Absolute Ethanol Embolization of Infiltrating-diffuse ... · Absolute Ethanol Embolization of...
8
Absolute Ethanol Embolization of Infiltrating-diffuse Extracranial Arteriovenous Malformations in the Head and Neck L. Su a , D. Wang b , Y. Han b , Z. Wang b , L. Zheng b , X. Fan b,* a Department of Oral Maxillofacial and Head-Neck Oncology Surgery, Shanghai Ninth People’ s Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, PR China b Department of Interventional Radiology, Shanghai Ninth People’ s Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, PR China WHAT THIS PAPER ADDS Ethanol embolotherapy has proved to be curative for the treatment of arteriovenous malformations (AVMs). However, the sole use of absolute ethanol embolization is not suitable for all types of AVMs. This study reports a single center experience and evaluates technical and clinical safety, and effectiveness of the sole use of absolute ethanol embolization for infiltrating-diffuse extracranial AVMs in the head and neck. Objective: Extracranial arteriovenous malformations (AVMs) of an infiltrative type in the head and neck can cause cosmetic, functional, and psychological problems. This study reports a single center experience and evaluates the clinical safety and effectiveness of the sole use of absolute ethanol embolotherapy for infiltrative extracranial AVMs in the head and neck. Method: From June 2011 to June 2013, 168 consecutive patients with extracranial AVMs in the head and neck underwent staged ethanol or other methods of embolization, of whom 66 patients had infiltrating-diffuse extracranial AVMs of type III in the head and neck. Absolute ethanol embolization was solely used and retrospectively evaluated. All patients were assessed at clinical follow up (mean 16.8 months; range 12e38 months). Therapeutic outcomes were determined by evaluating the clinical outcome of symptoms and signs, as well as the degree of devascularization by follow up angiography. Results: For the 96 sessions, the mean amount of ethanol used in a single embolization session was 13.6 mL and range was from 2 to 25 mL. Fifty-six of the 66 patients were effectively controlled with 100% of the AVMs devascularized, and the remaining 10 patients had partial remission with various degrees of AVM devascularization (50e99%). Transient hemoglobinuria occurred in five of the 66 patients for a total 16 out of 96 procedures. There were no major complications. Conclusions: The sole use of ethanol embolotherapy appears to be efficacious and safe in the management of infiltrating-diffuse extracranial AVMs in the head and neck. Ó 2015 European Society for Vascular Surgery. Published by Elsevier Ltd. All rights reserved. Article history: Received 8 November 2014, Accepted 27 February 2015, Available online 16 April 2015 Keywords: Arteriovenous malformations, Embolization, Ethanol, Head and neck INTRODUCTION Arteriovenous malformations (AVMs) of the extracranial head and neck can cause tremendous cosmetic, functional, and psychological problems. Small and superficial AVMs can be cured by surgical resection; however, most AVMs are inoperable as they are large and diffuse in nature and they involve important normal adjacent structures. With im- provements in catheter technology, superselective tech- niques, and the use of liquid embolic agents, embolotherapy has emerged as the primary mode of treatment for the management of peripheral AVMs. 1e4 Ethanol embolotherapy has proved to be effective, even in complex AVMs, by a combination of the direct denuding effect on the vascular wall and clumping of damaged erythrocytes and denatured proteins, which result in com- plete and permanent obliteration of the vessel lumen. 5e7 However, the sole use of absolute ethanol embolization is not suitable for all types of AVMs. AVMs were categorized by Cho et al. 8 according to the angiographic morphology of the nidus: type I (larger arteriovenous fistulae with no more than three separate arteries shunting to the initial single venous outflow component), type II (smaller arteriovenous fistulae with multiple arterioles shunting to the initial part of a plexiform appearance into a single venous component), type IIIa (arteriovenous fistulae with non-dilated fistulae with multiple fine shunts present between arterioles and * Corresponding author. Department of Interventional Radiology, Shanghai Ninth People’ s Hospital, Shanghai Jiao Tong University School of Medicine, No. 639 Zhi Zao Ju Road, Shanghai 200011, PR China. E-mail address: [email protected] (X. Fan). 1078-5884/Ó 2015 European Society for Vascular Surgery. Published by Elsevier Ltd. All rights reserved. http://dx.doi.org/10.1016/j.ejvs.2015.02.020 Eur J Vasc Endovasc Surg (2015) 50, 114e121
Transcript of Absolute Ethanol Embolization of Infiltrating-diffuse ... · Absolute Ethanol Embolization of...

Eur J Vasc Endovasc Surg (2015) 50, 114e121
Absolute Ethanol Embolization of Infiltrating-diffuse ExtracranialArteriovenous Malformations in the Head and Neck
L. Su a, D. Wang b, Y. Han b, Z. Wang b, L. Zheng b, X. Fan b,*
a Department of Oral Maxillofacial and Head-Neck Oncology Surgery, Shanghai Ninth People’s Hospital, Shanghai Jiao Tong University School of Medicine,Shanghai, PR Chinab Department of Interventional Radiology, Shanghai Ninth People’s Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, PR China
* CorShanghMediciE-ma1078
Elseviehttp:
WHAT THIS PAPER ADDS
Ethanol embolotherapy has proved to be curative for the treatment of arteriovenous malformations (AVMs).However, the sole use of absolute ethanol embolization is not suitable for all types of AVMs. This study reports asingle center experience and evaluates technical and clinical safety, and effectiveness of the sole use of absoluteethanol embolization for infiltrating-diffuse extracranial AVMs in the head and neck.Objective: Extracranial arteriovenous malformations (AVMs) of an infiltrative type in the head and neck cancause cosmetic, functional, and psychological problems. This study reports a single center experience andevaluates the clinical safety and effectiveness of the sole use of absolute ethanol embolotherapy for infiltrativeextracranial AVMs in the head and neck.Method: From June 2011 to June 2013, 168 consecutive patients with extracranial AVMs in the head and neckunderwent staged ethanol or other methods of embolization, of whom 66 patients had infiltrating-diffuseextracranial AVMs of type III in the head and neck. Absolute ethanol embolization was solely used andretrospectively evaluated. All patients were assessed at clinical follow up (mean 16.8 months; range 12e38months). Therapeutic outcomes were determined by evaluating the clinical outcome of symptoms and signs, aswell as the degree of devascularization by follow up angiography.Results: For the 96 sessions, the mean amount of ethanol used in a single embolization session was 13.6 mL andrange was from 2 to 25 mL. Fifty-six of the 66 patients were effectively controlled with 100% of the AVMsdevascularized, and the remaining 10 patients had partial remission with various degrees of AVMdevascularization (50e99%). Transient hemoglobinuria occurred in five of the 66 patients for a total 16 out of 96procedures. There were no major complications.Conclusions: The sole use of ethanol embolotherapy appears to be efficacious and safe in the management ofinfiltrating-diffuse extracranial AVMs in the head and neck.� 2015 European Society for Vascular Surgery. Published by Elsevier Ltd. All rights reserved.Article history: Received 8 November 2014, Accepted 27 February 2015, Available online 16 April 2015Keywords: Arteriovenous malformations, Embolization, Ethanol, Head and neck
INTRODUCTION
Arteriovenous malformations (AVMs) of the extracranialhead and neck can cause tremendous cosmetic, functional,and psychological problems. Small and superficial AVMs canbe cured by surgical resection; however, most AVMs areinoperable as they are large and diffuse in nature and theyinvolve important normal adjacent structures. With im-provements in catheter technology, superselective tech-niques, and the use of liquid embolic agents,
responding author. Department of Interventional Radiology,ai Ninth People’s Hospital, Shanghai Jiao Tong University School ofne, No. 639 Zhi Zao Ju Road, Shanghai 200011, PR China.il address: [email protected] (X. Fan).-5884/� 2015 European Society for Vascular Surgery. Published byr Ltd. All rights reserved.//dx.doi.org/10.1016/j.ejvs.2015.02.020
embolotherapy has emerged as the primary mode oftreatment for the management of peripheral AVMs.1e4
Ethanol embolotherapy has proved to be effective, evenin complex AVMs, by a combination of the direct denudingeffect on the vascular wall and clumping of damagederythrocytes and denatured proteins, which result in com-plete and permanent obliteration of the vessel lumen.5e7
However, the sole use of absolute ethanol embolization isnot suitable for all types of AVMs. AVMs were categorizedby Cho et al.8 according to the angiographic morphology ofthe nidus: type I (larger arteriovenous fistulae with no morethan three separate arteries shunting to the initial singlevenous outflow component), type II (smaller arteriovenousfistulae with multiple arterioles shunting to the initial partof a plexiform appearance into a single venous component),type IIIa (arteriovenous fistulae with non-dilated fistulaewith multiple fine shunts present between arterioles and

Absolute Ethanol Embolization 115
the venous component), and type IIIb (arteriovenousfistulae with dilated fistulae with multiple shunts presentbetween arterioles and the venous component). Similarangiographic morphology was found in the head and neckin the present study, although the Cho et al. classificationfocuses mainly on the trunk and extremities. The presentwork benefits from this classification, especially for theabsolute ethanol embolization procedure. As a result of theaugmented flow with the increased volume rate of types Iand II arteriovenous fistulae, most of the ethanol wasflushed away by the circulation. Intravascular occlusion coilswithin the venous component of the nidus must be used toreduce the rate and volume of blood flow. Sole absoluteethanol embolization was not as effective as seen with typeIII AVMs. Herein, these are referred to as “infiltrating-diffuse” AVMs.
This study reports outcomes and complications seen in aseries of 66 cases of infiltrating-diffuse type III extracranialAVMs, according to the Cho et al. classification, located inthe head and neck which were solely treated with absoluteethanol embolization.
METHODS
Patients
Approval from the institutional review board of the studyhospital was obtained for a retrospective review of patients’medical and imaging records, and informed patient consentfor the study was also obtained. From June 2011 to June2013, 168 consecutive patients with extracranial AVMs inthe head and neck underwent staged ethanol embolizationor other methods of embolization, of whom 66 patientswith type III extracranial AVMs were identified by angiog-raphy and treated. The study group consisted of 66 patients(28 males, 38 females) with a mean age of 26.8 years (agerange 16e46 years) at the time of treatment. Diagnosis ofAVMs was made by the referring center on the basis ofclinical and imaging findings. Eight patients had undergoneprevious partial resection or n-Butyl cyanoacrylate emboli-zation at other hospitals before undergoing ethanolembolotherapy.
Selective and superselective angiograms were performedbefore embolization in all patients to accurately define thefeeding arteries, draining veins, and nidus of the AVM.
Angiographic and embolization techniques
All procedures were performed by two experienced inter-ventional radiologists. Sixty-six patients with 96 emboliza-tion procedures received general anesthesia after nasalintubation. Blood pressure, electrocardiogram, oxygensaturation, and end tidal carbon dioxide levels wereconstantly monitored during the procedures.
To determine the detailed angio-architecture of theAVMs, selective angiograms of the feeding artery includingfacial artery, superficial temporal artery, posterior auricularartery, or the occipital artery were performed to furtheridentify the main feeding artery. It was also necessary to
identify any abnormal extracranial and intracranial com-munications. The major compartments of the AVMs andendovascular accesses to those compartments were delin-eated. All angiograms of these AVMs showed tortuousarteriolar components of the nidus, and arteriovenousfistulae without obvious dilated outflow vein formation.
For the patients whose external carotid arteries wereligated during prior therapies, angiograms of the commoncarotid artery, the vertebral artery, and the thyrocervicaltrunk were performed on the same side of the lesions, aswell as the external carotid artery on the opposite side.
Once the feeding vessels of the lesions were identified, amicrocatheter (Powler10, Cordis Endovascular, Miami Lakes,FL, USA) was inserted into the nidus. In cases in which thesecomplex maneuvers failed, a direct puncture of the niduswas performed. The area of percutaneous puncture wasprepped and draped. A 21 gauge butterfly needle wasadvanced under the guidance of repeated contrast in-jections. Super-selective placement of the catheter tip orthe needle tip was a requirement, only then could ethanolbe injected into the nidus with sparing of all normalvascular structures. Absolute ethanol (99.7%) was used asthe embolization agent. The intention was to direct ethanoltowards the nidus itself and not towards the vascularfeeders. Repeated angiograms through the needle wereused to ensure that there was no retrograde flow ofcontrast to the proximal part of ophthalmic artery or otherfeeding arteries before ethanol injections. The contrastmedium could only be seen in the nidus and outflow vein.The goal was to embolize all or part of the nidus until thedesired clinical results were achieved. For the 96 sessions ofethanol embolization performed, a solitary transarterialapproach was used in 28 sessions, solitary direct puncturein 26 sessions, and a combination of both in 42 sessions.
The ethanol was manually injected after several test in-jections with the contrast medium to determine the pres-sure required and the amount of ethanol to inject based onthe exact flow characteristics of the AVMs. The amount ofethanol used during embolization was based on the amountof contrast medium required to fill the portion of the AVMbeing treated. Arteriography was performed 5e10 minutesafter each ethanol injection to determine whether bloodflow stasis had been achieved. Meticulous repetition of theabove described technique was required until completeembolization of at least one compartment of the AVM wasachieved. Ethanol should not be injected again when theoutflow vein disappears and the feeding artery appearsrefilled in retrograde fashion. When the direct punctureembolization was performed, if the injected contrast wasseen out of the vascular nidus and staining normal tissues,no more ethanol was injected so as to avoid any possiblenecrosis. The total amount of absolute ethanol used persession was less than 1 mL/kg of body weight.
To minimize local soft tissue swelling and accompanyingpain, all patients received an intravenous injection ofdexamethasone prior to the procedure, usually 5e10 mg,depending on their body weight. Post-operative manage-ment included an intravenous infusion of dexamethasone.

116 L. Su et al.
Further medications usually included a tapering dose ofcorticosteroids over 7 days and Zantac (Sanofi, Hangzhou,China). Any hemoglobinuria that occurred during the pro-cedure was managed by means of hydration with anintravenously administered crystalloid solution. To evaluaterenal function, serum creatinine and urea levels weremeasured at least once during the hospital stay.
In some cases with almost 100% devascularization ofabnormal arteriovenous communications as seen on an-giograms, but which still presented with some degree ofcosmetic problems left by the AVM, further operation wasnecessary to correct the contour or function.
Table 1. Demographic data of treatment, results, andcomplications in 66 patients with 99 procedures.
Parameter ValueApproachTransarterial 28 (29.2%)Direct puncture 26 (27.1%)Combined 42 (43.7%)Total 96 (100%)
No. of embolization proceduresTotal 96Mean 1.44
Amount of injected ethanol (mL)Mean (range) 13.6 (2e25)
Degree of devascularization100% 56 (84.8%)76e99% 10 (15.2%)Total 66 (100%)
Complications (SIR classification)No complication 50 (75.8%)
Evaluation of clinical data and follow up results
Follow up evaluation was obtained on the basis of physicalexamination at 3 month intervals and telephone question-naire at 1 month intervals in all patients (follow up range12e38 months; mean 16.8 months) after the initial proce-dure. Additional embolization was recommended if thesymptoms and signs remained or if the AVMs were stillpresent on follow up imaging. The results were graded on afour point scale: worse (AVMs became larger); no change(AVMs �49% resolved); improved (AVMs were 50e99%resolved); and effective control (AVMs were 100%resolved). One oral and maxillofacial surgeon and oneinterventional radiologist evaluated the clinical outcome ofsymptoms and signs by consensus. Cure was defined ascomplete resolution of the clinical symptoms and signs,with 100% devascularization of AVMs as seen on angiog-raphy. Partial remission was defined as complete resolutionor improvement of the clinical symptoms and signs, with50e99% devascularization of AVMs as seen on angiography.No remission was defined as no improvement or no changeof the clinical symptoms and signs, with less than 50%devascularization of AVMs as seen on angiography. Aggra-vation was defined as an aggravation of the clinical symp-toms and signs, regardless of the degree of AVMdevascularization as seen on angiography. Cure and partialremission were considered effective therapeutic outcomesof ethanol embolization of AVMs.
Complications were classified into major and minor ac-cording to standards reported by the Society of Interven-tional Radiology.9 Minor complications were defined asthose that required no management and resulted in noconsequences. Major complications included those thatrequired therapy or caused permanent adverse sequelae ordeath. When complications were observed, the angiogramswere reviewed again to detect the possible cause of thecomplications.
B 16 (24.2%)Follow up (mo) (range) 16.8 (12e38)
Complications: Minor Complications: A. No therapy, noconsequence, B. Nominal therapy, no consequence; includesovernight admission for observation only. Major Complications:C. Require therapy, minor, hospitalization (48 hours), D. Requiremajor therapy, unplanned increase in level of care, prolongedhospitalization (48 hours), E. Permanent adverse sequelae, F.Death.
RESULTS
Clinical outcomes
The post-operative recovery in all the patients was un-eventful. There was no significant bleeding. After the needlewas removed, manual pressure on the puncture site wasperformed for 5 minutes until there was no more oozing.
After the procedure, patients exhibited focal swelling in thearea of the AVMs, which was resolved within 1e2 weeks.
For the 96 sessions, the mean volume of ethanol usedwas 13.6 mL and ranged from 2 mL to 25 mL for a singleembolization session. Even when the maximum amount ofethanol was used, the total dose did not exceed 1 mL/kg ofbody weight. No patient experienced ethanol induced sideeffects on the liver and kidneys (measured by appropriatelab tests). Hemoglobinuria occurred in five of the 66 pa-tients for a total of 16 out of 96 sessions, which disappearedat 5e6 hours after continuous intravenous infusion; nopatient showed elevation in creatinine or urea levels.
As a therapeutic outcome of ethanol embolization, therewas an obvious reduction in redness, swelling, and warmthin all of the patients. Fifty-six of the 66 patients were curedwith 100% of AVM devascularization, with the remaining 10having partial remission with various degrees of AVMdevascularization (50e99%).
The required number of embolization procedures in pa-tients varied depending on the volume and behavior of thelesion and the adjacent tissues involved. A single emboli-zation procedure was usually sufficient to achieve cure oflocalized AVMs, but diffuse cases involving adjacent softtissue required multiple sessions. In patients who neededtwo or more procedures, the time interval between theprocedures ranged from 1 to 2 months. The amount ofethanol used and results of treatment in 66 patients aresummarized in Table 1. Thirteen of the 66 patients hadfurther operations to correct persisting deformity after theembolization.

Absolute Ethanol Embolization 117
Complications
There was no procedure related mortality. Sixteen of the 66patients had minor complications classified as B using theSIR (Society of Interventional Radiology) classification.9
Minor complications included skin blistering or superficialskin necrosis. Skin blisters, superficial skin necrosis, andpyogenic granulomas from puncture points were healedwith wound dressing, and skin grafting was not required.One case with AVMs in the chin had ethanol backflow tothe distal part of the facial artery causing superficial skinnecrosis of the buccal area and an obvious but acceptablescar (Table 1).
Case illustrations
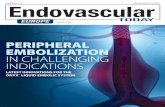
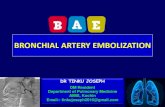
Case 1: A 26 year old male presenting with a red pulsatingmass at the left buccal region was treated successfully with5 mL absolute ethanol embolization by percutaneous directpuncture (Fig. 1). The pre-embolization angiogram demon-strated that the AVMs were supplied mainly by a tortuousfacial artery, and that these were type III (Fig. 2A). A lateralview of the vein phase of the pre-embolization angiogramshows an infiltrating-diffuse nidus of AVMs and outflowvein (Fig. 2B). Because of the tortuous facial artery, themicrocatheter failed to reach the center of the nidus of
Figure 1. Anterior lateral view (A) and anterior supine view (C) of a 28 yregion. Obvious shrinkage of AVM mass in the left buccal region was shmonth after ethanol embolization (D).
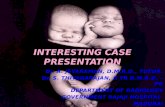
AVMs. A 21 gauge butterfly needle was used to directlypuncture the nidus. Contrast medium was injected to makesure that there was no backflow to the feeding arteriesbefore ethanol injection, and then followed by a total of5.0 mL absolute ethanol given in increments(2.0 mL þ 2.0 mL þ 1.0 mL) (Fig. 2C). Arteriography wasperformed 5 minutes after each ethanol injection todetermine whether thrombosis had occurred. Ethanolshould not be injected again when the outflow vein dis-appears and the feeding artery appears (Fig. 2D). A lateralview of the angiogram of the facial artery shows completeobliteration of AVMs and the outflow veins (Fig. 3).
Case 2: A 36 year old female presenting with an AVM inthe buccal region was treated successfully with two pro-cedures of absolute ethanol embolization(15.0 mL þ 3.0 mL) (Fig. 4A and B).
Case 3: A 22 year old male presenting with AVM at thelower lip and buccal area was treated successfully with oneprocedure of absolute ethanol embolization (8.0 mL)(Fig. 5A and B).
DISCUSSION
AVMs in the extracranial head and neck regions are rare andchallenging entities. Surgical treatment is the classic
ear old male presenting with a pulsating red mass in the left buccalown on the anterior lateral view (B) and the anterior supine view 1

Figure 2. (A) Lateral view of the pre-embolization angiogram showed AVMs mainly supplied by a tortuous facial artery (arrow). (B) Lateralview of the venous phase of the pre-embolization angiogram showed infiltrating-diffuse nidus (short arrow) of AVMs and outflow vein(long arrow). (C) Direct puncture of the nidus was performed. The area of percutaneous puncture was prepped and draped. A 21 gaugebutterfly needle was used for puncture (arrow). The contrast medium was injected through a needle to make sure that there was nobackflow of contrast to the proximal part of facial arteries before ethanol injection, followed by absolute ethanol injection three times inincrements (2.0 mL þ 2.0 mL þ 1.0 mL). (D) Arteriography through the 21 gauge butterfly needle was performed 5 minutes after eachethanol injection to determine whether thrombosis had occurred. Ethanol should not be injected again when the outflow vein disappearsand the feeding artery appears (arrow).
118 L. Su et al.
method for treating vascular malformations; either byligation of the feeding arteries or by attempted excisionafter embolization, but such procedures have not been verysuccessful.
With the development of interventional radiology,embolotherapy is playing an ever increasing role in themanagement of AVMs. There are many embolic agents foruse in various clinical scenarios, with the choice of agentdepending on several factors: the vascular territory to betreated, the type of abnormality being treated, the possi-bility of superselective delivery of an occlusive agent, thegoal of the procedure, and the permanence of the occlusionrequired. With regards to vascular malformations, perma-nent treatment is a significant issue. It has already beendocumented in the literature that embolization with ma-terials such as polyvinyl alcohol (PVA), tissue adhesives, andcoils is rarely curative and provides only temporary pallia-tion.10e13 The main reason for recanalization and neo-vascular recruitment is that none of the aforementionedembolic agents completely destroys the endothelial cells in
the nidus of the AVMs. These may sense decreased oxygentension, resulting in the release of angiogenesis factors thatstimulate neovascular formation and release of chemotacticsubstances that cause cellular infiltration contributing tothe removal of debris from the vascular channels.14 Oncethis happens recanalization occurs and previously embol-ized vessels re-endothelialize.
With the use of absolute ethanol, the endothelial cellsare denuded from the vascular wall, its protoplasm isprecipitated, and a fracture in the vascular wall at thelevel of the internal elastic lamina is formed, followed byshrinking of the lesion.9,15,16 In AVMs, these changes aredesirable and responsible for the curative effects andpermanence of ethanol embolization. This is quite impor-tant for AVMs of the face, considering the aesthetic as-pects. The judicious use of ethanol as an embolic agenthas revolutionized the ability to permanently cure theselesions in soft tissues, organs, bone, and brain asdescribed in 1994 by Coldwell, Yakes, and multiple otherauthors.17

Figure 3. Lateral view of the angiogram of the facial artery showedcomplete obliteration of AVMs and the outflow veins.
Absolute Ethanol Embolization 119
Even if ethanol, the most powerful embolizing agent, isused, sole absolute ethanol embolization cannot achievegood results in all extracranial AVMs in the head and neck.In some high flow cases with a dominant outflow vein(DOV), the injected ethanol may become diluted with bloodand may be swept away from the nidus before it causesnidus occlusion. Thus, flow occlusion techniques, includingexternal pneumatic pressure cuffs and intravascular occlu-sion balloon catheter or coil embolization of the DOV, aresometimes required to achieve effective ethanol emboli-zation of this subset of peripheral AVMs, as described byJackson, Cho, and Yakes.18e20
Angiographic classification of AVMs as described by Choet al. provides a useful classification for AVM treatment,especially for absolute ethanol embolization. Although their
Figure 4. (A) Lateral view of the venous phase of the pre-embolization aarrow) of AVMs and outflow vein (long arrow). (B) Lateral view of angand the outflow veins.
classification mainly focuses on the trunk and extremities,this classification is useful in the study of AVMs in face andneck, with similar findings on angiographic morphology.Based on this classification system, most of the AVM casesin the present study were mixed types and good resultswere obtained with ethanol embolization.
Another reason for the sole use of ethanol to embolizethe type III infiltrating-diffuse extracranial AVMs in the headand neck, is that cosmetic corrections should be considered.Most infiltrating-diffuse AVMs in this region present asfacial masses with superficial skin involvement. Obviousshrinkage of the AVM mass and cosmetic improvement canbe achieved after absolute ethanol embolization. Polymer-izing liquid agents such as nBCA and ONYX have commonlybeen used; however, they cannot cause shrinkage of theAVM’s mass like that caused by ethanol. Meanwhile, mostinfiltrating-diffuse AVMs in this region are superficial andskin is involved in the lesion. When coils lie very superfi-cially, they can erode through the overlying skin and causeulceration, and in addition, patients can feel somediscomfort because of the mass effect. In some cases ofAVMs with DOV, if coils have to be used to reduce the flowspeed and volume of DOV, extraction of these coils isrequired during the follow up period.
Complications are one of the most important issues forinterventional radiologists when treating AVMs with abso-lute ethanol, and cardiovascular collapse is the most severecomplication related to it. There was a case of cardiovas-cular collapse during ethanol embolization for a type I AVMof the upper lip, not in this group, and the patient died withDIC 2 days after cardio-pulmonary resuscitation was suc-cessfully performed. No relationship was found betweencardiovascular collapse and the dosage or method of in-jection of ethanol.21 To avoid such complications it is criticalthat the dose per kilogram and per 10 minutes is no morethan 0.14 mL/kg. This is well documented in previouspublications by Young So Do.22
ngiogram showed infiltrating-diffuse nidus in the buccal area (shortiogram of the facial artery showed complete obliteration of AVMs

Figure 5. (A) Lateral view of the venous phase of the pre-embolization angiogram showed infiltrating-diffuse nidus in the lower lip (arrow)of AVMs. (B) Lateral view of the angiogram of the facial artery showed complete obliteration of AVMs and the outflow veins.
120 L. Su et al.
Because of the comparatively low flow, ethanol emboli-zation for type III AVMs has a lower incidence of cardio-vascular collapse than for type I or type II. The maincomplication that should be considered when using ethanolto treat infiltrating-diffuse extracranial AVMs in the headand neck is local skin necrosis and ectopic embolism of anormal artery. Non-target embolization with ethanol willlead to tissue necrosis as capillary beds are entirelydestroyed. Being a fluid agent, ethanol penetrates to thecapillary level, devitalizing normal tissues. Skin blisters, su-perficial skin necrosis, and pyogenic granulomas were themost common complications in the present study, but thesehealed well with wound dressings and no scars were left.Only one case with AVMs in the chin had ethanol backflowto the distal part of the facial artery causing skin necrosis ofbuccal area and an obvious but acceptable scar.
Although ethanol is one of the strongest embolizationagents known, it must be remembered that ethanol is alsoan extremely dangerous intravascular sclerosant that cancause total tissue devitalization and neuropathy. In the faceand neck area it is important to be aware of all communi-cations that exist between the internal and external carotidartery domains.23,24 The internal carotid artery, whichsupplies the supraorbital area, nasal dorsum, and forehead,communicates with the external carotid artery along thesuborbital area and paranasal skin. These communicationsare of clinical importance, as they may open and lead tonon-target embolization of the ophthalmic artery, withpossible visual dysfunction or blindness. The backflow ofethanol from the occipital artery to the spinal artery shouldbe monitored when treating AVMs in the occipital scalpregion.
CONCLUSION
Ethanol is one of the strongest embolization agents and cancause severe complications if not properly used. The pre-sent study demonstrated that the sole use of ethanol forembolization is efficacious and safe in the management of
infiltrating-diffuse extracranial AVMs in the head and neck.Through transarterial embolization or direct punctureembolization, the nidus within the AVMs can be reachedand completely obliterated in one or more sessions by thecontrolled delivery of absolute ethanol.
CONFLICT OF INTEREST
None.
FUNDING
This research was supported by a grant from the NationalNatural Science Foundation of China, China (No. 81271681).
REFERENCES
1 Jeong HS, Baek CH, Son YI, Kim TW, Lee BB, Byun HS. Treatmentfor extracranial arteriovenous malformations of the head andneck. Acta Otolaryngol 2006;126(3):295e300.
2 Pompa V, Valentini V, Pompa G, Di Carlo S, Bresadola L.Treatment of arteriovenous malformations (AVMs) of the headand neck with embolization and surgical resection. Ann ItalChir 2011;82(4):253e9.
3 Tan KT, Simons ME, Rajan DK, Terbrugge K. Peripheral high flowarteriovenous vascular malformations: a single center experi-ence. J Vasc Interv Radiol 2004;15(10):1071e80.
4 Yakes WF, Rossi P, Odink H. How I do it. Arteriovenous mal-formation management. Cardiovasc Intervent Radiol1996;19(2):65e71.
5 Do YS, Park KB, Park HS, Cho SK, Shin SW, Moon JW, et al.Extremity arteriovenous malformations involving the bone:therapeutic outcomes of ethanol embolotherapy. J Vasc IntervRadiol 2010;21(6):807e16.
6 Hyun D, Do YS, Park KB, Kim DI, Kim YW, Park HS, et al. Ethanolembolotherapy of foot arteriovenous malformations. J VascSurg 2013;58(6):1619e26.
7 Yakes WF. Endovascular management of high flow arteriove-nous malformations. Zhonghua kou qiang yi xue za zhi ¼Zhonghua kouqiang yixue zazhi ¼ Chin J Stomatol 2008;43(6):327e32.
8 Cho SK, Do YS, Shin SW, Kim DI, Kim YW, Park KB, et al. Arte-riovenous malformations of the body and extremities: analysis

Absolute Ethanol Embolization 121
of therapeutic outcomes and approaches according to amodified angiographic classification. J Endovasc Ther2006;13(4):527e38.
9 Sacks D, McClenny TE, Cardella JF, Lewis CA. Society of Inter-ventional Radiology clinical practice guidelines. J Vasc IntervRadiol 2003;14(9 Pt 2):S199e202.
10 Aslan S, Yavuz H, Cagici AC, Kizilkilic O. Embolisation of anextensive arteriovenous malformation of the temporal regionas an alternate treatment: case report. J Laryngol Otol2008;122(7):737e40.
11 Bapuraj JR, Bilwani R, Khandelwal N, Gupta AK, Nehru VI,Suri S. Pre-operative embolization of auricular arteriovenousfistula. J Laryngol Otol 2002;116(1):42e5.
12 Hammer FD, Boon LM, Mathurin P, Vanwijck RR. Ethanol sclero-therapy of venous malformations: evaluation of systemic ethanolcontamination. J Vasc Interv Radiol 2001;12(5):595e600.
13 Lee BB, Lardeo J, Neville R. Arterio-venous malformation: howmuch do we know? Phlebology 2009;24(5):193e200.
14 Weinzweig N, Chin G, Polley J, Charbel F, Shownkeen H,Debrun G. Arteriovenous malformation of the forehead,anterior scalp, and nasal dorsum. Plast Reconstr Surg2000;105(7):2433e9.
15 Mitchell SE, Shah AM, Schwengel D. Pulmonary artery pressurechanges during ethanol embolization procedures to treatvascular malformations: can cardiovascular collapse be pre-dicted? J Vasc Interv Radiol 2006;17(2 Pt 1):253e62.
16 Vinson AM, Rohrer DG, Willcox CW, Sigfred SV, Wheeler JR,Jacobs JS, et al. Absolute ethanol embolization for peripheralarteriovenous malformation: report of two cures. South Med J1988;81(8):1052e5.
17 Coldwell DM, Stokes KR, Yakes WF. Embolotherapy: agents,clinical applications, and techniques. Radiographics 1994;14(3):623e43. quiz 645e6.
18 Cho SK, Do YS, Kim DI, Kim YW, Shin SW, Park KB, et al. Pe-ripheral arteriovenous malformations with a dominant outflowvein: results of ethanol embolization. Korean J Radiol2008;9(3):258e67.
19 Jackson JE, Mansfield AO, Allison DJ. Treatment of high flowvascular malformations by venous embolization aided by flowocclusion techniques. Cardiovasc Intervent Radiol 1996;19(5):323e8.
20 Yakes WF, Luethke JM, Merland JJ, Rak KM, Slater DD,Hollis HW, et al. Ethanol embolization of arteriovenous fis-tulas: a primary mode of therapy. J Vasc Interv Radiol1990;1(1):89e96.
21 Wang D, Su L, Fan X. Cardiovascular collapse and disseminatedintravascular coagulation as complications of ethanol emboli-zation of arteriovenous malformations in the upper lip: casereport and literature review. J Oral Maxillofac Surg 2014;72(2):346e51.
22 Do YS, Kim YW, Park KB, Kim DI, Park HS, Cho SK, et al.Endovascular treatment combined with emboloscleorotherapyfor pelvic arteriovenous malformations. J Vasc Surg 2012;55(2):465e71.
23 Volpe NJ, Sharma MC, Galetta SL, Langer DJ, Liu GT, Hurst RW,et al. Orbital drainage from cerebral arteriovenous malforma-tions. Neurosurgery 2000;46(4):820e4.
24 Warrier S, Prabhakaran VC, Valenzuela A, Sullivan TJ, Davis G,Selva D. Orbital arteriovenous malformations. Arch Ophthalmol2008;126(12):1669e75.