Abnormal Calcium Handling Properties Underlie Familial ... · PDF fileRepresentative...
20
1 Cell Stem Cell, Volume 12 Supplemental Information Abnormal Calcium Handling Properties Underlie Familial Hypertrophic Cardiomyopathy Pathology in Patient-Specific Induced Pluripotent Stem Cells Feng Lan, Andrew S. Lee, Ping Liang, Veronica Sanchez-Freire,Patricia K. Nguyen, Li Wang, Leng Han, Michelle Yen, Yongming Wang, Ning Sun, Oscar J. Abilez, Shijun Hu, Antje D. Ebert, Enrique G. Navarrete, Chelsey S. Simmons, Matthew Wheeler, Beth Pruitt, Richard Lewis, Yoshinori Yamaguchi, Euan A. Ashley, Donald M. Bers, Robert C. Robbins, Michael T. Longaker, and Joseph C. Wu
Transcript of Abnormal Calcium Handling Properties Underlie Familial ... · PDF fileRepresentative...

1
Cell Stem Cell, Volume 12
Supplemental Information
Abnormal Calcium Handling Properties Underlie
Familial Hypertrophic Cardiomyopathy Pathology
in Patient-Specific Induced Pluripotent Stem Cells
Feng Lan, Andrew S. Lee, Ping Liang, Veronica Sanchez-Freire,Patricia K. Nguyen, Li Wang, Leng Han, Michelle Yen, Yongming Wang, Ning Sun, Oscar J. Abilez, Shijun Hu, Antje D. Ebert, Enrique G. Navarrete, Chelsey S. Simmons, Matthew Wheeler, Beth Pruitt, Richard Lewis, Yoshinori Yamaguchi, Euan A. Ashley, Donald M. Bers, Robert C. Robbins, Michael T. Longaker, and Joseph C. Wu

2
Ⅲ -7Ⅲ -6 Ⅲ -5Ⅲ -3
Diastole SystoleA B
OCT4
iPSC Fibroblast
SOX2
ACTIN
NANOG
Control HCM
46, XY 46, XY
C
DTUJ1 DAPI SOX17 DAPI SMA1 DAPI
OCT4
NANOG
PAX2
SOX17
BRACHYURY
GAPDH
EB
iPS
C
EB
iPS
C
EB
iPS
C
EB
iPS
CE
BiP
SC
EB
iPS
C
EB
iPS
C
EB
iPS
C
EB
iPS
C
EB
iPS
C
E F
2x
Endodermal glandsGlands & Cartilage
Squamous Epithelium Cartilage
40x
G AmplificationHha I digestion
150 bp
300 bp
Ⅱ -1 Ⅱ -2 Ⅲ -1 Ⅲ -2 Ⅲ -4 Ⅲ -8
Figure S1 (Referenced from Figure 1). Genomic stability and pluripotency of patient-specific iPSCs. (A) Two dimensional echocardiographic images of the left ventricle in a 2 chamber short-axis view showing asymmetric thickening of the inferior wall and hyperdynamic function in the HCM proband. (B) Western blot of protein expression for pluripotency transcription factors OCT4, SOX2, and NANOG in patient specific iPSCs and fibroblasts derived from HCM (II-1, III-1, III-2, III-3, III-8) and control (II-2, III-4, III-5, III-6, III-7) family members. β-actin was used as control. (C) Karyotyping of patient specific iPSCs demonstrated a normal karyotype of 2n=46 (XX or XY) through passage 30 for both control and HCM cells. (D) Differentiation of patient-specific iPSCs into derivatives of 3 germ layers. Representative immunofluorescence staining photographs of EBs differentiated from patient-specific iPSCs for TUJ1 (ectoderm), SOX17 (endoderm), and SMA1 (mesoderm). (E) Representative hematoxylin and eosin staining of a solid encapsulated teratoma derived from a patient-specific iPSC line implanted into the sub-renal capsule of SCID mouse mice. (F) Semi-quantitative reverse transcription (RT)-PCR of patient-specific iPSC lines and EBs differentiated from these lines. OCT4 and NANOG were used as markers of pluripotency, whereas PAX2 (ectoderm), SOX17 (endoderm), and BRACHYURY (mesoderm) were used as markers of differentiation. (G) Genotyping of patient-specific iPSC lines derived from dermal fibroblasts of HCM subjects (II-1, III-1, III-2, III-3, III-8) and control matched family members (II-2, III-4, III-5, III-6, III-7). Restriction enzyme digestion and amplification confirmed presence and absence of the Arg663His mutation in HCM and control subjects, respectively.

3
Supplementary Figure 2
0
20
40
60
80A B
MLC2a MLC2v DAPI MLC2a MLC2v DAPI
MLC2a MLC2v DAPI MLC2a MLC2v DAPIC
0
20
40
60
80
% S
tain
ed
ce
lls
*
TNNT2 NFAT TNNT2NFATDAPIDAPI
HC
MC
s-A
FK
50
6
0
20
40
60
80
100
E F
HG I
TNNT2 F-ACTIN DAPI
HCMControl
0
20
40
60
80
100
D
% B
ea
tin
g E
Bs
% T
NN
T2
+ c
ells
% C
Ms w
ith
nu
cle
ar
NF
AT
C4
**
HCM Cs-A FK506
0
5
10
15
20
25
*
HCMControl
% C
ells w
ith
Dis
org
an
ize
d
Sa
rco
me
re(s
ing
le c
ells)
Ave
rag
e S
arc
om
eri
cC
on
ten
t
(In
teg
rate
d T
NN
T2
Flu
ore
sc
en
ce
In
ten
sit
y/c
ell )
1.0 E5
0.8 E5
0.6 E5
0.4 E5
0.2 E5
0
**
HCMControl
Figure S2 (Referenced from Figure 2). Characterization of patient-specific iPSC-CMs. (A) Efficiency of
cardiac differentiation for each patient-specific iPSC line as measured by the percentage of beating EBs (n=50 per
line, 10 patient lines total). (B) Percentage of differentiated cells per patient-specific EB expressing cardiac troponin
T (n=100 per line, 10 patient and control subject lines). (C) Staining of iPSC-CMs for markers of cardiac
differentiation. Sub-characterization of iPSC-CMs based on immunostaining for myosin light chain 2a (MLC2a) and
myosin light chain 2v (MLC2v) derived from family members with and without HCM. (D) Quantification of iPSC-
CM into ventricular, atrial, and double positive (immature) subtypes based on immunostaining for MLC2a and
MLC2v (n=235, 10 patient and control subject lines). * denotes P<0.001 MLC2a vs MLC2v vs double positive. (E)
Representative immunofluorescence staining for nuclear translocation of NFATc4 in HCM-iPS-CMs treated with
the calcineurin inhibitors Cs-A and FK506. (F) Quantification of HCM iPSC-CMs exhibiting nuclear translocation
of NFATc4 with and without treatment of Cs-A and Fk-506 (n=83, 5 patient lines per treatment group). (G)
Representative sarcomeric stainings for F-actin and TNNT2 in control and HCM iPSC-CMs demonstrating
organized and disorganized sarcomeres. (H) Quantification of average sarcomeric content in control and HCM
iPSC-CMs as measured by average fluorescence intensity of TNNT2 (HCM n=186, 5 patient lines, control n=173, 5
control subject lines). (I) Quantification of control and HCM iPSC-CMs exhibiting disorganized sarcomeres (HCM
n=186, 5 patient lines, control n = 173, 5 control subject lines). Cells with disorganized sarcomeres were defined as
having greater than 25% cell area of punctate troponin T distribution without striations.* denotes P<0.05 HCM vs
control, ** denotes P<0.001 HCM vs control. Error bars are standard error mean.

4
Day 20 Day 30 Day 400
1
2
3
4
*
Day 20 Day 30 Day 400
2
4
6 *
Day 20 Day 30 Day 400
5
10
15
20
25*
Day 20 Day 30 Day 400.0
0.5
1.0
1.5
Day 20 Day 30 Day 400.00
0.05
0.10
0.15
0.20
0.25*
Day 20 Day 30 Day 400.0
0.5
1.0
1.5
*
Day 20 Day 30 Day 400
20
40
60
80*
Day 20 Day 30 Day 400
1
2
3
4
5
*
Day 20 Day 30 Day 400
5
10
15
20
25 *
Day 20 Day 30 Day 400.0
0.2
0.4
0.6
0.8
1.0
Day 20 Day 30 Day 400
2
4
6
8
10
*
Day 20 Day 30 Day 400
50
100
150 *
A
B
C
F
020406080
100120
0
200
400
600
800
0
20
40
60
80 Control
HCM
D
G H
0
20
40
60
80 **
Control
HCM
VentricularNodal Atrial
0 mV
0 mV
0.2 S 40 m
V
-60
-40
-20
0
E
0
10
20
30
40
50
Rel
ativ
e ex
pre
ssio
n/G
AP
DH
Rel
ativ
e ex
pre
ssio
n/G
AP
DH
Rel
ativ
e ex
pre
ssio
n/G
AP
DH
GATA4
SERCA2
TNNT2
Day 20 Day 30 Day 40
MYL7
Day 20 Day 30 Day 40
ACTC1
Day 20 Day 30 Day 40
MYL2
Day 20 Day 30 Day 40
Day 20 Day 30 Day 40
MYH7
Day 20 Day 30 Day 40
ACTN2
Day 20 Day 30 Day 40
MYH6
Day 20 Day 30 Day 40
Day 20 Day 30 Day 40
MYOCD
Day 20 Day 30 Day 40
MAPK11
Day 20 Day 30 Day 40
MEF2C
Day 20 Day 30 Day 40
HCM
Control
HCMControl
% C
ells
VentricularNodal Atrial
Res
tin
g M
emb
ran
e P
ote
nti
al (
mV
)
VentricularNodal Atrial Up
stro
ke V
elo
city
(V
/ s
)
VentricularNodal Atrial
Am
plit
ud
e (m
V)
VentricularNodal Atrial
AP
D90
(m
s)
VentricularNodal Atrial Cel
l C
apac
itan
ce
(pF
)
HCMControl
Figure S3 (Referenced from Figure 3). Gene expression and electrophysiological profiling of patient-specific iPSC-CMs. (A) Changes in temporal gene expression for a panel of 12 transcripts related to HCM gene expression in control and HCM iPSC-CMs following cardiac differentiation (n=32, 5 patient and control subject lines per time point). (B) Whole cell patch clamp recordings from normal and HCM human iPSC-CMs. Single spontaneous action potentials from representative control and HCM iPSC-CMs indicating presence of myocytes exhibiting nodal, atrial, and ventricular waveforms. (C) Quantification of nodal, atrial, and ventricular sub-populations in control (n=144, 5 control subject lines) and HCM iPSC-CMs (n=131, 5 patient lines). (D) Quantification of nodal, atrial, and ventricular resting membrane potentials (RMPs) in control (n=144, 5 control subject lines) and HCM iPSC-CMs (n=131, 5 patient lines). (E) Quantification of nodal, atrial, and ventricular upstroke velocities in control (n=144, 5 control subject lines) and HCM iPSC-CMs (n=131, 5 patient lines). (F) Quantification of nodal, atrial, and ventricular action potential amplitudes in control (n=144, 5 control subject lines) and HCM iPSC-CMs (n=131, 5 patient lines). (G) Quantification of nodal, atrial, and ventricular action potential durations at 90% repolarization (APD90) for control (n=144, 5 control subject lines) and HCM iPSC-CMs (n=131, 5 patient lines). (H) Capacitance measurements of cell size using patch clamp (HCM n=131, 5 patient lines; control, n=144, 5 control subject lines,). * denotes P<0.01 HCM vs control, ** denotes P<0.001 HCM vs control. Error bars represent standard error mean.

5
Control HCM0
1
2
3
No
rmal
ized
Co
ntr
acti
leM
oti
on
(n
M/c
ell)
C
0
5
10
15
20
Control HCM
% C
ells
wit
h c
on
trac
tile
arr
hyt
hm
ia
2 .5
2 .0
1 .5
1 .0
0 .5
0 .0
43210
No
rmal
ized
Co
ntr
atci
le M
oti
on
(n
M/c
ell)
ControlHCMD E
Time (s)
0
2
4
6
8
10
12
14
16
18
20
Co
ntr
ol
-2
-1
0
1
2
3
0 10 20 30 40 50 60
-3
-2
-1
0
1
2
3
4
5
6
0 10 20 30 40 50 60
Qu
an
tity
of
mo
tio
n (
Inte
ns
ity
x1
0)
Time (s)
HC
M
Fre
qu
en
cy
Interval of the beating (s)
0
2
4
6
8
10
Fre
qu
en
cy
A B
0 1.0 2.0 3.0 4.0 5.0
0 1.0 2.0 3.0 4.0 5.0
Control HCM0
10
20
30
40
50
Fre
qu
en
cy o
f C
a2+ T
ran
sien
t(p
er m
in)
Control HCM0
1
2
3
4
Am
plit
ud
e o
f C
a2+ t
ran
sien
t(
F /
F0)
Control HCM0.00
0.05
0.10
0.15
0.20
Irre
gu
lar
of
amp
litu
de
(s.d
. / m
ean
)
Control HCM0
2
4
6
8
10
Inte
gra
ted
Ca2+
tra
nsi
ent
Control HCM0.0
0.1
0.2
0.3
0.4
Irre
gula
rity
of in
tegra
ted C
a2+
tran
sien
t (s
.d. /
mea
n)
Control HCM0.0
0.2
0.4
0.6
0.8
Irre
gu
lari
ty o
f ti
min
g(s
.d. /
me
an)
**
F G H
I J K *
1 . 0
0 . 9
0 . 8
0 . 7
0 . 6
1 5 01 0 05 00
S
0.5
F /
F0
Co
ntr
ol
HC
M
1 . 4
1 . 2
1 . 0
0 . 8
1 5 01 0 05 00
M
Co
ntr
ol
HC
M
L
ControlHCM0
5
10
15
20
% C
ells
wit
h ir
reg
ula
r C
a2+
tran
sien
ts
**N
HCMControlHCMControlHCMControl
HCMControlHCMControl HCMControl
HCMControl% C
ell
s w
ith
co
ntr
ac
tile
arr
hyt
hm
ia *6
8
0
2
4
10
12
16
0
4
8
20
1
2
-2
-1
0
3
10 20 30 40 50 0 60
10 20 30 40 50 0 60
3
6
-3
0
HCMControl
Fre
qu
en
cy
of
Ca
2+
Tra
ns
ien
t(p
er
min
)
Am
pli
tud
e o
f C
a2
+ t
ran
sie
nt
(DF
/ F
0)
*
Irre
gu
lari
ty o
f ti
min
g
(s.d
. / m
ea
n)
Irre
gu
lari
ty o
f a
mp
litu
de
(s
.d. /
me
an
)
Irre
gu
lari
ty o
f in
teg
rate
d C
a2
+
tra
nsi
ent (
s.d
. / m
ea
n)
% C
ell
s w
ith
irre
gu
lar
Ca
2+
tra
ns
ien
ts
Inte
gra
ted
Ca
2+
tra
ns
ien
t
Figure S4 (Referenced from Figure 4). Contractile analysis and calcium handling properties of patient specific iPSC-CMs. (A) Analysis of time-lapse video recordings for contractile arrhythmia in control and HCM iPSC-CMs. Representative software analysis profiles of contractile timing in single control and HCM iPSC-CMs. Red arrowheads indicate representative cell contractions as determined by the video analysis. (B) The length of time between cell contractions were quantified and mapped to demonstrate the spread of beat intervals in control (n=68, 5 control subject lines) and HCM iPSC-CMs (n=64, 5 patient lines). Control iPSC-CMs exhibit a narrow distribution of beat intervals, whereas HCM iPSC-CMs exhibit a wide distribution indicating arrhythmic contraction. (C) Quantification of control (n=68, 5 control subject lines) and HCM iPSC-CMs (n=64, 5 patient lines) exhibiting contractile arrhythmia as determined by video analysis of single beating cells. (D) Representative traces of contractile motion analysis for control and HCM iPSC-CMs. (E) Quantification of normalized contractile motion through pixel displacement analysis (HCM n=663, 5 patient lines; control n=604, 5 control subject lines). * denotes P<0.01 HCM vs control. (F-K) Quantification of parameters for frequency, amplitude, and integrated Ca2+ load of Fluo-4 AM Ca2+ dye transients, as well as irregularities in the above measurements in control (n=80, 5 control subject lines) and HCM iPSC-CMs (n=100, 5 patient lines). (L) Fluo-4 AM Ca2+ imaging of patient-specific iPSC-CMs paced at 1 Hz. Representative image of region of interest (ROI) analysis used to quantify Ca2+ transients in paced (1 Hz) iPSC-CMs derived from control and HCM subjects. (M) Representative Ca2+ waveforms of paced (1 Hz) iPSC-CMs from HCM patients and control matched family members. Red arrowheads indicate irregular transients. (N) Quantification of control (n=19, 5 control subject lines) and HCM iPSC-CMs (n=20, 5 patient lines) exhibiting irregular Ca2+ transients during 1 Hz pacing. Control iPSC-CMs were not observed to exhibit abnormal Ca2+ waveforms during pacing. * denotes P<0.05 HCM vs control, ** denotes P<0.0001 HCM vs control. Error bars represent standard error mean.

6
1E-3 0.01 0.1 1 10
0.0
0.4
0.8
1.2
1.6
2.0
Verapamil Concentration (uM)
Control HCM
-0.5
-0.4
-0.3
-0.2
-0.1
0.0
0.1
0.2
350300250200150100500Time (ms)
Baseline1nM10nM50nM100nM200nM500nM1uM
-0.5
-0.4
-0.3
-0.2
-0.1
0.0
0.1
0.2
FP
Am
plitu
de (
mV
)
350300250200150100500Time (ms)
Baseline1nM10nM50nM100nM200nM
Control HCM
A B
C D
E
Control HCM
0 nM
1 nM
10 nM
200 nM
100 nM
50 nM
2 S
10
0 U
V
Verapamil
0.0
0.5
1.0
1.5
Control HCM
0
20
40
60
Control iPSC-CMs
0
20
40
60
Control iPSC-CMsF
Verapamil Concentration (uM)
No
rma
lize
d B
PM
HCMControl
IC5
0 o
f B
PM
(m
M)
Verapamil *
% Ir
reg
ula
r C
a2+
Tra
ns
ien
t
Untreated 100 nMDiltiazem %
Cel
ls w
ith
pu
tati
ve
DA
Ds
Untreated 100 nMDiltiazem
* *
FP
Am
pli
tud
e (m
V)
Figure S5 (Referenced from Figure 6). MEA analysis and pharmacological treatment of multicellular iPSC-CM preparations with Ca2+ inhibition. (A) Representative field potentials (FPs) from control and HCM patient-derived iPSC-CM EBs. Verapamil had a concentration-dependent effect on beating frequency that is obvious at 100 nM and 200 nM in controls. Black arrowheads indicate arrhythmia triggered by higher doses of verapamil. (B) Representative FP waveforms for control and HCM iPSC-CM EBs. (C) Plots of average beat frequencies for control and HCM cardiomyocyte EBs against verapamil concentrations fitted to the Hill equation. (D) Quantification of control and HCM IC50 values for spontaneous beat frequency against verapamil (HCM n=13, 5 patient lines; control n = 11, 5 control subject lines). (E) Quantification of irregular Ca2+ transients in HCM iPSC-CMs with and without diltiazem treatment (n=40, 5 patient lines). (F) Quantification of DADs in HCM iPSC-CMs with and without diltiazem (n=25, 5 patient lines). * denotes P<0.001 HCM vs control. Error bars represent standard error mean.
7
0
20
40
60
-3
-2
-1
0
1
2
3
4
5
6
0 10 20 30 40 50 60
-3
-2
-1
0
1
2
3
4
5
6
0 10 20 30 40 50 60
-3
-2
-1
0
1
2
3
4
5
6
0 10 20 30 40 50 60
-3
-2
-1
0
1
2
3
4
5
6
0 10 20 30 40 50 60
Qu
an
tity
of
mo
tio
n (
Inte
ns
ity
x1
05 )
20
nM
0 n
M5
0 n
M
Wa
sh
Lidocaine TreatmentA
B
Blank 50 nM Lidocaine
S
10
μM
S
F
/F0
C D
Qu
an
tity
of
mo
tio
n (
Inte
ns
ity
x1
05 )
0 μ
M3
μM
Wa
sh
Ranolazine TreatmentE F
Fre
qu
en
cy
0
2
4
6
8
10
0 1.0 2.0 3.0
Beat interval (s)
Fre
qu
en
cy
0
2
4
6
8
10
0 1.0 2.0 3.00
2
4
6
8
10
0 1.0 2.0 3.00
2
4
6
8
10
0 1.0 2.0 3.0
0 nM 1 nM 5 nM Wash
Wash
5
10
20
15
00 2.0 4.0 6.0
Fre
qu
en
cy
30 nM
5
10
20
15
00 2.0 4.0 6.0
0 nM
5
10
20
15
00 2.0 4.0 6.0
10 20 30 40 50 0 60 10 20 30 40 50 0 60
10 20 30 40 50 0 60 10 20 30 40 50 0 60
3
6
-3
0
3
6
-3
0
3
6
-3
0
3
6
-3
0
% C
ell
s w
ith
irr
eg
ula
r C
a2
+
tra
ns
ien
ts
10 20 30 40 50 0 60
10 20 30 40 50 0 60
10 20 30 40 50 0 60
3
6
-3
0
3
6
-3
0
3
6
-3
0
HCM
Control
Blank 50 nM Lidocaine
##
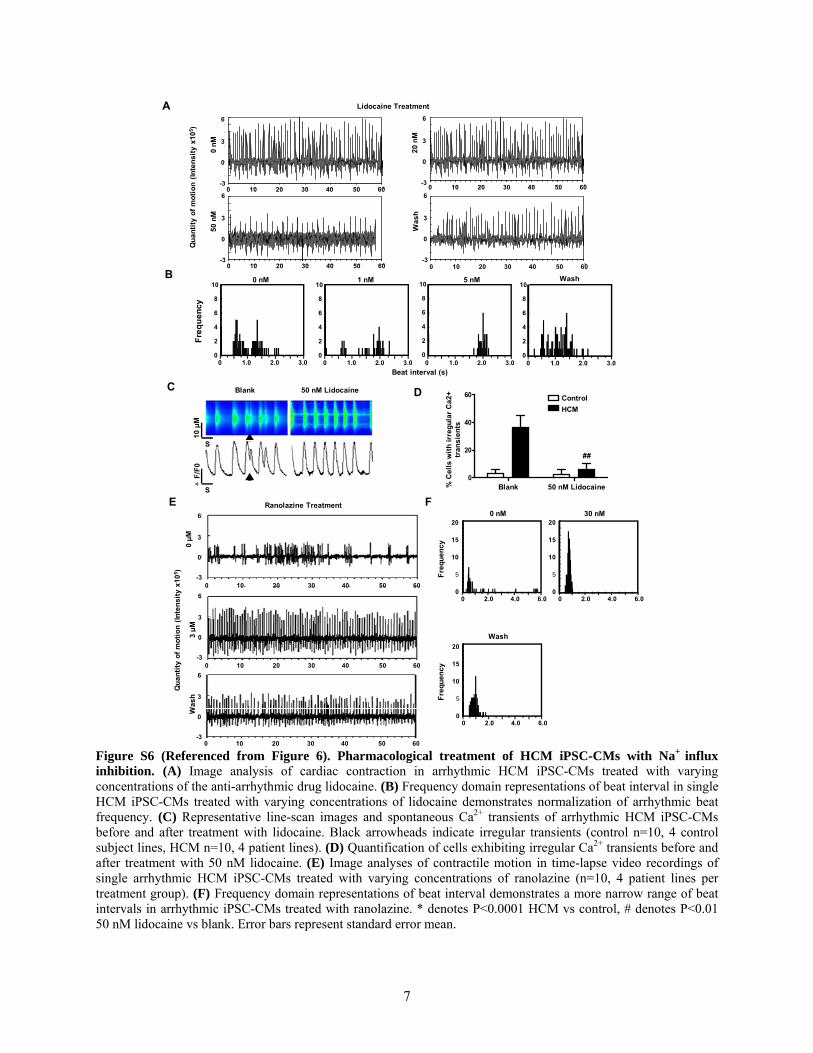
Figure S6 (Referenced from Figure 6). Pharmacological treatment of HCM iPSC-CMs with Na+ influx inhibition. (A) Image analysis of cardiac contraction in arrhythmic HCM iPSC-CMs treated with varying concentrations of the anti-arrhythmic drug lidocaine. (B) Frequency domain representations of beat interval in single HCM iPSC-CMs treated with varying concentrations of lidocaine demonstrates normalization of arrhythmic beat frequency. (C) Representative line-scan images and spontaneous Ca2+ transients of arrhythmic HCM iPSC-CMs before and after treatment with lidocaine. Black arrowheads indicate irregular transients (control n=10, 4 control subject lines, HCM n=10, 4 patient lines). (D) Quantification of cells exhibiting irregular Ca2+ transients before and after treatment with 50 nM lidocaine. (E) Image analyses of contractile motion in time-lapse video recordings of single arrhythmic HCM iPSC-CMs treated with varying concentrations of ranolazine (n=10, 4 patient lines per treatment group). (F) Frequency domain representations of beat interval demonstrates a more narrow range of beat intervals in arrhythmic iPSC-CMs treated with ranolazine. * denotes P<0.0001 HCM vs control, # denotes P<0.01 50 nM lidocaine vs blank. Error bars represent standard error mean.

8
Table S1 (Referenced from Figure 1). Clinical features of recruited family members
Patient ID Age
MYH7 Genotype Symptoms Holter Monitor
Ejection Fraction (%)
II-1 53 Arg663His Mutation
Exertional chest pain, palpitations, dizziness
Occasional PVCs 73.7
III-1 21 Arg663His Mutation
Exertional chest pain, palpitations, dizziness
Occasional PVCs 75.0
III-2 20 Arg663His Mutation Exertional chest pain
Occasional PVCs 70.1
III-3 18 Arg663His Mutation Exertional chest pain
Occasional PVCs 76.0
III-4 16 Wild type Normal None 61.3
III-5 14 Wild type None None 59.2
III-6 14 Wild type None None 62.0
III-7 13 Wild type None None 53.6
III-8 10 Arg663His Mutation None None 76.0
Clinical features of control and HCM family members recruited for this study including patient ID, age, MYH7 genotype, reported clinical symptoms, 24 hour Holter monitor for assessment of arrhythmia, and ejection fraction.

9
Table S2 (Referenced from Figure 5). Baseline electrophysiological parameters of iPSC-derived beating EBs obtained via MEA recordings
iPSC-CM Beats Per Minute
Interspike Interval (ms)
Field Potential Duration (ms)
Corrected Field Potential Duration (ms)
Control (n=25) 75.2±41.1 1592.2±2195.8 549.8±201.6 509.9±157.8
HCM (n=21) 62.9±24.0 1111.4±450.4 513.8±128.6 491.3±122.2
Electrophysiological characteristics of iPSC-derived beating EBs as assessed by MEA including beats per minute, interspike interval, and field potential duration.

10
Table S3 (Referenced from Figure 6). Drug screening of HCM iPSC-CMs for treatment of contractile arrhythmia
Drug Class Target Video
Analysis Therapeutic
Effect Concentrations
Tested
Quinidine Ia Na+ channel blocker
(intermediate association/dissociation)
× no 0.1-20 uM
Procainamide Ia Na+ channel blocker
(intermediate association/dissociation)
× no 1-200 uM
Lidocaine Ib Na+ channel blocker (fast association/ dissociation)
× yes 1-100 nM
Mexiletine Ib Na+ channel blocker (fast association/ dissociation)
× yes 1-50 uM
Ranolazine NA Late Na+ channel blocker × yes 0.1-10 uM
Flecainide Ic Na+ channel blocker (slow association/ dissociation)
× no 0.1-5 uM
Propafenone Ic Na+ channel blocker (slow association/ dissociation)
× no 1-100 uM
Propranolol II Beta-blocker × no 1-400 uM
Metoprolol II Beta-blocker × no 0.1-20 uM
Amiodarone II K+ channel blocker × no 0.1-10 uM
Sotalol III K+ channel blocker × no 1-400 uM
Dofetilide III K+ channel blocker × no 0.1-20 uM
Verapamil
IV Ca2+ channel blocker × yes* 1-100 uM
Diltiazem IV Ca2+ channel blocker
yes* 1-100 uM
Nifedipine NA Ca2+ channel blocker
yes 1-100 uM
Information of pharmacological agents used in screening assays for HCM iPSC-CMs. * Verapamil/Diltiazem were only observed to have a therapeutic effect upon HCM iPSC-CMs following continuous addition to the culture media for 5 or more days in a row. Treatment for a period of time less than 5 days was not observed to have any therapeutic effects upon Ca2+ handling or arrhythmogenicity. All other drug screening assays were conducted by incubating cells with respective pharmaceutical compounds at the listed concentrations for 10 minutes followed by washout.

11
SUPPLEMENTAL EXPERIMENTAL PROCEDURES
Patient recruitment. Clinical evaluation of the proband and family included physical
examination, cardiac echocardiography, ECG, cardiac magnetic resonance imaging (MRI), and
24-hour Holter monitoring. Results revealed hyperdynamic ventricular systolic function with
near complete obliteration of the apical walls at end systole in the proband (II-1) and the eldest
two carriers (III-1 and III-2). No delayed enhancement was found on contrast enhanced MRI in
the proband or carriers. Ambulatory monitoring revealed occasional premature ventricular
contractions. The youngest two carriers (III-3 and III-8; ages 14 and 10) exhibited hyperdynamic
cardiac function but no other clinical features of HCM most likely due to their young age.
Isolation and maintenance of fibroblast cells. Freshly isolated skin biopsies were rinsed with
PBS and transferred into a 1.5 ml tube. Tissue was minced in collagenase I (1 mg/ml in
Dulbecco’s modified Eagle medium (DMEM), Invitrogen, Carlsbad, CA) and allowed to digest
for 6 hours at 37 . Dissociated dermal fibroblasts were plated and maintained with DMEM
containing 10% FBS (Invitrogen), Glutamax (Invitrogen), 4.5 g/L glucose (Invitrogen), 110
mg/L sodium pyruvate (Invitrogen), 50 U/mL penicillin (Invitrogen), and 50 g/mL streptomycin
(Invitrogen) at 37 °C, 95% air, and 5% CO2 in a humidified incubator. All cells were used for
reprogramming within five passages.
Lentivirus production and transduction. 293FT cells (Invitrogen) were plated at 80%
confluency on 100-mm dishes and transfected with 12 μg of the lentiviral vectors (OCT4, SOX2,
KLF4, and c-MYC) plus 8 μg of packaging pPAX2 and 4 μg of VSVG plasmids using
Lipofectamine 2000 (Invitrogen) following the manufacturer’s instructions. Supernatant was
collected 48 h after transfection, filtered through a 0.45-μm pore-size cellulose acetate filter

12
(Millipore, Billerica, MA), and mixed with PEG-it Virus Concentration Solution (System
Biosciences, Mountain View, CA) overnight at 4°C. Viruses were precipitated at 1,500 g the
next day and resuspended with Opti-MEM medium (Invitrogen).
Derivation of patient-specific iPSCs. Generation, maintenance, and characterization of patient-
specific iPSC lines were performed as previously described using lentivirus as produced above
on Matrigel-coated tissue culture dishes (BD Biosciences, San Jose, CA) with mTESR-1 hESC
Growth Medium (StemCell Technology, Vancouver, Canada) (Sun et al., 2009).
Alkaline phosphatase staining. Alkaline phosphatase (AP) staining was conducted as in
previous studies using the Quantitative Alkaline Phosphatase ES Characterization KitS
(Millipore) using the manufacturer’s instructions (Sun et al., 2009).
Immunofluorescence staining. Immunofluorescent stains were performed using the following
primary antibodies: SSEA-3, SSEA-4, TRA-1-60, TRA-1-81, ANF, TUJ-1 (Millipore), OCT3/4,
Nanog, AFP (Santa Cruz, CA), SOX2 (Biolegend, San Diego, CA), smooth muscle actin
(Biolegend), sarcomeric α-actinin (Sigma, St. Louis, MO), (cTNT (Thermo Scientific Barrington,
IL), Alexa Fluor 488 Phalloidin (invitrogen), Myosin light chain 2a (MLC2a), Myosin light
chain 2v (MLC2v) (Synaptic Systems, Goettingen, Germnay), NFATc4 (Santa Cruz, Santa Cruz,
CA), and AlexaFluor conjugated secondary antibodies (Invitrogen) as previously described (Sun
et al., 2009).
Bisulphite pyrosequencing. The Zymo DNA Methylation Kit (Zymo Research, Irvine, CA) was
used to treat 1 μg of sample DNA with bisulfite as per the manufacturer’s instructions. Following

13
PCR, cDNA was converted to single-stranded DNA templates and sequenced by a
Pyrosequencing PSQ96 HS System (Biotage, Charlotte, NC). QCpG software (Biotage) was
used to analyze each individual locus as a T/C SNP.
Microarray hybridization and data analysis. RNA was isolated from iPSCs and hybridized to
an Affymetrix GeneChip Human Gene 1.0 ST Array (Affymetrix, Santa Clara, CA). Expression
was normalized and annotated by the Affymetrix Expression Console software (Affymetrix). The
Pearson Correlation Coefficient was calculated for each pair of samples using the expression
level of transcripts which shows standard deviation greater than 0.2 among all samples.
Spontaneous in vitro differentiation. For embroid body (EB) formation, iPSC colonies were
dissociated on Matrigel coated plates with collagenase Ⅳ (Invitrogen), and seeded into low
attachment 6-well plates in Knockout DMEM (Invitrogen) containing 15% KSR (Invitrogen),
Glutamax (Invitrogen), 4.5 g/L glucose (Invitrogen), 110 mg/L sodium pyruvate (Invitrogen), 50
U/mL penicillin (Invitrogen), and 50 g/mL streptomycin (Invitrogen) to form embroid bodies
(EBs). After 5 days, EBs were transferred to adherent, gelatin-coated chamber slides and
cultured in the same medium for another 8 days.
Teratoma formation. 1x106 undifferentiated iPSCs were suspended in 10 µL Matrigel (BD
Biosciences) and delivered by a 28.5 gauge syringe to the subrenal capsule of 8 week old SCID
Beige mice. Eight weeks after cell delivery, tumors were explanted for hematoxylin and eosin
staining.

14
Western blot. Whole cell extracts were isolated using RIPA buffer and 10 µg protein was
analyzed by Western blot using specific antibodies against OCT4, c-MYCc, KLF4, ACTIN
(Santa Cruz), and SOX2 (Biolegend).
Cardiac differentiation of human ESCs and iPSCs. Human H9 ESCs and iPSCs were
differentiated into cardiomyocytes as previously described (Sun et al., 2012). Briefly, pluripotent
stem cells were dissociated with accutase (Sigma) at 80% confluence into small clumps of 10-20
cells. Cells were resuspended in 2 ml basic media containing StemPro34 (Invitrogen), 2 mM
glutamine (Invitrogen), 0.4 mM monothioglycerol (Sigma), 50 μg/ml ascorbic acid (Sigma), and
0.5 ng/ml BMP4 (R&D Systems, Minneapolis, MN) to form EBs. For days 1-4 of cardiac
differentiation, cells were treated with 10 ng/ml BMP4, 5 ng/ml human bFGF (R&D Systems),
and 3 ng/ml activin A (R&D Systems) added to the basic media. From days 4-8, EBs were
refreshed with basic media containing human 50 ng/ml DKK1 (R&D Systems) and 10 ng/ml
human VEGF (R&D Systems). From day 8 onwards, cells were treated with basic media
containing 5 ng/ml human bFGF and 10 ng/ml human VEGF. Cultures were maintained in a 5%
CO2/air environment.
Measurement of cardiomyocyte size and sarcomeric content. For single cell cardiomyocyte
analysis, beating EBs were plated on gelatin-coated dishes. Three days after plating, EBs were
trypsinized, filtered through a 40-mm size pore-size filter, and single cells re-plated at low
density on gelatin-coated chamber slides (Nalgene Nunc International, Rochester, NY). Three
days after re-plating, cells were fixed with 4% paraformaldehyde (Sigma), permeabilized in 0.3%
Triton (Sigma), blocked using 5% BSA, and stained for cardiac troponin T (1:200, Thermo
15
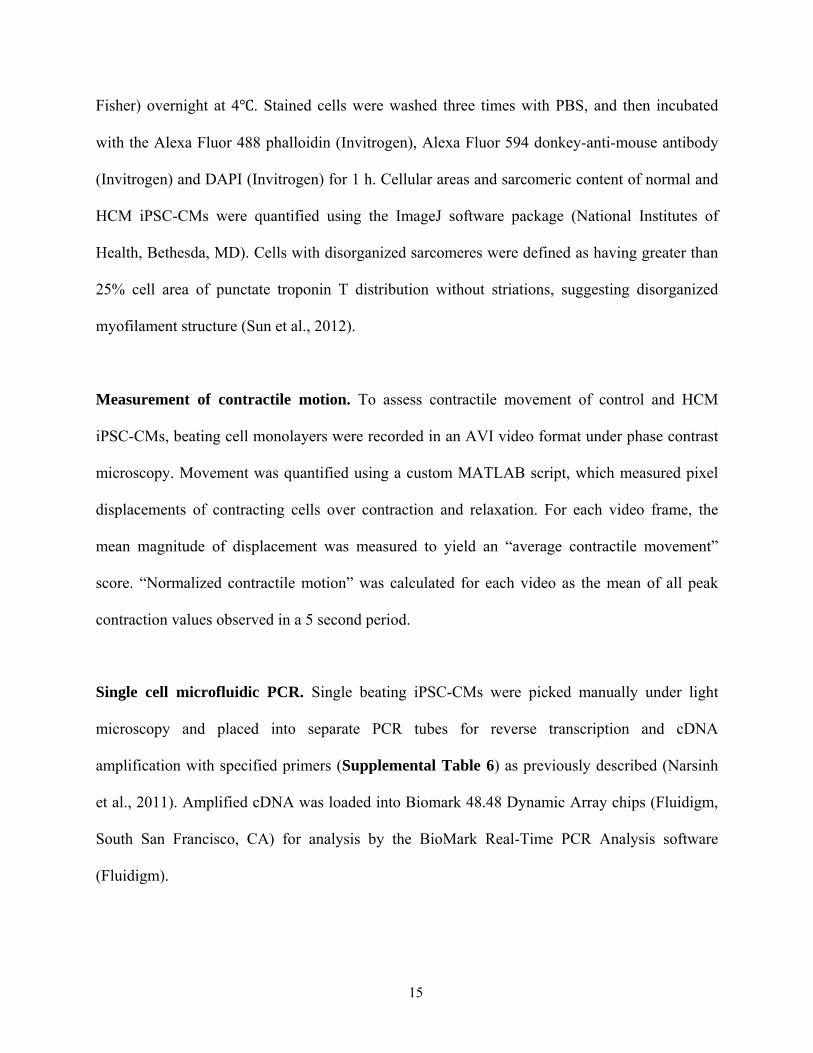
Fisher) overnight at 4 . Stained cells were washed three times with PBS, and then incubated
with the Alexa Fluor 488 phalloidin (Invitrogen), Alexa Fluor 594 donkey-anti-mouse antibody
(Invitrogen) and DAPI (Invitrogen) for 1 h. Cellular areas and sarcomeric content of normal and
HCM iPSC-CMs were quantified using the ImageJ software package (National Institutes of
Health, Bethesda, MD). Cells with disorganized sarcomeres were defined as having greater than
25% cell area of punctate troponin T distribution without striations, suggesting disorganized
myofilament structure (Sun et al., 2012).
Measurement of contractile motion. To assess contractile movement of control and HCM
iPSC-CMs, beating cell monolayers were recorded in an AVI video format under phase contrast
microscopy. Movement was quantified using a custom MATLAB script, which measured pixel
displacements of contracting cells over contraction and relaxation. For each video frame, the
mean magnitude of displacement was measured to yield an “average contractile movement”
score. “Normalized contractile motion” was calculated for each video as the mean of all peak
contraction values observed in a 5 second period.
Single cell microfluidic PCR. Single beating iPSC-CMs were picked manually under light
microscopy and placed into separate PCR tubes for reverse transcription and cDNA
amplification with specified primers (Supplemental Table 6) as previously described (Narsinh
et al., 2011). Amplified cDNA was loaded into Biomark 48.48 Dynamic Array chips (Fluidigm,
South San Francisco, CA) for analysis by the BioMark Real-Time PCR Analysis software
(Fluidigm).

16
Calcium (Ca2+) imaging. iPSC-CMs were dissociated and seeded in gelatin-coated 8-well LAB-
TEK® II chambers (Nalgene Nunc International) for calcium imaging. Cells were loaded with 5
μM Fluo-4 AM (Invitrogen) and 0.02 % Pluronic F-127 (Invitrogen) in Tyrodes solution (140
mM NaCl, 5.4 mM KCl, 1 mM MgCl2, 10 mM glucose, 1.8 mM CaCl2, and 10 mM HEPES pH
7.4 with NaOH at 25°C) for 15 min at 37°C. Following Fluo-4 loading, cells were washed three
times with Tyrodes solution. Imaging was conducted with a confocal microscope (Carl Zeiss,
LSM 510 Meta, Göttingen, Germany) with a 63x lens using Zen software (Carl Zeiss). For paced
calcium dye imaging, fluorescence was measured at 495 + 20 nm excitation and 515 ± 20 nm
emission. Videos were taken at 20 fps for 10 s recording durations. Cells were stimulated at 1
and 2 Hz. Measurements were taken on an AxioObserver Z1 (Carl Zeiss) inverted microscope
equipped with a Lambda DG-4 300 W Xenon light source (Sutter Instruments, Novato, CA), an
ORCA-ER CCD camera (Hamamatsu, Bridgewater, NJ), and AxioVison 4.7 software (Carl
Zeiss). In each video frame, regions of interest (ROIs) were analyzed for changes in dye
intensity f/f0, with the resting fluorescence value f0 determined at the first frame of each video.
Background intensity was subtracted from all values, and plots were normalized to zero.
Measurement of basal [Ca2+]i using Indo-1-AM. Cardiomyocytes were loaded in a culture
medium containing 5 µM Indo-1 AM (Invitrogen) and 0.02% Pluronic F-127 (Invitrogen) for 20
minutes at 37C. After Indo-1 loading, cells were washed three times with 2 mM Ca2+ Ringer
(155 mM NaCl, 4.5 mM KCl, 2 mM CaCl2, 1 mM MgCl2, 10 mM D-glucose, and 5 mM Na-
HEPES, pH 7.4) and incubated for 20 minutes at room temperature to allow for Indo-1 de-
esterification. Cardiomyocytes were imaged in 2 Ca2+ Ringer at 32C using a Zeiss Axiovert
200M epifluorescence microscope. Indo-1 was excited at 350 ± 10 nm using a 0.6 UVND filter

17
(to attenuate excitation intensity) and a 400 DCLP. The emitted light was separated using a
Cairn Optosplit II (425 dichroic, 488/22 bandpass filter, Kent, UK). Spontaneous Ca2+ transients
were collected with 4 x 4 pixel binning in stream acquisition mode using Metamorph software
(Molecular Devices, Sunnyvale, CA) at 100 ms exposures. For image analysis, short and long
wavelength emission channels were aligned using the Cairn Image Splitter ImageJ plugin.
Caffeine treatment of iPSC-CMs. Cells were perfused with PBS containing 1.8 mM Ca2+ and 1
mM Magnesium and paced at 1 Hz to view regular transients. A two second puff of 20 mM stock
caffeine solution was delivered through a perfusion apparatus. Pacing was turned off prior to
caffeine reaching the cells in order to accurately measure Ca2+ release.
Analysis of calcium imaging linescans. Average fluorescence intensity for Ca2+ linescans was
quantified using Fiji (National Institutes of Health). Timing between transients was defined as
the time between the peaks of two successive spikes. The Ca2+ baseline was defined as the
median of all minima of transients. Irregularity for spike timing was defined as the ratio of the
standard deviation (s.d.) to the mean.
Microelectrode array (MEA) recordings. Control and HCM iPSCs were differentiated into
beating EBs ranging from 60-80% purity of CMs and seeded onto multi-electrode arrays for
recording of field potential duration (FPD) and beating frequency (beats per minute, BPM) and
interspike intervals (ISI). Beating iPSC-CM EBs were plated on gelatin-coated MEA probes
(Alpha Med Scientific, Osaka, Japan) prior to experiments 20-40 days post-differentiation.
Signals were acquired at 20 kHz with a MED64 amplifier (Alpha Med Scientific) and digitized

18
using a PC with PCI -6071 A/D cards (National Instruments, Austin, TX) running MED64
Mobius QT software (Witwerx, Inc., Tustin, CA). All experiments were performed at 35.8 to
37.5°C in DMEM without serum or antibiotics. Stock verapamil solutions were made in double
distilled water at a 50 mM concentration. Dose-response experiments were performed by adding
0.4 to 2 µL of 1000x verapamil concentrations in DMEM to the 1-2 ml volume in the MEA
probe for 10 minutes at each dose. Beating frequencies and field potential waveform data were
extracted offline using Mobius QT and saved as CSV files. Waveform data was imported into
IGOR Pro (Wavemetrics, Portland, OR) for FPD and Vmax measurements. Beat frequencies
were normalized to baseline for verapamil dose-response experiments and FPDs were adjusted to
the beat frequency using the Bazett correction formula: cFPD = FPD/√Interspike interval.
Patch clamping. Whole-cell patch-clamp recordings were conducted using an EPC-10 patch-
clamp amplifier (HEKA, Lambrecht, Germany). Contracting EBs were mechanically isolated,
enzymatically dispersed into single cells and attached to gelatin-coated glass coverslips (CS-
22/40, Warner, Hamden, CT). While recordings, the coverslips containing plated cardiomyocytes
or the hERG-HEK293 cells were transferred to a RC-26C recording chamber (Warner) mounted
on to the stage of an inverted microscope (Nikon, Tokyo, Japan). The glass pipettes were
prepared using thin-wall borosilicate glass (Warner) using a micropipette puller (Sutter
Instrument, Novato, CA), polished using a microforge (Narishige, Tokyo, Japan) and had
resistances between 2-4 MΩ. Extracellular solution perfusion was continuous using a rapid
solution exchanger (Bio-logic, Grenoble, France) with solution exchange requiring 1 min. Data
were acquired using PatchMaster software (HEKA, Germany) and digitized at 1.0 kHz. Data
were analyzed using PulseFit (HEKA), Igor Pro (Wavemetrics, Portland, OR), Origin 6.1

19
(Microcal, Northampton, MA), and Prism (Graphpad, La Jolla, CA). For the whole-cell patch
clamp recordings of human cardiomyocytes generated from iPSCs, temperature was maintained
constant by a TC-324B heating system (Warner) at 36-37°C. Current-clamp recordings were
conducted in normal Tyrode solution containing 140 mM NaCl, 5.4 mM KCl, 1 mM MgCl2, 10
mM glucose, 1.8 mM CaCl2 and 10 mM HEPES (pH 7.4 with NaOH at 25°C). The pipette
solution contained 120 mM KCl, 1 mM MgCl2, 10 mM HEPES, 3 mM Mg-ATP, and 10 mM
EGTA (pH 7.2 with KOH at 25°C). Verapamil (Sigma) was dissolved in H2O and prepared as a
10 mM stock in a glass vial. The stock solution was mixed vigorously for 10 min at room
temperature. For testing, the compound was diluted in a glass vial using external solution; the
dilution was prepared no longer than 30 min before using. Equal amounts of DMSO (0.1%)
were present at final dilution.
Quantitative RT-PCR. Total mRNA was isolated using TRIZOL and 1 µg was used to
synthesize cDNA using the SuperscriptⅡ cDNA synthesis kit (Invitrogen). 0.25 µL of the
reaction mixture was used to quantify gene expression by qPCR using SYBR® Green Master
Mix (Invitrogen). Expression values were normalized to the average expression of GAPDH.
Drug treatment. Single contracting iPSC-CMs were treated with pharmaceutical agents for 10
minutes for immediate analysis followed by wash out. The respective concentrations of each
drug tested are listed in Supplemental Table 5. For inotropic stimulation experiments, 200 µM
isoproterenol and 400 µM propranolol were added to the cell medium for 5 continuous days.
Verapamil treatment was conducted by adding 50 µM and 100 µM to the culture medium of
iPSC-CMs for 10-20 continuous days on a daily basis.

20
SUPPLEMENTAL REFERENCES Narsinh, K.H., Sun, N., Sanchez-Freire, V., Lee, A.S., Almeida, P., Hu, S., Jan, T., Wilson, K.D., Leong, D., Rosenberg, J., et al. (2011). Single cell transcriptional profiling reveals heterogeneity of human induced pluripotent stem cells. The Journal of Clinical Investigation 121, 1217-1221. Sun, N., Panetta, N.J., Gupta, D.M., Wilson, K.D., Lee, A., Jia, F., Hu, S., Cherry, A.M., Robbins, R.C., Longaker, M.T., et al. (2009). Feeder-free derivation of induced pluripotent stem cells from adult human adipose stem cells. Proceedings of the National Academy of Sciences of the United States of America 106, 15720-15725. Sun, N., Yazawa, M., Liu, J., Han, L., Sanchez-Freire, V., Abilez, O.J., Navarrete, E.G., Hu, S., Wang, L., Lee, A., et al. (2012). Patient-specific induced pluripotent stem cells as a model for familial dilated cardiomyopathy. Science Translational Medicine 4, 130ra147.