Absence of hMLH1 or hMSH2 Expression as a Stage-Dependent Prognostic Factor in Sporadic Colorectal...
8
ORIGINAL ARTICLE – COLORECTAL CANCER Absence of hMLH1 or hMSH2 Expression as a Stage-Dependent Prognostic Factor in Sporadic Colorectal Cancers Ji Won Park, MD 1 , Hee Jin Chang, MD 1 , Sohee Park, PhD 2 , Byung Chang Kim, MD 1 , Dae Yong Kim, MD 1 , Ji-Yeon Baek, MD 1 , Sun Young Kim, MD 1 , Jae Hwan Oh, MD 1 , Hyo Seong Choi, MD 1 , Sung Chan Park, MD 1 , and Seung-Yong Jeong, MD 3 1 Center for Colorectal Cancer, Research Institute and Hospital, National Cancer Center, Goyang, Republic of Korea; 2 Cancer Biostatistics Branch, Research Institute, National Cancer Center, Goyang, Republic of Korea; 3 Department of Surgery, Seoul National University College of Medicine, Seoul, Republic of Korea ABSTRACT Background. The predictive role of mismatch repair (MMR) status for survival after sporadic colorectal cancer remains a point of controversy. This study was designed to test the prognostic value of MMR status in sporadic colo- rectal cancers. Methods. The study included 318 patients with sporadic colorectal cancer who underwent primary tumor resection. MMR status was determined by the immunohistochemical analysis of hMLH1 and hMSH2 expression. Results. Thirty-six carcinomas (11.3%) showed abnormal MMR protein expression (22 hMLH1 negative and 14 hMSH2 negative) and were classified as MMR-defective tumors. An MMR defect was strongly associated with a reduced likelihood of lymph node (odds ratio, 0.32; 95% confidence interval [95% CI], 0.13–0.75) or distant organ metastases at diagnosis (odds ratio, 0.07; 95% CI, 0.01– 0.62), independent of the clinicopathological features. Overall survival was significantly better in patients with MMR-defective tumors than in those with MMR-intact tumors (P = 0.013). In the subgroup analysis by stage, adjusted for other potential confounding variables, MMR status was not a statistically significant prognostic factor in stage I and II patients, while the MMR defect predicted a significantly better overall survival in stage III and IV patients (adjusted hazard ratio, 0.23; 95% CI, 0.06–0.97; P = 0.045). Conclusions. At initial diagnosis, metastases were found at lower rates in MMR-defective tumors. MMR status may be a stage-dependent prognostic factor in patients with sporadic colorectal cancer. Studies conducted in the past two decades have identified two well-defined pathways for colorectal carci- nogenesis. The first and more common pathway is the suppressor pathway, involving mutations in key oncogenes and the inactivation of tumor suppressor genes (APC, p53, DCC, Samd2, and Smad4). The second is the mutator pathway, in which the inactivation of mismatch repair (MMR) genes (mainly hMLH1 and hMSH2) is involved in the development of tumors in patients with hereditary nonpolyposis colorectal cancer (HNPCC). Approximately 80% of HNPCC can be ascribed to germ line mutations in either hMLH1 or hMSH2. 1 DNA MMR deficiency is also a feature of approximately 15% of sporadic colorectal cancers. 2 Although polymerase chain reaction amplification of microsatellite repeats remains the reference method for the recognition of MMR-defective tumors, this approach is clearly not feasible in routine pathology work. Some studies have demonstrated that it is possible to identify tumors with a defective MMR system by immunochemistry and that this technique could be a useful alternative to molecular biological methods. 3,4 The biological behavior of colorectal cancers with MMR deficiency seems to differ from that of cancers with intact MMR. 5 Paradoxically, despite a high risk of metachronous disease in patients harboring germ line mutations, their prognosis seems better than that of patients with MMR-competent tumors. 6 This also seems to be a Ó Society of Surgical Oncology 2010 First Received: 17 September 2009; Published Online: 12 June 2010 H. J. Chang, MD e-mail: [email protected] Ann Surg Oncol (2010) 17:2839–2846 DOI 10.1245/s10434-010-1135-8
-
Upload
ji-won-park -
Category
Documents
-
view
213 -
download
1
Transcript of Absence of hMLH1 or hMSH2 Expression as a Stage-Dependent Prognostic Factor in Sporadic Colorectal...

ORIGINAL ARTICLE – COLORECTAL CANCER
Absence of hMLH1 or hMSH2 Expression as a Stage-DependentPrognostic Factor in Sporadic Colorectal Cancers
Ji Won Park, MD1, Hee Jin Chang, MD1, Sohee Park, PhD2, Byung Chang Kim, MD1, Dae Yong Kim, MD1,
Ji-Yeon Baek, MD1, Sun Young Kim, MD1, Jae Hwan Oh, MD1, Hyo Seong Choi, MD1, Sung Chan Park, MD1,
and Seung-Yong Jeong, MD3
1Center for Colorectal Cancer, Research Institute and Hospital, National Cancer Center, Goyang, Republic of Korea;2Cancer Biostatistics Branch, Research Institute, National Cancer Center, Goyang, Republic of Korea; 3Department of
Surgery, Seoul National University College of Medicine, Seoul, Republic of Korea
ABSTRACT
Background. The predictive role of mismatch repair
(MMR) status for survival after sporadic colorectal cancer
remains a point of controversy. This study was designed to
test the prognostic value of MMR status in sporadic colo-
rectal cancers.
Methods. The study included 318 patients with sporadic
colorectal cancer who underwent primary tumor resection.
MMR status was determined by the immunohistochemical
analysis of hMLH1 and hMSH2 expression.
Results. Thirty-six carcinomas (11.3%) showed abnormal
MMR protein expression (22 hMLH1 negative and 14
hMSH2 negative) and were classified as MMR-defective
tumors. An MMR defect was strongly associated with a
reduced likelihood of lymph node (odds ratio, 0.32; 95%
confidence interval [95% CI], 0.13–0.75) or distant organ
metastases at diagnosis (odds ratio, 0.07; 95% CI, 0.01–
0.62), independent of the clinicopathological features.
Overall survival was significantly better in patients with
MMR-defective tumors than in those with MMR-intact
tumors (P = 0.013). In the subgroup analysis by stage,
adjusted for other potential confounding variables, MMR
status was not a statistically significant prognostic factor in
stage I and II patients, while the MMR defect predicted a
significantly better overall survival in stage III and IV
patients (adjusted hazard ratio, 0.23; 95% CI, 0.06–0.97;
P = 0.045).
Conclusions. At initial diagnosis, metastases were found
at lower rates in MMR-defective tumors. MMR status may
be a stage-dependent prognostic factor in patients with
sporadic colorectal cancer.
Studies conducted in the past two decades have
identified two well-defined pathways for colorectal carci-
nogenesis. The first and more common pathway is the
suppressor pathway, involving mutations in key oncogenes
and the inactivation of tumor suppressor genes (APC, p53,
DCC, Samd2, and Smad4). The second is the mutator
pathway, in which the inactivation of mismatch repair
(MMR) genes (mainly hMLH1 and hMSH2) is involved in
the development of tumors in patients with hereditary
nonpolyposis colorectal cancer (HNPCC). Approximately
80% of HNPCC can be ascribed to germ line mutations in
either hMLH1 or hMSH2.1 DNA MMR deficiency is also a
feature of approximately 15% of sporadic colorectal
cancers.2
Although polymerase chain reaction amplification of
microsatellite repeats remains the reference method for the
recognition of MMR-defective tumors, this approach is
clearly not feasible in routine pathology work. Some
studies have demonstrated that it is possible to identify
tumors with a defective MMR system by immunochemistry
and that this technique could be a useful alternative to
molecular biological methods.3,4
The biological behavior of colorectal cancers with
MMR deficiency seems to differ from that of cancers with
intact MMR.5 Paradoxically, despite a high risk of
metachronous disease in patients harboring germ line
mutations, their prognosis seems better than that of patients
with MMR-competent tumors.6 This also seems to be a
� Society of Surgical Oncology 2010
First Received: 17 September 2009;
Published Online: 12 June 2010
H. J. Chang, MD
e-mail: [email protected]
Ann Surg Oncol (2010) 17:2839–2846
DOI 10.1245/s10434-010-1135-8

feature of sporadic colorectal cancers that are MMR
deficient.7,8
Several studies that used microsatellite instability (MSI)
tests have shown that MSI contributes to improved survival
by its association with a lower pathological stage at diag-
nosis and as a stage-for-stage predictor of a more favorable
outcome.9,10 However, there have been few studies of the
relationship between MMR status and survival in patients
with sporadic colorectal cancers. The aim of this study was
to investigate the prognostic value of MMR status.
MATERIALS AND METHODS
Study Population
Five hundred seven consecutive patients underwent
colorectal surgery for primary colorectal cancer at the
National Cancer Center, Korea, between May 2001 and
December 2003. Patients were excluded from the study if
they had received preoperative chemoradiotherapy
(n = 142), had a family history of colorectal cancer
(n = 43), or underwent transanal excision (n = 4). Patients
with family histories of colorectal cancer were defined as
patients with familial adenomatous polyposis or HNPCC,
or patients with first-degree relatives with HNPCC-asso-
ciated cancers (cancer of the colon, endometrium, small
bowel, ureter, or renal pelvis). Finally, the study included
318 patients for analysis. Our study was performed in
accordance with the Declaration of Helsinki. Informed
consent was obtained from all patients. The research pro-
tocol was approved by the institutional review board of the
National Cancer Center, Korea (NCCNCS-07-073).
Tumors were classified and staged according to the sixth
edition of the TNM Classification of the American Joint
Committee on Cancer.11 Thirty-six cases were classified as
stage I, 94 as stage II, 114 as stage III, and 74 as stage IV.
One hundred ninety-one of the patients were men (59%)
and 127 were women (41%), with a mean ± standard
deviation age of 60.5 ± 11.8 years (range, 27–87 years).
Eighty-eight tumors were located in the right colon (from
the cecum to the transverse colon) and 230 in the left colon
(from the descending colon to the rectum).
Histopathological Evaluation
Histological sections of the tumors were examined and
the following features recorded: tumor location, size, depth
of invasion, lymphatic invasion, perineural invasion, pe-
ritumoral lymphocytic infiltration, and pattern of growth at
the tumor periphery. The peritumoral lymphocytic infil-
tration was regarded as conspicuous when there was a
distinct cuff of lymphocytes at the margin of the tumor.12
The growth pattern of the tumor was recorded as ‘‘push-
ing’’ when the advancing edge of the tumor was well
defined under low-power magnification and as ‘‘infiltrat-
ing’’ when there was an irregular infiltration of tumor cells
at the advancing front.12
Assessment of MMR Status by Immunochemistry
One block of 10% formalin-fixed, paraffin-embedded
carcinoma tissue was selected from each patient. In all
cases, this block comprised an area of normal colon
mucosa adjacent to the tumor. Immunochemical staining
was performed by the Labeled Streptavidin Biotin kit
(Dako, Glostrup, Denmark). The mouse antihuman mono-
clonal antibodies used were directed against hMLH1 (clone
G168-15, diluted 1:40; BD Pharmingen, San Diego, CA)
and hMSH2 (clone FE11, diluted 1:300; Oncogene
Research Products, Boston, MA). Antigen retrieval was
performed by steam heating in 1 mM EDTA for 30 min-
utes. As a negative control, nonimmune serum was
substituted for the primary antibody. The nuclei of normal
colonic epithelial cells and lymphocytes are strongly
stained for hMLH1 and hMSH2. This was used as a
positive internal control for the staining of these proteins.
Loss of expression was recorded when nuclear staining was
completely absent in all malignant cells. Diffuse nuclear
staining of these proteins in tumor cells was interpreted as
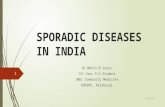
‘‘intact’’ (Fig. 1).
Treatment
The types of surgery were low anterior resection
(n = 97), anterior resection (n = 86), right hemicolectomy
(n = 82), subtotal or total colectomy (n = 18), left hemi-
colectomy (n = 12), Hartmann procedure (n = 12), and
abdominoperineal resection (n = 11). Patients with tumors
that had developed beyond stage II were considered for
adjuvant chemotherapy. Of the 318 patients, 258 (81.1%)
received adjuvant chemotherapy, which commenced
approximately 3 to 6 weeks after curative resection. Flu-
orouracil-based adjuvant chemotherapy was used as the
adjuvant chemotherapy regimen in 242 patients, and oxa-
liplatin- or irinotecan-based adjuvant chemotherapy was
used in 16 patients.
Follow-up
All patients underwent standardized follow-up, com-
prising a physical examination, complete blood count, liver
function tests, serum carcinoembryonic antigen (CEA)
tests, and chest radiographs every 3 months for the first
2 years and every 6 months thereafter, as well as
2840 J. W. Park et al.

abdominal and pelvic computed tomographic scanning
every 6 months. Colonovideoscopic examinations were
carried out 1 year after surgery, then once every 2 years.
Statistical Analysis
Statistical analysis was performed with SPSS software
(version 14.0; SPSS, Chicago, IL). The association
between the clinicopathological features and MMR status
was analyzed with Fisher’s exact test for categorical vari-
ables and with an unpaired Student’s t-test for continuous
variables. The association between MMR status and
metastasis to regional lymph nodes or distant organs was
evaluated with multivariate logistic regression including all
pathological variables. The period from the date of resec-
tion to the date of death was used for the survival analysis.
The log rank test was used to compare the Kaplan–Meier
survival curves. To test MMR status as a prognostic factor
for overall survival, we used a multivariate analysis
according to the Cox proportional hazard model. The
covariates that were statistically significant in the univari-
ate analysis were then included in the multivariate analysis.
Confounding exists between MMR status, stage of disease,
and survival outcomes. The significance of the above fac-
tors on overall survival was assessed by stratified
multivariate Cox regression analysis, with the stage at
diagnosis as the strata (stage I, II and stage III, IV). Two-
sided P values of \0.05 were considered statistically
significant.
RESULTS
Demographics and Clinicopathological Features
According to MMR Status
Of 318 patients with primary colorectal cancers, 36
(11.3%) had MMR-defective cancers (22 hMLH1 negative
and 14 hMSH2 negative). Table 1 shows the demo-
graphics and clinicopathological features of patients with
MMR-intact cancers compared with those of patients with
MMR-defective cancers. MMR-defective tumors had a
significantly lower tumor stage at the time of diagnosis
(P \ 0.001). They showed significantly lower N stages and
M stages (P = 0.007 and P = 0.002, respectively). MMR-
defective tumors developed at significantly higher fre-
quencies at proximal sites than did MMR-intact tumors
(52.8% vs. 24.5%, respectively; P \ 0.001) and tended to
be larger (mean ± standard deviation, 6.3 ± 2.3 cm vs.
5.2 ± 2.1 cm, respectively; P = 0.004). Lymphocytic
infiltration was more frequently observed in patients with
MMR-defective tumors (P \ 0.001). MMR-defective
tumors displayed infiltrative borders and lymphatic inva-
sion less frequently than did MMR-intact tumors (P =
0.009, P = 0.011, respectively).
Likelihood of Metastasis at Diagnosis
On univariate analysis, the factors related to lymph node
metastasis were MMR status, CEA, tumor invasion, tumor
FIG. 1 Immunohistochemically
detected expression of hMLH1
and hMSH2 in colorectal
adenocarcinomas. Moderately
differentiated adenocarcinoma
showing complete loss of hMLH1
expression (a) and intact hMSH2
expression (b). Poorly
differentiated adenocarcinoma
showing intact hMLH1
expression (c) and complete loss
of hMSH2 expression (d)
MMR Defect in Sporadic Colorectal Cancer 2841

grade, lymphatic invasion, lymphocytic infiltration, peri-
neural invasion, and tumor border. Multivariate logistic
analysis revealed that an MMR defect was associated with
a reduced likelihood of lymph node metastasis (odds ratio,
0.32; 95% confidence interval [95% CI], 0.13–0.75;
P = 0.009).
On univariate analysis, factors related to distant metas-
tasis were MMR status, CEA, tumor invasion, nodal status,
lymphatic invasion, lymphocytic infiltration, perineural
invasion, and tumor border. Multivariate logistic analysis
revealed that an MMR defect was strongly associated with
a reduced likelihood of distant metastasis (odds ratio, 0.07;
95% CI, 0.01–0.62; P = 0.017).
Survival Analysis
One hundred five deaths were registered among 318
patients over a median follow-up of 78 months (range, 51–
99 months). Median length of follow-up of 295 patients
with full follow-up was significantly longer than that of 23
patients with loss of follow-up (50.9 months vs.
38.3 months; P \ 0.001). By Kaplan-Meier analysis, the
overall survival of patients with MMR-defective tumors
was found to be significantly better than that of patients
with MMR-intact tumors (P = 0.013; Fig. 2). After strat-
ification by tumor stage (Fig. 3), the advantage in overall
survival for patients with MMR-defective tumors was not
maintained in stage I and II disease. In stage III and IV
disease, overall survival was significantly better in patients
with MMR-defective tumors than in those with MMR-
intact tumors (P = 0.026).
On univariate analysis, MMR status, preoperative CEA,
tumor stage, tumor grade, lymphatic invasion, perineural
invasion, lymphocytic infiltration, tumor border, and
postoperative chemotherapy were statistically significant
predictors of outcome. From the multivariable Cox pro-
portional hazard model on all patients, MMR status was not
a statistically significant predictor when the effect was
adjusted for potential confounding variables that showed
significant univariate association with overall survival
TABLE 1 Demographics and clinicopathologic features of MMR-
defective and MMR-intact tumors
Characteristic MMR intact MMR defectivea P
No. of patients 282 (88.7%) 36 (11.3%)
Age at diagnosis (y) 60.6 ± 11.7 60.3 ± 12.1 0.921
Sex 0.892
Male 169 (59.9%) 22 (61.1%)
Female 113 (40.1%) 14 (38.9%)
Tumor site \0.001
Proximal 69 (24.5%) 19 (52.8%)
Distal 213 (75.5%) 17 (47.2%)
Preoperative CEA 0.959
\5 ng/mL 197 (69.9%) 25 (69.4%)
C5 ng/mL 85 (30.1%) 11 (30.6%)
Tumor stage \0.001
I 34 (12.1%) 2 (5.6%)
II 73 (25.9%) 21 (58.3%)
III 102 (36.2%) 11 (33.3%)
IV 73 (25.9%) 1 (2.8%)
Tumor invasion 0.377
T1 12 (4.3%) 1 (2.8%)
T2 30 (10.6%) 1 (2.8%)
T3 170 (60.3%) 22 (61.1%)
T4 70 (24.8%) 12 (33.3%)
Nodal status 0.007
N0 113 (40.1%) 23 (63.9%)
N1 82 (29.1%) 10 (27.8%)
N2 87 (30.9%) 3 (8.3%)
Distant metastases 0.002
M0 219 (77.7%) 36 (100%)
M1 63 (22.3%) 0
Liver metastases 0.002
Negative 223 (78.0%) 36 (100%)
Positive 63 (22.0%) 0 (0%)
Tumor size (cm) 5.2 ± 2.1 6.3 ± 2.3 0.004
Tumor cell type 0.549
Nonmucinous 259 (91.8%) 32 (88.9%)
Mucinous 23 (8.2%) 4 (11.1%)
Tumor grade 0.299
WD/MD 246 (87.2%) 29 (80.6%)
PD 36 (12.8%) 7 (19.4%)
Lymphatic invasion 0.011
Negative 110 (39.0%) 22 (61.1%)
Positive 172 (61.0%) 14 (38.9%)
Perineural invasion 0.133
Negative 184 (65.2%) 28 (77.8%)
Positive 98 (34.8%) 8 (22.2%)
Lymphocytic infiltrationb \0.001
Negative 253 (91.0%) 23 (63.9%)
Positive 25 (9.0%) 13 (36.1%)
TABLE 1 continued
Characteristic MMR intact MMR defectivea P
Tumor border 0.009
Pushing 147 (52.1%) 27 (75.0%)
Infiltrative 135 (47.9%) 9 (25.0%)
MMR mismatch repair, CEA carcinoembryonic antigen, WD well
differentiated, MD moderately differentiated, PD poorly differenti-
ated. Data are expressed as n (%) or mean ± standard deviationa Loss of MLH1 or MSH2 expressionb Total of 314 cases available
2842 J. W. Park et al.

(adjusted hazard ratio, 0.58; 95% CI, 0.22–1.53;
P = 0.271). However, when analyzed separately by stage
at diagnosis, the MMR defect was shown to predict a
significantly better overall survival in stage III and IV
patients (adjusted hazard ratio, 0.23; 95% CI, 0.06–0.97;
P = 0.045), but this trend was not observed in stage I and
II patients (Table 2).
DISCUSSION
This study showed that 11.2% of patients with sporadic
colorectal cancers had an MMR defect, whereas the MMR
defect rate has been reported to be 9% to 20% in other
studies.2,13–15 This discrepancy in the MMR defect rate
may be attributable to the inclusion criteria or the analysis
methods used. The inclusion criteria may be an especially
important factor in explaining this discrepancy. One study,
which excluded familial adenomatous polyposis and
HNPCC, showed 20.4% MSI-positive cancers.13 Another
study, which excluded familial adenomatous polyposis,
HNPCC, and patients with first-degree relatives with can-
cers associated with HNPCC (cancer of the colon,
endometrium, small bowel, ureter, or renal pelvis), repor-
ted that 9.1% of cancers were MSI positive.14 Our study
showed a lower rate (11.3%) because we used an extended
definition of sporadic colorectal cancer, excluding patients
with cancers associated with HNPCC in first-degree rela-
tives. The analysis methods may also have affected the
detection rate of MMR-defective tumors.16 The markers
used (the five National Cancer Institute–recommended
markers, or more or fewer) and the definition of MSI-H
(30% or 40% positive, or positive for one specific marker)
may have affected MSI testing, whereas the positive cutoff
values or staining conditions, such as the antigen retrieval
method, could have affected the immunohistochemical
detection of MMR defects.17,18
Although MSI testing was not examined in this study,
most published studies have demonstrated that two anti-
bodies directed against the hMLH1 and hMSH2 proteins
allow a diagnosis of MSI with high specificity (95% to
100%) and usually with high sensitivity, although in some
studies, this sensitivity was between 70% and 80%.3,4,19–27
1.0
0.8
0.6
0.4
0.2
MMR defectMMR intactP = 0.013
Month0
36282
10
36259
20
33235
30
33220
40
33211
50
33204
60
30196
70
24161
80
1565
90
521
100
MMR defectMMR intact
Overall Survival rate
FIG. 2 Overall survival of 318 patients with sporadic colorectal
cancer according to mismatch repair (MMR) status (MMR defective
vs. MMR intact)
FIG. 3 Overall survival of patients with sporadic colorectal cancer
stratified by the stage, according to mismatch repair (MMR) status
(MMR defective vs. MMR intact). (a) stage I, II; (b) stage III, IV
MMR Defect in Sporadic Colorectal Cancer 2843

In a study combining the results of 16 series, representing
3494 cases, the immunohistochemical analysis of the MSI-
H phenotype had a sensitivity of 92.4% and a specificity of
99.6%.25 However, in purely hereditary cases, the sensi-
tivity of immunohistochemistry in predicting germ line
mutations in the MLH1 and MSH2 genes drops to 82%,
largely because of its lower sensitivity in detecting MLH1
mutations (74%). In the hereditary context, approximately
half the mutations in the MLH1 gene are missense muta-
tions, which usually result in mutant proteins that are
catalytically inactive but antigenically intact. Moreover,
even protein-truncating mutations in MLH1 can result in a
protein that reacts with the commonly used anti-MLH1
antibody.28 These observations explain the lower sensitiv-
ity of the immunohistochemical analysis in predicting germ
line mutations in MLH1. Unlike its efficacy in detecting
hereditary cancers, immunohistochemistry has an overall
sensitivity of approximately 90% and a specificity of[99%
in detecting MSI-positive colorectal tumors in patients with
sporadic colorectal cancer. Most patients ([90%) with
sporadic colorectal cancers with MMR abnormalities
acquire an MSI phenotype via the hypermethylation of the
TABLE 2 Multivariable
analysis for the prognostic
factors on overall survival,
separately by stage at diagnosis
MMR mismatch repair, CEAcarcinoembryonic antigen, WDwell differentiated, MDmoderately differentiated, PDpoorly differentiateda Oxaliplatin- or irinotecan-
based adjuvant chemotherapy
Prognostic factor No. of
patients
Hazard ratio 95% confidence
interval
P
Stage I and II
MMR status 0.573
Intact 107 1 (reference)
Defective 23 1.47 0.38–5.65
Preoperative CEA 0.018
\5 ng/mL 112 1 (reference)
C5 ng/mL 18 4.31 1.29–14.36
Lymphatic invasion 0.734
Negative 88 1 (reference)
Positive 42 1.24 0.36–4.34
Perineural invasion 0.329
Negative 109 1 (reference)
Positive 21 1.93 0.52–7.22
Stage III and IV
MMR status 0.045
Intact 175 1 (reference)
Defective 13 0.23 0.06–0.97
Preoperative CEA \0.001
\5 ng/mL 110 1 (reference)
C5 ng/Ml 78 2.75 1.72–4.39
Tumor grade 0.039
WD/MD 154 1 (reference)
PD 34 1.71 1.03–2.85
Lymphatic invasion 0.026
Negative 44 1 (reference)
Positive 144 2.17 1.10–4.28
Perineural invasion 0.186
Negative 103 1 (reference)
Positive 85 1.39 0.86–2.24
Tumor border 0.153
Pushing 85 1 (reference)
Infiltrative 103 1.45 0.87–2.41
Postoperative chemotherapy \0.001
No 22 1 (reference)
Fluorouracil-based 151 0.25 0.13–0.47
Othera 15 0.61 0.27–1.38
2844 J. W. Park et al.

promoter region of the MLH1 gene.29–31 Such a defect
usually results in the complete silencing of transcription
and the loss of protein expression. Thus, a far higher per-
centage of sporadic MSI-positive colorectal cancers show
negative MLH1 staining with immunohistochemistry. Even
if molecular MSI testing remains the current gold standard
for assessing DNA MMR competency in tumors, all these
studies confirm that the immunohistochemical detection of
hMLH1 and hMSH2 is a sensitive, rapid, and cost-effective
method, especially for sporadic colorectal cancer. For this
reason, we used immunohistochemistry as a tool for
detecting MMR deficiency.
The use of MSI in predicting the prognoses of patients
with colorectal cancer is controversial. Although several
studies have suggested better survival in patients with MSI-
H tumors, other studies could not confirm these find-
ings.8–10,32–36 MSI-positive tumors also have contradictory
prognostic features, such as poor differentiation and pe-
ritumoral lymphocytic infiltration. Only a few studies of
MMR status have been based on immunohistochemical
data as a prognostic factor. One study showed that MMR
status was an independent prognostic factor in stage II and
III disease.37 Another study demonstrated that MMR status
determined by immunohistochemistry is an independent
predictive factor of a good prognosis in T3N0M0 colon
cancer.38 However, our analysis of survival conducted in
patients with all stages of sporadic colorectal cancer sug-
gests that an MMR defect is a stage-dependent predictor of
better survival. In advanced colorectal cancer (stage III and
IV), MMR status was a statistically significant prognostic
factor, but not in stage I and II disease.
The advantage in overall survival for patients with an
MMR defect is partly dependent on the earlier stage at
which these cancers are diagnosed. These findings are
consistent with the results of a recent study conducted on a
large, single-institution series of consecutive and unse-
lected Italian patients. That study found that the lower
metastatic risk of MSI-H cancers is to be the main deter-
minant of their prognostic advantage.39 Given that patients
with MMR-defective tumors have a reduced likelihood of
metastasis at diagnosis, these findings clearly indicate that
the reduced metastatic potential of the primary tumor is the
one mechanism for the survival advantage of patients with
MMR-defective colorectal cancer. However, interestingly,
our results showed that an MMR defect predicted a sta-
tistically significantly better overall survival only in stage
III and IV disease. According to stage, MMR status had
different prognostic features. MMR status may be useful
for predicting the prognosis in advanced colorectal cancer.
Some studies also showed improved survival of MSI-H
tumors in stage III.37,40
Our study had the limitation of insufficient sample size
for definite conclusions. In the survival analysis for each
stage, only the survival curves for stage III disease seemed
to be divergent in favor of MMR-absent patients, but there
were no statistically significant differences (data not
shown). However, the estimated power did not obtain an
adequate level (41.33%). Further studies with larger sam-
ple sizes are needed to to be able to draw more definite
conclusions for each stage.
The accurate detection of lymph node and distant
metastases is critical in the analysis of the relationship
between MMR status and stage. Adequate lymph node
dissection and the meticulous pathological assessment of
lymph nodes have provided the most accurate clinico-
pathological staging of the disease. We have usually
performed a high ligation for left-colon and rectal cancers
and an extended lymph node dissection near the superior
mesenteric vessels for right-colon cancers. Entire colorec-
tal cancer specimens were examined two to three times to
obtain as many lymph nodes as possible. In our study, the
median number of collected lymph nodes was 23 (range, 7–
253). Because the imaging modalities for distant metastasis
have improved, more metastases are detected than were
detected in the 1990s. Metastases are more likely to be
undetected at the initial diagnosis among MMR-intact
patients who have a much greater likelihood of metastasis.
In conclusion, metastases were found at a lower rate in
MMR-defective tumors at initial diagnosis. MMR status
may be a stage-dependent prognostic factor in patients with
sporadic colorectal cancer.
ACKNOWLEDGMENT This study was supported by a grant from
the National Cancer Center of Korea (NCC-0910160).
REFERENCES
1. Lynch HT, de la Chapelle A. Genetic susceptibility to non-pol-
yposis colorectal cancer. J Med Genet. 1999;36:801–18.
2. Liu B, Nicolaides NC, Markowitz S, et al. Mismatch repair gene
defects in sporadic colorectal cancers with microsatellite insta-
bility. Nat Genet. 1995;9:48–55.
3. Lindor NM, Burgart LJ, Leontovich O, et al. Immunohisto-
chemistry versus microsatellite instability testing in phenotyping
colorectal tumors. J Clin Oncol. 2002;20:1043–8.
4. Thibodeau SN, French AJ, Roche PC, et al. Altered expression of
hMSH2 and hMLH1 in tumors with microsatellite instability and
genetic alterations in mismatch repair genes. Cancer Res.1996;56:4836–40.
5. Jass JR. Pathology of hereditary nonpolyposis colorectal cancer.
Ann N Y Acad Sci. 2000;910:62–73.
6. Sankila R, Aaltonen LA, Jarvinen HJ, Mecklin JP. Better survival
rates in patients with MLH1-associated hereditary colorectal
cancer. Gastroenterology. 1996;110:682–7.
7. Bubb VJ, Curtis LJ, Cunningham C, et al. Microsatellite insta-
bility and the role of hMSH2 in sporadic colorectalcancer.
Oncogene. 1996;12:2641–9.
8. Samowitz WS, Curtin K, Ma KN, et al. Microsatellite instability
in sporadic colon cancer is associated with an improved prognosis
at the population level. Cancer Epidemiol Biomarkers Prev.2001;10:917–23.
MMR Defect in Sporadic Colorectal Cancer 2845

9. Benatti P, Gafa R, Barana D, et al. Microsatellite instability and
colorectal cancer prognosis. Clin Cancer Res. 2005;11:8332–40.
10. Gryfe R, Kim H, Hsieh ET, et al. Tumor microsatellite instability
and clinical outcome in young patients with colorectal cancer. NEngl J Med. 2000;342:69–77.
11. Greene FL, Page DL, Fleming ID, et al. AJCC cancer stagingmanual. New York: Springer-Verlag, 2002.
12. Jass JR, Love SB, Northover JM. A new prognostic classification
of rectal cancer. Lancet. 1987;1:1303–6.
13. Gafa R, Maestri I, Matteuzzi M, et al. Sporadic colorectal ade-
nocarcinomas with high-frequency microsatellite instability.
Cancer. 2000;89:2025–37.
14. Jeong SY, Shin KH, Shin JH, et al. Microsatellite instability and
mutations in DNA mismatch repair genes in sporadic colorectal
cancers. Dis Colon Rectum. 2003;46:1069–77.
15. Thibodeau SN, Bren G, Schaid D. Microsatellite instability in
cancer of the proximal colon. Science. 1993;260:816–9.
16. Shia J, Ellis NA, Klimstra DS. The utility of immunohisto-
chemical detection of DNA mismatch repair gene proteins.
Virchows Arch. 2004;445:431–41.
17. Laghi L, Bianchi P, Malesci A. Differences and evolution of the
methods for the assessment of microsatellite instability. Onco-gene 2008;27:6313–21.
18. Muller W, Burgart LJ, Krause-Paulus R, et al. The reliability of
immunohistochemistry as a prescreening method for the diag-
nosis of hereditary nonpolyposis colorectal cancer (HNPCC)—
results of an international collaborative study. Fam Cancer.2001;1:87–92.
19. Cawkwell L, Gray S, Murgatroyd H, et al. Choice of management
strategy for colorectal cancer based on a diagnostic immunohis-
tochemical test for defective mismatch repair. Gut. 1999;45:409–
15.
20. Chaves P, Cruz C, Lage P, et al. Immunohistochemical detection
of mismatch repair gene proteins as a useful tool for the identi-
fication of colorectal carcinoma with the mutator phenotype. JPathol. 2000;191:355–60.
21. Dieumegard B, Grandjouan S, Sabourin JC, et al. Extensive
molecular screening for hereditary non-polyposis colorectal
cancer. Br J Cancer. 2000;82:871–80.
22. Iino H, Simms L, Young J, et al. DNA microsatellite instability
and mismatch repair protein loss in adenomas presenting in
hereditary non-polyposis colorectal cancer. Gut. 2000;47:37–42.
23. Jass JR. hMLH1 and hMSH2 immunostaining in colorectal
cancer. Gut. 2000;47:315–6.
24. Lanza G, Gafa R, Maestri I, et al. Immunohistochemical pattern
of MLH1/MSH2 expression is related to clinical and pathological
features in colorectal adenocarcinomas with microsatellite insta-
bility. Mod Pathol. 2002;15:741–9.
25. Rigau V, Sebbagh N, Olschwang S, et al. Microsatellite insta-
bility in colorectal carcinoma. The comparison of
immunohistochemistry and molecular biology suggests a role for
hMSH6 [correction of hMLH6] immunostaining. Arch PatholLab Med. 2003;127:694–700.
26. Salahshor S, Koelble K, Rubio C, Lindblom A. Microsatellite
instability and hMLH1 and hMSH2 expression analysis in
familial and sporadic colorectal cancer. Lab Invest. 2001;81:535–
41.
27. Ward R, Meagher A, Tomlinson I, et al. Microsatellite instability
and the clinicopathological features of sporadic colorectal cancer.
Gut. 2001;48:821–9.
28. Wahlberg SS, Schmeits J, Thomas G, et al. Evaluation of
microsatellite instability and immunohistochemistry for the pre-
diction of germ-line MSH2 and MLH1 mutations in hereditary
nonpolyposis colon cancer families. Cancer Res. 2002;62:3485–
92.
29. Cunningham JM, Christensen ER, Tester DJ, et al. Hyperme-
thylation of the hMLH1 promoter in colon cancer with
microsatellite instability. Cancer Res. 1998;58:3455–60.
30. Herman JG, Umar A, Polyak K, et al. Incidence and functional
consequences of hMLH1 promoter hypermethylation in colo-
rectal carcinoma. Proc Natl Acad Sci USA. 1998;95:6870–5.
31. Kane MF, Loda M, Gaida GM, et al. Methylation of the hMLH1
promoter correlates with lack of expression of hMLH1 in spo-
radic colon tumors and mismatch repair-defective human tumor
cell lines. Cancer Res. 1997;57:808–11.
32. Lim SB, Jeong SY, Lee MR, et al. Prognostic significance of
microsatellite instability in sporadic colorectal cancer. Int JColorectal Dis. 2004;19:533–7.
33. Ribic CM, Sargent DJ, Moore MJ, et al. Tumor microsatellite-
instability status as a predictor of benefit from fluorouracil-based
adjuvant chemotherapy for colon cancer. N Engl J Med.2003;349:247–57.
34. Barnetson RA, Tenesa A, Farrington SM, et al. Identification and
survival of carriers of mutations in DNA mismatch-repair genes
in colon cancer. N Engl J Med. 2006;354:2751–63.
35. Lamberti C, Lundin S, Bogdanow M, et al. Microsatellite insta-
bility did not predict individual survival of unselected patients
with colorectal cancer. Int J Colorectal Dis. 2007;22:145–52.
36. Salahshor S, Kressner U, Fischer H, et al. Microsatellite insta-
bility in sporadic colorectal cancer is not an independent
prognostic factor. Br J Cancer. 1999;81:190–3.
37. Lanza G, Gafa R, Santini A, et al. Immunohistochemical test for
MLH1 and MSH2 expression predicts clinical outcome in stage II
and III colorectal cancer patients. J Clin Oncol. 2006;24:2359–
67.
38. Parc Y, Gueroult S, Mourra N, et al. Prognostic significance of
microsatellite instability determined by immunohistochemical
staining of MSH2 and MLH1 in sporadic T3N0M0 colon cancer.
Gut. 2004;53:371–5.
39. Malesci A, Laghi L, Bianchi P, et al. Reduced likelihood of
metastases in patients with microsatellite-unstable colorectal
cancer. Clin Cancer Res. 2007;13:3831–9.
40. Wright CM, Dent OF, Barker M, et al. Prognostic significance of
extensive microsatellite instability in sporadic clinicopathological
stage C colorectal cancer. Br J Surg. 2000;87:1197–202.
2846 J. W. Park et al.