Abdominal/Thorax Unit 1. ABDOMINAL CAVITY ANATOMY 2.
64
Abdominal/Thorax Unit 1
-
Upload
barnard-johnston -
Category
Documents
-
view
270 -
download
0
Transcript of Abdominal/Thorax Unit 1. ABDOMINAL CAVITY ANATOMY 2.

1
Abdominal/Thorax Unit

2
ABDOMINAL CAVITY ANATOMY

3
Terminology
• Absorption: a process where digested food moves into the bloodstream to be used throughout the body
• Antibodies: a type of cell produced by the spleen to defend the body against foreign cells
• Bile: a substance produced by the liver that neutralizes the acid of the stomach and helps digest fat in the small intestine

4
Terminology
• Chyme: a semi-liquid substance formed when ingested food is mixed with digestive fluids from the stomach
• Detoxify: the process of breaking down harmful chemicals
• Diaphragm: a large muscle located between the chest and the abdomen that helps control breathing

5
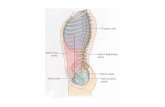
Abdominal Cavity Borders
• Anterior– Abdominal
musculature
• Posterior– Lumbar spine
• Superior– Diaphragm
• Inferior– Pelvis

6
The Abdominal Cavity• Divided into 4
quadrants which intersect at the navel– Upper right– Upper left– Lower right– Lower left

7
The Abdominal Cavity• Contains organs from 3 body systems– Digestive– Urinary– Reproductive

8
The Liver
• Secretes bile for digestion• Detoxifies harmful chemicals

9
The Gall Bladder• Stores bile from the liver used in digestion

10
The Pancreas
• Produces insulin & glucagon• Secretes pancreatic juice for digestion

11
The Kidneys
• Filter blood from the rest of the body & excrete waste products in the form of urine

12
The Stomach
• Food mixes with secretions to form chyme

13
The Spleen
• Stores and regulates the number of red blood cells in the body
• Produces antibodies

14
Small Intestine
• The majority of digestion and absorption occurs here

15
Large Intestine
• Final digestion and absorption of food occurs
• Chyme is converted to feces to be expelled

16
Urinary Bladder• Stores urine

17
Abdominal Organs
• Solid organs– Organs that contain a large blood supply– Injury to these organs is generally life-threatening– Examples: liver, kidneys, spleen & pancreas
• Hollow organs– Organs that are able to bend & move– Injury to these organs is less serious– Examples: stomach, intestines, appendix

18
THORACIC CAVITY ANATOMY

19
Terminology
• Atrium: upper chamber of the heart• Intercostal: refers to the area between the
ribs• Thorax: the chest; the part of the body
located between the neck and the abdomen• Ventricle: lower chamber of the heart

20
Thoracic Cavity Borders
• Superior– Clavicle
• Inferior– Diaphragm
• Anterior– Sternum, ribs and intercostal muscles
• Posterior– Spine, ribs, scapulae & erector spinae muscle

21
The Rib Cage

22
The Rib Cage
• 12 pairs of ribs– True ribs (first 7 pairs): attach directly to the
sternum by individual cartilage– False ribs (next 3 pairs): attach indirectly to the
sternum by shared cartilage– Floating ribs (next 2 pairs): have no attachment to
the sternum

23
Organs in the Thoracic Cavity
• Esophagus• Trachea• Lungs• Heart

24
The Esophagus
• Location:– In the throat,
behind the trachea
• Function:Structure for
food to pass from the mouth to the stomach

25
The Trachea
• Location:–A cartilage structure in the throat, directly
in front of the esophagus– The trachea divides into 2 branches
(bronchi) which enter the lungs• Function:–Allows air to pass into and out of the lungs

26
Divisions of the Respiratory System

27
The Lungs

28
The Lungs• Location:
On either side of the heart
• Functions:• Exchange carbon dioxide for oxygen • Help to remove heat from the body

29
The Heart
• Location:–Under the sternum (slightly to the left) and
between the lungs• Function: to pump blood throughout the body–Blood carries oxygen and nutrients to the
cells–Blood carries carbon dioxide and waste
products away from the cells

30
The Heart

31
The Heart
• Divided into 4 chambers– R and L atrium (upper chambers)– R and L ventricles (lower chambers)
• Heart valves separate each chamber and prevent a backflow of the blood– Tricuspid valve– Biscuspid (mitral) valve– Pulmonary valve– Aortic valve

32
ABDOMINAL INJURIES (EXTERNAL)

33
Terminology
• Hernia: a section of abdominal tissue comes through the abdominal wall
• Solar plexus: a group of nerves in the upper part of the abdomen that control breathing

34
Abdominal Injuries
• 1. Contusion / solar plexus injury• 2. Abdominal strain• 3. Hernia• 4. Testicular pathology

35
Contusion / Solar Plexus Injury
• Mechanism– A blow to the area causes a contusion or temporary paralysis of
the diaphragm muscle (“wind knocked out”)• Signs & Symptoms
– Pain– Temporary breathing difficulty - usually resolves quickly but may
result in loss of consciousness with more serious injury• Treatment
– Reassure the athlete– Loosen any restrictive clothing / padding– Apply ice for contusion– Monitor athlete for possible complications including shock

36
Abdominal Strain
• Mechanism– Hyperextension or reaching over head (rectus
abdominis) – Twisting / over-rotation , ie, baseball pitcher (obliques)
• Signs & Symptoms– Pain that increases during movement– Possible swelling / discoloration
• Treatment– Follow RICE – Gentle stretching / strengthening– Gradual pain-free return to activity

37
Hernia• Mechanism– Increase in abdominal pressure, such as holding one’s breath
during weightlifting• Signs & Symptoms– Deformity – bulge in abdominal area– Pain (usually decreases while lying & increases while
standing)– Increase in pain with activity
• Treatment– Temporary – strap to put pressure over the area– Surgery needed for repair, followed by extended recovery
period– Untreated may lead to tissue strangulation and death

38
Testicular Pathology• Explanation
– Injury to reproductive organs are more common in males because the genitalia of males are exposed.
• Mechanism:– Direct blow to the area or twisting mechanism (cut to the side while
foot is planted)• Signs & Symptoms:
– Acute testicular pain– Localized swelling– Nausea / vomiting possible
• Treatment:– Ice for contusion or area– Refer if pain doesn’t resolve or increases after 20 minutes– Need prompt medical attention to prevent atrophy/ other
complications

39
ABDOMINAL INJURIES (INTERNAL)

Kehr’s sign: radiating pain in the left shoulder and arm, resulting from an injury to the spleenReferred pain: pain that begins in one area, but is felt in another area of the body
40
TERMINOLOGY

Internal Abdomen Injuries
• 1. Kidney contusion / laceration• 2. Liver contusion• 3. Spleen rupture• 4. Pancreas injury
41

Kidney Contusion / Laceration
• Mechanism– Direct blow over area results in a contusion, laceration or rupture of
the kidney• Signs & Symptoms
– Pain under – Pain with trunk extension + hip and knee flexion– Blood in urine– Monitor for shock– Nausea, vomiting
• Treatment– Call EMS– Treat for shock– Surgical repair required– Long-term complications may include tissue scarring, hypertension 42

Liver Contusion• Mechanism– Blow to area (more vulnerable during hepatitis)
• Signs & Symptoms– Abdominal pain & referred pain in R shoulder– Rapid blood loss resulting in shock, weak pulse, ↓
blood pressure• Treatment– Call EMS– Treat for shock– Surgical repair required
43

Spleen Rupture• Mechanism
– Fall or direct blow to upper left quadrant (more likely to rupture when enlarged or infected, i.e., mononucleosis)
• Signs & Symptoms– Abdominal pain– Pain in L shoulder (Kehr’s sign)– Shock, progressing to loss of consciousness (LOC)– ↑ heart rate, ↓ blood pressure– Nausea, abdominal spasms & cramping
• Treatment– Call EMS– Treat for shock– Generally requires surgical removal– Unable to participate in contact sports 44

Pancreas Injury• Mechanism– Deceleration injury– Occurs when athlete is running and hits a wall, causing
pancreas to change directions suddenly• Signs & Symptoms– Pain in middle abdomen to back– Signs of shock– Vomiting / nausea
• Treatment– Call EMS– Treat for shock– Requires surgical repair 45

46
THORACIC INJURIES

47
Apnea: temporary stopping of breathingAsthma: condition in which the air passages constrict in response to a stimulus Dyspnea: difficulty breathingHemothorax: blood in the thoracic cavityPneumothorax: air in the thoracic cavity due to a collapsed lung
TERMINOLOGY

48
Thoracic Injuries
• Rib contusion / fracture• Exercise-induced asthma• Pneumothorax• Hemothorax• Myocardial contusion• Sudden death syndrome

49
Rib Contusion / Fracture • Mechanism
– Impact over area / compression• Signs & Symptoms
– Dyspnea– Pain is key to determine whether there is a contusion or a
fracture• Contusion? Pain remains constant during inhalation and exhalation• Fracture? Pain ↑ during inhalation and ↓ during exhalation
– Point tenderness– Possible deformity
• Treatment– Apply ice– Refer for x-ray

50
Exercise-Induced Asthma• Mechanism
– Physical activity and/or environmental conditions trigger a stimulus– The stimulus causes airway to constrict and/or ↑ mucous production
• Signs & Symptoms– Coughing– Wheezing– Dyspnea– Chest pain / tightness– Anxiety
• Treatment– Treat with inhaler (medication used to dilate bronchi)– Reassure and calm athlete– Call EMS if condition worsens– Gradual increase of activity in athletes with EIA

51
Hemothorax• Mechanism
– Internal injury: ruptured blood vessel or ruptured lung– External injury: penetrating wound
• Signs & Symptoms– Dyspnea– Bluish skin tone– Rapid, weak pulse– No breath sounds from injured side– Loss of consciousness
• Treatment– Call EMS– Control bleeding– Perform CPR if necessary

52
Pneumothorax
• Mechanism– Spontaneous (non-traumatic): lung tissue weakness– Tension (traumatic): laceration or rib fracture punctures lung
• Signs & Symptoms– Dyspnea / gasping for air– Chest pain– Bluish tint to skin
• Treatment– Call EMS– Place athlete on side with injured lung closest to the ground– Treat for shock

53
Myocardial Contusion• Mechanism
– Compression force (i.e., baseball player hit by pitch, barbell dropped on chest)
• Signs & Symptoms– Immediate, severe pain in chest– Rapid onset of shock– Possible complications of myocardial contusion
• Fluid buildup around the heart• Failure of electrical activity of heart• Fluid backup in lungs (congestive heart failure)• Damage to heart valves or muscle
• Treatment– Call EMS– Treat athlete for shock; administer CPR if needed

54
Sudden Death Syndrome• Mechanism
– Non-traumatic - caused by a pre-existing heart condition such as:• Thickening of heart muscle (hypertrophic cardiomyopathy)• Weakness of connective tissue (Marfan’s syndrome)• Congenital heart disease
• Signs & Symptoms– Chest pain during exercise– Irregular heart beat / racing of the heart– Shortness of breath– Excessive sweating– LOC due to lack of oxygen to the brain
• Treatment– Call EMS– Perform CPR with AED

55
REHAB/EVALUATION

56
HOPS Injury EvaluationHistory—a series of questions asked to determine nature and location of injuryObservation—A visual examination of the injury
Palpation—A hands-on approach where examiner feels for deformity or other abnormal findings Stress tests—A series of tests to check range of motion and degree of function of tissues at a joint

57
SOAP NOTES
Subjective—detailed information about the history of injury and athlete; chief complaints, sign, and symptoms
Objective—information that is record of test measurements; data gained from inspection
Assessment---Identification of problem; determine injury; severity of injury
Plan of Action--Treatment

58
Subjective - Questioning PromptsWhat happened? When did it happen?Was there a previous injury?What did you feel then?How do you feel now?Describe the type of pain.Where does it hurt?Did it make a sound?Have you had difficulty breathing?Are certain positions more comfortable than others?
Do you feel faint, light-headed or nauseous?How long has it been since you last ate?What did you eat?Do you have a personal or family history of any heart problems or abdominal problems?
* Ask for a witness if the person is incapable of answering

59
Objective: Inspection Prompts
Observe for the following:ApneaDyspneaBreathing patternsLack of deep breathingChest symmetry during breathingBody posture/position including leaning to the side or splinting/protecting with opposite hand
Deformity or protrusionsDiscolorationSwelling Gait / WalkFacial expressionsBleedingSkin colorScars

60
Completing the S & O
Subjective:History(Symptoms)
Objective:Observation & Palpation (Signs)

61
Abdomen & Thorax Palpation
• Bones– R & L chest walls– Movement of chest during inspiration & expiration– Rib(s) and intercostal space specific to injury
• Musculature– Rectus abdominis– Transverse abdominis– Obliques

62
Abdomen & Thorax Palpation• Palpate kidneys with athlete:
– Lying prone or standing
• Palpate the rest of the organs in each of the abdominal quadrants with athlete:– Lying supine– Arms at side– Hips and knees flexed

63
Abdomen & Thorax Palpation• When palpating , begin with upper right quadrant and move
clockwise.• Palpate for the following indications of abdominal injury or
internal bleeding:
– Muscle guarding or involuntary muscle contraction– Areas of rigidity or tightness– Areas of abdominal pain– Rebound tenderness– Referred pain

64
Abdomen & Thorax – Special Tests
• Trunk movements – perform active ROM, followed by resistive– Forward flexion or bending– Twisting– Side bending– Extension