
Abdominal CT Findings in Small Bowel Perforation
10
PICTORIAL REVIEW Abdominal CT findings in small bowel perforation 1 R ZISSIN, MD, 1 A OSADCHY, MD and 2 G GAYER, MD 1 Department of Diagnostic Imaging, Meir Medical Center, Kfar Saba and 2 Department of Diagnostic Imaging, Assaf Harofe Medical Center, Zrifin, Sackler Faculty of Medicine, Tel-Aviv University, Tel-Aviv, Israel ABSTRACT. Small bowel perforation is an emergent medical condition for which the diagnosis is usually not made clinically but by CT, a common imaging modality used for the diagnosis of acute abdomen. Direct CT features that suggest perforation include extraluminal air and oral contrast, which are often associated with secondary CT signs of bowel pathology. This pictorial review illustrates the CT findings of small bowel perforation caused by various clinical entities. Received 24 October 2006 Revised 13 January 2007 Accepted 16 January 2007 DOI: 10.1259/bjr/78772574 ’ 2009 The British Institute of Radiology Small bowel (SB) perforation is an emergency medical situation that presents as an acute abdomen, and is only rarely diagnosed clinically. Nowadays, as CT is often the initial modality used to assess patients with acute abdomen, the radiologist may be the first to suggest such a diagnosis [1–5]. CT provides superb anatomical detail and diagnostic specificity by directly imaging the intestinal wall, detecting secondary signs of bowel disease within the surrounding mesentery and depicting even small amounts of extraluminal air or oral contrast leakage into the peritoneal cavity [4, 5]. The purpose of this article is to illustrate the CT features of a spectrum of SB perforation caused by different aetiologies. CT technique Our abdominal CT protocol for evaluating the acute abdomen includes the administration of both oral and intravenous contrast medium unless contraindications exist. The use of a multislice helical scanner with both axial images and multiplanar reformations allows for high-quality visualization of the entire abdomen (Figure 1) [3, 5]. Water-soluble contrast agents do not provoke an inflammatory reaction when leaking into the peritoneal cavity, as they are rapidly absorbed [4]. Assessment of bone and lung window settings, in addition to the routine abdominal window setting, serves as a useful complementary tool for detecting intra- or extra-luminal radio-opaque foreign bodies and free intra-abdominal air (Figure 2) [6]. CT findings Diagnostically, extraluminal oral contrast is a specific sign of gastrointestinal tract (GIT) perforation, although its sensitivity is rather low (19–42%) [5]. Free intraper- itoneal air (more clearly seen on a lung window setting) is another specific sign of perforation in the intact abdomen. CT is the most reliable imaging modality for detecting even small amounts of free air (Figure 3) [1–4]. Additional CT signs that may also indicate the site of the perforation include discontinuity of the bowel wall on an enhanced scan and focal thickening of the bowel wall adjacent to extraluminal gas bubbles with localized mesenteric fatty infiltration (Figures 4 and 5) [2,4–7]. The overall accuracy in diagnosing the site of the perforation is .80% [5]. Yeung et al [2] also found that the presence of air in both sides of the falciform ligament (Figure 6) may differentiate more certainly proximal from distal GIT perforation. Aetiology SB perforation can be caused by traumatic, inflamma- tory, ischaemic and neoplastic aetiologies. When asses- sing a patient with CT findings suggestive of such a perforation, the relevant clinical and laboratory data should be taken into consideration, together with the presence of additional CT findings, in order to establish its aetiology (Table 1). Trauma and small bowel perforation Blunt abdominal trauma SB injury following blunt trauma is an infrequent insult with a difficult and challenging clinical diagnosis. Abdominal CT plays an important role in its early detection, with overall sensitivity of 64%, specificity of 97% and accuracy of 82% [7]. Extraluminal oral contrast and free air in the peritoneum, in the absence of a pneumothorax or pneumomediastinum, or even a few tiny gas bubbles within the mesentery are specific but Address correspondence to: R Zissin, Deptartment of Diagnostic Imaging, Meir Medical Center, Kfar Saba, 44281, Israel. E-mail: [email protected] The British Journal of Radiology, 82 (2009), 162–171 162 The British Journal of Radiology, February 2009
-
Upload
lisa-ekapratiwi -
Category
Documents
-
view
56 -
download
1
Transcript of Abdominal CT Findings in Small Bowel Perforation

PICTORIAL REVIEW
Abdominal CT findings in small bowel perforation
1R ZISSIN, MD, 1A OSADCHY, MD and 2G GAYER, MD
1Department of Diagnostic Imaging, Meir Medical Center, Kfar Saba and 2Department of Diagnostic Imaging, Assaf
Harofe Medical Center, Zrifin, Sackler Faculty of Medicine, Tel-Aviv University, Tel-Aviv, Israel
ABSTRACT. Small bowel perforation is an emergent medical condition for which thediagnosis is usually not made clinically but by CT, a common imaging modality used forthe diagnosis of acute abdomen. Direct CT features that suggest perforation includeextraluminal air and oral contrast, which are often associated with secondary CT signsof bowel pathology. This pictorial review illustrates the CT findings of small bowelperforation caused by various clinical entities.
Received 24 October 2006Revised 13 January 2007Accepted 16 January 2007
DOI: 10.1259/bjr/78772574
’ 2009 The British Institute of
Radiology
Small bowel (SB) perforation is an emergency medicalsituation that presents as an acute abdomen, and is onlyrarely diagnosed clinically. Nowadays, as CT is often theinitial modality used to assess patients with acuteabdomen, the radiologist may be the first to suggestsuch a diagnosis [1–5]. CT provides superb anatomicaldetail and diagnostic specificity by directly imaging theintestinal wall, detecting secondary signs of boweldisease within the surrounding mesentery and depictingeven small amounts of extraluminal air or oral contrastleakage into the peritoneal cavity [4, 5]. The purpose ofthis article is to illustrate the CT features of a spectrum ofSB perforation caused by different aetiologies.
CT technique
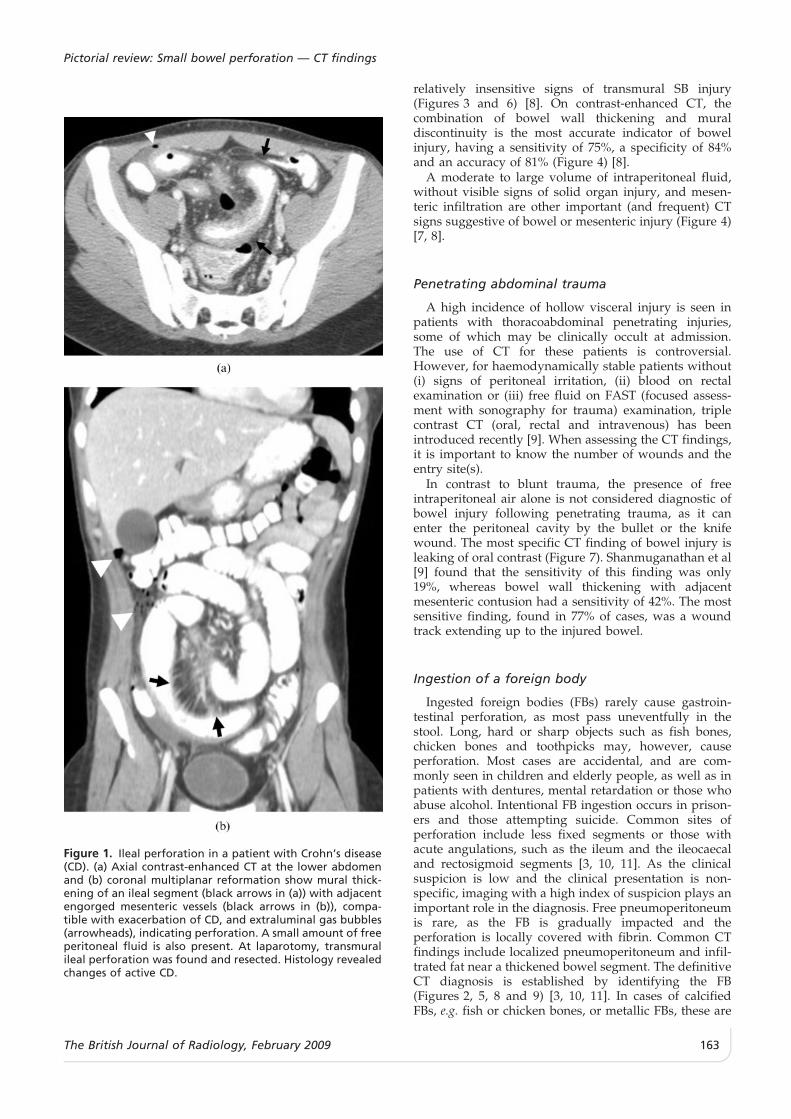
Our abdominal CT protocol for evaluating the acuteabdomen includes the administration of both oral andintravenous contrast medium unless contraindicationsexist. The use of a multislice helical scanner with bothaxial images and multiplanar reformations allows forhigh-quality visualization of the entire abdomen(Figure 1) [3, 5]. Water-soluble contrast agents do notprovoke an inflammatory reaction when leaking into theperitoneal cavity, as they are rapidly absorbed [4].Assessment of bone and lung window settings, inaddition to the routine abdominal window setting,serves as a useful complementary tool for detectingintra- or extra-luminal radio-opaque foreign bodies andfree intra-abdominal air (Figure 2) [6].
CT findings
Diagnostically, extraluminal oral contrast is a specificsign of gastrointestinal tract (GIT) perforation, although
its sensitivity is rather low (19–42%) [5]. Free intraper-itoneal air (more clearly seen on a lung window setting)is another specific sign of perforation in the intactabdomen. CT is the most reliable imaging modality fordetecting even small amounts of free air (Figure 3) [1–4].Additional CT signs that may also indicate the site of theperforation include discontinuity of the bowel wall on anenhanced scan and focal thickening of the bowel walladjacent to extraluminal gas bubbles with localizedmesenteric fatty infiltration (Figures 4 and 5) [2,4–7].The overall accuracy in diagnosing the site of theperforation is .80% [5].
Yeung et al [2] also found that the presence of air inboth sides of the falciform ligament (Figure 6) maydifferentiate more certainly proximal from distal GITperforation.
Aetiology
SB perforation can be caused by traumatic, inflamma-tory, ischaemic and neoplastic aetiologies. When asses-sing a patient with CT findings suggestive of such aperforation, the relevant clinical and laboratory datashould be taken into consideration, together with thepresence of additional CT findings, in order to establishits aetiology (Table 1).
Trauma and small bowel perforation
Blunt abdominal trauma
SB injury following blunt trauma is an infrequentinsult with a difficult and challenging clinical diagnosis.Abdominal CT plays an important role in its earlydetection, with overall sensitivity of 64%, specificity of97% and accuracy of 82% [7]. Extraluminal oral contrastand free air in the peritoneum, in the absence of apneumothorax or pneumomediastinum, or even a fewtiny gas bubbles within the mesentery are specific but
Address correspondence to: R Zissin, Deptartment of DiagnosticImaging, Meir Medical Center, Kfar Saba, 44281, Israel. E-mail:[email protected]
The British Journal of Radiology, 82 (2009), 162–171
162 The British Journal of Radiology, February 2009
relatively insensitive signs of transmural SB injury(Figures 3 and 6) [8]. On contrast-enhanced CT, thecombination of bowel wall thickening and muraldiscontinuity is the most accurate indicator of bowelinjury, having a sensitivity of 75%, a specificity of 84%and an accuracy of 81% (Figure 4) [8].
A moderate to large volume of intraperitoneal fluid,without visible signs of solid organ injury, and mesen-teric infiltration are other important (and frequent) CTsigns suggestive of bowel or mesenteric injury (Figure 4)[7, 8].
Penetrating abdominal trauma
A high incidence of hollow visceral injury is seen inpatients with thoracoabdominal penetrating injuries,some of which may be clinically occult at admission.The use of CT for these patients is controversial.However, for haemodynamically stable patients without(i) signs of peritoneal irritation, (ii) blood on rectalexamination or (iii) free fluid on FAST (focused assess-ment with sonography for trauma) examination, triplecontrast CT (oral, rectal and intravenous) has beenintroduced recently [9]. When assessing the CT findings,it is important to know the number of wounds and theentry site(s).
In contrast to blunt trauma, the presence of freeintraperitoneal air alone is not considered diagnostic ofbowel injury following penetrating trauma, as it canenter the peritoneal cavity by the bullet or the knifewound. The most specific CT finding of bowel injury isleaking of oral contrast (Figure 7). Shanmuganathan et al[9] found that the sensitivity of this finding was only19%, whereas bowel wall thickening with adjacentmesenteric contusion had a sensitivity of 42%. The mostsensitive finding, found in 77% of cases, was a woundtrack extending up to the injured bowel.
Ingestion of a foreign body
Ingested foreign bodies (FBs) rarely cause gastroin-testinal perforation, as most pass uneventfully in thestool. Long, hard or sharp objects such as fish bones,chicken bones and toothpicks may, however, causeperforation. Most cases are accidental, and are com-monly seen in children and elderly people, as well as inpatients with dentures, mental retardation or those whoabuse alcohol. Intentional FB ingestion occurs in prison-ers and those attempting suicide. Common sites ofperforation include less fixed segments or those withacute angulations, such as the ileum and the ileocaecaland rectosigmoid segments [3, 10, 11]. As the clinicalsuspicion is low and the clinical presentation is non-specific, imaging with a high index of suspicion plays animportant role in the diagnosis. Free pneumoperitoneumis rare, as the FB is gradually impacted and theperforation is locally covered with fibrin. Common CTfindings include localized pneumoperitoneum and infil-trated fat near a thickened bowel segment. The definitiveCT diagnosis is established by identifying the FB(Figures 2, 5, 8 and 9) [3, 10, 11]. In cases of calcifiedFBs, e.g. fish or chicken bones, or metallic FBs, these are
Figure 1. Ileal perforation in a patient with Crohn’s disease(CD). (a) Axial contrast-enhanced CT at the lower abdomenand (b) coronal multiplanar reformation show mural thick-ening of an ileal segment (black arrows in (a)) with adjacentengorged mesenteric vessels (black arrows in (b)), compa-tible with exacerbation of CD, and extraluminal gas bubbles(arrowheads), indicating perforation. A small amount of freeperitoneal fluid is also present. At laparotomy, transmuralileal perforation was found and resected. Histology revealedchanges of active CD.
Pictorial review: Small bowel perforation — CT findings
The British Journal of Radiology, February 2009 163
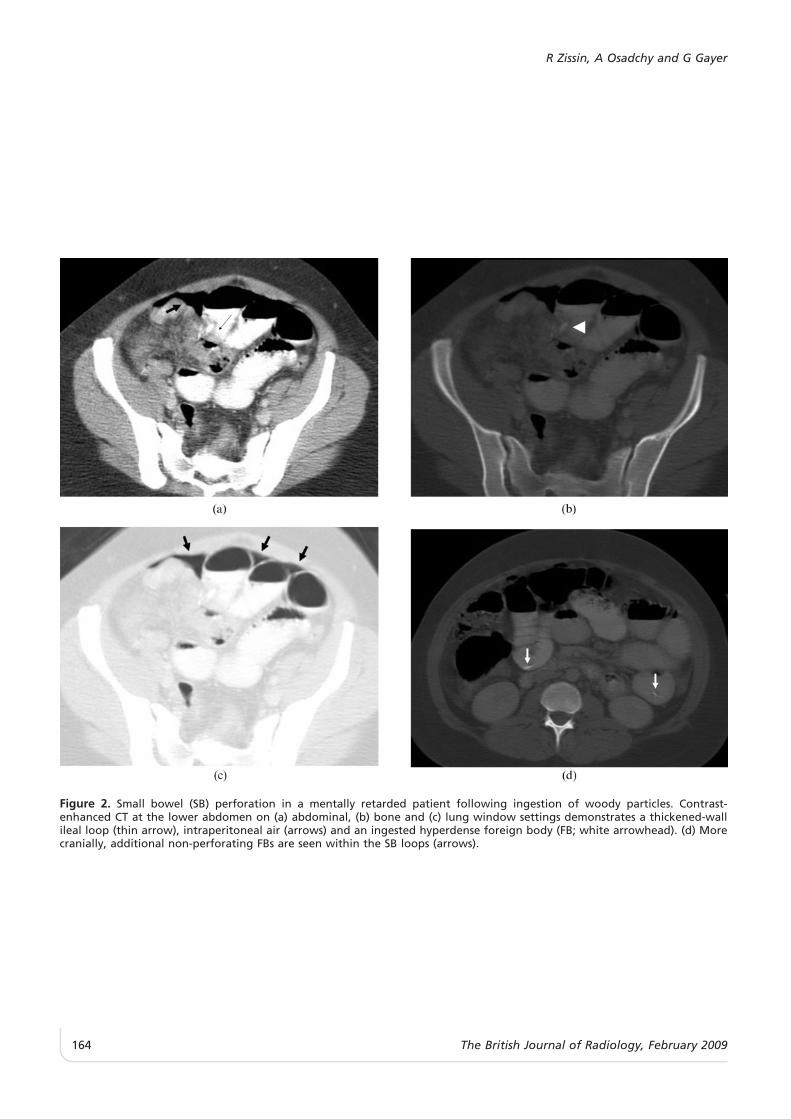
Figure 2. Small bowel (SB) perforation in a mentally retarded patient following ingestion of woody particles. Contrast-enhanced CT at the lower abdomen on (a) abdominal, (b) bone and (c) lung window settings demonstrates a thickened-wallileal loop (thin arrow), intraperitoneal air (arrows) and an ingested hyperdense foreign body (FB; white arrowhead). (d) Morecranially, additional non-perforating FBs are seen within the SB loops (arrows).
R Zissin, A Osadchy and G Gayer
164 The British Journal of Radiology, February 2009
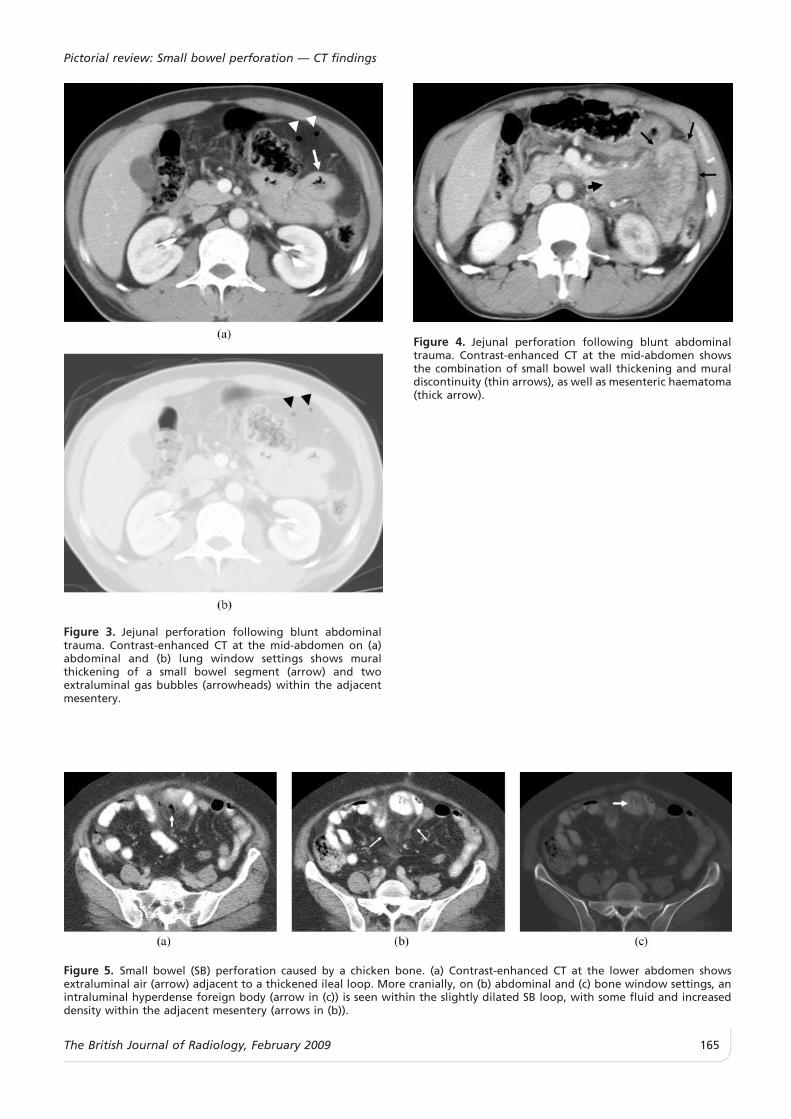
Figure 3. Jejunal perforation following blunt abdominaltrauma. Contrast-enhanced CT at the mid-abdomen on (a)abdominal and (b) lung window settings shows muralthickening of a small bowel segment (arrow) and twoextraluminal gas bubbles (arrowheads) within the adjacentmesentery.
Figure 4. Jejunal perforation following blunt abdominaltrauma. Contrast-enhanced CT at the mid-abdomen showsthe combination of small bowel wall thickening and muraldiscontinuity (thin arrows), as well as mesenteric haematoma(thick arrow).
Figure 5. Small bowel (SB) perforation caused by a chicken bone. (a) Contrast-enhanced CT at the lower abdomen showsextraluminal air (arrow) adjacent to a thickened ileal loop. More cranially, on (b) abdominal and (c) bone window settings, anintraluminal hyperdense foreign body (arrow in (c)) is seen within the slightly dilated SB loop, with some fluid and increaseddensity within the adjacent mesentery (arrows in (b)).
Pictorial review: Small bowel perforation — CT findings
The British Journal of Radiology, February 2009 165
more easily detected on a bone window setting(Figures 5 and 8). In cases of wooden FBs, e.g. skewersand chopsticks, these have either low or high attenua-tion: dry wood has high air content, seen on a lungwindow setting (Figure 9), whereas fresh wood has highwater content and a higher density (Figure 2).
Iatrogenic SB injury
Intra-operative injuryLaparoscopic surgery has now replaced many lapar-
otomy procedures. Rarely, serious complications invol-ving the GIT may occur, caused by the laparoscopicinstruments [12, 13]. The SB is the most commonlyaffected site and the injury is usually discovered andtreated during surgery. Unrecognized laparoscopy-induced bowel injury is associated with a high post-operative morbidity rate, necessitating early CTimaging. In reconstructive GIT surgery, the finding of
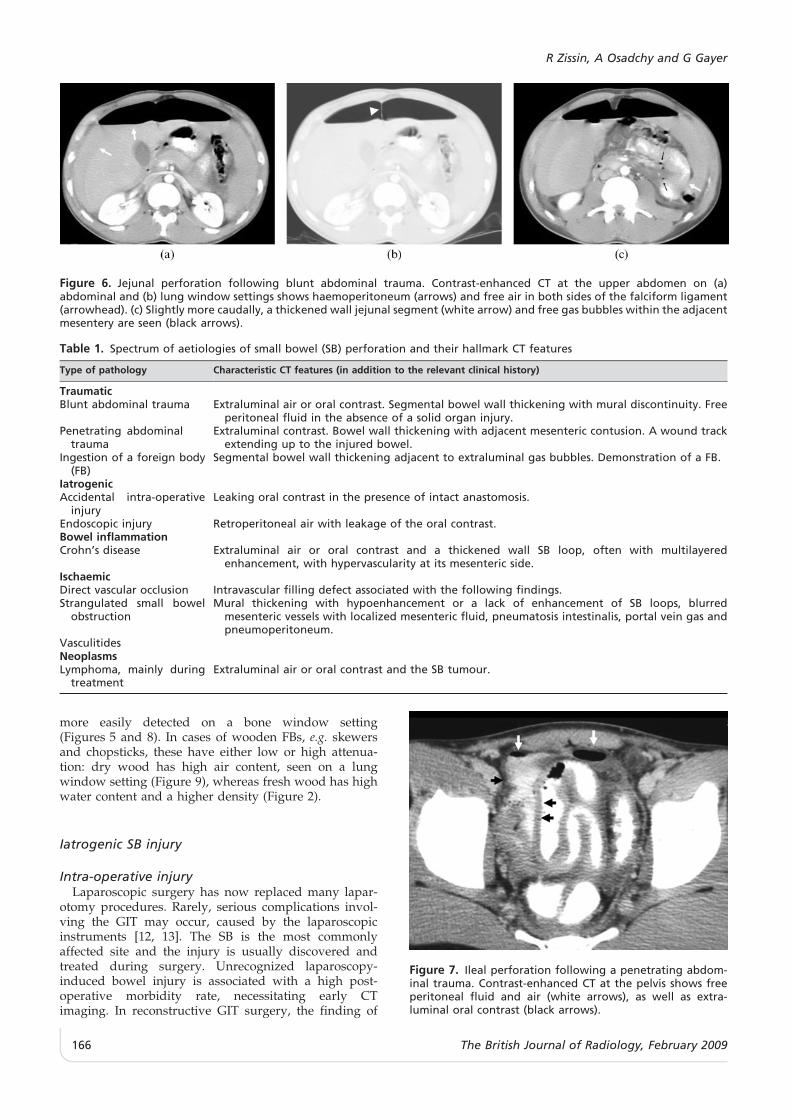
Figure 6. Jejunal perforation following blunt abdominal trauma. Contrast-enhanced CT at the upper abdomen on (a)abdominal and (b) lung window settings shows haemoperitoneum (arrows) and free air in both sides of the falciform ligament(arrowhead). (c) Slightly more caudally, a thickened wall jejunal segment (white arrow) and free gas bubbles within the adjacentmesentery are seen (black arrows).
Table 1. Spectrum of aetiologies of small bowel (SB) perforation and their hallmark CT features
Type of pathology Characteristic CT features (in addition to the relevant clinical history)
TraumaticBlunt abdominal trauma Extraluminal air or oral contrast. Segmental bowel wall thickening with mural discontinuity. Free
peritoneal fluid in the absence of a solid organ injury.Penetrating abdominal
traumaExtraluminal contrast. Bowel wall thickening with adjacent mesenteric contusion. A wound track
extending up to the injured bowel.Ingestion of a foreign body
(FB)Segmental bowel wall thickening adjacent to extraluminal gas bubbles. Demonstration of a FB.
IatrogenicAccidental intra-operative
injuryLeaking oral contrast in the presence of intact anastomosis.
Endoscopic injury Retroperitoneal air with leakage of the oral contrast.Bowel inflammationCrohn’s disease Extraluminal air or oral contrast and a thickened wall SB loop, often with multilayered
enhancement, with hypervascularity at its mesenteric side.IschaemicDirect vascular occlusion Intravascular filling defect associated with the following findings.Strangulated small bowel
obstructionMural thickening with hypoenhancement or a lack of enhancement of SB loops, blurred
mesenteric vessels with localized mesenteric fluid, pneumatosis intestinalis, portal vein gas andpneumoperitoneum.
VasculitidesNeoplasmsLymphoma, mainly during
treatmentExtraluminal air or oral contrast and the SB tumour.
Figure 7. Ileal perforation following a penetrating abdom-inal trauma. Contrast-enhanced CT at the pelvis shows freeperitoneal fluid and air (white arrows), as well as extra-luminal oral contrast (black arrows).
R Zissin, A Osadchy and G Gayer
166 The British Journal of Radiology, February 2009
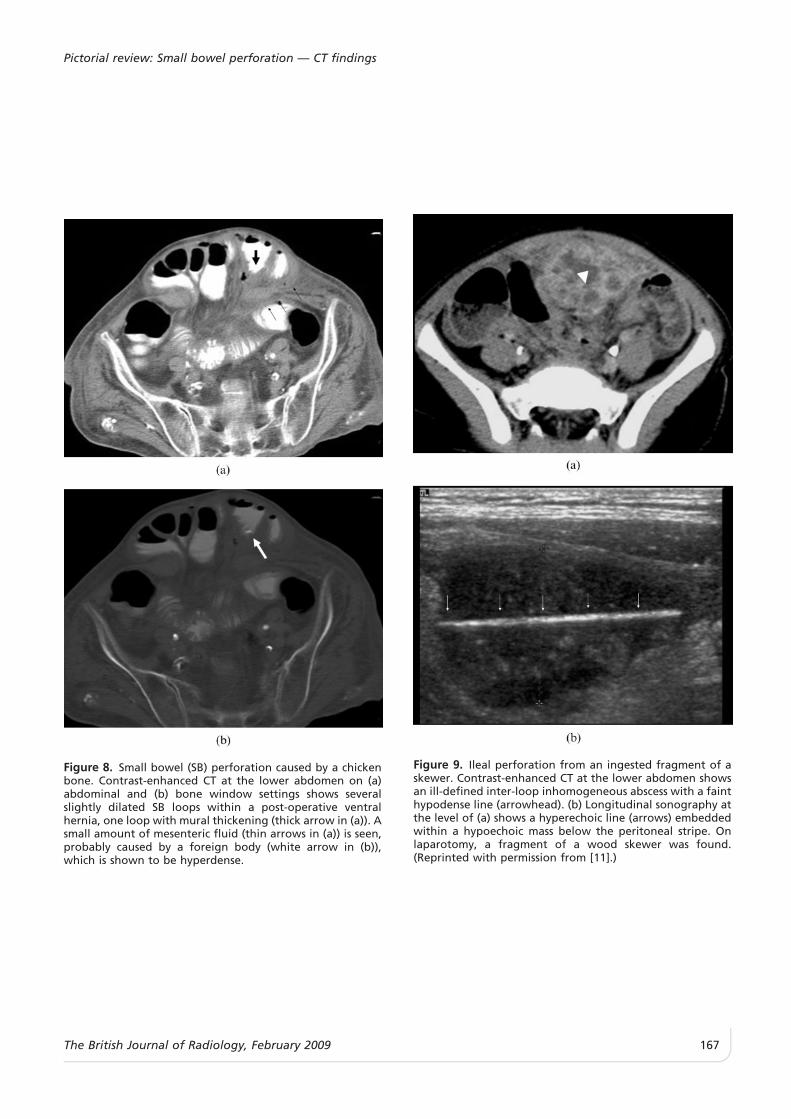
Figure 8. Small bowel (SB) perforation caused by a chickenbone. Contrast-enhanced CT at the lower abdomen on (a)abdominal and (b) bone window settings shows severalslightly dilated SB loops within a post-operative ventralhernia, one loop with mural thickening (thick arrow in (a)). Asmall amount of mesenteric fluid (thin arrows in (a)) is seen,probably caused by a foreign body (white arrow in (b)),which is shown to be hyperdense.
Figure 9. Ileal perforation from an ingested fragment of askewer. Contrast-enhanced CT at the lower abdomen showsan ill-defined inter-loop inhomogeneous abscess with a fainthypodense line (arrowhead). (b) Longitudinal sonography atthe level of (a) shows a hyperechoic line (arrows) embeddedwithin a hypoechoic mass below the peritoneal stripe. Onlaparotomy, a fragment of a wood skewer was found.(Reprinted with permission from [11].)
Pictorial review: Small bowel perforation — CT findings
The British Journal of Radiology, February 2009 167
extraluminal oral contrast, indicating a leak, in thepresence of an intact anastomotic site suggests diagnosisof accidental bowel injury (Figure 10).
Endoscopic injuryPerforation of the duodenum may occur during
endoscopic procedures such as endoscopic ultrasoundand endoscopic retrograde cholangiopancreatography.Duodenal perforation may be retroperitoneal or, rarely,intraperitoneal, with rapid development of peritonitisand sepsis.
In retroperitoneal perforation (either ductal or duode-nal), air within the anterior pararenal space is demon-strated (Figure 11a), sometimes associated withintraperitoneal and even mediastinal air. We recommendthe use of non-contrast CT to verify any extraluminalcontrast originating from the endoscopic procedure.
Whenever a retroperitoneal perforation is detected,administration of oral contrast is indicated, as its leakageis diagnostic of a duodenal perforation (Figure 11b) [6].
Crohn’s disease and perforation
The usual ileal-perforating complications of Crohn’sdisease (CD) are often sealed off because of inter-loopadhesions, leading to phlegmon and abscess formationwith localized peritonitis. Free perforation, althoughrare, is a life-threatening complication reported in up to3% of cases [14, 15]. SB perforation may occur in a patientwith known CD, or may rarely be the first presentation ofpreviously unknown inflammatory bowel disease. CThelps to detect both the perforation and the unsuspectedCD as its cause, often presenting with typical findings ofactive CD (Figures 1 and 12) [14].
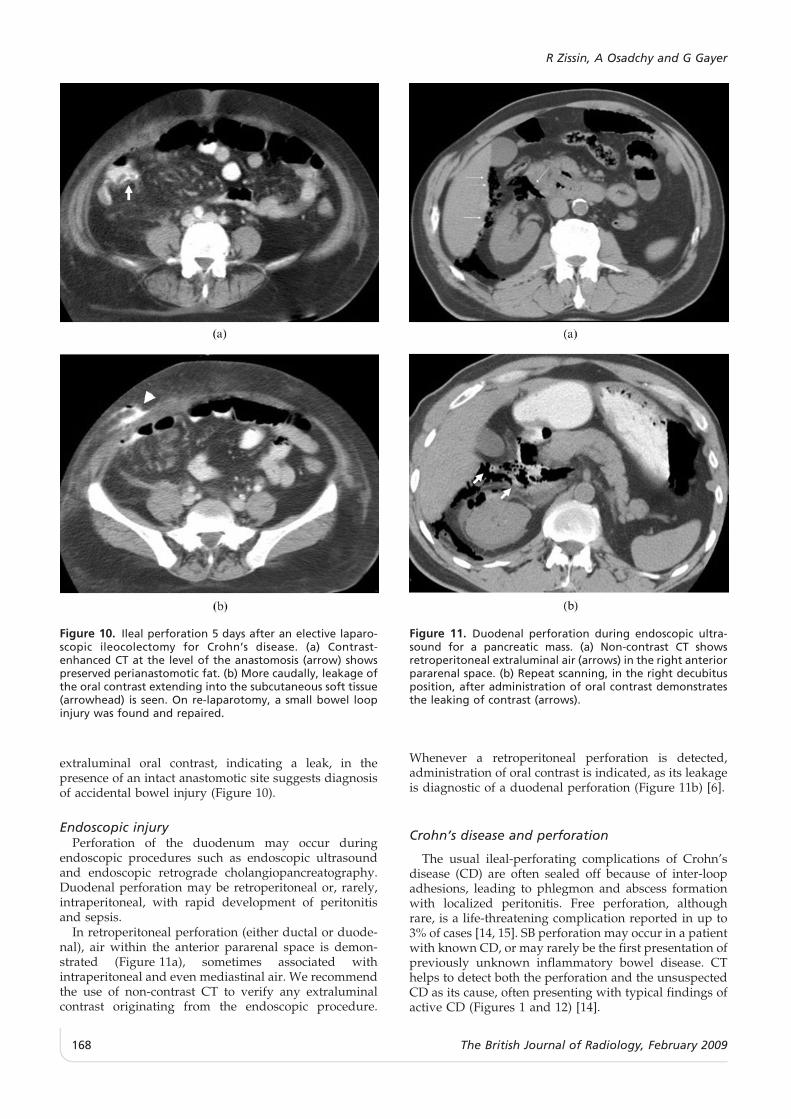
Figure 10. Ileal perforation 5 days after an elective laparo-scopic ileocolectomy for Crohn’s disease. (a) Contrast-enhanced CT at the level of the anastomosis (arrow) showspreserved perianastomotic fat. (b) More caudally, leakage ofthe oral contrast extending into the subcutaneous soft tissue(arrowhead) is seen. On re-laparotomy, a small bowel loopinjury was found and repaired.
Figure 11. Duodenal perforation during endoscopic ultra-sound for a pancreatic mass. (a) Non-contrast CT showsretroperitoneal extraluminal air (arrows) in the right anteriorpararenal space. (b) Repeat scanning, in the right decubitusposition, after administration of oral contrast demonstratesthe leaking of contrast (arrows).
R Zissin, A Osadchy and G Gayer
168 The British Journal of Radiology, February 2009
SB ischaemia and perforation
The two most common aetiologies that cause vascularimpairment of the SB wall leading to perforationare direct vascular occlusion (Figure 13) and strangu-lated SB obstruction (Figures 14 and 15) [16, 17]. Variousvasculitides, characterized by inflammation and necrosisof small systemic blood vessels, including the visceralvessels of the GIT, have been reported rarely as a causeof ischaemic intestinal perforation [16].
Prompt diagnosis and treatment is required for astrangulated bowel. The CT findings suggestive ofstrangulation include intestinal wall thickening, muralhypoperfusion, blurring of the mesenteric vessels withlocalized mesenteric fluid, and free peritoneal fluid.More specific findings of bowel infarction are lack ofbowel wall enhancement, pneumatosis intestinalis, gas inthe portal vein or pneumoperitoneum (Figures 14 and15) [16–18].
SB neoplasm and perforation
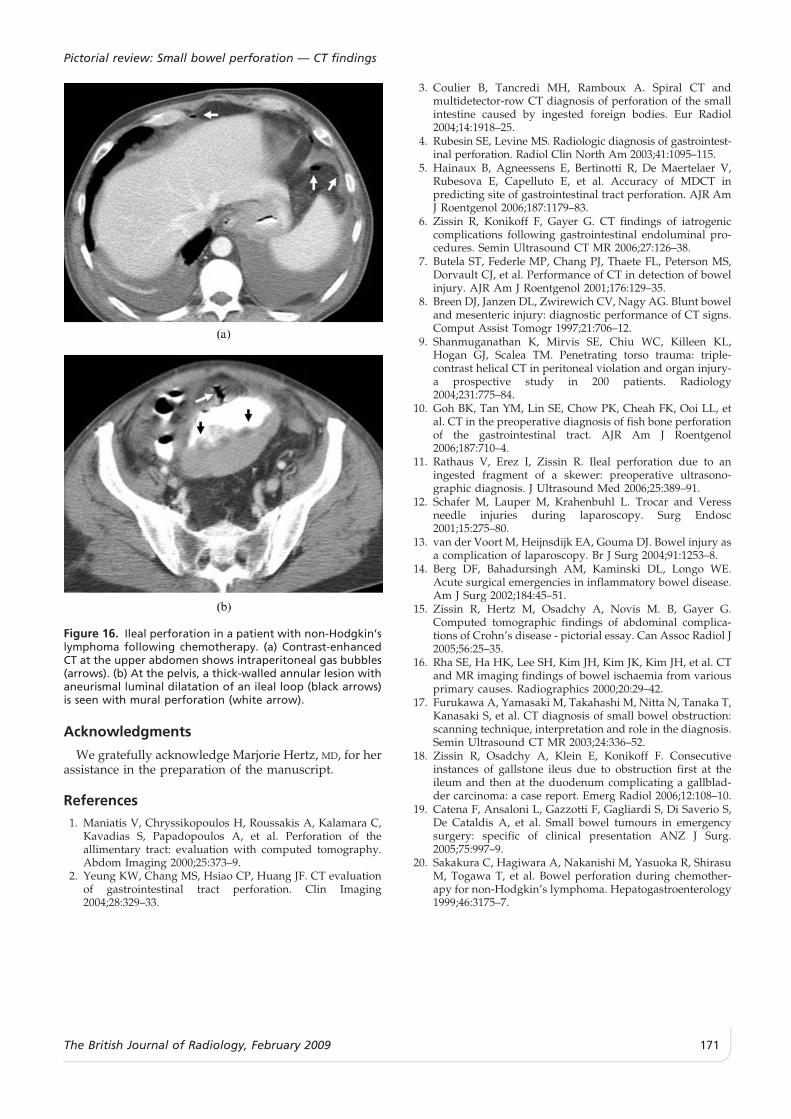
Primary or metastatic SB tumours are uncommon,and have non-specific clinical manifestations. Rarely,perforation of a SB neoplasm occurs, presenting with anacute abdomen [4, 19]. Perforation is most often relatedto SB lymphoma, especially in patients with primarymalignant lymphoma receiving chemotherapy andsteroids (Figure 16); it can also occur in malignantstromal tumours of the SB [20]. On CT, both theperforation and the cavitary tumour can be seen(Figure 16).
Conclusions
Familiarity with the specific CT features of SBperforation, i.e. the presence of extraluminal air or oralcontrast in an intact abdomen coupled with additionalCT findings, and the clinical setting should lead to arapid and accurate diagnosis.
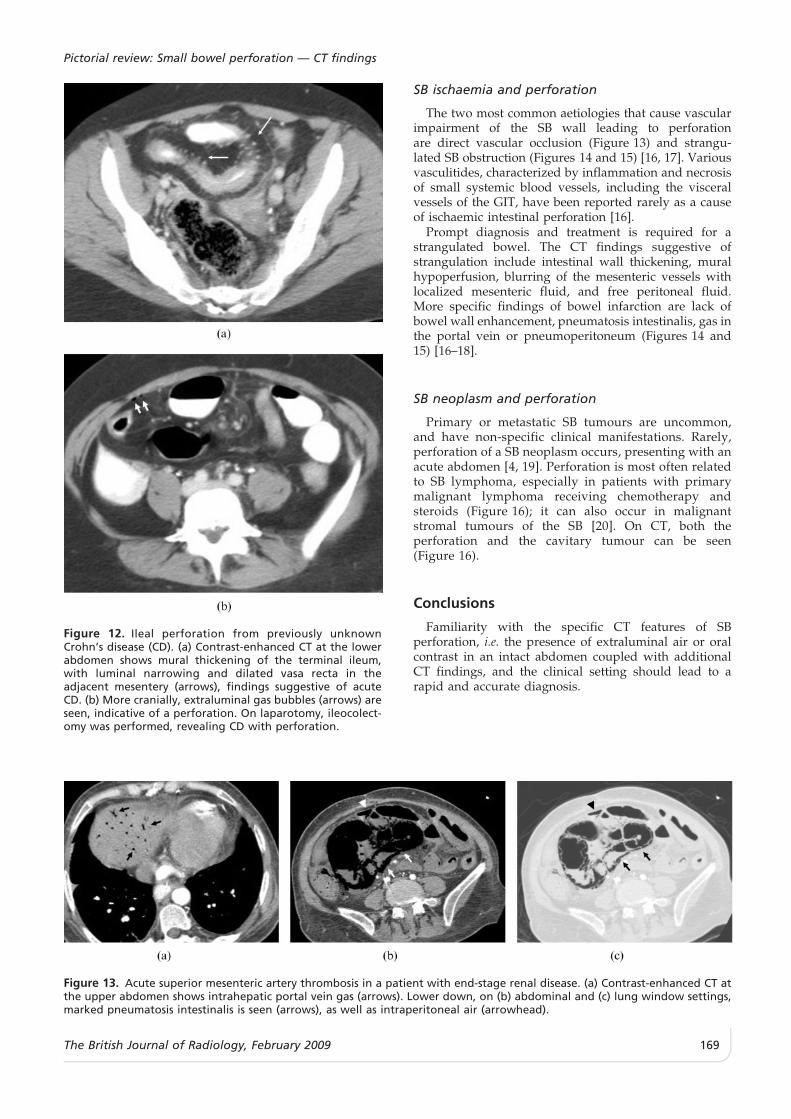
Figure 12. Ileal perforation from previously unknownCrohn’s disease (CD). (a) Contrast-enhanced CT at the lowerabdomen shows mural thickening of the terminal ileum,with luminal narrowing and dilated vasa recta in theadjacent mesentery (arrows), findings suggestive of acuteCD. (b) More cranially, extraluminal gas bubbles (arrows) areseen, indicative of a perforation. On laparotomy, ileocolect-omy was performed, revealing CD with perforation.
Figure 13. Acute superior mesenteric artery thrombosis in a patient with end-stage renal disease. (a) Contrast-enhanced CT atthe upper abdomen shows intrahepatic portal vein gas (arrows). Lower down, on (b) abdominal and (c) lung window settings,marked pneumatosis intestinalis is seen (arrows), as well as intraperitoneal air (arrowhead).
Pictorial review: Small bowel perforation — CT findings
The British Journal of Radiology, February 2009 169
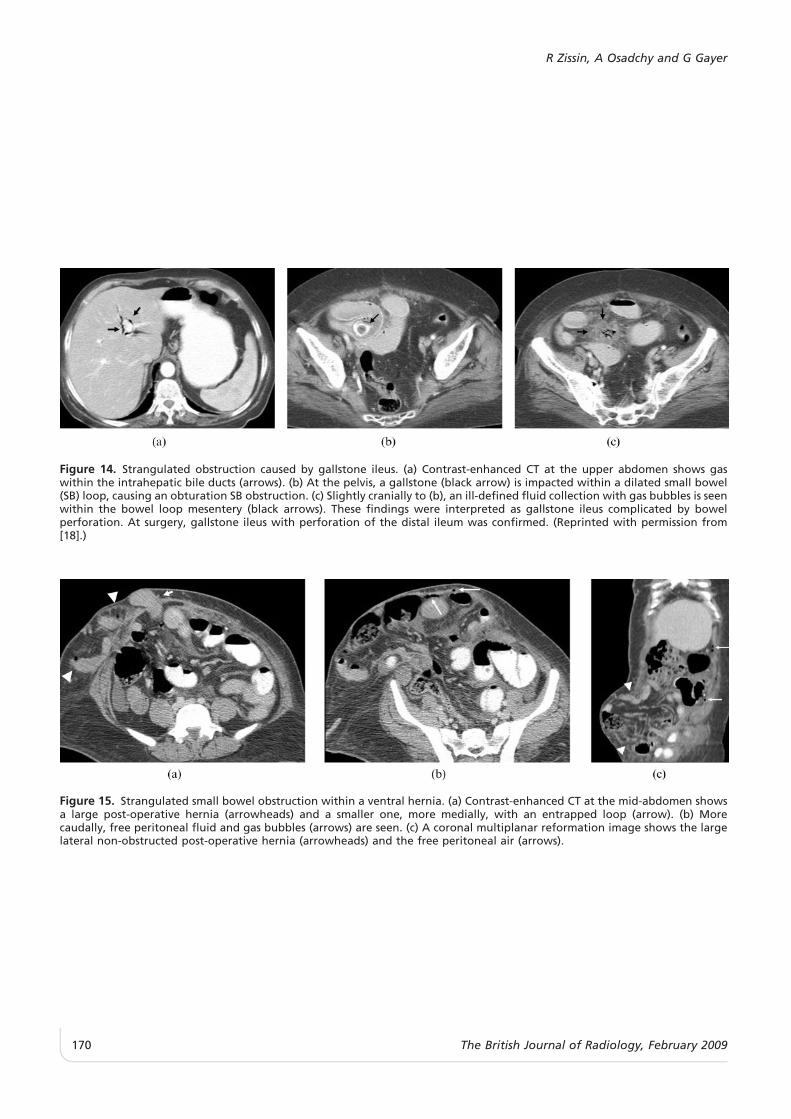
Figure 14. Strangulated obstruction caused by gallstone ileus. (a) Contrast-enhanced CT at the upper abdomen shows gaswithin the intrahepatic bile ducts (arrows). (b) At the pelvis, a gallstone (black arrow) is impacted within a dilated small bowel(SB) loop, causing an obturation SB obstruction. (c) Slightly cranially to (b), an ill-defined fluid collection with gas bubbles is seenwithin the bowel loop mesentery (black arrows). These findings were interpreted as gallstone ileus complicated by bowelperforation. At surgery, gallstone ileus with perforation of the distal ileum was confirmed. (Reprinted with permission from[18].)
Figure 15. Strangulated small bowel obstruction within a ventral hernia. (a) Contrast-enhanced CT at the mid-abdomen showsa large post-operative hernia (arrowheads) and a smaller one, more medially, with an entrapped loop (arrow). (b) Morecaudally, free peritoneal fluid and gas bubbles (arrows) are seen. (c) A coronal multiplanar reformation image shows the largelateral non-obstructed post-operative hernia (arrowheads) and the free peritoneal air (arrows).
R Zissin, A Osadchy and G Gayer
170 The British Journal of Radiology, February 2009
Acknowledgments
We gratefully acknowledge Marjorie Hertz, MD, for herassistance in the preparation of the manuscript.
References
1. Maniatis V, Chryssikopoulos H, Roussakis A, Kalamara C,Kavadias S, Papadopoulos A, et al. Perforation of theallimentary tract: evaluation with computed tomography.Abdom Imaging 2000;25:373–9.
2. Yeung KW, Chang MS, Hsiao CP, Huang JF. CT evaluationof gastrointestinal tract perforation. Clin Imaging2004;28:329–33.
3. Coulier B, Tancredi MH, Ramboux A. Spiral CT andmultidetector-row CT diagnosis of perforation of the smallintestine caused by ingested foreign bodies. Eur Radiol2004;14:1918–25.
4. Rubesin SE, Levine MS. Radiologic diagnosis of gastrointest-inal perforation. Radiol Clin North Am 2003;41:1095–115.
5. Hainaux B, Agneessens E, Bertinotti R, De Maertelaer V,Rubesova E, Capelluto E, et al. Accuracy of MDCT inpredicting site of gastrointestinal tract perforation. AJR AmJ Roentgenol 2006;187:1179–83.
6. Zissin R, Konikoff F, Gayer G. CT findings of iatrogeniccomplications following gastrointestinal endoluminal pro-cedures. Semin Ultrasound CT MR 2006;27:126–38.
7. Butela ST, Federle MP, Chang PJ, Thaete FL, Peterson MS,Dorvault CJ, et al. Performance of CT in detection of bowelinjury. AJR Am J Roentgenol 2001;176:129–35.
8. Breen DJ, Janzen DL, Zwirewich CV, Nagy AG. Blunt boweland mesenteric injury: diagnostic performance of CT signs.Comput Assist Tomogr 1997;21:706–12.
9. Shanmuganathan K, Mirvis SE, Chiu WC, Killeen KL,Hogan GJ, Scalea TM. Penetrating torso trauma: triple-contrast helical CT in peritoneal violation and organ injury-a prospective study in 200 patients. Radiology2004;231:775–84.
10. Goh BK, Tan YM, Lin SE, Chow PK, Cheah FK, Ooi LL, etal. CT in the preoperative diagnosis of fish bone perforationof the gastrointestinal tract. AJR Am J Roentgenol2006;187:710–4.
11. Rathaus V, Erez I, Zissin R. Ileal perforation due to aningested fragment of a skewer: preoperative ultrasono-graphic diagnosis. J Ultrasound Med 2006;25:389–91.
12. Schafer M, Lauper M, Krahenbuhl L. Trocar and Veressneedle injuries during laparoscopy. Surg Endosc2001;15:275–80.
13. van der Voort M, Heijnsdijk EA, Gouma DJ. Bowel injury asa complication of laparoscopy. Br J Surg 2004;91:1253–8.
14. Berg DF, Bahadursingh AM, Kaminski DL, Longo WE.Acute surgical emergencies in inflammatory bowel disease.Am J Surg 2002;184:45–51.
15. Zissin R, Hertz M, Osadchy A, Novis M. B, Gayer G.Computed tomographic findings of abdominal complica-tions of Crohn’s disease - pictorial essay. Can Assoc Radiol J2005;56:25–35.
16. Rha SE, Ha HK, Lee SH, Kim JH, Kim JK, Kim JH, et al. CTand MR imaging findings of bowel ischaemia from variousprimary causes. Radiographics 2000;20:29–42.
17. Furukawa A, Yamasaki M, Takahashi M, Nitta N, Tanaka T,Kanasaki S, et al. CT diagnosis of small bowel obstruction:scanning technique, interpretation and role in the diagnosis.Semin Ultrasound CT MR 2003;24:336–52.
18. Zissin R, Osadchy A, Klein E, Konikoff F. Consecutiveinstances of gallstone ileus due to obstruction first at theileum and then at the duodenum complicating a gallblad-der carcinoma: a case report. Emerg Radiol 2006;12:108–10.
19. Catena F, Ansaloni L, Gazzotti F, Gagliardi S, Di Saverio S,De Cataldis A, et al. Small bowel tumours in emergencysurgery: specific of clinical presentation ANZ J Surg.2005;75:997–9.
20. Sakakura C, Hagiwara A, Nakanishi M, Yasuoka R, ShirasuM, Togawa T, et al. Bowel perforation during chemother-apy for non-Hodgkin’s lymphoma. Hepatogastroenterology1999;46:3175–7.
Figure 16. Ileal perforation in a patient with non-Hodgkin’slymphoma following chemotherapy. (a) Contrast-enhancedCT at the upper abdomen shows intraperitoneal gas bubbles(arrows). (b) At the pelvis, a thick-walled annular lesion withaneurismal luminal dilatation of an ileal loop (black arrows)is seen with mural perforation (white arrow).
Pictorial review: Small bowel perforation — CT findings
The British Journal of Radiology, February 2009 171











![Intra-Abdominal and Abdominal Wall Desmoid Fibromatosis · intra-abdominal and involving the small bowel mesentery [2]. TREATMENT Surgery Margin-negative resection has historically](https://static.fdocuments.net/doc/165x107/5e5a290071d21b380f5b7e74/intra-abdominal-and-abdominal-wall-desmoid-fibromatosis-intra-abdominal-and-involving.jpg)





