
Abnormal immune response Hypersensitivity & Autoimmunity · Abnormal immune response...
64
Abnormal immune response Hypersensitivity & Autoimmunity Lecture 7 Pathology and Clinical Science 1 (BIOC211) Department of Bioscience Text Reference: Grossman, S.C. & Porth, C.M. (2014). Porth’s Pathophysiology: concepts of altered health states, (9th ed.). Philadelphia, U.S.A. Walters Kluwer Health - Lippincott, Williams & Wilkins. © endeavour.edu.au
Transcript of Abnormal immune response Hypersensitivity & Autoimmunity · Abnormal immune response...

Abnormal immune response
Hypersensitivity & Autoimmunity
Lecture 7
Pathology and Clinical
Science 1 (BIOC211)
Department of BioscienceText Reference:
Grossman, S.C. & Porth, C.M. (2014). Porth’s Pathophysiology: concepts of
altered health states, (9th ed.). Philadelphia, U.S.A. Walters Kluwer Health -
Lippincott, Williams & Wilkins.
© endeavour.edu.au

© Endeavour College of Natural Health endeavour.edu.au 2
Session Learning Outcomes:
This session aims to understand and describe
o The mechanism of hypersensitivity
o Understand the difference between type I to IV
hypersensitivity
o Auto-immunity
o The inflammatory pathway that occurs in
autoimmunity
o The immunodeficiency

© Endeavour College of Natural Health endeavour.edu.au 3
REVISION - THE NORMAL
IMMUNE RESPONSE• The immune system is organised into lines of
defence to protect the body from microbial invasion
First
(non specific)
Physical and chemical defences (skin and mucous membranes)
Second
(non specific)
Complement, neutrophils, macrophages, inflammation, fever
Third
(specific)
Antibodies – B-cells
Cell Mediated – T-cells

© Endeavour College of Natural Health endeavour.edu.au 4
THE NORMAL IMMUNE RESPONSE:
SPECIFIC IMMUNITY
Antibody Immunity:
• Primary responses
– IgM
• Secondary responses
– IgG and/or IgA
• Specific antigens will
stimulate
– IgE (parasites in
particular)
Cellular Immunity:
• Killer T cells:
– lyse infected body
cells

© Endeavour College of Natural Health endeavour.edu.au 5
TYPES OF IMMUNITY THAT DEVELOPS UPON
ENCOUNTER WITH VARIOUS TYPES OF ANTIGENS

© Endeavour College of Natural Health endeavour.edu.au 6
ABNORMAL IMMUNE
RESPONSES• The immune system can responds in an abnormal way
such that the response elicited may be
– Unnecessary
– Excessive
• Normal immune reactions will cause some damage to the body which is necessary to rid the body of a greater threat (unchecked infection-fatal)
– Normal immunity causes damage but has long term benefit
• Abnormal immunity causes damage with no benefit to the body
• Hypersensitivity is an abnormal immune response

© Endeavour College of Natural Health endeavour.edu.au 7
WHAT IS HYPERSENSITIVITY
• Unusual and often damaging immune responses to normally harmless substances
• There are four basic types of hypersensitivity reactions
– Type I, II, III, IV
• These differ in ways in which they cause tissue injury

© Endeavour College of Natural Health endeavour.edu.au 8
TYPE I HYPERSENSITIVITY
(ALLERGY AND ANAPHYLAXIS)
• Allergy is a type I hypersensitivity reaction
– A local reaction
• Anaphylaxis is a type I hypersensitivity
reaction
– Added to local effects, there are
extreme severe systemic effects

© Endeavour College of Natural Health endeavour.edu.au 9
TYPE I HYPERSENSITIVITY
(ALLERGY)• Also known as immediate hypersensitivity reaction
• Occurs within 5-10 minutes of exposure to a specific
allergen
• Must be previously sensitised to the allergen
• Predisposed genetic tendency (atopic) for IgE production
to variable allergens (normally harmless in others)
• The specific allergen can be:
– Food – nuts, shellfish, strawberries
– Chemicals
– Drugs – Aspirin, penicillin, local anaesthetics
– Pollen

© Endeavour College of Natural Health endeavour.edu.au 10
MECHANISM OF TYPE I
HYPERSENSITIVITY REACTIONS
Un-needed immune response involving the
development of IgE antibodies
• Primary exposure(s) to the allergen
- IgE produced and sensitises mast cells and
basophils
• Secondary (re)exposure to the allergen
stimulates sensitised mast cells
- Degranulation and histamine release (phase l)

© Endeavour College of Natural Health endeavour.edu.au 11
Mechanism of
Type I
Hypersensitivity
Reactions
From Porth’s Pathophysiology: concepts of altered health states, (9th ed., p. 342), by Grossman, S.C. & Porth, C.M. (2014), Philadelphia, U.S.A. Walters Kluwer Health - Lippincott, Williams & Wilkins.
© Endeavour College of Natural Health endeavour.edu.au 12
MECHANISM OF TYPE I
HYPERSENSITIVITY REACTIONS• Vasodilation and vascular leakage
• Results in itching and mild pain
• Duration 5-30 mins induction of the inflammatory
response (phase ll)
• Prostaglandins and leukotrienes
• Increased vasodilation, increased permeability, tissue
destruction
• Increased inflammation and clinical features
• Duration starts 2-8 hours post exposure – can last for
several days
• Induction of bronchoconstriction if in the lungs (asthma)

© Endeavour College of Natural Health endeavour.edu.au 13
TYPE I HYPERSENSITIVITY
REACTIONS
• Skin rashes
• Extrinsic asthma (wet asthma)
• Eczema (some forms)
• Hay fever (allergic rhinitis)
• Allergic conjunctivitis
• Vomiting (food allergies)
• Anaphylaxis

© Endeavour College of Natural Health endeavour.edu.au 14
HYPERSENSITIVITY REACTIONS
http://www.dermnet.com/dn2/allJPGThumb3/eczema-acute-1.jpg
Eczema Allergic Conjunctivitis
Anaphylaxis - Drug ReactionContact Dermatitis
© Endeavour College of Natural Health endeavour.edu.au 15
TYPE I HYPERSENSITIVITY
• Clinical Features of second exposure
– pruritus (itchy)
– vesicles (blisters)
– redness
– Swelling
• Testing for Type I
– Skin prick testing
• Weal and flare reaction in response to pricking
skin with allergen solution
– Measuring specific IgE in serum
© Endeavour College of Natural Health endeavour.edu.au 16
SKIN-PRICK TESTINGThe skin prick test introduces a tiny amount of allergen into the skin. These
tests can be carried out on all age groups, including babies, although the
response will be considerably smaller than in an adult.
o Skin testing is usually carried out on the inner forearm or larger areas on the
back.
o The test allergens are selected in accordance with the patient’s history
o As few as 3 or 4 or up to about 25 allergens can be tested
o The prick area is coded with a marker pen for the allergens to be tested
o A drop of the allergen (extract) solution is placed by the relevant name or
number
o The skin is then pricked through the drop using the tip of a lancet – this can feel
a little uncomfortable but should not be painful
o The patient needs to avoid taking anti-histamines and certain other medications
for 48 hours before the test

© Endeavour College of Natural Health endeavour.edu.au 17
Skin Prick Testing
http://www.mitchellzhomes.com/AZAPAA/skintest.bmp

© Endeavour College of Natural Health endeavour.edu.au 18
HYPERSENSITIVITY REACTIONS
• Treatment options include:
– Allergy testing to identify and avoid the
allergen
– Drugs
• Antihistamine drugs
• Glucocorticoids and steroidal derivatives to
stabilise the vascular system
• New drugs include leukotriene receptor blockers
for asthma
– Desensitisation treatment

© Endeavour College of Natural Health endeavour.edu.au 19
COMMON HYPERSENSITIVITIES
http://dermimages.med.jhmi.edu/images/Papular_Urticaria_1_100606.jpg
Urticaria (Hives)
• Allergic rhinitis– Nasal mucosa
– Sneezing, copious watery secretion, itching
– Eyes often affected also
– Often seasonal due to increases in allergen exposure (pollen)
• Food allergies– Digestive tract mucosa
– Nausea, vomiting, diarrhoea
– Skin rashes (hives), pruritic
– If severe hives can occur in pharyngeal mucosa obstructing airflow

© Endeavour College of Natural Health endeavour.edu.au 20
COMMON HYPERSENSITIVITIES
http://www.sciencephoto.com/image/256384/530wm/M1500252-Atopic_eczema-SPL.jpg
• Atopic eczema
– Chronic skin condition
– Often a genetic component
– Common in infants and young
children
– Skin rash can occur anywhere
– Associated with ingested foods,
irritating fabrics, dry
atmosphere
– Remission with growth and
development
– Reoccurrences can occur in
adulthood
Atopic Eczema

© Endeavour College of Natural Health endeavour.edu.au 21
COMMON HYPERSENSITIVITIES
Image Source:http://trialx.com/curetalk/wp-
content/blogs.dir/7/files/2011/05/diseases/Asthma_Bronchial-3.jpg
• Asthma (extrinsic)• Lung disorder
• May result from allergic response in
bronchial mucosa
• Severe but reversible bronchial
obstruction
• Long term can lead to irreversible
damage (COPD)
• Familial history of other allergic
conditions, onset common in children
• Remission can occur with
development to adulthood
Asthma

© Endeavour College of Natural Health endeavour.edu.au 22
ANAPHYLAXIS
http://dccdn.de/pictures.doccheck.com/photos/e/d/7fd15798ce17750_m.jpg
Wasp Sting
• Is an extreme, life threatening,
systemic manifestation of type
I hypersensitivity
• Occurs within minutes of
exposure
• Common causes include:
– Insect stings
– Food allergies (nuts,
shellfish)
– Administration of drugs
(penicillin, anaesthetics)

© Endeavour College of Natural Health endeavour.edu.au 23
ANAPHYLAXIS
• Pathophysiology of Anaphylaxis
– Release of large amounts of chemical
mediators
– General or systemic vasodilation
– Oedema of the lungs
– Bronchoconstriction
– Respiratory and circulatory impairment
– Loss of consciousness
– May be fatal if untreated

© Endeavour College of Natural Health endeavour.edu.au 24
Anaphylaxsis

© Endeavour College of Natural Health endeavour.edu.au 25
ANAPHYLAXIS• Clinical Features
– Generalised itching or tingling sensation over the body
– Coughing and difficulty breathing
– Weakness, dizziness or fainting
– Fear and panic
– Oedema may be present around eyes, lips, tongue, hands and feet
– Skin may break out in hives
– Collapse and loss of consciousness in minutes

© Endeavour College of Natural Health endeavour.edu.au 26
ANAPHYLAXIS
http://www.emergency.com.au/flex/course-in-first-aid-management-of-anaphylaxis/546/1
• Emergency Treatment
– Call an ambulance
– Epinephrine immediately (sufferers often carry Epipens)
– Administer oxygen if available
– Treat for shock
– Administer CPR if needed

© Endeavour College of Natural Health endeavour.edu.au 27
TYPE II HYPERSENSITIVITY
(CYTOTOXIC)
• Location of the antigen is on the surface of cells or other tissue components
• Involvement of IgG, and IgM antibodies
• Involves complement dependent mechanisms
– Lysis via membrane attack complex (MAC)
– Opsonisation via macrophages
• Involves antibody dependent mechanisms
– Antibody dependent cell mediated cytotoxicity (ADCC). This involves lysis of target cell expressing the antigen.

© Endeavour College of Natural Health endeavour.edu.au 28
Type II
Hypersensitivity
(Cytotoxic)
From Porth’s Pathophysiology: concepts of altered health states, (9th ed., p. 345), by Grossman, S.C. & Porth, C.M. (2014), Philadelphia, U.S.A. Walters Kluwer Health - Lippincott, Williams & Wilkins.

© Endeavour College of Natural Health endeavour.edu.au 29
OUTCOMES OF TYPE II
RESPONSES• Death of cell
• Common type II reactions:
– Transfusion reactions from incompatible donor
– Erythroblastosis fetalis (rhesus incompatibility)
– Drug reactions (where drug is adsorbed to cell surface)
– Auto immune reactions : Grave’s disease, Myathenia Gravis
• Treatment
– Exchange transfusion
– Immunosuppressive drugs
– Cytotoxic drugs
– Plasmapheresis
– Surgery

© Endeavour College of Natural Health endeavour.edu.au 30
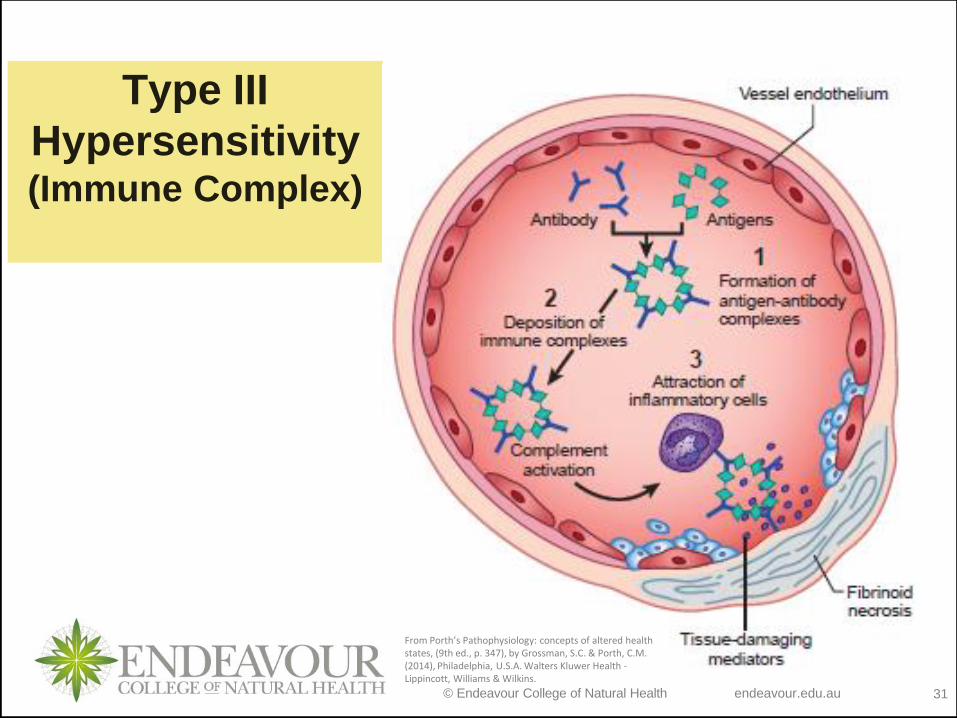
TYPE III HYPERSENSITIVITY
(IMMUNE COMPLEX)
• Abnormal or persistent antibody- antigen
complex formation which has not been cleared
by normal mechanisms
• Deposits of immune complexes in tissues
– Localised inflammation caused by activation
of complement and neutrophils by the
immune complex
– Can lead to vasodilation and oedema
– Can lead to necrosis
© Endeavour College of Natural Health endeavour.edu.au 31
Type III
Hypersensitivity (Immune Complex)
From Porth’s Pathophysiology: concepts of altered health states, (9th ed., p. 347), by Grossman, S.C. & Porth, C.M. (2014), Philadelphia, U.S.A. Walters Kluwer Health -Lippincott, Williams & Wilkins.

© Endeavour College of Natural Health endeavour.edu.au 32
TYPE III HYPERSENSITIVITY• Types
– Serum sickness
– Raynaud's phenomena - cryoglobulins deposition
– Arthus reaction
• injection, ingestion or inhalation of allergens, egallergic alveolitis ( farmers lung, pigeons disease coeliac reaction)
• Treatment
– Corticosteroids
– Immunosuppressive drugs
– Environmental removal or avoidance of antigen if possible
– Plasmapheresis

© Endeavour College of Natural Health endeavour.edu.au 33
TYPE IV HYPERSENSITIVITY
(CELL MEDIATED DELAYED)
• Activation of T cells over time
• 48-72 hours for reaction to develop
• Results in inflammation, cell lysis and tissue destruction
• Common Type IV Activators
– Cosmetics
– Dyes
– Soaps
– Metals
– Rubber and latex
– Elastoplast
– Plant toxins (poison ivy)

© Endeavour College of Natural Health endeavour.edu.au 34
TYPE IV HYPERSENSITIVITYMechanism
• Antigens are cell or tissue bound
• Two mechanisms involved- both involving T cells:
• First mechanism:
– Subsets of CD4 T cells are activated (first exposure)
– On second exposure activated CD4 T cells secrete cytokines which in turn activate macrophages
– Associated with inflammation and granuloma formation
• Second mechanism:
– Direct cell cytotoxicity via sensitised CD8 T cells
– T cells become sensitised over time
– CD8 T cells lyse cells bearing antigen

© Endeavour College of Natural Health endeavour.edu.au 35
Type IV
Hypersensitivity
From Porth’s Pathophysiology: concepts of altered health states, (9th ed., p. 348), by Grossman, S.C. & Porth, C.M. (2014), Philadelphia, U.S.A. Walters Kluwer Health -Lippincott, Williams & Wilkins.
Cell-mediated
Delayed Hypersensitivity Response

© Endeavour College of Natural Health endeavour.edu.au 36
TYPE IV HYPERSENSITIVITY
• Clinical Features - generally do not occur immediately after direct contact
– Localised rash
– Pruritis
– Redness
– Vesicles
– Serous exudate
• Treatment
– Immunosuppressive drugs
– Corticosteroids
– Removal of the antigen

© Endeavour College of Natural Health endeavour.edu.au 37
POISON IVY REACTION
http://www.babymd.net/poisonivy4.jpg

© Endeavour College of Natural Health endeavour.edu.au 38
AUTOIMMUNITY

© Endeavour College of Natural Health endeavour.edu.au 39
WHAT IS AUTOIMMUNITY?o 7o A sustained adaptive immune response to a self
antigen which causes tissue damage
o Influenced by both environmental and genetic factors
Environmental
• Occupation
• UV light
• Drugs
• Infections
(viruses, bacteria, mycoplasmas
Genetic
• Inherited chromosomal mutations
• Presence of particular genes such as HLA B2

© Endeavour College of Natural Health endeavour.edu.au 40
GENETIC BIAS OF COMMON
AUTOIMMUNE DISEASES
o Ankylosing spondylitis HLA-B27 (90%)
o Myasthenia gravis HLA-DR3 (5%)
o Graves disease HLA-DR3 (5%)
o SLE HLA-DR3 (5%)
o IDDM HLA-DR3 (20%)
HLA-DR4
o RA HLA-DR4 (5%)
© Endeavour College of Natural Health endeavour.edu.au 41
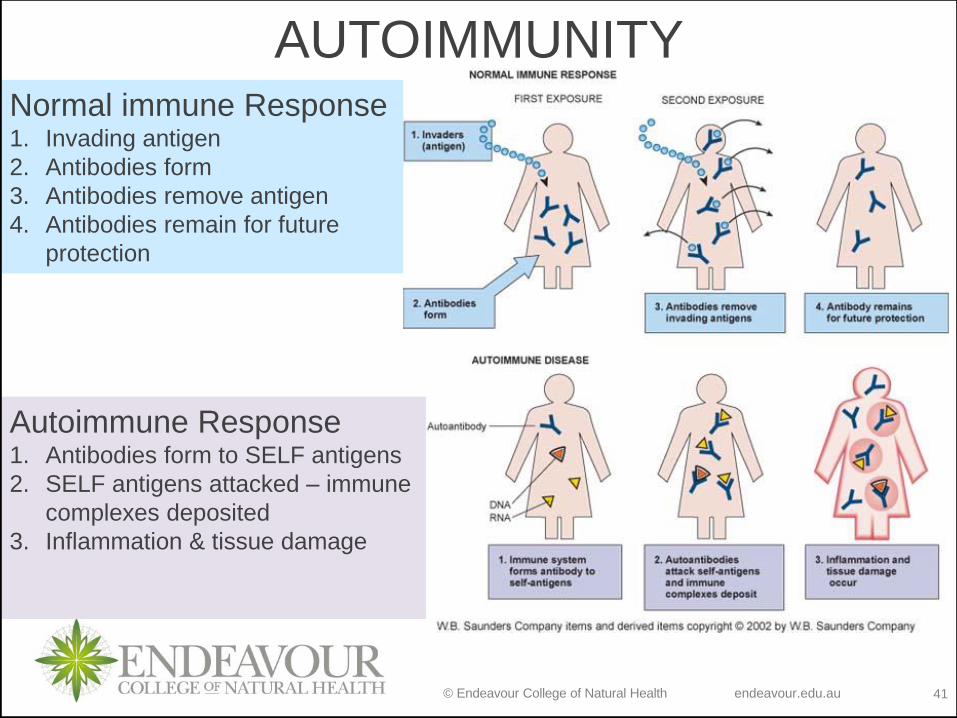
AUTOIMMUNITYNormal immune Response1. Invading antigen
2. Antibodies form
3. Antibodies remove antigen
4. Antibodies remain for future
protection
Autoimmune Response1. Antibodies form to SELF antigens
2. SELF antigens attacked – immune
complexes deposited
3. Inflammation & tissue damage

© Endeavour College of Natural Health endeavour.edu.au 42
AUTOIMMUNITYImmunological Tolerance
− “a state in which an individual is incapable of developing
an immune response against a specific antigen. Self
tolerance specifically refers to a lack of immune
responsiveness to one’s own tissue antigens.”- Kumar, Cotran and Robbins. Robbins Basic Pathology, 7th Ed, Saunders,
Philadelphia. 2003
o Exact processes of the development of autoimmunity
have not been established
o Self antigens are usually tolerated by the immune
system (the immune system does not react to them)
o When self tolerance is lost the immune system is unable
to differentiate self antigens from foreign antigens

© Endeavour College of Natural Health endeavour.edu.au 43
AUTOIMMUNE REACTIONSSome immune reactions are known to be involved
o After self tolerance is broken down different components of the immune system can be activated
o Mediated by either antibodies or T cells
o The antigen cannot be eradicated from the body as it is part of the body
o The antigen involved and the mechanism of action determines the clinical expression of the disease
o The immune reaction may be local or systemic

© Endeavour College of Natural Health endeavour.edu.au 44
AUTOIMMUNITY REACTIONSo Autoimmunity reactions have similar mechanism/
processes as the hypersensitivity reactions
o The difference is that autoimmune mechanisms involve self antigens not foreign antigens
o Absence of type I responses
o Reactions involving type II hypersensitivity are common where reactions involve the induction of IgG or IgM
o Reactions involving type III autoimmunity are common where immune complexes form
o In organ specific autoimmunity T cell responses are directly involved in causing the tissue damage (type IV)

© Endeavour College of Natural Health endeavour.edu.au 45
TYPE II AUTOIMMUNITYo Auto-antigen is cell bound
o Immune reaction to the auto-antigen results in type II hypersensitivity mechanisms becoming activated:
• Complement dependent lysis
• Antibody dependent cellular cytotoxicity
• Anti-receptor antibodies
o Common Type II Autoimmune Reactions
• Autoimmune haemolytic anaemia
• Part of Hashimoto’s thyroiditis
• Binding of antibodies to a receptor-
–Graves disease
–Myasthenia gravis

© Endeavour College of Natural Health endeavour.edu.au 46
TYPE III AUTOIMMUNITYo Auto-antigen is free
o Immune reaction to the auto-antigen results in type III hypersensitivity mechanisms becoming activated:
• Antibodies are produced to the auto-antigen
• Immune complex formation can occur locally or systemically
o Common Type III Autoimmune Reactions
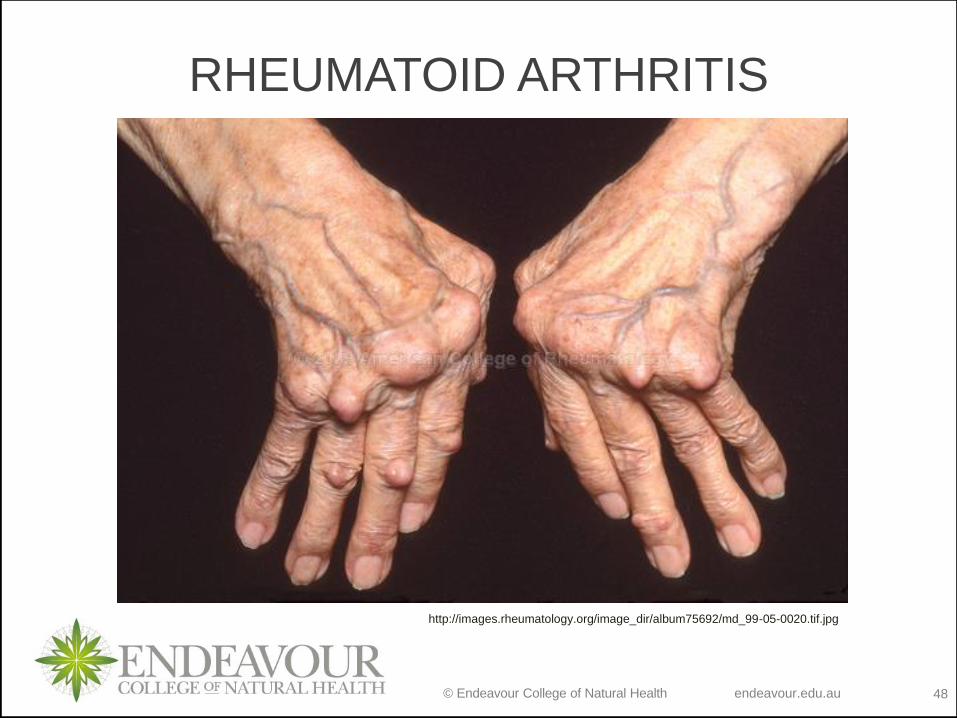
• Rheumatoid Arthritis
• Systemic Lupus Erythematosus (SLE)

© Endeavour College of Natural Health endeavour.edu.au 47
RHEUMATOID ARTHRITIS STAGES
http://emedicine.medscape.com/article/401271-overview
Early
MidLate
MidA B
C D
© Endeavour College of Natural Health endeavour.edu.au 48
RHEUMATOID ARTHRITIS
http://images.rheumatology.org/image_dir/album75692/md_99-05-0020.tif.jpg

© Endeavour College of Natural Health endeavour.edu.au 49
SYSTEMIC LUPUS
ERYTHEMATOSUS (SLE)
http://imaging.ubmmedica.com/consultantlive/images/articles/2003/07012003/0307ConPERheum1A.jpg

© Endeavour College of Natural Health endeavour.edu.au 50
TREATMENT OF AUTOIMMUNITY
oGlucocorticoids (only in non-organ
specific conditions)
oPrednisone (high dose during
exacerbation)
oSystem specific therapy
oSymptom relief

© Endeavour College of Natural Health endeavour.edu.au 51
IMMUNODEFICIENCYo A partial or total loss of function of one or more
components of the immune system
o Can be inherited or acquired
o Can be transient or permanent
o Can be induced by immunosuppression
o Most common form of immunodeficiency worldwide is malnutrition
o However, in developed countries most immunodeficiency's are inherited
o Certain immunodeficiency's correlate to an individuals susceptibility to particular infections or diseases
o Two forms / types - Primary and Secondary

© Endeavour College of Natural Health endeavour.edu.au 52
PRIMARY IMMUNODEFICIENCY'So A basic developmental failure somewhere in the
immune system
• Inherited or congenital
• Genetic basis
o Congenital hypoglobulinemia
• Affect B cell
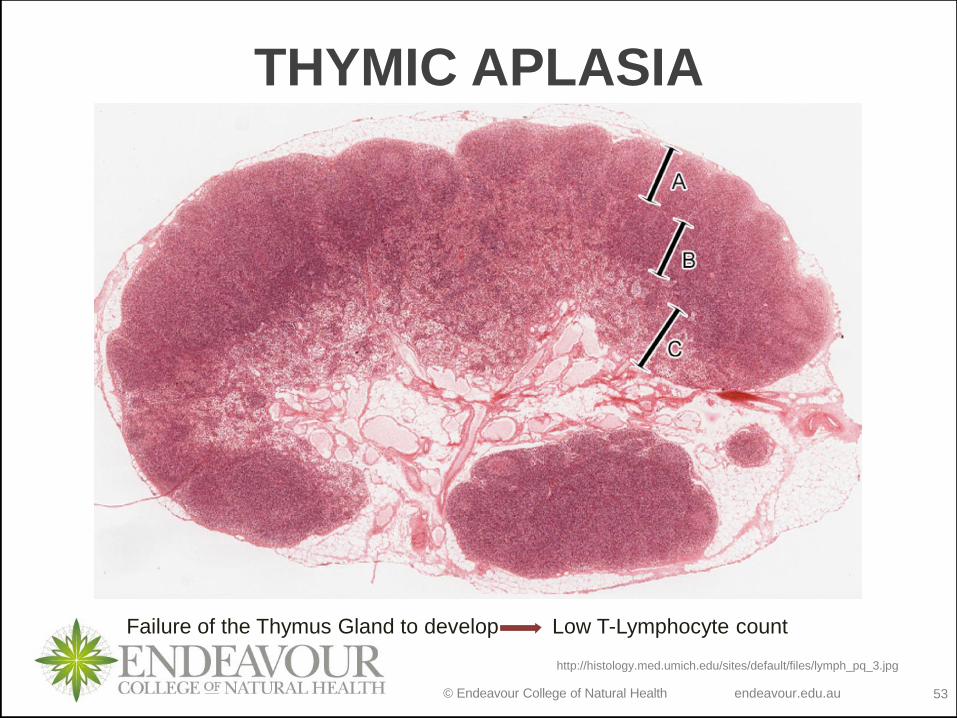
o Thymic aplasia
• Low T cell
o DiGeorge’s syndrome
• Low mature T cells
o Inherited combined immunodeficiency syndromes
• Affect B & T cell
o Inherited deficit of one or more components
• Affect complement
© Endeavour College of Natural Health endeavour.edu.au 53
THYMIC APLASIA
Failure of the Thymus Gland to develop Low T-Lymphocyte count
http://histology.med.umich.edu/sites/default/files/lymph_pq_3.jpg
© Endeavour College of Natural Health endeavour.edu.au 54
SECONDARY IMMUNODEFICIENCYo Secondary
• Acquired
• Loss of immune function due to specific causes
• May occur at any time in the lifespan
o Causes
• Infection (particularly viral)
• Malnutrition
• Liver disease (hypoproteinemia)
• Cancer
• as a result of malnutrition and blood loss and commonly effects of treatment (decreased bone marrow production)
• Immunosuppressive drugs
• Severe stress (prolonged glucocorticoid secretion)

© Endeavour College of Natural Health endeavour.edu.au 55
SECONDARY
IMMUNODEFICIENCY'So Kidney disease with globulin loss
• Affects Humoral immunity
o Hodgkin's disease (cancer of the lymph nodes)
• Affect T Cell
o AIDS
• T Cell
o Immunosuppression, radiation, chemotherapy
• Loss of phagocytes
o Malnutrition
• complement
o Cirrhosis of the liver
• Complement

© Endeavour College of Natural Health endeavour.edu.au 56
HODGKIN’S LYMPHOMA
http://www.healthoma.com/hodgkins-lymphoma-and-its-symptoms/
Reed Sternberg
cells in Hodgkin’s
Lymphomas

© Endeavour College of Natural Health endeavour.edu.au 57
LIVER CIRRHOSIS
http://medicalpicturesinfo.com/wp-content/uploads/2011/09/Cirrhosis-2.jpg

© Endeavour College of Natural Health endeavour.edu.au 58
SECONDARY
IMMUNODEFICIENCY'S
http://theness.com/neurologicablog/wp-
content/uploads/2011/10/malaria.jpg
Insect Image: http://www.gossipjackal.com/wp-
content/uploads/2010/07/malaria-proof-
mosquitoes.jpg
Malaria
As anaemia worsens, liver and
spleen start lysing ALL blood cells
and platelets leading to:
- Immunodeficiency - WBC’’s
- Worsening anaemia - RBC’s
- Excessive bruising - Platelets

© Endeavour College of Natural Health endeavour.edu.au 59
TREATMENT OF
IMMUNODEFICIENCY'S
oReplacement of antibodies with
gammaglobulins
• (blood transfusions)
oBone marrow or thymus transplants
• Limited success
• Not suitable in all cases

© Endeavour College of Natural Health endeavour.edu.au 60
HIV AND AIDS
oEpidemiologyoTransmissionoViral structureoMechanism of infectionoProgression of the disease - when
does HIV positive become AIDSoClinical signs and symptomsoTreatment

© Endeavour College of Natural Health endeavour.edu.au 61
HIV AND AIDS
From Porth’s Pathophysiology: concepts of altered health states, (9th ed., p. 364), by Grossman, S.C.
& Porth, C.M. (2014), Philadelphia, U.S.A. Walters Kluwer Health - Lippincott, Williams & Wilkins.

© Endeavour College of Natural Health endeavour.edu.au 62
HIV LIFE
CYCLE
From Porth’s Pathophysiology: concepts of altered health states, (9th ed., p. 365), by Grossman,
S.C. & Porth, C.M. (2014), Philadelphia, U.S.A. Walters Kluwer Health - Lippincott, Williams &
Wilkins.

© Endeavour College of Natural Health endeavour.edu.au 63
Readings and ResourcesResources:
o Set Textbooks:
Colledge, N.R., Walker, B.R. & Ralston S.H. (2014). Davidson’s Principles and Practice of Medicine, (22nd ed.). Edinburgh.
Churchill Livingstone.
Grossman, S.C. & Porth, C.M. (2014). Porth’s Pathophysiology: concepts of altered health states, (9th ed.). Philadelphia,
U.S.A. Walters Kluwer Health - Lippincott, Williams & Wilkins.
o Additional textbooks:
Davies, A. & Moores, C. (2010). The respiratory system: basic science and clinical conditions, (2nd ed.). Edinburgh. Churchill,
Livingstone, Elsevier.
Field, M., Pollock, C., Harris, D. (2010). Systems of the Body: The Renal System; Basic Science and Clinical Conditions. (2nd
ed.). United Kingdom: Churchill Livingstone.
Jamison, J.R. (2006) Differential Diagnosis for Primary Care: a handbook for health care practitioners. (2nd ed.). Edinburgh.
Churchill Livingstone.
Lee, G. & Bishop, P. (2013). Microbiology and Infection Control for Health Professionals, (5th ed.). Frenchs Forest, NSW.
Pearson Education.
McCance, K.L. & Huether, S.E. (2014). Pathophysiology: the biological basis for disease in adults and children, (7th ed.). St.
Louis, MO. Elsevier.
Murphy, K. (2011). Janeway’s immunobiology, (8th ed.). New York. Garland Science.
Noble, A., Johnson, R. & Bass, P. (2010). The cardiovascular system: basic science and clinical conditions, (2nd ed.).
Edinburgh. Churchill, Livingstone, Elsevier.
Pagana, K.D. & Pagana, T.J. (2013). Mosby’s diagnostic and laboratory test reference, (11th ed.). St. Louis, MO. Elsevier.
Smith, M.E. & Morton, D.G. (2010). The digestive system: basic science and clinical conditions, (2nd ed.). Edinburgh.
Churchill, Livingstone, Elsevier.
VanMeter, K.C. & Hubert, R. (2014). Gould’s pathophysiology for health professions, (5th ed.). St. Louis, MO. Elsevier.

© Endeavour College of Natural Health endeavour.edu.au 64
COMMONWEALTH OF AUSTRALIA
Copyright Regulations 1969
WARNING
This material has been reproduced and
communicated to you by or on behalf of
the Endeavour College of Natural Health pursuant to
Part VB of the Copyright Act 1968 (the Act).
The material in this communication may
be subject to copyright under the Act.
Any further reproduction or
communication of this material by you
may be the subject of copyright
protection under the Act.
Do not remove this notice.


















