
ABUHB Liver Disease Delivery Plan 2015-2020 1. … Liver Disease... · Sclerosing Cholangitis)...
42
ABUHB Liver Disease Delivery Plan 2015-2020 V0e Page 1 of 42 1. BACKGROUND AND CONTEXT “Together for Health – Liver Disease Delivery Plan” was published by the Welsh Government in 2015 and provides a framework for action by Local Health Boards and NHS Trusts working together with their partners to develop and improve services for people with liver disease. It sets out the Welsh Government’s requirement of NHS Wales and its partners to assess population need and plan the delivery of liver disease, to work to reduce the burden of liver disease, to deliver liver disease services to the highest possible standard, and to demonstrate improved outcomes for people with liver disease. It focuses on how to prevent the disease in the first instance and also, where necessary, to ensure people have access to excellent care, reaching across 6 themes. For each theme it sets out: Delivery aspirations for the prevention and treatment of liver disease Specific priorities to 2020 Responsibility to develop and deliver actions to achieve the specific priorities Population outcome indicators and NHS assurance measures The vision: Our vision for the care for patients with liver disease is: Before 2020 halt the rise in morbidity and mortality related to liver disease. For NHS Wales to collaborate equally with its partners in social services and the third sector to provide seamless care to patients, where possible in the community. For clinical leadership and multi-disciplinary working to help improve the quality of the patient pathway and drive down harm, waste and variation. For better medical undergraduate, postgraduate and healthcare professional understanding of liver disease. Patients responsible for their health, having an equal voice in their treatment and through the third sector having shared responsibility to determine the shape of services for liver disease. We will use a range of indicators to measure success. These are a number of population outcome indicators and NHS assurance measures in the Liver Disease Delivery Plan. These will be developed further and refined over time. The Drivers: The liver is the second largest organ in the body and it performs hundreds of complex functions including: fighting infections and illness; removing toxins (such as alcohol) from the body; controlling cholesterol levels; helping blood to clot; and releasing bile (a liquid that breaks down fats and aids digestion). There are many diseases that can affect the liver leading to chronic liver disease, cirrhosis, liver failure and potentially liver cancer. The main types of liver disease include:
-
Upload
nguyenhuong -
Category
Documents
-
view
219 -
download
0
Transcript of ABUHB Liver Disease Delivery Plan 2015-2020 1. … Liver Disease... · Sclerosing Cholangitis)...
ABUHB Liver Disease Delivery Plan 2015-2020
V0e Page 1 of 42
1. BACKGROUND AND CONTEXT “Together for Health – Liver Disease Delivery Plan” was published by the Welsh Government in 2015 and provides a framework for action by Local Health Boards and NHS Trusts working together with their partners to develop and improve services for people with liver disease. It sets out the Welsh Government’s requirement of NHS Wales and its partners to assess population need and plan the delivery of liver disease, to work to reduce the burden of liver disease, to deliver liver disease services to the highest possible standard, and to demonstrate improved outcomes for people with liver disease. It focuses on how to prevent the disease in the first instance and also, where necessary, to ensure people have access to excellent care, reaching across 6 themes. For each theme it sets out:
Delivery aspirations for the prevention and treatment of liver disease
Specific priorities to 2020
Responsibility to develop and deliver actions to achieve the specific priorities
Population outcome indicators and NHS assurance measures The vision: Our vision for the care for patients with liver disease is:
Before 2020 halt the rise in morbidity and mortality related to liver disease.
For NHS Wales to collaborate equally with its partners in social services and the third sector to provide seamless care to patients, where possible in the community.
For clinical leadership and multi-disciplinary working to help improve the quality of the patient pathway and drive down harm, waste and variation.
For better medical undergraduate, postgraduate and healthcare professional understanding of liver disease.
Patients responsible for their health, having an equal voice in their treatment and through the third sector having shared responsibility to determine the shape of services for liver disease.
We will use a range of indicators to measure success. These are a number of population outcome indicators and NHS assurance measures in the Liver Disease Delivery Plan. These will be developed further and refined over time. The Drivers: The liver is the second largest organ in the body and it performs hundreds of complex functions including: fighting infections and illness; removing toxins (such as alcohol) from the body; controlling cholesterol levels; helping blood to clot; and releasing bile (a liquid that breaks down fats and aids digestion). There are many diseases that can affect the liver leading to chronic liver disease, cirrhosis, liver failure and potentially liver cancer. The main types of liver disease include:
ABUHB Liver Disease Delivery Plan 2015-2020
V0e Page 2 of 42
Alcohol-related liver disease – where the liver is damaged after years of alcohol misuse.
Non-alcoholic fatty liver disease – a build-up of fat within liver cells, usually seen in overweight or obese people.
Viral Hepatitis – inflammation of the liver caused by a viral infection.
Autoimmune liver disease – where the body’s immune system attacks the liver cells (Autoimmune hepatitis) or bile ducts (Primary Biliary Cirrhosis and Primary Sclerosing Cholangitis)
Inherited metabolic liver diseases such as Haemochromatosis, alpha-1 antitrypsin deficiency or Wilson’s disease – these disorders occur due to inherited abnormalities of metabolism leading to accumulation of abnormal products within the liver and lead to its damage.
Mortality1 rates for liver disease in the UK have increased 400% since 1970 and liver disease is now a common cause of death after cancer, heart disease, stroke and respiratory disease.2 It is also the third biggest cause of premature mortality in the UK and accounts for 62,000 years of working life lost per year across the UK. Admissions to hospital because of liver disease are increasing with most patients admitted with end-stage disease, liver cirrhosis or liver failure. This is primarily the result of an increase of excess alcohol consumption and an epidemic of obesity in the population but viral hepatitis also plays a major role in terms of the burden of end stage liver disease. The prevalence of key risk factors associated with liver disease and its outcomes are linked to social deprivation and inequality. Obesity is an increasing challenge in all age groups and may become the main cause of liver disease in the future. The most recent report from the child measurement programme for Wales indicated in 2012-13 26% of children age 4-5 were overweight or obese. There was variation across Wales with 21% being overweight or obese in the least deprived parts of Wales and 29% in the most deprived areas. Failure to address this problem will lead to an increase in the burden of obesity-related liver disease in the future. There are also groups of individuals with higher risk of exposure to blood borne viral hepatitis who may have, or go onto develop, chronic viral hepatitis. The Welsh Government’s Blood Borne Viruses Action Plan for Wales 2010-2015 provides a strong platform for further efforts in this plan to tackle liver disease related to blood borne viruses and the associated risk factors. Prevalence of hepatitis C is known to be higher among some populations, for example injecting drug users and those born in countries of high prevalence. Many of these populations have higher prevalence for different reasons and targeted action in different communities and settings will be required. The Welsh Government's Substance Misuse Delivery Plan 2013-15 has helped to tackle unsafe injector practice and excessive alcohol consumption.
1 Addressing liver disease in the UK: a blueprint for attaining excellence in health care and reducing premature mortality from lifestyle issues of excess consumption of alcohol, obesity, and viral hepatitis. (Roger Williams et al; Lancet; 2014; 384: 1953–97) 2 http://www.britishlivertrust.org.uk/about-us/media-centre/facts-about-liver-disease/

ABUHB Liver Disease Delivery Plan 2015-2020
V0e Page 3 of 42
What do we want to achieve? The Delivery Plan sets out action to improve outcomes in the following key areas between now and 2020:
Preventing liver disease
Timely detection of liver disease
Fast and effective care
Living with liver disease
Improving Information
Targeting research
2. ORGANISATIONAL PROFILE Organisational overview The ABUHB liver service is provided under the auspices of the Gwent Liver Unit, which sits within the Department of Gastroenterology and Hepatology in the Unscheduled Care Division. The workforce currently comprises 2 substantive consultant Hepatologists (spend more than 50% of their time dedicated to the care of liver disease). Both consultants are based on the Royal Gwent Hospital (RGH) site. The consultant who provided liver care to patients admitted to Nevill Hall Hospital (NHH) and saw outpatients within that locality left in December 2014 and has not been substantively replaced although a locum is in place from September 2015. Furthermore the senior consultant on the RGH site who contributes to the care of liver inpatients and undertakes some outpatient work has delayed retirement due to the recent inability to recruit to the post based at RGH. The service is supported by 2 Hepatology Nurse specialists (one funded by the BBV plan), a community Blood Borne Virus (BBV) nurse and a Community Psychiatric Nurse (CPN). In addition Advanced Nurse Practitioners within Gastroenterology on both the RGH and NHH site support the medical teams in management of complex liver disease (abdominal drains predominantly). The service is further supported by diagnostic and interventional radiology and by the intensive care units at RGH and NHH. Waiting times for new and follow up appointments are longer than required across the health board for Gastroenterology patients and data has proven difficult to obtain for Liver specific referrals and this is an informatics issue that will need to be addressed. Despite workforce limitations the liver service provides a wide array of diagnostic and therapeutic options for patients with liver disease. The Liver Unit was the first in Wales to have a Fibroscan and the first to have an portable Fibroscan for use prisons and remote sites. In addition to a full array of relevant diagnostic tests (including transjugular liver biopsy which is not universally available) the Gwent Liver Unit is the only centre in Wales able to offer both radiofrequency ablation (RFA) and trans arterial
ABUHB Liver Disease Delivery Plan 2015-2020
V0e Page 4 of 42
chemoebolisation (TACE) for patients with primary liver cancer. The ability exists within the Liver Unit to also offer TIPS procedures to control bleeding or fluid overload in liver disease but is not currently financially supported. Inpatients on the RGH site are managed by dedicated Hepatologists although the same is not true at NHH though planned centralisation of this service is implicit within the Clinical Futures model. For outpatients, selected stable patients with cirrhosis are managed by the Specialist nurses and a HCC surveillance programme is in operation but requires a more formalised approach (automatic recall system not in place). Fully dedicated liver clinics do not currently exist though the Monday County clinic is attended by the 2 RGH Hepatologists and the NHH locum and this provides the possibility to fully ring fence these clinics for patients with liver disease. Overview of local health need related to liver disease prevention and service provision This needs profile is based on the data provided by the Public Health Wales Observatory in support of local Liver Disease Plans. The profile is split into three sections: lifestyle indicators, hospital activity and mortality indicators. We have included charts here to illustrate the most notable points, with the remainder in Appendix 1 for reference. 1. Lifestyle indicators
Adult obesity
The latest Welsh Health Survey data indicates 25% of adults in Aneurin Bevan
University Health Board (ABUHB) area are obese (report height and weight
equivalent to a Body Mass Index (BMI) of 30+).
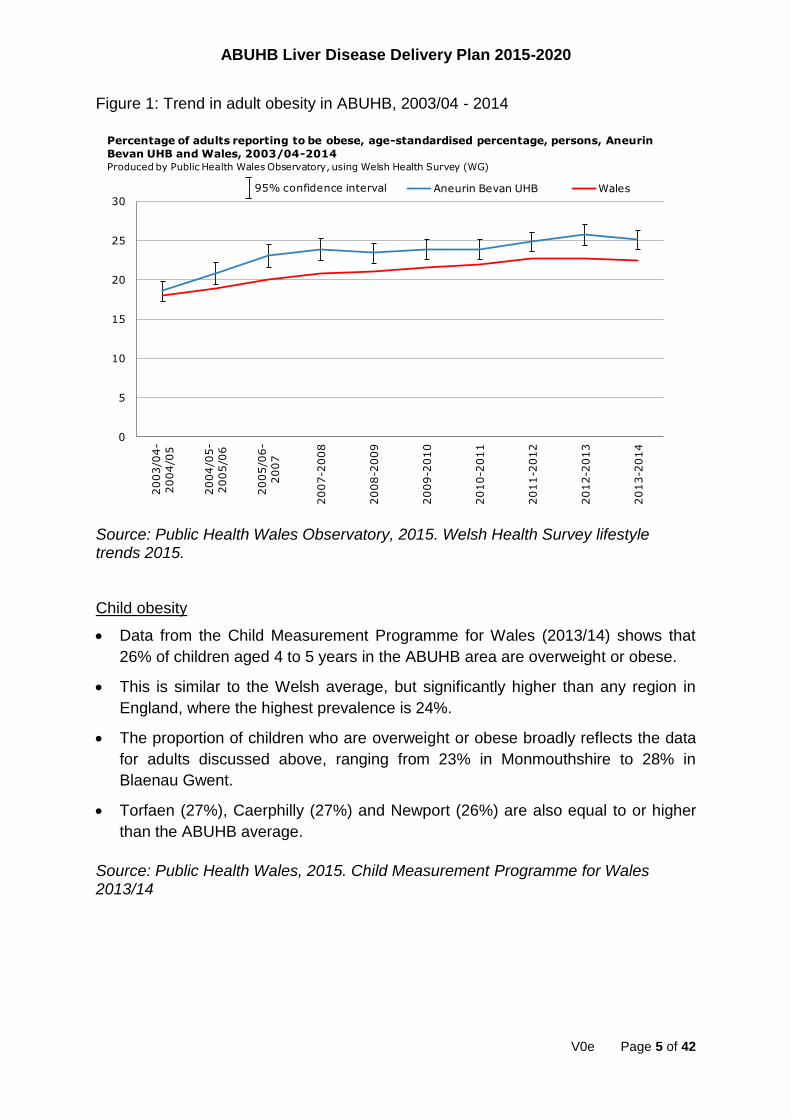
This percentage is significantly higher than the all Wales average (22%) and
shows an upwards trend since 2003/04 (see Figure 1).
The boroughs of Caerphilly (28%), Blaenau Gwent (29%) and Torfaen (27%) in
particular are significantly higher than the Wales average, with Newport at 23%.
Monmouthshire is the only authority in ABUHB that is significantly lower than the
Wales average (18%).
ABUHB Liver Disease Delivery Plan 2015-2020
V0e Page 5 of 42
Figure 1: Trend in adult obesity in ABUHB, 2003/04 - 2014
Source: Public Health Wales Observatory, 2015. Welsh Health Survey lifestyle trends 2015. Child obesity
Data from the Child Measurement Programme for Wales (2013/14) shows that
26% of children aged 4 to 5 years in the ABUHB area are overweight or obese.
This is similar to the Welsh average, but significantly higher than any region in
England, where the highest prevalence is 24%.
The proportion of children who are overweight or obese broadly reflects the data
for adults discussed above, ranging from 23% in Monmouthshire to 28% in
Blaenau Gwent.
Torfaen (27%), Caerphilly (27%) and Newport (26%) are also equal to or higher
than the ABUHB average.
Source: Public Health Wales, 2015. Child Measurement Programme for Wales 2013/14
0
5
10
15
20
25
30
2003/0
4-
2004/0
5
2004/0
5-
2005/0
6
2005/0
6-
2007
2007-2
008
2008-2
009
2009-2
010
2010-2
011
2011-2
012
2012-2
013
2013-2
014
Aneurin Bevan UHB Wales
Percentage of adults reporting to be obese, age-standardised percentage, persons, Aneurin
Bevan UHB and Wales, 2003/04-2014Produced by Public Health Wales Observatory, using Welsh Health Survey (WG)
95% confidence interval
ABUHB Liver Disease Delivery Plan 2015-2020
V0e Page 6 of 42
Months of life lost due to alcohol misuse This is an estimate of the increase in life expectancy at birth that would be expected if all alcohol-attributable deaths among persons aged under 75 years were prevented. The number of months lost due to alcohol is 12.4 for males and 5.8 for females in the ABUHB area. The average for Wales is 13.5 for males and 6.5 for females. Source: Public Health Wales Observatory, 2014. Alcohol and Health in Wales Profile 2. Hospital Activity
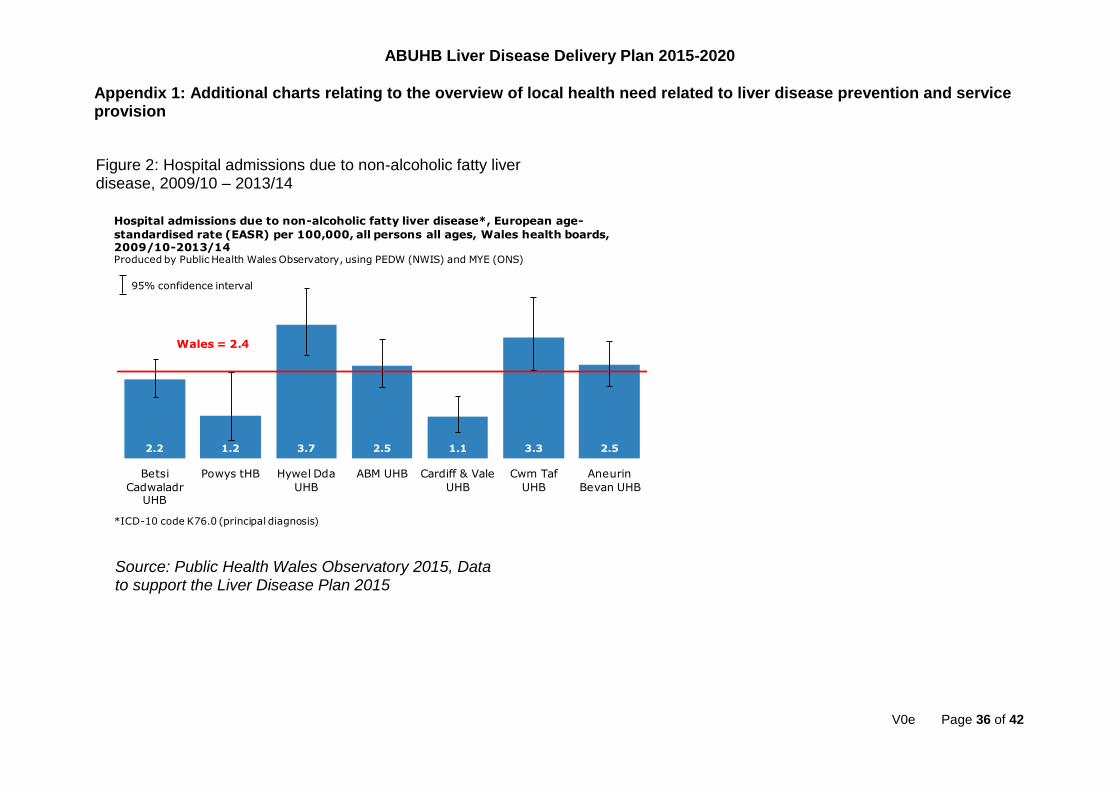
Hospital admissions due to non-alcoholic fatty liver disease
In the ABUHB area, the admission rate due to non-alcoholic fatty liver disease (NAFLD) is 2.5 per 100,000, which is similar to the all Wales average and third highest in Wales (Appendix 1: Figure 2). Hospital admissions due to alcoholic liver disease
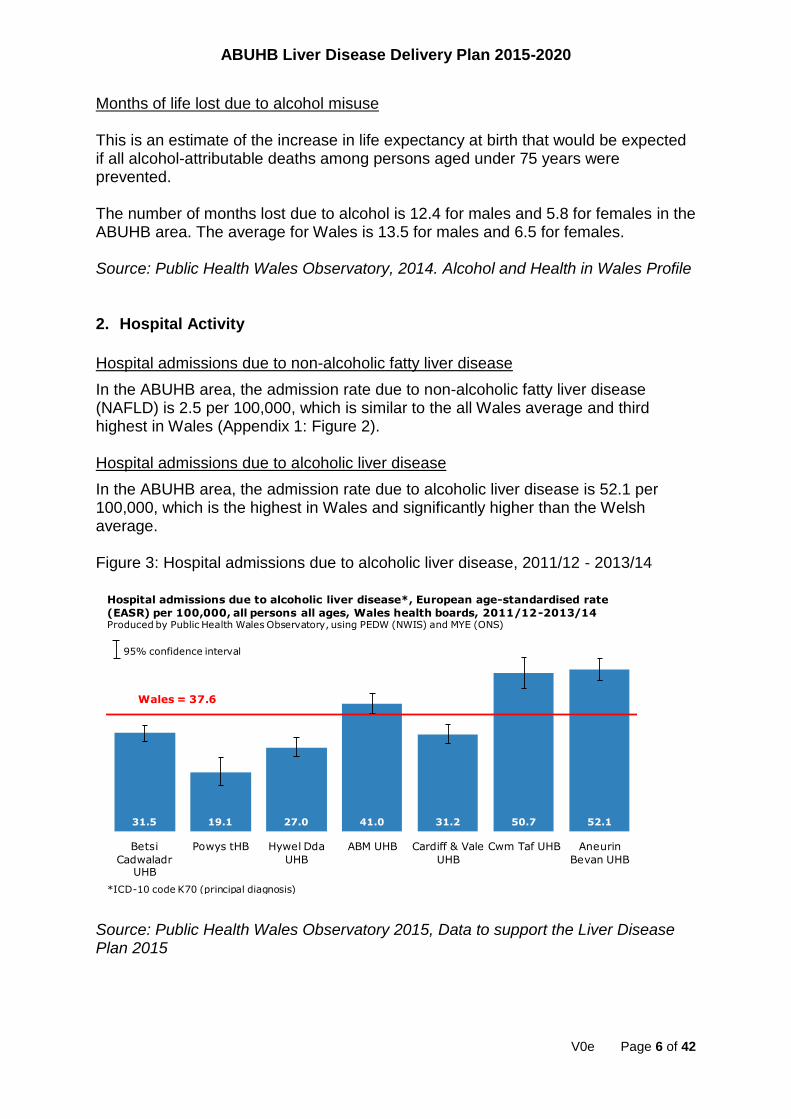
In the ABUHB area, the admission rate due to alcoholic liver disease is 52.1 per 100,000, which is the highest in Wales and significantly higher than the Welsh average. Figure 3: Hospital admissions due to alcoholic liver disease, 2011/12 - 2013/14
Source: Public Health Wales Observatory 2015, Data to support the Liver Disease Plan 2015
31.5 19.1 27.0 41.0 31.2 50.7 52.1
Betsi
Cadwaladr UHB
Powys tHB Hywel Dda
UHB
ABM UHB Cardiff & Vale
UHB
Cwm Taf UHB Aneurin
Bevan UHB
Hospital admissions due to alcoholic liver disease*, European age-standardised rate
(EASR) per 100,000, all persons all ages, Wales health boards, 2011/12-2013/14Produced by Public Health Wales Observatory, using PEDW (NWIS) and MYE (ONS)
95% confidence interval
Wales = 37.6
*ICD-10 code K70 (principal diagnosis)
ABUHB Liver Disease Delivery Plan 2015-2020
V0e Page 7 of 42
Alcohol-specific hospital admissions (all ages)
There were 2,126 people admitted with an alcohol-specific condition either in the
primary or secondary diagnosis in the ABUHB area during 2012/13.
ABUHB has the highest rate of alcohol-specific hospital admissions in Wales,
significantly higher than the all Wales average (see Figure 4).
There are more males than females admitted with an alcohol-specific condition,
but the rates for both are significantly higher than the average for Wales.
The rate of alcohol-specific hospital admissions has been trending upwards in the
ABUHB area and has been significantly higher than the Wales average since
2009/10, although there is an indication of this gap starting to decrease in
2012/13 (see Figure 5).
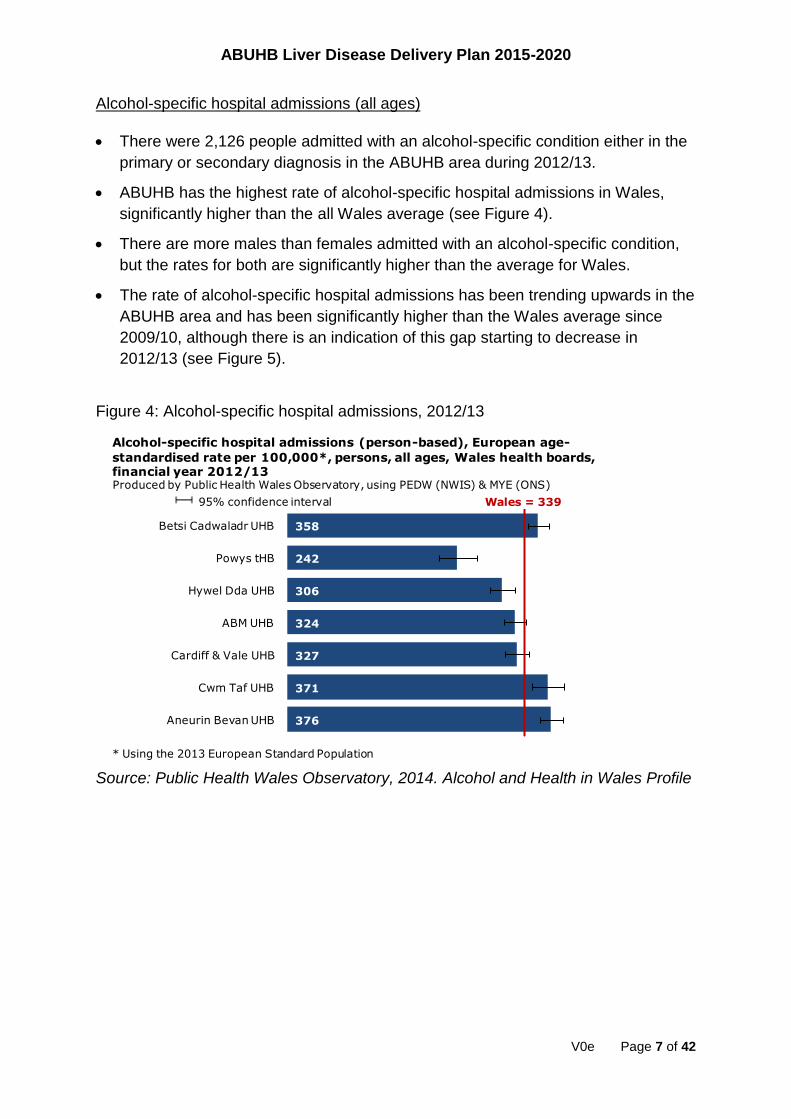
Figure 4: Alcohol-specific hospital admissions, 2012/13
Source: Public Health Wales Observatory, 2014. Alcohol and Health in Wales Profile
358
242
306
324
327
371
376
Wales = 339
Betsi Cadwaladr UHB
Powys tHB
Hywel Dda UHB
ABM UHB
Cardiff & Vale UHB
Cwm Taf UHB
Aneurin Bevan UHB
Alcohol-specific hospital admissions (person-based), European age-
standardised rate per 100,000*, persons, all ages, Wales health boards, financial year 2012/13Produced by Public Health Wales Observatory, using PEDW (NWIS) & MYE (ONS)
* Using the 2013 European Standard Population
95% confidence interval

ABUHB Liver Disease Delivery Plan 2015-2020
V0e Page 8 of 42
Figure 5: Trend in alcohol-specific hospital admissions, 2003/04 – 2012/13
Source: Public Health Wales Observatory, 2014. Alcohol and Health in Wales Profile Alcohol-specific hospital admissions (under 18)
On average, 88 people aged under 18 were admitted annually in ABUHB with an
alcohol-specific condition during the period 2010/11 – 2012/13.
The ABUHB rate is not significantly higher than the all Wales average (see Figure
6), but it should be noted that Wales has a significantly higher alcohol-specific
admission rate (under 18) than that observed in England.
In this age group there are more females than males admitted with an alcohol-
specific condition.
The rate of alcohol-specific hospital admissions for under 18s has been trending
downwards in the ABUHB area since the period 2005/06 – 2006/07, with the gap
between the Health Board and Wales rates closing (see Figure 7).
0
50
100
150
200
250
300
350
400
450
2003/04 2004/05 2005/06 2006/07 2007/08 2008/09 2009/10 2010/11 2011/12 2012/13
Aneurin Bevan UHB Wales
Alcohol-specific hospital admissions (person-based), European age-standardised rate
per 100,000*, persons, all ages, Aneurin Bevan UHB and Wales, financial years 2003/04-2012/13
Produced by Public Health Wales Observatory, using PEDW (NWIS) & MYE (ONS)
95% confidence interval
* Using the 2013 European Standard Population

ABUHB Liver Disease Delivery Plan 2015-2020
V0e Page 9 of 42
Figure 6: Alcohol-specific hospital admissions (under 18), 2010/11 – 2012/13
Source: Public Health Wales Observatory, 2014. Alcohol and Health in Wales Profile Figure 7: Trend in alcohol-specific hospital admissions (under 18), 2003/04 – 2012/13
Source: Public Health Wales Observatory, 2014. Alcohol and Health in Wales Profile
76
50
85
52
30
87
70
Wales = 65
Betsi Cadwaladr UHB
Powys tHB
Hywel Dda UHB
ABM UHB
Cardiff & Vale UHB
Cwm Taf UHB
Aneurin Bevan UHB
Alcohol-specific hospital admissions (person-based), crude rate per 100,000,
persons aged under 18, Wales health boards, financial years 2010/11-2012/13Produced by Public Health Wales Observatory, using PEDW (NWIS) & MYE (ONS)
95% confidence interval
0
20
40
60
80
100
120
140
160
2003/04-2005/06
2004/05-2006/07
2005/06-2007/08
2006/07-2008/09
2007/08-2009/10
2008/09-2010/11
2009/10-2011/12
2010/11-2012/13
Aneurin Bevan UHB Wales
Alcohol-specific hospital admissions (person-based), 3-year rolling crude rate per
100,000, persons aged under 18, Aneurin Bevan UHB and Wales, financial years 2003/04-2012/13
Produced by Public Health Wales Observatory, using PEDW (NWIS) & MYE (ONS)
95% confidence interval
ABUHB Liver Disease Delivery Plan 2015-2020
V0e Page 10 of 42
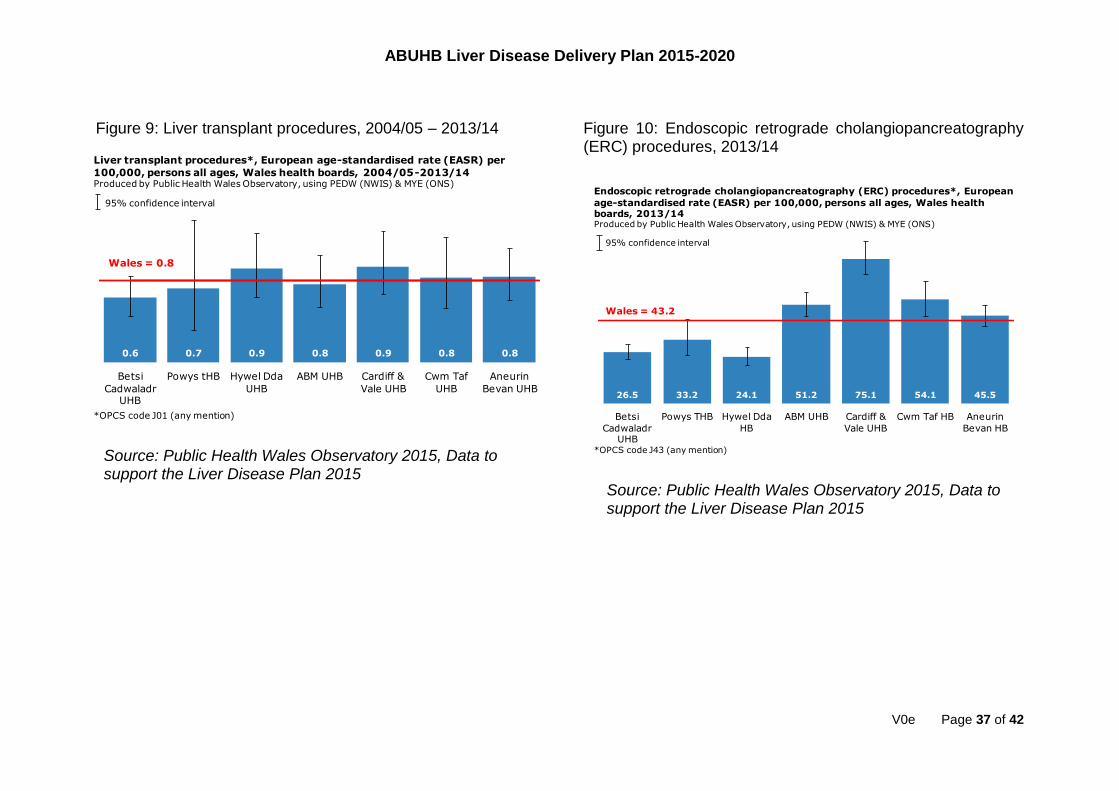
Liver transplant procedures The rate of liver transplant procedures in ABUHB is low at 0.8 per 100,000 (for the period 2004/05 – 2013/14), and is consistent with the all Wales average (Appendix 1: Figure 9). Endoscopic retrograde cholangiopancreatography (ERC) procedures
The rate of ERC procedures in ABUHB in 2013/14 is 45.5 per 100,000 which is among the highest in Wales, but not significantly higher than the all Wales average (Appendix 1: Figure 10). Paracetamol overdose hospital admissions
The ABUHB rate of hospital admissions due to paracetamol overdose (accidental or intentional poisoning) was 100.8 per 100,000 which is significantly lower than the all Wales average in 2013/14 (Appendix 1: Figure 11). Liver disease hospital admissions
The ABUHB rate of liver disease hospital admissions in 2013/14 was 91.8 per 100,000 which is consistent with the all Wales average (Appendix 1: Figure 12). Hepatitis B related end-stage liver disease/hepatocellular carcinoma hospital admissions
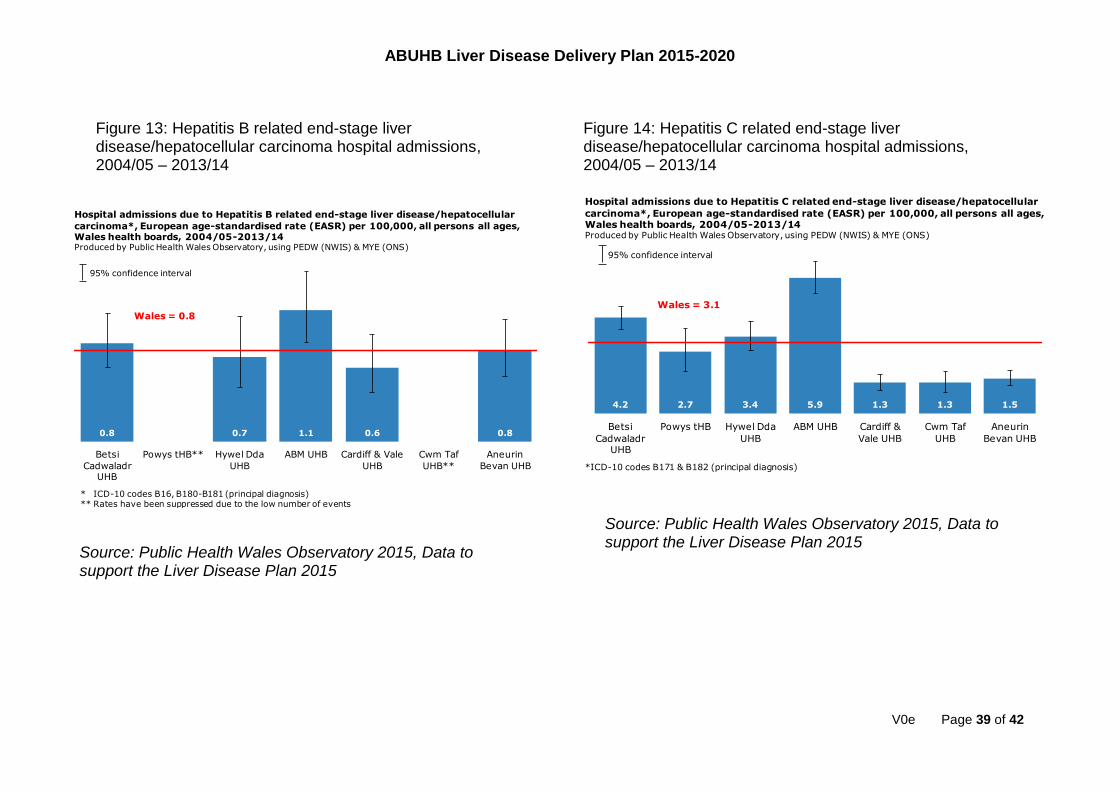
The ABUHB rate of hospital admissions due to Hepatitis B related end-stage liver disease / hepatocellular carcinoma is low at 0.8 per 100,000 (for the period 2004/05 – 2013/14) and is consistent with the all Wales average (Appendix 1: Figure 13). Hepatitis C related end-stage liver disease/hepatocellular carcinoma hospital admissions
The ABUHB rate of hospital admissions due to Hepatitis C related end-stage liver disease / hepatocellular carcinoma is 1.5 per 100,000 (for the period 2004/05 – 2013/14) and significantly lower than the all Wales average (Appendix 1: Figure 14). 3. Mortality Indicators
Pancreatic cancer mortality
The ABUHB mortality rate from pancreatic cancer (under 75 years of age) is 8.4 per 100,000, which is lower than the all Wales average (not significantly) and similar to other Health Boards in Wales (Appendix 1: Figure 15). Paracetamol poisoning mortality
The mortality rate from paracetamol poisoning is low across Wales, with the ABUHB rate being slightly lower than the Wales average at 0.5 per 100,000 in the period 2004-2013 (Appendix 1: Figure 16). Chronic liver disease (including cirrhosis) mortality
The mortality rate in ABUHB from chronic liver disease (all ages) is 14.6 per
100,000, which is consistent with the all Wales average (Appendix 1: Figure 17).
ABUHB Liver Disease Delivery Plan 2015-2020
V0e Page 11 of 42
Mortality is higher in males than females and this is also consistent with the
national picture.
The majority of chronic liver disease mortality occurs in those under 75 (Appendix
1: Figure 18).
All cause liver disease mortality, aged under 75 years
The mortality rate in ABUHB from chronic liver disease (under 75) is 22.3 per 100,000, which is slightly higher (not significant) than the all Wales average (Appendix 1: Figure 19). The mortality rate is higher in males than females and this is also consistent with the national picture. Liver cancer mortality, aged under 75 years
Liver cancer mortality rates are relatively small in the ABUHB area, at 5.1 per 100,000 in the period 2009-13. This is slightly higher than the all Wales average (which is 4 per 100,000) and this difference appears to be statistically significant (Appendix 1: Figure 20). Key points from the needs analysis
One quarter of the adult population in ABUHB are obese, and one quarter of
children aged 4 to 5 years are overweight or obese, with an upward trend in
obesity rates. It is anticipated that this will result in additional non-alcoholic
fatty liver disease that we are not yet seeing reflected in treatment services.
The health board has significantly more alcohol-specific hospital admissions
and admissions due to alcoholic liver disease in adults compared with the
Wales average, indicating that further work is needed on early identification
and treatment of alcohol misuse problems.
While use of treatment services and mortality rates from liver disease are
generally consistent with the all Wales average, they are still too high in
comparison to the rest of the UK and we must do more to improve the
detection and treatment of liver disease.
This needs analysis has highlighted that there is a data development agenda,
with better quality data needed to assist with planning and evaluating
services. There is a need for additional capacity to extract and analyse local
hospital-collected data which is of a good enough quality to use for audit and
evaluation purposes. In addition, there is a need for data on BBV testing and
treatment to ensure we are reaching all the groups at risk of developing viral
hepatitis.

ABUHB Liver Disease Delivery Plan 2015-2020
V0e Page 12 of 42
3. DEVELOPMENT OF ANEURIN BEVAN UNIVERSITY HEALTH BOARD LIVER DISEASE LOCAL DELIVERY PLAN
In response to the “Together for Health – Liver Disease Delivery Plan” (2015), Health Boards are required, together with their partners, to produce and publish a detailed local service delivery plan. The Blood Borne Viruses (BBV) Action Plan for Wales 2010-2015 and the Substance Misuse Delivery Plan 2013-15 have provided a strong platform for tackling blood borne viral hepatitis as a leading cause of liver disease. There is also important related work contained in the All Wales Obesity Pathway and other delivery plans covering Sexual Health, Stroke, Heart Disease, Diabetes, Cancer, the Critically Ill, End of Life Care and Organ Donation. This work will continue, and where relevant link across to this plan to tackle the burden of liver disease. Important contributions to tackling liver disease have been made by the British Society of Gastroenterology in its reports: the National Plan for Liver Services UK (2009) and Alcohol Related Disease (2010); as well as the 2014 Lancet report ‘Addressing Liver Disease in the UK’. A number of challenges in the provision of specialist care were also highlighted in the 2013 UK National Confidential Enquiry into Patient Outcome and Death (NCEPOD) report into alcohol-related liver disease deaths. The ABUHB Executive Lead for liver disease will need to report progress formally to their Boards against milestones in these delivery plans and publish these reports on their websites at least annually. Additional resource is required to deliver the Liver Disease Deliver Plan. Welsh Government have pledged £1 million to support the delivery of the plan, but it is yet unknown how this will be allocated. In relation to Health Board funding, a business case will be prepared for each scheme proposed in the plan. These scheme will highlight what additional benefit will be accrued from investment and these will be considered as part of the refresh of the IMTP for 2016/17 and the Clinical Futures programme. This plan is based on available data supplied by the PHW Observatory. The Public Health Team has also undertaken a review of local progress against Welsh Government’s BBV Hepatitis Action Plan to inform future action in this area. Partners from across the directorates within the health board, including Gastroenterology, Dietetics and local Alcohol Misuse Services have worked together to identify actions required to meet the priorities of the “Together for Health – Liver Disease Delivery Plan”, and these are detailed in the action plan below.
ABUHB Liver Disease Delivery Plan 2015-2020
V0e Page 13 of 42
4. SUMMARY OF THE PLAN - THE PRIORITIES TO 2020 Following the completion of our local population needs assessment, the key findings have been incorporated into our local delivery plan for liver disease. This delivery plan includes actions against each of the priorities within the Welsh Government’s Liver Disease Delivery Plan (2015) and to the challenges that have arisen through our population needs analysis. We have summarised the ABUHB key priorities first, followed by the priorities as laid out in the national plan.
Aneurin Bevan University Health Board Key Priorities to 2020 1. Preventing Liver Disease: Develop an Integrated Alcohol Care Pathway
through the development of a secondary care based Alcohol Care Team (ACT) in
line with recent multi-agency reports and a NICE quality and efficiency guidance
which strongly endorse their implementation
2. Timely Detection: Build stronger links with primary care, supported by
guidelines, alerts and rapid access to specialist advice to ensure high quality of
liver care across the whole pathway
3. Fast and Effective Care: Planned expansion of the workforce providing care to
patients with liver disease which will ally with the Clinical Futures model with the
SCCC at its centre.
4. Living with Liver Disease: Support the introduction of ring-fenced liver “super”
clinics, attended by consultants, trainee doctors, specialist nurses, ANP’s and
dedicate dietetic support will be essential
5. Improving information: Set up a Gwent Liver Patient Panel and Support Group
to facilitate the co-productive approach to healthcare service redesign
6. Research: Dedicated data clerk time is essential and also supports delivery of
the whole plan. Dedicated data clerk time is essential and also supports delivery
of the whole plan, as well as research and evaluation
Priorities within the Welsh Government’s Liver Disease Delivery Plan (2015) 1) Preventing liver disease
The priorities are: 1. Work with the Public Health Wales Health Improvement Programme to ensure
appropriate effort is allocated to reducing the risk factors for liver disease and programmes reflect the potential contribution to reducing liver disease. This work should include optimisation of services and strategies for the primary prevention of liver disease, as well as increasing awareness of liver disease throughout the pathway and related pathways.
2. Take forward the legacy of the Blood Borne Virus Hepatitis Action Plan in all relevant settings and continue the effort to eradicate viral hepatitis; including working to identify and treat individuals with a diagnosis of hepatitis B or C
ABUHB Liver Disease Delivery Plan 2015-2020
V0e Page 14 of 42
infection and working with the Welsh Health Specialised Services Committee and All Wales Medicines Strategy Group on the phased introduction of new hepatitis C drugs.
3. Further develop the opportunistic assessment of alcohol intake in different settings and develop in house alcohol care teams within health boards to provide timely interventions as appropriate; including helping to take forward the systematic process for reviewing alcohol-related deaths and make recommendations about how Substance Misuse Services and Alcohol Liaison Services can better assist the management of risk factors for liver disease.
4. Examine opportunities and make costed recommendations to increase the availability of targeted community testing for viral hepatitis and fatty liver disease particularly in areas of socio-economic deprivation to address health inequity; including the community availability of non-invasive testing (NITs) for liver fibrosis among high risk populations.
5. Continue to review and monitor the content of the online over-50s health and wellbeing assessment Add to your Life in relation to risk factors for liver disease.
6. Develop an approach to help de-stigmatise liver disease.
2) Timely detection of liver disease
The priorities are: 1. Improve provision of assessment and testing of those at highest risk of
developing liver disease. 2. Improve awareness and understanding of liver disease among primary and
community care, and local government partners to help detect early liver disease and make appropriate referral.
3. Develop a nationally agreed care pathway for patients with abnormal liver function tests and develop a national audit to support this.
4. Develop a nationally agreed care pathway for the risk assessment of those incidentally found to have fatty liver disease.
5. Develop nationally agreed referral guidelines to improve consistency and quality in referral practices, manage demand and minimise inappropriate investigation of those at low risk. This will include appropriate links to guidance and related care pathways and service frameworks
6. Develop a costed proposal for identifying those at greatest risk of fatty liver disease.
7. Encourage primary care clusters/locality groups to identify a champion for liver disease who will work with the health board liver disease team to improve risk management, detection and referral practices.
8. Undertake a cost assessment of improving the effectiveness of the routine use of risk assessment tools (such as routine provision of AST/ALT ratio) to identify those at greatest risk of significant liver disease.
9. Measure performance against key standards in the developed national audit of the care pathway for the investigation and management of abnormal Liver Function Tests, across primary and secondary care.

ABUHB Liver Disease Delivery Plan 2015-2020
V0e Page 15 of 42
3) Fast and effective care
The priorities are: 1. Plan to establish a liver disease unit in each health board staffed by at least one
consultant hepatologist supported by additional consultant hepatologists or gastroenterologists with appropriate training in managing liver disease. Each unit should provide support to primary care clusters and through a hub and spoke arrangement support neighbouring hospitals to facilitate high quality inpatient care.
2. Health boards review liver disease pathways, including adoption of the BSG/BASL care bundle for decompensated cirrhosis patients, and take forward work to optimise the pathway efficiency and link to related pathways.
3. Health board liver disease units to work with WAGE to meet common standards and meet routinely to share best practice and assess performance against standards.
4. Improve access to related services such as diagnostics (particularly fibroscan and biopsy, including transjugular biopsy), dietetics and interventional radiology.
5. Implementation group to support the development of regional networks to facilitate optimal service delivery and improvement including outreach services with transplant centres.
6. Implementation group to support access to national or regional hepatocellular carcinoma Multi-Disciplinary Teams.
4) Living with liver disease
The priorities are: 1. Facilitate the strengthening of the co-productive approach to designing services
and treatment plans. 2. Consider the feasibility of developing one-stop-shop cirrhosis clinics where
patients can have their disease monitored and surveillance ultrasound scans undertaken as appropriate.
3. Examine opportunities to encourage and support better primary care management of those diagnosed with liver disease including improved uptake of appropriate vaccinations.
4. Improve access to specialist dietetic advice and psychological support, especially for patients with cirrhosis and chronic liver failure so that they can better self-manage their condition.
5. Support the provision of palliative care services for patients with chronic liver failure.
6. Encourage each health board to engage community support groups to help patients manage their condition in the community.

ABUHB Liver Disease Delivery Plan 2015-2020
V0e Page 16 of 42
5) Improving Information
The priorities are: 1. Review the quality of existing data systems for the reporting of liver-related
morbidity, mortality and associated risk factors and make recommendations for improvement.
2. Develop a clinical management system to support the care of individuals with chronic liver disease, provide measurement of health outcomes and support high quality audit and research.
3. Develop information to increase public awareness of risks factors related to these conditions in a way which is specific and relevant to each of the at risk communities; this work must have as its focus the de-stigmatisation of liver disease and its causes.
4. Develop national management guidelines facilitating the assessment of individuals with abnormal LFTs; these should include guidelines for the management of common complications of liver disease and indicators for referral.
5. Develop and implement electronic alerts for patients with abnormal liver function tests linked to national pathway guidance directing the requesting clinician to advise on further investigation and, if necessary onwards referrals to specialist services.
6. Health boards work to increase awareness of relevant educational material for staff (e.g. RCN liver disease toolkit, RCGP online resource on Hepatitis B and C: Detection, Diagnosis and Management).Increase provision of medical and nursing training in hepatology and introduce wider educational opportunities for clinicians to increase awareness of liver disease, its risk factors and symptoms.
7. To develop the delivery plan set of measures in order to understand the current situation and the size of the issue, including:
Identify existing care pathways for the investigation and management of chronically elevated LFTs and map local provision of services.
Establish the number of people diagnosed with cirrhosis in each health board.
Establish and report the waiting time measures for patients referred for outpatient specialist assessment.
Collated data on admissions related to liver disorders
Estimated number of years of life lost from liver disease in Wales.
Geographical deprivation gaps for liver disease morbidity and mortality. 6) Targeting Research
The priorities are: 1. Undertake a gap analysis and identify key pieces of research needed and work
with NISCHR to develop opportunities to address such gaps. 2. Explore the utilisation of data linkage to better understand liver disease and its
risk factors. 3. Establish a database for liver disease to facilitate all Wales research and funding;
including mechanisms for the application of research findings.

ABUHB Liver Disease Delivery Plan 2015-2020
V0e Page 17 of 42
4. Explore undertaking research into methods for improving surveillance strategies in hepatocellular carcinoma.
5. Explore undertaking research into the relationship between lifestyle choices and liver disease and how these can be tackled.
6. Assess the impact of the “Have a Word” brief intervention training programme. 7. Increase the number of joint academic appointments between health boards and
local universities. 5. PERFORMANCE MEASURES/MANAGEMENT The Welsh Government’s Liver Disease Delivery Plan (2015) contains an outline description of the national metrics that health boards and other organisations will publish:
Outcome indicators which will demonstrate success in delivering positive changes in outcome for the population of Wales.
NHS assurance measures which will quantify an organisation’s progress with implementing key areas of the delivery plan.
Indicators and assurance measures will be further developed by the All Wales Liver Disease Implementation Group. Progress with these outcome indicators will form the basis of each health board’s annual report on liver disease. They will be calculated on behalf of the NHS annually at both a national and health board population level. Health boards will produce annual progress reports starting in April 2016. Health boards will also report progress against the local delivery plan milestones to their Boards at least annually and to the public via their websites. It is expected that Local Delivery Plan and their milestones are reviewed and are updated annually from August 2015.

ABUHB Liver Disease Delivery Plan 2015-2020
V0e Page 18 of 42
Action Plan
Preventing liver disease
Priority Actions Expected outcome Risks to delivery Timescales / Milestones
Lead
Preventing harm from alcohol misuse
Ensure appropriate effort is allocated to reducing the risk factors for liver disease and programmes reflect the potential contribution to reducing liver disease.
Respond to Welsh Government’s public consultation on the draft Public Health (Minimum Price for Alcohol) Bill
Clarification of the Health Board’s position on MUP as an effective way of targeting the heaviest drinkers and other groups at risk of alcohol related harm
None Dec 2015 Aneurin Bevan Gwent Public Health Team
Ensure appropriate effort is allocated to reducing the risk factors for liver disease and programmes reflect the potential contribution to reducing liver disease.
Maximising the Health Board’s role as a Responsible Authority under the Licensing Act Review Statement of Licensing Policies for each Local Authority as appropriate. Introduce a data sharing agreement and protocol for alcohol misuse
Reduction in irresponsible sales of alcohol through effective use of licensing legislation e.g. cumulative impact areas
None Dec 2015 Dec 2015 Aug 2015
Aneurin Bevan Gwent Public Health Team Aneurin Bevan Gwent Public Health Team Aneurin Bevan Gwent Public Health Team

ABUHB Liver Disease Delivery Plan 2015-2020
V0e Page 19 of 42
Preventing liver disease
Priority Actions Expected outcome Risks to delivery Timescales / Milestones
Lead
statistics Put in place a protocol to improve the quality of alcohol misuse data collection in A&E
December 2016
A&E Department
Ensure appropriate effort is allocated to reducing the risk factors for liver disease and programmes reflect the potential contribution to reducing liver disease.
Introduce and use the Gwent Substance Misuse Area Planning Board (APB) ‘Substance Misuse Primary Prevention Best Practice Guidance’ Conduct a refresh of the Gwent APB ‘Substance Misuse Primary Prevention Best Practice Guidance’ in conjunction with partner agencies and service users Identify and introduce evidence-based alcohol
Local priorities, plans and programmes reflect the available evidence in order to delay the onset of drinking among children, challenge the norms around drinking and reduce the harm to those who do drink.
None December 2015 December 2016 September 2016
Aneurin Bevan Gwent Public Health Team Aneurin Bevan Gwent Public Health Team Aneurin Bevan Gwent Public Health Team

ABUHB Liver Disease Delivery Plan 2015-2020
V0e Page 20 of 42
Preventing liver disease
Priority Actions Expected outcome Risks to delivery Timescales / Milestones
Lead
misuse prevention programmes in schools. Develop and design an appropriate intervention to address alcohol misuse in the 50+ age group
March 2016
Aneurin Bevan Gwent Public Health Team
Further develop the opportunistic assessment of alcohol intake in different settings and develop in house alcohol care teams within health boards to provide timely interventions as appropriate
Development of an Alcohol Care Team as part of an integrated alcohol pathway Advocate for the inclusion of alcohol misuse as an Neighbourhood Care Network (NCN) priority for 2016/17
Improved quality of care for patients admitted with alcohol misuse problems and cost savings relating to length of stay and service usage Use of appropriate screening tools to identify patients with alcohol use disorders for brief intervention and appropriate referral to the Gwent Drug & Alcohol Service.
Subject to approval of business case Funding required for GPs with Special Interest (GPwSI) and to commission enhanced services
April 2016 – 3 year rolling programme September 2016
Consultant Gastroenterologist Primary Care and Networks

ABUHB Liver Disease Delivery Plan 2015-2020
V0e Page 21 of 42
Preventing liver disease
Priority Actions Expected outcome Risks to delivery Timescales / Milestones
Lead
Implement the Living Well, Living Longer programme in deprived areas Explore the potential for extending Nalemefene prescribing for harmful drinking and mildly dependant drinkers
As above. Reduce alcohol consumption in people with alcohol dependence
Capacity within primary care to provide on-going psychological support
Programme implementation ongoing 2015 - 2018 September 2016
Primary Care and Networks Primary Care and Networks
Preventing the transmission and improving the diagnosis and treatment of Blood Borne Viruses (BBVs)
Take forward the legacy of the Blood Borne Viral Hepatitis Action Plan in all relevant settings and continue the effort to eradicate viral hepatitis
Perform review of progress against BBV action plan in ABUHB
Clarity around the actions which need to be taken forward over the next 3 years
None September 2015
Aneurin Bevan Gwent Public Health Team
Take forward the legacy of the Blood Borne Viral Hepatitis
Establish baseline data to be able to monitor and evaluate future
Ability to monitor and audit actions necessary to prevent the
Dependant on continued funding for Data Clerk
January 2016 Aneurin Bevan Gwent Public Health Team

ABUHB Liver Disease Delivery Plan 2015-2020
V0e Page 22 of 42
Preventing liver disease
Priority Actions Expected outcome Risks to delivery Timescales / Milestones
Lead
Action Plan in all relevant settings and continue the effort to eradicate viral hepatitis
actions to prevent the transmission and improve the diagnosis and treatment of BBVs in all high risk groups
transmission and improve the diagnosis and treatment of BBVs in all high risk groups
Take forward the legacy of the Blood Borne Virus Hepatitis Action Plan in all relevant settings and continue the effort to eradicate viral hepatitis
Ensure effective supply of Needle Exchange services in the ABUHB area
Prevention of BBV spread in the people who inject drugs (PWID) community
Ability to meet the ongoing costs of Needle Exchange services
Stepped upgrade of service provision each year between 2015 – 2020 to establish gold standard provision
APB
Take forward the legacy of the Blood Borne Virus Hepatitis Action Plan in all relevant settings and continue the effort to eradicate viral hepatitis
Design and deliver a targeted community testing for Hep B and Hep C in Newport for those born in countries with high prevalence Promote and increase uptake of a targeted community testing for Hep B and Hep C in
Raised awareness and increase in targeted community testing for Hep B and Hep C Raised awareness and increase in targeted community testing for Hep B and Hep C
March 2016 In place and ongoing
ABGPHT/ Hepatology APB Secondary Prevention Group

ABUHB Liver Disease Delivery Plan 2015-2020
V0e Page 23 of 42
Preventing liver disease
Priority Actions Expected outcome Risks to delivery Timescales / Milestones
Lead
PWID Conduct a baseline audit of targeted community testing for Hep B and Hep C in HMP Usk and Prescoed to inform future action to ensure it is a routine part of screening Conduct an audit of targeted Hep B testing of pregnant women in high risk populations and post-exposure Hep B immunisation for babies born to infected mothers
Testing for Hep B and Hep C, and immunisation for Hep B to become routine part of screening medicals in HMP Usk and Prescoed Ensure all at risk women and babies are offered HBV testing and vaccination as appropriate
March 2016 March 2016
Primary Care & Networks / Public Health Wales / BBV Lead Maternity Services
Preventing child obesity and improving access to weight management services
Ensure appropriate effort is allocated to reducing the risk factors for liver disease and
Develop a multi-agency Child Obesity Strategy for Gwent based on the system causes of obesity
Tackle the causes of overweight and obesity in children
2014/15
ABUHB Local Authorities LSBs/PSBs

ABUHB Liver Disease Delivery Plan 2015-2020
V0e Page 24 of 42
Preventing liver disease
Priority Actions Expected outcome Risks to delivery Timescales / Milestones
Lead
programmes reflect the potential contribution to reducing liver disease.
A Gwent wide Childhood Obesity Action Plan developed and agreed by all key partners
2015/16
Agree weight management and obesity as a priority for NCN plans for 2015/16
Increase the identification of obese patients within primary care and appropriate referral to Adult Weight Management Service
September 2015
Primary Care and Networks Division
Present annual report for Adult Weight Management Service (AWMS) to Board Present business case for extension of the service
Extending AWMS to meet demand
Resources/ capacity available to meet demand
Professional Manager - Adult Weight Management Service
Introduce Child Weight Management Service
Integrated Business case developed
Approval of business case
Possible implementation by April 2016
Professional Manager - Adult Weight Management Service

ABUHB Liver Disease Delivery Plan 2015-2020
V0e Page 25 of 42
Timely detection of liver disease
Priority Actions Expected outcome Risks to delivery Timescales / Milestones
Lead
Improve provision of assessment and testing of those at highest risk of developing liver disease.
Contribute to national pathways of care and referral guidelines
Standardisation of care in line with evidence based principles
None 2016/17 Consultant Gastroenterologist
Improve awareness and understanding of liver disease among primary and community care, and local government partners to help detect early liver disease and make appropriate referral
Develop a simple referral pathway for abnormal liver function test pending national guideline publication Agree NCN lead to support introduction of new guidance for GP clusters on risk management and referral
Improvements in risk management, detection and referral
None April 2016 April 2016
Consultant Gastroenterologist Consultant Gastroenterologist /NCN lead
Undertake a cost assessment of improving the effectiveness of the
Work with clinical biochemistry to introduce AST/ALT ratio risk assessment pilot
Improvements in early detection in advanced disease and greater efficiency in testing
Capacity with Pathology
April 2016
National work taking into account the soon to be reported Scottish

ABUHB Liver Disease Delivery Plan 2015-2020
V0e Page 26 of 42
routine use of risk assessment tools (such as routine provision of AST/ALT ratio) to identify those at greatest risk of significant liver disease.
resulting in reduced cost, in line prudent healthcare principles.
experience
Develop nationally agreed referral guidelines to improve consistency and quality in referral practices, manage demand and minimise inappropriate investigation of those at low risk. This will include appropriate links to guidance and related care pathways and service frameworks
Refine the pathway for low risk patients in light of national guidance and local evidence
Improved system of appropriate ongoing monitoring and investigation to detect the possibility of disease progression in patients initially identified as low risk
None December 2017
National Implementation Group
Measure performance against key standards in the
Measure performance locally as part of the national audit of the
Ability to benchmark against national standards to ensure
None 2017/18 Consultant Gastroenterologist /NCN lead

ABUHB Liver Disease Delivery Plan 2015-2020
V0e Page 27 of 42
developed national audit of the care pathway for the investigation and management of abnormal Liver Function Tests, across primary and secondary care.
pathway
appropriate outcomes are being met.
Fast and effective care
Priority Actions Expected outcome Risks to delivery Timescales / Milestones
Lead
Plan to establish a liver disease unit in each health board staffed by at least one consultant hepatologist supported by additional consultant hepatologists or gastroenterologists with appropriate training in managing liver disease.
Implement the Clinical Future model to centralise services within the Specialist and Critical Care Centre (SCCC).
Increase in Consultant Gastroeterologists with specialist interest in Hepatology to support 7 day working and SCCC model.
Costs Challenges in recruitment
Need is immediate though implementation will be determined by ability to recruit which likely will take 2-3 years
Clinical Director Gastro/Directorate manager/Divisional Director/Clinical Futures Team
Health boards review liver disease
Continue to introduce the BSG
Improvements in the quality of care provided
None January 2016 Consultant Gastroenterologist

ABUHB Liver Disease Delivery Plan 2015-2020
V0e Page 28 of 42
pathways, including adoption of the BSG/BASL care bundle for decompensated cirrhosis patients, and take forward work to optimise the pathway efficiency and link to related pathways.
decompensated care bundle within MAU and work with Informatics to include on Clinical Work Station (CWS)
within the first 24 hours of admission.
Health board liver disease units to work with WAGE to meet common standards and meet routinely to share best practice and assess performance against standards.
Update existing ABUHB guidance and publish on intranet web pages to align with national standards Contribute to the development of national standards through the Welsh Association for Gastroenterology and Endoscopy (WAGE)
Ability to ensure that guidance reflects current best practice
None August 2016 2016/17
Consultant Gastroenterologist

ABUHB Liver Disease Delivery Plan 2015-2020
V0e Page 29 of 42
Living with liver disease
Priority Actions Expected outcome Risks to delivery Timescales / Milestones
Lead
Facilitate the strengthening of the co-productive approach to designing services and treatment plans. Engage community support groups to help patients manage their condition in the community.
Establish a liver disease patient panel with support from the British Liver Trust
Patient voice in service design and delivery
None September 2016
Consultant Gastroenterologist
Consider the feasibility of developing one-stop-shop cirrhosis clinics where patients can have their disease monitored and surveillance ultrasound scans undertaken as appropriate.
Develop a multi-disciplinary liver clinic to include consultants, doctors in training, specialist nurses and dieticians in training.
Improvements in the quality of care provided for complex patients with appropriate monitoring and advice given and improved concordance with treatment plans and dietary advice.
Subject to greater availability of dedicated dietetic sessions. Ability to recruit to vacant post following retiring consultant.
Consultant Gastroenterologist Clinical Director Gastroenterology Directorate Manager

ABUHB Liver Disease Delivery Plan 2015-2020
V0e Page 30 of 42
Improve access to specialist dietetic advice and psychological support, especially for patients with cirrhosis and chronic liver failure so that they can better self-manage their condition.
Produce a business case for dedicated dietetic support. Recruitment of dietician as part of the multi-disciplinary team
Appropriate care for decompensated cirrhosis patients.
Subject to resources being made available
Dec 2015 Clinical Director Gastroenterology
Examine opportunities to encourage and support better primary care management of those diagnosed with liver disease including improved uptake of appropriate vaccinations.
Advocate for inclusion of liver disease management and alcohol misuse as a priority within NCN plans for 2016/17, particularly within areas of deprivation
Better access to and consistency of information about the management of liver disease across the primary/ secondary care interface.
Ability to get Liver Disease onto NCN plans
2016/17 Consultant Gastroenterologist in conjunction with NCN lead for Gastroenterology and Hepatology and NCN lead for substance misuse
Support the provision of palliative care services for patients with chronic liver failure.
Formalise the existing links and information to guide appropriate referral to palliative care
Improved symptom management for patients living with liver disease
None – maximising the use of existing resources
Immediately and for review in 2016/17
Consultant Gastroenterologist

ABUHB Liver Disease Delivery Plan 2015-2020
V0e Page 31 of 42
Improving information
Priority Actions Expected outcome Risks to delivery Timescales / Milestones
Lead
Develop a clinical management system to support the care of individuals with chronic liver disease, provide measurement of health outcomes and support high quality audit and research.
Work with NWIS to review existing clinical system and improvement of clinical management systems through representation on the Implementation Board
Standardised care to limit variations in outcomes
Engagement of NWIS
2018-2020 National Implementation Group/ NWIS
Develop a local care plan for people with advanced liver disease to streamline the care they receive.
Improved patient understand of the management of advanced liver disease.
Time constraints on consultant staff
2016 Consultant Gastroenterologist
Develop national management guidelines facilitating the assessment of individuals with abnormal LFTs; these should include guidelines for the management of
See above on early detection of disease.
Standardise care, and improve information resources
2017 WAGE

ABUHB Liver Disease Delivery Plan 2015-2020
V0e Page 32 of 42
common complications of liver disease and indicators for referral.
Health boards work to increase awareness of relevant educational material for staff (e.g. RCN liver disease toolkit, RCGP online resource on Hepatitis B and C: Detection, Diagnosis and Management).Increase provision of medical and nursing training in hepatology and introduce wider educational opportunities for clinicians to increase awareness of liver disease, its risk factors and symptoms.
Continue to organise annual CPD event for nurses and allied health professionals Continue to disseminate the liver disease handbook for nurses. Work with University of South Wales to develop a Masters degree module on liver disease
Annual Ongoing 2017/18
Consultant Gastroenterologist
To develop the Develop a proposal to Clear and timely Subject to funding March 2016 Consultant
ABUHB Liver Disease Delivery Plan 2015-2020
V0e Page 33 of 42
delivery plan set of measures in order to understand the current situation and the size of the issue
expand existing data clerk capacity to extract, collate and present hospital activity data and links to Informatics for analysis
understanding of capacity gaps, support for audit and evaluation to advance service developments.
Gastroenterologist with support from Data Clerk and Informatics Department
Targeting research
Priority Actions Expected outcome Risks to delivery Timescales / Milestones
Lead
Undertake a gap analysis and identify key pieces of research needed and work with NISCHR to develop opportunities to address such gaps.
Explore the utilisation of data linkage to better understand liver disease and its risk factors.
Establish a database for liver disease to facilitate
National work needed to steer this. However local work is progressing in researching the issue of alcohol misuse and the prevalence, aetiology and outcomes of liver disease in the over 65’s Review current data capture and how this could be improved As described. ABUHB however already has a
Better understand the behaviour of liver disease in the elderly More sophisticated and specific data capture and linkage to provide incidence, outcome and develop quality metrics As described
Clinician time as there are no joint academic/clinical appointments within the department NWIS support Data support availability
2017-2018 2017-2018 2017
National Implementation Group on national issues and Consultant Gastroenterologist for all others National Implementation Group/NWIS National Implementation

ABUHB Liver Disease Delivery Plan 2015-2020
V0e Page 34 of 42
all Wales research and funding; including mechanisms for the application of research findings.
Explore undertaking research into methods for improving surveillance strategies in hepatocellular carcinoma.
Explore undertaking research into the relationship between lifestyle choices and liver disease and how these can be tackled.
Assess the impact of the “Have a Word” brief intervention training programme.
nascent liver disease database comprising 1,600 individuals that is in the process of being updated and refined This will require national work As described Measure the outcome of the training programme
Improved understanding of which patient benefits most form HCC surveillance As described Ensure return on investment and to refine the programme if necessary
Will require a large funding grant Funding Needs to become a NISCHR priority area Funding
2020+ Up to 2020 2018
Group/NWIS NISCHR, National Implementation Group PHW/NISCHR PHW

ABUHB Liver Disease Delivery Plan 2015-2020
V0e Page 35 of 42
Increase the number of joint academic appointments between health boards and local universities.
As described
Improve research output to improve patient care
Funding of research sessions for clinicans with the skills/interest
2018
National Implementation Group, Health Board to explore links with partner University
ABUHB Liver Disease Delivery Plan 2015-2020
V0e Page 36 of 42
Figure 2: Hospital admissions due to non-alcoholic fatty liver disease, 2009/10 – 2013/14
Appendix 1: Additional charts relating to the overview of local health need related to liver disease prevention and service provision
2.2 1.2 3.7 2.5 1.1 3.3 2.5
Betsi
Cadwaladr UHB
Powys tHB Hywel Dda
UHB
ABM UHB Cardiff & Vale
UHB
Cwm Taf
UHB
Aneurin
Bevan UHB
*ICD-10 code K76.0 (principal diagnosis)
95% confidence interval
Hospital admissions due to non-alcoholic fatty liver disease*, European age-
standardised rate (EASR) per 100,000, all persons all ages, Wales health boards, 2009/10-2013/14Produced by Public Health Wales Observatory, using PEDW (NWIS) and MYE (ONS)
Wales = 2.4
Source: Public Health Wales Observatory 2015, Data to support the Liver Disease Plan 2015
ABUHB Liver Disease Delivery Plan 2015-2020
V0e Page 37 of 42
Figure 9: Liver transplant procedures, 2004/05 – 2013/14
Figure 10: Endoscopic retrograde cholangiopancreatography (ERC) procedures, 2013/14
0.6 0.7 0.9 0.8 0.9 0.8 0.8
Betsi
Cadwaladr UHB
Powys tHB Hywel Dda
UHB
ABM UHB Cardiff &
Vale UHB
Cwm Taf
UHB
Aneurin
Bevan UHB
Wales = 0.8
95% confidence interval
Liver transplant procedures*, European age-standardised rate (EASR) per
100,000, persons all ages, Wales health boards, 2004/05-2013/14 Produced by Public Health Wales Observatory, using PEDW (NWIS) & MYE (ONS)
*OPCS code J01 (any mention)
Source: Public Health Wales Observatory 2015, Data to support the Liver Disease Plan 2015
26.5 33.2 24.1 51.2 75.1 54.1 45.5
Betsi
Cadwaladr UHB
Powys THB Hywel Dda
HB
ABM UHB Cardiff &
Vale UHB
Cwm Taf HB Aneurin
Bevan HB
Endoscopic retrograde cholangiopancreatography (ERC) procedures*, European
age-standardised rate (EASR) per 100,000, persons all ages, Wales health boards, 2013/14Produced by Public Health Wales Observatory, using PEDW (NWIS) & MYE (ONS)
95% confidence interval
Wales = 43.2
*OPCS code J43 (any mention)
Source: Public Health Wales Observatory 2015, Data to support the Liver Disease Plan 2015

ABUHB Liver Disease Delivery Plan 2015-2020
V0e Page 38 of 42
Figure 11: Paracetamol overdose hospital admissions, 2013/14
Figure 12: Liver disease hospital admissions, 2013/14
128.6 73.7 95.0 97.8 130.4 118.3 100.8
Betsi
Cadwaladr UHB
Powys tHB Hywel Dda
UHB
ABM UHB Cardiff &
Vale UHB
Cwm Taf
UHB
Aneurin
Bevan UHB
Hospital admissions due to paracetamol overdose*, European age-standardised rate
(EASR) per 100,000, all persons all ages, Wales health boards, 2013/14Produced by Public Health Wales Observatory, using PEDW (NWIS) & MYE (ONS)
95% confidence interval
Wales = 110.5
*Paracetamol overdose has been identified using ICD-10 codes T39.1 and either X40 (accidental poisoning) or X60 (intentional poisoning) occuring on the admitting episode of care (any diagnosis position)
Source: Public Health Wales Observatory 2015, Data to support the Liver Disease Plan 2015
94.0 62.0 84.4 87.5 89.6 118.9 91.8
Betsi
Cadwaladr UHB
Powys tHB Hywel Dda
UHB
ABM UHB Cardiff & Vale
UHB
Cwm Taf
UHB
Aneurin
Bevan UHB
Hospital admissions due to liver disease*, European age-standardised rate (EASR) per
100,000, all persons all ages, Wales health boards, 2013/14Produced by Public Health Wales Observatory, using PEDW (NWIS) & MYE (ONS)
*ICD-10 codes B15-B19, C22, I81, I85, K70-K77 & T86.4 (principal diagnosis)
Wales = 91.4
Source: Public Health Wales Observatory 2015, Data to support the Liver Disease Plan 2015
ABUHB Liver Disease Delivery Plan 2015-2020
V0e Page 39 of 42
Figure 13: Hepatitis B related end-stage liver disease/hepatocellular carcinoma hospital admissions, 2004/05 – 2013/14
Figure 14: Hepatitis C related end-stage liver disease/hepatocellular carcinoma hospital admissions, 2004/05 – 2013/14
0.8 0.7 1.1 0.6 0.8
Betsi
Cadwaladr UHB
Powys tHB** Hywel Dda
UHB
ABM UHB Cardiff & Vale
UHB
Cwm Taf
UHB**
Aneurin
Bevan UHB
* ICD-10 codes B16, B180-B181 (principal diagnosis)** Rates have been suppressed due to the low number of events
Hospital admissions due to Hepatitis B related end-stage liver disease/hepatocellular
carcinoma*, European age-standardised rate (EASR) per 100,000, all persons all ages, Wales health boards, 2004/05-2013/14Produced by Public Health Wales Observatory, using PEDW (NWIS) & MYE (ONS)
95% confidence interval
Wales = 0.8
Source: Public Health Wales Observatory 2015, Data to support the Liver Disease Plan 2015
4.2 2.7 3.4 5.9 1.3 1.3 1.5
Betsi
Cadwaladr UHB
Powys tHB Hywel Dda
UHB
ABM UHB Cardiff &
Vale UHB
Cwm Taf
UHB
Aneurin
Bevan UHB
Hospital admissions due to Hepatitis C related end-stage liver disease/hepatocellular
carcinoma*, European age-standardised rate (EASR) per 100,000, all persons all ages, Wales health boards, 2004/05-2013/14Produced by Public Health Wales Observatory, using PEDW (NWIS) & MYE (ONS)
95% confidence interval
Wales = 3.1
*ICD-10 codes B171 & B182 (principal diagnosis)
Source: Public Health Wales Observatory 2015, Data to support the Liver Disease Plan 2015

ABUHB Liver Disease Delivery Plan 2015-2020
V0e Page 40 of 42
Figure 15: Pancreatic cancer mortality, 2011-13
Figure 16: Paracetamol poisoning mortality, 2004-13
8.2 9.0 8.1 9.2 9.7 7.7 8.4
Betsi
Cadwaladr UHB
Powys tHB Hywel Dda
UHB
ABM UHB Cardiff &
Vale UHB
Cwm Taf
UHB
Aneurin
Bevan UHB
Pancreatic cancer mortality*, European age-standardised rate (EASR) per 100,000, all
persons aged under 75, Wales health boards, 2011-13Produced by Public Health Wales Observatory using PHM & MYE (ONS)
95% confidence interval
Wales = 8.6
*ICD-10 code C25 (underlying cause)
0.7 0.0 0.8 0.8 0.8 0.5
Betsi
Cadwaladr UHB
Powys tHB** Hywel Dda
UHB**
ABM UHB Cardiff & Vale
UHB
Cwm Taf UHB Aneurin
Bevan UHB
Paracetamol overdose mortality*, European age-standardised rate (EASR) per 100,000,
all persons all ages, Wales health boards, 2004-13Produced by Public Health Wales Observatory using PHM & MYE (ONS)
95% confidence interval
Wales = 0.6
*Paracetamol overdose mortality has been identified where a record contains any mention of ICD-10 codes T39.1 and either X40 (accidental poisoning) or X60 (intentional poisoning) in any cause position**Rates have been suppressed due to the low number of events
Source: Public Health Wales Observatory 2015, Data to support the Liver Disease Plan 2015
Source: Public Health Wales Observatory 2015, Data to support the Liver Disease Plan 2015

ABUHB Liver Disease Delivery Plan 2015-2020
V0e Page 41 of 42
Figure 17: Mortality from chronic liver disease, including cirrhosis, all ages, 2011-13
Figure 18: Mortality from chronic liver disease, including cirrhosis, by age group, 2004-06 to 2011-13
0
20
40
60
80
100
Betsi Cadwaladr UHB
Mortality from chronic liver disease including cirrhosis*, annual average deaths by age group, all
persons aged 20 and over, Wales health boards, 2004-06 to 2011-13
0
20
40
60
80
100
Powys tHB Hywel Dda UHB
Cardiff & Vale UHB
0
20
40
60
80
100ABM UHB
An
nu
al average d
eath
s
Produced by Public Health Wales Observatory, using PHM (ONS)
0
20
40
60
80
100
2004-0
6
2005-0
7
2006-0
8
2007-0
9
2008-1
0
2009-1
1
2010-1
2
2011-1
3
Cwm Taf UHB
2004-0
6
2005-0
7
2006-0
8
2007-0
9
2008-1
0
2009-1
1
2010-1
2
2011-1
3
Aneurin Bevan UHB
*ICD-10 codes K70, K73 & K74 (underlying cause)
0
20
40
60
80
100
120
20-74 75+
Source: Public Health Wales Observatory 2015, Data to support the Liver Disease Plan 2015
14.5 9.6 11.4 15.6 14.8 16.5 14.6
Mortality from chronic liver disease including cirrhosis*, European age-standardised
rate (EASR) per 100,000, males, females and persons all ages, Wales health boards, 2011-13Produced by Public Health Wales Observatory using PHM & MYE (ONS)
95% confidence interval
Wales = 14.3
Persons
18.0 10.8 15.3 20.3 19.3 20.6 18.2
Wales = 18.1
Males
11.0 8.6 8.1 11.4 10.5 12.6 11.3
Betsi
Cadwaladr UHB
Powys tHB Hywel Dda
UHB
ABM UHB Cardiff & Vale
UHB
Cwm Taf UHB Aneurin
Bevan UHB
Wales = 10.7
*ICD-10 codes K70, K73 & K74 (underlying cause)
Females
Source: Public Health Wales Observatory 2015, Data to support the Liver Disease Plan 2015

ABUHB Liver Disease Delivery Plan 2015-2020
V0e Page 42 of 42
Figure 19: Mortality from all cause liver disease, under 75 years, 2011-13
Figure 20: Liver cancer mortality, 2009-13
3.1 3.8 2.8 3.9 5.1 5.0 5.1
Betsi
Cadwaladr UHB
Powys tHB Hywel Dda
UHB
ABM UHB Cardiff &
Vale UHB
Cwm Taf
UHB
Aneurin
Bevan UHB
Mortality from liver cancer*, European age-standardised rate (EASR) per 100,000, all
persons aged under 75, Wales health boards, 2009-13
95% confidence interval
Wales = 4.0
*ICD-10 code C22 (underlying cause)
20.2 14.1 15.3 21.8 20.4 25.2 22.3
Mortality from all liver disease*, European age-standardised rate (EASR) per 100,000,
males, females and persons aged under 75, Wales health boards, 2011-13Produced by Public Health Wales Observatory using PHM & MYE (ONS)
95% confidence interval
Wales = 20.4
Persons
24.7 17.6 18.2 29.2 27.7 31.8 29.0
Wales = 26.1
Males
15.8 10.8 12.5 14.9 13.6 18.9 15.9
Betsi
Cadwaladr UHB
Powys tHB Hywel Dda
UHB
ABM UHB Cardiff &
Vale UHB
Cwm Taf
UHB
Aneurin
Bevan UHB
Wales = 15.0
Females
*ICD-10 codes B15-B19, C22, I81, I85, K70-K77 & T86.4 (underlying cause)
Source: Public Health Wales Observatory 2015, Data to support the Liver Disease Plan 2015
Source: Public Health Wales Observatory 2015, Data to support the Liver Disease Plan 2015


















