ABIM Allergy Immunology Review 2014
72
ABIM ALLERGY IMMUNOLOGY REVIEW 2014 Richard D. deShazo, MD with thanks to the many colleagues from whom I have borrowed material
description
ABIM Allergy Immunology Review 2014 . Richard D. deShazo, MD with thanks to the many colleagues from whom I have borrowed material. Questions:. What are the major diagnostic criteria for asthma?. How can you separate asthma from COPD?. - PowerPoint PPT Presentation
Transcript of ABIM Allergy Immunology Review 2014

ABIM ALLERGY IMMUNOLOGY REVIEW2014
Richard D. deShazo, MD with thanks to the many colleagues from whom I
have borrowed material

Questions:• What are the major diagnostic
criteria for asthma?• How can you separate asthma
from COPD?• What does a positive methacholine
inhalation test mean?
3
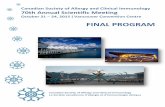
Spirometry before and after an inhaled bronchodilator showing reversible airway obstruction

4
Asthma Diagnosis FEV1 improvement of 12% and 200mL
after beta-agonist is evidence for asthma according to ATS
Decreased FEV1/FVC ratio 20-39yr 85% 40-59yr 80% 60-80yr 70%
Methacholine challenge – not diagnostic of asthma + with 20% decrease FEV1 with <8-16mg/mL True benefit is in negative predictive value
Question:• What test should be considered in
a young asthmatic female with recurrent episodes of wheezing poorly responsive to bronchodilators?

6
Vocal Cord Dysfunction Is Not Asthma, But May Occur In AsthmaticsFlow volume loops showing maximum inspiratory and expiratory flow-volume relationships in a patient with vocal cord dysfunction during asymptomatic (left) and symptomatic (right) periods. Note also the marked adduction of the vocal cords with severe reduction of the glottic aperture during a symptomatic period (right) of airway obstruction.

7
Vocal Cord Dysfunction Female 2:1 Athletes Bronchodilator non
responsive
Many (up to 1/3) can have coexist asthma
Difficulty getting breath in

2 Questions:• What is the likely diagnosis in a man with
persistent cough, shortness of breath, dyspnea, and episodic wheeze that developed after working as a police officer in the 9/11 exposure area in NYC?
• A 22 year old with recent onset cough and wheeze works in a custom sailboat shop in Biloxi sealing the inside of boats with epoxy resins. What is the most likely low molecular weight chemical causing his symptoms?

9
Reactive Airways Dysfunction Syndrome (RADS): Not Asthma
Treatment – Time + corticosteroids Occurs after a single inhalation of a
caustic irritant in a non-asthmatic Obstruction on PFT (+) methalcholine inhalation challenge Limited PFT-response to beta-agonists Not “reactive airways disease”
10
Occupational Asthma Basically, asthma occurring because of
exposure at work. Testing difficult, so sometimes need to do
pulmonary evaluation at the workplace. (Start with peak flows at work versus home).
Earlier you diagnose the better, because may lead to permanent asthma even when removed from environment.

11
Risk Factors for Asthma Death
Previous life-threatening asthma such as respiratory arrest
Hospitalization or ED visit for asthma within the last year
Use of 2 or more canisters of rescue inhaler/month
Poor perception of hypoxia or airway obstruction
Psychosocial disturbance

12
Components of Severity
Mild Moderate Severe
Impairment Intermittent ------------------------
----Persistent---- ------------------------
Symptoms <2 days/weeks >2 days/week but not daily
>1 x/week but not nightly
Throughout the day
Nighttime awakenings
<2 x/month 3-4 x/month >1 x/week but not nightly
Often 7 x/week
SABA use for symptom control (not prevention of EIB)
< 2 days/week >2 days/week but not more than 1 x/d
Daily Several times a day
Interference with normal activity
None Minor limitation Some limitation Extremely limited
Lung function Normal FEV1 between exacerbations FEV1 >80% of predicted FEV1/FVC normal
FEV1 >80% of predicted FEV1/FVC normal
FEV1 >60% but <80% of predicted FEV1/FVC reduced 5%
FEV1 <60% of predicted FEV1/FVC reduced >5%
RiskExacerbations (consider frequency and severity)
0-2/year >2/year
Classification of Asthma Severity
13
Asthma Pharmacotherapy Rescue medicines
Short acting agonists (SABA) Anticholinergic
Controller medicines Inhaled corticosteroids (ICS) Long acting agonists (LABA) Leukotriene receptor antagonists (LTRA) Combinations of ICS & LABA Anti-IgE (omalizamab) Others

14
Stacking Asthma Drugs
15
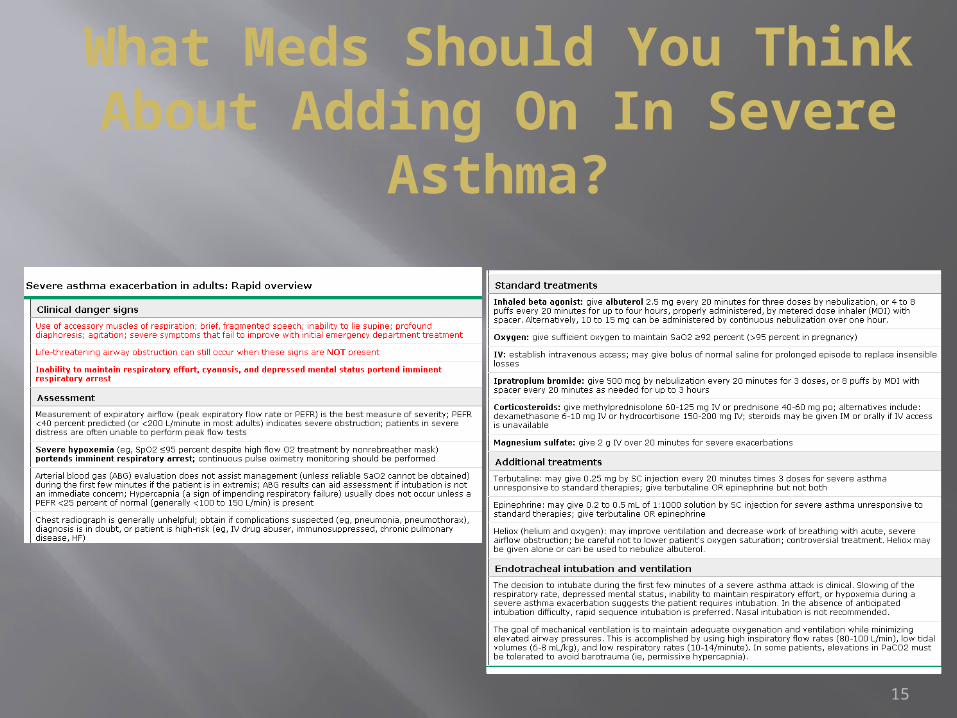
What Meds Should You Think About Adding On In Severe
Asthma?
16
Things to consider in the out of control asthmatic
Vocal cord dysfunction GERD Sinusitis Churg-Strauss syndrome ABPA Compliance/technique

17
How Do You Assess Asthma Control?

18
How Do You Use A
Metered Dose Inhaler (MDI)?

19
What Does Every Asthmatic Have to Have?

20
3 Eosinophilic Lung Diseases
Churg-Strauss Vasculitis Sinusitis, asthma, eosinophilia, vasculitis Transient pulmonary infiltrates Small vessel vasculitis Neuropathies (mononeuritis multiplex) MPO- ab/P-ANCA test (+) in about 50% RX: steroids (cyclophosphamide/azathioprine
in severe) ? relationship to LTRA

21
Allergic Bronchopulmonary Mycosis (ABPM)
Includes allergic bronchopulmonary aspergillosis (ABPA) and other allergic mycoses
Criteria Asthma Fleeting pulmonary infiltrates High total IgE (>1000 ng/mL or 417 kU/L) Positive immediate skin test (IgE) to fungus (A.
fumigatus, etc.) or Positive RAST test Elevated serum specific IgE to fungus (A.
fumigatus, etc.) CT with central bronchiectasis reflects chronic
disease

22
Treatment of ABPM
Oral corticosteroids Follow total serum IgE and CXR No long term studies on Itraconazole as
steroid sparing agent

23
Hypereosinophilic Syndrome
No increase asthma but may have allergic – like dermatitis
Paramalignant syndrome Peripheral blood eos count >1500 µL for at least 6
months Absence of any other known cause of eosinophilia Presumptive signs/symptoms of organ invasion by
eosinophils 9:1 male:female Systemic disease Cardiac disease (thrombosis, fibrosis, necrosis) is the
most common cause of death FIP1L1/PDGFA fusion-gene present in some patients
24
Organs Involved in Hypereosinophlic
Syndrome Heart Skin, Lungs, GI tract, Nervous System Vascular thrombosis is a feared
complication Treatment
Steroids Hydroxyurea Interferon α Gleevac (imatinib) - for FIP1L1-PDGFRα gene
rearrangement
Question:• A 50 year old woman with asthma
and atopic dermatitis has her 3rd episode of food impaction. What findings should be sought from endoscopy to confirm the diagnosis?

26
Eosinophilic Gastroenteritis
Atopic individuals Usually in upper tract Food impaction in esophagus Mucous furrowing and white specks on
endoscopy More than 12 eosinophils/HPF on biopsy Food allergy in some Treated with non-absorbable steroids
Question:• A 50 year old bird breeder has
persistent shortness of breath, cough, and dyspnea. What should be done?

28
Hypersensitivity Pneumonitis Fever, chills, malaise, cough, dyspnea Acute, subacute, chronic A systemic illness Also known as “extrinsic allergic alveolitis” Non allergic, not IgE mediated, no eosinophilia,
no asthma except pigeon breeder’s (bird fancier’s) lung
T-cell mediated CXR/CT scan abnormal: ground glass/diffuse
alveolar pattern PFT – restriction not obstruction except for pigeon
breeders Chronic pulmonary fibrosis

29
Approach to Allergic Rhinitis
Characterize chronicity looking for seasonal variation.
Ask for family history, indoor triggers and nasal itching.
Swollen nasal mucosa usually more blue that red. Treat If there is treatment failure, do allergy skin tests or
RASTs to determine specific allergen and consider allergy shots.
Allergy shots are very effective for allergic rhinitis and insect anaphylaxis.
30
Allergic Rhinitis Nasal steroids – first line treatment Antihistamines and leukotriene receptor
antagonists – second line (about equal efficacy as second line agents)
To prevent symptoms on planned exposures, chromolyn or antihistamines work best
Allergen immunotherapy by subcutaneous or sublingual techniques

31
Mimics of Allergic Rhinitis Vasomotor rhinitis Rhinitis medicamentosa Nasal manifestations of systemic disease:
Diabetes mellitus – mucor mycosis (nasal eschar; black crust)
Wegener’s granulomatosis (saddle nose) Midline granuloma (saddle nose) Relapsing polychondritis (saddle nose) Sarcoidosis (bloody crusts) Cystic fibrosis (nasal polyps) CSF leak – check beta 2 transferrin (very specific)

32
Rhinosinusitis Syndromes withNasal Polyposis
Immunodeficiency Cystic fibrosis Aspirin – sensitive respiratory disease Allergic fungal sinusitis Anosmia is a big tip off for polyps

33
Acute & Chronic Sinusitis
Ethmoid cell

Question:• A 30 year old nurse has a severe
chronic dry and cracking dermatitis of both hands. What should you do first?

35
Patch testing can detect both irritant and allergic contact dermatitis, if the tests are read at appropriate times. Consider a patch test a TB skin test. Positive results are
erythema and induration maximum at 24-48 hours.
Irritant vs. Allergic Contact Dermatitis
36
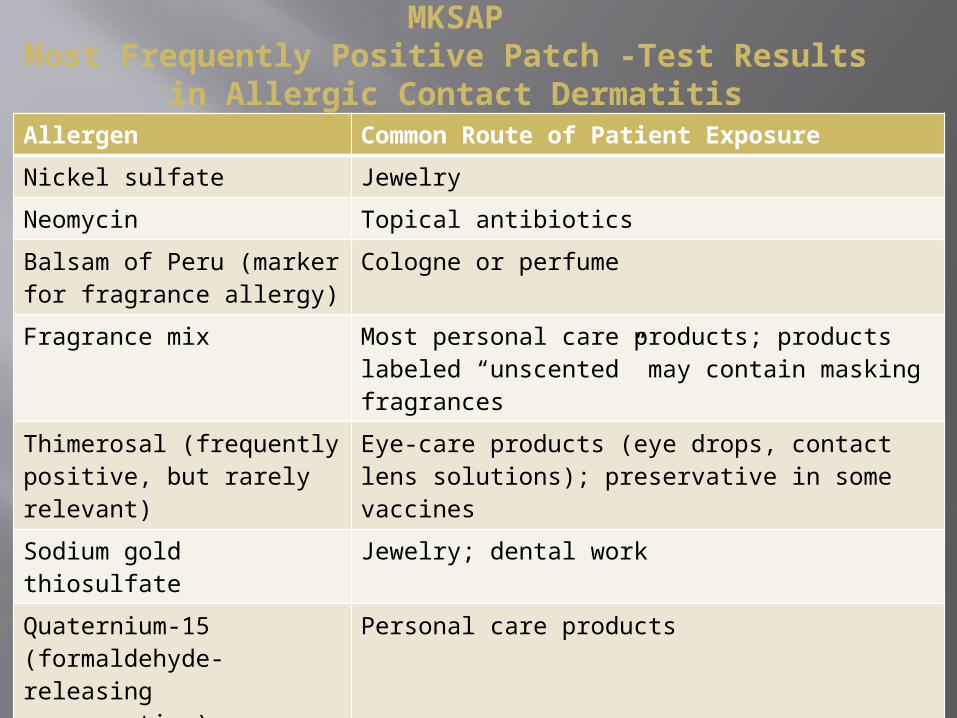
Allergen Common Route of Patient ExposureNickel sulfate JewelryNeomycin Topical antibioticsBalsam of Peru (marker for fragrance allergy)
Cologne or perfume
Fragrance mix Most personal care products; products labeled “unscented” may contain masking fragrances
Thimerosal (frequently positive, but rarely relevant)
Eye-care products (eye drops, contact lens solutions); preservative in some vaccines
Sodium gold thiosulfate Jewelry; dental workQuaternium-15 (formaldehyde-releasing preservative)
Personal care products
Formaldehyde Personal care productsBacitracin Topical antibiotic; may cross-react with
neomycinCobalt chloride Blue paint; vitamin B12 (cyanocobalamin); may
cross-react with other metals, including nickel
MKSAPMost Frequently Positive Patch -Test Results
in Allergic Contact Dermatitis

Question:• A 16 year old male with asthma
has a chronic pruritic dermatitis in the flexural areas of his elbows and knees. What treatment would be best for this problem?

38
Atopic dermatitis with involvement of a flexural surface. The frequently involved anticubital and popliteal fossae.
Atopic Dermatitis (Eczema) (1)

39
Atopic Dermatitis (2) Increased susceptibility to
Staph aureus, HSV (eczema herpeticum), vaccinia Differential diagnosis
Allergic contact dermatitis Irritant contact dermatitis (gloves) Cutaneous T – cell lymphoma
An adult presenting with eczematous dermatitis with an erythrodermatous appearance by skin biopsy with genetic studies
Atopic dermatitis is associated with abnormalities in the filaggrin gene which encodes for filaggrin protein important in statium corneam moisturization

40
Treatment of Atopic Dermatitis
Skin hydration/moisturization (Aquaphor) Medium strength topical corticosteroids
and combinations (equal parts 0.1% triamcinolone and Aquaphor)
Oral antibiotics (Staph) Antihistamines (control itch) Topical calcineurin inhibitors (protopic/
elidel)
41
Cause History Physical Examination Findings
Laboratory Findings
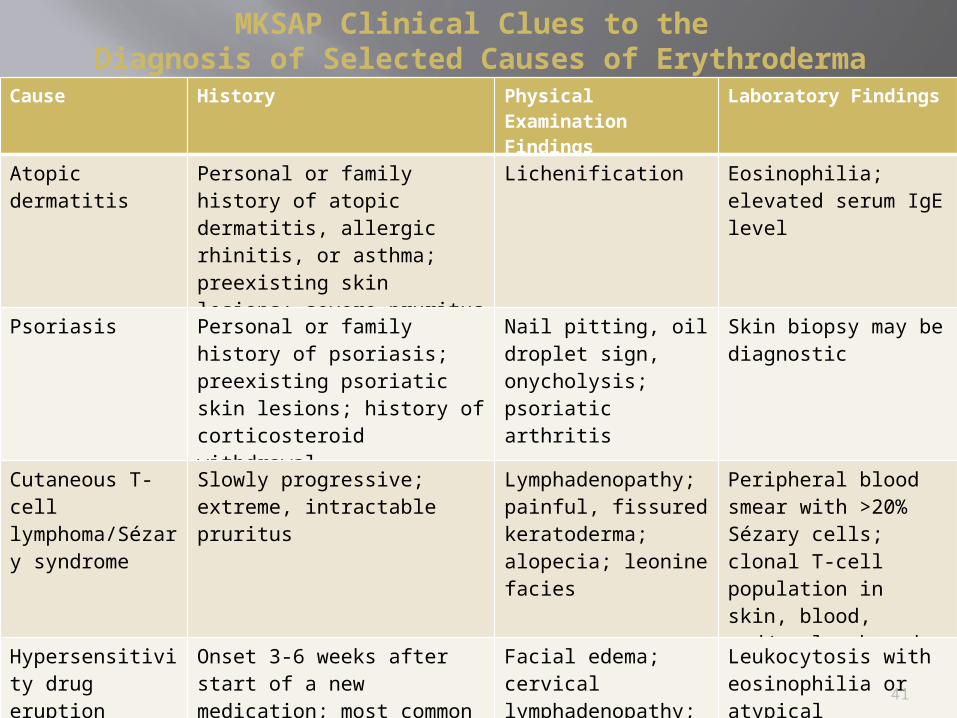
Atopic dermatitis
Personal or family history of atopic dermatitis, allergic rhinitis, or asthma; preexisting skin lesions; severe pruritus
Lichenification Eosinophilia; elevated serum IgE level
Psoriasis Personal or family history of psoriasis; preexisting psoriatic skin lesions; history of corticosteroid withdrawal
Nail pitting, oil droplet sign, onycholysis; psoriatic arthritis
Skin biopsy may be diagnostic
Cutaneous T-cell lymphoma/Sézary syndrome
Slowly progressive; extreme, intractable pruritus
Lymphadenopathy; painful, fissured keratoderma; alopecia; leonine facies
Peripheral blood smear with >20% Sézary cells; clonal T-cell population in skin, blood, and/or lymph node
Hypersensitivity drug eruption
Onset 3-6 weeks after start of a new medication; most common causative medications are allopurinol, aromatic anticonvulsants, dapsone, NSAIDs, sulfonamides, lamotrigine
Facial edema; cervical lymphadenopathy; fine scale around nose; hepatosplenomegaly
Leukocytosis with eosinophilia or atypical lymphocytosis; elevated serum aminotransferases; elevated blood urea nitrogen or serum creatinine levels
MKSAP Clinical Clues to the Diagnosis of Selected Causes of Erythroderma

42
Urticaria
Classification of Urticaria• Acute urticaria (<6 weeks)• Chronic urticaria (>6 weeks)• Physical urticaria (pressure, cold,
vibratory, etc.)• Urticarial vasculitis• Contact urticaria (touching a cat)• Urticaria and angioedema as
components of anaphylaxis

43
Classification CharacteristicsPapular urticaria Associated with insect bitesCholinergic urticaria Occurs in response to an increase
in core body temperature; lesions present as small papules with a prominent surrounding erythematous flare
Delayed pressure-induced urticaria
Patients often experience systemic symptoms
Exercise-induced urticaria On a continuum with exercise-induced anaphylaxis; many patients only develop symptoms if primed by an ingested allergen prior to exercise
Solar urticaria Some patients who appear to have solar urticaria prove to have lupus erythematosus or porphyria
Cold urticaria Acquired cold urticaria is often related to an underlying infection, whereas familial cold urticaria represents an autoinflammatory syndrome
Vibrational urticaria —
Classification of Physical Urticarias

44
Palpable purpura is a clinical sign of a small vessel (leukocytoclastic) vasculitis which may present as chronic urticaria.

Question:
• A 68 year old female with chronic mylogenous leukemia presents with non itchy swelling of the lips and throat. What diagnostic tests would be most useful to diagnose acquired angioedema?

46
Differential Diagnosis: Cutaneous and/or Laryngeal Swelling
Allergic reactions and anaphylaxis Idiopathic angioedema Drug induced angioedema Allergic contact dermatitis Autoimmune conditions Thyroid disorders Superior vena cava syndrome and tumors Cheilitis granulomatosa (Miescher’s cheilitis) and
Melkersson-Rosenthal syndrome Trichinosis Low C-4 levels

47
Hereditary Angioedema Autosomal Dominant Hiveless, itchless edema Hereditary angioedema form more
likely to have symptoms precipitated by trauma - dental visit, surgery, auto accident, menses, puberty Visceral attacks may present as an
acute abdomen with normal findings at surgery

48
Symptoms: Painless, itchless angioedma with/without family history
Diagnosis of HAE5
HAE 1 - low C41, 2 low C1 INH, low C1INH-F HAE2 - low C41, 2 normal C1 INH, low C1INH-F Acquired – low C41, 3 low C1 INH, low C1INH-F, low Clq HAE3 – normal C4 4 normal C1 INH, normal C1INH-F,
normal C1f level
1. Always low during attacks2. SERPING1 gene abnormalities3. Antibodies to C1INH4. Abnormalities in Factor XII genes5. Family members should be screened in all types
49
Acquired Angioedema
Associated with lymphoproliferative disorders
Have low C1q levels Mechanism unclear Low C1 of levels appear to reflect
autoactivationAnti – C1 esterase inhibitor antibodies have been described as well

50
Tests for Hereditary/Acquired
Angioedema C4 – is a great screening test, but is
normal in HAE Type 3 Test for C1 esterase inhibitor level and
function to discriminate between two hereditary types
Test C1q level for the acquired form Genetic testing for HAE Type 3

51
Therapy of HAE On-demand treatment
Treatment of attacks with upper airways symptoms is mandatory
Acute attacks should be treated with C1INH (plasma derived) Berinert Escallantide (inhibits HMW Kininogen to bradykinen) Kalbitor Icatibant (bradykinen recepptor antagonist) Firazyr
Intubation or trachestomy should be early in progressive airway obstruction
Antifibronolytics are not to be used Procedural prophylaxis with procedures involving the
upper airway is recommended without evidence Pregnancy – C1INH advised Long-term Prophylaxis
C1INH - immunizations, screens Androgens – frequent screens for liver toxicity Antifibrolytics not recommended

52
First-line therapies for acute attacks of HAE include
Purified (C1INHRP) or recombinant (rhC1INH) human C1 inhibitor (various products available worldwide)
Ecallantide, a kallikrein inhibitor (available only in the United States)
Icatibant, a bradykinin B2 receptor antagonist (available in the United States and the European Union)
Question 23:• What should be prescribed for a
patient after treatment for acute anaphylaxis and how should it be used?

54
Anaphylaxis Usually starts with urticaria and itching but can
present with syncope, hypotension, or erythoderma.
Most common causes are foods (peanut/ tree nut ingestion, etc.), insect stings, drug allergy (beta lactam)
Don’t forget latex, especially in medical spaces No obvious trigger- think mastocytosis (check
serum mast cell tryptase) or idiopathic anaphylaxis
All who have insect anaphylaxis patients require evaluation for venom immunotherapy

55
AnaphylaxisEarly Management
Hypotension - supine, IV (NS) Respiratory distress - oxygen and albuterol,
intubation Epinephrine
1:1000 .3-.5cc IM for adults (note this is NOT the 1:10,000 dilution - (1mg/10ml) on crash carts
Can repeat in 5 minutes If on beta blocker and not responsive to epi, consider
glucagon 1mg IM, IV, SC Can start epi infusion if not responsive to IM epi
(1:10,000) 1-3 mg over 3 min, then 3-5mg over 3 minutes, then 4-10ug/min infusion
All who recover must leave with an Epipen®.
Consider 1 mg of glucagon IV if on beta blocker

56
Cutaneous Mastocytosis Cutaneous Mastocytosis
Have urticaria pigmentosa – reddish brown or tan macules. Darier’s sign
Indolent, benign course Itching, burning skin, flushing, CNS
symptoms

57
Criteria for Systemic Mastocytosis
Major Multifocal dense infiltrates of mast cells in bone
marrow or extracutaneous organ Minor
>25% mast cells are spindle-shaped or atypical Presence of c-kit point mutation Mast cells co-express Kit and CD2 Persistent serum tryptase >20ng/mL
Need one major and one minor, or 3 minor Other:
Skin involvement improves prognosis Insect stings may induce anaphylactoid reactions
in patients with mastocytosis.

58
Drug Reactions MKSAP
Common Drug Reaction Patterns

59
Vancomycin Reactions “Red man syndrome” – pruritis and
erythema of face, neck, upper torso, occasionally with hypotension
Non-immunologic release of histamine Not IgE mediated Rx: slow the infusion and pre-treat

60
Anticonvulsant Hypersensitivity Cause the “hypersensitivity
syndrome” Deficiency of epoxide hydrolase Fever, maculopapular rash, generalized
lymphadenopathy Node bx resembles Hodgkin’s Phenytoin, carbamazepine, phenobarb Can also cause DRESS: Drug reaction
with eosinophilia and systemic symptoms. Rash, fever, multi-organ failure
½ actually have eosinophilia

61
Serum Sickness

Question 24:• A 21 year old college student has
recurrent sinupulmonary infections. What test in addition to HIV should be performed to exclude immunodeficiency?

63
Immunodeficiency T- cell (cellular immunity) – virus, fungi,
protozoa, mycobacteria and other intracellular organisms
Humoral (antibody mediated immunity) – infection with extracellular pyogenic organisms Haemophilus Pneumococcus Streptococcus Increased infections Recurrent respiratory infections Multiple systems involved Unusual organisms Malabsorption Big LNs or absent LNs

64
Common Variable Immunodeficiency
Decreased IgG, M, A, normal to increased IgE
Recurrent sinopulmonary infections Lymph tissue present or enlarged High incidence of autoimmune disease
(22%) Increased risk of adenocarcinoma and
lymphomas In addition to encapsulated organisms
Giardia, yersinia, H. pylori, and H. jejuni are common

65
IgA deficiency Most common form of primary
immunodeficiency (1:333) IgA <5mg/dL (VERY LOW) Most patients with IgA def. are NORMAL Have increased risk of infections:
collagen vascular , allergic, and GI disease, and malignancy
Can make anti-IgA antibodies Leads to anaphylaxis with IgA containing
blood products
66
IVIG Indicated for common variable
immunodeficiency and specific antibody deficiency
Not indicated for IgA deficiency Side effects
Never transmitted of HIV Fever, chills, HA, muscle pain. Aseptic meningitis Renal failure (was due to osmotic load, not as
common now), stroke, MI

67
Complement Deficiency C2 deficiency (most common) – sepsis,
pneumonia, meningitis, pyogenic arthritis with Strep pneumo
C2 deficiency – increased risk of rheumatoid arthritis, SLE
Terminal Complement Components – Neisseria sp infections Think about if recurrent meningitis or if
unusual strain

68
Live Vaccines to Avoid in Cellular Immune Deficiency
Measles Mumps Oral Polio Rubella Varicella MMR Smallpox (vaccinia) Flumist
69
Egg Allergy and Vaccines Influenza and Yellow fever
Question 28:What dietary pattern do bedbugs follow?

71
Bedbug Bites Often Occur in a Series
“Breakfast, lunch, and dinner”Lesions are usually painless and appear as pruritic, urticarial-like
papules. Dinner
Lunch
Breakfast
72
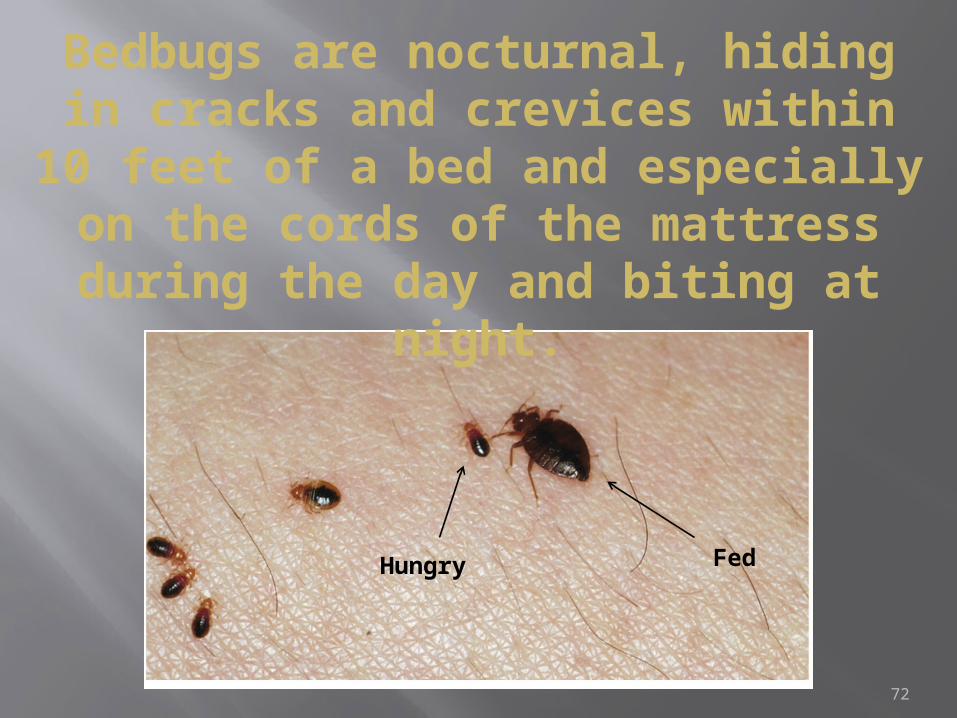
Bedbugs are nocturnal, hiding in cracks and crevices within 10
feet of a bed and especially on the cords of the mattress during
the day and biting at night.
Hungry Fed