Antenatal Consults: A guide for neonatologists and paediatricians
Upload
frederica-mortonCategory
view
214download
0
A Vaccination Primer
• One would think that the public trusts neonatologists, pediatricians, family practitioners and the CDC to know what is best for their children.
• One might think that trust would be built upon the tremendous historical perspective and successes of vaccination programs.
• One would be wrong….• The public believes it is Caveat Emptor when
it comes to vaccinations. What is going on?

What comes up when you typeWhat comes up when you type “Should I Vaccinate My “Should I Vaccinate My
Child?” Child?” into Google:into Google:

There are 13 diseases that the CDC issues recommendations for vaccination against: diptheria, tetanus, pertusis, polio, measles, mumps, rubella, varicella haeomophilus infleunza type b, hepatitis A & B, meningococemia, influenza, pneumoccocus and influenza virus. Children are inoculated against these diseases with nine different immunizations.
DTaP:
Polio Vaccine:
MMR / MMRV:
Hib:
Influenza:
Hepatitis A:
Hepatitis B:
Men C:
Pneumococcal Vaccine:
Varicella:
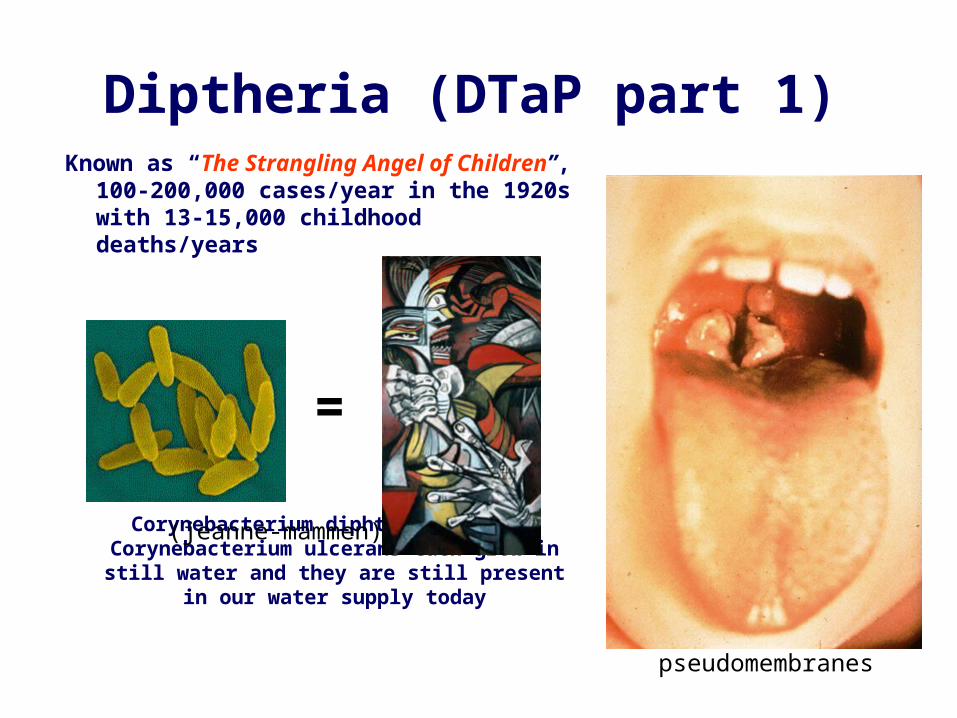
Diptheria (DTaP part 1) Known as “The Strangling Angel of
Children”, 100-200,000 cases/year in the 1920s with 13-15,000 childhood deaths/years
Corynebacterium diphtheriae and Corynebacterium ulcerans each grow in still water and they are still present in our water
supply today
pseudomembranes
=
(jeanne-mammen)

Tetanus (DTaP part 2) Tetanus is caused by the
toxin from clostridium tetaniInfants acquire “Lock Jaw” and
“Opisthotonos” from a soiled / infected umbilicus. Adults acquire infections
most commonly from puncture wounds. Patients are fully aware during the
height of their symptoms (often dying from a rigid chest versus starvation).
Most sadly of all, the disease does not confer immunity.
“Opisthotonus” by SirCharles Bell, 1809.

Pertussis (DTaP part 3)
paroxysmal cough, whooping, vomiting,
cyanosis, and irregular breathing

Polio Vaccine (part 1)Franklin Roosevelt contracts polio at age 39 in 1921, he (along with Eddie Cantor) go on to found the March of Dimes - the organization credited for polio vaccine funding. Congress puts him on the dime in memorial.
The King gets the Salk Vaccine

Polio Vaccine (part 2)1 in 520,000 children acquires vaccine-related
polio after receiving their 1st OPV dose.
The overall incidence of vaccine-related polio is 1 per 2.5-3 million cases (i.e. almost all are 1st dose related). For this reason, The CDC and WHO recommend that the 1st two doses be IPV and doses 3 & 4 be OPV to provide optimal immunity (however, this still does not completely eliminate the risk of paralysis in immunocompromized recipients or herd infectants – thus OPV has become a source of public mistrust). The Red Book now recommends that all 4 doses be IPV.
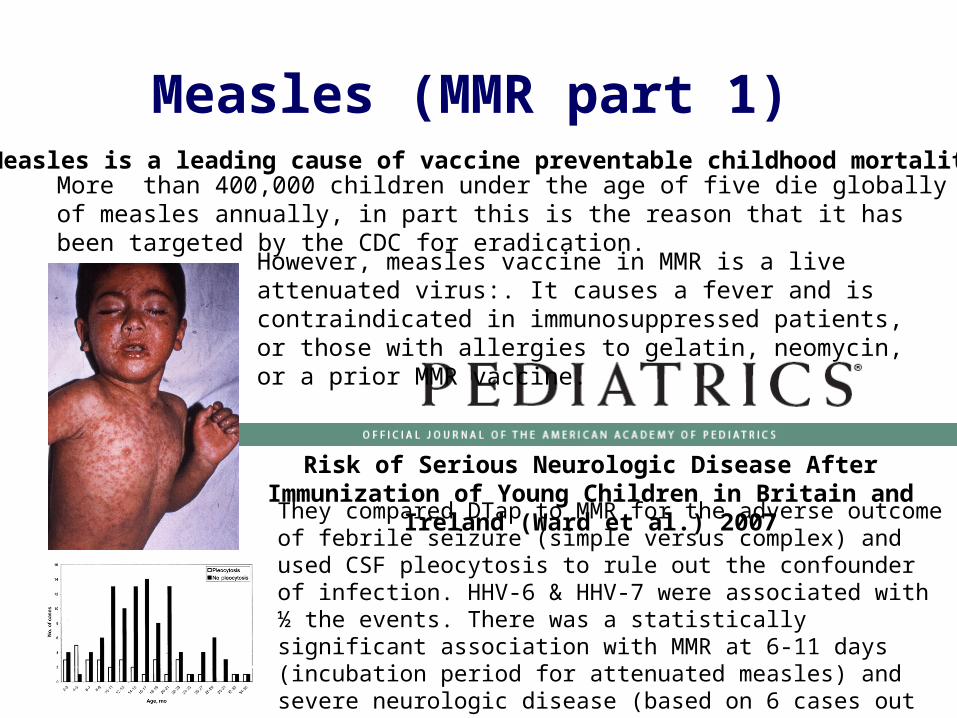
Measles (MMR part 1) Measles is a leading cause of vaccine preventable childhood mortality
More than 400,000 children under the age of five die globally of measles annually, in part this is the reason that it has been targeted by the CDC for eradication.
However, measles vaccine in MMR is a live attenuated virus:. It causes a fever and is contraindicated in immunosuppressed patients, or those with allergies to gelatin, neomycin, or a prior MMR vaccine.
Risk of Serious Neurologic Disease After Immunization of Young Children in Britain and Ireland (Ward et al.) 2007
They compared DTap to MMR for the adverse outcome of febrile seizure (simple versus complex) and used CSF pleocytosis to rule out the confounder of infection. HHV-6 & HHV-7 were associated with ½ the events. There was a statistically significant association with MMR at 6-11 days (incubation period for attenuated measles) and severe neurologic disease (based on 6 cases out of 117).

Mumps (MMR part 2) Mumps vaccine in MMR is a live attenuated virus derived from Jeryl Lynn Hillman (the then 5 year old Daughter of Dr Maurice Hillman). It is one of most efficacious vaccines ever created. One dose is sufficient to prevent mumps outbreaks (although two MMRs are given because of measles).
One picture is worth a thousand words: Necrotising epidymo-orchitis (from mumps). Need I say more about the importance of
mumps vaccination?
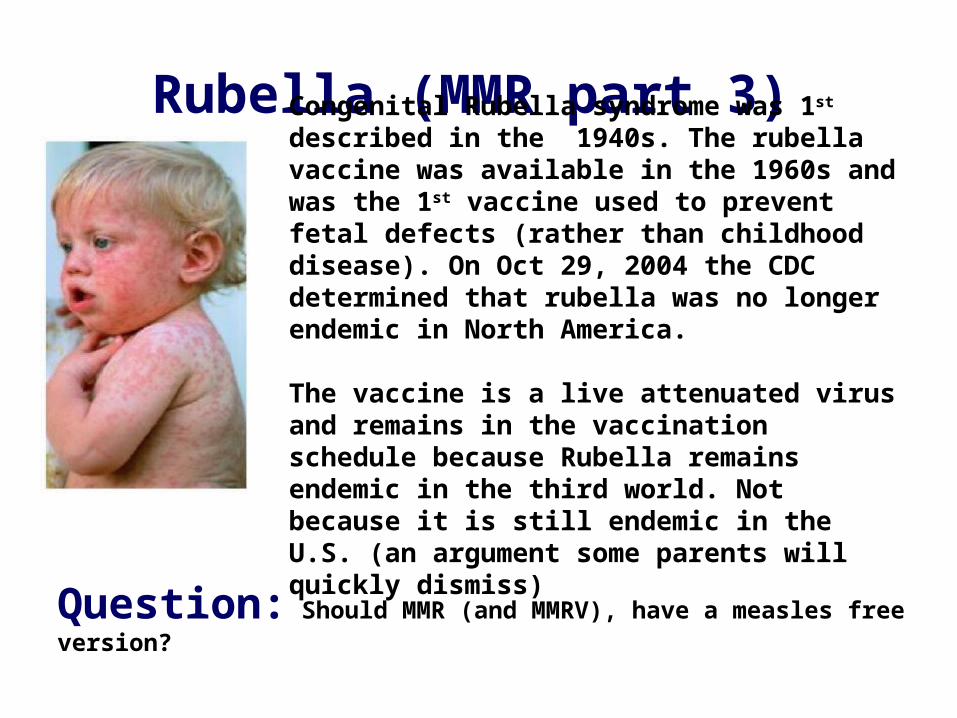
Rubella (MMR part 3) Congenital Rubella syndrome was 1st described in the 1940s. The rubella vaccine was available in the 1960s and was the 1st vaccine used to prevent fetal defects (rather than childhood disease). On Oct 29, 2004 the CDC determined that rubella was no longer endemic in North America.
The vaccine is a live attenuated virus and remains in the vaccination schedule because Rubella remains endemic in the third world. Not because it is still endemic in the U.S. (an argument some parents will quickly dismiss)
Question: Should MMR (and MMRV), have a measles free version?

Haemophilus Influenza Type B
Steeple sign
The first Hib vaccine was licensed in 1985. Scientists later reformulated the vaccine so that it would be effective in children under 18 months of age, and the FDA licensed this improved version in 1987. The currently used Hib vaccine protects infants as young as six weeks old.
Prior to universal Hib immunization, Hib was the most common cause of bacterial meningitis in infants and preschool-age children, and caused approximately 20,000 cases of invasive disease annually (in the U.S). Epiglottitis was the version of the disease that most physicians feared most (although the public has remained largely unaware of this lethal complication - which masquerades as croup).

InfluenzaThe influenza pandemic of 1918-1919 killed more people than World War I
The origin of the Grim Reaper
Trivalent vaccines have been available since 1945 and are adjusted annually according to the prevalent flu strains in circulation. The primary pediatric controversy surrounding the influenza vaccine surrounds its administration to infants and toddlers.
Vaccine. 2006 Feb 13;24(7):957-63. 2005 Inactivated influenza vaccine effectiveness in children under 6 years of age during the 2002-2003 season (Fujieda et al.)In a prospectively collected cohort of 2913 patients comprised of 6 month to 6 years olds, the authors compared vaccinated to non-vaccinated infants for incidence of influenza infection. There was no efficacy of vaccination in children less than two years. But the CDC and the Red Book still recommend influenza vaccination from 6 months on…. Why should we do this?

What is the take home message?
Some parents are confused about OPV versus IPV
A family history of allergies or febrile seizures may be a valid reason to refuse the MMR / MMRV
There is no sane rationale for giving the influenza virus to infants under 2 years of age (and you can quote me on that)
We cannot rest on our laurels or become complacent with vaccine technology. Intelligent parental concerns must be addressed so that they don’t just refuse vaccinations across the board. That is the real danger, that conquered diseases will return due to parental vaccination refusal (as has already occurred with measles and mumps)