
ABCs of CVA Meds Final 2016 - Baptist Health of CVA Meds...HMG-CoA-Reductase (Statins) Blood ... SBP
31
October 20, 2016 ABCs of CVA Meds HyeJin Son, PharmD, BCPS
Transcript of ABCs of CVA Meds Final 2016 - Baptist Health of CVA Meds...HMG-CoA-Reductase (Statins) Blood ... SBP
October20,2016
ABCs of CVA Meds HyeJinSon,PharmD,BCPS

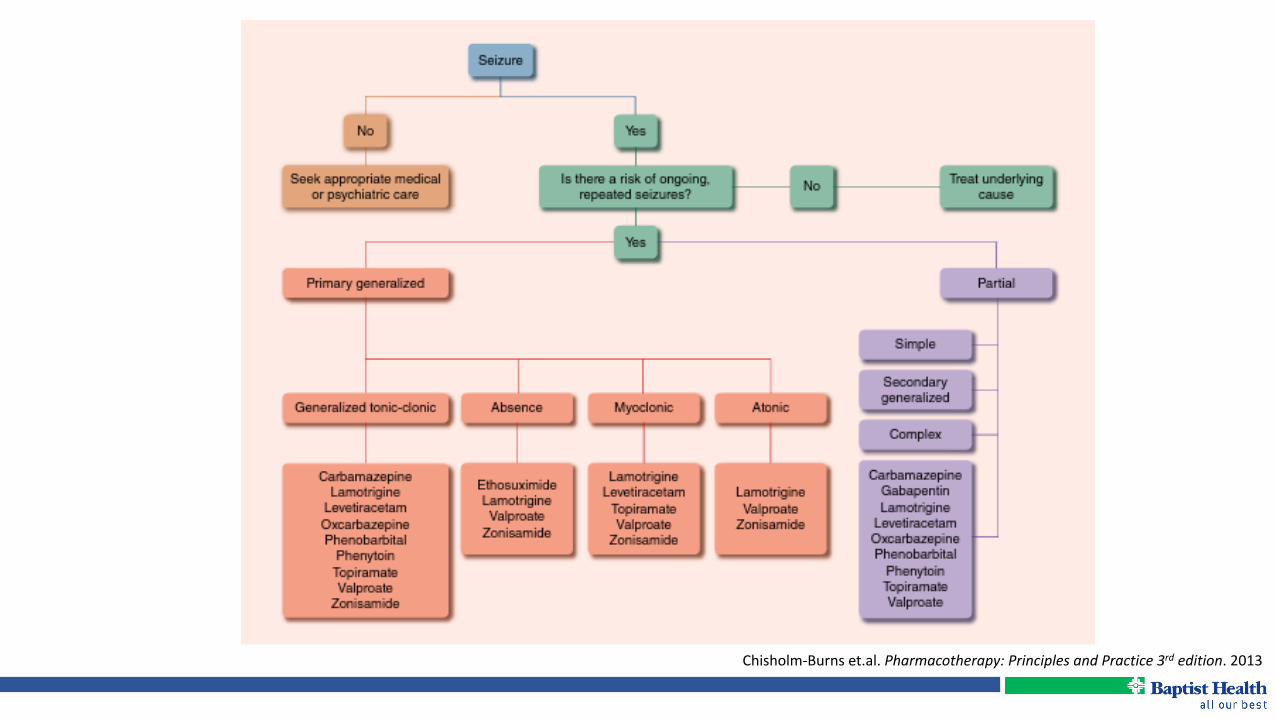
Chisholm-Burnset.al.Pharmacotherapy:PrinciplesandPractice3rdedition.2013

OriginofStroke
Chisholm-Burnset.al.Pharmacotherapy:PrinciplesandPractice3rdedition.2013

GoldenHourofStroke
• “Time is brain” • Stroke scales • Diagnostic studies
• Neuroimaging • Glucose • PT/INR • BMP/CBC • ECG/Cardiac biomarkers • O2 saturation
• Differential diagnosis • Hypoglycemia • Seizures • Intoxication • Complicated migraine • CNS tumor • CNS infection
Jauchetal.EarlyManagementofAcuteIschemicStroke.Stroke.2013;44:870-947

Chisholm-Burnset.al.Pharmacotherapy:PrinciplesandPractice3rdedition.2013

Initial Care Acute Intervention
Secondary Prevention
Respiratory Support
TPA BP Lowering
Aspirin Antiplatelets
Hemodynamic Support Interventional
Radiology
Anticoagulants for Afib • Warfarin• Novel Anticoagulants
HMG-CoA-Reductase (Statins)

BloodPressureinAcuteIschemicStroke(AIS)

• Hypertension predominates AIS • Goal BP dependent on intervention • If TPA à BP < 180/105 for first 24 hours • If no TPA à SBP < 220 or DBP < 120
• Hypotension suggests alternative cause • Arrhythmia • Cardiac Ischemia • Aortic dissection • Shock/Sepsis
Jauchetal.EarlyManagementofAcuteIschemicStroke.Stroke.2013;44:870-947
BloodPressureinAcuteIschemicStroke(AIS)

AcuteHypertensionTreatment
Drug Mechanism Dose(IV) Onset Duration
Labetalol Alpha/BetaBlocker10-20mg2-8mg/mininfusion
2-5min 2-6hr
Nicardipine CalciumChannelBlocker 5-15mg/hrinfusion 5-10min 2-6hr
Hydralazine Arterialvasodilator 5-20mg 10min 1-4hr
Enalaprilat ACE-Inhibitor 0.625-1.25mgq6hr 15-30min 12-24hr
Nitroprusside Arterial/venousvasodilator 0.5-3mcg/kg/min Seconds 1-2min
Jauchetal.EarlyManagementofAcuteIschemicStroke.Stroke.2013;44:870-947

Long-termAntihypertensiveTherapy
• The most important intervention • When
• Reasonable after the first 24 hours • Whom
• Initiate for previously untreated patients • Resume for previously treated patients
• Secondary prevention • Goal: SBP <140 and DBP <90 • Lifestyle modification • Thiazide ± ACE Inhibitor Jauchetal.EarlyManagementofAcuteIschemicStroke.Stroke.2013;44:870-947
Kernanetal.StrokePreventioninPatientswithStrokeandTIA.Stroke.2014;45:2160-2236

JAMA2014;311(5):507-520

Antiplatelets
• Aspirin 325 mg x1, then 81-325 mg/day within 24-48 hours
• Do not initiate aspirin within 24 hours of tPA • Secondary Prevention of noncardioembolic stroke or TIA
• Aspirin 75-100 mg once daily • Clopidogrel 75 mg once daily • Aspirin/ER dipyridamole 25 mg/200 mg twice daily • Cilostazol 100 mg twice daily
Kernanetal.StrokePreventioninPatientswithStrokeandTIA.Stroke2014;45:2160-2236Lansbergetal.Antithromboticandthrombolytictherapyforischemicstroke.Chest2012;141:e601S-36S

AnticoagulantsforAtrialFibrillation(Afib)
• Use of CHA2DS2-VASc score • 0: recommend no antithrombotic therapy • 1: recommend antithrombotic therapy with oral anticoagulation or
antiplatelet therapy but preferably oral anticoagulation • ≥2: recommend oral anticoagulation with
• Warfarin • Dabigatrin • Rivaroxaban • Apixaban
Laneetal.Circulation.2012;126:860-865Kernanetal.StrokePreventioninPatientswithStrokeandTIA.Stroke2014;45:2160-2236
Januaryatel.2014AHA/ACC/HRSGuidelineforAtrialFibrillation.JAmCollCardiol.2014;64(21):2246-2280

Anticoagulants–StrokeRiskAssessmentTool
CHADS2 CHA2DS2-VASc
CHF–1point CHF–1point
Hypertension–1point Hypertension–1point
Age≥75year–1point Age≥75year–1point
Diabetes–1point Diabetes–1point
PriorStrokeorTIA–2points PriorStrokeorTIA–2points
Vasculardisease–1point
Age≥65year–1points
Sexcategory(female)–1point
Laneetal.Circulation.2012;126:860-865

Warfarin(Coumadin)
Dabigatran(Pradaxa)
Rivaroxaban(Xarelto) Apixaban(Eliquis)
Edoxaban(Savaysa)
Mechanism VitaminKAntagonist
DirectThrombinInhibitor DirectFactorXaInhibitor
DirectFactorXaInhibitor
DirectFactorXaInhibitor
Comparedtowarfarin
Canuseinpatientswithvalvularafib
Non-inferiorSimilarratesofhemorrhagebutlessICH,moreGIB.IncreasedMI
Non-inferiorSimilarriskofmajorbleedingbutlowerICHandfatalbleeding,moreGIB
SuperiorLessriskofbleedingandmortality
Non-inferiorLowerratesofbleeding
Trial SPAF RE-LY ROCKETAF ARISTOTLE EngageAF-TIMI48
DoseforAfib Variousdosesdaily
150mgtwicedaily 20mgdailywitheveningmeal
5mgtwicedaily 60mgdaily
Renaladjustment
No CrCl30-49:Ifconcomitantdronedaroneorketoconazole75mgtwicedailyCrCl15-30:75mgtwicedailyoravoidCrCl<15:Avoiduse
CrCl15-50ml/min:15mgdailyCrCl<15ml/min:Donotuse
Decreasedoseto2.5mgtwicedailyif≥2ofthefollowing:≥80yearsold;Weight≤60kg;SCr≥1.5
DonotuseifCrClis>95ml/minCrCl15-50ml/min:30mgdailyCrCl<15ml/min:Donotuse
Reversalagent VitaminK Idarucizumab(Praxbind) Indevelopment:Andexanetalfa(PRT064445)–PhaseIIItrialsAripazine(PER977)–PhaseIItrials
Hanleyelal.JThoracDis.2015Feb;7(2):165–171,Stacyetal.CardiolTher2016June;5(1):1-8

Relative risk reductions of various outcomes in patients with nonvalvular atrial fibrillation receiving various antithrombotic regimens as compared with warfarin or its derivatives
Antonio Culebras et al. Neurology 2014;82:716-724
Acenocoum = acenocoumarol ASA = acetylsalicylic acid CI = confidence interval

HemorrhagicStrokePearls
• No pharmacotherapy to directly treat bleeding • Pharmacotherapy is aimed at supportive care
• Anticoagulation reversal • FFP, PCC, etc • Blood pressure/cerebral perfusion pressure • Cerebral edema/Intracranial pressure
• Vasospasm management (Aneurysmal SAH)
Jauchetal.EarlyManagementofAcuteIschemicStroke.Stroke.2013;44:870-947Kernanetal.StrokePreventioninPatientswithStrokeandTIA.Stroke.2014;45:2160-2236

HemorrhagicStrokeBloodPressure
• SBP < 160 • MAP < 110 • CPP = MAP – ICP • CPP > 60 • Short acting medications
• Antihypertensives • Vasopressors
Jauchetal.EarlyManagementofAcuteIschemicStroke.Stroke.2013;44:870-947Kernanetal.StrokePreventioninPatientswithStrokeandTIA.Stroke.2014;45:2160-2236
Prevent hematoma expansion
Maintain cerebral perfusion

CholesterolManagement
• Continue statin during the acute period • Secondary prophylaxis
• Statin therapy with intensive lipid-lowering effects (SPARCL study) • Manage according to 2013 ACC/AHA cholesterol guidelines
Jauchetal.EarlyManagementofAcuteIschemicStroke.Stroke.2013;44:870-947Kernanetal.StrokePreventioninPatientswithStrokeandTIA.Stroke.2014;45:2160-2236
ASCVD = atherosclerotic cardiovascular disease ACC = American College of Cardiology AHA = American Heart Association

FourStatinBenefitGroups
Individuals: 1. Clinical ASCVD 2. Primary elevations of LDL-C > 190 mg/dL 3. Diabetes aged 40 to 75 yrs with LDL-C 70-189 mg/dL and without clinical ASCVD 4. Without clinical ASCVD or diabetes with LDL-C 70-189 mg/dL and estimated 10-yr ASCVD risk > 7.5%
http://my.americanheart.org/cvriskcalculator
Stone et al. Circulation 2013;00:000–000

Stone et al. Circulation 2013;00:000–000

Stone et al. Circulation 2013;00:000–000

Chisholm-Burnset.al.Pharmacotherapy:PrinciplesandPractice3rdedition.2013
• LDL-C reduction 25-62% • “Rule of 6” = Each doubling of daily dose produces an additional 6%
average reduction • Moderately effective at lowering triglycerides • Modestly raise HDL-C
StatinsEfficacy

• Constipation • Abdominal pain • Diarrhea • Dyspepsia • Nausea • LFT increase (< 2%) • Myopathy, including rhabdomyolysis (0- <0.5%)
StatinsAdverseEffects
Stone et al. Circulation 2013;00:000–000

Post-StrokeSeizures
• Post stroke seizure: <10% • Recurrence: rare to ~6%
• Early vs. late onset • Predictors: hemorrhagic transformation (HT), severity and
cortical location • No primary prophylaxis • Secondary prophylaxis if multiple early seizures or ICH or HT
• Short term/monotherapy with antiepileptic agent
Jauchetal.EarlyManagementofAcuteIschemicStroke.Stroke.2013;44:870-947Belezaetal.Neurologist.2012May;18(3):109-19.

Post-StrokeSeizures
• Recurrent seizures after stroke should be treated in a manner similar to other acute neurological conditions, and antiepileptic agents should be selected by specific patient characteristics.
Jauchetal.EarlyManagementofAcuteIschemicStroke.Stroke.2013;44:870-947
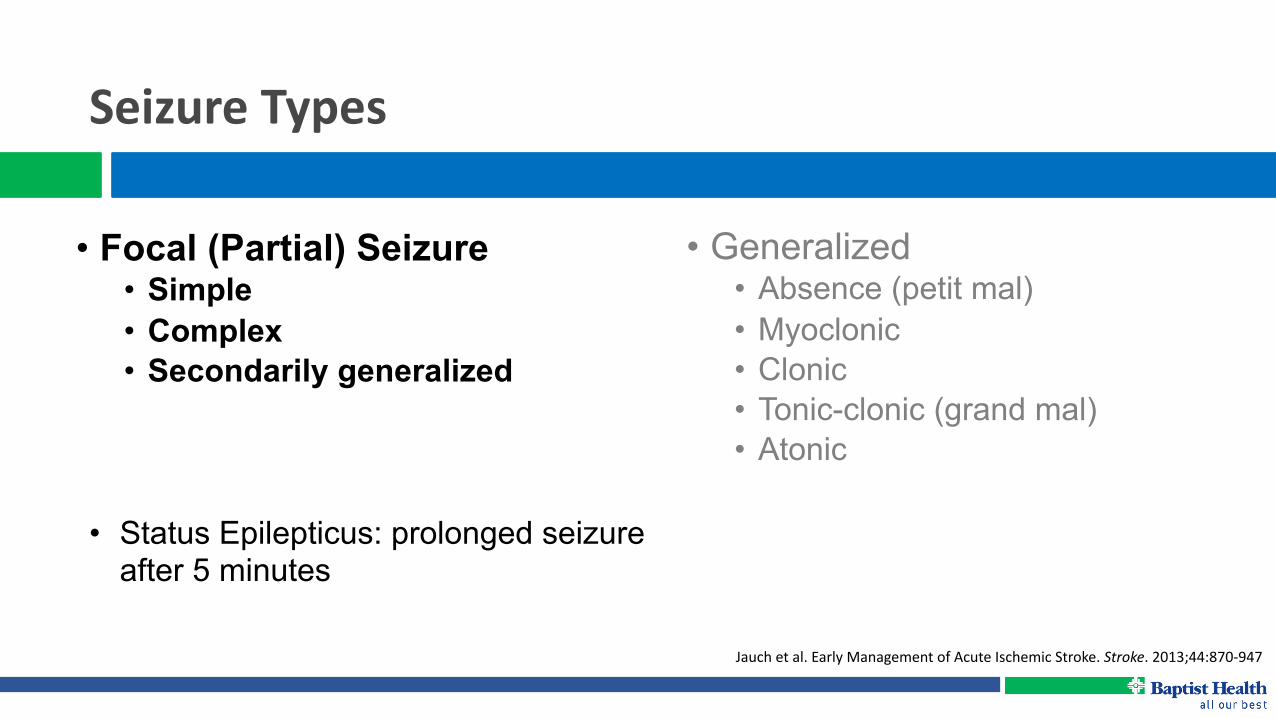
SeizureTypes
• Generalized • Absence (petit mal) • Myoclonic • Clonic • Tonic-clonic (grand mal) • Atonic
Jauchetal.EarlyManagementofAcuteIschemicStroke.Stroke.2013;44:870-947
• Focal (Partial) Seizure • Simple • Complex • Secondarily generalized
• Status Epilepticus: prolonged seizure after 5 minutes

StatusEpilepticusTreatment
NeurocritCare2012;17:3-23
• First-linetherapy(Benzodiazepinetherapypreferred)• Lorazepam0.1mg/kgintravenously(max4mg/dose)• Midazolam5–10mgintramuscularly
• Second-linetherapy• Valproate20–40mg/kgintravenously• (Fos)Phenytoin18–20mg/kgintravenously• Phenobarbital20mg/kgintravenously• Levetiracetam1–3gintravenously
Chisholm-Burnset.al.Pharmacotherapy:PrinciplesandPractice3rdedition.2013
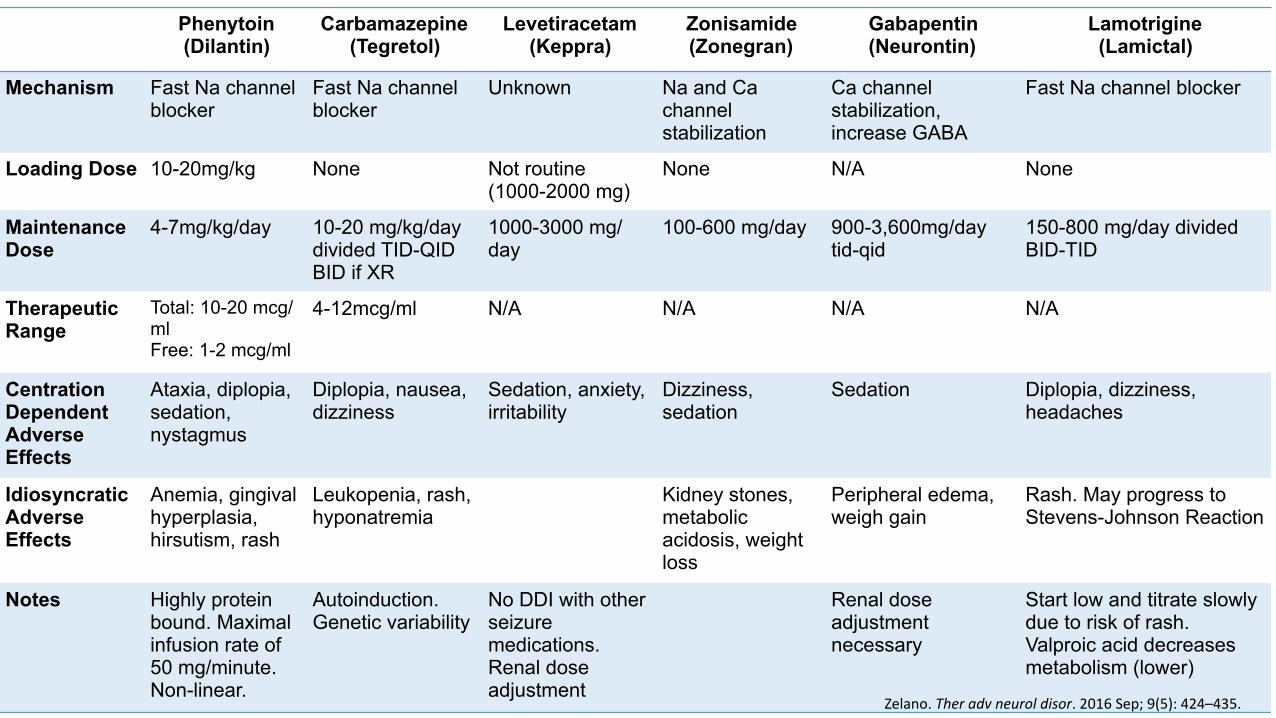
Phenytoin (Dilantin)
Carbamazepine (Tegretol)
Levetiracetam (Keppra)
Zonisamide (Zonegran)
Gabapentin (Neurontin)
Lamotrigine (Lamictal)
Mechanism Fast Na channel blocker
Fast Na channel blocker
Unknown Na and Ca channel stabilization
Ca channel stabilization, increase GABA
Fast Na channel blocker
Loading Dose 10-20mg/kg None Not routine (1000-2000 mg)
None N/A None
Maintenance Dose
4-7mg/kg/day 10-20 mg/kg/day divided TID-QID BID if XR
1000-3000 mg/day
100-600 mg/day 900-3,600mg/day tid-qid
150-800 mg/day divided BID-TID
Therapeutic Range
Total: 10-20 mcg/ml Free: 1-2 mcg/ml
4-12mcg/ml N/A N/A N/A N/A
Centration Dependent Adverse Effects
Ataxia, diplopia, sedation, nystagmus
Diplopia, nausea, dizziness
Sedation, anxiety, irritability
Dizziness, sedation
Sedation Diplopia, dizziness, headaches
Idiosyncratic Adverse Effects
Anemia, gingival hyperplasia, hirsutism, rash
Leukopenia, rash, hyponatremia
Kidney stones, metabolic acidosis, weight loss
Peripheral edema, weigh gain
Rash. May progress to Stevens-Johnson Reaction
Notes Highly protein bound. Maximal infusion rate of 50 mg/minute. Non-linear.
Autoinduction. Genetic variability
No DDI with other seizure medications. Renal dose adjustment
Renal dose adjustment necessary
Start low and titrate slowly due to risk of rash. Valproic acid decreases metabolism (lower)
Zelano.Theradvneuroldisor.2016Sep;9(5):424–435.

Thank you!
http://www.stroke.org/understand-stroke/recognizing-stroke/act-fast


















