Abnormal Uterine Bleedingcme.baptisthealth.net/pfs/documents/2018/presentations/sun_fink... ·...
19
6/26/2018 1 Abnormal Uterine Bleeding Randy A. Fink, MD, FACOG Obstetrics & Gynecology A simplified approach for primary care Disclosures I have no relevant disclosures pertaining to this program. Learning Objectives • Demystify and understand a simple, straightforward template to evaluate premenopausal abnormal uterine bleeding in the primary care setting. • Review up to date treatment options for heavy menstrual bleeding. Appreciate the evaluation and management of postmenopausal bleeding.
Transcript of Abnormal Uterine Bleedingcme.baptisthealth.net/pfs/documents/2018/presentations/sun_fink... ·...

6/26/2018
1
Abnormal Uterine Bleeding
Randy A. Fink, MD, FACOGObstetrics & Gynecology
A simplified approach for primary care
Disclosures
I have no relevant disclosures pertaining to this program.
Learning Objectives
• Demystify and understand a simple, straightforward template to evaluate premenopausal abnormal uterine bleeding in the primary care setting.
• Review up to date treatment options for heavy menstrual bleeding.
Appreciate the evaluation and management of postmenopausal bleeding.

6/26/2018
2
What’s In a Name?
• AUB• DUB (Dysfunctional Uterine Bleeding)• Irregular Menstruation• Metrorrhagia• Menorrhagia• Menometrorrhagia• “Hemorrhaging”• “It’s like a murder scene.”
What’s In a Code?
International Classification of Diseases, Tenth Revision (ICD-10): http://www.cdc.gov/nchs/icd/icd10.htm
Oh yeah, it’s a problem…
• One-third of visits to GYN practice1
• 11-13% of reproductive age women at any given time2
• Increasing prevalence with age to 24% by 36-40 years old.
1Kjerulff KH, Erickson BA, Langenberg PW. Am J Public Health. 1996 Feb;86(2):195-9.2Liu Z, Doan QV, Blumenthal P, et al. Value Health. 2007 May-Jun;10(3):183-94.

6/26/2018
3
Risk Factors for Endometrial Cancer
• Increasing Age (50-70yo)• Early menarche
• Late menopause (after 55yo)
• Chronic anovulation
• Diabetes• Obesity
• tamoxifen• Unopposed estrogen
• Nulliparity• Lynch Syndrome• Estrogen secreting
neoplasm
Smith RA, von Eschenbach AC, Wender R, et al. American Cancer Society guidelines for theearly detection of cancer: Update of early detection guidelines for prostate, colorectal, and endometrial cancers. CA Cancer J Clin 2001; 51:38.
PRE-MENOPAUSAL POST-MENOPAUSAL
PERI-MENOPAUSAL
PRE-MENOPAUSAL WHAT’S NORMAL??

6/26/2018
4
NORMAL MENSES
• Frequency of menses within a 24 to 38 day window• Regularity (cycle-to-cycle variation) within ± 2 to 20
days• Duration of flow from 4 to 8 days• Volume of blood loss from 5 to 80 ml
Fritz MA, Speroff L. Clinical gynecologic endocrinology and infertility. 8th ed. Philadelphia: Wolters Kluwer Health/Lippincott Williams & Wilkins; 2011.
!!!!!!!!!!!

6/26/2018
5
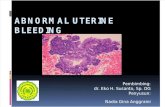
SURGICAL ANATOMY OF UTERUS
PRE-MENOPAUSAL WHAT’S NORMAL??
Pregnancy Test (“Do a Beta”)

6/26/2018
6
Beta-HCG
• Urine Pregnancy Test - within 2 weeks of conception– (20-50 mIU/mL)
• Serum Pregnancy Test (QUANTITATIVE ) – by 1 week after conception– (1-2 mIU/mL)
• False positive (rare)• False negative (more common)
Norman RJ, Menabawey M, Lowings C, Buck RH, Chard T. Obstet Gynecol. 1987 Apr;69(4):590-3.
PRE-MENOPAUSAL WHAT’S NORMAL??
Pregnancy Test (“Do a Beta”) POS �
REFER
Early Pregnancy Bleeding
• RULE-OUT ECTOPIC (2% of all pregnancies)– “Discriminatory Zone”: If Beta-HCG ≥ 2000, Intrauterine
Pregnancy is generally seen by transvaginal ultrasound1
– Normal: Beta-HCG rises by 35% in 48 hours OR doubles in 72 hours during 1st 40 days of pregnancy2
• MISCARRIAGE (15-20% of all pregnancies)– If Fetal Heart Rate is observed, 90-96% of these pregnancies
continue3
1Connolly A, Ryan DH, Stuebe AM, Wolfe HM. Obstet Gynecol. 2013;121(1):65.2Morse CB, et al. Fertil Steril. 2012 Jan;97(1):101-6.e2.3Tannirandorn Y, et al. Int J Gynaecol Obstet. 2003;81(3):263.

6/26/2018
7
PRE-MENOPAUSAL WHAT’S NORMAL??
Pregnancy Test (“Do a Beta”) POS �
REFERNeg
HORMONAL STRUCTURAL
OVULATIONAN
ANOVULATORY PATTERN
• Polycystic Ovarian Syndrome (PCOS)– Chronic Oligo or Anovulation– Clinical or Biochemical Signs of Hyperandrogenism– Polycystic Morphology by Ultrasound
Rotterdam ESHRE/ASRM-Sponsored PCOS consensus workshop group. Revised 2003 consensus on diagnostic criteria and long-term health risks related topolycystic ovary syndrome (PCOS). Hum Reprod 2004; 19:41.

6/26/2018
8
Signs of Hyperandrogenism
• Biochemical– Elevated Testosterone (<150
ng/mL)
– Elevated DHEA-S– 8am 17-OHP
– TSH, FSH, Prolactin
Signs of Hyperandrogenism
• Hirsutism– Hair growth in androgen
dependent areas:• Upper lip, chin• Midsternum• Upper and lower abdomen• Upper and lower back• Buttocks
• Differs from – “Unwanted Hair”– Hypertrichosis Madnani N et al. Indian J Dermatol Venereol Leprol 2013;79:310-21
Ferriman-Gallway Hirsutism Scoring
• Score 1-7: Focal (common normal variant)
• Score ≥8: Generalized
• Norms lower in Asians, higher in Mediterraneans
Hatch R, Rosenfield RS, Kim MH, Tredway D. Hirsutism: implications, etiology,and management. Am J Obstet Gynecol 1981; 140:815.

6/26/2018
9
Signs of Hyperandrogenism
• Hirsutism with Acanthosis Nigricans– Insulin resistance
Madnani N et al. Indian J Dermatol Venereol Leprol 2013;79:310-21
Signs of Hyperandrogenism
• Acne Vulgaris– Minimally responsive to
traditional treatment
– Lower half of face and jawline
– Back, chest– Rapid recurrence on cessation
of treatment
– Persist beyond typical 5-7 days
Archer JS, Chang RJ. Hirsutism and acne in polycystic ovary syndrome. Best Pract Res Clin Obstet Gynaecol 2004;18:737-54.
Signs of Hyperandrogenism
• Androgenic Alopecia– May be difficult to distinguish
from other patterns of hair loss in women
Olsen EA. Female pattern hair loss. J Am Acad Dermatol 2001;45:70-80.

6/26/2018
10
ANOVULATORY PATTERN
• Common Clinical Presentation– 33yo nulligravid, BMI 30, states not sexually active.
• c/o vaginal bleeding daily for the past 24 days• LNMP 3 months prior, no bleeding since until this episode
• Hormone Dysfunction: Estrogen Dominance– Progesterone Challenge
• Medroxyprogesterone acetate 10mg PO BID x 5 days or 1 PO QD x 10 days
• Norethindrone acetate 10mg PO QD x 5 days
Deeper Issues
• Prolactinoma• Thyroid abnormalities• Premature Ovarian Insufficiency• Coagulopathy/Bleeding Diathesis
TSH, FSH, PROLACTIN

6/26/2018
11
PRE-MENOPAUSAL WHAT’S NORMAL??
Pregnancy Test (“Do a Beta”) ➕ � REFER
Neg
HORMONAL STRUCTURAL• Cervical• Fibroids• Polyps• Adenomyosis
Is it Uterine Bleeding? Remember Cervix!
• Cervical Dysplasia– Is Pap up to date? If not, DO IT!
• Cervicitis– Friable cervix– Purulent discharge
– Pelvic tenderness

6/26/2018
12
Fibroids
• Most common pelvic tumor in women1
• Prevalence as high as 77%
• Clinically significant (4cm, 9 weeks size, Submucosal) by u/s2
– 50% of Black Women
– 35% White Women1Baird DD, Dunson DB, Hill MC, Cousins D, Schectman JM. Am J Obstet Gynecol. 2003;188(1):100.2Marshall LM, et al. Obstet Gynecol. 1997;90(6):967.
Fibroids
• Heavy or prolonged menstrual bleeding• Bulk-related symptoms, such as pelvic pressure and
pain
• Reproductive dysfunction (i.e., infertility or obstetric complications)

6/26/2018
13
Endometrial Polyps
• Common source of perimenopausal and postmenopausal bleeding
• Receptor issue• Saline sonography• Can be stimulated by estrogen therapy, tamoxifen,
endogenous estrogen• 95% are benign
Baiocchi G., et al. Am J Obstet Gynecol. 2009;201(5):462.e1.

6/26/2018
14
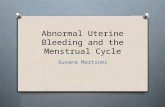
Adenomyosis
Adenomyosis
• Common cause of pelvic pain, dysmenorrhea, abnormal uterine bleeding
• Globular uterus• Asymetric endometrial growth• Heterogeneous echotexture• Diffuse or confined (Adenomyoma)
Templeman C, et al. Fertil Steril. 2008;90(2):415. Epub 2007 Oct 24.

6/26/2018
15
Treatment Options - HMB
• NSAID• Hormonal Contraceptives
• Tranexamic Acid 650mg, 2 tabs PO TID starting at onset of menses, not to exceed 5 days use
• LNG IUD
• Endometrial Ablation
PRE-MENOPAUSAL POST-MENOPAUSAL
Post-Menopausal Bleeding
• IS IT UTERINE?– Cervical– Vaginal Atrophy– Urethral– Rectal
• IS IT MEDICAL?– HRT– Anti-coagulants

6/26/2018
16
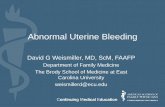
TRANS-VAGINAL ULTRASOUND
4 mm

6/26/2018
17
4mm Endometrial Stripe
• Essentially rules out endometrial cancer• >4mm suggestive of proliferative process
– Filling defect (polyp, fibroid)– PMP proliferative endometrium– Endometrial hyperplasia
– Endometrial cancer
Sladkevicius P, Opolskiene G, Valentin L. Ultrasound Obstet Gynecol. 2017;49(5):649. Epub 2017 Apr 6.

6/26/2018
18
PRE-MENOPAUSAL POST-MENOPAUSAL
ULTRASOUND
4 mm or less >4mm
REFERProbably Refer
The Take Home:A simplified approach for primary care.
PRE-MENOPAUSAL POST-MENOPAUSAL
ULTRASOUND
4 mm or less >4mm
REFERProbably Refer
Is it NORMAL?
Pregnancy Test (“Do a Beta”) POS � REFER
NEG
HORMONAL STRUCTURAL
• Relatedto Ovulation
• Cervical• Fibroids• Polyps• Adenomyosis

6/26/2018
19
Randy A. Fink, MD, FACOGOffice Contact: 305-515-5425