ABDOMINAL AND PELVIC TRAUMA - … 1 ABDOMINAL AND PELVIC TRAUMA Salwa Malik ST6 Emergency Medicine...
14
23/11/2016 1 ABDOMINAL AND PELVIC TRAUMA Salwa Malik ST6 Emergency Medicine Objectives • Anatomy of the Abdomen • Mechanisms of Abdominal injury • Examination of the Abdomen and Pelvis • Adjuncts used in assessment • When to do a laparotomy • Pelvic fractures and management
Transcript of ABDOMINAL AND PELVIC TRAUMA - … 1 ABDOMINAL AND PELVIC TRAUMA Salwa Malik ST6 Emergency Medicine...

23/11/2016
1
ABDOMINAL AND
PELVIC TRAUMASalwa Malik
ST6 Emergency Medicine
Objectives
• Anatomy of the Abdomen
• Mechanisms of Abdominal injury
• Examination of the Abdomen and Pelvis
• Adjuncts used in assessment
• When to do a laparotomy
• Pelvic fractures and management

23/11/2016
2
Important points
• Unrecognised abdominal and pelvic injury continues to be
a cause of preventable death after truncal trauma.
• Significant blood loss can be present in the abdominal
cavity without any dramatic change in appearance or
dimensions and without any signs of peritoneal irritation
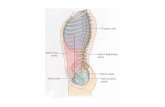
Anatomy of the Abdomen

23/11/2016
3
Retroperitoneal Anatomy:
Aorta, IVC, most of duodenum, pancreas, KUB, asc and
desc colons, rectum, female reproductive organs
Mechanisms of Injury
• Blunt
• Penetrating
• Explosion

23/11/2016
4
Types of Blunt trauma
• Direct blow
• E.g. intrusion of car door
• Compression and crushing
• Deform solid organs -> rupture
• Shearing
• Form of crushing
• Safety devices
• Deceleration injuries – movement of fixed and nonfixed parts of
body e.g. liver and spleen
• Airbag deployment = can still have abdominal injury!
Blunt trauma
• Spleen (40-55%)
• Liver (35-45%)
• Small bowel (5-10%)
• 15% incidence of retroperitoneal haematoma in patients who undergo laparotomy for blunt trauma

23/11/2016
5
Penetrating Trauma
• Stab wounds
• Low kinetic energy
• Liver, small bowel, diaphragm, colon
• Low-velocity v high-velocity gunshot wounds
• LV -> laceration and cutting; HV -> more damage
• Based on trajectory, cavitation effect, bullet fragmentation
• Small bowel, colon, liver, abdominal vasculature
• Explosions
• Combined blunt and penetrating
• Blast injuries – injuries obtained depends on distance/closed area
Assessment – history…be nosey!
• RTC
• Speed of vehicle
• Type of vehicles involved
• Type of collision
• Intrusion
• Safety devices – wearing seatbelts, airbags deployed
• Self-extricated?
• Patient’s position
• Status of passengers
• Penetrating trauma
• Time of injury
• Type of weapon
• Distance from patient (more distance, less damage)
• Number of wounds
• Amount of external bleeding at scene

23/11/2016
6
Assessment - Examination
• Full exposure
• Inspection
• Palpation
• Percussion
• Auscultation
• Don’t forget perineum!
• 50% incidence of significant transabdominal injuries
Assessment of Pelvis
• Findings suggestive of pelvic fractures
• Evidence of ruptured urethra:
• High riding prostate
• Scrotal haematoma
• Blood at urethral meatus
• Limb length discrepancy
• Rotational deformity of leg
PELVIS MANIPULATION CAN BE DETRIMENTAL – DO
NOT TOUCH!
23/11/2016
7
Adjuncts to Examination
• Gastric tube• Decompress stomach
• Remove gastric contents
• Reduce aspiration
• Blood indicates injury to GI tract
• DO NOT DO NASALLY IN BASILAR SKULL FRACTURES/FACIAL INJURIES – can be done ORALLY ONLY in these cases
• Urinary catheter• Relieve retention
• Decompression
• Assessing C
• Gross haematuria -> trauma to GU tract -> retrograde urethrogram to confirm intact urethra before catheterising. Otherwise SP catheter.
Adjuncts to Examination
• FAST Scan
• Hepatorenal
• Splenorenal
• Pericardial sac
• Pelvis
• XRAYs
• Chest and pelvis
• CT
• ONLY FOR HAEMODYNAMICALLY STABLE PATIENTS and NO
IMMEDIATE INDICATION FOR EMERGENCY LAPAROTOMY

23/11/2016
8
What does “Snow White and the 7 Dwarfs” really represent?
FAST v CT
FAST Scan
• Early diagnosis• Non invasive• Rapid• Repeatable• 86-97% sensitive• Portable• Operator dependent• Misses diaphragm, bowel,
pancreatic injuries• Negative scan does not
exclude pathology• For unstable blunt trauma
CT Scan
• Most specific for injury
• 92-98% specific
• Non-invasive
• Cost and time
• Contrast
• Misses diaphragm, bowel and some pancreas injuries
• Needs transportation
• Stable blunt trauma and penetrating back/flank trauma

23/11/2016
9
Who needs a laParotomy?
• Perforation
• Peritonism
• Protuding contents
• Penetrating wounds
• Positive FAST/CT
• …& haem unstable patients with blunt abdominal
injury
-> immediate exploratory laparotomy
Specific Injuries
• Diaphragm
• Left hemidiaphragm more commonly injured
• Look for elevation/blurring/NG tube in chest on CXR
• Confirm with laparotomy
• Duodenal
• Unrestrained drivers, bicycle handlebars
• Bloody gastric aspirate, retroperitoneal air
• Double contract CT
• Pancreatic
• Early normal amylase does not exclude
• Direct epigastric blow
• Double and triple contrast CT

23/11/2016
10
Specific Injuries
• Genitourinary
• Direct blows to back, flank -> ecchymoses, haematomas
• Gross haematuria
• Abdominal CT with contrast
• Anterior pelvic fractures cause urethral injuries
• Posterior - multisystem trauma
• Anterior - straddle impact
• 95% treated non-operatively
• Hollow viscus (intestines)
• Blunt injuries, deceleration
• Transverse linear ecchymoses (seatbelt sign) or lumbar “Chance”
fracture
• Solid organ
Pelvic trauma
• 1) AP compression (Open Book)
• E.g. Fall from height, ped v car, direct crush to pelvis
• Disruption of symphysis pubis -> haemorrhage
• 2) Lateral compression
• E.g. RTC
• Internal rotation of involved hemipelvis
• Not life-threatening haemorrhage
• 3) Vertical shear
• E.g. Fall
• High energy force
• Majorly unstable and haemorrhage
• 4) Complex (combination)

23/11/2016
11
Open Book (AP) Fracture

23/11/2016
12
Lateral Compression Fracture
Vertical Shear Fracture

23/11/2016
13
Complex pelvic fracture
Management of Pelvic fractures
• ABC…Haemorrhage control!
• Binders/splints
• Moving away from these
• Angiographic embolisation
• But if intraperitoneal blood -> laparotomy first
• Haemorrhage control fixation device

23/11/2016
14
Questions?
Conclusion
• Be nosey!
• Be thorough!
• Don’t touch pelvis!