Abdominoplasty With Direct Resection of Deep Fat.26
7
COSMETIC Abdominoplasty with Direct Resection of Deep Fat Robert R. Brink, M.D. Joel B. Beck, M.D. Catherine Michelle Anderson Anne Christine Lewis San Mateo, Calif. Background: Suction-assisted lipectomy is an integral component of abdomi- noplasty for many surgeons. Its potential to affect the vascularity of the abdom- inal flap is usually offset by limiting the extent of undermining and not suc- tioning the central flap. The authors address whether these guidelines apply to direct excision of subscarpal fat and whether direct excision provides aesthet- ically superior abdominoplasty results with fewer complications. Methods: A 10-year review of consecutive abdominoplasty patients (n 181) was conducted. Undermining was done to the xyphoid and just beyond the lower rib margins superiorly and at least as far as the anterior axillary line laterally. Fat deep to Scarpa’s fascia was removed by tangential excision in all zones of the abdominal flap, including those considered at high risk for vascular compromise if subjected to liposuction after similar undermining. Concurrent liposuction of the abdominal flap was not done. Thirty patients had concurrent flank liposuction. Results: No patients experienced major full-thickness tissue loss. The incidence of limited necrosis at the incision line requiring subsequent scar revision was 0.7 percent in the 151 patients having abdominoplasty and 6.7 percent in the 30 patients having abdominoplasty combined with flank liposuction. Erythema and/or epidermolysis was seen in 4.8 percent of the abdominoplasty patients and 10 percent of the abdominoplasty/ flank liposuction group. The rate of seroma formation in both groups was approximately 16.5 percent. Conclusions: Direct excision of subscarpal fat does not subject any zone of the abdominoplasty flap to increased risks of vascular compromise. It is a safe technique that provides excellent abdominoplasty results. (Plast. Reconstr. Surg. 123: 1597, 2009.) T he first description of abdominal dermoli- pectomy in the American literature is attrib- uted to Kelly 1 in 1889. Many variations on the theme followed until Pitanguy’s 2 classic descrip- tion in 1967, which served as the prototype for the evolution of modern abdominoplasty. Neither Pitan- guy nor his predecessors described removal of any adipose tissue beyond the confines of the resected segment. Grazer 3 appears to be the first to have done so in 1980 when he described limited “bev- eling” of the flap in tangential fashion in heavier patients. In recent years, liposuction has become a standard component of abdominoplasty for many surgeons, 4–9 and its use to thin the abdom- inal flap has supplanted tangential excision. The risks liposuction presents to the central zones of an abdominoplasty flap were described by Matarasso, 10 who also advocated limited under- mining to preserve perforators in the upper ab- dominal quadrants. The validity of limited under- mining and zonal awareness as essential to flap survivability when liposuction is combined with ab- dominoplasty has been repeatedly confirmed. 11,12 Many researchers have studied the blood supply of the anterior abdominal wall. In 1975, Taylor and Daniel 13 reported that the superficial inferior epi- gastric artery traveled superficial to Scarpa’s fascia, which Hester et al. 14 and Worseg et al. 15 indepen- dently confirmed in 1984. Recently, Schaverien et al. 16 have shown by three- and four-dimensional computed tomographic angiography and venog- From the San Mateo Surgery Center. Received for publication September 16, 2008; accepted No- vember 17, 2008. Copyright ©2009 by the American Society of Plastic Surgeons DOI: 10.1097/PRS.0b013e3181a07708 Disclosure:No grants or financial support have been received in conjunction with this study. None of the authors has any financial interest or commer- cial association with any of the subject matter or products mentioned in this article. www.PRSJournal.com 1597
-
Upload
reylaberinto -
Category
Documents
-
view
79 -
download
0
Transcript of Abdominoplasty With Direct Resection of Deep Fat.26

COSMETIC
Abdominoplasty with Direct Resection ofDeep Fat
Robert R. Brink, M.D.Joel B. Beck, M.D.
Catherine Michelle AndersonAnne Christine Lewis
San Mateo, Calif.
Background: Suction-assisted lipectomy is an integral component of abdomi-noplasty for many surgeons. Its potential to affect the vascularity of the abdom-inal flap is usually offset by limiting the extent of undermining and not suc-tioning the central flap. The authors address whether these guidelines apply todirect excision of subscarpal fat and whether direct excision provides aesthet-ically superior abdominoplasty results with fewer complications.Methods: A 10-year review of consecutive abdominoplasty patients (n � 181) wasconducted. Undermining was done to the xyphoid and just beyond the lower ribmargins superiorly and at least as far as the anterior axillary line laterally. Fat deepto Scarpa’s fascia was removed by tangential excision in all zones of the abdominalflap, including those considered at high risk for vascular compromise if subjectedto liposuction after similar undermining. Concurrent liposuction of the abdominalflap was not done. Thirty patients had concurrent flank liposuction.Results: No patients experienced major full-thickness tissue loss. The incidence oflimited necrosis at the incision line requiring subsequent scar revision was 0.7percent in the 151 patients having abdominoplasty and 6.7 percent in the 30patients having abdominoplasty combined with flank liposuction. Erythema and/orepidermolysis was seen in 4.8 percent of the abdominoplasty patients and 10 percentof the abdominoplasty/ flank liposuction group. The rate of seroma formation inboth groups was approximately 16.5 percent.Conclusions: Direct excision of subscarpal fat does not subject any zone of theabdominoplasty flap to increased risks of vascular compromise. It is a safe techniquethat provides excellent abdominoplasty results. (Plast. Reconstr. Surg. 123: 1597,2009.)
The first description of abdominal dermoli-pectomy in the American literature is attrib-uted to Kelly1 in 1889. Many variations on the
theme followed until Pitanguy’s2 classic descrip-tion in 1967, which served as the prototype for theevolution of modern abdominoplasty. Neither Pitan-guy nor his predecessors described removal of anyadipose tissue beyond the confines of the resectedsegment. Grazer3 appears to be the first to havedone so in 1980 when he described limited “bev-eling” of the flap in tangential fashion in heavierpatients. In recent years, liposuction has becomea standard component of abdominoplasty formany surgeons,4–9 and its use to thin the abdom-inal flap has supplanted tangential excision.
The risks liposuction presents to the centralzones of an abdominoplasty flap were described by
Matarasso,10 who also advocated limited under-mining to preserve perforators in the upper ab-dominal quadrants. The validity of limited under-mining and zonal awareness as essential to flapsurvivability when liposuction is combined with ab-dominoplasty has been repeatedly confirmed.11,12
Many researchers have studied the blood supplyof the anterior abdominal wall. In 1975, Taylor andDaniel13 reported that the superficial inferior epi-gastric artery traveled superficial to Scarpa’s fascia,which Hester et al.14 and Worseg et al.15 indepen-dently confirmed in 1984. Recently, Schaverien etal.16 have shown by three- and four-dimensionalcomputed tomographic angiography and venog-
From the San Mateo Surgery Center.Received for publication September 16, 2008; accepted No-vember 17, 2008.Copyright ©2009 by the American Society of Plastic Surgeons
DOI: 10.1097/PRS.0b013e3181a07708
Disclosure:No grants or financial support havebeen received in conjunction with this study. Noneof the authors has any financial interest or commer-cial association with any of the subject matter orproducts mentioned in this article.
www.PRSJournal.com 1597

raphy that planar perfusion of the superficial in-ferior epigastric artery and deep inferior epigas-tric perforator is via a subdermal plexus and asuprafascial plexus.
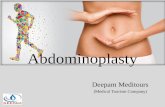
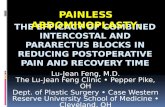
These studies have verified our intraoperativeobservations that all major vasculature of the ab-dominoplasty flap courses in the layer of adiposetissue superficial to Scarpa’s fascia (Fig. 1) andthat removal of fat deep to Scarpa’s fascia is notaccompanied by bleeding or subsequent compro-mise of the abdominal flap. Others have recognizedthat the deep fat may be directly excised duringabdominoplasty,17 but its efficacy in providing safeand consistently superior abdominoplasty resultsfree of contour irregularities has been widely ig-nored in the rush to embrace liposuction. Thecurrent retrospective analysis was undertaken toconfirm our impression that excellent abdomino-plasty results can be safely obtained by removingonly the adipose tissue deep to Scarpa’s fascia inall topographical zones of the abdominal flap andthat manipulations of the superficial fatty layer,whether intentional or inadvertent, are unneces-sary, implicitly dangerous, and aesthetically coun-terproductive.
PATIENTS AND METHODS
Procedure DescriptionStandard full abdominoplasties were performed
with little variation over the last decade. All pa-tients were postpartum females. The consistent
features of the procedure were as follows: (1) Allmarkings were made preoperatively with the pa-tient standing. A line was drawn from one anterioriliac spine to the other, sweeping low across thecentral abdomen either at or as much as 4 cmbelow the superior margin of the escutcheon, de-pending on the mobility of the pubic tissues andthe location of the umbilicus. The segment ofabdominal tissue to be excised was predeterminedby connecting one anterior iliac spine to the otherwith a curving line that arched just above the um-bilicus. The specimen always included the umbil-ical aperture; because of the mobility that wideundermining affords, no “T” incisions were evernecessary. (2) General anesthesia and sequentialcompression booties (Plexipulse) were used on allpatients. (3) Six patients had preinfiltration oftumescent solution (1 liter of saline, 30 cc of 1%lidocaine, 1 cc of 1:1000 epinephrine) into thesubcutaneous space to facilitate dissection; 175did not. (4) To gain direct access to the deep fat,traditional wide elevation was done to the xyphoidand beyond the lower rib margins superiorly andlaterally at least as far as the anterior axillary line.(5) Perforating vessels and bleeders in the super-ficial fatty layer were carefully cauterized. (6) Mid-line diastasis was corrected with nonabsorbable 0Mersilene sutures after the predetermined excessskin/fat segment was removed. (7) Starting at thecut edge of the flap where Scarpa’s fascia can bemost easily identified and using Wilkinson scissors(Padgett P6873TC) the deep fat in all zones of flapas far superiorly as the xyphoid and as far laterallyas it was identifiable was easily skived off evenindistinct fascia. (The broad flat blades of thesescissors glide along Scarpa’s fascia even when it isindistinct. Penetrations are unusual and heraldedby brisk bleeding.) Amounts removed rangedfrom a few cubic centimeters in very thin patientsto more than a liter in heavier patients. (8) Lipo-suction of the abdominal flap was never done, butconcurrent flank liposuction was performed whendeemed appropriate, usually because it was theonly additional area needing attention. (9) Suc-tion drains were placed and exited in the supra-pubic region. (10) The neoumbilicus was locatedwith the patient in a flexed position by placingtemporary sutures to coapt the deep fascia andskin at the midline. (11) Temporary sutures wereremoved, the flap was everted, and perineoum-bilical and supraneoumbilical fat contouring wasdone at the midline to create an aesthetic umbi-licus. (12) The main incision was closed in twolayers using 2-0 Mersilene to coapt the deep fasciallayer and 3-0 running subcuticular polydioxanone
Fig. 1. The two sets of arrows show Scarpa’s fascia and the largeblood vessels running in the superficial fatty layer. There is nosignificant blood supply deep to Scarpa’s fascia. This photographwas taken after the deep fat was removed from the right half ofthe abdominoplasty flap in the zone considered at risk for lipo-suction (“terrible abdominoplasty triangle”), leaving the superfi-cial fat in pristine condition.
Plastic and Reconstructive Surgery • May 2009
1598

suture in the skin. (13) Tegaderm was used as thesole incisional dressing. (14) The umbilicus wasclosed with interrupted half-buried 5-0 nylon hor-izontal and vertical mattress sutures and dressedwith antibiotic ointment and a single 4 � 4 gauze.(15) An abdominal binder was applied in therecovery room to apply modest support; it wasfrequently adjusted and routinely kept in placefor 21 days.
Chart ReviewsChart reviews were performed of patients who
underwent abdominoplasty in the 10-year periodbetween January of 1998 and December of 2007.The incidence of flap erythema, minor epidermol-ysis, frank tissue necrosis, seroma, deep vein throm-bosis, pulmonary embolism, transfusion, and deathwere noted.
RESULTSIn the 10-year period between January of 1998
and December of 2007, 179 primary abdomino-plasties were performed on patients who had hadno previous transabdominal surgery and two pa-tients who had had previous subcostal cholecys-tectomies. Within the group of 181 patients, therewere 30 who had concurrent flank liposuction.This subgroup was analyzed separately to ascertainwhether the addition of flank liposuction had anyeffect on the incidence of complications. All pro-cedures were performed at the same outpatientfacility under general anesthesia. In the first yearsof the study, the procedures were performed ex-clusively by the senior author, whose techniquewas adopted by the junior surgeon upon his arrivalin 2003 without variation, except for six patients inwhom tumescent solution was preinfiltrated to fa-cilitate dissection. The average operative time inthe main study group was 120 minutes for bothsurgeons.
The entire study group of 181 patients expe-rienced no deep vein thromboses, pulmonary em-bolisms, transfusions, or death. The addition ofthe tumescent wetting solution had no effect onthe rate of any complication. One of the two pa-tients with a cholecystectomy scar developed a se-roma, but neither patient experienced any wound-healing difficulties.
In the main group of 151 patients who did notreceive flank liposuction, there were five instances(3.3 percent) of limited epidermolysis at the in-cision line that healed spontaneously, two instances(1.3 percent) of localized skin erythema suggestiveof cellulitis treated with oral antibiotics with res-
olution, and one instance (0.7 percent) of limitedfull-thickness tissue loss at the incision line requir-ing subsequent scar revision.
The group of 30 patients who had concurrentflank liposuction had one instance (3.3 percent) oflocalized erythema treated with antibiotics, two in-stances (6.7 percent) of epidermolysis that healedspontaneously, and two instances (6.7 percent) offull-thickness tissue loss at the incision line sufficientto require wound management and later scar revi-sion. (Table 1).
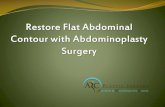
In the abdominoplasty group of 151 patients,there were 12 seromas treated successfully by aspi-ration (7.9 percent) and 14 that were treated byinsertion of a Penrose drain (9.2 percent; combinedseroma rate of 17.1 percent). The group of 30 pa-tients having concurrent flank liposuction devel-oped two seromas treated by aspiration (6.7 percent)and two with Penrose drain insertion (6.7 percent;combined seroma rate of 13.4 percent) (Table 2). Inall cases, the procedure fulfilled patient expectationsto such a degree that the inconvenience of manag-ing the occasional seroma or transient wound-heal-ing problems or the need for minor scar revision didnot have a discernible impact on patient satisfaction(Figs. 2 through 4).
DISCUSSIONThe amount of abdominal wall fat varies in re-
lation to body mass index. At any weight, the thick-ness of the superficial layer is commensurate withsubcutaneous tissue in other locations (this can beconfirmed with a standard “pinch test” after thedeep fat is removed), and for this reason it is aes-thetically unwise to manipulate it. The deep layer ismuch more variable, and its accumulation, as with
Table 1. Wound-Healing Complications
AllPatients
AbdominoplastyAlone
ConcurrentFlank
Liposuction
No. of patients 181 151 30Epidermolysis 3.9% 3.3% 6.7%Cellulitis 1.7% 1.3% 3.3%Necrosis 1.7% 0.7% 6.7%Total 7.3% 5.5% 16.7%
Table 2. Seroma Rate
AllPatients
AbdominoplastyAlone
ConcurrentFlank
Liposuction
No. of patients 181 151 30Aspiration 7.7% 7.9% 6.7%Penrose 8.8% 9.2% 6.7%Total 16.5% 17.1% 13.4%
Volume 123, Number 5 • Abdominoplasty with Deep Fat Resection
1599

that of intra-abdominal fat, may be geneticallydetermined.18 At any thickness, removal of deep fatis aesthetically beneficial as it slenderizes the abdo-men without risking the contour deformities asso-ciated with manipulations of the superficial layer.
Although the deep layer is completely expend-able, we have been unable to accomplish its entire
removal using liposuction without inadvertentdamage to the superficial layer. Our limitations inthis regard do not appear to be unusual. Exami-nation of resected abdominoplasty specimens ofpatients who have had previous abdominal li-posuction elsewhere have consistently revealedincomplete removal of the deep fat and nearly
Fig. 2. Patient 1 was 46 years old, 5 feet 5 inches tall, and weighed 194 pounds. No liposuction was performed. Note that deep fatremoval facilitates matching the thickness of the superior and inferior edges of the incision.
Fig. 3. Patient 2 was 49 years old, 5 feet 2 inches tall, and 155 pounds. No liposuction was performed. Continuous wide underminingto the xyphoid and beyond the lower rib margins ensured correction of laxity in the superior abdomen.
Plastic and Reconstructive Surgery • May 2009
1600

universal violation of the superficial layer with re-sulting contour irregularities. The inherent inabil-ity of liposuction to discriminate deep from su-perficial fat provides the justification for cautionwhen using it during an abdominoplasty. The realdanger zone, however, is not the “terrible abdomi-noplasty triangle,”10 from which deep fat can beremoved with impunity, but the entire superficiallayer. The 0.7 percent incidence of limited full-thickness healing problems we report in our maingroup of 151 patients is lower than that of mostprevious reports9,18–21 and substantiates the safetyof direct resection of deep fat from all areas of theabdominoplasty flap, including the central zoneconsidered dangerous for liposuction. In fact, thecentral “danger” zone provides the majority of theharvested fat, a fact that underscores the malad-aptation of liposuction to abdominoplasty.
Limited peri-incisional full-thickness loss re-quiring scar revision occurred in two of the 30patients who had abdominoplasty combined withflank liposuction. Although these two problemscaused the rate of this complication to escalatefrom 0.7 percent in the main group to 6.7 percentin this group, the small sample size (n � 30) makesthis difference insignificant (two-proportion z test,z � 1.572; two-tail confidence level, 88.4 percent).In addition to these two patients, three others inthe group of 30 having concomitant flank lipo-suction experienced cellulitis or epidermolysis not
requiring surgical intervention. Again, althoughthe percentage of these combined problems es-calated from 4.6 percent in the main group (n �151) to 10 percent in the smaller group (n � 30),there is no statistically significant difference be-tween the two frequencies (two-proportion z test,z � 0.0736l; two-tail confidence level, 53.8 per-cent). When all three categories of wound-healingproblems in each group are taken together and theoverall rates compared using the same two-propor-tion z test, the difference (somewhat surprisingly) isjust barely significant (z � 1.816, two-tail confidencelevel, 93.1 percent). A brief discussion is warranted.
Aggressive multidirectional liposuction of theflanks may damage collateral flow,10 especially if itis done widely enough to extend above the waist-line, and it is generally acknowledged that wound-healing problems escalate when procedures arecombined,9 operative times are prolonged, or coretemperature drops.22,23 Both patients requiringscar revision had ultrasonic liposuction over ex-tended areas of the posterolateral flanks, and onehad inner and outer thigh ultrasonic liposuctionas well. Operative times were prolonged to 3.5hours and 4.5 hours, respectively, from an averagetime of 2 hours. Neither patient was a smoker, butboth were overweight (body mass index of 26.5and 27.4, respectively) and both developed post-operative seromas. The small sample size and themultiplicity of risk factors make it impossible to
Fig. 4. Patient 3 was 38 years old, 5 feet 8 inches tall, and 205 pounds. No liposuction was performed. Even in obese patients, removalof just the deep fat is sufficient to slenderize the abdomen.
Volume 123, Number 5 • Abdominoplasty with Deep Fat Resection
1601

draw any definitive conclusions about the cause ofthe marginally significant increase in wound-heal-ing problems seen in the flank liposuction group.The commonality of liposuction to all the cases,however, suggests that collateral circulation can becompromised with aggressive flank liposuctioneven when the flap is otherwise robust. These ex-periences reinforce our general preference to per-form an abdominoplasty as a stand-alone proce-dure and account for why only 30 of 181 patientshad combined procedures.
Our rate of seroma formation (Table 2) isabout midrange when compared with that inother reports in the literature, which vary from 6.5to 90 percent.24–27 Variations in observational dil-igence and patient obesity have been cited as pos-sible contributing factors to differences in re-ported rates of seroma formation,24 as has theextent of undermining,10 which in our procedurecannot be easily limited due to the need for directaccess to deep fat. Although they were widely un-dermined in our practice, slim patients with little orno fat removed rarely developed seromas. Thiswould seem to minimize the effect of wide under-mining and point instead to a consequence of fatremoval, which, in the case of our patients who de-veloped seromas, was often extensive and locatedentirely at the adipose-fascial interface (it may alsomean that binders are more effective in maintainingtissue apposition when the abdominal flap is thin).We have used either small-caliber (10 Fr) rounddrains (Axiom Atraum CWV 3626AT, Torrance,Calif.) or larger 10 � 4-mm flat drains (AxiomAtraum CMV 3642AT) monitored for effectivenessand kept in place until drainage ceases, usually be-tween 7 and 14 days. There was no relationship be-tween the amount of drainage and the size of thedrain, and no fluid collections were noted while thedrains were in place. Because seromas formed afterthe drains were removed, neither drain size exertedany influence on the rate of their discovery (we sus-pect but cannot prove that imperfect patient com-pliance with admonitions to limit bending and twist-ing motions and to continue using the compressionbinder may contribute to seroma formation afterdrain removal). Promptly identified and adequatelytreated seromas represent temporary and relativelyminor management problems, the inconvenience ofwhich has not tempted us to alter our technique oremploy questionably effective measures, such as pro-gressive tension (quilting) sutures.28–31
The absence of major flap necrosis and the low0.7 percent incidence of limited full-thickness tis-sue compromise we report in our main studygroup can be largely attributable to protection of
the superficial fatty layer that is home to the es-sential vasculature of the abdominal wall. In ad-dition, we think the following factors may alsohave played some role in contributing to our lowrate of tissue compromise:
1. Traditional wide undermining superiorlyand laterally provides maximum flap mobil-ity and minimum closure tension.
2. Tangential resection of all deep adipose tissuemay diminish metabolic demand enough toprovide the flap with a small survival advan-tage.
3. Aggressive removal of all deep fat from thepart of the flap that is advanced to cover thearea from umbilicus to pubis (the “terribleabdominoplasty triangle”) facilitates healingby debulking the flap where closure tensionis highest (removal of deep fat from this areaalso eliminates the characteristic step-off de-formity along the incision line resultingfrom mismatched tissue thicknesses).
4. Perineoumbilical and supraneoumbilical mid-line defatting provides additional relief of clo-sure tension at the midline.
5. Reapposition of Scarpa’s fascia and runningsubcuticular skin closure eliminates the pointpressure that interrupted dermal sutures placeon the subcutaneous tissue or dermis.
6. Avoidance of all gauze dressings at the inci-sion line eliminates any bulk that could putfocal pressure on the flap.
7. The use of the abdominal binder providessupport and gentle apposition of the tissueplanes rather than compression to preventhematoma.
CONCLUSIONSJust the adipose tissue located deep to Scarpa’s
fascia needs be removed to attain the aestheticgoals of abdominoplasty, and this can be accom-plished safely with an open, direct approach. Be-cause liposuction easily compromises flap surviv-ability, it presents risks that are not associated withdirect tangential resection of subscarpal fat duringabdominoplasty.
Robert R. Brink, M.D.San Mateo Surgery Center
66 Bovet RoadSuite 101-103
San Mateo, Calif. [email protected]
REFERENCES1. Kelly HA. Report of gynecological cases (excessive growth of
fat). Case 3. Bull Johns Hopkins Hosp. 1889;10:197.
Plastic and Reconstructive Surgery • May 2009
1602

2. Pitanguy I. Abdominal lipectomy: An approach to it throughan analysis of 300 consecutive cases. Plast Reconstr Surg. 1967;40:384.
3. Grazer FM. Body Image, a Surgical Perspective. St. Louis: C. V.Mosby; 1980:63–145.
4. Illouz YG. A new safe and aesthetic approach to suctionabdominoplasty, Aesthet Plast Surg. 1992;16:237.
5. Brauman D. Liposuction abdominoplasty: An evolving con-cept. Plast Reconstr Surg. 2003;112:288.
6. Dillerud E. Abdominoplasty combined with suction lipo-plasty: A study of complications, revisions, and risk factors in487 cases. Ann Plast Surg. 1990;25:333.
7. Ousterhout DK. Combined suction-assisted lipectomy, sur-gical lipectomy and surgical abdominoplasty. Ann Plast Surg.1990;24:126.
8. Ramierz O. Abdominoplasty and abdominal wall rehabilita-tion: A comprehensive approach. Plast Reconstr Surg. 2000;105:425.
9. Matarasso A, Swift RW, Rankin M. Abdominoplasty and ab-dominal contour surgery: A national plastic surgery survey.Plast Reconstr Surg. 2006;117:1797.
10. Matarasso A. Liposuction as an adjunct to full abdomino-plasty. Plast Reconstr Surg. 1995;95:829.
11. Saldanha OR, Pinto EBDS, Mattos WN, et al. Lipoabdomi-noplasty with selective and safe undermining. Aesthet PlastSurg. 2003;27:322.
12. Brauman D. Liposuction abdominoplasty: An evolving con-cept. Plast Reconstr Surg. 2003;112:288.
13. Taylor GI, Daniel RK. The anatomy of several free flap donorsites. Plast Reconstr Surg. 1975;56:243.
14. Hester TR Jr, Nahai F, Beegle PE, Bostwick J III. Blood supplyof the abdomen revisited, with emphasis on the superficialinferior epigastric artery. Plast Reconstr Surg. 1984;74:657.
15. Worseg AP, Kuzbari R, Hubsch P, et al. Scarpa’s fascia flap:Anatomic studies and clinical application, Plast Reconstr Surg.1984;74:1368.
16. Schaverien M, Saint-Cyr M, Arbique G, Brown SA. Arterialand venous anatomies of the deep inferior epigastric perfo-rator and superficial inferior epigastric artery flaps. PlastReconstr Surg. 2008;121:1909.
17. Gradinger GP, Rosenfield LK, Nahai FR. The Art of AestheticSurgery. St Louis: Quality Medical Publishing; 2005:2355.
18. Lear SA, Humphries KH, Kohli S, Chockalingam A, FrohlichJJ, Birmingham CL. Visceral adipose tissue accumulationdiffers according to ethnic background: results of the Mul-
ticultural Community Health Assessment Trial (M-CHAT).Am J Clin Nutr. 2007;86:353–359.
19. Stewart KJ, Steware DA, Coghlan B, Harrison DH, Jones BM,Waterhouse N. Complications of 278 consequetive abdomi-noplasties, J Plast Reconstr Aesthet Surg. 2006;59:1152–1155.
20. Hensel JM, Lehman JA Jr, Tantri MP, Parker MG, WagnerDS, Topham NS. An outcomes analysis and satisfaction sur-vey of 199 consecutive abdominoplasties. Ann Plast Surg.2001;46:357–363.
21. Mayr M, Holm C, Hofter E, Becker A, Pfeiffer U, MuhlbauerW. Effects of aesthetic abdominoplasty on abdominal wallperfusion: A quantitive evaluation, Plast Reconstr Surg. 2004114:1586–1594.
22. Heller JB, Teng E, Knoll BI, Persing J. Outcome analysis ofcombined lipoabdominoplasty versus conventional abdomi-noplasty. Plast Reconstr Surg. 2008;121:1821–1829.
23. Kutz A, Sessler DI, Lenhardt R. Perioperative normothermiato reduce the incidence of surgical-wound infection andshorten hospitalization: Study of Wound Infection and Tem-perature Group. N Engl J Med. 1996;334:1209–1215.
24. Beilin B, Shavit Y, Razumovsky J, Wolloch Y, Zeidel A, BesslerH. Effects of mild perioperative hypothermia on cellularimmune response. Anesthesiology 1998;89:1133–1140.
25. Kim J, Stevenson TR. Abdominoplasty, liposuction of theflanks and obesity: Analyzing risk factors for seroma forma-tion. Plast Reconstr Surg. 2006;117:773.
26. Kryger ZB, Fine NA, Mustoe TA. The outcome of abdomi-noplasty performed under conscious sedation: Six-year ex-perience in 153 consecutive cases. Plast Reconstr Surg. 2004;113:1807.
27. Chaouat M, Levan P, Lalanne B, Buisson T, Nicolau P, Mi-moun M. Abdominal dermolipectomies: Early post-operativecomplications and long-term unfavorable results. Plast Re-constr Surg. 2000;106:1614.
28. Baroudi R, Ferreria A. Contouring the hip and abdomen.Clin Plast Surg. 1996;23:551.
29. Khan S, Teotia SS, Mullis WF, et al. Do progressive tensionsutures really decrease complications in abdominoplasty?Ann Plast Surg. 2006;56:14–20.
30. Khan UD. Risk of seroma with simultaneous liposuction andabdominoplasty and the role of progressive tension sutures.Aesthet Plast Surg. 2008;32:93–99.
31. Andrades P, Prado A, Danilla S, et al. Progressive tensionsutures in the prevention of postabdominoplasty seroma: Aprospective, randomized, double-blind clinical trial. Plast Re-constr Surg. 2007;120:935–946.
Volume 123, Number 5 • Abdominoplasty with Deep Fat Resection
1603