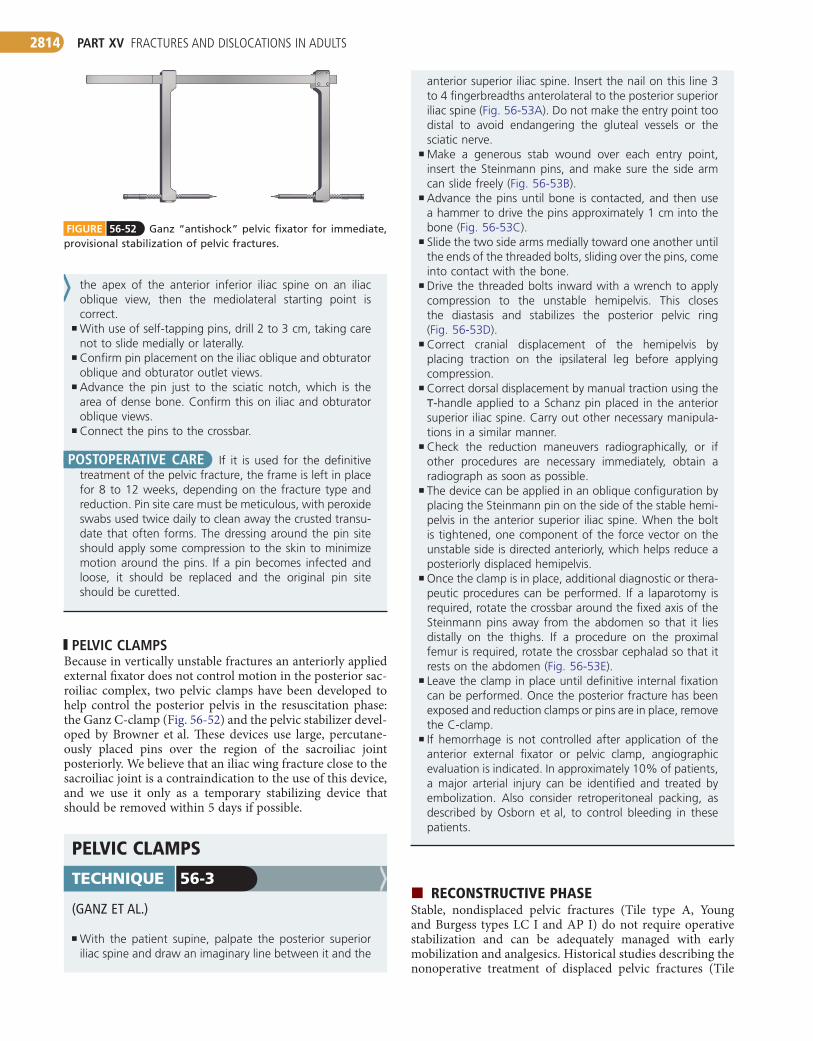
PART XV FRACTURES AND DISLOCATIONS IN ADULTS2814
FIGURE 56-52 Ganz “antishock” pelvic fixator for immediate, provisional stabilization of pelvic fractures.
the apex of the anterior inferior iliac spine on an iliac oblique view, then the mediolateral starting point is correct.
■ With use of self-tapping pins, drill 2 to 3 cm, taking care not to slide medially or laterally.
■ Confirm pin placement on the iliac oblique and obturator oblique and obturator outlet views.
■ Advance the pin just to the sciatic notch, which is the area of dense bone. Confirm this on iliac and obturator oblique views.
■ Connect the pins to the crossbar.
POSTOPERATIVE CARE If it is used for the definitive treatment of the pelvic fracture, the frame is left in place for 8 to 12 weeks, depending on the fracture type and reduction. Pin site care must be meticulous, with peroxide swabs used twice daily to clean away the crusted transu-date that often forms. The dressing around the pin site should apply some compression to the skin to minimize motion around the pins. If a pin becomes infected and loose, it should be replaced and the original pin site should be curetted.
PELVIC CLAMPSBecause in vertically unstable fractures an anteriorly applied external fixator does not control motion in the posterior sac-roiliac complex, two pelvic clamps have been developed to help control the posterior pelvis in the resuscitation phase: the Ganz C-clamp (Fig. 56-52) and the pelvic stabilizer devel-oped by Browner et al. These devices use large, percutane-ously placed pins over the region of the sacroiliac joint posteriorly. We believe that an iliac wing fracture close to the sacroiliac joint is a contraindication to the use of this device, and we use it only as a temporary stabilizing device that should be removed within 5 days if possible.
PELVICCLAMPS
(GANZ ET AL.)
■ With the patient supine, palpate the posterior superior iliac spine and draw an imaginary line between it and the
TECHNIQUE 56-3
anterior superior iliac spine. Insert the nail on this line 3 to 4 fingerbreadths anterolateral to the posterior superior iliac spine (Fig. 56-53A). Do not make the entry point too distal to avoid endangering the gluteal vessels or the sciatic nerve.
■ Make a generous stab wound over each entry point, insert the Steinmann pins, and make sure the side arm can slide freely (Fig. 56-53B).
■ Advance the pins until bone is contacted, and then use a hammer to drive the pins approximately 1 cm into the bone (Fig. 56-53C).
■ Slide the two side arms medially toward one another until the ends of the threaded bolts, sliding over the pins, come into contact with the bone.
■ Drive the threaded bolts inward with a wrench to apply compression to the unstable hemipelvis. This closes the diastasis and stabilizes the posterior pelvic ring (Fig. 56-53D).
■ Correct cranial displacement of the hemipelvis by placing traction on the ipsilateral leg before applying compression.
■ Correct dorsal displacement by manual traction using the T-handle applied to a Schanz pin placed in the anterior superior iliac spine. Carry out other necessary manipula-tions in a similar manner.
■ Check the reduction maneuvers radiographically, or if other procedures are necessary immediately, obtain a radiograph as soon as possible.
■ The device can be applied in an oblique configuration by placing the Steinmann pin on the side of the stable hemi-pelvis in the anterior superior iliac spine. When the bolt is tightened, one component of the force vector on the unstable side is directed anteriorly, which helps reduce a posteriorly displaced hemipelvis.
■ Once the clamp is in place, additional diagnostic or thera-peutic procedures can be performed. If a laparotomy is required, rotate the crossbar around the fixed axis of the Steinmann pins away from the abdomen so that it lies distally on the thighs. If a procedure on the proximal femur is required, rotate the crossbar cephalad so that it rests on the abdomen (Fig. 56-53E).
■ Leave the clamp in place until definitive internal fixation can be performed. Once the posterior fracture has been exposed and reduction clamps or pins are in place, remove the C-clamp.
■ If hemorrhage is not controlled after application of the anterior external fixator or pelvic clamp, angiographic evaluation is indicated. In approximately 10% of patients, a major arterial injury can be identified and treated by embolization. Also consider retroperitoneal packing, as described by Osborn et al, to control bleeding in these patients.
RECONSTRUCTIVEPHASEStable, nondisplaced pelvic fractures (Tile type A, Young and Burgess types LC I and AP I) do not require operative stabilization and can be adequately managed with early mobilization and analgesics. Historical studies describing the nonoperative treatment of displaced pelvic fractures (Tile
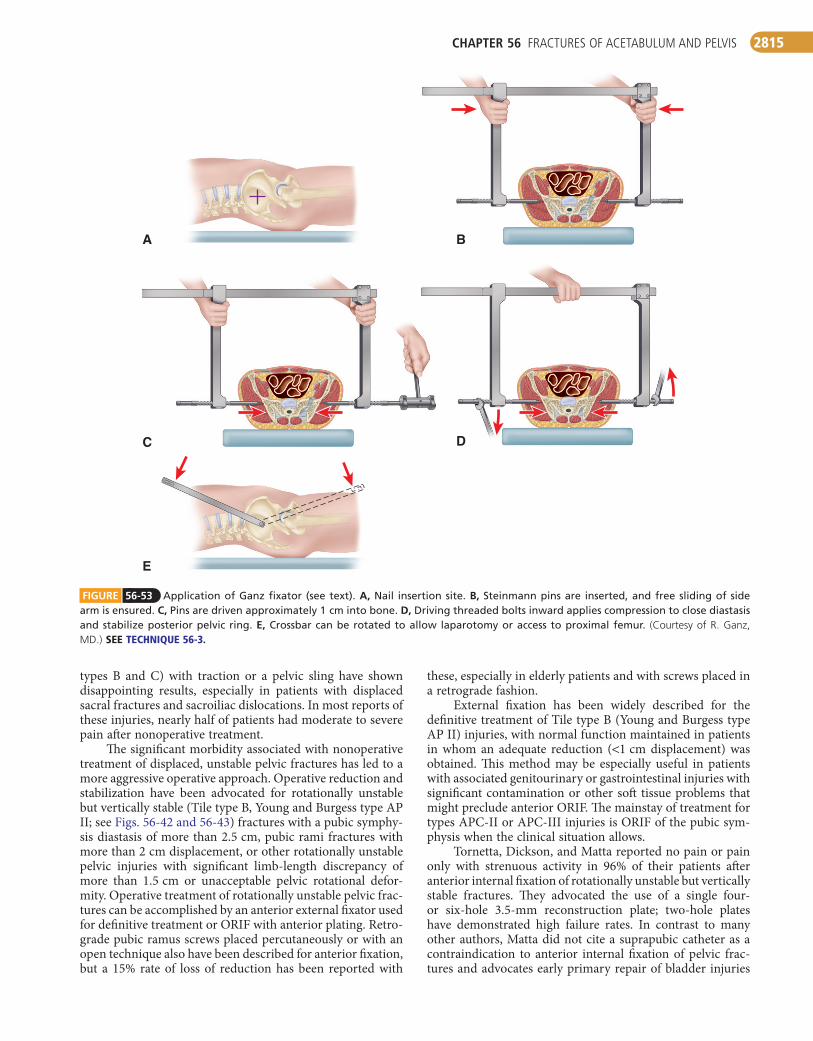
CHAPTER 56 FRACTURES OF ACETABULUM AND PELVIS 2815
these, especially in elderly patients and with screws placed in a retrograde fashion.
External fixation has been widely described for the definitive treatment of Tile type B (Young and Burgess type AP II) injuries, with normal function maintained in patients in whom an adequate reduction (<1 cm displacement) was obtained. This method may be especially useful in patients with associated genitourinary or gastrointestinal injuries with significant contamination or other soft tissue problems that might preclude anterior ORIF. The mainstay of treatment for types APC-II or APC-III injuries is ORIF of the pubic sym-physis when the clinical situation allows.
Tornetta, Dickson, and Matta reported no pain or pain only with strenuous activity in 96% of their patients after anterior internal fixation of rotationally unstable but vertically stable fractures. They advocated the use of a single four- or six-hole 3.5-mm reconstruction plate; two-hole plates have demonstrated high failure rates. In contrast to many other authors, Matta did not cite a suprapubic catheter as a contraindication to anterior internal fixation of pelvic frac-tures and advocates early primary repair of bladder injuries
types B and C) with traction or a pelvic sling have shown disappointing results, especially in patients with displaced sacral fractures and sacroiliac dislocations. In most reports of these injuries, nearly half of patients had moderate to severe pain after nonoperative treatment.
The significant morbidity associated with nonoperative treatment of displaced, unstable pelvic fractures has led to a more aggressive operative approach. Operative reduction and stabilization have been advocated for rotationally unstable but vertically stable (Tile type B, Young and Burgess type AP II; see Figs. 56-42 and 56-43) fractures with a pubic symphy-sis diastasis of more than 2.5 cm, pubic rami fractures with more than 2 cm displacement, or other rotationally unstable pelvic injuries with significant limb-length discrepancy of more than 1.5 cm or unacceptable pelvic rotational defor-mity. Operative treatment of rotationally unstable pelvic frac-tures can be accomplished by an anterior external fixator used for definitive treatment or ORIF with anterior plating. Retro-grade pubic ramus screws placed percutaneously or with an open technique also have been described for anterior fixation, but a 15% rate of loss of reduction has been reported with
FIGURE 56-53 Application of Ganz fixator (see text). A, Nail insertion site. B, Steinmann pins are inserted, and free sliding of side arm is ensured. C, Pins are driven approximately 1 cm into bone. D, Driving threaded bolts inward applies compression to close diastasis and stabilize posterior pelvic ring. E, Crossbar can be rotated to allow laparotomy or access to proximal femur. (Courtesy of R. Ganz, MD.) SEE TECHNIQUE56-3.
A B
C D
E

PART XV FRACTURES AND DISLOCATIONS IN ADULTS2816
to prevent contamination of the pelvic fracture hematoma. He reported no infections in seven patients with suprapubic catheters and anterior pelvic internal fixation. Tile advocated double plating of the symphysis in type C injuries when pos-terior fixation is contraindicated by soft tissue problems.
BA
FIGURE 56-54 Anterior internal fixation of pelvic fracture (see text). A, Patient positioning. B, Retractor placed. C and D, Type II symphysis diastasis is reduced with Weber clamp placed anterior to rectus muscle.
C D
OPENREDUCTIONANDINTERNALFIXATIONOFTHEPUBICSYMPHYSIS
■ Position the patient supine on a radiolucent table.■ Maintain the legs in internal rotation to aid in reductions
(Fig. 56-54A).■ Drape the area distal to the pubic tubercles.■ Use a Pfannenstiel incision (see Technique 1-73).■ Incise the rectus longitudinally at the decussation of the
fibers. Do not transect the rectus heads.■ Use a malleable retractor in the space of Retzius to protect
the bladder (Fig. 56-54B).
TECHNIQUE 56-4
■ Place narrow sharp Hohmann retractors underneath the rectus and over the pubis to expose the pubic symphysis (Fig. 56-54C and D).
■ Place a Weber pointed reduction clamp anteriorly onto the body of the pubis for reduction (Fig. 56-54E and F).
■ In fractures with cephalad displacement of the hemipel-vis, apply traction. In more severe cases, use pelvic reduc-tion forceps by placing a 4.5-mm screw anteriorly on each side of the symphysis. Use of a plate and nut on the displaced side will allow full mechanical advantage without the risk of screw pull-out (Fig. 56-54G).
■ After satisfactory reduction, place a six-hole curved 3-mm reconstruction plate on the superior surface of the sym-physis (Fig. 56-54H).
■ Eccentrically drill to yield a small amount of compression.■ Confirm reduction and fixation with fluoroscopy.■ For type C injuries for which posterior fixation is not pos-
sible, apply a double plate.■ Place a closed suction drain in the space of Retzius.■ In cases of pubic rami fractures in which a Pfannenstiel
approach is not sufficient for ORIF, use a modified Stoppa or ilioinguinal approach.
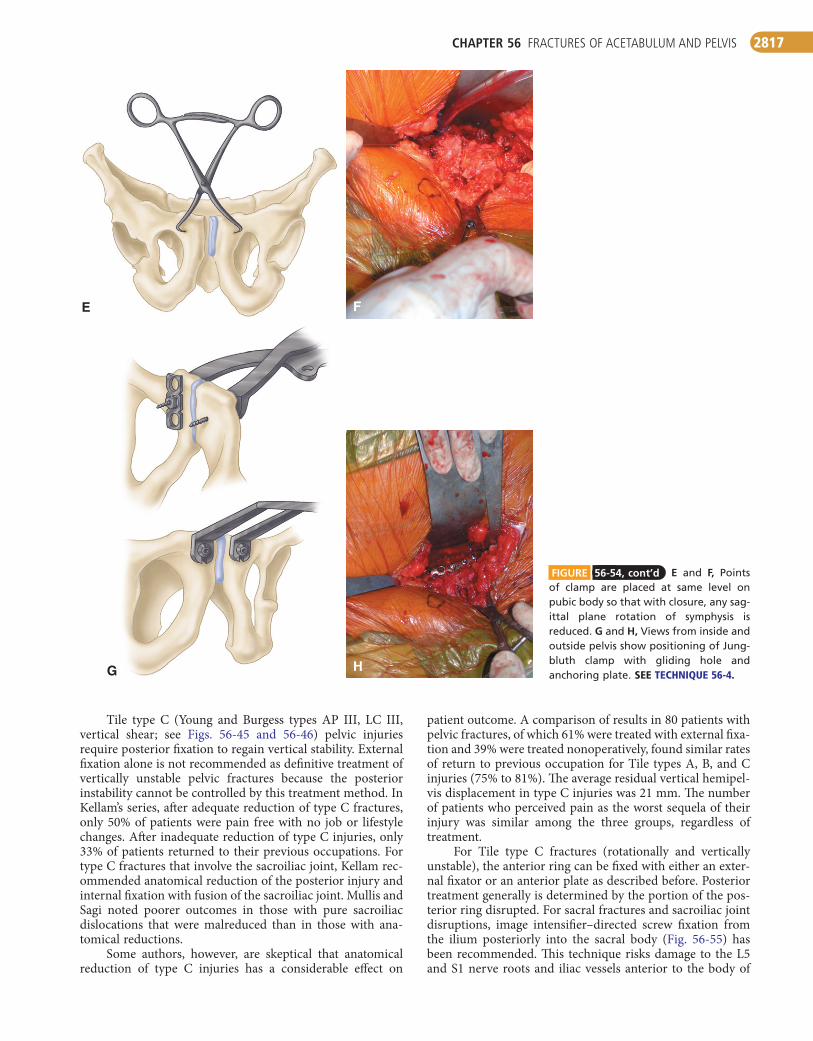
CHAPTER 56 FRACTURES OF ACETABULUM AND PELVIS 2817
E F
G H
FIGURE 56-54, cont’d E and F, Points of clamp are placed at same level on pubic body so that with closure, any sag-ittal plane rotation of symphysis is reduced. G and H, Views from inside and outside pelvis show positioning of Jung-bluth clamp with gliding hole and anchoring plate. SEETECHNIQUE56-4.
Tile type C (Young and Burgess types AP III, LC III, vertical shear; see Figs. 56-45 and 56-46) pelvic injuries require posterior fixation to regain vertical stability. External fixation alone is not recommended as definitive treatment of vertically unstable pelvic fractures because the posterior instability cannot be controlled by this treatment method. In Kellam’s series, after adequate reduction of type C fractures, only 50% of patients were pain free with no job or lifestyle changes. After inadequate reduction of type C injuries, only 33% of patients returned to their previous occupations. For type C fractures that involve the sacroiliac joint, Kellam rec-ommended anatomical reduction of the posterior injury and internal fixation with fusion of the sacroiliac joint. Mullis and Sagi noted poorer outcomes in those with pure sacroiliac dislocations that were malreduced than in those with ana-tomical reductions.
Some authors, however, are skeptical that anatomical reduction of type C injuries has a considerable effect on
patient outcome. A comparison of results in 80 patients with pelvic fractures, of which 61% were treated with external fixa-tion and 39% were treated nonoperatively, found similar rates of return to previous occupation for Tile types A, B, and C injuries (75% to 81%). The average residual vertical hemipel-vis displacement in type C injuries was 21 mm. The number of patients who perceived pain as the worst sequela of their injury was similar among the three groups, regardless of treatment.
For Tile type C fractures (rotationally and vertically unstable), the anterior ring can be fixed with either an exter-nal fixator or an anterior plate as described before. Posterior treatment generally is determined by the portion of the pos-terior ring disrupted. For sacral fractures and sacroiliac joint disruptions, image intensifier–directed screw fixation from the ilium posteriorly into the sacral body (Fig. 56-55) has been recommended. This technique risks damage to the L5 and S1 nerve roots and iliac vessels anterior to the body of
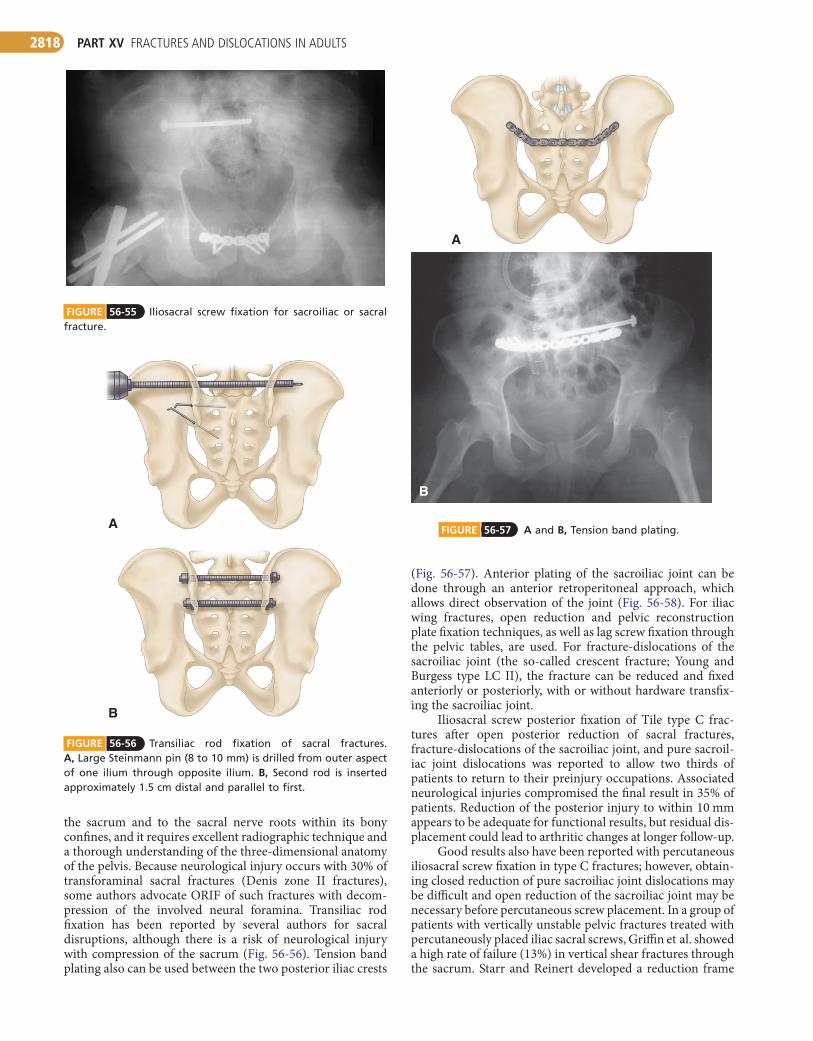
PART XV FRACTURES AND DISLOCATIONS IN ADULTS2818
FIGURE 56-55 Iliosacral screw fixation for sacroiliac or sacral fracture.
FIGURE 56-56 Transiliac rod fixation of sacral fractures. A, Large Steinmann pin (8 to 10 mm) is drilled from outer aspect of one ilium through opposite ilium. B, Second rod is inserted approximately 1.5 cm distal and parallel to first.
A
B
FIGURE 56-57 A and B, Tension band plating.
A
B
the sacrum and to the sacral nerve roots within its bony confines, and it requires excellent radiographic technique and a thorough understanding of the three-dimensional anatomy of the pelvis. Because neurological injury occurs with 30% of transforaminal sacral fractures (Denis zone II fractures), some authors advocate ORIF of such fractures with decom-pression of the involved neural foramina. Transiliac rod fixation has been reported by several authors for sacral disruptions, although there is a risk of neurological injury with compression of the sacrum (Fig. 56-56). Tension band plating also can be used between the two posterior iliac crests
(Fig. 56-57). Anterior plating of the sacroiliac joint can be done through an anterior retroperitoneal approach, which allows direct observation of the joint (Fig. 56-58). For iliac wing fractures, open reduction and pelvic reconstruction plate fixation techniques, as well as lag screw fixation through the pelvic tables, are used. For fracture-dislocations of the sacroiliac joint (the so-called crescent fracture; Young and Burgess type LC II), the fracture can be reduced and fixed anteriorly or posteriorly, with or without hardware transfix-ing the sacroiliac joint.
Iliosacral screw posterior fixation of Tile type C frac-tures after open posterior reduction of sacral fractures, fracture-dislocations of the sacroiliac joint, and pure sacroil-iac joint dislocations was reported to allow two thirds of patients to return to their preinjury occupations. Associated neurological injuries compromised the final result in 35% of patients. Reduction of the posterior injury to within 10 mm appears to be adequate for functional results, but residual dis-placement could lead to arthritic changes at longer follow-up.
Good results also have been reported with percutaneous iliosacral screw fixation in type C fractures; however, obtain-ing closed reduction of pure sacroiliac joint dislocations may be difficult and open reduction of the sacroiliac joint may be necessary before percutaneous screw placement. In a group of patients with vertically unstable pelvic fractures treated with percutaneously placed iliac sacral screws, Griffin et al. showed a high rate of failure (13%) in vertical shear fractures through the sacrum. Starr and Reinert developed a reduction frame

CHAPTER 56 FRACTURES OF ACETABULUM AND PELVIS 2819
FIGURE 56-58 A and B, Anterior plating of sacroiliac joint.
BA
that allows directed forces to be applied to aid in reduction (Fig. 56-59). Percutaneous transiliac fixation also has been used for posterior pelvic ring injuries in small numbers of patients for whom iliosacral screw fixation was not feasible.
Whatever fixation method is chosen, the surgeon must be familiar with the variations of upper sacral anatomy and fluoroscopic imaging, including the lateral sacral view, must be excellent. Graves and Routt recorded the sagittal plane tilt of the fluoroscope from the vertical required to obtain ideal inlet and outlet views during placement of iliosacral screws (Fig. 56-60). The average degree of tilt required to obtain the ideal inlet view was 25 degrees, and for the ideal outlet view it was 42 degrees.
FIGURE 56-59 Starr and Reinert reduction device (see text).
FIGURE 56-60 Patient positioning and average angular tilts from perpendicular to achieve ideal inlet and outlet views. (Redrawn from Graves ML, Routt MLC Jr: Iliosacral screw placement: are uniplanar changes realistic based on standard fluoroscopic imaging? J Trauma 71:204, 2011.)
Outlet viewInlet view
42° 25°
INTERNALFIXATION:POSTERIORSCREWFIXATIONOFSACRALFRACTURESANDSACROILIACDISLOCATIONS(PRONE)
(MATTA AND SAUCEDO)
■ Position the patient prone on a long radiolucent board to allow anteroposterior, caudal, and cephalad projections with an image intensifier (Fig. 56-61).
■ Use a standard posterior vertical incision, 2 cm lateral to the posterior superior iliac spine for sacroiliac dislocations, fracture-dislocations, or sacral fractures.
TECHNIQUE 56-5
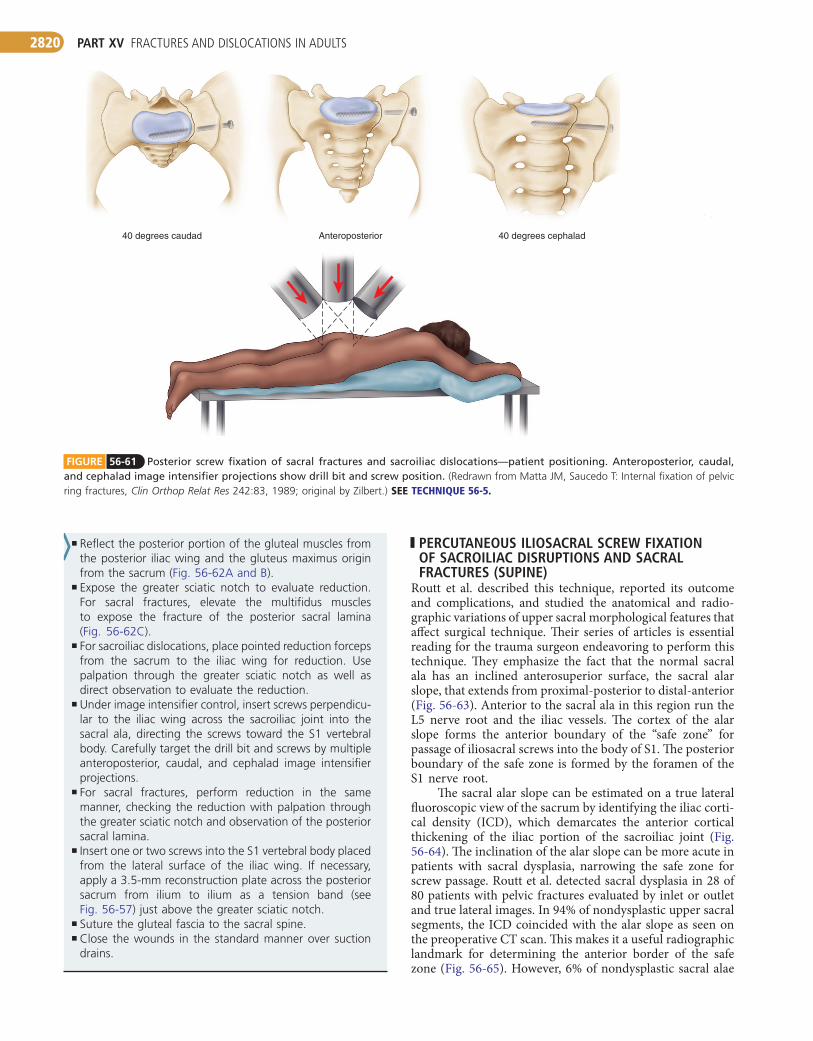
PART XV FRACTURES AND DISLOCATIONS IN ADULTS2820
PERCUTANEOUS ILIOSACRAL SCREW FIXATION OF SACROILIAC DISRUPTIONS AND SACRAL FRACTURES (SUPINE)
Routt et al. described this technique, reported its outcome and complications, and studied the anatomical and radio-graphic variations of upper sacral morphological features that affect surgical technique. Their series of articles is essential reading for the trauma surgeon endeavoring to perform this technique. They emphasize the fact that the normal sacral ala has an inclined anterosuperior surface, the sacral alar slope, that extends from proximal-posterior to distal-anterior (Fig. 56-63). Anterior to the sacral ala in this region run the L5 nerve root and the iliac vessels. The cortex of the alar slope forms the anterior boundary of the “safe zone” for passage of iliosacral screws into the body of S1. The posterior boundary of the safe zone is formed by the foramen of the S1 nerve root.
The sacral alar slope can be estimated on a true lateral fluoroscopic view of the sacrum by identifying the iliac corti-cal density (ICD), which demarcates the anterior cortical thickening of the iliac portion of the sacroiliac joint (Fig. 56-64). The inclination of the alar slope can be more acute in patients with sacral dysplasia, narrowing the safe zone for screw passage. Routt et al. detected sacral dysplasia in 28 of 80 patients with pelvic fractures evaluated by inlet or outlet and true lateral images. In 94% of nondysplastic upper sacral segments, the ICD coincided with the alar slope as seen on the preoperative CT scan. This makes it a useful radiographic landmark for determining the anterior border of the safe zone (Fig. 56-65). However, 6% of nondysplastic sacral alae
FIGURE 56-61 Posterior screw fixation of sacral fractures and sacroiliac dislocations—patient positioning. Anteroposterior, caudal, and cephalad image intensifier projections show drill bit and screw position. (Redrawn from Matta JM, Saucedo T: Internal fixation of pelvic ring fractures, Clin Orthop Relat Res 242:83, 1989; original by Zilbert.) SEE TECHNIQUE56-5.
40 degrees cephaladAnteroposterior40 degrees caudad
■ Reflect the posterior portion of the gluteal muscles from the posterior iliac wing and the gluteus maximus origin from the sacrum (Fig. 56-62A and B).
■ Expose the greater sciatic notch to evaluate reduction. For sacral fractures, elevate the multifidus muscles to expose the fracture of the posterior sacral lamina (Fig. 56-62C).
■ For sacroiliac dislocations, place pointed reduction forceps from the sacrum to the iliac wing for reduction. Use palpation through the greater sciatic notch as well as direct observation to evaluate the reduction.
■ Under image intensifier control, insert screws perpendicu-lar to the iliac wing across the sacroiliac joint into the sacral ala, directing the screws toward the S1 vertebral body. Carefully target the drill bit and screws by multiple anteroposterior, caudal, and cephalad image intensifier projections.
■ For sacral fractures, perform reduction in the same manner, checking the reduction with palpation through the greater sciatic notch and observation of the posterior sacral lamina.
■ Insert one or two screws into the S1 vertebral body placed from the lateral surface of the iliac wing. If necessary, apply a 3.5-mm reconstruction plate across the posterior sacrum from ilium to ilium as a tension band (see Fig. 56-57) just above the greater sciatic notch.
■ Suture the gluteal fascia to the sacral spine.■ Close the wounds in the standard manner over suction
drains.
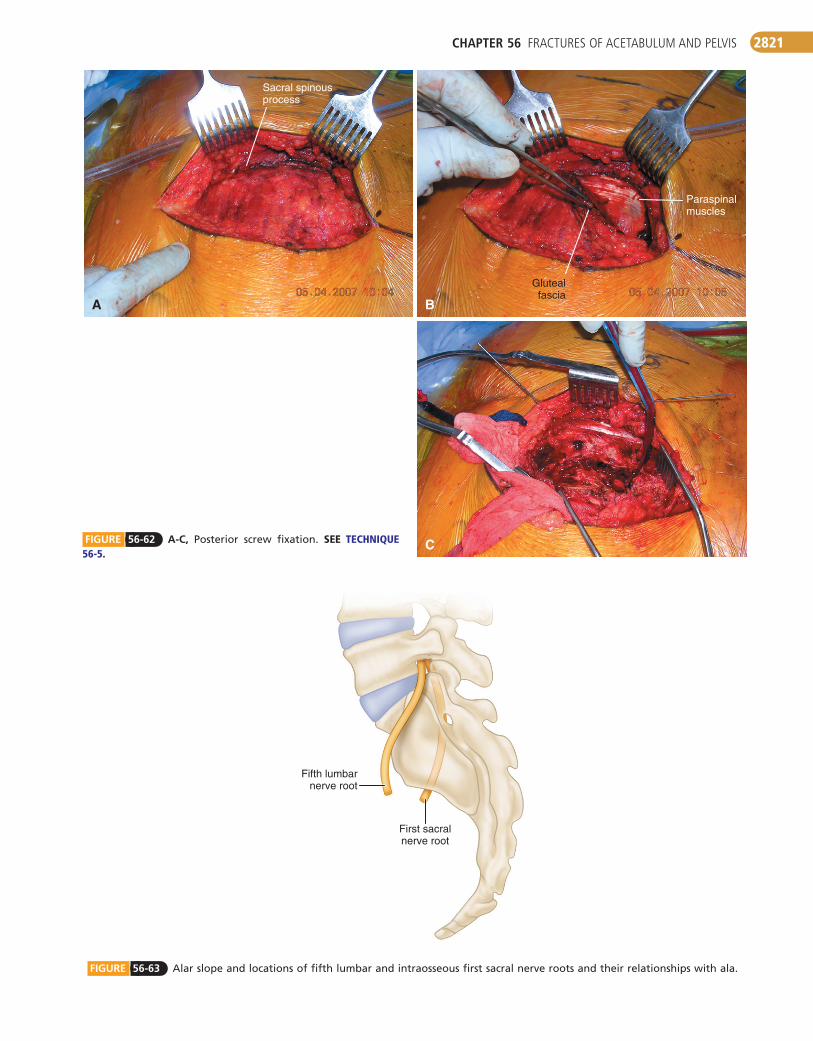
CHAPTER 56 FRACTURES OF ACETABULUM AND PELVIS 2821
FIGURE 56-63 Alar slope and locations of fifth lumbar and intraosseous first sacral nerve roots and their relationships with ala.
Fifth lumbarnerve root
First sacralnerve root
BA
C
Sacral spinousprocess
Glutealfascia
Paraspinalmuscles
FIGURE 56-62 A-C, Posterior screw fixation. SEE TECHNIQUE56-5.
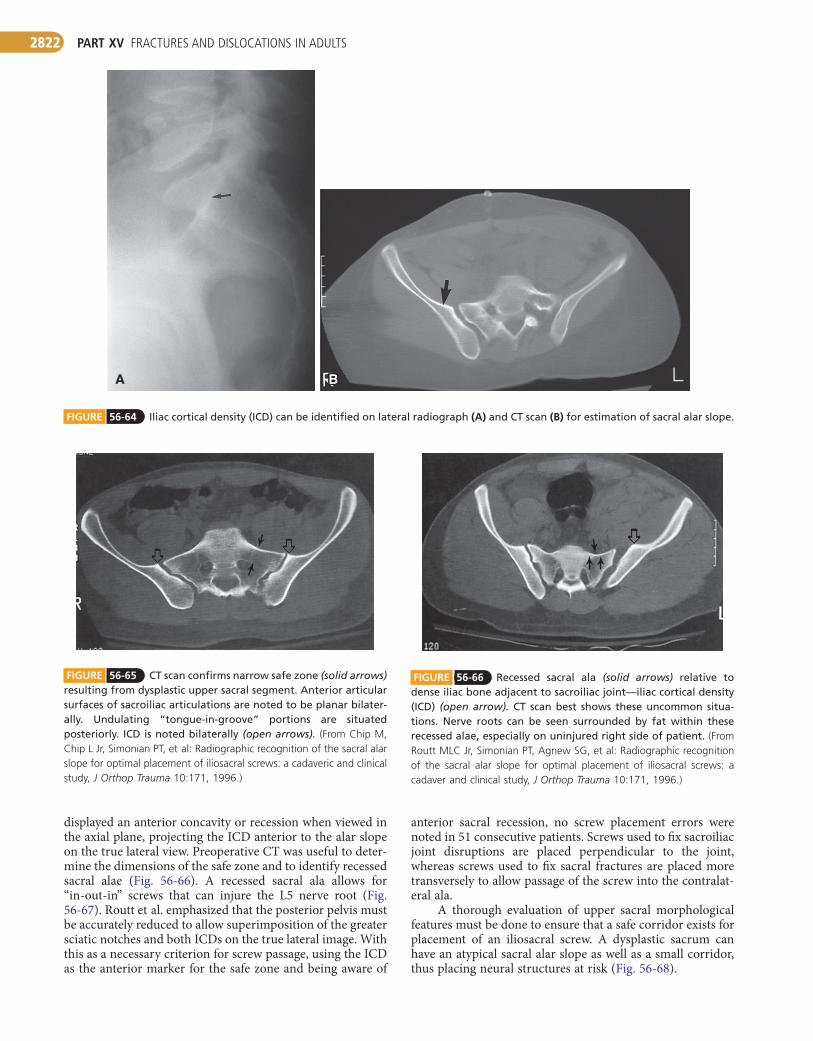
PART XV FRACTURES AND DISLOCATIONS IN ADULTS2822
anterior sacral recession, no screw placement errors were noted in 51 consecutive patients. Screws used to fix sacroiliac joint disruptions are placed perpendicular to the joint, whereas screws used to fix sacral fractures are placed more transversely to allow passage of the screw into the contralat-eral ala.
A thorough evaluation of upper sacral morphological features must be done to ensure that a safe corridor exists for placement of an iliosacral screw. A dysplastic sacrum can have an atypical sacral alar slope as well as a small corridor, thus placing neural structures at risk (Fig. 56-68).
displayed an anterior concavity or recession when viewed in the axial plane, projecting the ICD anterior to the alar slope on the true lateral view. Preoperative CT was useful to deter-mine the dimensions of the safe zone and to identify recessed sacral alae (Fig. 56-66). A recessed sacral ala allows for “in-out-in” screws that can injure the L5 nerve root (Fig. 56-67). Routt et al. emphasized that the posterior pelvis must be accurately reduced to allow superimposition of the greater sciatic notches and both ICDs on the true lateral image. With this as a necessary criterion for screw passage, using the ICD as the anterior marker for the safe zone and being aware of
FIGURE 56-64 Iliac cortical density (ICD) can be identified on lateral radiograph (A) and CT scan (B) for estimation of sacral alar slope.
BBA
FIGURE 56-65 CT scan confirms narrow safe zone (solid arrows) resulting from dysplastic upper sacral segment. Anterior articular surfaces of sacroiliac articulations are noted to be planar bilater-ally. Undulating “tongue-in-groove” portions are situated posteriorly. ICD is noted bilaterally (open arrows). (From Chip M, Chip L Jr, Simonian PT, et al: Radiographic recognition of the sacral alar slope for optimal placement of iliosacral screws: a cadaveric and clinical study, J Orthop Trauma 10:171, 1996.)
FIGURE 56-66 Recessed sacral ala (solid arrows) relative to dense iliac bone adjacent to sacroiliac joint—iliac cortical density (ICD) (open arrow). CT scan best shows these uncommon situa-tions. Nerve roots can be seen surrounded by fat within these recessed alae, especially on uninjured right side of patient. (From Routt MLC Jr, Simonian PT, Agnew SG, et al: Radiographic recognition of the sacral alar slope for optimal placement of iliosacral screws: a cadaver and clinical study, J Orthop Trauma 10:171, 1996.)

CHAPTER 56 FRACTURES OF ACETABULUM AND PELVIS 2823
FIGURE 56-68 Variable structure of upper sacrum on outlet views. ICD, iliac cortical density.
Variableslopes
ICD
C
BA
FIGURE 56-67 Screws inserted without use of lateral sacral image and ICD. Screws appear to be intraosseous on inlet (A) and outlet (B) pelvic radiographs, yet postoperative CT scan (C) shows that cephalad anterior No. 2 iliosacral screw on patient’s left side is extraosseous. Left L5 nerve root was injured. (From Routt MLC Jr, Simonian PT, Agnew SG, et al: Radiographic recognition of the sacral alar slope for optimal placement of iliosacral screws: a cadaver and clinical study, J Orthop Trauma 10:171, 1996.)
PERCUTANEOUSILIOSACRALSCREWFIXATIONOFSACROILIACDISRUPTIONSANDSACRALFRACTURES(SUPINE)
■ Position the patient supine on a radiolucent table. Place a soft support underneath the lumbosacral spine to elevate the patient from the table.
TECHNIQUE 56-6
■ Place the C-arm fluoroscopy unit opposite the injured hemipelvis.
■ Obtain anteroposterior, inlet, outlet, and lateral sacral views to ensure adequate visualization. The position of the inlet and outlet are noted to facilitate changing views throughout the case (Fig. 56-69A and B).
■ Reduce the posterior pelvis first. Aids for reduction include traction, Schanz screws in the iliac wings, anterior external fixation frame, and prior anterior pelvic internal fixation.
■ On the lateral sacral fluoroscopic view, identify the ante-rior and posterior portals of the first sacral segment. The exact starting point depends on the number of screws planned and the type of injury: sacral fractures require a transverse screw, whereas sacroiliac dislocations travel posteroinferior to anterior proximal (and require a screw perpendicular to the sacroiliac joint).
■ Mark the starting point on the skin and make a 1-cm stab incision.
■ Advance a cannulated guide into the ilium (Fig. 56-69C and D).
■ On the lateral view, place the tip of the guide on the ideal starting spot and impact it into place with a mallet to prevent slipping (Fig. 56-69E).
■ With use of biplanar imagery (inlet and outlet views), adjust the trajectory of the guide to safely enter the first sacral segment (Fig. 56-69F and G).
■ Advance the guidewire, confirming safe passage on both the inlet and outlet views (Fig. 56-69H to J).
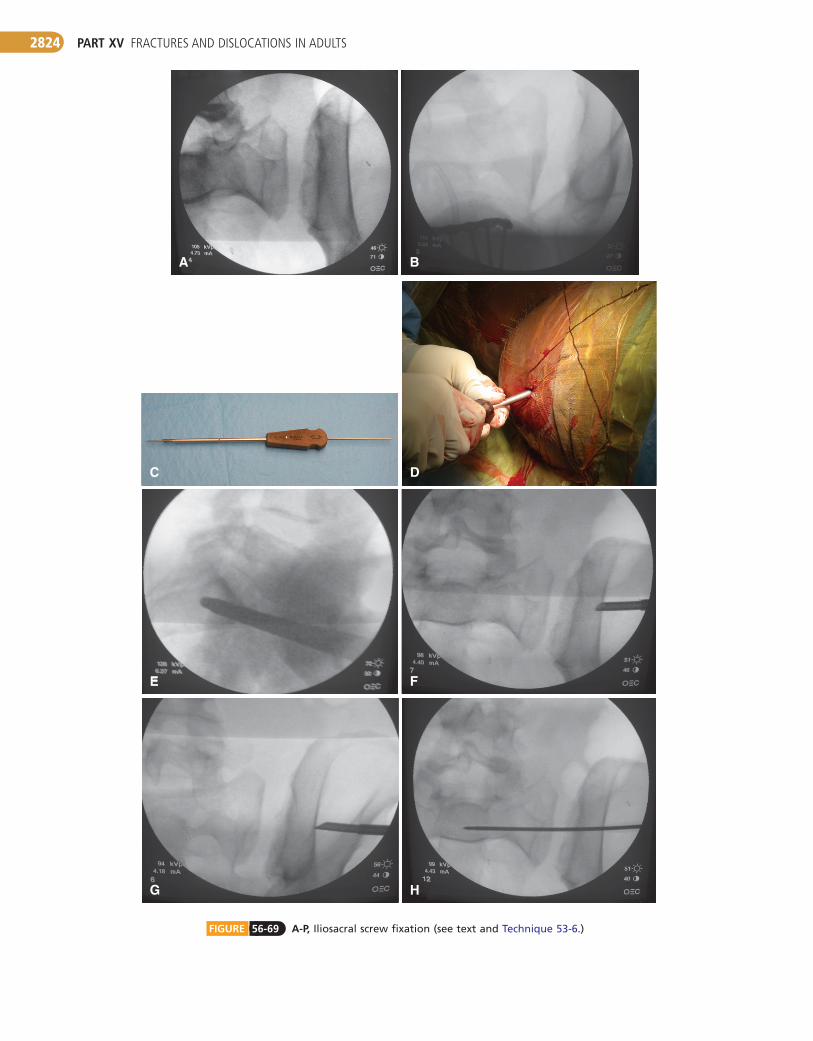
PART XV FRACTURES AND DISLOCATIONS IN ADULTS2824
FIGURE 56-69 A-P, Iliosacral screw fixation (see text and Technique 53-6.)
BA
HG
C
FE
D
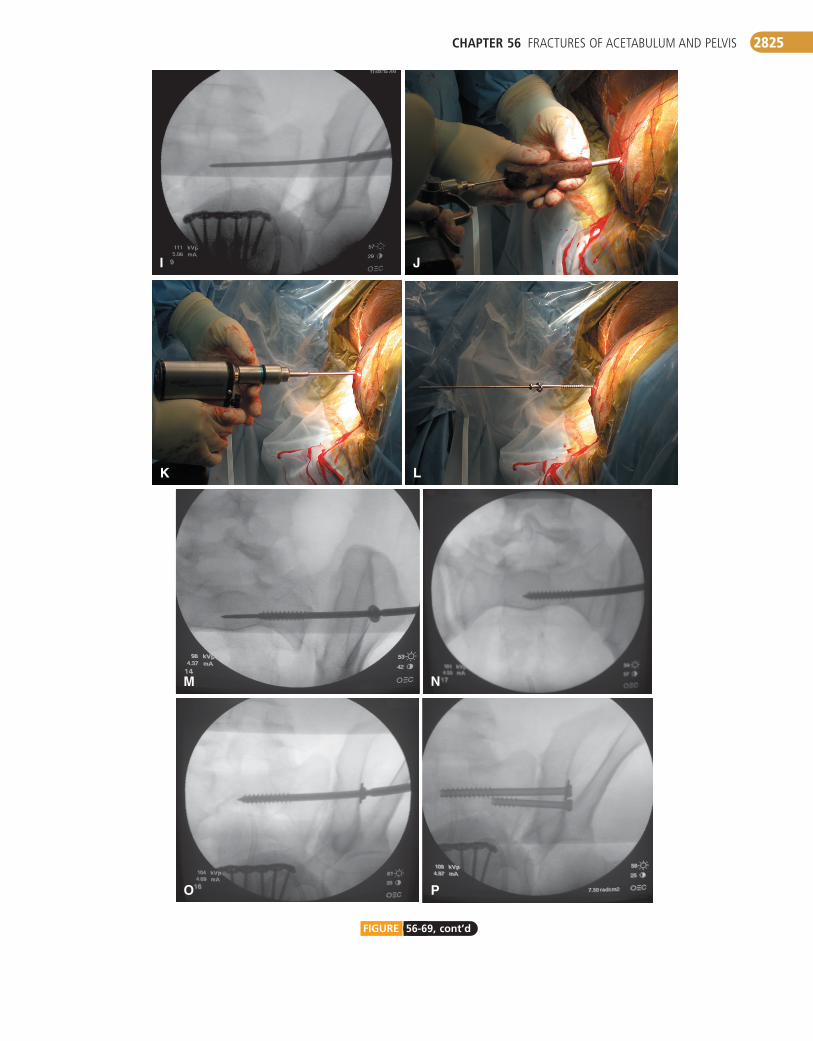
CHAPTER 56 FRACTURES OF ACETABULUM AND PELVIS 2825
PO
LK
NM
I J
FIGURE 56-69, cont’d
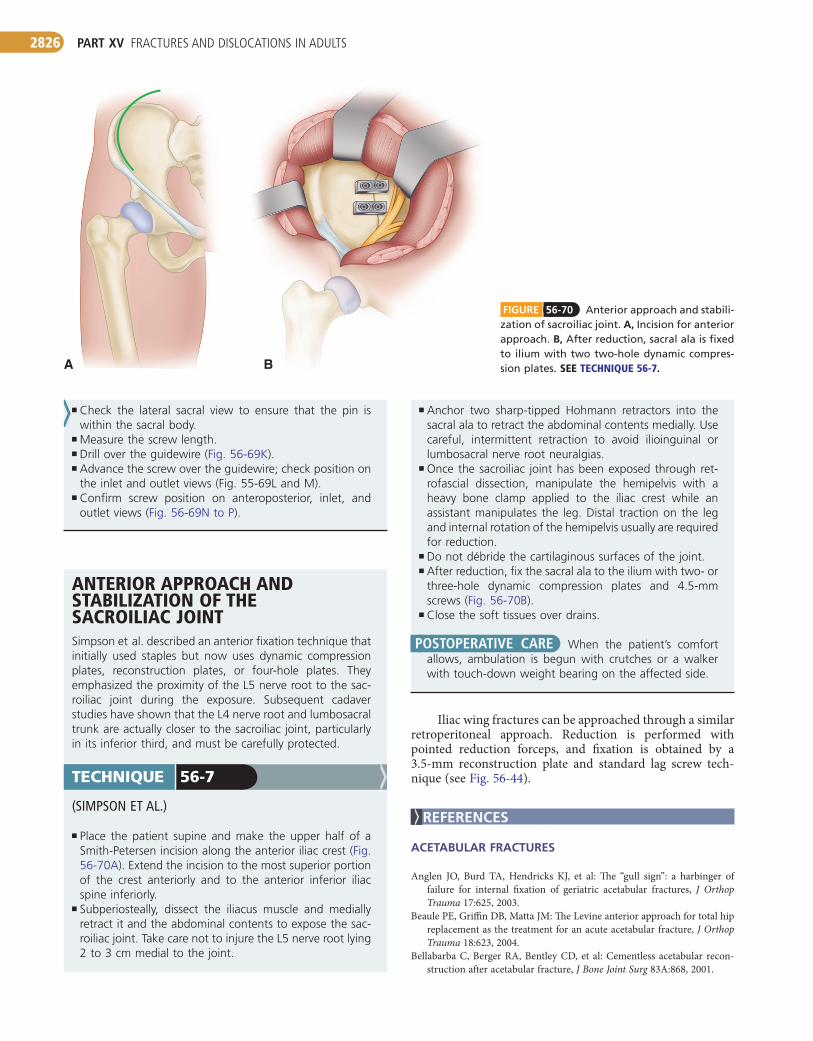
PART XV FRACTURES AND DISLOCATIONS IN ADULTS2826
FIGURE 56-70 Anterior approach and stabili-zation of sacroiliac joint. A, Incision for anterior approach. B, After reduction, sacral ala is fixed to ilium with two two-hole dynamic compres-sion plates. SEETECHNIQUE56-7.A B
■ Check the lateral sacral view to ensure that the pin is within the sacral body.
■ Measure the screw length.■ Drill over the guidewire (Fig. 56-69K).■ Advance the screw over the guidewire; check position on
the inlet and outlet views (Fig. 55-69L and M).■ Confirm screw position on anteroposterior, inlet, and
outlet views (Fig. 56-69N to P).
ANTERIORAPPROACHANDSTABILIZATIONOFTHESACROILIACJOINTSimpson et al. described an anterior fixation technique that initially used staples but now uses dynamic compression plates, reconstruction plates, or four-hole plates. They emphasized the proximity of the L5 nerve root to the sac-roiliac joint during the exposure. Subsequent cadaver studies have shown that the L4 nerve root and lumbosacral trunk are actually closer to the sacroiliac joint, particularly in its inferior third, and must be carefully protected.
(SIMPSON ET AL.)
■ Place the patient supine and make the upper half of a Smith-Petersen incision along the anterior iliac crest (Fig. 56-70A). Extend the incision to the most superior portion of the crest anteriorly and to the anterior inferior iliac spine inferiorly.
■ Subperiosteally, dissect the iliacus muscle and medially retract it and the abdominal contents to expose the sac-roiliac joint. Take care not to injure the L5 nerve root lying 2 to 3 cm medial to the joint.
TECHNIQUE 56-7
■ Anchor two sharp-tipped Hohmann retractors into the sacral ala to retract the abdominal contents medially. Use careful, intermittent retraction to avoid ilioinguinal or lumbosacral nerve root neuralgias.
■ Once the sacroiliac joint has been exposed through ret-rofascial dissection, manipulate the hemipelvis with a heavy bone clamp applied to the iliac crest while an assistant manipulates the leg. Distal traction on the leg and internal rotation of the hemipelvis usually are required for reduction.
■ Do not débride the cartilaginous surfaces of the joint.■ After reduction, fix the sacral ala to the ilium with two- or
three-hole dynamic compression plates and 4.5-mm screws (Fig. 56-70B).
■ Close the soft tissues over drains.
POSTOPERATIVE CARE When the patient’s comfort allows, ambulation is begun with crutches or a walker with touch-down weight bearing on the affected side.
Iliac wing fractures can be approached through a similar retroperitoneal approach. Reduction is performed with pointed reduction forceps, and fixation is obtained by a 3.5-mm reconstruction plate and standard lag screw tech-nique (see Fig. 56-44).
REFERENCES
ACETABULAR FRACTURES
Anglen JO, Burd TA, Hendricks KJ, et al: The “gull sign”: a harbinger of failure for internal fixation of geriatric acetabular fractures, J Orthop Trauma 17:625, 2003.
Beaule PE, Griffin DB, Matta JM: The Levine anterior approach for total hip replacement as the treatment for an acute acetabular fracture, J Orthop Trauma 18:623, 2004.
Bellabarba C, Berger RA, Bentley CD, et al: Cementless acetabular recon-struction after acetabular fracture, J Bone Joint Surg 83A:868, 2001.

CHAPTER 56 FRACTURES OF ACETABULUM AND PELVIS 2827
Morgan SJ, Jeray KJ, Phieffer LS, et al: Attitudes of orthopaedic trauma sur-geons regarding current controversies in the management of pelvic and acetabular fractures, J Orthop Trauma 15:526, 2001.
Naranje S, Shamshery P, Yadav CS, et al: Digastric trochanteric flip osteotomy and surgical dislocation of hip in the management of acetabular fractures, Arch Orthop Trauma Surg 130:93, 2010.
Pagenkopf E, Grose A, Partal G, Helfet DI: Acetabular fractures in the elderly: treatment recommendations, HSS J 2:161, 2006.
Pascarella R, Maresca A, Reggiani LM, Boriani S: Intraarticular fragments in acetabular fracture-dislocation, Orthopedics 32:402, 2009.
Porter SE, Russell CV, Dews RC, et al: Complications of acetabular fracture surgery in morbidly obese patients, J Orthop Trauma 22:589, 2008.
Qureshi AA, Archdeacon MT, Jenkins MA, et al: Infrapectineal plating for acetabular fractures: a technical adjunct to internal fixation, J Orthop Trauma 18:175, 2004.
Rath EM, Russell GV Jr, Washington WJ, Rourt MI Jr: Gluteus minimus necrotic muscle debridement diminishes heterotopic ossification after acetabular fracture fixation, Injury 33:751, 2002.
Rubel IF, Potter H, Barie P, et al: Magnetic resonance venography to evaluate deep venous thrombosis in patients with pelvic and acetabular trauma, J Trauma 51:622, 2001.
Siebenrock KA, Gautier E, Ziran BH, et al: Trochanteric flip osteotomy for cranial extension and muscle protection in acetabular fracture fixa-tion using a Kocher-Langenbeck approach, J Orthop Trauma 20:S52, 2006.
Slobogean GP, Lefaivre KA, Nicolaou S, O’Brien PJ: A systematic review of thromboprophylaxis for pelvic and acetabular fractures, J Orthop Trauma 23:379, 2009.
Solberg BD, Moon CN, Franco DP: Use of a trochanteric flip osteotomy improves outcomes in Pipkin IV fractures, Clin Orthop Relat Res 467:929, 2009.
Stannard JP, Riley RS, McClenney MD, et al: Mechanical prophylaxis against deep-vein thrombosis after pelvic and acetabular fractures, J Bone Joint Surg 83A:1047, 2001.
Starr AJ, Jones AL, Reinert CM, et al: Preliminary results and complications following limited open reduction and percutaneous screw fixation of displaced fractures of the acetabulum, Injury 32:SA45, 2001.
Starr AJ, Watson JT, Reinert CM, et al: Complications following the “T extensile” approach: a modified extensile approach for acetabular frac-ture surgery—report of forty-three patients, J Orthop Trauma 16:535, 2002.
Stover MD, Morgan SJ, Bosse MJ, et al: Prospective comparison of contrast-enhanced computed tomography versus magnetic resonance venography in the detection of occult deep pelvic vein thrombosis in patients with pelvic and acetabular fractures, J Orthop Trauma 16:613, 2002.
Tile M, Helfet DL, Kellam JF, editors: Fractures of the pelvis and acetabulum, ed 3, Philadelphia, 2003, Lippincott Williams & Wilkins.
Tseng S, Tornetta P 3rd: Percutaneous management of Morel-Lavallée lesions, J Bone Joint Surg 88A:92, 2006.
Vallier HA, Cureton BA, Ekstein C, et al: Early definitive stabilization of unstable pelvis and acetabulum fractures reduces morbidity, J Trauma 69:677, 2010.
Vanderschot P: Treatment options of pelvic and acetabular fractures in patients with osteoporotic bone, Injury 38:497, 2007.
Wolf H, Wieland T, Pajenda C, et al: Minimally invasive ilioinguinal approach to the acetabulum, Injury 35:2270, 2007.
PELVIC FRACTURES
Arrington ED, Hochschild DP, Steinagle TJ, et al: Monitoring of somatosen-sory and motor evoked potentials during open reduction and internal fixation of pelvis and acetabular fractures, Orthopedics 23:1081, 2000.
Atlihan D, Tekdemir I, Ates Y, et al: Anatomy of the anterior sacroiliac joint with reference to lumbosacral nerves, Clin Orthop Relat Res 376:236, 2000.
Bellabarba C, Ricci WM, Bolhofner BR: Distraction external fixation in lateral compression pelvic fractures, J Orthop Trauma 14:475, 2000.
Berry DJ, Halasy M: Uncemented acetabular components for arthritis after acetabular fracture, Clin Orthop Relat Res 405:164, 2002.
Boraiah S, Ragsdale M, Achor T, et al: Open reduction internal fixation and primary total hip arthroplasty of selected acetabular fractures, J Orthop Trauma 23:243, 2009.
Borrelli J Jr, Goldfarb C, Catalano L, et al: Assessment of articular frag-ment displacement in acetabular fractures: a comparison of computer-ized tomography and plain radiographs, J Orthop Trauma 16:449, 2002.
Borrelli J Jr, Goldfarb C, Ricci W, et al: Functional outcome after isolated acetabular fractures, J Orthop Trauma 16:73, 2002.
Borrelli J Jr, Ricci WM, Steger-May K, et al: Postoperative radiographic assessment of acetabular fractures: a comparison of plain radiographs and CT scans, J Orthop Trauma 19:299, 2005.
Burd TA, Lowry KJ, Anglen JO: Indomethacin compared with local-ized irradiation for prevention of heterotopic ossification following surgical treatment of acetabular fractures, J Bone Joint Surg 83A:1783, 2001.
Genuario J, Koval KJ, Cantu RV, Spratt KF: Does hospital surgical volume affect in-hospital outcomes in surgically treated pelvic and acetabular fractures? Bull NYU Hosp Jt Dis 66:282, 2008.
Giannoudis PV, Brotz MRW, Papkostidis C, Dinopoulos H: Operative treat-ment of displaced fractures of the acetabulum: a meta-analysis, J Bone Joint Surg 87B:2, 2005.
Giannoudis PV, Tzioupis C, Moed BR: Two-level reconstruction of commi-nuted posterior-wall fractures of the acetabulum, J Bone Joint Surg 89B:503, 2007.
Harris AM, Althausen P, Bellam JF, Bosse MJ: Simultaneous anterior and posterior approaches for complex acetabular fractures, J Orthop Trauma 22:494, 2008.
Karunakar MA, Shah SN, Jerabek S: Body mass index as a predictor of com-plications after operative treatment of acetabular fractures, J Bone Joint Surg 87A:1498, 2005.
Karunakar MA, Sen A, Bosse MJ, et al: Indomethacin as prophylaxis for heterotopic ossification after the operative treatment of fractures of the acetabulum, J Bone Joint Surg 88B:1613, 2006.
Laird A, Keating JF: Acetabular fractures: a 16-year prospective epidemio-logical study, J Bone Joint Surg 87B:969, 2005.
Lefaivre KA, Starr AJ, Reinert CM: Reduction of displaced pelvic ring disruptions using a pelvic reduction frame, J Orthop Trauma 23:299, 2009.
Luitse JS: Internal fracture fixation using the Stoppa approach in pelvic ring and acetabular fractures: technical aspects and operative results, J Trauma 61:662, 2006.
Madhu R, Kotnis R, Al-Mousawi A, et al: Outcome of surgery for reconstruc-tion of fractures of the acetabulum: the time dependent effect of delay, J Bone Joint Surg 88B:1197, 2006.
Matta JM: Operative treatment of acetabular fractures through the ilio-inguinal approach: a 10-year perspective, J Orthop Trauma 210:S20, 2006.
Matta JM, Ferguson TA: Total hip replacement after acetabular fracture, Orthopedics 28:959, 2005.
Mears DC, Velyvis JH: Primary total hip arthroplasty after acetabular frac-ture, Instr Course Lect 50:335, 2001.
Mears DC, Velyvis JH: Acute total hip arthroplasty for selected displaced acetabular fractures: two to twelve-year results, J Bone Joint Surg 84A:1, 2002.
Mears DC, Velyvis JH, Chang CP: Displaced acetabular fractures managed operatively: indicators of outcome, Clin Orthop Relat Res 407:173, 2003.
Moed BR, Ajibade DA, Israel H: Computed tomography as a predictor of hip stability status in posterior wall fractures of the acetabulum, J Orthop Trauma 23:7, 2009.
Moed BR, Carr SE, Gruson KI, et al: Computed tomographic assessment of fractures of the posterior wall of the acetabulum after operative treat-ment, J Bone Joint Surg 85A:512, 2003.
Moed BR, Yu PH, Gruson KI: Functional outcomes of acetabular fractures, J Bone Joint Surg 85A:1879, 2003.
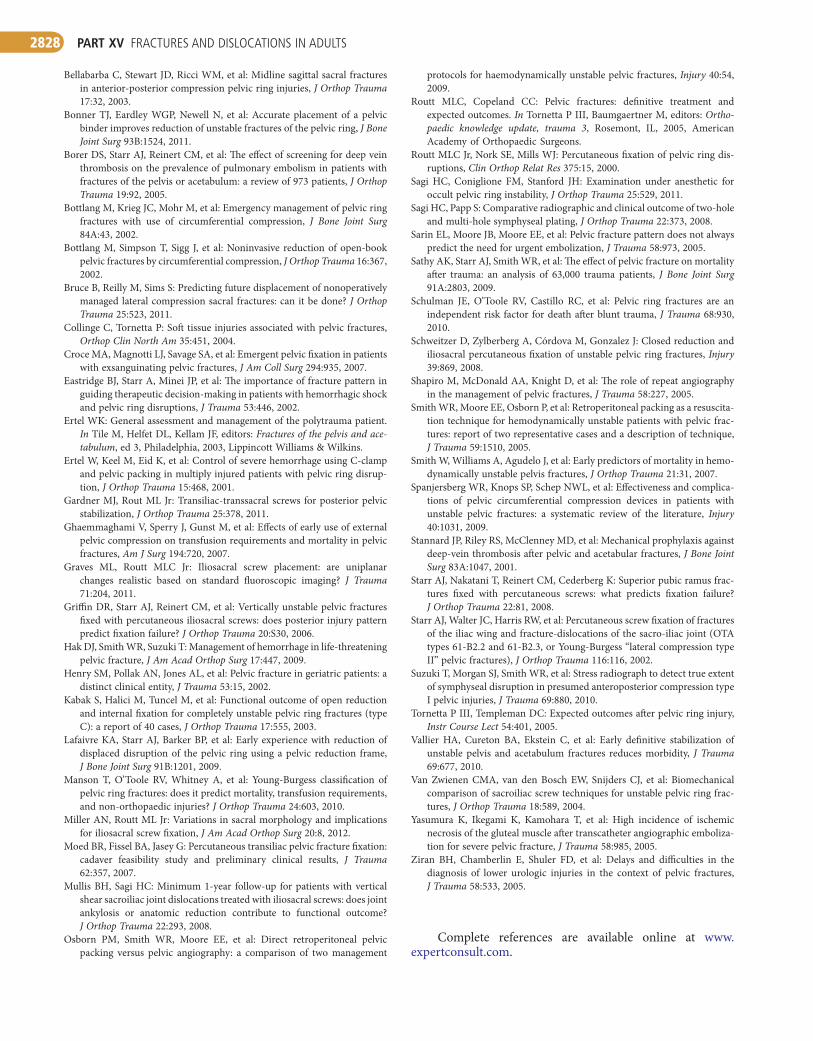
PART XV FRACTURES AND DISLOCATIONS IN ADULTS2828
protocols for haemodynamically unstable pelvic fractures, Injury 40:54, 2009.
Routt MLC, Copeland CC: Pelvic fractures: definitive treatment and expected outcomes. In Tornetta P III, Baumgaertner M, editors: Ortho-paedic knowledge update, trauma 3, Rosemont, IL, 2005, American Academy of Orthopaedic Surgeons.
Routt MLC Jr, Nork SE, Mills WJ: Percutaneous fixation of pelvic ring dis-ruptions, Clin Orthop Relat Res 375:15, 2000.
Sagi HC, Coniglione FM, Stanford JH: Examination under anesthetic for occult pelvic ring instability, J Orthop Trauma 25:529, 2011.
Sagi HC, Papp S: Comparative radiographic and clinical outcome of two-hole and multi-hole symphyseal plating, J Orthop Trauma 22:373, 2008.
Sarin EL, Moore JB, Moore EE, et al: Pelvic fracture pattern does not always predict the need for urgent embolization, J Trauma 58:973, 2005.
Sathy AK, Starr AJ, Smith WR, et al: The effect of pelvic fracture on mortality after trauma: an analysis of 63,000 trauma patients, J Bone Joint Surg 91A:2803, 2009.
Schulman JE, O’Toole RV, Castillo RC, et al: Pelvic ring fractures are an independent risk factor for death after blunt trauma, J Trauma 68:930, 2010.
Schweitzer D, Zylberberg A, Córdova M, Gonzalez J: Closed reduction and iliosacral percutaneous fixation of unstable pelvic ring fractures, Injury 39:869, 2008.
Shapiro M, McDonald AA, Knight D, et al: The role of repeat angiography in the management of pelvic fractures, J Trauma 58:227, 2005.
Smith WR, Moore EE, Osborn P, et al: Retroperitoneal packing as a resuscita-tion technique for hemodynamically unstable patients with pelvic frac-tures: report of two representative cases and a description of technique, J Trauma 59:1510, 2005.
Smith W, Williams A, Agudelo J, et al: Early predictors of mortality in hemo-dynamically unstable pelvis fractures, J Orthop Trauma 21:31, 2007.
Spanjersberg WR, Knops SP, Schep NWL, et al: Effectiveness and complica-tions of pelvic circumferential compression devices in patients with unstable pelvic fractures: a systematic review of the literature, Injury 40:1031, 2009.
Stannard JP, Riley RS, McClenney MD, et al: Mechanical prophylaxis against deep-vein thrombosis after pelvic and acetabular fractures, J Bone Joint Surg 83A:1047, 2001.
Starr AJ, Nakatani T, Reinert CM, Cederberg K: Superior pubic ramus frac-tures fixed with percutaneous screws: what predicts fixation failure? J Orthop Trauma 22:81, 2008.
Starr AJ, Walter JC, Harris RW, et al: Percutaneous screw fixation of fractures of the iliac wing and fracture-dislocations of the sacro-iliac joint (OTA types 61-B2.2 and 61-B2.3, or Young-Burgess “lateral compression type II” pelvic fractures), J Orthop Trauma 116:116, 2002.
Suzuki T, Morgan SJ, Smith WR, et al: Stress radiograph to detect true extent of symphyseal disruption in presumed anteroposterior compression type I pelvic injuries, J Trauma 69:880, 2010.
Tornetta P III, Templeman DC: Expected outcomes after pelvic ring injury, Instr Course Lect 54:401, 2005.
Vallier HA, Cureton BA, Ekstein C, et al: Early definitive stabilization of unstable pelvis and acetabulum fractures reduces morbidity, J Trauma 69:677, 2010.
Van Zwienen CMA, van den Bosch EW, Snijders CJ, et al: Biomechanical comparison of sacroiliac screw techniques for unstable pelvic ring frac-tures, J Orthop Trauma 18:589, 2004.
Yasumura K, Ikegami K, Kamohara T, et al: High incidence of ischemic necrosis of the gluteal muscle after transcatheter angiographic emboliza-tion for severe pelvic fracture, J Trauma 58:985, 2005.
Ziran BH, Chamberlin E, Shuler FD, et al: Delays and difficulties in the diagnosis of lower urologic injuries in the context of pelvic fractures, J Trauma 58:533, 2005.
Complete references are available online at www.expertconsult.com.
Bellabarba C, Stewart JD, Ricci WM, et al: Midline sagittal sacral fractures in anterior-posterior compression pelvic ring injuries, J Orthop Trauma 17:32, 2003.
Bonner TJ, Eardley WGP, Newell N, et al: Accurate placement of a pelvic binder improves reduction of unstable fractures of the pelvic ring, J Bone Joint Surg 93B:1524, 2011.
Borer DS, Starr AJ, Reinert CM, et al: The effect of screening for deep vein thrombosis on the prevalence of pulmonary embolism in patients with fractures of the pelvis or acetabulum: a review of 973 patients, J Orthop Trauma 19:92, 2005.
Bottlang M, Krieg JC, Mohr M, et al: Emergency management of pelvic ring fractures with use of circumferential compression, J Bone Joint Surg 84A:43, 2002.
Bottlang M, Simpson T, Sigg J, et al: Noninvasive reduction of open-book pelvic fractures by circumferential compression, J Orthop Trauma 16:367, 2002.
Bruce B, Reilly M, Sims S: Predicting future displacement of nonoperatively managed lateral compression sacral fractures: can it be done? J Orthop Trauma 25:523, 2011.
Collinge C, Tornetta P: Soft tissue injuries associated with pelvic fractures, Orthop Clin North Am 35:451, 2004.
Croce MA, Magnotti LJ, Savage SA, et al: Emergent pelvic fixation in patients with exsanguinating pelvic fractures, J Am Coll Surg 294:935, 2007.
Eastridge BJ, Starr A, Minei JP, et al: The importance of fracture pattern in guiding therapeutic decision-making in patients with hemorrhagic shock and pelvic ring disruptions, J Trauma 53:446, 2002.
Ertel WK: General assessment and management of the polytrauma patient. In Tile M, Helfet DL, Kellam JF, editors: Fractures of the pelvis and ace-tabulum, ed 3, Philadelphia, 2003, Lippincott Williams & Wilkins.
Ertel W, Keel M, Eid K, et al: Control of severe hemorrhage using C-clamp and pelvic packing in multiply injured patients with pelvic ring disrup-tion, J Orthop Trauma 15:468, 2001.
Gardner MJ, Rout ML Jr: Transiliac-transsacral screws for posterior pelvic stabilization, J Orthop Trauma 25:378, 2011.
Ghaemmaghami V, Sperry J, Gunst M, et al: Effects of early use of external pelvic compression on transfusion requirements and mortality in pelvic fractures, Am J Surg 194:720, 2007.
Graves ML, Routt MLC Jr: Iliosacral screw placement: are uniplanar changes realistic based on standard fluoroscopic imaging? J Trauma 71:204, 2011.
Griffin DR, Starr AJ, Reinert CM, et al: Vertically unstable pelvic fractures fixed with percutaneous iliosacral screws: does posterior injury pattern predict fixation failure? J Orthop Trauma 20:S30, 2006.
Hak DJ, Smith WR, Suzuki T: Management of hemorrhage in life-threatening pelvic fracture, J Am Acad Orthop Surg 17:447, 2009.
Henry SM, Pollak AN, Jones AL, et al: Pelvic fracture in geriatric patients: a distinct clinical entity, J Trauma 53:15, 2002.
Kabak S, Halici M, Tuncel M, et al: Functional outcome of open reduction and internal fixation for completely unstable pelvic ring fractures (type C): a report of 40 cases, J Orthop Trauma 17:555, 2003.
Lafaivre KA, Starr AJ, Barker BP, et al: Early experience with reduction of displaced disruption of the pelvic ring using a pelvic reduction frame, J Bone Joint Surg 91B:1201, 2009.
Manson T, O’Toole RV, Whitney A, et al: Young-Burgess classification of pelvic ring fractures: does it predict mortality, transfusion requirements, and non-orthopaedic injuries? J Orthop Trauma 24:603, 2010.
Miller AN, Routt ML Jr: Variations in sacral morphology and implications for iliosacral screw fixation, J Am Acad Orthop Surg 20:8, 2012.
Moed BR, Fissel BA, Jasey G: Percutaneous transiliac pelvic fracture fixation: cadaver feasibility study and preliminary clinical results, J Trauma 62:357, 2007.
Mullis BH, Sagi HC: Minimum 1-year follow-up for patients with vertical shear sacroiliac joint dislocations treated with iliosacral screws: does joint ankylosis or anatomic reduction contribute to functional outcome? J Orthop Trauma 22:293, 2008.
Osborn PM, Smith WR, Moore EE, et al: Direct retroperitoneal pelvic packing versus pelvic angiography: a comparison of two management

CHAPTER 56 FRACTURES OF ACETABULUM AND PELVIS 2828.e1
SUPPLEMENTAL REFERENCES
ACETABULAR FRACTURES
Baumgaertner MR, Wenger D, Booke J: SSEP monitoring during pelvic and acetabular fracture surgery, J Orthop Trauma 8:127, 1994.
Bosse MJ: Posterior acetabular wall fractures: a technique for screw place-ment, J Orthop Trauma 5:167, 1991.
Bosse MJ, Poka A, Reinert CM, et al: Heterotopic ossification as a complica-tion of acetabular fracture: prophylaxis with low-dose irradiation, J Bone Joint Surg 70A:1231, 1988.
Bosse MJ, Poka A, Reinert CM, et al: Preoperative angiographic assessment of the superior gluteal artery in acetabular fractures requiring extensile surgical exposures, J Orthop Trauma 2:303, 1989.
Bray TJ, Esser M, Fulkerson L: Osteotomy of the trochanter in open reduc-tion and internal fixation of acetabular fractures, J Bone Joint Surg 69A:711, 1987.
Brooker AF, Bowerman JW, Robinson RA, et al: Ectopic ossification follow-ing total hip replacement: incidence and a method of classification, J Bone Joint Surg 55A:1629, 1973.
Calder HB, Mast J, Johnstone C: Intraoperative evoked potential monitoring in acetabular surgery, Clin Orthop Relat Res 305:160, 1994.
Calkins MS, Zynch G, Latta L, et al: Computed tomography evaluation of stability in posterior fracture dislocation of the hip, Clin Orthop Relat Res 230:152, 1988.
Cole JD, Bolhofner BR: Acetabular fracture fixation via a modified Stoppa limited intrapelvic approach: description of operative technique and pre-liminary treatment results, Clin Orthop Relat Res 305:112, 1994.
Collins DN, Barnes CL, McCowan TC, et al: Vena caval filter use in ortho-paedic trauma patients with recognized preoperative venous thrombo-embolic disease, J Orthop Trauma 6:135, 1992.
Fassler PR, Swiontkowski MF, Kilroy AW, et al: Injury of the sciatic nerve associated with acetabular fracture, J Bone Joint Surg 75A:1157, 1993.
Geerts WH, Code KI, Jay RM, et al: A prospective study of venous throm-boembolism after major trauma, N Engl J Med 331:1601, 1994.
Ghalambor N, Matta JM, Bernstein L: Heterotopic ossification following operative treatment of acetabular fractures: an analysis of risk factors, Clin Orthop Relat Res 305:96, 1994.
Gorczyca JT, Powell JN, Tile M: Lateral extension of the ilioinguinal incision in the operative treatment of acetabulum fractures, Injury 26:207, 1995.
Goulet JA, Bray TJ: Complex acetabular fractures, Clin Orthop Relat Res 240:9, 1989.
Goulet JA, Rouleau JP, Mason DJ, et al: Comminuted fractures of the poste-rior wall of the acetabulum: a biomechanical evaluation of fixation methods, J Bone Joint Surg 76A:1457, 1994.
Guy RL, Butler-Manuel PA, Holder P, et al: The role of 3D CT in the assess-ment of acetabular fractures, Br J Radiol 65:384, 1992.
Hak DJ, Olson SA, Matta JM: Diagnosis and management of closed internal degloving injuries associated with pelvic and acetabular fractures: the Morel-Lavallée lesions, J Trauma 42:1046, 1997.
Heeg M, Oostvogel HJ, Klasen HJ: Conservative treatment of acetabular fractures: the role of the weight-bearing dome and anatomic reduction in the ultimate results, J Trauma 27:555, 1987.
Helfet DL, Anand N, Malkani ALL, et al: Intraoperative monitoring of motor pathways during operative fixation of acute acetabular fractures, J Orthop Trauma 11:2, 1997.
Helfet DL, Borrelli J Jr, DiPasquale T, et al: Stabilization of acetabular frac-tures in elderly patients, J Bone Joint Surg 74A:753, 1992.
Helfet DL, Hissa EA, Sergay S, et al: Somatosensory evoked potential moni-toring in the surgical management of acute acetabular fractures, J Orthop Trauma 5:161, 1991.
Helfet DL, Schmeling GJ: Management of complex acetabular fractures through single nonextensile exposures, Clin Orthop Relat Res 305:58, 1994.
Helfet DL, Schmeling GJ: Somatosensory-evoked potential monitoring in the surgical treatment of acute, displaced acetabular fractures: results of a prospective study, Clin Orthop Relat Res 301:213, 1994.
Jimenez M, Tile M, Schenk RS: Total hip replacement after acetabular frac-ture, Orthop Clin North Am 28:435, 1997.
Johnson EE, Kay RM, Dorey FJ: Heterotopic ossification prophylaxis follow-ing operative treatment of acetabular fracture, Clin Orthop Relat Res 305:88, 1994.
Johnson EE, Matta JM, Mast JW, et al: Delayed reconstruction of acetabular fractures 21 to 120 days following injury, Clin Orthop Relat Res 305:20, 1994.
Judet R, Judet J, Letournel E: Fractures of the acetabulum: classification and surgical approaches for open reduction: preliminary report, J Bone Joint Surg 46A:1615, 1964.
Juliano PJ, Bosse MJ, Edwards KJ: The superior gluteal artery in complex acetabular procedures: a cadaver angiographic study, J Bone Joint Surg 76A:244, 1994.
Kebaish AS, Roy A, Rennie W: Displaced acetabular fractures: long-term follow-up, J Trauma 31:1539, 1991.
Keith JE Jr, Brashear R Jr, Guilford WB: Stability of posterior fracture-dislocations of the hip: quantitative assessment using computed tomog-raphy, J Bone Joint Surg 70A:711, 1988.
Kellam JF, Messer A: Evaluation of the role of coronal and sagittal axial CT scan reconstructions for the imaging of acetabular fractures, Clin Orthop Relat Res 305:152, 1994.
Letournel E: Acetabulum fractures: classification and management, Clin Orthop Relat Res 151:81, 1980.
Letournel E: The treatment of acetabular fractures through the ilioinguinal approach, Clin Orthop Relat Res 292:62, 1993.
Letournel E, Judet R, eds: Fractures of the acetabulum, ed 2, Berlin, 1993, Springer-Verlag.
Martinez CD, DiPasquale TG, Helfet DL, et al: Evaluation of acetabular fractures with two- and three-dimensional CT, RadioGraphics 12:227, 1992.
Matta JM: Operative indications and choice of surgical approach for fractures of the acetabulum, Tech Orthop 1:13, 1986.
Matta JM: Fractures of the acetabulum: accuracy of reduction and clinical results in patients managed operatively within three weeks after the injury, J Bone Joint Surg 78A:1632, 1996.
Matta JM, Anderson LM, Epstein HC, et al: Fractures of the acetabulum: a retrospective analysis, Clin Orthop Relat Res 205:230, 1986.
Matta JM, Merritt PO: Displaced acetabular fractures, Clin Orthop Relat Res 230:83, 1988.
Matta JM, Siebenrock KA: Does indomethacin reduce heterotopic bone for-mation after operations for acetabular fractures? J Bone Joint Surg 79B:959, 1997.
Mayo KA: Open reduction and internal fixation of fractures of the acetabu-lum: results in 163 fractures, Clin Orthop Relat Res 301:31, 1994.
Mayo KA, Letournel E, Matta JM, et al: Surgical revision of malreduced acetabular fractures, Clin Orthop Relat Res 305:47, 1994.
McLaren AC: Prophylaxis with indomethacin for heterotopic bone after open reduction of fractures of the acetabulum, J Bone Joint Surg 72A:245, 1990.
Mears DC: Surgical treatment of acetabular fractures in elderly patients with osteoporotic bone, J Am Acad Orthop Surg 7:128, 1999.
Mears DC, Rubash HE, Sawaguchi T: Fractures of the acetabulum, Hip 95, 1985.
Moed BR, Karges DE: Prophylactic indomethacin for the prevention of heterotopic ossification after acetabular fracture surgery in high-risk patients, J Orthop Trauma 8:34, 1994.
Moed BR, Letournel E: Low-dose irradiation and indomethacin prevent heterotopic ossification after acetabular fracture surgery, J Bone Joint Surg 76B:895, 1994.
Moed BR, Maxey JW: The effect of indomethacin on heterotopic ossification following acetabular fracture surgery, J Orthop Trauma 7:33, 1993.
Moed BR, Maxey JW, Minster GJ: Intraoperative somatosensory evoked potential monitoring of the sciatic nerve: an animal model, J Orthop Trauma 6:59, 1992.
Montgomery KD, Potter HG, Helfet DL: Magnetic resonance venography to evaluate the deep venous system of the pelvis in patients who have an acetabular fracture, J Bone Joint Surg 77A:1639, 1995.
PART VII GENERAL PRINCIPLES OF INFECTION2828.e2
Montgomery KD, Potter HG, Helfet DL: The detection and management of proximal deep venous thrombosis in patients with acute acetabular frac-tures: a follow-up report, J Orthop Trauma 11:330, 1997.
Moore KD, Goss K, Anglen JO: Indomethacin versus radiation therapy for prophylaxis against heterotopic ossification in acetabular fractures, J Bone Joint Surg 80B:259, 1998.
Moroni A, Caja VL, Sabato C, et al: Surgical treatment of both-column fractures by staged combined ilioinguinal and Kocher-Langenbeck approaches, Injury 26:219, 1995.
Olson SA, Matta JM: The computerized tomography subchondral arc: a new method of assessing acetabular articular congruity after fracture (a pre-liminary report), J Orthop Trauma 7:402, 1993.
Olson SA, Matta JM: Surgical treatment of acetabulum fractures. In Browner BD, Jupiter JB, Levine AM, Trafton PG, editors: Skeletal trauma: fractures, dislocations, ligamentous injuries, ed 2, Philadelphia, 1998, WB Saunders.
Parker PJ, Copeland C: Percutaneous fluoroscopic screw fixation of acetabu-lar fractures, Injury 28:597, 1997.
Pennal GF, Davidson J, Garside H, et al: Results of treatment of acetabular fractures, Clin Orthop Relat Res 151:115, 1980.
Reinert CM, Bosse MJ, Poka A, et al: A modified extensile exposure for the treatment of complex or malunited acetabular fractures, J Bone Joint Surg 70A:329, 1988.
Romness DW, Lewallen DG: Total hip arthroplasty after fracture of the acetabulum: long-term results, J Bone Joint Surg 72B:761, 1990.
Routt MLC Jr, Swiontkowski MF: Operative treatment of complex acetabular fractures: combined anterior and posterior exposures during the same procedure, J Bone Joint Surg 72A:897, 1990.
Rowe CR, Lowell JD: Prognosis of fractures of the acetabulum, J Bone Joint Surg 43A:30, 1961.
Ruesch PD, Holdener H, Ciaramitaro M, et al: A prospective study of surgi-cally treated acetabular fractures, Clin Orthop Relat Res 305:38, 1994.
Schmidt CC, Gruen GJ: Non-extensile surgical approaches for two-column acctabular fractures, J Bone Joint Surg 75B:556, 1993.
Schopfer A, Willett K, Powell J, et al: Cerclage wiring in internal fixation of acetabular fractures, J Orthop Trauma 7:236, 1993.
Slawson RG, Poka A, Bathon H, et al: The role of postoperative radiation in the prevention of heterotopic ossification in patients with post-traumatic acetabular fracture, Int J Radiat Oncol Biol Phys 17:669, 1989.
Stannard JP, Alonso JE: Controversies in acetabular fractures, Clin Orthop Relat Res 353:74, 1998.
Tabor OB, Bosse MJ, Greene KG, et al: Effects of surgical approaches for acetabular fractures with associated gluteal vascular injury, J Orthop Trauma 12:78, 1998.
Templeman DC, Olson S, Moed BR, et al: Surgical treatment of acetabular fractures, Instr Course Lect 48:481, 1999.
Tornetta P III: Nonoperative management of acetabular fractures: the use of dynamic stress views, J Bone Joint Surg 81B:67, 1999.
Tornetta P III, Hochwald N, Levine R: Corona mortis, Clin Orthop Relat Res 329:97, 1996.
Vailas JC, Hurwitz S, Wiesel SW: Posterior acetabular fracture-dislocations: fragment size, joint capsule, and stability, J Trauma 29:1494, 1989.
Vrahas M, Gordon RG, Mears DC, et al: Intraoperative somatosensory evoked potential monitoring of pelvic and acetabular fractures, J Orthop Trauma 6:50, 1992.
Vrahas MS, Widding KK, Thomas KA: The effects of simulated transverse, anterior column, and posterior column fractures of the acetabulum on the stability of the hip joint, J Bone Joint Surg 81A:966, 1999.
Webb LX, Rush PT, Fuller SB, et al: Greenfield filter prophylaxis of pulmo-nary embolism in patients undergoing surgery for acetabular fracture, J Orthop Trauma 6:139, 1992.
Weber TG, Mast JW: The extended ilioinguinal approach for specific both column fractures, Clin Orthop Relat Res 305:106, 1994.
Winquist RA: Open reduction and internal fixation of central acetabular fractures by anterior and posterior approach, Orthop Trans 6:93, 1982.
Wright R, Barrett K, Christie MJ, et al: Acetabular fractures: long-term follow-up of open reduction and internal fixation, J Orthop Trauma 8:397, 1994.
PELVIC FRACTURES
Agnew SG: Hemodynamically unstable pelvic fractures, Orthop Clin North Am 25:715, 1994.
Agolini SF, Shah K, Jaffe J, et al: Arterial embolization is a rapid and effective technique for controlling pelvic fracture hemorrhage, J Trauma 43:395, 1997.
Altman DT, Jones CB, Routt MLC Jr: Superior gluteal artery injury during iliosacral screw placement, J Orthop Trauma 13:220, 1999.
Bartlett C, Asprinio D, Louis S, et al: Intrapelvic dislocation of the left hemi-pelvis as a complication of the pelvic “C” clamp: a case report and review, J Orthop Trauma 11:540, 1997.
Bassam D, Cephas GA, Ferguson KA, et al: A protocol for the initial manage-ment of unstable pelvic fractures, Am Surg 64:862, 1998.
Baumgartner F, White GH, White RA, et al: Controversies in the manage-ment of retroperitoneal hemorrhage associated with pelvic fractures, J Natl Med Assoc 87:33, 1995.
Ben-Menachem Y, Coldwell DM, Young JWR, et al: Hemorrhage-associated pelvic fractures: causes, diagnosis, and emergent management, AJR Am J Roentgenol 157:1005, 1991.
Borrelli J, Koval KJ, Helfet DL: Operative stabilization of fracture dislocations of the sacroiliac joint, Clin Orthop Relat Res 329:141, 1996.
Brenneman FD, Katyal D, Boulanger BR, et al: Long-term outcomes in open pelvic fractures, J Trauma 42:773, 1997.
Browner BD, Cole JD, Graham JM, et al: Delayed posterior internal fixation of unstable pelvic fractures, J Trauma 27:998, 1987.
Bucholz RW: The pathological anatomy of Malgaigne fracture-dislocations of the pelvis, J Bone Joint Surg 63A:400, 1981.
Bucholz RW: Pathomechanics of pelvic ring disruptions, Adv Orthop Surg 10:167, 1987.
Bucholz RW, Peters P: Assessment of pelvic stability, Instr Course Lect 37:119, 1988.
Buckle R, Browner BD, Morandi M: Emergency reduction for pelvic ring disruptions and control of associated hemorrhage using the pelvic stabi-lizer, Tech Orthop 9:258, 1994.
Buckley SL, Burkus JK: Computerized axial tomography of pelvic ring frac-tures, J Trauma 27:496, 1987.
Buerger PM, Peoples JB, Lemmon GW, et al: Risk of pulmonary embolism in patients with pelvic fractures, Am Surg 59:505, 1993.
Burgess AR, Eastridge BJ, Young JW, et al: Pelvic ring disruptions: effective classification system and treatment protocols, J Trauma 30:848, 1990.
Carrillo EH, Wohltmann CD, Spain DA, et al: Common and external iliac artery injuries associated with pelvic fractures, J Orthop Trauma 13:351, 1999.
Cass AS, Behrens F, Comfort T, et al: Bladder problems in pelvic injuries with external fixator and direct urethral drainage, J Trauma 23:50, 1983.
Cecil ML, Rollins JR, Ebraheim NA, et al: Projection of the S2 pedicle onto the posterolateral surface of the ilium: a technique for lag screw fixation of sacral fractures or sacroiliac joint dislocations, Spine 21:875, 1996.
Cole JD, Blum DA, Ansel LJ: Outcome after fixation of unstable posterior pelvic ring injuries, Clin Orthop Relat Res 329:160, 1996.
Comstock CP, van der Meulen MCH, Goodman SB: Biomechanical compari-son of posterior internal fixation techniques for unstable pelvic fractures, J Orthop Trauma 10:517, 1996.
Copeland CE, Bosse MJ, McCarthy ML, et al: Effect of trauma and pelvic fracture on female genitourinary, sexual, and reproductive function, J Orthop Trauma 11:73, 1997.
Cotler HB, LaMont JG, Hansen ST Jr: Immediate spica casting for pelvic fractures, J Orthop Trauma 2:222, 1988.
Cryer HM, Miller FB, Evers M, et al: Pelvic fracture classification: correlation with hemorrhage, J Trauma 28:973, 1988.
Dahners LE, Jacobs RR, Jayraman G, et al: A study of external fixation systems for unstable pelvic fractures, J Trauma 24:876, 1984.
Dalal SA, Burgess AR, Siegel JH, et al: Pelvic fracture in multiple trauma: classification by mechanism is key to pattern of organ injury, resuscitative requirements, and outcome, J Trauma 29:981, 1989.
CHAPTER 56 FRACTURES OF ACETABULUM AND PELVIS 2828.e3
Davidson BS, Simmons GT, Williamson PR, et al: Pelvic fractures associ-ated with open perineal wounds: a survivable injury, J Trauma 35:36, 1993.
Denis F, Davis S, Comfort T: Sacral fractures: an important problem—retrospective analysis of 236 cases, Clin Orthop Relat Res 227:67, 1988.
DePaolo CJ, Russell TA, Armistead C, et al: Unstable vertical shear fractures of the pelvis: functional results after open reduction and internal fixation, Orthop Trans 16:190, 1992.
Draijer F, Egbers H-J, Haveman D: Quality of life after pelvic ring injuries: follow-up results of a prospective study, Arch Orthop Trauma Surg 116:22, 1997.
Dujardin FH, Hossenbaccus M, Duparc F, et al: Long-term functional prog-nosis of posterior injuries in high-energy pelvic disruption, J Orthop Trauma 12:145, 1998.
Duwelius PJ, Van Allen M, Bray TJ, et al: Computed tomography–guided fixation of unstable posterior pelvic ring disruptions, J Orthop Trauma 6:420, 1992.
Eastridge BJ, Burgess AR: Pedestrian pelvic fractures: 5-year experience of a major urban trauma center, J Trauma 42:695, 1997.
Ebraheim NA, Rusin JJ, Coombs RJ, et al: Percutaneous computed tomogra-phy stabilization of pelvic fractures: preliminary report, J Orthop Trauma 1:197, 1987.
Ebraheim NA, Xu R, Biyani A, et al: Morphologic considerations of the first sacral pedicle for iliosacral screw placement, Spine 22:841, 1997.
Edeiken-Monroe BS, Browner BD, Jackson H: The role of standard radio-graphs in the evaluation of instability of pelvic ring disruption, Clin Orthop Relat Res 240:63, 1989.
Eers BM, Cryer HM, Miller FB: Pelvic fracture hemorrhage: priorities in management, Arch Surg 124:422, 1989.
Failinger MS, McGanity PL: Unstable fractures of the pelvic ring, J Bone Joint Surg 74A:781, 1992.
Fallat ME, Weaver JM, Hertweck SP, et al: Late follow-up and functional outcome after traumatic reproductive tract injuries in women, Am Surg 64:858, 1998.
Faringer PD, Mullins RJ, Feliciano PD, et al: Selective fecal diversion in complex open pelvic fractures from blunt trauma, Arch Surg 129:958, 1994.
Ferrera PC, Hill DA: Good outcomes of open pelvic fractures, Injury 30:187, 1999.
Fishmann AJ, Greeno RA, Brooks LR, et al: Prevention of deep vein throm-bosis and pulmonary embolism in acetabular and pelvic fracture surgery, Clin Orthop Relat Res 305:133, 1994.
Ganz R, Krushell RJ, Jakob RP, et al: The antishock pelvic clamp, Clin Orthop Relat Res 267:71, 1991.
Ghanayem AJ, Stover MD, Goldstein JA, et al: Emergent treatment of pelvic fractures: comparison of methods for stabilization, Clin Orthop Relat Res 318:75, 1995.
Ghanayem AJ, Wiber JH, Lieberman JM, et al: The effect of laparotomy and external fixator stabilization on pelvic volume in an unstable pelvic injury, J Trauma 83:396, 1995.
Gill K, Bucholz RW: The role of computerized tomographic scanning in the evaluation of major pelvic fractures, J Bone Joint Surg 66A:34, 1984.
Gilliland MD, Ward RE, Barton RM, et al: Factors affecting mortality in pelvic fractures, J Trauma 22:691, 1982.
Goldstein A, Phillips T, Sclafani JA, et al: Early open reduction and internal fixation of the disrupted pelvic ring, J Trauma 26:325, 1986.
Gorczyca JT, Varga E, Woodside T, et al: The strength of iliosacral lag screws and transiliac bars in the fixation of vertically unstable pelvic injuries with sacral fractures, Injury 27:561, 1996.
Gruen GS, Leit ME, Gruen RJ, et al: The acute management of hemodynami-cally unstable multiple trauma patients with pelvic ring fractures, J Trauma 36:706, 1994.
Gruen GS, Leit ME, Gruen RJ, et al: Functional outcome of patients with unstable pelvic ring fractures stabilized with open reduction and internal fixation, J Trauma 39:838, 1995.
Hanson PB, Milne JC, Chapman MW: Open fractures of the pelvis: review of 43 cases, J Bone Joint Surg 73B:325, 1991.
Heini PF, Witt J, Ganz R: The pelvic C-clamp for the emergency treatment of unstable pelvic ring injuries: a report on clinical experience of 30 cases, Injury 27:SA38, 1996.
Henderson RC: The long-term results of nonoperatively treated major pelvic disruptions, J Orthop Trauma 3:41, 1989.
Hirvensale E, Lindahl J, Böstman O: A new approach to the internal fixation of unstable pelvic fractures, Clin Orthop Relat Res 297:28, 1993.
Holdsworth FW: Fracture-dislocations of the pelvis, J Bone Joint Surg 30B:461, 1948.
Huittinen VM, Slätis P: Fractures of the pelvis: trauma, mechanisms, type of injury, principles of treatment, Acta Chir Scand 138:563, 1972.
Hupel TM, McKee MD, Waddell JP, et al: Primary external fixation of rota-tionally unstable pelvic fractures in obese patients, J Trauma 45:111, 1998.
Jones AL, Powell JN, Kellam JF, et al: Open pelvic fractures: a multicenter retrospective analysis, Orthop Clin North Am 28:345, 1997.
Keating JF, Werier J, Blachut P, et al: Early fixation of the vertically unstable pelvis: the role of iliosacral screw fixation of the posterior lesion, J Orthop Trauma 13:107, 1999.
Kellam JF: The role of external fixation in pelvic disruptions, Clin Orthop Relat Res 241:66, 1989.
Kellam JF, McMurty RY, Paley D, et al: The unstable pelvic fracture: operative treatment, Orthop Clin North Am 18:25, 1987.
Kiely N, Williams N: Sexual dysfunction in women following pelvic fractures with sacro-iliac disruption, Injury 27:45, 1996.
Kim WY, Hearn TC, Seleem O, et al: Effect of pin location on stability of pelvic external fixation, Clin Orthop Relat Res 361:237, 1999.
Koraitim MM: Pelvic fracture urethral injuries: the unresolved controversy, J Urol 161:1433, 1999.
Koval KJ, Aharonoff GB, Schwartz MC, et al: Pubic rami fracture: a benign pelvic injury, J Orthop Trauma 11:7, 1997.
Kraemer W, Hearn T, Tile M, et al: The effect of thread length and location on extraction strengths of iliosacral lag screws, Injury 25:5, 1994.
Kregor PJ, Routt MLC Jr: Unstable pelvic ring disruptions in unstable patients, Injury 30:SB19, 1999.
Lange RH, Hansen ST Jr: Pelvic ring disruptions with symphysis pubis dias-tasis: indications, technique, and limitations of anterior internal fixation, Clin Orthop Relat Res 201:130, 1985.
Latenser BA, Gentilello LM, Tarver AA, et al: Improved outcome with early fixation of skeletally unstable pelvic fractures, J Trauma 31:28, 1991.
Leenen LPH, van der Werken C, Schoots F, et al: Internal fixation of open unstable pelvic fractures, J Trauma 35:220, 1993.
Leighton RK, Waddell JP, Bray TJ, et al: Biomechanical testing of new and old fixation devices for vertical shear fractures of the pelvis, J Orthop Trauma 5:313, 1991.
Lindahl J, Hirvensalo E, Böstman O, et al: Failure of reduction with an external fixator in the management of injuries of the pelvic ring: long-term evaluation of 110 patients, J Bone Joint Surg 81B:955, 1999.
MacAvoy MC, McClellan RT, Goodman SB, et al: Stability of open-book pelvic fractures using a new biomechanical model of single-limb stance, J Orthop Trauma 11:590, 1997.
MacLeod M, Powell JN: Evaluation of pelvic fractures: clinical and radio-logic, Orthop Clin North Am 28:299, 1997.
Majeed SA: Grading the outcome of pelvic fractures, J Bone Joint Surg 71B:304, 1989.
Malgaigne JF: Traité des fractures et des luxations, Paris, 1847-1855. Treatise on fractures, English translation by JH Packard, Philadelphia, 1959, JB Lippincott.
Matta JM: Indications for anterior fixation of pelvic fractures, Clin Orthop Relat Res 329:88, 1996.
Matta JM, Saucedo T: Internal fixation of pelvic ring fractures, Clin Orthop Relat Res 242:83, 1989.
Matta JM, Tornetta P III: Internal fixation of unstable pelvic ring fractures, Clin Orthop Relat Res 329:129, 1996.
McCarthy ML, MacKenzie EJ, Bosse MJ, et al: Functional status following orthopedic trauma in young women, J Trauma 39:828, 1995.
McMurtry R, Walton D, Dickinson D, et al: Pelvic disruption in the poly-traumatized patient: a management protocol, Clin Orthop Relat Res 151:22, 1980.
PART VII GENERAL PRINCIPLES OF INFECTION2828.e4
Mears DC, Fu FH: External fixation in pelvic fractures, Orthop Clin North Am 11:465, 1980.
Mears DC, Fu FH: Modern concepts of external skeletal fixation of the pelvis, Clin Orthop Relat Res 151:65, 1980.
Mears DC, Rubash HE: Extensile exposure of the pelvis, Contemp Orthop 6:21, 1983.
Miranda MA, Riemer BL, Butterfield S, et al: Functional outcome of pelvic ring disruptions. Paper presented at the 10th annual meeting of the Orthopaedic Trauma Association, San Francisco, 1984.
Miranda MA, Riemer BL, Butterfield SL, et al: Pelvic ring injuries: a long-term functional outcome study, Clin Orthop Relat Res 329:152, 1996.
Moreno C, Moore EE, Rosenberger A, et al: Hemorrhage associated with major pelvic fracture: a multispecialty challenge, J Trauma 26:987, 1986.
Nelson DW, Duwelius PJ: CT-guided fixation of sacral fractures and sacro-iliac joint disruptions, Radiology 180:527, 1991.
O’Brien PJ, Dickson KF: Pelvic fractures: evaluation and acute management. In Tornetta P III, Baumgaertner M, editors: Orthopaedic knowledge update, trauma 3, Rosemont, IL, 2005, American Academy of Orthopae-dic Surgeons.
Ochsner MG, Hoffman AP, DiPasquale D, et al: Associated aortic rupture-pelvic fracture: an alert for orthopedic and general surgeons, J Trauma 33:429, 1992.
Oliver CW, Twaddle B, Agel J, et al: Outcome after pelvic ring fractures: evaluation using the medical outcomes short form SF-36, Injury 27:635, 1996.
Oransky M, Gasparini G: Associated lumbosacral junction injuries (LSJIs) in pelvic fractures, J Orthop Trauma 11:509, 1997.
Palmer S, Fairbank AC, Bircher M: Surgical complications and implications of external fixation of pelvic fractures, Injury 28:649, 1997.
Pell M, Flynn WJ, Seibel RW: Is colostomy always necessary in the treatment of open pelvic fractures? J Trauma 45:317, 1998.
Pennal GF, Tile M, Waddell JP, et al: Pelvic disruption: assessment and clas-sification, Clin Orthop Relat Res 151:12, 1980.
Perez JV, Hughes TMD, Bowers K: Angiographic embolisation in pelvic fracture, Injury 29:187, 1998.
Perry JF Jr: Pelvic open fractures, Clin Orthop Relat Res 151:41, 1980.Podesta ML, Medel R, Castera R, et al: Immediate management of posterior
urethral disruptions due to pelvic fracture: therapeutic alternatives, J Urol 157:1444, 1997.
Pohlemann T, Anst M, Schneider E, et al: Fixation of transforaminal sacrum fractures: a biomechanical study, J Orthop Trauma 7:107, 1993.
Pohlemann T, Bosch U, Gänsslen A, et al: The Hannover experience in management of pelvic fractures, Clin Orthop Relat Res 305:69, 1994.
Pohlemann T, Gänsslen A, Bosch U, et al: The technique of packing for control of hemorrhage in complex pelvic fractures, Tech Orthop 9:267, 1994.
Pohlemann T, Kiessling B, Gänsslen A, et al: Standardized osteosynthesis techniques for the pelvic ring: analysis of a patient sample and surgical technique, Orthopade 21:373, 1992.
Poka A, Libby EP: Indications and techniques for external fixation of the pelvis, Clin Orthop Relat Res 329:54, 1996.
Poole GV, Ward EF: Causes of mortality in patients with pelvic fractures, Orthopedics 17:691, 1994.
Poole GV, Ward EF, Muakkassa FF, et al: Pelvic fracture from major blunt trauma: outcome is determined by associated injuries, Ann Surg 213:532, 1991.
Raf L: Double vertical fractures of the pelvis, Acta Chir Scand 131:298, 1966.Reilly MC, Zinar DM, Matta JM: Neurologic injuries in pelvic ring fractures,
Clin Orthop Relat Res 329:28, 1996.Richardson JD, Harty J, Amin M, et al: Open pelvic fractures, J Trauma
22:533, 1982.Richardson JD, Harty J, Amin M, et al: Open pelvic fractures, J Trauma
25:547, 1985.Riemer BL, Butterfield SL, Diamond DL, et al: Acute mortality associated
with injuries to the pelvic ring: the role of early patient mobilization and external fixation, J Trauma 35:671, 1993.
Routt MLC Jr, Meier MC, Kregor PJ, et al: Percutaneous iliosacral screws with the patient supine technique, Tech Orthop 3:35, 1993.
Routt MLC Jr, Simonian PT: Closed reduction and percutaneous skeletal fixation of sacral fractures, Clin Orthop Relat Res 329:121, 1996.
Routt MLC Jr, Simonian PT: Internal fixation of pelvic ring disruptions, Injury 27:SB20, 1996.
Routt MLC Jr, Simonian PT, Agnew SG, et al: Radiographic recognition of the sacral alar slope for optimal placement of iliosacral screws: a cadaver and clinical study, J Orthop Trauma 10:171, 1996.
Routt MLC Jr, Simonian PT, Ballmer F: A rational approach to pelvic trauma: resuscitation and early definitive stabilization, Clin Orthop Relat Res 318:61, 1995.
Routt MLC, Simonian PT, Defalco AJ, et al: Internal fixation in pelvic frac-tures and primary repairs of associated genitourinary disruptions: a team approach, J Trauma 40:784, 1996.
Routt MLC Jr, Simonian PT, Grujic L: The retrograde medullary superior pubic ramus screw for the treatment of anterior pelvic ring disruptions: a new technique, J Orthop Trauma 9:35, 1995.
Routt MLC Jr, Simonian PT, Mills WJ: Iliosacral screw fixation: early complications of the percutaneous technique, J Orthop Trauma 11:584, 1997.
Salome F, Cazaux P, Setton D, et al: Bladder entrapment during internal fixa-tion of a pelvic fracture, J Urol 161:213, 1999.
Schütz M, Stöckle U, Hoffmann R, et al: Clinical experience with two types of pelvic C-clamps for unstable pelvic ring injuries, Injury 27:SA46, 1996.
Seibel R, LaDuca J, Hassett JM, et al: Blunt multiple trauma (ISS 36), femur traction and a pulmonary failure-septic state, Ann Surg 202:283, 1985.
Semba RT, Yasukawa K, Gustilo RB: Critical analysis of results of 53 Mal-gaigne fractures of the pelvis, J Trauma 23:535, 1983.
Shaw JA, Mino DE, Werner FW, et al: Posterior stabilization of pelvic frac-tures by use of threaded compression rods: case reports and mechanical testing, Clin Orthop Relat Res 192:240, 1985.
Simonian PT, Routt MLC Jr, Harrington RM, et al: Internal fixation of the unstable anterior pelvic ring: a biomechanical comparison of standard plating techniques and the retrograde medullary superior pubic ramus screw, J Orthop Trauma 8:476, 1994.
Simonian PT, Routt MLC Jr, Harrington RM, et al: Box plate fixation of the symphysis pubis: biomechanical evaluation of a new technique, J Orthop Trauma 8:483, 1994.
Simonian PT, Routt MLC Jr, Harrington RM, et al: Anterior versus posterior provisional fixation in the unstable pelvis: a biomechanical comparison, Clin Orthop Relat Res 310:245, 1995.
Simonian PT, Routt MLC Jr, Harrington RM, et al: Internal fixation for the transforaminal sacral fracture, Clin Orthop Relat Res 323:202, 1996.
Simonian PT, Routt MLC Jr, Harrington RM, et al: The unstable iliac fracture: a biomechanical evaluation of internal fixation, Injury 28:469, 1997.
Simpson LA, Waddell JP, Leighton RK, et al: Anterior approach and stabiliza-tion of the disrupted sacroiliac joint, J Trauma 27:1332, 1987.
Slätis P, Karaharju EO: External fixation of unstable pelvic fractures: experi-ences in 22 patients treated with a trapezoid compression frame, Clin Orthop Relat Res 151:73, 1980.
Stevens SCC, Male TA, Turner JH: Pelvic fractures diagnosed by bone scin-tigraphy in patients with normal radiographs after a fall, Med J Aust 171:476, 1999.
Taffet R: Management of pelvic fractures with concomitant urologic injuries, Orthop Clin North Am 28:389, 1997.
Templeman D, Goulet J, Duwelius PJ, et al: Internal fixation of displaced fractures of the sacrum, Clin Orthop Relat Res 329:180, 1996.
Templeman D, Schmidt A, Freese J, et al: Proximity of iliosacral screws to neurovascular structures after internal fixation, Clin Orthop Relat Res 329:194, 1996.
Tile M: Pelvic ring fractures: should they be fixed? J Bone Joint Surg 70B:1, 1988.
Tile M: Acute pelvic fractures: I. Causation and classification, J Am Assoc Orthop Surg 4:143, 1996.
Tile M: Acute pelvic fractures: II. Principles of management, J Am Assoc Orthop Surg 4:152, 1996.

CHAPTER 56 FRACTURES OF ACETABULUM AND PELVIS 2828.e5
Tile M: Anatomy of the pelvic ring. In Tile M, Helfet DL, Kellam JF, editors: Fractures of the pelvis and acetabulum, ed 3, Philadelphia, 2003, Lippin-cott Williams & Wilkins.
Tile M, Pennal GF: Pelvic disruption: principles of management, Clin Orthop Relat Res 151:56, 1980.
Tonetti J, Carrat L, Lavallee S, et al: Percutaneous iliosacral screw placement using image guided techniques, Clin Orthop Relat Res 354:103, 1998.
Tornetta P III, Dickson K, Matta JM: Outcome of rotationally unstable pelvic ring injuries treated operatively, Clin Orthop Relat Res 329:147, 1996.
Tornetta P III, Matta JM: Outcome of operatively treated unstable posterior pelvic ring disruptions, Clin Orthop Relat Res 329:186, 1996.
Van den Bosch EW, Van der Kleyne R, Hogervorst M, et al: Functional outcome of internal fixation for pelvic ring fractures, J Trauma 47:365, 1999.
Van Veen IHPAA, van Leeuwen AAM, van Popta T, et al: Unstable pelvic fractures: a retrospective analysis, Injury 26:81, 1995.
Vrahas MS, Wilson SC, Cummings PD, et al: Comparison of fixation methods for preventing pelvic ring expansion, Orthopedics 21:286, 1998.
Ward EF, Tomasin J, Vander Griend RA: Open reduction and internal fixa-tion of vertical shear pelvic fractures, J Trauma 27:291, 1987.
Ward LD, Morandi MM, Pearse M, et al: The immediate treatment of pelvic ring disruption with the pelvic stabilizer, Bull Hosp Jt Dis 56:104, 1997.
Webb LX, Gristina AG, Wilson JR, et al: Two-hole plate fixation for traumatic symphysis pubis diastasis, J Trauma 28:813, 1988.
Wolinsky PR: Assessment and management of pelvic fracture in the hemo-dynamically unstable patient, Orthop Clin North Am 28:321, 1997.
Woods RK, O’Keefe G, Rhee P, et al: Open pelvic fracture and fecal diversion, Arch Surg 133:281, 1998.
Young JWR, Burgess AR, editors: Radiologic management of pelvic ring fractures: systemic radiographic diagnosis, Baltimore, 1987, Urban & Schwarzenberg.
Zagaja GP, Cromie WJ: Heterotopic bone formation in association with pelvic fracture and urethral disruption, J Urol 161:1950, 1999.




![PELVIS - users.atw.huusers.atw.hu/aokszote/download.php?fname=./01] ALAPOZO MODUL... · ramus inferior et superior ossis ischii – corpus ossis ischii v) Acetabulum (Y alakú synostosis](https://static.fdocuments.net/doc/165x107/5b81d6fb7f8b9a2b678d4594/pelvis-usersatw-alapozo-modul-ramus-inferior-et-superior-ossis-ischii.jpg)