Abolarin A. T, FMCPath Lecturer/Consultant Haematologist ...
66
Abolarin A. T, FMCPath Lecturer/Consultant Haematologist, Bowen University, Iwo.
Transcript of Abolarin A. T, FMCPath Lecturer/Consultant Haematologist ...

Abolarin A. T, FMCPath
Lecturer/Consultant Haematologist,
Bowen University, Iwo.
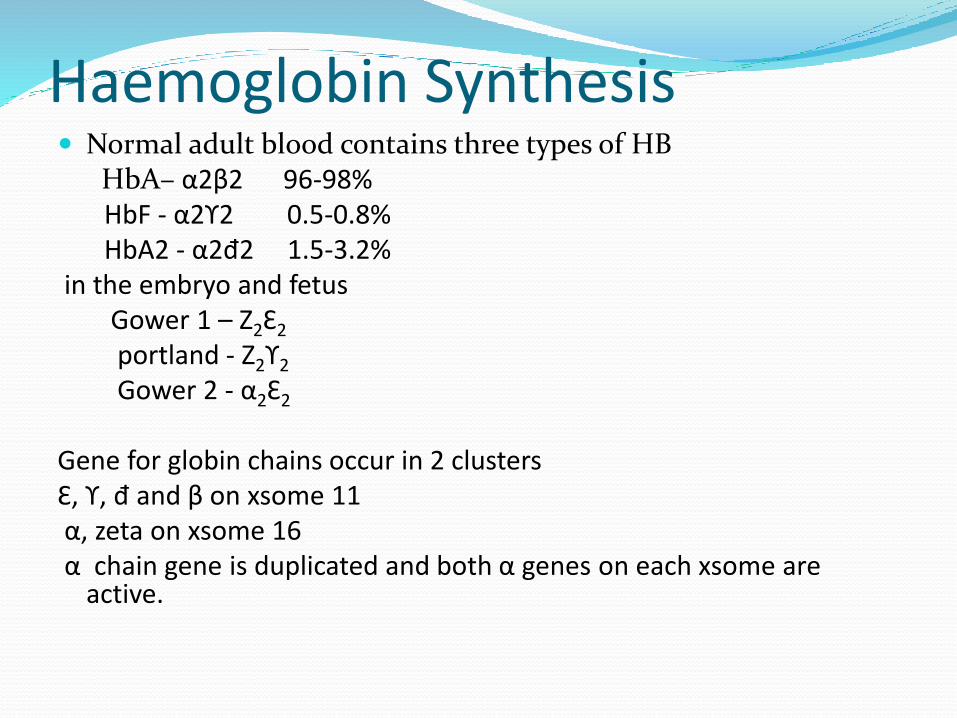
Haemoglobin Synthesis Normal adult blood contains three types of HB
HbA– α2β2 96-98%HbF - α2ϒ2 0.5-0.8% HbA2 - α2đ2 1.5-3.2%
in the embryo and fetusGower 1 – Z2Ɛ2
portland - Z2ϒ2
Gower 2 - α2Ɛ2
Gene for globin chains occur in 2 clusters Ɛ, ϒ, đ and β on xsome 11α, zeta on xsome 16α chain gene is duplicated and both α genes on each xsome are
active.

Haemoglobin Abnormalities 1. synthesis of abnormal haemoglobin(sickle cell
disorder)
2. Reduced rate of synthesis of normal α or β globinchains (α and β thalassaemias )

What is sickle cell disorder? It is a haemoglobinopathy. It is a structural
abnormality of the beta globin chain.
It is caused by a point mutation.
Inheritance is autosomal recessive


Name the abnormal red cells you see on this slide


What is the sickle cell disorder? Sickle cell disease/ disorder are a group of
haemoglobinopathies that are due to presence of the S hemoglobin and another abnormal hemoglobin – E, C , Beta thalassemia.
SCD= HbS + others
Sickle cell anaemia is the homozygous state. The inheritance of two S hemoglobin
Sickle cell trait means the inheritance of the S with a normal A

Epidemiology The commonest haemoglobinopathy in the world is S
in terms of distribution and number affected and the second is C.
Due to immigration now found in other parts of the world .
Sickle cell disease is still a disease of black Africa
25-30% have sickle cell trait AS and 2-3% are homozygous SS in Nigeria

Epidemiology Sickle cell disease is found in the and
parts of the because malaria used to be endemic in these environment.

MOLECULAR BASIS.
Sickle cell disease was the first disease to be molecularly analyzed.
The defect was localized to the beta globin chain
On the sixth amino acid.
In the normal adult HBA, in position 6 there is glutamic acid (acidic).
In Hb S, there is valine (neutral).
In Hb C there is lysine(basic)


PATHOGENESIS Hemoglobin S when
deoxygenated, then it precipitates out of solution.
This is initially reversible when normal oxygen supply is restored.
But over time the red cell becomes permanently sickled because repeated sickling destroys the red cell membrane and the sickle shape is retained even when oxygen tension is restored.

PATHOGENESIS In vivo, sickling occurs in the microcirculation where
deoxygenation occurs namely in capillaries and venules

CLINICAL PATHOLOGY
Its rigid structure makes it difficult for sickle cells to pass through the capillaries.
Therefore in the spleen, the macrophages have time to consume the sluggish red cells leading to chronic hemolysis .
There is impaired splenic function from congestion, poor blood flow, infarction and ultimately autosplenectomy.

CLINICAL PATHOLOGY The spleen normally produces complement. There is
defect in alternate pathway of complement activation in sickle cell anaemia.
Impaired opsonization of encapsulated organisms .egpneumococci and haemophilus.
Sickle cell anaemia have increased susceptibility to infections .e.g. pneumococcus , viral and malaria
Salmonella infections are increased due to availability of iron from breakdown of hemoglobin

CLINICAL PATHOLOGY There is diminished cell mediated immunity.
The irreversibly sickled erythrocytes , by occluding capillaries, lead to ischemic tissue damage thereby giving further role to inflammation.
Infarcted tissue also provides foci for infections especially in the bones and kidneys.
Hemoglobin from lysed cells bind and inactivates nitrous oxide, a potent vasodilator and inhibitor of platelet aggregation leading to undesirable vasoconstriction.

Factors affecting the rate and frequency of sickling
The amount of hemoglobin S and its interaction with other hemoglobins HBF particularly inhibits polymerization of HBS and
situations with high F is protective e.g in infants less than 6 months
Higher hemoglobin S levels in the red cell will increase the probability of aggregation and polymerization during deoxygenation
A decreased pH which decreases the hemoglobin’s affinity for oxygen will worsen sickling.
The length of time of exposure of red blood cells to low oxygen tension, in the venules and capillaries. Prolonged hypoxia worsens sickling.
How do you diagnosis sickle cell anaemia? By combining the presenting clinical features (signs
and symptoms) with laboratory investigations.

Clinical Features of sickle cell anaemiaSickle cell disease (SCD) usually manifests early in childhood. Typically after 6 months of age.
Anemia is universally present. It is chronic, hemolytic and very well tolerated. (6-7gm/dL)
Jaundice

What is wrong with this young man?

Clinical Features of sickle cell anaemia Infections are also a common first presentation in
sickle cell anaemia e.g osteomyelitis, pyelonephritis.
During childhood and adolescence, sickle cell disease is associated with growth retardation, delayed sexual maturation, and being underweight.

Crises in Sickle Cell Anaemia And Disease
The word ‘sickle cell crises’ refers to episodic, life threatening exacerbations of symptoms.
They often constitute medical emergencies and occur more commonly in sickle cell anaemia than other sickle cell diseases like Hb SC
Factors which commonly precipitate crisis are infections, extremes of temperature ,
dehydration,
rigorous exercise,
onset of menses in females etc

Crises in Sickle Cell Anaemia And Disease
The most common clinical manifestation of SCD is pain from vaso-occlusive crisis. This is the most distinguishing clinical feature of sickle cell disease.
Vasoocclusive Crises can occur in any organ.
- Manifestations of VOC include:
Dactilytis
Bone pain/ joint swelling
stroke
Acute chest syndrome
priapism
Abdominal pain

dactylitisThe hand and foot syndrome(Dactylitis) is a well
known vaso occlusive crisis in infants . The syndrome develops suddenly and lasts 1-2 weeks. Hand-foot syndrome occurs between age 6 months and 3 years; it is not seen after age 5 years because hematopoiesis in the small bones of the hands and feet ceases at this age.

Dactylitis
ACSIn young children, the acute chest syndrome a VOC
presents with
chest pain,
fever,
cough,
tachypnea,
leukocytosis, and
pulmonary infiltrates in the upper lobes.
Adults are usually afebrile and dyspneic with severe chest pain.

Stroke One of the most severe manifestation of sickle cell
anaemia patients is stroke. Stroke affects 30% of children and 11% of patients by 20 years. It is usually ischemic in children and hemorrhagic in adults.

Priapism Priapism is an unwanted, painful, and persistent erection of the
penis. Most priapism episodes begin during sleep or early in the
morning; they may be associated with physiologic dehydration and hypoventilation, which results in metabolic acidosis followed by increases in sickling and stagnation of blood within the penile sinusoids or the corpora cavernosa.
Patients with priapism have increased hemolysis within the penis, leading to a diminished availability of circulating NO, which plays an important role in erectile function.
Although priapism is usually self-limited and of relatively short duration, it is often recurrent and may become chronic.
“Stuttering” priapism refers to multiple episodes, each <4 hours in duration, which may occur several times a week and may herald a prolonged event.

Other Crises in Sickle Cell AnaemiaAnd Disease Hematologic “crises,” characterized by sudden
exaggeration of anemia, are pathogenetically unrelated to vaso-occlusive crises.
they include
- Sequestration crisis
- Aplastic crisis
- Hemolytic (hyperhemolytic crisis)
- Megaloblastic crisis

Aplastic Crisis - Aplasia is the result of direct cytotoxicity of the parvovirus to erythroid precursors, especially colony-forming units, erythroid (CFU-E).
• Because red cell survival in Hb SS is no more than 10 to 20 days cessation of erythropoiesis is followed by a rapid decrease in Hb concentration.
• The process is self-limited, within 10 days, red cell production resumes spontaneously, and large numbers of reticulocytes and nucleated erythrocytes appear in the peripheral blood.

Sequestration crisis – is characterized by sudden trapping of blood in the spleen/ liver.
A splenic sequestration crisis is defined by a decrease in the steady-state Hb concentration of at least 2
g/dl,
evidence of compensatory marrow erythropoiesis,
and an acutely enlarging spleen.
May lead to hypovolemic shock and death in a few hours.
occur in the spleen and liver commonly in children under the age of 9 years. Repeated episodes are common, until fibrosis of the spleen occurs and limits its expansion.

Hemolytic (hyperhemolytic) crises - result from a sudden acceleration of the hemolytic process
Occurs due to -
1. Concurrent mycoplasma infection
2. Coinheritance of hereditary spherocytosis
3. Drug induced hemolysis
4. Acute and delayed transfusion reactions

Megaloblastic crises - results from the sudden arrest of erythropoiesis by folate depletion.
Chronic erythroid hyperplasia imposes a drain on folate reserves, and biochemical evidence of mild folate deficiency has been demonstrated with high frequency in subjects with SCA.
Megaloblastic crises likely occurs when food consumption is interrupted by illness or alcoholism or when the folate requirement is augmented by rapid growth or pregnancy.
Clinical Features of sickle cell anaemiaPhysical findings are multisystemic
Gnathopathy
Frontal bossing
Asthenia
Shortening of fingers or toes
Pale and jaundiced

Laboratory investigationsFBC and PBF
Screening tests:
1. Sickling test
2. Solubility test
Confirmatory test:
1. Electrophoresis(alkaline and acid)
2. High performance liquid chromatography
3. Iso-electric focusing

Blood Smear Marked anisopoikilocytosis
Target cells
Poikiloctyes
Hypochromasia
Sickled RBC
Nucleated RBCs
Howell-Jolly bodies

FBC anaemia
leukocytosis – Corrected wbc count is needed due to high numbers of nucleated red cells
neutrophilia in infections
thrombocytosis may be seen, platelets usually adequate.

Comparism btw normal and sickle cell•Disc-Shaped•Deformable•Life span of 120 days
•Sickle-Shaped•Rigid •Lives for 20 days or less

Laboratory investigations 1. Sickling test: Sickling is demonstrated on a thin wet
film of blood that is sealed with a petroleum jelly/paraffin wax mixture or nail varnish/ petroleum jelly mixure. If Hb S is present, the red cells lose their smooth, round shape and become sickle.

Laboratory investigations This process takes 12 h in AS and 1 hour in SS
To hasten the process, add sodium dithionite a reducing agent.

Laboratory investigations 2. The solubility test: Hemoglobin S is insoluble in the
deoxygenated state in a high molarity phosphate buffer.
Crystals form that refract light and cause turbidity. Addition of a reducing agent like sodium dithionate will cause hemoglobin S containing blood to be turbid quickly.

Confirmatory tests Cellulose Acetate Electrophoresis
At Alkaline pH (8.4–8.6) using cellulose acetate membrane is simple, reliable and rapid. At alkaline pH, normal hemoglobin is a negatively charged protein and during electrophoresis will migrate toward the positively charged anode.
Structural variants that have a change in the charge on the surface of the molecule at alkaline pH will separate from Hb A and migrate at different speeds.

Interpretation and Comments Satisfactory separation of Hbs C, S, F, A, and J is obtained
Hbs S, D, and G migrate closely together as do Hbs C, E, and Oarab
Differentiation between these haemoglobins can be obtained by using acid agarose gels, citrate agar electrophoresis, HPLC, or IEF.


Mobilities of variants at pH 8.5 on cellulose acetate.

Confirmatory tests Citrate agar electrophoresis and acid agarose gel agar
are performed at acidic pH (6.0 – 6.2)


Confirmatory tests High performance liquid chromatography depends
on the exchange of charged groups on an exchange medium with charged groups on the hemoglobin molecule.
The surface of the support is modified by carboxyl groups to have a weakly cationic charge, which allows the separation of haemoglobin molecules with different charges by ion exchange.

Confirmatory tests When a hemolysate containing a mixture of
haemoglobin is adsorbed onto the support, the rate of separation of different haemoglobins is determined by the pH and ionic strength of any buffer applied to the column.

Confirmatory testsIso electric focusing IEF: IEF utilizes a matrix
containing carrier ampholytes of low molecular weight and varying isoelectric points . These molecules migrate to their respective isoelectric points when a current is applied, resulting in a pH.
Hemoglobin molecules migrate through the gel until they reach the point at which their individual isoelectric points is equal to the corresponding pH on the gel. The migration ceases.

Iso electric focusing

Chronic complications of sickle cell anaemia1. Pulmonary hypertension, cor-pulmonale,
2. Chronic leg ulcers,
3. Sickle cell hepatic fibrosis
4. Hepatomegaly
5. Hepatic infarcts
6. gall stones(rare).

A leg ulcer

Chronic complications of sickle cell anaemia Tropical splenomegaly syndrome in childhood,
autosplenectomy in adult
Delayed menarche, hypospermia
Bone infarction ( especially in children less than 2 years, which leads to osteomyelitis due to salmonellaand staph aureas. and aseptic necrosis of joints particularly of hip joints

Chronic complications of sickle cell anaemia The kidneys are functionally impaired in SCA giving
rise to an impaired ability to concentrate urine Hypostenuria.
Chronic pyelonephritis.
Renal papillary necrosis. It may be life threatening.
Marrow infarction can lead to embolism.
Hyperdynamic circulation can lead to cardiomegalyand finally heart failure.

Chronic complications of sickle cell anaemia Priapism: there is an intense engorgement of corporal
carvenosa leading to persistent and painful penile erections. Massive sickling with accompanied thrombosis which may lead to fibrosis. Impotence is a complication!!!
Retinopathy involving the retinal vessels which can result in blindness
Osteonecrosis

Organ changes

Management of sickle cell anaemia The 8 point agenda
I. Primary prevention of crises and complications
II. Management of vaso-occlusive crisis
III. Management of chronic pain syndromes
IV. Management of chronic hemolytic anemia
V. Prevention and treatment of infections
VI. Management of the complications and the various organ damage syndromes associated with the disease
VII. Prevention of stroke
VIII. Detection and treatment of pulmonary hypertension

Primary prevention of Crises:
Constant clinic appointments with a haematologist
Baseline test: FBC, LFT, tests of Renal Function, CXR
Pharmacology: Commence on folic acid 5 mg daily, Vitamin B12, Hydroxyurea 500mg daily
Primary Prevention of infections:
Malarial prophylaxis i.e Paludrine
Pneumococcus vaccine
Meningococcus vacine
In cold climates penicillin prophylaxis is given
Management goals for VOC Proper hydration
liberal analgesia – opioids, nsaids
identify and treat any underlying infections
antimalarial treatment
transfusion if pcv is less than steady state
Chronic transfusion therapy – with AA blood.
Hydroxyurea is of benefit in patients with recurrent VOC.

hydroxyureaHU ,
leading to S-phase arrest of replicating cells, and is used in SCD because of its ability to stimulate production of HbF.
HU increases HbF as a result of stress erythropoiesis induced by its myelosuppressive effect
hydroxyurea therapy
HU is started at a dose of 15 mg/kg per day and increased to 25 mg/kg per day provided that there are no side-effects.
HU therapy is offered to patients (adults and children over 6 years) with frequent pain episodes and acute chest syndrome

analgesics and rehydrationAdequate hydration should be provided
along with analgesia with narcotics and non-steroidal anti inflammatory agents, narcotic for oral and parenteral use and the choice of medicine depends upon local experience as well as the patients.
Pain must not be left untreated and must be eliminated….

Transfusion is not usually needed in usual anaemia or pain.
Urgent exchange is needed in:1. Acute infarctive stroke2. Severe acute chest syndrome3. Multiorgan failure syndromes4. Right upper quadrant syndrome ??5. Unresolving Priaprism6. Pregnancy7. Patients going for surgery
Blood transfusion and exchange

Haemoglobin SC Better clinical course but more of end organ
complications.
Worse thromboembolic phenomenon
Worse retinopathy
Numerous target cells seen.