Abnormal Biomarkers of Homocysteine Metabolism in Neonates ... · ResearchArticle Abnormal...
6
Research Article Abnormal Biomarkers of Homocysteine Metabolism in Neonates with Conotruncal Heart Defects Piotr Surmiak, MaBgorzata Baumert, and Magdalena Paprotny Department of Neonatology, School of Medicine in Katowice, Medical University of Silesia, Katowice, Poland Correspondence should be addressed to Piotr Surmiak; [email protected] Received 25 January 2017; Revised 4 May 2017; Accepted 28 June 2017; Published 27 July 2017 Academic Editor: Betti Giusti Copyright © 2017 Piotr Surmiak et al. is is an open access article distributed under the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Objectives. e etiology of conotruncal heart defects (CHD) remains unknown; however relation between homocysteine, folate levels, and congenital heart disease was found. With this perspective in mind, the aim of the study was to investigate biomarkers of homosyteine metabolism pathway in mothers and their neonates with CHD. Material and Methods. Forty-three pairs of mothers and their neonates with CHD and forty pairs of mothers and neonates with nonconotruncal heart defects (non-CHD) were enrolled. e control group (CG) consisted of fiſty-nine pairs of mothers and their healthy neonates. For estimating the plasma total homocysteine (tHcy), serum folates, and cobalamin levels, mothers’ venous blood samples and umbilical cord blood were taken in all groups. Results. We observed higher tHcy levels in newborns with CHD in comparison to their mothers and to neonates with non-CHD. Cobalamin levels were significantly lower in neonates with CHD compared to other children. Folates and cobalamin levels were lower in CHD mothers compared to their children. Conclusions. Elevated homocysteine levels in neonates with CHD and folate metabolism disturbances in their mothers were noticed. e observed differences in homocysteine and cobalamin levels between neonates with CHD suggest the influence of various agents disturbing homocysteine metabolic pathways. 1. Introduction e most common problem of contemporary perinatology is a high number of congenital anomalies of which conotruncal heart defects (CHD) are one of the common defects in the developmental period [1, 2]. Conotruncal heart defects represent an anatomically heterogeneous group of cardiac malformations affecting the outflow tract of the ventricles and the arterial pole of the heart. According to current knowledge, more than 80% of congenital defects with recognized etiology are stimulated by genetic and environmental factors [2]. Chief among the aforementioned influences was a deficiency of essential microelements and vitamins in the preconception period, such as the B-vitamins (i.e., folic acid and cobalamin). Some reports suggested that folates play a key role in utilization reactions of many biogenic compounds, including homocysteine [3, 4]. Recent studies suggested that maternal hyperhomocys- teinemia is an independent risk factor for congenital heart defects, by interfering with the development of conotruncal septum of the heart [5, 6]. e aim of our study was to evaluate the differences in total homocysteine (tHcy), folate, and cobalamin levels of maternal and umbilical cord blood samples in groups of children with congenital heart defects. 2. Material and Method A prospective, case-control study was conducted in the Department of Neonatology at the Medical University of Silesia in Katowice between January 2012 and January 2015. e study was approved by the Ethics Committee of the Medical University of Silesia (nr KNW/0022/KB1/25/13). Among 1,271 childbirths in our unit at the time of the study we enrolled 83 neonates (6.5%) with prenatally diag- nosed congenital heart defects. e control group (CG) is comprised of 59 pairs of healthy mothers residing in the unit during the study and their healthy, full-term newborns. All mothers from the study group underwent at least two prenatal examinations in which the congenital heart defects were diagnosed. Congenital heart defects in neonates Hindawi BioMed Research International Volume 2017, Article ID 7404397, 5 pages https://doi.org/10.1155/2017/7404397
Transcript of Abnormal Biomarkers of Homocysteine Metabolism in Neonates ... · ResearchArticle Abnormal...
-
Research ArticleAbnormal Biomarkers of Homocysteine Metabolism inNeonates with Conotruncal Heart Defects
Piotr Surmiak, MaBgorzata Baumert, andMagdalena Paprotny
Department of Neonatology, School of Medicine in Katowice, Medical University of Silesia, Katowice, Poland
Correspondence should be addressed to Piotr Surmiak; [email protected]
Received 25 January 2017; Revised 4 May 2017; Accepted 28 June 2017; Published 27 July 2017
Academic Editor: Betti Giusti
Copyright © 2017 Piotr Surmiak et al. This is an open access article distributed under the Creative Commons Attribution License,which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited.
Objectives. The etiology of conotruncal heart defects (CHD) remains unknown; however relation between homocysteine, folatelevels, and congenital heart disease was found. With this perspective in mind, the aim of the study was to investigate biomarkers ofhomosyteine metabolism pathway in mothers and their neonates with CHD. Material and Methods. Forty-three pairs of mothersand their neonates with CHD and forty pairs of mothers and neonates with nonconotruncal heart defects (non-CHD) wereenrolled.The control group (CG) consisted of fifty-nine pairs ofmothers and their healthy neonates. For estimating the plasma totalhomocysteine (tHcy), serum folates, and cobalamin levels, mothers’ venous blood samples and umbilical cord blood were taken inall groups. Results. We observed higher tHcy levels in newborns with CHD in comparison to their mothers and to neonates withnon-CHD. Cobalamin levels were significantly lower in neonates with CHD compared to other children. Folates and cobalaminlevels were lower in CHD mothers compared to their children. Conclusions. Elevated homocysteine levels in neonates with CHDand folate metabolism disturbances in their mothers were noticed.The observed differences in homocysteine and cobalamin levelsbetween neonates with CHD suggest the influence of various agents disturbing homocysteine metabolic pathways.
1. Introduction
Themost common problem of contemporary perinatology isa high number of congenital anomalies of which conotruncalheart defects (CHD) are one of the common defects inthe developmental period [1, 2]. Conotruncal heart defectsrepresent an anatomically heterogeneous group of cardiacmalformations affecting the outflow tract of the ventricles andthe arterial pole of the heart. According to current knowledge,more than 80%of congenital defects with recognized etiologyare stimulated by genetic and environmental factors [2]. Chiefamong the aforementioned influences was a deficiency ofessential microelements and vitamins in the preconceptionperiod, such as the B-vitamins (i.e., folic acid and cobalamin).Some reports suggested that folates play a key role inutilization reactions of many biogenic compounds, includinghomocysteine [3, 4].
Recent studies suggested that maternal hyperhomocys-teinemia is an independent risk factor for congenital heartdefects, by interfering with the development of conotruncalseptum of the heart [5, 6].
The aim of our study was to evaluate the differences intotal homocysteine (tHcy), folate, and cobalamin levels ofmaternal and umbilical cord blood samples in groups ofchildren with congenital heart defects.
2. Material and Method
A prospective, case-control study was conducted in theDepartment of Neonatology at the Medical University ofSilesia in Katowice between January 2012 and January 2015.The study was approved by the Ethics Committee of theMedical University of Silesia (nr KNW/0022/KB1/25/13).
Among 1,271 childbirths in our unit at the time of thestudy we enrolled 83 neonates (6.5%) with prenatally diag-nosed congenital heart defects.
The control group (CG) is comprised of 59 pairs of healthymothers residing in the unit during the study and theirhealthy, full-term newborns.
All mothers from the study group underwent at leasttwo prenatal examinations in which the congenital heartdefects were diagnosed. Congenital heart defects in neonates
HindawiBioMed Research InternationalVolume 2017, Article ID 7404397, 5 pageshttps://doi.org/10.1155/2017/7404397
https://doi.org/10.1155/2017/7404397
-
2 BioMed Research International
were confirmed by echocardiography performed as soon aspossible after delivery.
The exclusion criteria comprised neonates with chromo-somal aberrations, complex congenital malformations, new-borns frommultiple pregnancies, and neonates with evidenceof congenital infections, as well as those that were born tomothers with clinical chorioamnionitis. We also excludedmothers who administered medications during pregnancy,which could possibly affect homocysteine and vitamin Bmetabolism (i.e., folate antagonists, antiepileptic drugs, oralcontraceptives, barbiturates, and levodopa) within the periodof six months before conception, as well as pregnant womensuffering from hypertension, thromboembolic diseases, kid-ney, and heart defects. Neonates from the control groupunderwent a cranial ultrasound and an echocardiographicexamination after delivery.
All included mothers and their children with prenatallydiagnosed congenital heart defect were divided into twosubgroups: with conotruncal heart defects (CHD, 𝑛 = 43)and nonconotruncal heart defects (non-CHD, 𝑛 = 40). CHDgroup included neonates with diagnosed Persistent TruncusArteriosus, PTA (𝑛 = 13, 30.1%), Tetralogy of Fallot, TOF(𝑛 = 11, 25.6%), Interrupted Aortic Arch, IAA (𝑛 = 6, 13.9%),and Double Outlet Right Ventricle, DORV (𝑛 = 5, 11.6%).
Nonconotruncal heart defects (non-CHD) comprisedchildren with Atrial Septum Defect, ASD (𝑛 = 16, 40.0%),Ventricular Septum Defect, VSD (𝑛 = 15, 37.5%), andAtrioventricular Septal Defect, AVSC (𝑛 = 9, 22.5%). Allcongenital anomalies were reported to the Polish Registry ofCongenital Malformations.
2.1. Laboratory Performances. During childbirth, 5 millilitersof maternal blood was collected from ulnar vein and 5 ml ofblood from umbilical artery from the placental side.
All blood samples were collected in EDTA-containingtubes, centrifuged for 10 minutes (2500 rotations/min) andstored at −70∘C until full analysis had beenmade.The follow-ing was assessed: folate, cobalamin, and total homocysteineconcentrations. Folate and cobalamin in serum were deter-mined with the aid of microparticle enzyme immunoassay(MEIA), using ABBOTT reagent sets in an immunochemicalanalyzer (AxSYM). Total homocysteine concentration inplasmawas determined by an immunochemicalmethodwiththe fluorescence polarization immunoassay (FPIA) using anIMx analyzer and special ABBOTT sets. All procedures wererecommended by the ABBOTT company which producestesting sets used in our examination.
2.2. Statistical Analysis. Results were analyzed statisticallywith the certified program STATISTICA 10 (StatSoft PolskaInc.). The distribution of the data was analyzed by theShapiro-Wilk test. Results were presented as means andstandard deviations or as percentiles of the total. Baselinecharacteristics and biomarkers of homocysteine metabolismbetween all study groups were compared using Kruskal-Wallis test, 𝑈Mann–Whitney test, or chi square tests.
The association between variables was measured by aSpearman’s rank correlation test. For all the statistical proce-dures 𝑝 value < 0.05 was considered to be significant.
Umbilical cord bloodExtreme values
Mothers’ venous bloodExtreme values
CHD Non-CHD ControlsGroup
0
5
10
15
20
25
30
35
40
Tota
l hom
ocys
tein
e lev
el (u
mol
/l)
∗
∗
∗
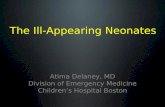
Figure 1: Maternal and umbilical cord blood total homocysteineconcentrations in conotruncal heart defects (CHD), nonconotrun-cal heart defects (non-CHD), and controls (CG). Results presentedasmeans and standard deviations aswell as 95% confidence intervalsand extreme values. ∗Extreme values.
3. Results
Mothers and their neonates from all investigated groupswere comparable to controls with respect to demographic-perinatal characteristics, presented in Table 1.
We have noticed that daily dietary supplementation offolic acid (0.4mg) was taken by 86.0% (𝑛 = 37) of mothersfrom CHD group, 87.5% (𝑛 = 35) of mothers from non-CHD group, and 89.8% (𝑛 = 53) from controls. However,those results were not statistically significant (𝑝 = 0.3). Weobserved no relevant differences in creatinine levels in allinvestigated mothers (CHD 0.75mg/dl, non-CHD 0.72mg/dl, CG 0.74mg/dl, 𝑝 = 0.7).
3.1. Total Homocysteine Levels. In our study, we observedsignificantly higher tHcy levels in umbilical cord blood innewborns with CHD compared to their mothers. Significantdifferences in tHcy concentrations were observed in umbili-cal cord blood between CHD compared to non-CHD groups.We also noticed higher umbilical cord tHcy levels in CHDneonates compared to controls.
However, we observed no significant differences in tHcylevels in neonates with non-CHD in comparison to theirmothers and to controls.
We found no relevant differences in tHcy between moth-ers in all investigated groups.
All results are presented on Figure 1 and Table 2.
3.2. Folate Levels. No differences were shown in umbilicalcord folate levels in all investigated children. However, we
-
BioMed Research International 3
Table 1: Demographic characteristics of investigated neonates and their mothers.
Variable Conotruncal heart defects(𝑛 = 43)Nonconotruncal heart defects
(𝑛 = 40)Controls(𝑛 = 59) 𝑝 value
Mothers(i) Age (years) 26 [4.3] 29 [5.8] 31 [5.4] 0.5(ii) Primigravida [𝑛,%] 26, 60.5% 27, 67.5% 35, 59.3% 0.4(iii) Dietary supplementation of folic acid [𝑛,%] 37, 86.0% 35, 87.5% 53, 89.8% 0.3(iv) Delivery mode: caesarean section [𝑛,%] 26, 60.5% 22, 55.0% 30, 50.8% 0.1Newborns(i) Gender female [𝑛,%] 20, 46.5% 23, 57.5% 30, 50.8% 0.7(ii) Gestational age (weeks) 38.5 [3.6] 37 [2.7] 39.5 [4.2] 0.6(iii) Birth weight (g) 3090 [620] 3313 [840] 3230 [750] 0.4(iv) Head circumference (cm) 34.5 [2.0] 34.5 [1.5] 34.0 [2.5] 0.1(v) Body length (cm) 53.0 [1.5] 54.5 [2.5] 53.5 [1.5] 0.5(vi) Apgar 1st min [𝑛,%]
0–3 pts 2, 4.7% 1, 2.3% 0 0.64–7 pts 5, 11.6% 8, 20.0% 8, 13.6%8–10 pts 36, 83.7% 32, 80.0% 51, 86.4%
(vii) Apgar 5th min [𝑛,%]0–3 pts 0 0 0 0.54–7 pts 2, 4.7% 6, 15.0% 5, 8.5%8–10 pts 41, 95.3% 34, 85.0% 54, 81.5%
Results are shown as mean and standard deviation [SD] or percentile; 𝑝 value from Kruskal-Wallis test or chi square test.
Table 2: Total homocysteine (tHcy), folate, and cobalamin levels in umbilical cord blood andmothers’ venous blood samples in all investigatedgroups.
Variable Conotruncal heart defects(𝑛 = 43)
Nonconotruncal heart defects(𝑛 = 40)
Controls(𝑛 = 59) p value
Umbilical cord blood(i) tHcy level [𝜇mol/l] 12.6 [2.4] 7.7 [2.3] 8.1 [2.6] 0.01(ii) Folate level [ng/ml] 13.7 [4.1] 14.3 [2.7] 15.0 [1.3] 0.2(iii) Cobalamin level [pg/ml] 300.5 [95.7] 425.1 [120.7] 325.4 [105.2]
-
4 BioMed Research International
Umbilical cord bloodExtreme values
Mothers’ venous bloodExtreme values
CHD Non-CHD ControlsGroup
0
5
10
15
20
25
30
35
40
Folat
e lev
el (n
g/m
l)
∗
Figure 2: Maternal and umbilical cord blood folate concentrationsin conotruncal heart defects (CHD), nonconotruncal heart defects(non-CHD), and controls (CG). Results presented as means andstandard deviations as well as 95% confidence intervals and extremevalues. ∗Extreme values.
4. Discussion
In this study, we analyzed biomarkers of the folate-dependenthomocysteine pathway metabolism in neonates with con-genital heart defects and their mothers. We noticed elevatedhomocysteine levels in umbilical cord blood in neonatesborn with conotruncal heart defects in comparison to new-borns with nonconotruncal heart defects. However, somestudies indicate maternal elevated homocysteine level asa main risk factor for congenital heart defects in theiroffspring [7, 8]. We did not observe such differences inhomocysteine levels between investigated mothers. Perhapsthose differences are the result of the proportionally smallgroup of participants in our study. Additionally, our studydemonstrated decreased cobalamin levels in neonates withcongenital heart defects and their mothers compared to con-trols. Some studies presented cobalamin and folate deficiencyin pregnancy complicated by congenital anomaly, which maysuggest inadequate daily folic acid and cobalamin dietarysupplementation during pregnancy [9, 10]. Different resultsare presented by Hobbs et al., where vitamin B-12 andfolic acid concentrations did not differ significantly betweenmothers with congenital heart defect and control subjects[8]. However, other authors suggested that congenital heartanomalies are associated with low maternal folate as well aswith hyperhomocysteinemia [11, 12]. Authors revealed thatcobalamin and folate administration may help to reduce thedevelopment of cardiac malformations [13, 14].
The etiology of conotruncal heart diseases is complex,with both environmental and genetic causes. It has been
Umbilical cord bloodExtreme values
Mothers’ venous bloodExtreme values
0
100
200
300
400
500
600
700
Cob
alam
in le
vel (
pg/m
l)
CHD Non-CHD ControlsGroup
Figure 3: Maternal and umbilical cord blood cobalamin concen-trations in conotruncal heart defects (CHD), nonconotruncal heartdefects (non-CHD), and controls (CG). Results presented as meansand standard deviations as well as 95% confidence intervals andextreme values.
well documented that hyperhomocysteinemia, which is oftenaccompanied by the defects of folic acid metabolism, isassociated with the occurrence of congenital defects, and itseems to be an independent risk factor of conotruncal heartdefects [15–17].
Based on our results, we postulated that mothers’ homo-cysteine levels had no direct influence on the developmentof conotruncal heart defects. Thus, we suggested that hyper-homocysteinemia and decreased folate levels observed inumbilical cord bloodmay be associated with the disturbancesin homocysteine pathway metabolism in newborns withCHD. Zhao et al. found in children with CHD a gene muta-tion coding for an enzyme, which plays an important rolein the homocysteine remethylation process [18]. It is prob-able that, in fetuses with CHD, the excess homocysteine ismetabolized by remethylation, as we discovered a decreasedconcentration of folic acid in children with CHD comparedto those with non-CHD.
According to Solanky et al., remethylation of Hcy tomethionine using methyl donation from folate is the preva-lent pathway in the human placenta, indicating a markedreliance on folate availability [19]. Consequently, vitamin Bdeficiency in mothers whose offspring have congenital mal-formations additionally causes a disturbance in the mainpathway of Hcy remethylation in the placenta and results inan increased transfer of Hcy from maternal to fetal circu-lation.
The basis for the observed abnormal metabolic profileamong neonates with conotruncal heart defects and their
-
BioMed Research International 5
mothers cannot be defined without further analysis of rele-vant genetic and environmental factors.Therefore, confirma-tion by future prospective multicentre cohorts is needed.
5. Conclusions
Elevated homocysteine levels in neonates with conotruncalheart defects and folate metabolism disturbances in theirmothers were noticed.
The observed differences in homocysteine and cobalaminlevels between neonates with congenital heart defects suggestthe influence of various agents disturbing homocysteinemetabolic pathways.
Conflicts of Interest
The authors declare that they have no conflicts of interest.
References
[1] H. Dolk,M. Loane, and E. Garne, “The prevalence of congenitalanomalies in Europe,” Advances in Experimental Medicine andBiology, vol. 686, pp. 349–364, 2010.
[2] A. Latos-Bielenska, A. Materna-Kiryluk, M. Badura-Stronka etal., “Wrodzone wady rozwojowe w Polsce w latach 2005-2006,”in Dane z Polskiego Rejestru Wrodzonych Wad Rozwojowych,Ośrodek Wydaw Nauk, Poznań, Poland, 2010.
[3] C. L. Ulrey, L. Liu, L. G. Andrews, and T. O. Tollefsbol, “Theimpact of metabolism onDNAmethylation,”HumanMolecularGenetics, vol. 14, no. 1, pp. R139–R147, 2005.
[4] H. Jakubowski, “Metabolism of homocysteine thiolactone inhuman cell cultures: Possible mechanism for pathological con-sequences of elevated homocysteine levels,” Journal of BiologicalChemistry, vol. 272, no. 3, pp. 1935–1942, 1997.
[5] K. Livia, L. M. H. Michele, and A. P. S. Eric, “Congenitalheart defects andmaternal derangement of homocysteinemeta-bolism,” The Journal of Pediatrics, vol. 135, no. 6, pp. 773-774,1999.
[6] Y. Li, X. Chen, X. Zhao, and B. Hu, “Relationship betweenhomocysteine induced apoptosis and teratogenesis in develop-ing embryo,”Wei Sheng Yan Jiu, vol. 28, pp. 257-258, 1999.
[7] R. P. M. Steegers-Theunissen, L. M. J. W. Van Driel, R. De Jongeet al., “Maternal global methylation status and risk of congenitalheart diseases,” Obstetrics and Gynecology, vol. 112, no. 2, pp.277–283, 2008.
[8] C. A. Hobbs, M. A. Cleves, S. Melnyk, W. Zhao, and S. J. James,“Congenital heart defects and abnormalmaternal biomarkers ofmethionine and homocysteine metabolism,” American Journalof Clinical Nutrition, vol. 81, no. 1, pp. 147–153, 2005.
[9] J. A. Greenberg, S. J. Bell, Y. Guan et al., “Folic acid supple-mentation and pregnancy: more than just neural tube defectprevention,” Reviews in Obstetrics and Gynecology, vol. 4, no. 2,pp. 52–59, 2011.
[10] O. A. Ladipo, “Nutrition in pregnancy: mineral and vitaminsupplements,” The American Journal of Clinical Nutrition, vol.72, Supplement 1, pp. 280S–290S, 2000.
[11] L. D. Botto, J. Mulinare, and J. D. Erickson, “Occurrence of con-genital heart defects in relation to maternal multivitamin use,”American Journal of Epidemiology, vol. 151, no. 9, pp. 878–884,2000.
[12] MRC Vitamin Study Research Group, “Prevention of neuraltube defects: results of the medical research council vitaminstudy,”The Lancet, vol. 338, no. 8760, pp. 131–137, 1991.
[13] T. J. Siddiqua, S. M. Ahmad, K. B. Ahsan et al., “Vitamin B12supplementation during pregnancy and postpartum improvesB12 status of both mothers and infants but vaccine responsein mothers only: a randomized clinical trial in Bangladesh,”European Journal of Nutrition, vol. 55, no. 1, pp. 281–293, 2016.
[14] DM. El-Abd, RN. Said, and BM. Hanna, “MTHFR C677Tpolymorphism is associated with certain subgroups of CHDs.Maternal folic acid supplementation proved protective againstCHDs,” Comp Clin Pathol, vol. 23, p. 317, 2014.
[15] M. J. Boot, R. P.M. Steegers-Theunissen, R. E. Poelmann, L. VanIperen, J. Lindemans, and A. C. Gittenberger-de Groot, “Folicacid and homocysteine affect neural crest and neuroepithelialcell outgrowth and differentiation in vitro,” DevelopmentalDynamics, vol. 227, no. 2, pp. 301–308, 2003.
[16] S. K. Ratan, K. N. Rattan, R. M. Pandey et al., “Evaluation of thelevels of folate, vitamin B12, homocysteine and fluoride in theparents and the affected neonates with neural tube defect andtheir matched controls,” Pediatric Surgery International, vol. 24,no. 7, pp. 803–808, 2008.
[17] A. C. Verkleij-Hagoort, M. Verlinde, N. T. C. Ursem et al.,“Maternal hyperhomocysteinaemia is a risk factor for congen-ital heart disease,” BJOG: An International Journal of Obstetricsand Gynaecology, vol. 113, no. 12, pp. 1412–1418, 2006.
[18] J.-Y. Zhao, X.-Y. Yang, X.-H. Gong et al., “Functional variant inmethionine synthase reductase intron-1 significantly increasesthe risk of congenital heart disease in the Han Chinese popula-tion,” Circulation, vol. 125, no. 3, pp. 482–490, 2012.
[19] N. Solanky, A. R. Jimenez, S. W. D’Souza, C. P. Sibley, and J. D.Glazier, “Expression of folate transporters in human placentaand implications for homocysteine metabolism,” Placenta, vol.31, no. 2, pp. 134–143, 2010.
-
Submit your manuscripts athttps://www.hindawi.com
Stem CellsInternational
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
MEDIATORSINFLAMMATION
of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Behavioural Neurology
EndocrinologyInternational Journal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Disease Markers
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
BioMed Research International
OncologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Oxidative Medicine and Cellular Longevity
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
PPAR Research
The Scientific World JournalHindawi Publishing Corporation http://www.hindawi.com Volume 2014
Immunology ResearchHindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Journal of
ObesityJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Computational and Mathematical Methods in Medicine
OphthalmologyJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Diabetes ResearchJournal of
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Research and TreatmentAIDS
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Gastroenterology Research and Practice
Hindawi Publishing Corporationhttp://www.hindawi.com Volume 2014
Parkinson’s Disease
Evidence-Based Complementary and Alternative Medicine
Volume 2014Hindawi Publishing Corporationhttp://www.hindawi.com



![Homocysteine-lowering interventions for preventing … · 2018. 12. 15. · [Intervention Review] Homocysteine-lowering interventions for preventing cardiovascular events Arturo J](https://static.fdocuments.net/doc/165x107/5ff89452656730039f05d58a/homocysteine-lowering-interventions-for-preventing-2018-12-15-intervention.jpg)