A systematic literature review
101
Bisphosphonates in early breast cancer A systematic literature review November 2011 Funded by the National Breast Cancer Foundation
Transcript of A systematic literature review

Bisphosphonates in early breast cancer
A systematic literature review
November 2011
Funded by the National Breast Cancer Foundation

Bisphosphonates in early breast cancer: a systematic literature review was prepared and produced by: Cancer Australia Locked Bag 3 Strawberry Hills NSW 2012 Australia Tel: +61 2 9357 9400 Fax: +61 2 9357 9477 Website: www.canceraustralia.gov.au © Cancer Australia 2011 ISBN Online: 978-1-74127-168-3 Recommended citation Cancer Australia. Bisphosphonates in early breast cancer: a systematic literature review. Cancer Australia, Surry Hills, NSW, 2011.
Copyright statements: Paper-based publications This work is copyright. You may reproduce the whole or part of this work in unaltered form for your own personal use or, if you are part of an organisation, for internal use within your organisation, but only if you or your organisation do not use the reproduction for any commercial purpose and retain this copyright notice and all disclaimer notices as part of that reproduction. Apart from rights to use as permitted by the Copyright Act 1968 or allowed by this copyright notice, all other rights are reserved and you are not allowed to reproduce the whole or any part of this work in any way (electronic or otherwise) without first being given the specific written permission from Cancer Australia to do so. Requests and inquiries concerning reproduction and rights are to be sent to the Publications and Copyright contact officer, Cancer Australia, Locked Bag 3, Strawberry Hills, NSW 2012. Internet sites This work is copyright. You may download, display, print and reproduce the whole or part of this work in unaltered form for your own personal use or, if you are part of an organisation, for internal use within your organisation, but only if you or your organisation do not use the reproduction for any commercial purpose and retain this copyright notice and all disclaimer notices as part of that reproduction. Apart from rights to use as permitted by the Copyright Act 1968 or allowed by this copyright notice, all other rights are reserved and you are not allowed to reproduce the whole or any part of this work in any way (electronic or otherwise) without first being given the specific written permission from Cancer Australia to do so. Requests and inquiries concerning reproduction and rights are to be sent to the Publications and Copyright contact officer, Cancer Australia, Locked Bag 3, Strawberry Hills, NSW 2012 Copies of Bisphosphonates in early breast cancer: a systematic literature review can be downloaded from the Cancer Australia website: www.canceraustralia.gov.au.



Systematic review of bisphosphonates in early breast cancer i
Contents
Acknowledgements .................................................................................................................... iv
Executive summary ..................................................................................................................... 1
1 Background ..................................................................................................................... 2
1.1 Breast cancer in Australia ..................................................................................... 2
1.2 Bisphosphonates in early breast cancer ............................................................... 2
1.3 Clinical practice guidelines .................................................................................... 2
2 Methods ........................................................................................................................... 4
2.1 Criteria for determining study eligibility ................................................................. 4
2.2 Literature search methodology ............................................................................. 4
2.3 Assessment of study eligibility .............................................................................. 5
2.4 Included studies .................................................................................................... 6
2.5 Conference abstracts ............................................................................................ 9
2.6 Appraisal of included studies .............................................................................. 12
2.7 Data analysis ...................................................................................................... 14
3 Description of included studies ................................................................................... 15
3.1 Systematic reviews ............................................................................................. 15
3.2 Primary studies ................................................................................................... 17
4 Results of included studies ......................................................................................... 32
4.1 Disease-free survival, recurrence-free survival, and survival without bone metastasis ....................................................................................................................... 32
4.2 Mortality and overall survival ............................................................................... 34
4.3 Adverse events ................................................................................................... 37
4.4 Cancer recurrence and metastasis ..................................................................... 43
4.5 Quality of life ....................................................................................................... 49
4.6 Spinal bone mineral density (BMD) .................................................................... 49
4.7 Bone mineral density (BMD) at locations other than the spine ........................... 57
4.8 Osteopenia/osteoporosis .................................................................................... 68
4.9 Fracture occurrence ............................................................................................ 74
5 Clinical practice guidelines .......................................................................................... 79
5.1 European Society for Medical Oncology (ESMO) 2010 ...................................... 79
5.2 New Zealand Ministry of Health 2009 ................................................................. 79
5.3 UK Expert Group 2008 ....................................................................................... 80

ii Systematic review of bisphosphonates in early breast cancer
6 Discussion ..................................................................................................................... 81
7 Conclusion .................................................................................................................... 83
Abbreviations ............................................................................................................................ 84
Appendix A Contributors ...................................................................................................... 89
Appendix B Literature search strategy ................................................................................ 90
Appendix C Conference abstract literature search ............................................................ 92
Appendix D Clinical practice guideline literature search ................................................... 93

Systematic review of bisphosphonates in early breast cancer iii
Tables
Table 1 Criteria for determining study eligibility ....................................................................... 4
Table 2 Exclusion criteria ......................................................................................................... 5
Table 3 Included and excluded citations .................................................................................. 6
Table 4 Included systematic reviews ....................................................................................... 6
Table 5 Included randomised controlled trials (RCTs) ............................................................. 7
Table 6 Characteristics of the identified conference abstracts describing unpublished RCTs ......................................................................................................................... 10
Table 7 NHMRC dimensions of evidence8 ............................................................................. 12
Table 8 NHMRC interim levels of evidence9 .......................................................................... 13
Table 9 Quality criteria for different levels of evidence9 ......................................................... 14
Table 10 Key characteristics of included RCTs ....................................................................... 19
Table 11 Disease-free survival, recurrence-free survival, and survival free of bone metastasis ................................................................................................................. 33
Table 12 Mortality and overall survival ..................................................................................... 36
Table 13 Adverse events ......................................................................................................... 40
Table 14 Cancer recurrence and metastasis ........................................................................... 46
Table 15 Spinal BMD ............................................................................................................... 52
Table 16 BMD at locations other than the spine ...................................................................... 61
Table 17 ZO-FAST: shift table for LS BMD measurementsa at month 1214 ............................. 70
Table 18 Osteopenia/osteoporosis .......................................................................................... 72
Table 19 Fracture occurrence .................................................................................................. 76
Table 20 Search strategy ......................................................................................................... 90
Table 21 Conference abstract literature search ....................................................................... 92
Table 22 Clinical practice guideline literature search ............................................................... 93

iv Systematic review of bisphosphonates in early breast cancer
Acknowledgements
This review was developed on behalf of National Breast and Ovarian Cancer Centre (NBOCC)* by Gregory Merlo, Sonja Reibe, and Adele Weston of Health Technology Analysts.
Funding
The funding for the development of this review was provided by the National Breast Cancer Foundation.
Contributors
The contribution and support of the many individuals and groups in the development of this document are gratefully acknowledged.
See Appendix A for more information.
*In July 2011, National Breast and Ovarian Cancer Centre (NBOCC) amalgamated with Cancer Australia to form a single national agency, Cancer Australia, to provide leadership in cancer control and improve outcomes for Australians affected by cancer.

Systematic review of bisphosphonates in early breast cancer 1
Executive summary
Breast cancer is the most common cancer in women in Australia (excluding non-reportable skin cancer).1 Treatment for breast cancer is often associated with bone loss, which increases the risk of skeletal morbidity. Bisphosphonates are a class of drugs that work by reducing bone turnover. Additional to the role of preventing bone loss, preliminary data indicate that adjuvant therapy with bisphosphonates may lower the risk of breast cancer recurrence.
The use of bisphosphonates in early breast cancer was identified as a topic for evidence review and guideline recommendation development. The following clinical question was selected as the focus of the systematic literature review:
What is the role of bisphosphonates in early breast cancer?
A Cochrane review was first published in 2005,2 with evidence updated until 2007, which assessed the effect of bisphosphonates on skeletal events (SE), bone pain, quality of life (QoL) and survival in women with early and advanced breast cancer. National Breast and Ovarian Cancer Centre commissioned this systematic review of literature published between January 2007 and August 2010 to identify evidence published since 2007 about the use of bisphosphonates for women with early breast cancer, building on the published Cochrane review as the primary reference for evidence prior to 2007.
A total of 31 publications were included in this review, comprising of four systematic reviews and 27 publications describing 13 randomised controlled trials (RCTs). Meta-analyses were conducted to pool the results for selected outcomes, using the data from previously published systematic reviews, updated with the results from subsequently published RCTs.
Short-term use of bisphosphonates (up to four years) can reduce lumbar spine, hip and femoral neck BMD loss associated with treatment for early breast cancer. Zoledronic acid reduces the incidence of osteoporosis; however there is insufficient evidence to demonstrate an effect on osteoporosis with other bisphosphonates.
Zoledronic acid may lower the risk of cancer recurrence, and the addition of zoledronic acid to endocrine therapy may increase disease-free survival and recurrence-free survival in premenopausal women. There is no evidence that other bisphosphonates have an effect on cancer recurrence or disease-free survival.
Bisphosphonates are generally associated with mild and infrequent toxicity. Zoledronic acid significantly increases the incidence of osteonecrosis of the jaw; although the overall incidence is low (approximately 0.2% of women taking bisphosphonates). None of the included studies reported quality of life as an outcome.

2 Systematic review of bisphosphonates in early breast cancer
1 Background
1.1 Breast cancer in Australia
Breast cancer is the most common cancer in women (excluding non-reportable skin cancer). In 2007, 12 567 invasive breast cancer cases (including both early and advanced breast cancer) were diagnosed, representing 27% of all reported cancer cases in Australian women. It is the second most common cause of cancer-related death for women after lung cancer.1
1.2 Bisphosphonates in early breast cancer
Treatment for breast cancer is often associated with bone loss, which increases the risk of skeletal morbidity.3 Ovarian suppression and chemotherapy are breast cancer treatments, which cause premature menopause and accelerate the risk of bone loss. Ovarian suppression is an endocrine therapy used in hormone responsive breast cancer patients for reducing the risk of cancer recurrence and improving overall survival. Chemotherapy can result in premature menopause via direct toxicity to ovarian tissue. Aromatase inhibitors (AIs), which work by reducing tissue and plasma oestrogen levels through the inhibition of peripheral conversion of androgens to oestrogens, have also been associated with higher risk of accelerated bone loss, osteoporosis, and fractures.
Bisphosphonates are a class of drugs that work by reducing bone turnover. Bisphosphonates promote apoptosis (programmed cell death) in osteoclasts, the cells responsible for bone resorption. In combination with calcium and vitamin D, bisphosphonates are the standard care in the treatment of osteoporosis. Additional to the role of preventing bone loss, preliminary data indicate that adjuvant therapy with bisphosphonates may lower the risk of breast cancer recurrence4.
There are two classes of bisphosphonates. The newer nitrogenous bisphosphonates are more potent than the non-nitrogenous bisphosphonates.
1. Nitrogenous (alendronate, ibandronate, neridronate, olapadronate, pamidronate, risedronate and zoledronic acid).
2. Non-nitrogenous (clodronate, etidronate and tiludronate).
1.3 Clinical practice guidelines
In 2001, NBOCC published the second edition of the Clinical practice guidelines for the management of early breast cancer5. These guidelines did not include any specific recommendations regarding the use of bisphosphonates in early breast cancer.
Based on input from a multidisciplinary Steering Committee and additional consultation by NBOCC, the use of bisphosphonates in early breast cancer has been identified as a topic for evidence review and guideline recommendation development.

Systematic review of bisphosphonates in early breast cancer 3
The Bisphosphonates Working Group selected the following clinical question as the focus of the systematic literature review:
What is the role of bisphosphonates in early breast cancer?
The methods and results are described in detail in the following sections.

4 Systematic review of bisphosphonates in early breast cancer
2 Methods
2.1 Criteria for determining study eligibility
The criteria for determining study eligibility are shown in Table 1. Publications were eligible for inclusion in the systematic literature review if they described a randomised controlled trial (RCT), or a systematic review of RCTs, which recruited women with early (invasive) breast cancer. Early invasive breast cancer has been defined as tumours of not more than five centimetres diameter, with either impalpable or palpable but not fixed lymph nodes and with no evidence of distant metastases. This corresponds to tumours that are T1-2, N0-1, M0 as currently defined by the Union for International Cancer Control (UICC).
Eligible studies must have compared bisphosphonates with either: 1) no bisphosphonates (ie, placebo or standard care); 2) other bisphosphonate regimens, or 3) other bone targeting agents.
The following outcomes were extracted from the publications: 1) disease-free survival; 2) overall survival; 3) adverse events; 4) type of recurrence (bone metastases and other metastases); 5) quality of life (assessed using a quality of life instrument); 6) bone health (bone mineral density/number and time and type of skeletal events). Results for subgroups were extracted where available.
As this systematic review was an update, only studies published from 2007 onwards were eligible for inclusion.
Table 1 Criteria for determining study eligibility
Study year Studies published from 2007 onward
Study type Randomised controlled trial or a systematic review of randomised controlled trials
Population Women with early breast cancer
Intervention Bisphosphonates
Comparator No bisphosphonates Other bisphosphonate regimens Other bone targeting agents
Outcomes Disease-free survival Overall survival Adverse events Type of recurrence (bone metastases and other metastases) Quality of life (as measured by a quality of life instrument) Bone health (bone mineral density/number and time and type of skeletal events6)
2.2 Literature search methodology
A systematic method of literature searching and selection was employed in the preparation of this review. Searches for full-length publications and abstracts were conducted in EMBASE and Medline (via EMBASE.com) and the Cochrane Database of Systematic Reviews. At the request of NBOCC and the Bisphosphonates Working Group, searches were restricted to English language studies published from 2007 onwards.

Systematic review of bisphosphonates in early breast cancer 5
Search terms were approved by NBOCC before searches were conducted. The reference lists of included papers were reviewed to identify any peer-reviewed evidence that may have been missed in the literature search. Contacting of authors for unpublished research was not undertaken. The searches were conducted on 18 August 2010. Therefore, studies published after this time were not eligible for inclusion in the systematic review.
The search strategy for the online bibliographic databases is shown in Appendix B.
A search of key clinical practice guidelines was also undertaken but no additional relevant RCTs were identified.
2.3 Assessment of study eligibility
Publications identified in the literature search were reviewed and the exclusion criteria shown in Table 2 applied hierarchically. Publications were excluded if they were published before 2007, if they were the wrong study type (not an RCT), if they were in the wrong population (not women with early breast cancer), evaluated the wrong intervention (not bisphosphonates), or the wrong comparator (therapies other than placebo, bisphosphonates, or other bone targeting agents). Publications were excluded if they did not report any of the relevant outcomes (as described in Table 2). Only English language publications were eligible for inclusion.
Table 2 Exclusion criteria
Wrong year Study published before 2007
Wrong study type Not a systematic review or a randomised controlled trial
Wrong population Not in women with early (invasive) breast cancer
Wrong intervention Not bisphosphonates
Wrong comparator Therapies other than placebo, bisphosphonates, or other bone targeting agents
Wrong outcome Study did not report disease-free survival, overall survival, adverse events, recurrence (bone metastases or other metastases), quality of life, or bone health
Not in English Not in English
The exclusion criteria were applied to all citations by reviewing the abstract and title, with 890 publications excluded. A total of 34 publications remained, and the full text version of each publication was retrieved and reviewed. The same exclusion criteria were then applied to the full text articles. A total of 31 publications met the inclusion criteria.
Table 3 provides a summary of the included and excluded citations.
A full list of excluded citations annotated by the key reason for exclusion is shown in the supplementary information (available on request from Cancer Australia).

6 Systematic review of bisphosphonates in early breast cancer
Table 3 Included and excluded citations
Exclusion criteria Number
Citations excluded after review of abstract/title Published before 2007 Duplicate Wrong study type Wrong population Wrong intervention Wrong comparator Wrong outcome Not in English Total excluded citations
2 39 756 81 52 1 1 1 890
Full papers reviewed 34
Citations excluded after review of full publication
Wrong study type 2
Wrong population Wrong intervention Wrong comparator Wrong outcome Not in English
1 0 0 0 0
Total excluded citations 3
Total included citations 31
2.4 Included studies
The literature search identified four systematic reviews (shown in Table 4) and 27 publications (including five conference abstracts) describing 13 RCTs (shown in Table 5). Brufsky 20087 described combined results from both Z-FAST and ZO-FAST and is therefore shown twice in Table 5.
Table 4 Included systematic reviews
Study ID Citation
Ha 2007 Ha TC, Li H. (2007) Meta-analysis of clodronate and breast cancer survival. British Journal of Cancer 96(12):1796-1801.
Mauri 2009 Mauri D, Valachis A, Polyzos IP, Polyzos NP, Kamposioras K, and Pesce LL. (2009) Osteonecrosis of the jaw and use of bisphosphonates in adjuvant breast cancer treatment: a meta-analysis. Breast Cancer Research and Treatment 116:433-439.
Mauri 2010 Mauri D, Valachis A, Polyzos NP, Tsali L, Mavroudis D, Georgoulias V, and Casazza G. (2010) Does adjuvant bisphosphonate in early breast cancer modify the natural course of the disease? A meta-analysis of randomized controlled trials. JNCCN Journal of the National Comprehensive Cancer Network 8:279-286.
Valachis 2010 Valachis A, Polyzos NP, Georgulias V, Mavroudis D, and Mauri D. (2010) Lack of evidence for fracture prevention in early breast cancer bisphosphonate trials: A meta-analysis. Gynecologic Oncology 117:139-145.

Systematic review of bisphosphonates in early breast cancer 7
Table 5 Included randomised controlled trials (RCTs)
Study ID Citation
Clodronate
Diel 2008 Diel IJ, Solomayer EF, Costa SD, Gollan C, Goerner R, Wallwiener D, Kaufmann M, and Bastert G. (1998) Reduction in new metastases in breast cancer with adjuvant clodronate treatment. New England Journal of Medicine 339:357-363. Diel IJ, Jaschke A, Solomayer EF, Gollan C, Bastert G, Sohn C, and Schuetz F. (2008) Adjuvant oral clodronate improves the overall survival of primary breast cancer patients with micrometastases to the bone marrow: a long-term follow-up. Annals of oncology : official journal of the European Society for Medical Oncology / ESMO 19:2007-2011.
Saarto 2008 Saarto T, Vehmanen L, Blomqvist C, and Elomaa I. (2008) Ten-year follow-up of 3 years of oral adjuvant clodronate therapy shows significant prevention of osteoporosis in early-stage breast cancer. Journal of clinical oncology: official journal of the American Society of Clinical Oncology 26:4289-4295.
McCloskey 2010
McCloskey E, Paterson A, Kanis J, Tahtela R, and Powles T. (2010) Effect of oral clodronate on bone mass, bone turnover and subsequent metastases in women with primary breast cancer. European Journal of Cancer 46:558-565.
Ibandronate
ARIBON Lester JE, Dodwell D, Purohit OP, Gutcher SA, Ellis SP, Thorpe R, Horsman JM, Brown JE, Hannon RA, and Coleman RE. (2008) Prevention of anastrozole-induced bone loss with monthly oral ibandronate during adjuvant aromatase inhibitor therapy for breast cancer. Clinical Cancer Research 14:6336-6342.
Pamidronate
Kristensen 2008 Kristensen B, Ejlertsen B, Mouridsen HT, Jensen MB, Andersen J, Bjerregaard B, Cold S, Edlund P, Ewertz M, Kamby C, Lindman H, Nordenskjold B, and Bergh J. (2008) Bisphosphonate treatment in primary breast cancer: Results from a randomised comparison of oral pamidronate versus no pamidronate in patients with primary breast cancer. Acta Oncologica 47:740-746.
Risedronate
Hines 2009a Hines SL, Mincey BA, Sloan JA, Thomas SP, Chottiner E, Loprinzi CL, Carlson MD, Atherton PJ, Salim M, and Perez EA. (2009) Phase III randomized, placebo-controlled, double-blind trial of risedronate for the prevention of bone loss in premenopausal women undergoing chemotherapy for primary breast cancer. Journal of Clinical Oncology 27:1047-1053.
REBBeCa Greenspan SL, Bhattacharya RK, Sereika SM, Brufsky A, and Vogel VG. (2007) Prevention of bone loss in survivors of breast cancer: A randomized, double-blind, placebo-controlled clinical trial. Journal of Clinical Endocrinology and Metabolism 92:131-136.
Greenspan SL, Brufsky A, Lembersky BC, Bhattacharya R, Vujevich KT, Perera S, Sereika SM, and Vogel VG. (2008) Risedronate prevents bone loss in breast cancer survivors: A 2-year, randomized, double-blind, placebo-controlled clinical trial. Journal of Clinical Oncology 26:2644-2652.
van Londen GJ, Perera S, Vujevich KT, Sereika SM, Bhattacharya R, and Greenspan SL. (2008) Effect of risedronate on hip structural geometry: a 1-year, double-blind trial in chemotherapy-induced postmenopausal women. Bone 43:274-278.
van Londen GJ, Perera S, Vujevich KT, Sereika SM, Bhattacharya R, and Greenspan SL. (2010) The effect of risedronate on hip structural geometry in chemotherapy-induced postmenopausal women with or without use of aromatase inhibitors: A 2-year trial. Bone 46:655-659.

8 Systematic review of bisphosphonates in early breast cancer
Study ID Citation
SABRE Van Poznak C, Hannon R, Clack G, Campone M, Mackey JR, Apffelstaedt J, and Eastell R. (2009) Managing cancer treatment-induced bone loss: 24-month results from the study of anastrozole with the bisphosphonate risedronate (SABRE). Cancer Research 69. [conference abstract]
Van Poznak C, Hannon RA, Mackey JR, Campone M, Apffelstaedt JP, Clack G, Barlow D, Makris A, and Eastell R. (2010) Prevention of aromatase inhibitor-induced bone loss using risedronate: the SABRE trial. Journal of clinical oncology: official journal of the American Society of Clinical Oncology 28:967-975.
Zoledronic acid
ABCSG-12 Gnant MFX, Mlineritsch B, Luschin-Ebengreuth G, Grampp S, Kaessmann H, Schmid M, Menzel C, Piswanger-Soelkner JC, Galid A, Mittlboeck M, Hausmaninger H, and Jakesz R. (2007) Zoledronic acid prevents cancer treatment-induced bone loss in premenopausal women receiving adjuvant endocrine therapy for hormone-responsive breast cancer: A report from the Austrian Breast and Colorectal Cancer Study Group. Journal of Clinical Oncology 25:820-828.
Gnant M, Mlineritsch B, Luschin-Ebengreuth G, Kainberger F, Kassmann H, Piswanger-Solkner JC, Seifert M, Ploner F, Menzel C, Dubsky P, Fitzal F, Bjelic-Radisic V, Steger G, Greil R, Marth C, Kubista E, Samonigg H, Wohlmuth P, Mittlbock M, and Jakesz R. (2008) Adjuvant endocrine therapy plus zoledronic acid in premenopausal women with early-stage breast cancer: 5-year follow-up of the ABCSG-12 bone-mineral density substudy. The Lancet Oncology 9:840-849.
Gnant M, Mlineritsch B, Schippinger W, Luschin-Ebengreuth G, Steger GG, Bjelic-Radisic V, Jakesz R, Kubista E, Marth C, and Greil R. (2008) Zoledronic acid (ZOL) improves disease-free (DFS) and recurrence-free survival (RFS) in premenopausal women with early breast cancer (ERBC) receiving adjuvant endocrine therapy: Multivariate analysis of efficacy data from the austrian breast and colorectal cancer study group (ABCSG)-12. Annals of Oncology 19:viii44. [conference abstract]
Gnant M, Mlineritsch B, Schippinger W, Luschin-Ebengreuth G, Postlberger S, Menzel C, Jakesz R, Seifert M, Hubalek M, Bjelic-Radisic V, Samonigg H, Tausch C, Eidtmann H, Steger G, Kwasny W, Dubsky P, Fridrik M, Fitzal F, Stierer M, Rucklinger E, and Greil R. (2009) Endocrine therapy plus zoledronic acid in premenopausal breast cancer. New England Journal of Medicine 360:679-691.
Gnant M, Mlineritsch B, Schippinger W, Luschin-Ebengreuth G, Steger G, Bjelic-Radisic V, Jakesz R, Kubista E, Marth C, and Greil R. (2009) The number needed to treat (NNT) as a measure of drug efficacy: The case of zoledronic acid for early hormone-responsive breast cancer in the ABCSG-12 trial. Cancer Research 69. [conference abstract]
Hershman 2010 Hershman DL, McMahon DJ, Crew KD, Cremers S, Irani D, Cucchiara G, Brafman L, and Shane E. (2008) Zoledronic acid prevents bone loss in premenopausal women undergoing adjuvant chemotherapy for early-stage breast cancer. Journal of Clinical Oncology 26:4739-4745.
Hershman DL, McMahon DJ, Crew KD, Shao T, Cremers S, Brafman L, Awad D, and Shane E. (2010) Prevention of bone loss by zoledronic acid in premenopausal women undergoing adjuvant chemotherapy persist up to one year following discontinuing treatment. Journal of Clinical Endocrinology and Metabolism 95:559-566.
Hines 2009b Hines SL, Mincey B, Dentchev T, Sloan JA, Perez EA, Johnson DB, Schaefer PL, Alberts S, Liu H, Kahanic S, Mazurczak MA, Nikcevich DA, and Loprinzi CL. (2009) Immediate versus delayed zoledronic acid for prevention of bone loss in postmenopausal women with breast cancer starting letrozole after tamoxifen-N03CC. Breast Cancer Research and Treatment 117:603-609.

Systematic review of bisphosphonates in early breast cancer 9
Study ID Citation
Z-FAST Brufsky A, Harker WG, Beck JT, Carroll R, Tan CE, Seidler C, Hohneker J, Lacerna L, Petrone S, and Perez EA. (2007) Zoledronic acid inhibits adjuvant letrozole-induced bone loss in postmenopausal women with early breast cancer. Journal of clinical oncology: official journal of the American Society of Clinical Oncology 25:829-836.
Brufsky A, Bundred N, Coleman R, Lambert-Falls R, Mena R, Hadji P, Jin L, Schenk N, Ericson S, and Perez EA. (2008) Integrated analysis of zoledronic acid for prevention of aromatase inhibitor-associated bone loss in postmenopausal women with early breast cancer receiving adjuvant letrozole. Oncologist 13:503-514.
Brufsky A, Bosserman LD, Caradonna RR, Haley BB, Jones CM, Moore HCF, Jin L, Warsi GM, Ericson SG, and Perez EA. (2009) Zoledronic acid effectively prevents aromatase inhibitor- associated bone loss in postmenopausal women with early breast cancer receiving adjuvant letrozole: Z-fast study 36-month follow-up results. Clinical Breast Cancer 9:77-85.
ZO-FAST Brufsky A, Bundred N, Coleman R, Lambert-Falls R, Mena R, Hadji P, Jin L, Schenk N, Ericson S, and Perez EA. (2008) Integrated analysis of zoledronic acid for prevention of aromatase inhibitor-associated bone loss in postmenopausal women with early breast cancer receiving adjuvant letrozole. Oncologist 13:503-514.
Bundred NJ, Campbell ID, Davidson N, DeBoer RH, Eidtmann H, Monnier A, Neven P, von Minckwitz G, Miller JC, Schenk NL, and Coleman RE. (2008) Effective inhibition of aromatase inhibitor-associated bone loss by zoledronic acid in postmenopausal women with early breast cancer receiving adjuvant letrozole: ZO-FAST study results. Cancer 112:1001-1010.
Bundred N, Cramer A, Morris J, Landberg G, Renshaw L, Winter M, Coleman RE, Grassby S, Knox WF, and Dixon JM. (2010) Randomised placebo controlled trial studying short term biological effects of the combination of letrozole and zoledronic acid on invasive breast cancer. European Journal of Cancer, Supplement 8:90-91. [conference abstract]
Eidtmann H, Bundred NJ, DeBoer R, Llombart A, Davidson N, Neven P, von Minckwitz G, Miller J, Schenk N, and Coleman R. (2009) The effect of zoledronic acid on aromatase inhibitor associated bone loss in postmenopausal women with early breast cancer receiving adjuvant letrozole: 36 months follow-up of ZO-FAST. Cancer Research 69. [conference abstract]
2.5 Conference abstracts
Bisphosphonate terms were used to search conference websites for abstracts to identify RCTs of bisphosphonates in early breast cancer that have not been published as full articles (see Appendix C for full search strategy). The websites were selected by NBOCC and the Bisphosphonates Working Group as relevant for the clinical question. The search was limited to conference abstracts published between 2009 and 2010. Searching relied on available electronic search functions and no manual searching was undertaken.
The literature search identified seven conference abstracts. No formal data extraction or quality assessment has been undertaken, and these abstracts are not considered further within this systematic review.
Table 6 presents the characteristics of the seven identified conference abstracts.
10 Systematic review of bisphosphonates in early breast cancer
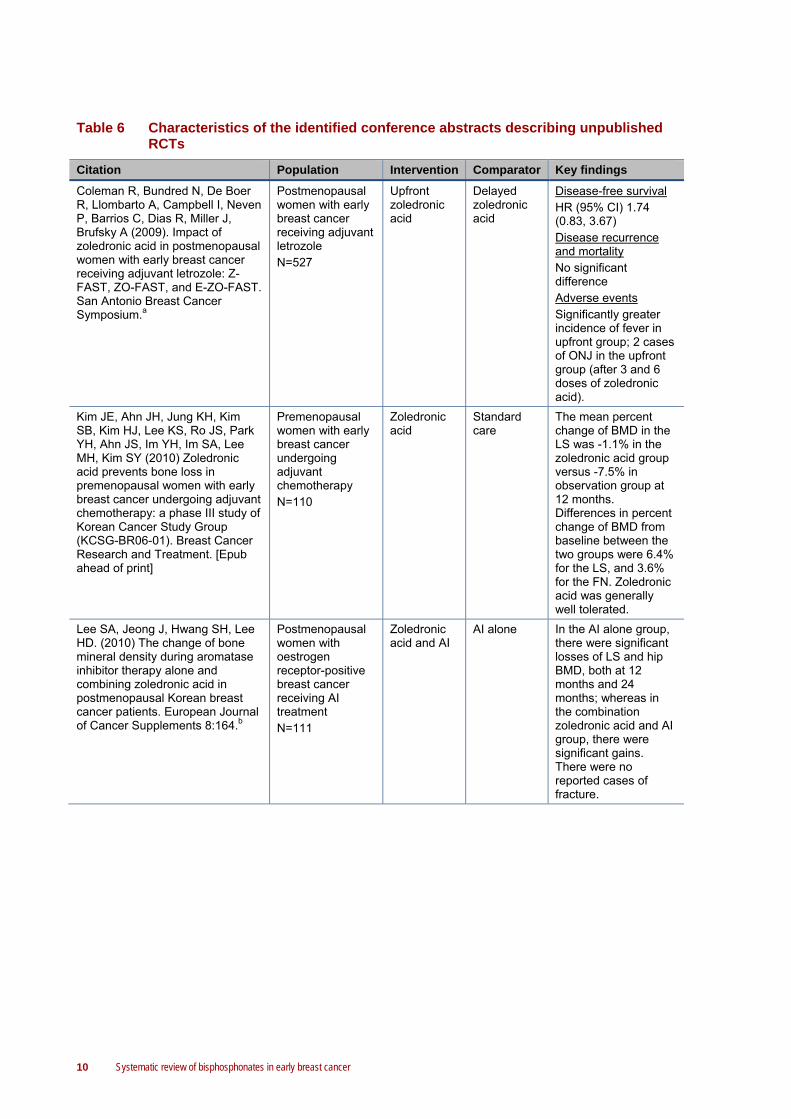
Table 6 Characteristics of the identified conference abstracts describing unpublished RCTs
Citation Population Intervention Comparator Key findings
Coleman R, Bundred N, De Boer R, Llombarto A, Campbell I, Neven P, Barrios C, Dias R, Miller J, Brufsky A (2009). Impact of zoledronic acid in postmenopausal women with early breast cancer receiving adjuvant letrozole: Z-FAST, ZO-FAST, and E-ZO-FAST. San Antonio Breast Cancer Symposium.a
Postmenopausal women with early breast cancer receiving adjuvant letrozole N=527
Upfront zoledronic acid
Delayed zoledronic acid
Disease-free survival HR (95% CI) 1.74 (0.83, 3.67) Disease recurrence and mortality No significant difference Adverse events Significantly greater incidence of fever in upfront group; 2 cases of ONJ in the upfront group (after 3 and 6 doses of zoledronic acid).
Kim JE, Ahn JH, Jung KH, Kim SB, Kim HJ, Lee KS, Ro JS, Park YH, Ahn JS, Im YH, Im SA, Lee MH, Kim SY (2010) Zoledronic acid prevents bone loss in premenopausal women with early breast cancer undergoing adjuvant chemotherapy: a phase III study of Korean Cancer Study Group (KCSG-BR06-01). Breast Cancer Research and Treatment. [Epub ahead of print]
Premenopausal women with early breast cancer undergoing adjuvant chemotherapy N=110
Zoledronic acid
Standard care
The mean percent change of BMD in the LS was -1.1% in the zoledronic acid group versus -7.5% in observation group at 12 months. Differences in percent change of BMD from baseline between the two groups were 6.4% for the LS, and 3.6% for the FN. Zoledronic acid was generally well tolerated.
Lee SA, Jeong J, Hwang SH, Lee HD. (2010) The change of bone mineral density during aromatase inhibitor therapy alone and combining zoledronic acid in postmenopausal Korean breast cancer patients. European Journal of Cancer Supplements 8:164.b
Postmenopausal women with oestrogen receptor-positive breast cancer receiving AI treatment N=111
Zoledronic acid and AI
AI alone In the AI alone group, there were significant losses of LS and hip BMD, both at 12 months and 24 months; whereas in the combination zoledronic acid and AI group, there were significant gains. There were no reported cases of fracture.

Systematic review of bisphosphonates in early breast cancer 11
Citation Population Intervention Comparator Key findings
Markopoulos C, Tzorakoleftherakis E, Polychronis A, Venizelos V, Xepapadakis G, Kalogerakos K, Papadiamantis J, Zobolas V, Janinis J, Dafni U. (2009) Management of bone loss in breast cancer patients: 24-month results from the ARBI trial of anastrozole with risedronate. Journal of Clinical Oncology 27:15s.
Postmenopausal, breast cancer patientsc treated with anastrozole N=70
Risedronate Standard care
T-score change from baseline was significantly different only for LS at 24 months (P=0.007) and was significantly higher from baseline for the risedronate arm. At 12 months, 4 (12.1%) patients in the control arm had a T-score < -2.0 without becoming osteoporotic, while 2 (6.1%) moved to the normal BMD region; from the risedronate patients, only 2 (5.4%) had a T-score < -2.0 without becoming osteoporotic, while 2 (6.1%) moved to the normal BMD region.
Mobus V, Conrad B, Schneeweis A, Kreinberg R, Solomayer EF, Clemens MR, Tesch H, Loibl V, Nekljudova V, von Minckwitz G. (2009) A phase III trial to compare ETC versus EC-TX and ibandronate versus observation in patients with node-positive primary breast cancer. Journal of Clinical Oncology 27:15s.
Patients with node-positive primary breast cancer randomised to receive either ETC or EC-TX N=3024
Ibandronate Standard care
NR
Safra T, Bernstein Molho R, Stephansky I, Yaal-Hahoshen N, Inbar M, Ackerstein A, Geffen D. (2009) Effect of zoledronic acid on bone loss in postmenopausal women with early breast cancer treated with sequential tamoxifen and letrozole. Journal of Clinical Oncology 27:15s.
Postmenopausal women with early breast cancer treated with sequential tamoxifen and letrozole N=74
Zoledronic acid
Standard care
A significant interaction between groups and time was found, in favour of zoledronic acid in lumbar T-score. While in the control group a significant decline in LS BMD was noticed, in the treatment group BMD did not change over time. Adverse events with zoledronic acid were mild with some flu like syndromes. No serious renal adverse event or ONJ cases were reported.

12 Systematic review of bisphosphonates in early breast cancer
Citation Population Intervention Comparator Key findings
Ziller M, Hadji P, Kauka K, Bauer T, Albert US, Muth M, Kalder M. (2009) Influence of zoledronic acid on bone mineral density in premenopausal women with hormone receptor positive or negative breast cancer and neoadjuvant chemotherapy or endocrine treatment. European Journal of Cancer Supplements 7:277.
Premenopausal women with hormone receptor-positive or negative breast cancer and neoadjuvant or adjuvant chemotherapy or endocrine treatment N=74
Zoledronic acid
Placebo NR
Abbreviations: AI, aromatase inhibiter; BMD, bone mineral density; CI, confidence interval; EC-TX, epirubicin and cyclophosphamide followed by paclitaxel and capecitabine; ETC, epirubicin, paclitaxel and cyclophosphamide; FN, femoral neck; HR, hazard ratio; LS, lumbar spine; NR, not reported; ONJ, osteonecrosis of the jaw; RCT, randomised controlled trial a Reports results of ZO-FAST, Z-FAST, and E-ZO-FAST. Only the key findings regarding the E-ZO-FAST trial are reported in this table. b It is not clear from the abstract whether the findings are from an RCT or an observational study. c It is not clear from the abstract whether the population was limited to patients with early breast cancer.
2.6 Appraisal of included studies
2.6.1 Dimensions of evidence
The aim of this review was to find the highest quality evidence to answer the clinical questions being asked. In accordance with National Health and Medical Research Council (NHMRC) guidance, the following dimensions of evidence were reviewed for each of the included studies (shown in Table 7). It is important to recognise that the value of a piece of evidence is determined by all of these dimensions, not just the level of evidence.
Table 7 NHMRC dimensions of evidence8
Dimension Reviewer’s definition
Strength of the evidence
Level The study design used, as an indication of the degree to which bias has been eliminated by the design alone. The levels reflect the effectiveness of the study design to answer the research question.
Quality The methods used to minimise bias within an individual study (ie, other than design per se).
Statistical precision An indication of the precision of the estimate of effect reflecting the degree of certainty about the existence of a true effect, as opposed to an effect due to chance.
Size of effect Determines the magnitude of effect and whether this is of clinical importance.
Relevance of evidence Considers the relevance of the study to the specific research question and the context in which the information is likely to be applied, with regard to a) the nature of the intervention, b) the nature of the population and c) the definition of the outcomes.
Each study was assigned a level of evidence in accordance with the NHMRC (2005) interim levels of evidence (see Table 8). The highest level of evidence available is a systematic review of

Systematic review of bisphosphonates in early breast cancer 13
RCTs, which is considered the study type least subject to bias. Individual RCTs also represent good evidence. Only systematic reviews and RCTs were eligible for inclusion in this systematic review.
Table 8 NHMRC interim levels of evidence9
Level Intervention
I * A systematic review of level II studies
II A randomised controlled trial
III-1 A pseudorandomised controlled trial (ie, alternate allocation or some other method)
III-2 A comparative study with concurrent controls: • Non-randomised, experimental triala • Cohort study • Case-control study • Interrupted time series with a control group
III-3 A comparative study without concurrent controls: • Historical control study • Two or more single arm studiesb • Interrupted time series without a parallel control group
IV Case series with either post-test or pre-test/post-test outcomes
Note: When a level of evidence is attributed in the text of a document, it should also be framed according to its corresponding research question eg, level II intervention evidence; level IV diagnostic evidence; level III-2 prognostic evidence. * A systematic review will only be assigned a level of evidence as high as the studies it contains, excepting where those studies are of level II evidence. a This also includes controlled before-and-after (pre-test/post-test) studies, as well as indirect comparisons (ie, utilise A vs B and B vs C, to determine A vs C). b Comparing single arm studies ie, case series from two studies.
Even within the levels of evidence stated above, there is considerable variability in the quality of evidence. In accordance with NHMRC guidelines, it was necessary to consider the quality of each of the included studies. Quality assessment was based on criteria reported by the NHMRC (2000), as shown in Table 9, with studies rated as good, fair or poor quality.

14 Systematic review of bisphosphonates in early breast cancer
Table 9 Quality criteria for different levels of evidence9
Study type Quality criteria
Systematic review
Was an adequate search strategy used? Were the inclusion criteria appropriate and applied in an unbiased way? Was a quality assessment of included studies undertaken? Were the characteristics and results of the individual studies appropriately summarised? Were the methods for pooling the data appropriate? Were sources of heterogeneity explored?
Randomised controlled trials
Was allocation to treatment groups concealed from those responsible for recruiting patients? Was the study double-blinded? Were outcomes assessors blinded to treatment allocation? Were all randomised participants included in the analysis? Were treatment groups well matched at baseline? Was the study powered to detect a difference in primary outcome?
2.6.2 Data synthesis
In addition to the level and quality of evidence of individual studies, the review considered the body of evidence in total. This involved consideration of the volume of evidence and its consistency.
2.7 Data analysis
Meta-analyses were conducted using the data from previously published systematic reviews (Pavlakis 20052 and Mauri 201010), updated with the results from subsequently published RCTs. When updates of RCTs reported in the previously published systematic reviews were identified (e.g. Saarto 200811 and Diel 200812), the most recent results were used in the meta-analyses. The results of the Z-FAST13 and ZO-FAST14 trials were not included in the meta-analyses, as the comparator was delayed treatment rather than placebo or standard care.

Systematic review of bisphosphonates in early breast cancer 15
3 Description of included studies
3.1 Systematic reviews
The literature search identified four systematic literature reviews (Ha 2007,15 Mauri 2009,16 Mauri 2010,10 and Valachis 201017). The systematic reviews evaluated the impact of bisphosphonates on osteonecrosis of the jaw, disease course, and incidence of bone fracture when used by women with early breast cancer.
3.1.1 Ha 2007
Ha 200715 assessed the effect of adjuvant oral clodronate for breast cancer patients in terms of overall survival, bone metastasis-free survival and non-skeletal metastasis-free survival. Eligible studies were RCTs that compared oral clodronate therapy with no active treatment in patients with histologic- or cytologic-proven breast cancer but no prior history of other malignant diseases (besides recurrent breast cancer) or bisphosphonate usage. The systematic review included patients with both early and advanced breast cancer, but the review provides subgroup analyses specifically in the early breast cancer population.
The systematic review identified three RCTs in early breast cancer (Diel 199818, Saarto 200119, and Powles 200620). Diel 199818 and Powles 200620 found that clodronate treatment in early breast cancer significantly increased overall survival compared with no clodronate treatment, whereas Saarto 200119 found the opposite trend. The meta-analysis demonstrated no statistically significant difference in the overall survival between patients treated with adjuvant clodronate therapy and those receiving no treatment (HR [95% CI] 0.75 [0.31, 1.82]). Similarly, the meta-analysis did not find any statistically significant difference in bone metastasis-free survival (HR [95% CI] 0.68 [0.38, 1.23]) and non-skeletal metastasis-free survival (HR [95% CI] 0.89 [0.40, 1.98]) between patients who received adjuvant clodronate compared with those who did not.
3.1.2 Mauri 2009
Mauri 200916 assessed the relationship between osteonecrosis of the jaw and the use of bisphosphonates as adjuvant breast cancer treatment. Eligible studies were controlled trials that randomised patients with primary breast cancer to receive adjuvant bisphosphonate treatment versus either placebo or standard care. Only studies that clearly stated the number of patients with osteonecrosis of the jaw were eligible for inclusion.
The literature search identified 15 trials that were included in the meta-analysis. Overall, osteonecrosis of the jaw was a rare event, occurring in 13 of the 5312 patients receiving bisphosphonates (0.24%), and in one of the 5382 patients in the control group. All the 13 events among the bisphosphonates arms occurred in patients randomised to zoledronic acid (N=3987). No events of osteonecrosis of the jaw were reported among patients randomised to clodronate (N=669), pamidronate (N=460), risedronate (N=171), and ibandronate (N=25). Although the absolute incidence was low, meta-analysis results found that zoledronic acid significantly increased the incidence of osteonecrosis of the jaw (OR [95% CI] 3.23 [1.7, 8]) compared with control.

16 Systematic review of bisphosphonates in early breast cancer
Mauri 200916 included results from abstracts of studies that were not published as full papers. The impact of zoledronic acid on osteonecrosis of the jaw was driven by the interim results of the yet to be published AZURE trial, where there have been 13 (0.8%) confirmed cases of osteonecrosis of the jaw in women treated with zoledronic acid21.
3.1.3 Mauri 2010
Mauri 201010 assessed the impact of bisphosphonates on disease course in patients with early breast cancer. Eligible studies were controlled trials that randomised patients with primary breast cancer to receive adjuvant bisphosphonate treatment versus either placebo or standard care.
The literature search identified 13 trials that were included in the meta-analysis. Meta-analysis results showed no significant differences between bisphosphonates and control for mortality (OR [95% CI] 0.708 [0.482, 1.041]; P=0.079; N=6689), disease recurrence (OR [95% CI] 0.843 [0.602, 1.181]; P=0.321; N=5631), and bone metastases (OR [95% CI] 0.925 [0.768, 1.114]; P=0.413; N=5571). There were no differences between study arms for type of recurrence, including distant metastases (OR [95% CI] 0.896 [0.674, 1.192]; P=0.453; N=4618), visceral recurrence (OR [95% CI] 1.051 [0.686, 1.609]; P=0.820; N=1693), and local relapses (OR [95% CI] 1.056 [0.750, 1.487]; P=0.756; N=4276).
Subgroup analyses for cancer recurrence according to the type of bisphosphonate used revealed a significantly lower risk with zoledronic acid (OR [95% CI] 0.675 [0.479, 0.952]; P=0.025; N=4142). Zoledronic acid did not have a significant effect on mortality (OR [95% CI] 0.642 [0.388, 1.063]; P=0.085; N=3990) or bone metastasis (OR [95% CI] 0.661 [0.379, 1.151]; P=0.144; N=2925) compared with treatment without bisphosphonates.
3.1.4 Valachis 2010
Valachis 201017 assessed the impact of bisphosphonates on fracture prevention in patients with early breast cancer. Eligible studies were controlled trials that randomised patients with primary breast cancer to receive adjuvant bisphosphonate treatment versus either placebo or standard care.
The literature search identified 14 trials that were included in the meta-analysis. Meta-analysis results showed no significant difference between study arms in incidence of fracture (OR [95% CI] 0.84 [0.65, 1.09]). The authors conducted a sensitivity analysis excluding two studies where fractures were only evaluated and reported in patients who developed bone metastasis during the study period. There was still no significant difference between treatment arms in fracture incidence (OR [95% CI] 0.99 [0.73, 1.34]). Treatment with bisphosphonates did not reduce the fracture rate in postmenopausal women with early breast cancer (OR [95% CI] 0.82 [0.55, 1.20]) or in women with breast cancer receiving AIs (OR [95% CI] 0.79 [0.53, 1.17]).

Systematic review of bisphosphonates in early breast cancer 17
3.2 Primary studies
The literature search identified 13 RCTs, including three investigating clodronate, one study investigating ibandronate, and one pamidronate, three studying risedronate, and the other five investigating the use of zoledronic acid. The study populations included both pre- and post-menopausal women, women on chemotherapy, and women on endocrine therapy. The study characteristics of the included RCTs are presented in Table 10.


Systematic review of bisphosphonates in early breast cancer 19
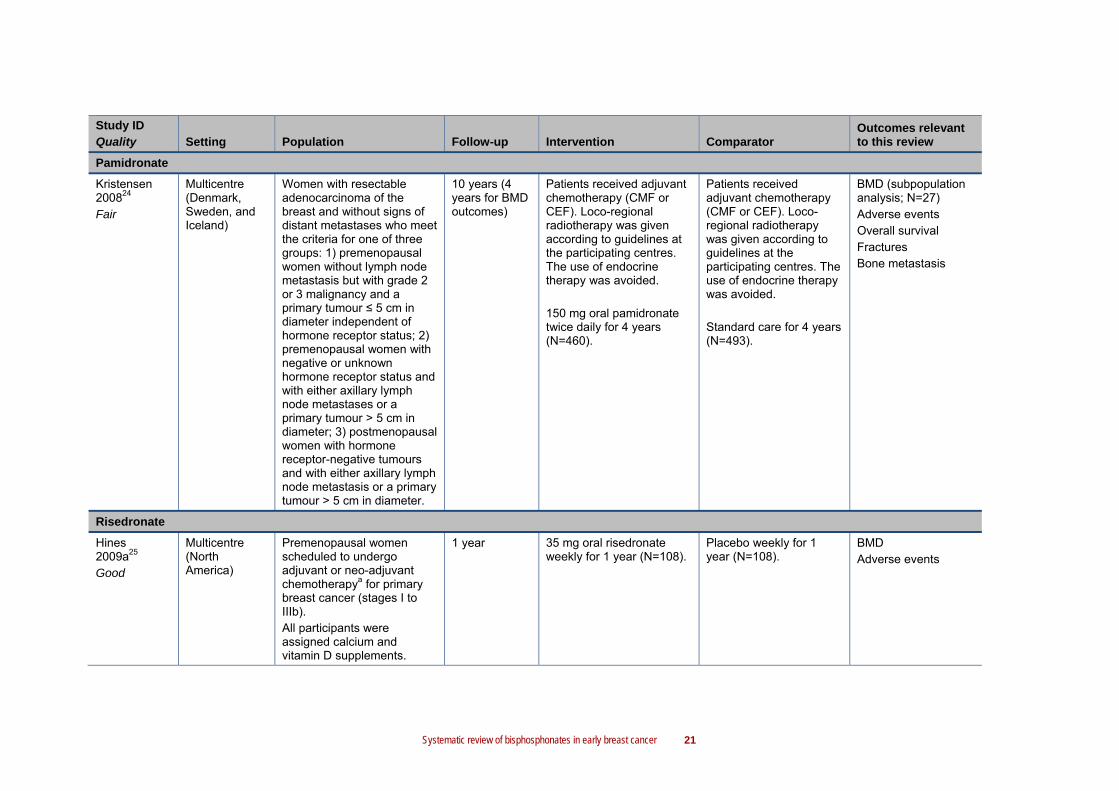
Table 10 Key characteristics of included RCTs
Study ID Quality Setting Population Follow-up Intervention Comparator
Outcomes relevant to this review
Clodronate
Diel 200812,18 Fair
Germany Pre- and post-menopausal women with primary breast cancer (classified as stage T1, T2, T3, or T4 and histologically classified as N0, N1 or N2). All patients had immunocytochemical evidence of at least one tumour cell per million cells in the bone marrow. Patients with confirmed distant metastasis, or secondary malignant disease were not eligible for enrolment. All patients received standard surgical treatment and customary adjuvant endocrine therapy or chemotherapy with or without radiotherapy. Approximately one-third of patients in both treatment arms received tamoxifen.
Median 8.5 years
1600 mg/day oral clodronate for 2 years (N=157).
Standard care for 2 years (N=145).
Mortality Distant, bone and visceral metastasis
McCloskey 201022 Fair
Multicentre Pre- and post-menopausal women having surgery, radiotherapy, and/or drug treatment for primary operable breast cancer with no evidence of metastasis.
2 years 1600 mg/day oral clodronate for 2 years (N=419).
Placebo for 2 years (N=432).
BMD

20 Systematic review of bisphosphonates in early breast cancer
Study ID Quality Setting Population Follow-up Intervention Comparator
Outcomes relevant to this review
Saarto 200811 Fair
Finland Pre- and post-menopausal women with newly diagnosed breast cancer. The participants underwent surgery with total mastectomy or breast-conserving resection and axillary evacuation and all received postoperative radiotherapy. Premenopausal women received 6 cycles of cyclophosphamide, 40 mg/ms methotrexate, and 600 mg/m2 fluorouracil administered IV on day one and thereafter at 3-week intervals.
10 years Premenopausal 1600 mg/day oral clodronate for 3 years (N=20). Postmenopausal 1600 mg/day oral clodronate for 3 years; and randomised to receive either 20 mg tamoxifen (N=14) or 60 mg/d toremifene (N=10), for 3 years.
Premenopausal Standard care for 3 years (N=35). Postmenopausal Randomised to receive either 20 mg tamoxifen (N=11) or 60 mg/d toremifene (N=6), for 3 years.
BMD
Ibandronate
ARIBON23 Fair
UK Osteopenic (T-score of > -2.5 and < -1.0 either at the LS or hip), postmenopausal women with a confirmed diagnosis of oestrogen receptor-positive breast cancer. All patients received anastrozole 1 mg once a day as well as calcium and vitamin D supplements.
2 years 150 mg oral ibandronate every 28 days for 2 years (N=25).
Placebo every 28 days for 2 years (N=25).
BMD Adverse events Fractures
Systematic review of bisphosphonates in early breast cancer 21
Study ID Quality Setting Population Follow-up Intervention Comparator
Outcomes relevant to this review
Pamidronate
Kristensen 200824 Fair
Multicentre (Denmark, Sweden, and Iceland)
Women with resectable adenocarcinoma of the breast and without signs of distant metastases who meet the criteria for one of three groups: 1) premenopausal women without lymph node metastasis but with grade 2 or 3 malignancy and a primary tumour ≤ 5 cm in diameter independent of hormone receptor status; 2) premenopausal women with negative or unknown hormone receptor status and with either axillary lymph node metastases or a primary tumour > 5 cm in diameter; 3) postmenopausal women with hormone receptor-negative tumours and with either axillary lymph node metastasis or a primary tumour > 5 cm in diameter.
10 years (4 years for BMD outcomes)
Patients received adjuvant chemotherapy (CMF or CEF). Loco-regional radiotherapy was given according to guidelines at the participating centres. The use of endocrine therapy was avoided. 150 mg oral pamidronate twice daily for 4 years (N=460).
Patients received adjuvant chemotherapy (CMF or CEF). Loco-regional radiotherapy was given according to guidelines at the participating centres. The use of endocrine therapy was avoided. Standard care for 4 years (N=493).
BMD (subpopulation analysis; N=27) Adverse events Overall survival Fractures Bone metastasis
Risedronate
Hines 2009a25 Good
Multicentre (North America)
Premenopausal women scheduled to undergo adjuvant or neo-adjuvant chemotherapya for primary breast cancer (stages I to IIIb). All participants were assigned calcium and vitamin D supplements.
1 year 35 mg oral risedronate weekly for 1 year (N=108).
Placebo weekly for 1 year (N=108).
BMD Adverse events

22 Systematic review of bisphosphonates in early breast cancer
Study ID Quality Setting Population Follow-up Intervention Comparator
Outcomes relevant to this review
REBBeCa26-29 Good
USA Women with breast cancer who were newly postmenopausal (up to 8 years) after being treated with chemotherapy with or without tamoxifen or aromatase inhibitors24. Women with a daily calcium intake less than 1200 mg received supplementary calcium with vitamin D.
2 years25,27 35 mg oral risedronate weekly for 2 years (N=43).
Placebo weekly for 2 years (N=44).
BMD Adverse events Cancer recurrence
SABRE30 Good
Multicentre Postmenopausal women with non-metastatic breast cancer, moderate risk of fractureb, and scheduled to receive anastrozole. All participants were assigned calcium and vitamin D supplements.
2 years 35 mg oral risedronate weekly for 2 years (N=77).
Placebo weekly for 2 years (N=77).
BMD Adverse events Mortality
Zoledronic acid
ABCSG-1231,32 Fair
Austria Premenopausal women who had undergone primary surgery for stage I or II oestrogen- and/or progesterone- receptor-positive breast cancer, who had fewer than 10 positive lymph nodes, and who were scheduled to receive standard therapy with goserelin.
Overall Median 47.8 months BMD sub-study 5 years
GTZ for 3 years Goserelin (3.6 mg s.c. every 28 days); tamoxifen (20 mg/day orally); zoledronic acid (initially 8 mg IV every 4 weeks)c (N=449). GAZ for 3 years Goserelin (3.6 mg s.c. every 28 days); anastrozole (1 mg/day orally); zoledronic acid (initially 8 mg IV every 4 weeks)c (N=450).
GT for 3 years Goserelin (3.6 mg s.c. every 28 days); tamoxifen (20 mg/day orally) (N=451). GA for 3 years Goserelin (3.6 mg s.c. every 28 days); anastrozole (1 mg/day orally) (N=453).
BMD Adverse events Mortality Fractures Cancer recurrence and bone metastasis Disease-free survival

Systematic review of bisphosphonates in early breast cancer 23
Study ID Quality Setting Population Follow-up Intervention Comparator
Outcomes relevant to this review
Hershman 201033 Fair
USA Newly diagnosed premenopausal women receiving chemotherapy for histologically proven non-metastatic breast cancer. All participants were assigned calcium and vitamin D supplements.
2-year follow-up for BMD; 52 week follow-up for adverse events and recurrence
Zoledronic acid 4 mg IV over 15 minutes every 3 months for 1 year (N=57).
Placebo for 1 year (N=57).
BMD Adverse events Cancer recurrence
Hines 2009b34 Fair
USA Postmenopausal women with a history of stage I-IIIa, oestrogen and/or progesterone receptor-positive breast cancer who had completed ≤ 6 years of tamoxifen, and had no evidence of recurrent or metastatic disease. All participants were assigned calcium and vitamin D supplements.
2 years Letrozole 2.5 mg orally daily for 5 years. Upfrontd 4 mge zoledronic acid IV over 15 minutes every 6 months for 5 years or until breast cancer recurrence (N=279).
Letrozole 2.5 mg orally daily for 5 years. Delayedf 4 mge zoledronic acid 4 mg IV over 15 minutes every 6 months for 5 years or until breast cancer recurrence
(N=279).
BMD Adverse events
Z-FAST13 Fair
RCT USA and Canada
Postmenopausal women who had a history of surgically resectable stage I, II, or IIIa oestrogen and/or progesterone receptor-positive breast cancer. Baseline LS and TH T-scores of -2.0 or greater. All participants were assigned calcium and vitamin D supplements.
3 years Letrozole 2.5 mg orally daily for 5 years. Upfrontd zoledronic acid 4 mg IV over 15 minutes every 6 months for 5 years (N=301).
Letrozole 2.5 mg orally daily for 5 years. Delayedf zoledronic acid 4 mg IV over 15 minutes every 6 months for 5 years (N=301).
BMD Adverse events Fractures Cancer recurrence

24 Systematic review of bisphosphonates in early breast cancer
Study ID Quality Setting Population Follow-up Intervention Comparator
Outcomes relevant to this review
ZO-FAST14 Fair
RCT Multicentre (112 centres in 28 countries)
Postmenopausal women who had a history of surgically resectable stage I, II, or IIIa oestrogen and/or progesterone receptor-positive breast cancer. Baseline LS and TH T-scores of -2.0 or greater. All participants were assigned calcium and vitamin D supplements.
1 year Letrozole 2.5 mg orally daily for 5 years. Upfrontd zoledronic acid 4 mg IV over 15 minutes every 6 months for 5 years (N=532).
Letrozole 2.5 mg orally daily for 5 years. Delayedf zoledronic acid 4 mg IV over 15 minutes every 6 months for 5 years (N=533).
BMD Disease progression Adverse events Mortality Fractures Cancer recurrence
Abbreviations: BMD, bone mineral density; CEF, cyclophosphamide, epirubicin, and 5-fluoracil; CMF, cyclophosphamide, methotrexate, and 5-fluoracil; GA, goserelin (3.6 mg s.c. every 28 days) plus anastrozole (1 mg/day orally); GAZ, goserelin (3.6 mg s.c. every 28 days) plus anastrozole (1 mg/day orally) plus zoledronic acid (initially 8 mg IV every 4 weeks); GT, goserelin (3.6 mg s.c. every 28 days) plus tamoxifen (20 mg/day orally); GTZ, goserelin (3.6 mg s.c. every 28 days) plus tamoxifen (20 mg/day orally) plus zoledronic acid (initially 8 mg IV every 4 weeks); IU, International Unit; IV, intravenous; LS, lumbar spine; RCT, randomised controlled trial; s.c., subcutaneously; TH, total hip
a The use of ancillary treatments, as appropriate for symptom control and cancer therapy management, was allowed, except for use of bisphosphonates, oestrogen, or selective oestrogen receptor modulators other than tamoxifen. b Defined as having a BMD T-score < -1.0 but ≥ -2.0 at either the LS or TH and with no history of fragility fracture. c Protocol amendments were made after 254 patients had been enrolled; the dose of zoledronic acid was reduced to 4 mg every 6 months and the infusion time was increased to 15 minutes. d After random assignment. e The dosage of zoledronic acid was adjusted for a creatinine clearance < 60 mL/min, such that patients with a creatinine clearance of 50-60 mL/min received 3.5 mg zoledronic acid, those with a creatinine clearance of 40-49 mL/min received 3.3 mg zoledronic acid, and those with a creatinine clearance of 30-39 mL/min received 3.0 mg zoledronic acid. f The delayed group received zoledronic acid when either post-baseline LS or TH T-score decreased to less than -2.0 or a non-traumatic clinical fracture occurred.

Systematic review of bisphosphonates in early breast cancer 25
3.2.1 Clodronate
Diel 2008
Eligible participants were pre- and post-menopausal women with primary breast cancer classified as stage T1, T2, T3, or T4 and histologically classified as N0, N1 or N212. All patients had immunocytochemical evidence of at least one tumour cell per million cells in the bone marrow*. Patients with confirmed distant metastasis or secondary malignant disease were not eligible for enrolment.
Participants were randomised to receive either 1600 mg/day oral clodronate (N=157) or standard care (N=145) for 2 years. The primary outcomes included the incidence and number of new metastases and overall survival. Participants were recruited between 1990 and 1995. The women in the two study arms (clodronate and standard care) had similar baseline characteristics.
McCloskey 2010
McCloskey 201022 reports a subgroup analysis of the two-year follow-up of a randomised, double-blind, placebo-controlled study (previously described in articles published before 200735,36).
Eligible participants were pre- and post-menopausal women with histologically or cytologically confirmed primary operable breast cancer with no evidence of metastasis.36 Patients were excluded if they had significant renal, hepatic, or non-malignant bone disease; other exclusion criteria included a history of malignant bone disease or previous bisphosphonate use.
Participants were randomised to receive either 1600 mg/day oral clodronate (N=419) or matching placebo (N=432) for 2 years. The trial was powered to detect a difference in lumbar spine (LS) bone mineral density (BMD). Participants were recruited between 1989 and 1995. The women in the two study arms (clodronate and placebo) had similar baseline characteristics.
Saarto 2008
Eligible participants were pre- and post-menopausal women with newly diagnosed node-positive breast cancer11.
The patients underwent surgery with total mastectomy or breast-conserving resection and axillary evacuation. All patients had postoperative radiotherapy with 50 Gy megavoltage irradiation in 25 fractions to regional lymph nodes, and to operative scar or remaining breast after breast-conserving resection, which was done concomitantly with adjuvant therapy. Premenopausal patients (N=55) received six cycles of chemotherapy, consisting of 600 mg/m2 cyclophosphamide, 40 mg/m2 methotrexate, and 600 mg/m2 fluorouracil administered intravenously on day one and thereafter at 3-week intervals. Postmenopausal patients (N=41) were randomly assigned to receive anti-oestrogens, either 20 mg/d tamoxifen (N=25) or 60 mg/d toremifene (N=16), for 3 years. In addition, the patients were randomly assigned to either 1,600 mg oral clodronate daily for 3 years (N=44) or to no further therapy (N=52).
* Diel 2008 includes patients with micrometastases in the bone marrow. Micrometastases are not explored further in this systematic review.

26 Systematic review of bisphosphonates in early breast cancer
Data from 172 of the initial 268 patients were excluded from the current analyses, primarily because of breast cancer death (110 patients) and metastatic disease (26 patients). In addition, 10 patients were excluded because of non-cancer death, nine patients discontinued follow-up and six patients were diagnosed with other malignancies. Nine patients had diseases or were taking medications that could possibly affect bone metabolism; these patients were excluded from the analysis because of hormone replacement therapy (four patients), tamoxifen after chemotherapy (one patient), cortisone therapy (one patient), antiepileptic use (one patient), hyperparathyreosis (one patient), and hyperthyreosis (one patient). In addition, two patients were excluded because of pregnancy. Overall, 96 metastasis-free patients were eligible for analysis at 10 years of follow-up.
The women in the two study arms had similar baseline characteristics.
3.2.2 Ibandronate
ARIBON
Eligible subjects were postmenopausal women with a histologically confirmed diagnosis of oestrogen receptor-positive breast cancer23. Subjects were excluded if their menopause was induced by either prior chemotherapy or by drug therapy. Other exclusion criteria included concurrent administration of medication(s) with the effects on bone such as bisphosphonates or hormone replacement therapy, abnormal renal function, disorders of bone metabolism, and previous bilateral hip fractures or bilateral hip prostheses that would have made BMD assessments impossible.
All patients received anastrozole 1 mg once a day and calcium (500 mg) and vitamin D (400 IU) supplements daily.
Patients with normal BMD (T-score > -1 at both the LS and hip) were allocated to an observation group with a follow-up BMD assessment at 2 years. Patients with osteoporosis (T-score < -2.5 at either the LS or hip) received open-label ibandronate 150 mg every 28 days orally. Patients classified as osteopenic (T-scores of > -2.5 and < -1.0 either at the LS and hip) were randomised to receive either ibandronate tablets 150 mg every 28 days orally (N=25) or placebo tablets of identical appearance also every 28 days orally for 2 years (N=25), and are therefore the subject of the RCT.
The trial was powered to detect a change in LS and hip BDM. Patients were recruited between December 2003 and October 2005. Follow-up occurred after one and two years. Women in the two study arms (ibandronate and placebo) had similar baseline characteristics.
3.2.3 Pamidronate
Kristensen 2008
Eligible subjects were women with resectable adenocarcinoma of the breast without signs of distant metastases according to an initial physical examination, X-ray examination of the chest, and axial X-ray examination of the skeleton or a whole-body bone scintigraphy confirmed by X-ray examination if suspect for bone metastases24. Patients for the trial were recruited from the

Systematic review of bisphosphonates in early breast cancer 27
following three groups: 1) premenopausal women without lymph node metastases but with grade 2 or 3 malignancy and a primary tumour ≤ 5 cm in diameter independent of hormone receptor status; 2) premenopausal women with negative or unknown hormone receptor status and with either axillary lymph node metastases or a primary tumour > 5 cm in diameter; 3) postmenopausal women with hormone receptor-negative tumours and with either axillary lymph node metastases or a primary tumour > 5 cm in diameter.
The patients received adjuvant chemotherapy i.e. cyclophosphamide, methotrexate, and 5-fluoracil (CMF) or cyclophosphamide, epirubicin, and 5-fluoracil (CEF) as has been described elsewhere. Loco-regional radiotherapy was given according to guidelines at the participating centres. The use of endocrine therapy was avoided. Participants were randomised to either oral pamidronate 150 mg twice daily for 4 years (N=460) or standard care (N=493).
Participants were recruited between January 1990 and January 1996. Follow-up occurred every 12 weeks for the first year. Subsequently the interval was increased to every six months for the next four years and follow-up occurred annually thereafter. The women in the two study arms had similar baseline characteristics.
3.2.4 Risedronate
Hines 2009a
Eligible subjects were premenopausal women scheduled to undergo adjuvant or neo-adjuvant chemotherapy for primary breast cancer (stages I to IIIb)25. Premenopausal status was defined as ≤ 6 months since last menstrual period, no prior bilateral oophorectomy, and no treatment with menopausal oestrogen therapy. If a total abdominal hysterectomy had been performed, with at least one intact ovary, or if more than 3 months since the last menstrual period had lapsed, then patients must have had documented premenopausal oestrogen levels (≤ 1 month before study entry). Women must have been at least 18 years of age, with an Eastern Cooperative Oncology Group (ECOG) performance status of 0 or 1.
Participants were assigned to take calcium 600 mg with 400 IU of vitamin D per day and were randomly assigned to oral risedronate 35 mg (N=108) or placebo (N=108), weekly for 1 year, beginning within 1 month of the start of chemotherapy. The use of ancillary treatments, as appropriate for symptom control and cancer therapy management, was allowed, except for use of bisphosphonates, oestrogen, or selective oestrogen receptor modulators other than tamoxifen.
The trial was powered to detect a difference in LS BMD. Participants were recruited between March 2003 and March 2006. Follow-up occurred after 1 year. The women in the two study arms (risedronate and placebo) had similar baseline characteristics.
Risedronate’s Effect on Bone loss in Breast Cancer (REBBeCa) Study
Eligible participants were women with breast cancer who were newly postmenopausal (up to 8 years) after being treated with chemotherapy with or without tamoxifen or aromatase inhibitors26. Women were excluded if they had stage IV breast cancer (presence of distant metastases), a history of illness known to affect bone and mineral metabolism, malignancy, hyperparathyroidism, and malabsorption. Women were allowed to begin or continue with tamoxifen or an aromatase inhibitor if prescribed by their physician. Participants who had been
28 Systematic review of bisphosphonates in early breast cancer
treated with other medications known to affect bone and mineral metabolism were excluded. The treatment groups were well matched with regard to demographic and baseline disease characteristics.
All participants had an assessment of their dietary calcium intake using a validated questionnaire, and those with daily calcium intake less than 1200 mg received supplementary calcium. Participants were randomly assigned to either oral risedronate (N=43), 35 mg once weekly, or placebo (N=44).
The study was powered to detect a difference in LS BMD. Participants were followed-up at 12 and 24 months.
Study of Anastrozole with the Bisphosphonate Risedronate (SABRE) Study
Eligible subjects were postmenopausal women with breast cancer scheduled to receive anastrozole30. Exclusion criteria included metastatic disease, recent hormonal treatment, and medications known to alter BMD.
Patients were allocated to one of three groups on the basis of their risks of fracture (ie, higher, moderate, or lower risk). Patients were deemed to be at a higher risk if their T-score was less than -2.0 in either the LS or hip or if they had a personal history of fragility fracture. The higher-risk group was an open-label, non-comparative group, in which patients received oral anastrozole 1 mg/d with risedronate sodium 35 mg/wk. Patients with a T-score of -1.0 or greater in either LS or total hip (TH), and with no history of fragility fracture, were classified as lower risk. The lower-risk group was open-label and non-comparative, and patients received anastrozole 1 mg/d. Patients with a T-score less than -1.0 but greater than or equal to -2.0 at either the LS or TH and with no history of fragility fracture could enter either the higher- or moderate-risk stratum. The decision to enter into the higher-risk stratum was based on T-score combined with clinical criteria associated with an increased risk of fracture: advanced age, early menopause (age < 45 years), low body weight (< 127 lbs or 58 kg), current smoking, and history of fragility fracture in a first-degree relative. Patients stratified to the moderate-risk group were randomly assigned in a double-blind manner to either anastrozole or risedronate (N=77) or anastrozole and matching placebo for risedronate (N=77) and therefore are the subject of the RCT.
Study medications were given for two years. All women were counselled on calcium and vitamin D intake and were provided with combination tablets of elemental calcium (500 mg) and vitamin D (200 IU) to be used twice daily as food supplements.
The trial was powered to detect a change in LS BMD. Follow-up occurred at 12 and 24 months. Women in the two study arms (risedronate and placebo) had similar baseline characteristics.
3.2.5 Zoledronic acid
ABCSG-12
Premenopausal women who had undergone primary surgery for stage I or II oestrogen receptor-positive breast cancer, progesterone receptor-positive breast cancer, or both, who had fewer than 10 positive lymph nodes, and who were scheduled to receive standard therapy with goserelin were eligible for enrolment31. Exclusion criteria were T1a (except yT1a), T4d, and yT4 tumours; a history of other neoplasms; preoperative radiotherapy; pregnancy, lactation, or both;

Systematic review of bisphosphonates in early breast cancer 29
and contraindications for study medications. Preoperative chemotherapy was allowed, but none of the patients received adjuvant chemotherapy.
Patients were randomly assigned to receive goserelin (3.6 mg given subcutaneously every 28 days) plus either tamoxifen (20 mg per day given orally) or anastrozole (1 mg per day given orally), with or without zoledronic acid (initially 8 mg given intravenously every 4 weeks) for three years. Protocol amendments were made after 254 patients had been enrolled; the dose of zoledronic acid was reduced to 4 mg every 6 months and the infusion time was increased to 15 minutes.
The trial was powered to detect a difference in disease-free survival. Subjects were recruited between 1999 and 2006. The treatment groups were well matched with regard to demographic and baseline disease characteristics.
Of the 1803 patients randomly assigned to the four treatment groups, 404 were prospectively included in the BMD sub-study32. The patient demographics and baseline characteristics were similar between the treatment groups, and were representative of patients enrolled in the main trial at the same trial centres.
Hershman 2010
Eligible subjects were newly diagnosed premenopausal women with histologically proven, non-metastatic breast cancer37. Premenopausal status was defined as last menstruation ≤ 6 months earlier or follicle-stimulating hormone less than 20 mU/L. Patients were enrolled after surgery but before initiating chemotherapy. The chemotherapeutic regimens were not dictated by study investigators. Exclusion criteria included T-score of less than -2.0 at any site, fragility fracture, prior therapy with a bisphosphonate or calcitonin, LS anatomy precluding accurate BMD measurement of three or more lumbar vertebrae, serum creatinine of 2 mg/dL or greater, or pregnancy.
Patients were randomly allocated to either zoledronic acid 4 mg IV over 15 minutes every 3 months (n=57) for 12 months or placebo (n=57). The trial was powered to detect a change in LS BMD. Hershman 2008 reports the follow-up results at 6 and 12 months. Hershman 2010 reports the follow-up at 24 months (1 year after discontinuation). Women in the intervention and control groups had similar baseline characteristics.
Of 103 patients who completed the baseline evaluation, 85 completed all evaluations through the 12-month visit. For the 24-month visit, 62 completed serum assessments and 57 completed both serum and BMD assessments. The majority of the remaining 23 patients (n=18) had the 24-month BMD performed more than 30 months after randomisation and were therefore not included 24-month follow-up analysis (Hershman 2010). Other reasons for discontinuation included disease progression (n=3) and loss to follow-up (n=2).
Hines 2009b
Eligible subjects were postmenopausal women with a history of stage I-IIIa, oestrogen and/or progesterone receptor-positive breast cancer who had completed 6 or fewer years of tamoxifen, and had no evidence of recurrent or metastatic disease34. Postmenopausal status was defined as women older than 55 years with cessation of menses; women 55 years old or younger with spontaneous menses for less than 1 year but with postmenopausal oestradiol levels were also

30 Systematic review of bisphosphonates in early breast cancer
eligible. Patients must have had a life expectancy of 5 years or greater, and must have had an ECOG performance score of 0 to 2. Laboratory studies obtained within 30 days before randomisation must have included a white blood cell count of ≥ 3000 (3.0 x 109/L) or granulocyte count of ≥ 1500 (1.5 x 109/L), platelet count of at least 100,000 (100 x 109/L), alkaline phosphatase no more than three times the upper limit of normal, aspirate aminotransferase no more than three times the upper limit of normal, and creatinine of < 2.0 mg/dL. Oral bisphosphonates must have been discontinued more than 3 weeks before randomisation.
All patients were assigned to take letrozole 2.5 mg daily, vitamin D 400 IU daily, and calcium 500 mg twice daily. Patients were randomised (open-label) to receive zoledronic acid upfront (N=279) versus zoledronic acid being delayed (N=279) until either a post-baseline T-score of < -2.0 at either the LS or femoral neck (FN) was obtained, a clinical fracture unrelated to trauma was found, or an asymptomatic fracture was discovered. All doses of zoledronic acid were provided IV over 15 minutes at a dosage of 4 mg. Doses were given every six months for 5 years or until breast cancer recurrence. The dosage of zoledronic acid was adjusted for creatinine clearance less than 60 mL/min, such that patients with a creatinine clearance of 50-60 mL/min received 3.5 mg zoledronic acid, those with a creatinine clearance of 4-49 mL/min received 3.3 mg zoledronic acid and those with a creatinine clearance of 30-39 received 3.0 mg zoledronic acid. Patients were to receive letrozole for five years or until breast cancer recurrence. The use of ancillary treatments including short-term corticosteroids was allowed, except for treatments that would be expected to affect osteoclast activity, additional anticancer therapy, other bisphosphonates (other than the study medication), calcitonin, sodium fluoride, parathyroid hormone, tibolone, or any investigational drug or device (excluding study medications).
The trial was powered to detect a change in LS BMD. Subjects were recruited between 2005 and 2006. Follow-up occurred after two years. Women in the upfront and delayed groups had similar baseline characteristics.
A total of 558 patients were enrolled. There were seven cancellations, five in the upfront arm and two on the delayed arm. About 120 patients went off study for reasons which included patient refusal, adverse events, disease progression, and death. Of these, 34 provided BMD data at baseline and 1 year. One patient on the upfront arm did not provide usable BMD data. This left 395 patients with data available for the primary analysis (one-year change in BMD at the LS). A total of 310 provided BMD data at 2 years.
During the first year, 19 patients in the delayed arm started zoledronic acid while 32 started zoledronic acid within the first 2 years.
Z-FAST
Eligible subjects were postmenopausal women who had a history of surgically resectable stage I, II, or IIIa, oestrogen receptor-positive and/or progesterone receptor-positive breast cancer; a baseline ECOG performance status of ≤ -2.013. All subjects underwent tumour resection, completed chemotherapy and/or radiation therapy within 12 weeks of study entry, and had no evidence of residual disease.
Patients received letrozole 2.5 mg orally daily for 5 years or until disease progression and were randomised to upfront or delayed zoledronic acid 4 mg IV over 15 minutes every 6 months for 5 years. The upfront group (N=301) received zoledronic acid after random assignment, whereas the delayed group (N=301) received zoledronic acid when either post-baseline LS or TH T-score decreased to less than -2.0 or a non-traumatic clinical fracture occurred.

Systematic review of bisphosphonates in early breast cancer 31
The trial was powered to detect a change in LS BMD. Subjects were recruited between 2002 and 2003. Follow-up occurred after 36 months. Women in the upfront and delayed groups had similar baseline characteristics.
Twenty-nine (9.7%), 42 (14%), and 62 (20.7%) patients in the delayed group received zoledronic acid therapy by 6 months, 12 months, and 36 months respectively. Of these, 45 received zoledronic acid per protocol (LS T-score < –2.0, n=27; TH T-score < –2.0, n=15; clinical fracture unrelated to trauma, n=3). Seventeen patients received zoledronic acid because of administration errors (patients started zoledronic acid without meeting protocol criteria), 16 of which occurred before month 6 and the other between months 12 and 24; these patients were included in all analyses. Six additional patients met the protocol criteria (LS T-score < –2.0, n=5; TH T-score < –2.0, n=1) but did not initiate zoledronic acid at the appropriate time.
ZO-FAST
Eligible subjects were postmenopausal women who had oestrogen receptor-positive early breast cancer and baseline LS and TH T-scores above -2.014.
Patients received letrozole 2.5 mg orally daily for 5 years or until disease progression and were randomised to upfront or delayed zoledronic acid 4 mg IV over 15 minutes every 6 months for 5 years. The upfront group (N=532) received zoledronic acid after random assignment, whereas the delayed group (N=533) received zoledronic acid when a) post-baseline LS or TH T-score decreased to less than -2.0; b) a non-traumatic clinical fracture occurred; or 3) asymptomatic fracture was discovered at the month-36 scheduled visit. Patients were instructed to take an oral calcium supplement (500 mg) and a multivitamin tablet containing vitamin D (400 IU to 800 IU) daily during the study.
The trial was powered to detect a change in LS BMD. Subjects were recruited between 2002 and 2004.
Of the 1065 randomised patients, one patient did not undergo the post-baseline assessment because she withdrew consent. Women in the upfront and delayed groups had similar baseline characteristics. In the delayed arm, 75 patients had started zoledronic acid by the time of the 12-month analysis. Of these, 54 were started based on the lumbar or hip BMD T-score falling to less than -2, and one patient had experienced a non-traumatic clinical fracture. Twenty patients were started because of misunderstanding of the protocol at the site level38.
32 Systematic review of bisphosphonates in early breast cancer
4 Results of included studies
4.1 Disease-free survival, recurrence-free survival, and survival without bone metastasis
Two included studies reported either disease-free survival, recurrence-free survival, or survival without bone metastasis (Table 11). One study assessed the impact of pamidronate and the other assessed zoledronic acid.
Disease-free survival was defined as the time from randomisation to the first occurrence of one or more of the following: a local or regional recurrence, cancer in the contralateral breast, distant metastasis, second primary carcinoma, or death from any cause. Recurrence-free survival and survival without bone metastasis were defined as the time from randomisation to the first occurrence of local or regional recurrence and bone metastasis respectively.
4.1.1 Pamidronate
Participants in the Kristensen 200824 trial were randomised to 150 mg oral pamidronate twice daily for 4 years or standard care. All participants received chemotherapy (either CMF or CEF). Kristensen 200824 reported survival without bone metastasis rather than disease-free survival or recurrence-free survival. In the multivariable model the hazard rate ratio for recurrence in bone in the pamidronate group compared to standard care was not significant (HR [95% CI] 1.03 [0.75, 1.40]; P=0.86).
4.1.2 Zoledronic acid
In ABCSG-1231, participants were randomised to goserelin (3.6 mg s.c. every 28 days) plus either tamoxifen (20 mg/day) or anastrozole (1 mg/day), with or without zoledronic acid (initially 8 mg IV every 4 weeks*). The women who received treatment regimens with zoledronic acid had a significantly longer disease-free survival (HR [95% CI]: 0.64 [0.46, 0.91]) and recurrence-free survival (HR [95% CI]: 0.65 [0.46, 0.92]), compared with women who received the treatment regimens that did not include zoledronic acid. Zoledronic acid did not have a significant impact on survival free of bone metastasis (HR [95% CI]: 0.68 [0.36, 1.27]).
Sensitivity analyses that excluded patients in the BMD sub-study revealed hazard ratios for disease progression that were similar to those in the intention-to-treat population for zoledronic acid compared with no zoledronic acid (HR [95% CI] 0.70 [0.46, 1.06]). Similarly, the results for patients who received only 4 mg of zoledronic acid and those in the per-protocol population were consistent with the intention-to-treat analyses.
* Protocol amendments, after 254 patients had been enrolled, reduced the dose of zoledronic acid to 4 mg every 6 months and increased the infusion time to 15 minutes.

Systematic review of bisphosphonates in early breast cancer 33
4.1.3 Conclusion
Zoledronic acid appears to improve disease-free survival and recurrence-free survival in premenopausal women receiving adjuvant endocrine therapy for hormone-responsive breast cancer. Pamidronate had no significant impact on survival without bone metastasis.
Table 11 Disease-free survival, recurrence-free survival, and survival free of bone metastasis
Study ID Quality N
Comparison (intervention vs control) Outcome Intervention Comparator
Statistical significance
Pamidronate
Kristensen 200824 Fair
953 150 mg oral pamidronate twice daily for 4 years vs standard care
HR for recurrence in the bone
NA NA HR (95% CI): 1.03 (0.75, 1.40); P=0.86
Zoledronic acid
ABCSG-1231 Fair
1803
GTZ/GAZ vs GT/GA
Disease-free survival
NR NR HR (95% CI): 0.64 (0.46, 0.91); favouring zoledronic acida
P=0.01 (Wald test) P=0.01 (log-rank test)
Recurrence-free survival
NR NR HR (95% CI): 0.65 (0.46, 0.92); favouring zoledronic acida P=0.02 (Wald test) P=0.01 (log-rank test)
Survival free of bone metastasis
NR NR 32% risk reduction HR (95% CI): 0.68 (0.36, 1.27); non-significantly favouring zoledronic acid P=0.22
Abbreviations: CI, confidence interval; GA, goserelin (3.6 mg s.c. every 28 days) plus anastrozole (1 mg/day orally); GAZ, goserelin (3.6 mg s.c. every 28 days) plus anastrozole (1 mg/day orally) plus zoledronic acid (initially 8 mg IV every 4 weeks); GT, goserelin (3.6 mg s.c. every 28 days) plus tamoxifen (20 mg/day orally); GTZ, goserelin (3.6 mg s.c. every 28 days) plus tamoxifen (20 mg/day orally) plus zoledronic acid (initially 8 mg IV every 4 weeks); HR, hazard ratio; NA, not applicable; NR, not reported a Compared with the use of endocrine therapy alone (ie, GT/GA).

34 Systematic review of bisphosphonates in early breast cancer
4.2 Mortality and overall survival
Five of the included studies reported mortality or overall survival (Table 12). The studies assessed the impact of clodronate, pamidronate, risedronate, and zoledronic acid.
4.2.1 Clodronate
Participants in the Diel 2008 trial12 were randomised to 1600 mg/day oral clodronate for 2 years or standard care. The participants who received clodronate had a significantly lower mortality compared with control at median 36-month follow-up (3.8% vs 15.2%; P=0.001), median 55-month follow-up (8.3% vs 22.1%; P<0.002), and median 8.5-year follow-up (20.4% vs 40.7%; P=0.049).
4.2.2 Pamidronate
Participants in the Kristensen 200824 trial were randomised to 150 mg oral pamidronate twice daily for 4 years or standard care. All participants received chemotherapy (either CMF or CEF). No significant difference in overall survival was found between the treatment groups.
4.2.3 Risedronate
Participants in the SABRE trial30 were randomised to receive either 35 mg/week risedronate and anastrozole or placebo. At two-year follow-up, there were no deaths in either study arm.
4.2.4 Zoledronic acid
In ABCSG-1231, participants were randomised to goserelin (3.6 mg s.c. every 28 days) plus either tamoxifen (20 mg/day) or anastrozole (1 mg/day), with or without zoledronic acid (initially 8 mg IV every 4 weeks*). The use of zoledronic acid did not have a significant impact on overall survival (HR [95% CI] 0.60 [0.32, 1.11]), overall mortality (1.8% vs 2.9%; RR [95% CI] 0.62 [0.33, 1.15]), or mortality without previous recurrence (0.0% vs 0.2%: RR [95% CI] 0.20 [0.01, 4.18]) compared with treatment without zoledronic acid.
Consistent with the results of the ABCSG-12 trial, the ZO-FAST14 study found no significant difference in mortality between participants randomly assigned to receive upfront versus delayed† zoledronic acid (0.8% vs 0.9%; RR [95% CI] 0.80 [0.22, 2.97]).
4.2.5 Meta-analysis of results
Figure 1 and Figure 2 present meta-analyses for the effect of bisphosphonates on mortality in early breast cancer using the results from the Pavlakis 20052 systematic review and the subsequently published RCTs.
* Protocol amendments, after 254 patients had been enrolled, reduced the dose of zoledronic acid to 4 mg every 6 months and increased the infusion time to 15 minutes. † The upfront group received zoledronic acid immediately after random assignment. The delayed group received zoledronic acid when either post-baseline LS or TH T-score decreased to less than -2.0 or a non-traumatic clinical fracture occurred.

Systematic review of bisphosphonates in early breast cancer 35
Figure 1 presents an analysis of the impact of bisphosphonates by menopausal status. Overall, there was no significant difference between treatment arms for patients treated with bisphosphonates compared with control (RR [95% CI] 0.75 [0.51, 1.10]). There was no significant difference between treatment arms for studies specifically in premenopausal women receiving adjuvant endocrine therapy (RR [95% CI] 0.62 [0.33, 1.15]), or in the studies where both pre- and post-menopausal women were enrolled (RR [95% CI] 0.78 [0.50, 1.23]).
Figure 2 presents an analysis of the impact of bisphosphonates on mortality by bisphosphonate type. There was no significant difference between treatment arms for the studies evaluating zoledronic acid (RR [95% CI]: 0.62 [0.33, 1.15]) or clodronate (RR [95% CI] 0.78 [0.50, 1.23]).
A potential source of heterogeneity in this meta-analysis is the differences in length of follow-up in the included trials. Diel 2008,12 ABCSG-1231 and SABRE30 had lengths of follow-up of 8.5 years, 4 years and 2 years respectively. Powles 200235 and Saarto 200119 both had a 5-year follow-up.
Figure 1 Meta-analysis of mortality by menopausal status
Study or Subgroup1.1.2 Premenopausal women
ABCSG-12Subtotal (95% CI)
Total eventsHeterogeneity: Not applicableTest for overall effect: Z = 1.53 (P = 0.13)
1.1.3 Pre- and post-menopausal women
Diel 2008Powles 2002Saarto 2001Subtotal (95% CI)
Total eventsHeterogeneity: Tau² = 0.13; Chi² = 14.66, df = 2 (P = 0.0007); I² = 86%Test for overall effect: Z = 1.06 (P = 0.29)
1.1.4 Postmenopausal women
SABRESubtotal (95% CI)
Total eventsHeterogeneity: Not applicableTest for overall effect: Not applicable
Total (95% CI)
Total eventsHeterogeneity: Tau² = 0.12; Chi² = 15.50, df = 3 (P = 0.001); I² = 81%Test for overall effect: Z = 1.45 (P = 0.15)
Events
16
16
329864
194
0
0
210
Total
899899
157530139826
7777
1802
Events
26
26
5912955
243
0
0
269
Total
904904
145539143827
7777
1808
Weight
17.7%17.7%
25.2%29.1%28.0%82.3%
100.0%
M-H, Random, 95% CI
0.62 [0.33, 1.15]0.62 [0.33, 1.15]
0.50 [0.35, 0.72]0.77 [0.61, 0.98]1.20 [0.91, 1.58]0.78 [0.50, 1.23]
Not estimableNot estimable
0.75 [0.51, 1.10]
Bisphosphonates Control Risk Ratio Risk RatioM-H, Random, 95% CI
0.2 0.5 1 2 5Favours bisphosphonates Favours control
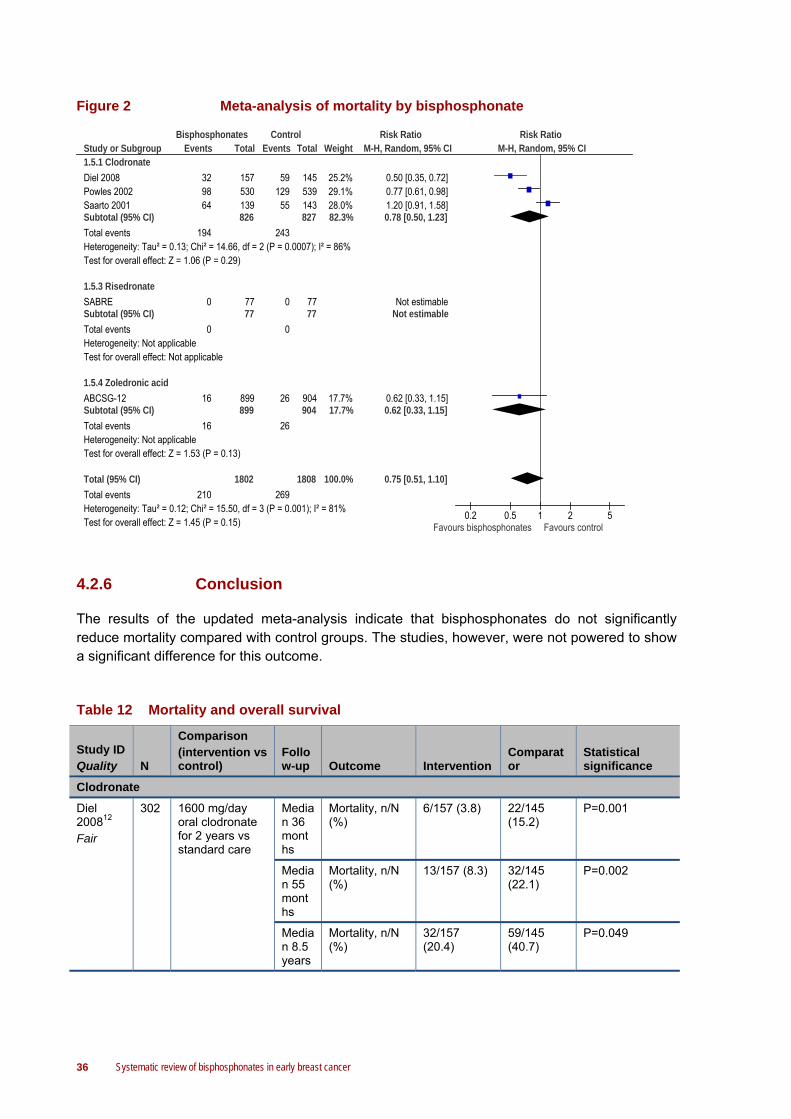
36 Systematic review of bisphosphonates in early breast cancer
Figure 2 Meta-analysis of mortality by bisphosphonate
Study or Subgroup1.5.1 Clodronate
Diel 2008Powles 2002Saarto 2001Subtotal (95% CI)
Total eventsHeterogeneity: Tau² = 0.13; Chi² = 14.66, df = 2 (P = 0.0007); I² = 86%Test for overall effect: Z = 1.06 (P = 0.29)
1.5.3 Risedronate
SABRESubtotal (95% CI)
Total eventsHeterogeneity: Not applicableTest for overall effect: Not applicable
1.5.4 Zoledronic acid
ABCSG-12Subtotal (95% CI)
Total eventsHeterogeneity: Not applicableTest for overall effect: Z = 1.53 (P = 0.13)
Total (95% CI)
Total eventsHeterogeneity: Tau² = 0.12; Chi² = 15.50, df = 3 (P = 0.001); I² = 81%Test for overall effect: Z = 1.45 (P = 0.15)
Events
329864
194
0
0
16
16
210
Total
157530139826
7777
899899
1802
Events
5912955
243
0
0
26
26
269
Total
145539143827
7777
904904
1808
Weight
25.2%29.1%28.0%82.3%
17.7%17.7%
100.0%
M-H, Random, 95% CI
0.50 [0.35, 0.72]0.77 [0.61, 0.98]1.20 [0.91, 1.58]0.78 [0.50, 1.23]
Not estimableNot estimable
0.62 [0.33, 1.15]0.62 [0.33, 1.15]
0.75 [0.51, 1.10]
Bisphosphonates Control Risk Ratio Risk RatioM-H, Random, 95% CI
0.2 0.5 1 2 5Favours bisphosphonates Favours control
4.2.6 Conclusion
The results of the updated meta-analysis indicate that bisphosphonates do not significantly reduce mortality compared with control groups. The studies, however, were not powered to show a significant difference for this outcome.
Table 12 Mortality and overall survival
Study ID Quality N
Comparison (intervention vs control)
Follow-up Outcome Intervention
Comparator
Statistical significance
Clodronate
Diel 200812 Fair
302 1600 mg/day oral clodronate for 2 years vs standard care
Median 36 months
Mortality, n/N (%)
6/157 (3.8) 22/145 (15.2)
P=0.001
Median 55 months
Mortality, n/N (%)
13/157 (8.3) 32/145 (22.1)
P=0.002
Median 8.5 years
Mortality, n/N (%)
32/157 (20.4)
59/145 (40.7)
P=0.049

Systematic review of bisphosphonates in early breast cancer 37
Study ID Quality N
Comparison (intervention vs control)
Follow-up Outcome Intervention
Comparator
Statistical significance
Pamidronate
Kristensen 200824 Fair
953 150 mg oral pamidronate twice daily for 4 years vs standard care
10 years
Overall survival
NR NR No significant differences between the treatment groups were found
Risedronate
SABRE3
0 Good
154 35 mg/week risedronate vs placebo
2 years
Mortality, n/N (%)
0/77 (0.0) 0/77 (0.0) NA
Zoledronic acid
ABCSG-1231 Fair
1803
GTZ/GAZ vs GT/GA
Median 47.8 months
Overall survival
NR NR HR (95% CI) for death: 0.60 (0.32, 1.11); non-significantly favouring zoledronic acida P=0.11 (Wald test) P=0.10 (log-rank test)
Mortality, n/N (%)
16/899 (1.8) 26/904 (2.9)
RR (95% CI): 0.62 (0.33, 1.15); P>0.05b
Mortality (without previous recurrence), n/N (%)
0/899 (0.0) 2/904 (0.2) RR (95% CI): 0.20 (0.01, 4.18); P>0.05b
ZO-FAST 14 Fair
1065
Upfront vs delayed zoledronic acid 4 mg IV over 15 minutes every 6 months.
1 year
Mortality, n/N (%)
4/532 (0.8) 5/533 (0.9) RR (95% CI): 0.80 (0.22, 2.97); P>0.05b
Abbreviations: CI, confidence interval; GA, goserelin (3.6 mg s.c. every 28 days) plus anastrozole (1 mg/day orally); GAZ, goserelin (3.6 mg s.c. every 28 days) plus anastrozole (1 mg/day orally) plus zoledronic acid (initially 8 mg IV every 4 weeks); GT, goserelin (3.6 mg s.c. every 28 days) plus tamoxifen (20 mg/day orally); GTZ, goserelin (3.6 mg s.c. every 28 days) plus tamoxifen (20 mg/day orally) plus zoledronic acid (initially 8 mg IV every 4 weeks); HR, hazard ratio; IV, intravenous; NA, not applicable; NR, not reported; LS, lumbar spine; RR, risk ratio a Compared with the use of endocrine therapy alone (ie, GT/GA). b Calculated for this technical report using Review Manager 5.
4.3 Adverse events
Ten of the included studies reported the incidence of adverse events. One study assessed the impact of ibandronate, one study assessed pamidronate, three studies assessed risedronate, and the other five studies assessed zoledronic acid. Table 13 summarises the clinically relevant adverse outcomes. An adverse outcome was considered clinically relevant if the outcome causes substantial morbidity or if there was a statistically significant difference in incidence between treatment arms.

38 Systematic review of bisphosphonates in early breast cancer
4.3.1 Ibandronate
The women in the ARIBON23 trial were randomised to receive either 150 mg ibandronate every 28 days or placebo. Participants were postmenopausal women with osteopenia who all received adjuvant 1mg/day anastrozole during the study period. Ibandronate did not have a significant effect on adverse events, including joint pains and upper gastrointestinal tract symptoms. There were no cases of osteonecrosis of the jaw in either study arm.
4.3.2 Pamidronate
Participants in the Kristensen 200824 trial were randomised to 150 mg oral pamidronate twice daily for 4 years or standard care. All participants received chemotherapy (either CMF or CEF). Neither nausea, vomiting, stomatitis, nor abdominal pain occurred more frequently among pamidronate treated patients than in control patients.
4.3.3 Risedronate
Hines 2009a25, REBBeCa27, and SABRE30 all compared 35 mg/week risedronate with placebo. None of the studies found a higher incidence of adverse events for women treated with risedronate compared with placebo. In Hines 2009a25, treatment with risedronate significantly decreased the incidence of arthralgia (P=0.045) and chest pain (P=0.045) compared with placebo. In the REBBeCa27 and SABRE trials30, there were no significant differences in adverse events between treatment arms. There were no cases of osteonecrosis of the jaw in any of the three studies.
4.3.4 Zoledronic acid
In ABCSG-1231, participants were randomised to goserelin (3.6 mg s.c. every 28 days) plus either tamoxifen (20 mg/day) or anastrozole (1 mg/day), with or without zoledronic acid (initially 8 mg IV every 4 weeks*). The use of zoledronic acid significantly increased incidence of arthralgia (23.9% vs 18.1%; RR [95% CI] 1.32 [1.10, 1.58]), bone pain (35.3% vs 24.6%; RR [95% CI] 1.44 [1.24, 1.66]), cognitive disorder (1.4% vs 0.3%; RR [95% CI] 4.36 [1.25, 15.24]), nausea and vomiting (8.6% vs 6.1%; RR [95% CI] 1.41 [1.01, 1.97]), fever (8.9% vs 2.2%; RR [95% CI] 4.02 [2.49, 6.51]), and tachycardia (2.1% vs 0.8%; RR [95% CI] 2.73 [1.15, 6.46]) compared with treatment without zoledronic acid. Zoledronic acid significantly reduced the incidence of cutaneous reaction (2.2% vs 4.1%; RR [95% CI] 0.54 [0.32, 0.93]). Zoledronic acid did not significantly increase the incidence of serious events for any of these adverse outcomes. There were no confirmed cases of osteonecrosis of the jaw. Three suspected cases of osteonecrosis of the jaw were reported in patients who received zoledronic acid. In all three patients, the diagnosis was ruled out after a detailed review of dental records.
Hershman 201033 compared 4 mg zoledronic acid IV over 15 minutes every 3 months with placebo. Hershman 2010 found no significant difference in adverse events between the study groups except that the women who received zoledronic acid had a significantly higher incidence of eye discomfort compared with those who received placebo (38.6 vs 22.8; RR [95% CI] NR;
* Protocol amendments, after 254 patients had been enrolled, reduced the dose of zoledronic acid to 4 mg every 6 months and increased the infusion time to 15 minutes.

Systematic review of bisphosphonates in early breast cancer 39
P<0.05).
Participants in the Hines 2009b34, Z-FAST38, and ZO-FAST14 trials were randomised to receive either upfront or delayed* zoledronic acid (4 mg IV over 15 minutes every 6 months). In postmenopausal women starting letrozole after tamoxifen (Hines 2009b34), upfront zoledronic acid significantly increased the incidence of fever (6% vs 0%; P=0.0001), maximum grade of creatinine (4% vs 1%; P=0.045), limb oedema (1% vs 0%; P=0.042), fatigue (5% vs 2%; P=0.038), and nausea (11% vs 6%; P=0.048) compared with delayed zoledronic acid. In Z-FAST, women randomised to upfront zoledronic acid had a significantly higher incidence of fever (9.0% vs 2.0%; RR [95% CI] 4.50 [1.89, 10.74]), and bone pain (13.0% vs 6.7%; RR [95% CI] 1.95 [1.17, 3.26]) compared with patients receiving delayed zoledronic acid. In ZO-FAST, 14 upfront zoledronic acid patients had a significantly higher incidence of bone pain (12.2% vs 6.8%; RR [95% CI] 1.81 [1.23, 2.67]), headache (9.6% vs 5.3%; RR [95% CI] 1.82 [1.17, 2.85]), and fever (14.5% vs 0.6%; RR [95% CI] 25.71 [8.17, 80.98]) compared with delayed zoledronic acid patients. On the other hand, the upfront zoledronic acid group had a significantly lower incidence of depression (2.8% vs 5.3%; RR [95% CI] 0.54 [0.29, 0.99]) in the ZO-FAST trial.
Two women in the upfront group of the Z-FAST trial experienced grade 1 or 2 adverse events related to renal dysfunction by month 36. One patient remained in the study and received subsequent zoledronic acid doses without complication; the second patient was discontinued from the study. In ZO-FAST14, only two patients experienced renal impairment, and both cases were unrelated to study medication as neither had started zoledronic acid at the time of the event.
Although osteonecrosis of the jaw was not specifically defined in the protocol for either Z-FAST or ZO-FAST, the study database was searched for adverse events that could capture this type of event. For Z-FAST, the search identified two suspected cases of osteonecrosis of the jaw in the upfront group. These cases were reviewed by an independent adjudication committee; one case was adjudicated as not osteonecrosis of the jaw, and the other was deemed “indeterminate” because of insufficient information. One suspected case of osteonecrosis of the jaw was identified in ZO-FAST. This patient, who had been randomised to the upfront arm, had experienced a delay in dental healing (grade 2) of 60 days duration. The event was suspected to be related to the study medication; however, no action was taken, and the event resolved without study drug interruption.
Brufsky 20087 reported an integrated analysis of the Z-FAST and ZO-FAST trials. Overall, upfront zoledronic acid significantly increased the incidence of bone pain (12.2% vs 5.9%; RR [95% CI] 2.06 [1.48, 2.85]), fever (12.1% vs 1.0%; RR [95% CI] 12.47 [6.11, 25.46]), and headache (9.4% vs 6.1%; RR [95% CI] 1.56 [1.11, 2.19]) compared with delayed zoledronic acid, and significantly decreased the incidence of depression (3.9% vs 6.7%; RR [95% CI] 0.58 [0.38, 0.89]).
4.3.5 Conclusion
Ibandronate and risedronate are well tolerated compared with placebo. Moreover, risedronate use may decrease the incidence of arthralgia and chest pain.
* The upfront group received zoledronic acid immediately after random assignment. The delayed group received zoledronic acid when either post-baseline LS or TH T-score decreased to less than -2.0 or a non-traumatic clinical fracture occurred.

40 Systematic review of bisphosphonates in early breast cancer
Zoledronic acid use in women undergoing adjuvant endocrine therapy for hormone-responsive breast cancer may increase incidence of arthralgia, bone pain, cognitive disorder, nausea and vomiting, peripheral nerve disease, hot flushes, fever, and tachycardia. Zoledronic acid may, on the other hand, reduce the incidence of cutaneous reactions. Some of these adverse events may be a result of the transfusion process rather than zoledronic acid itself.
In women with early hormone receptor-positive breast cancer receiving adjuvant letrozole, upfront zoledronic acid may decrease the incidence of depression and increase the incidence of fever, bone pain, and headache.
No RCTs published after 2007 identified confirmed cases of osteonecrosis of the jaw. The Mauri 200916 systematic review discusses cases of osteonecrosis of the jaw reported in conference abstracts and RCTs published before 2007.
Table 13 Adverse events
Study ID Quality N
Comparison (intervention vs control) Outcome Intervention Comparator
Statistical significance
Ibandronate
ARIBON23 Fair
50 150 mg/28 days ibandronate vs placebo
ONJ, n/N (%) 0/25 (0) 0/25 (0) NA
Pamidronate
Kristensen 200824 Fair
726a
CMF vs CEF vs CMF/pamidronate vs CEF/pamidronate
Severe nausea/vomiting, n (%)
CMF/pamidronate 26 (11) CEF/pamidronate 32 (19)
CMF 30 (11) CEF 44 (22)
NR
Severe abdominal pain, n (%)
CMF/pamidronate 5 (2) CEF/pamidronate 5 (3)
CMF 8 (3) CEF 4 (2)
NR
Severe stomatitis, n (%)
CMF/pamidronate 5 (2) CEF/pamidronate 2 (1)
CMF 6 (2) CEF 7 (4)
NR
Risedronate
Hines 2009a25 Good
212a
35 mg/week risedronate vs placebo
Arthralgia, n/N (%)
Grade 1/2
0/106 (0) 1/106 (1) P=0.045
Grade 3 0/106 (0 3/106 (3)
Grade 4 0/106 (0) 0/106 (0)
Chest pain, n/N (%)
Grade 1/2
0/106 (0) 2/106 (2) P=0.045

Systematic review of bisphosphonates in early breast cancer 41
Study ID Quality N
Comparison (intervention vs control) Outcome Intervention Comparator
Statistical significance
Grade 3 0/106 (0) 2/106 (2)
Grade 4 0/106 (0) 0/106 (0)
REBBeCa 27 Good
87 35 mg/week risedronate vs placebo
AEs “Risedronate was well tolerated with no differences in AE rates between women receiving risedronate and placebo. There were no significant differences in gastrointestinal symptoms or arthralgias.”
SABRE3
0 Good
154 35 mg/week risedronate vs placebo
At least one AE, n/N (%)
70/77 (90.9) 70/77 (90.9) RR (95% CI): 1.00 (0.90, 1.11); P>0.05b
SAE, n/N (%) 8/77 (10.4) 12/77 (15.6) RR (95% CI): 0.67 (0.29, 1.54); P>0.05b
AE leading to permanent treatment discontinuation, n/N (%)
7/77 (9.1) 15/77 (19.5) RR (95% CI): 0.47 (0.20, 1.08); P>0.05b
SAE leading to permanent treatment discontinuation
0/77 (0.0) 2/77 (2.6) RR (95% CI): 0.20
(0.01, 4.10);
P>0.05b
Zoledronic acid
ABCSG-1231 Fair
1803
GTZ/GAZ vs GT/GA
Arthralgia, n/N (%) 215/899 (23.9) 164/904 (18.1)
RR (95% CI): 1.32 (1.10, 1.58); P<0.05b
Bone pain, n/N (%)
317/899 (35.3) 222/904 (24.6)
RR (95% CI): 1.44 (1.24, 1.66); P<0.05b
Cognitive disorder, n/N (%)
13/899 (1.4) 3/904 (0.3) RR (95% CI): 4.36 (1.25, 15.24); P<0.05b
Nausea and vomiting, n/N (%)
77/899 (8.6) 55/904 (6.1) RR (95% CI): 1.41 (1.01, 1.97); P<0.05b
Peripheral nerve disease, n/N (%)
51/899 (5.7) 31/904 (3.4) RR (95% CI): 1.65 (1.07, 2.56); P<0.05b
Hot flushes, n/N (%)
52/899 (5.8) 53/904 (5.9) RR (95% CI):0.99 (0.68, 1.43); P>0.05b
Fever, n/N (%) 80/899 (8.9) 20/904 (2.2) RR (95% CI): 4.02 (2.49, 6.51); P<0.05b
Tachycardia, n/N (%)
19/899 (2.1) 7/904 (0.8) RR (95% CI): 2.73 (1.15, 6.46); P<0.05b
Cutaneous reaction, n/N (%)
20/899 (2.2) 37/904 (4.1) RR (95% CI): 0.54 (0.32, 0.93); P<0.05b
Skin disease, n/N (%)
58/899 (6.5) 39/904 (4.3) RR (95% CI): 1.50 (1.01, 2.22); P<0.05b

42 Systematic review of bisphosphonates in early breast cancer
Study ID Quality N
Comparison (intervention vs control) Outcome Intervention Comparator
Statistical significance
Periodontal disease, n/N (%)
9/899 (1.0) 5/904 (0.5) RR (95% CI): 1.81 (0.61, 5.38); P>0.05b
Periodontal disease (serious event), n/N (%)
2/899 (0.2) 1/904 (0.1) RR (95% CI): 2.01 (0.18, 22.14); P>0.05b
Renal events, n/N (%)
0/899 (0.0) 0/904 (0.0) NA
Hershman 201033 Fair
114 Zoledronic acid 4 mg IV over 15 minutes every 3 months vs placebo
Eye discomfort, n/N (%)
22/57 (38.6) 13/57 (22.8) P<0.05
Renal failure, n/N (%)
0/57 (0.0) 0/57 (0.0) NA
ONJ, n/N (%) 0/57 (0.0) 0/57 (0.0) NA
Hines 2009b34 Fair
541a
Upfront vs delayed zoledronic acid 4 mg IV over 15 minutes every 6 months
Fever, n/N (%) 18/267 (6) 1/274 (0) P=0.0001
Creatinine, n/N (%)
10/267 (4) 3/274 (1) P=0.045
Limb oedema, n/N (%)
4/267 (1) 0/274 (0) P=0.042
Fatigue, n/N (%) 15/267 (5) 6/274 (2) P=0.038
Nausea, n/N (%) 29/267 (11) 17/274 (6) P=0.048
Z-FAST38 Fair
602 Upfront vs delayed zoledronic acid 4 mg IV over 15 minutes every 6 months
Fever, n/N (%) 27/300 (9.0) 6/300 (2.0) RR (95% CI): 4.50 (1.89, 10.74); P<0.05b
Bone pain, n/N (%)
39/300 (13.0) 20/300 (6.7) RR (95% CI): 1.95 (1.17, 3.26); P<0.05b
ZO-FAST 14 Fair
1065
Upfront vs delayed zoledronic acid 4 mg IV over 15 minutes every 6 months
Renal impairment “Only 2 patients experienced renal impairment, and both cases were unrelated to study medication as neither had started zoledronic acid at the time of the event.”
SAEs, n/N (%) 44/532 (8.3) 36/533 (6.8) RR (95% CI): 1.22 (0.80, 1.87); P>0.05b
Withdrawal from study due to adverse events, n/N (%)
28/532 (5.3) 25/533 (4.7) RR (95% CI): 1.12 (0.66, 1.90); P>0.05b
Discontinuation of therapy due to serious adverse events, n/N (%)
8/532 (1.5) 5/533 (1.0) RR (95% CI): 1.60 (0.53, 4.87); P>0.05b
Bone pain, n/N (%)
65/532 (12.2) 36/533 (6.8) RR (95% CI): 1.81 (1.23, 2.67); P<0.05b
Headache, n/N (%)
51/532 (9.6) 28/533 (5.3) RR (95% CI): 1.82 (1.17, 2.85); P<0.05b
Fever, n/N (%) 77/532 (14.5) 3/533 (0.6) RR (95% CI): 25.71 (8.17, 80.98); P<0.05b
Depression, n/N (%)
15/532 (2.8) 28/533 (5.3) RR (95% CI): 0.54 (0.29, 0.99); P<0.05b

Systematic review of bisphosphonates in early breast cancer 43
Study ID Quality N
Comparison (intervention vs control) Outcome Intervention Comparator
Statistical significance
Z-FAST and ZO-FAST7
1667
Upfront vs delayed zoledronic acid 4 mg IV over 15 minutes every 6 months
Bone pain, n/N (%)
101/827 (12.2) 49/825 (5.9) RR (95% CI): 2.06 (1.48, 2.85); P<0.05b
Fever, n/N (%) 100/827 (12.1) 8/825 (1.0) RR (95% CI): 12.47 (6.11, 25.46); P<0.05b
Headache, n/N (%)
78/827 (9.4) 50/825 (6.1) RR (95% CI): 1.56 (1.11, 2.19); P<0.05b
Depression, n/N (%)
32/827 (3.9) 55/825 (6.7) RR (95% CI): 0.58 (0.38, 0.89); P<0.05b
Abbreviations: AE, adverse event; CEF, cyclophosphamide, epirubicin, and 5-fluoracil; CI, confidence interval; CMF, cyclophosphamide, methotrexate, and 5-fluoracil; GA, goserelin (3.6 mg s.c. every 28 days) plus anastrozole (1 mg/day orally); GAZ, goserelin (3.6 mg s.c. every 28 days) plus anastrozole (1 mg/day orally) plus zoledronic acid (initially 8 mg IV every 4 weeks); GT, goserelin (3.6 mg s.c. every 28 days) plus tamoxifen (20 mg/day orally); GTZ, goserelin (3.6 mg s.c. every 28 days) plus tamoxifen (20 mg/day orally) plus zoledronic acid (initially 8 mg IV every 4 weeks); IV, intravenous; NA, not applicable; NR, not reported; ONJ, osteonecrosis of the jaw; RCT, randomised controlled trial; RR, risk ratio; SAE, serious adverse event; UGIT, upper gastrointestinal tract a This represents the safety population rather than the ITT population. b Calculated for this technical report using Review Manager 5.
4.4 Cancer recurrence and metastasis
Seven studies reported on the impact of bisphosphonates on cancer recurrence or metastasis (Table 14). The studies evaluated the impact of clodronate, pamidronate, risedronate, and zoledronic acid.
4.4.1 Clodronate
Participants in the Diel 200812 trial were randomised to 1600 mg/day oral clodronate for 2 years or standard care. At a median follow-up of 36 months, participants randomised to clodronate had a significantly lower incidence of distant metastasis (13.4% vs 29.0%; P<0.001), bone metastasis (7.6% vs 17.2%; P=0.003), and visceral metastasis (8.3% vs 18.6%; P=0.003). By the 8.5-year median follow-up there was no significant difference between treatment arms in distant, bone or visceral metastasis.
4.4.2 Pamidronate
Participants in the Kristensen 200824 trial were randomised to 150 mg oral pamidronate twice daily for 4 years or standard care. All participants received chemotherapy (either CMF or CEF). There was no significant difference between pamidronate and standard care in the incidence of metastases (20.2% vs 17.8%; RR [95% CI] 1.13 [0.87, 1.47]; P=0.35).
4.4.3 Risedronate
In the REBBeCa27 trial, participants were randomised to receive either 35 mg/week risedronate

44 Systematic review of bisphosphonates in early breast cancer
or placebo. There was no significant difference in cancer recurrence rates in the two trials; however, the incidence values have not been reported.
4.4.4 Zoledronic acid
In ABCSG-1231, participants were randomised to goserelin (3.6 mg s.c. every 28 days) plus either tamoxifen (20 mg/day) or anastrozole (1 mg/day), with or without zoledronic acid (initially 8 mg IV every 4 weeks*). The use of a zoledronic acid regimen significantly reduced the incidence of cancer recurrence compared with therapy without zoledronic acid (RR [95% CI] 0.67 [0.48, 0.93]), but did not have a significant effect on the incidence of loco-regional recurrence (1.1% vs 2.2%; RR [95% CI] 0.50 [0.24, 1.07]), distant recurrence (3.2% vs 4.5%; RR [95% CI] 0.71 [0.45, 1.13]), bone metastasis (1.8% vs 2.5%; RR [95% CI] 0.70 [0.37, 1.32]), contralateral breast cancer (0.7% vs 1.1%; RR [95% CI] 0.60 [0.22, 1.65]), or secondary malignant conditions (1.0% vs 1.1%; RR [95% CI] 0.91 [0.37, 2.22]). Hershman 201031 compared 4 mg zoledronic acid IV over 15 minutes every 3 months with placebo. At 52-weeks, there were no cases of cancer recurrence.
Participants in the Z-FAST38 and ZO-FAST14 trials were randomised to receive either upfront or delayed† zoledronic acid (4 mg IV over 15 minutes every 6 months). There was no significant difference in cancer recurrence between study groups in either Z-FAST (3.0% vs 5.3%; P=0.127) or ZO-FAST (4.1% vs 6.9%; P=0.05) at 3-year follow-up. There was no significant difference in distant recurrence between treatment arms in the ZO-FAST trial at 1-year follow-up (2.3% vs 2.1%; P>0.05).
4.4.5 Meta-analysis of results
Figure 3 presents a meta-analysis of the effect of bisphosphonates on cancer recurrence in early breast cancer based on the results of the included RCTs and the results of RCTs published before 2008 (Saarto 200439, Vehmanen 200440, and Delmas 199741), as reported in Mauri 201010. The results from Z-FAST and ZO-FAST were not included in the meta-analysis as the comparator in these trials was delayed treatment rather than placebo or standard care.
There was no significant difference in cancer recurrence for women treated with clodronate (RR [95% CI] 1.12 [0.84, 1.49]), or risedronate (RR [95% CI] 0.32 [0.04, 2.89]) compared with control; but women treated with zoledronic acid had a significantly lower incidence of cancer recurrence compared with control (RR [95% CI] 0.67 [0.48, 0.93]).
* Protocol amendments, after 254 patients had been enrolled, reduced the dose of zoledronic acid to 4 mg every 6 months and increased the infusion time to 15 minutes. † The upfront group received zoledronic acid immediately after random assignment. The delayed group received zoledronic acid when either post-baseline LS or TH T-score decreased to less than -2.0 or a non-traumatic clinical fracture occurred.

Systematic review of bisphosphonates in early breast cancer 45
Figure 3 Meta-analysis of cancer recurrence by bisphosphonate
Study or Subgroup1.4.1 Clodronate
Powles 2006Saarto 2004Vehmanen 2004Subtotal (95% CI)
Total eventsHeterogeneity: Tau² = 0.03; Chi² = 3.32, df = 1 (P = 0.07); I² = 70%Test for overall effect: Z = 0.76 (P = 0.45)
1.4.3 Risedronate
Delmas 1997Subtotal (95% CI)
Total eventsHeterogeneity: Not applicableTest for overall effect: Z = 1.01 (P = 0.31)
1.4.4 Zoledronic acid
ABCSG-12Hershman 2010Subtotal (95% CI)
Total eventsHeterogeneity: Not applicableTest for overall effect: Z = 2.36 (P = 0.02)
Total (95% CI)
Total eventsHeterogeneity: Tau² = 0.07; Chi² = 11.63, df = 3 (P = 0.009); I² = 74%Test for overall effect: Z = 0.36 (P = 0.72)
Events
139760
215
1
1
540
54
270
Total
53013921
690
2727
89957
956
1673
Events
145600
205
3
3
810
81
289
Total
53914324
706
2626
90457
961
1693
Weight
35.5%33.3%
68.8%
2.2%2.2%
29.0%
29.0%
100.0%
M-H, Random, 95% CI
0.97 [0.80, 1.19]1.30 [1.02, 1.67]
Not estimable1.12 [0.84, 1.49]
0.32 [0.04, 2.89]0.32 [0.04, 2.89]
0.67 [0.48, 0.93]Not estimable
0.67 [0.48, 0.93]
0.94 [0.67, 1.31]
Bisphosphonates Control Risk Ratio Risk RatioM-H, Random, 95% CI
0.05 0.2 1 5 20Favours bisphosphonates Favours control
Figure 4 presents a meta-analysis of the effect of bisphosphonates on metastasis based on the results of the included RCTs and the results of previously published RCTs (as reported in Mauri 201010). There was no significant difference in the incidence of metastasis for women treated with clodronate (RR [95% CI] 0.94 [0.79, 1.13]), pamidronate (RR [95% CI] 1.04 [0.66, 1.65]), zoledronic acid (RR [95% CI] 0.71 [0.45, 1.13]), or any bisphosphonate (RR [95% CI] 0.96 [0.82, 1.11]) compared with control.

46 Systematic review of bisphosphonates in early breast cancer
Figure 4 Meta-analysis of metastasis by bisphosphonate
Study or Subgroup1.8.1 Clodronate
Diel 2008Powles 2006Saarto 2004Subtotal (95% CI)
Total eventsHeterogeneity: Tau² = 0.00; Chi² = 1.77, df = 2 (P = 0.41); I² = 0%Test for overall effect: Z = 0.66 (P = 0.51)
1.8.2 Pamidronate
Fuleihan 2005Kristensen 2008Subtotal (95% CI)
Total eventsHeterogeneity: Tau² = 0.00; Chi² = 0.52, df = 1 (P = 0.47); I² = 0%Test for overall effect: Z = 0.81 (P = 0.42)
1.8.3 Zoledronic acid
ABCSG-12Subtotal (95% CI)
Total eventsHeterogeneity: Not applicableTest for overall effect: Z = 1.43 (P = 0.15)
Total (95% CI)
Total eventsHeterogeneity: Tau² = 0.00; Chi² = 5.18, df = 5 (P = 0.39); I² = 4%Test for overall effect: Z = 0.52 (P = 0.60)Test for subgroup differences: Chi² = 2.88, df = 2 (P = 0.24), I² = 30.6%
Events
616344
168
393
96
29
29
293
Total
157530139826
21460481
899899
2206
Events
578042
179
488
92
41
41
312
Total
145539143827
19493512
904904
2243
Weight
24.6%20.8%16.0%61.5%
1.1%28.1%29.2%
9.3%9.3%
100.0%
M-H, Random, 95% CI
0.99 [0.75, 1.31]0.80 [0.59, 1.09]1.08 [0.76, 1.53]0.94 [0.79, 1.13]
0.68 [0.17, 2.65]1.13 [0.87, 1.47]1.11 [0.86, 1.44]
0.71 [0.45, 1.13]0.71 [0.45, 1.13]
0.96 [0.83, 1.11]
Bisphosphonates Control Risk Ratio Risk RatioM-H, Random, 95% CI
0.2 0.5 1 2 5Favours bisphosphonates Favours control
4.4.6 Conclusion
The results of the meta-analysis indicate that zoledronic acid may reduce the incidence of cancer recurrence. Zoledronic acid had no significant impact on the incidence of metastasis. None of the studies found that any of the other bisphosphonates had a significant effect on cancer recurrence or metastasis.
Table 14 Cancer recurrence and metastasis
Study ID Quality N
Comparison (intervention vs control) Outcome Intervention Comparator
Statistical significance
Clodronate
Diel 200812 Fair
302 1600 mg/day oral clodronate for 2 years vs standard care
Incidence of distant metastasis (median 36-month follow-up), n/N (%)
21/157 (13.4)
42/145 (29.0)
P<0.001
Incidence of distant metastasis (median 55-month follow-up), n/N (%)
32/157 (20.4)
51/145 (35.2)
P=0.022
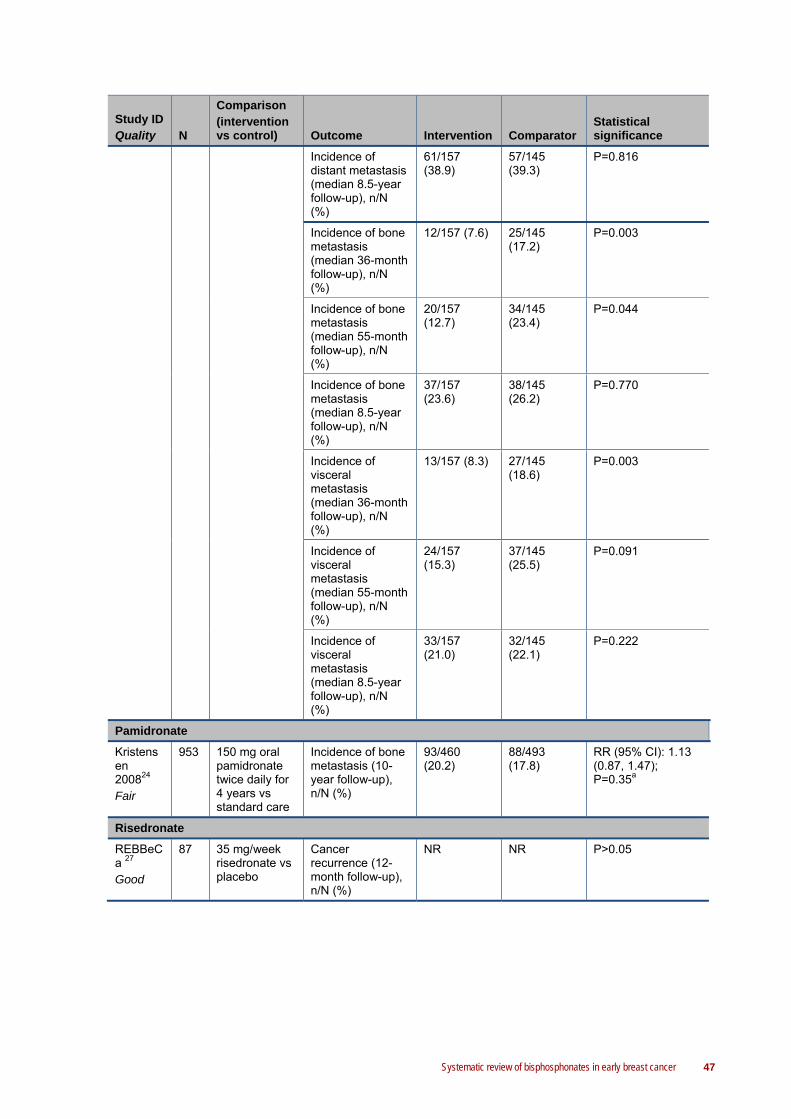
Systematic review of bisphosphonates in early breast cancer 47
Study ID Quality N
Comparison (intervention vs control) Outcome Intervention Comparator
Statistical significance
Incidence of distant metastasis (median 8.5-year follow-up), n/N (%)
61/157 (38.9)
57/145 (39.3)
P=0.816
Incidence of bone metastasis (median 36-month follow-up), n/N (%)
12/157 (7.6) 25/145 (17.2)
P=0.003
Incidence of bone metastasis (median 55-month follow-up), n/N (%)
20/157 (12.7)
34/145 (23.4)
P=0.044
Incidence of bone metastasis (median 8.5-year follow-up), n/N (%)
37/157 (23.6)
38/145 (26.2)
P=0.770
Incidence of visceral metastasis (median 36-month follow-up), n/N (%)
13/157 (8.3) 27/145 (18.6)
P=0.003
Incidence of visceral metastasis (median 55-month follow-up), n/N (%)
24/157 (15.3)
37/145 (25.5)
P=0.091
Incidence of visceral metastasis (median 8.5-year follow-up), n/N (%)
33/157 (21.0)
32/145 (22.1)
P=0.222
Pamidronate
Kristensen 200824 Fair
953 150 mg oral pamidronate twice daily for 4 years vs standard care
Incidence of bone metastasis (10-year follow-up), n/N (%)
93/460 (20.2)
88/493 (17.8)
RR (95% CI): 1.13 (0.87, 1.47); P=0.35a
Risedronate
REBBeCa 27 Good
87 35 mg/week risedronate vs placebo
Cancer recurrence (12-month follow-up), n/N (%)
NR NR P>0.05

48 Systematic review of bisphosphonates in early breast cancer
Study ID Quality N
Comparison (intervention vs control) Outcome Intervention Comparator
Statistical significance
Zoledronic acid
ABCSG-1231 Fair
1803
GTZ/GAZ vs GT/GA
Cancer recurrence (3-year follow-up)b, n/N (%)
54/899 (6.0) 81/904 (8.9) RR (95% CI): 0.67 (0.48, 0.93); P<0.05a
Loco-regional recurrence (3-year follow-up), n/N (%)
10/899 (1.1) 20/904 (2.2) RR (95% CI): 0.50 (0.24, 1.07); P>0.05a
Distant recurrence (3-year follow-up), n/N (%)
29/899 (3.2) 41/904 (4.5) RR (95% CI): 0.71 (0.45, 1.13); P>0.05a
Distant recurrence (bone metastasis; 3-year follow-up), n/N (%)
16/899 (1.8) 23/904 (2.5) RR (95% CI): 0.70 (0.37, 1.32); P>0.05a
Distant recurrence (contralateral breast cancer; 3-year follow-up), n/N (%)
6/899 (0.7) 10/904 (1.1) RR (95% CI): 0.60 (0.22, 1.65); P>0.05a
Secondary malignant condition (3-year follow-up), n/N (%)
9/899 (1.0) 10/904 (1.1) RR (95% CI): 0.91 (0.37, 2.22); P>0.05a
Hershman 201033 Fair
114 Zoledronic acid 4 mg IV over 15 minutes every 3 months vs placebo
Cancer recurrence (24-month follow-up), n/N (%)
0/57 (0.0) 0/57 (0.0) NA
Z-FAST38 Fair
602 Upfront vs delayed zoledronic acid 4 mg IV over 15 minutes every 6 months
Cancer recurrence (36-month follow-up), n/N (%)
9/300 (3.0) 16/300 (5.3) P=0.127
ZO-FAST14,4
2 Fair
1065
Upfront vs delayed zoledronic acid 4 mg IV over 15 minutes every 6 months
Cancer recurrence (36-month follow-up), n/N (%)
22/532 (4.1) 37/533 (6.9) RR (95% CI): 0.60 (0.36, 1.00); P=0.05a
Distant recurrence (12-month follow-up), n/N (%)
12/532 (2.3) 11/533 (2.1) RR (95% CI): 1.09 (0.49, 2.46); P>0.05a
Abbreviations: CEF, cyclophosphamide, epirubicin, and 5-fluoracil; CI, confidence interval; CMF, cyclophosphamide, methotrexate, and 5-fluoracil; GA, goserelin (3.6 mg s.c. every 28 days) plus anastrozole (1 mg/day orally); GAZ, goserelin (3.6 mg s.c. every 28 days) plus anastrozole (1 mg/day orally) plus zoledronic acid (initially 8 mg IV every 4 weeks); GT, goserelin (3.6 mg s.c. every 28 days) plus tamoxifen (20 mg/day orally); GTZ, goserelin (3.6 mg s.c. every 28 days) plus tamoxifen (20 mg/day orally) plus zoledronic acid (initially 8 mg IV every 4 weeks); IV, intravenous; NA, not applicable; NR, not reported; RR, risk ratio a Calculated for this technical report using Review Manager 5. b Calculated by subtracting the incidence of death without previous recurrence from the incidence of all events (including loco-regional recurrence, distant recurrence, secondary malignant condition, or death).

Systematic review of bisphosphonates in early breast cancer 49
4.5 Quality of life
None of the included studies reported quality of life as an outcome.
4.6 Spinal bone mineral density (BMD)
All of the included studies reported spinal BMD as the primary outcome (Table 15); this includes two studies assessing the impact of clodronate, one for ibandronate, one for pamidronate, three studies for risedronate, and five studies for zoledronic acid. In ARIBON and SABRE, the patient population was limited to osteopenic women with breast cancer.
4.6.1 Clodronate
In both McCloskey 201022 and Saarto 200811, the intervention arm received 1600 mg/day clodronate, with placebo as the comparator in McCloskey 2010, and standard care as the comparator in Saarto 2008. McCloskey 201022 found that the use of clodronate resulted in a significant reduction in the loss of LS BMD from baseline at 2 years compared with placebo (mean [95% CI] 0.06% [-0.72, 0.73] vs -1.87% [-2.52, -1.22]; mean difference [95% CI] 1.92% [0.99, 2.86]; P<0.001). This was consistent for premenopausal (mean [SD] -2.54% [0.43] vs -3.95% [0.45]; P=0.004) and postmenopausal women (mean [SD] 2.09% [0.42] vs 0.05% [0.40]; P<0.001), with no significant interaction between menopausal status and the ability of clodronate to prevent bone loss (P>0.05). In the placebo group, the greatest loss of spine BMD occurred during the first year. At 5-year follow-up (ie, 3 years following cessation of therapy), the LS BMD remained greater (mean difference [95% CI] 1.10% [-0.26%, 2.46%]; P=0.11) in women treated with clodronate compared with placebo.
Reports of the Saarto 200811 trial published before 2007 determined that 3-year clodronate therapy significantly reduced LS bone loss compared with standard care. After termination of clodronate therapy, no accelerated bone loss was found. The bone-loss rate did not differ between the groups within the next seven years of follow-up. From 3 to 10 years, the mean change in LS BMD was -5.0% (SD 6.7) in the control group versus -4.1% (SD 7.7) in the clodronate group (P=0.81). The total LS bone loss during the 10-year period was -10.3% (SD 9.6) in the control group, and -5.5% (SD 10.7) in the clodronate group (P=NR).
4.6.2 Ibandronate
The women in the ARIBON23 trial were randomised to receive either 150 mg ibandronate every 28 days or placebo. Participants were postmenopausal women with osteopenia who all received adjuvant 1 mg/day anastrozole during the study period. Ibandronate significantly reduced the loss of LS BMD from baseline to follow-up at 1 year (mean [range] 3.11% [-3.8, 15.1] vs -2.35% [NR]; P<0.001), and 2 years (mean [range] 2.98% [-8.9, 19.9] vs -3.22% [NR]; P<0.001) compared with placebo.
4.6.3 Pamidronate
Participants in the Kristensen 200824 trial were randomised to 150 mg oral pamidronate twice daily for 4 years or standard care. All participants received chemotherapy (either CMF or CEF).

50 Systematic review of bisphosphonates in early breast cancer
The linear mixed models analyses revealed a significant decrease in LS BMD in the control group compared with pamidronate (P=0.0001). Additionally, there was a significant interaction between time and pamidronate treatment in the LS BMD (P=0.0092).
4.6.4 Risedronate
Participants in the Hines 2009a25, REBBeCa27, and SABRE30 trials were randomised to 35 mg/week risedronate or placebo.
Although Hines 2009a25 found that participants randomised to risedronate had a significantly greater LS BMD at 1-year follow-up compared with placebo (mean [95% CI] 1.18 g/cm2 [1.15, 1.22] vs 1.12 g/cm2 [1.09, 1.15]; P=0.008), there was no significant difference in the change in LS BMD from baseline (mean [95% CI] -4.3% [-5.46, -3.22] vs -5.4% [-6.76, -3.98]; P=0.18) and there was no significant difference at 1-year follow-up in the proportion of participants with LS bone loss 5% or greater (31.1% vs 35.8%; RR [95% CI] 0.87 [0.59, 1.27]; P=0.47).
In the REBBeCa27 trial, risedronate did not significantly reduce posteroanterior LS BMD loss (mean [SD] 0.4% [0.8] vs -1.2% [0.7]; P=0.082) compared with placebo; but did significantly reduce lateral LS BMD loss (mean [SD] 0.1% [1.1] vs -2.4% [1.1]; P=0.048).
The SABRE30 trial included only osteopenic women. There was a significant difference between risedronate and placebo in the change from baseline in LS BMD at 1-year follow-up (mean [95% CI] 1.2% [0.22, 2.19] vs -1.2% [-2.19, -0.24]; P<0.001), and 2-year follow-up (mean [95% CI] 2.2% [0.73, 3.76] vs -1.8% [-3.25, -0.25]; P<0.001).
4.6.5 Zoledronic acid
In ABCSG-1232, participants were randomised to goserelin (3.6 mg s.c. every 28 days) plus either tamoxifen (20 mg/day) or anastrozole (1 mg/day), with or without zoledronic acid (initially 8 mg IV every 4 weeks*). There was a significant reduction in LS BMD for the patients randomised to the regimes without zoledronic acid at 1-year (mean [95% CI] -0.077 g/cm3 [-0.104, -0.049]; P<0.001), 3-year (-0.119 g/cm3 [-0.146, -0.091]; P<0.001), and 5-year follow-up (-0.067 g/cm3 [-0.106, -0.027]; P<0.001). Similarly, there was a significant reduction in the LS BMD T-score for these patients at 1-year (-0.7 [-0.9, -0.4]; P<0.001), 3-year (-1.1 [-1.3, -0.8]; P<0.001), and 5-year follow-up (-0.6 [-1.0, -0.2]; P<0.001). For patients randomised to the treatment regimes with zoledronic acid, there was a significant improvement in LS BMD at 5-yearfollow-up (0.039 g/cm3 [0.005, 0.075]; P=0.022), and a non-significant improvement at 1–year (0.015 g/cm3 [-0.011, 0.041]; P=0.260) and 3-year follow-up (0.004 g/cm3 [-0.024, 0.032]). Similarly, the improvement in LS BMD T-score was significant at 5-year follow-up (0.4 [0.0, 0.7]; P=0.030) but not at 1-year follow-up (0.1 [-0.1, 0.4]; P=0.295) or at 3-year follow-up (0.0 [-0.2, 0.3]; P=0.865).
Hershman 201033 compared 4 mg zoledronic acid IV over 15 minutes every 3 months with placebo. Zoledronic acid significantly increased LS BMD compared with placebo at 1-year follow-up (mean [SE] 1.3% [0.58] vs -5.4% [0.55]) and 2-year follow-up (mean [SE] -0.6% [0.84] vs -6.3% [0.83]; P<0.001†). In the placebo group, change in BMD was not correlated with type of
* Protocol amendments, after 254 patients had been enrolled, reduced the dose of zoledronic acid to 4 mg every 6 months and increased the infusion time to 15 minutes. † P value for the comparison of the difference between treatment group means ignoring time.

Systematic review of bisphosphonates in early breast cancer 51
chemotherapy, baseline BMD, hormonal therapy, or permanence of menstrual cessation.
Participants in the Hines 2009b34, Z-FAST38, ZO-FAST14 trials were randomised to receive either upfront or delayed* zoledronic acid (4 mg IV over 15 minutes every 6 months). The study population in Hines 2009b was postmenopausal women with early breast cancer starting letrozole after tamoxifen. Upfront zoledronic acid significantly reduced the loss of LS BMD compared with delayed zoledronic acid at 1-year follow-up (mean [SD] 3.66% [NR] vs -1.66% [NR]; P<0.001), and 2-year follow-up (mean [SD] 4.94% [NR] vs -2.28% [NR]; P<0.001). The proportion of subjects with 5% or greater bone loss at 1-year follow-up was significantly lower in the upfront group compared with the delayed group (2.2% vs 14.7%; P<0.001).
In Z-FAST38, upfront zoledronic acid significantly increased LS BMD compared with delayed zoledronic acid at 1-year follow-up (least squares mean difference [LSMD; 95% CI] 4.3% [3.7, 5]), and 3-year follow-up (LSMD [95% CI] 6.7% [5.6, 7.7]), but not at 2-year follow-up (LSMD [95% CI] 6.0% [5.1, -6.9]). Upfront zoledronic acid was significantly more effective than delayed treatment in preventing BMD loss, regardless of baseline T-score, risk factor frequency, or chemotherapy.
In the ZO-FAST14 trial, upfront zoledronic acid significantly increased LS BMD compared with delayed zoledronic acid at 1-year follow-up (LSMD [95% CI] 5.7% [5.2, 6.1]; P<0.001); this was consistent when the population of interest was restricted to postmenopausal women (mean [95% CI] -0.2% [-1.1, 0.7] vs -5.5% [-6.3, -4.7]; P<0.001). There was a trend toward more rapid bone loss in the recently postmenopausal women versus established postmenopausal women†. This is demonstrated by looking at the delayed arm in the two groups. The losses in BMD are -5.49% in the recently postmenopausal group versus -2.61% in the established postmenopausal group.
Brufsky 20087 reported an integrated analysis of the Z-FAST and ZO-FAST trials. Upfront zoledronic acid significantly increased LS BMD compared with delayed zoledronic acid at 1-year follow-up (LSMD [95% CI] 5.2% [4.8, 5.6]; P<0.0001). Patients with mild-moderate osteopenia (T-score of -1.0 or lower and -2.0 or greater) at baseline receiving upfront zoledronic acid were found to have a greater LS BMD increase compared with patients with normal BMD (T-score more than -1.0) at baseline (2.6% vs 1.8%). Patients in the delayed group with normal baseline BMD experienced a greater decrease in LS BMD (-3.4% vs -2.5%) compared with patients with low baseline BMD. The proportion of patients with a cumulative decrease in LS BMD of at least 8% from baseline to month 12 was lower in patients receiving upfront zoledronic acid than in patients randomised to the delayed group (0.1% vs 9.7%). Furthermore, patients in the delayed group with normal baseline BMD were significantly more likely to have BMD decreases of at least 8% compared with low baseline BMD patients.
4.6.6 Conclusion
Short-term use (up to four years) of clodronate, ibandronate, risedronate, or zoledronic acid significantly reduces the spinal bone loss associated with the treatment of early breast cancer.
* The upfront group received zoledronic acid immediately after random assignment. The delayed group received zoledronic acid when either post-baseline LS or TH T-score decreased to less than -2.0 or a non-traumatic clinical fracture occurred. † The difference between recent and established post-menopause was not defined.
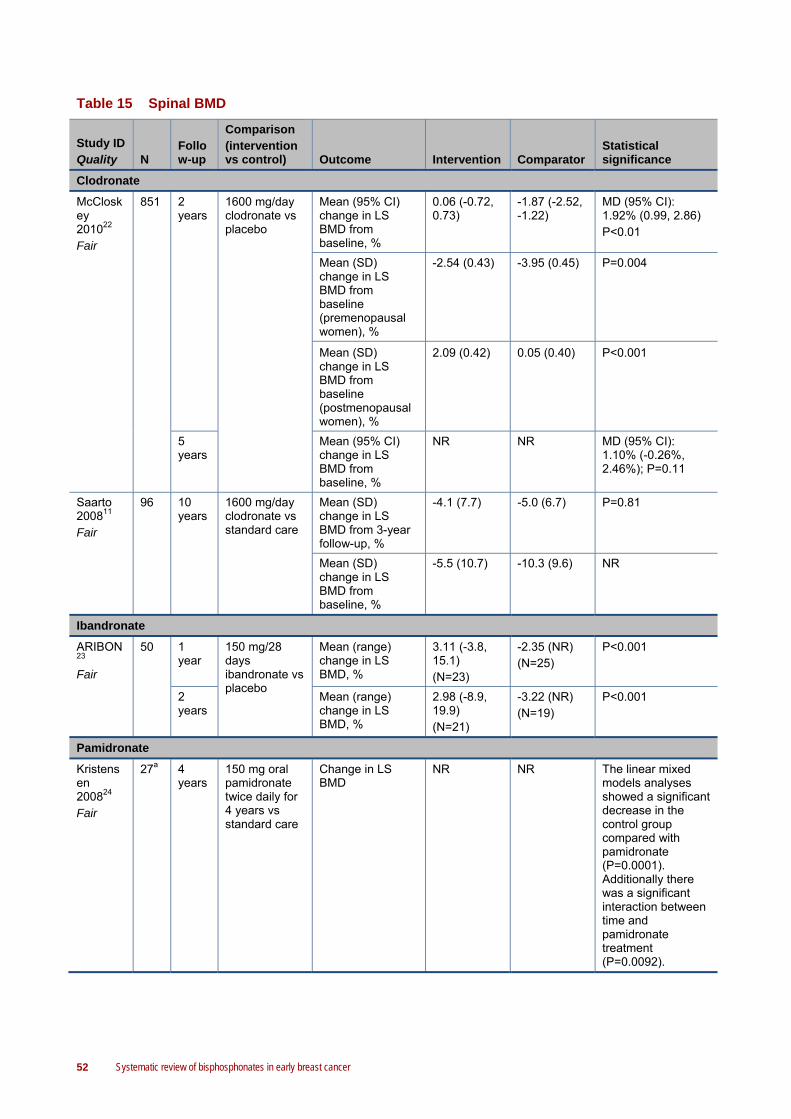
52 Systematic review of bisphosphonates in early breast cancer
Table 15 Spinal BMD
Study ID Quality N
Follow-up
Comparison (intervention vs control) Outcome Intervention Comparator
Statistical significance
Clodronate
McCloskey 201022 Fair
851 2 years
1600 mg/day clodronate vs placebo
Mean (95% CI) change in LS BMD from baseline, %
0.06 (-0.72, 0.73)
-1.87 (-2.52, -1.22)
MD (95% CI): 1.92% (0.99, 2.86) P<0.01
Mean (SD) change in LS BMD from baseline (premenopausal women), %
-2.54 (0.43) -3.95 (0.45) P=0.004
Mean (SD) change in LS BMD from baseline (postmenopausal women), %
2.09 (0.42) 0.05 (0.40) P<0.001
5 years
Mean (95% CI) change in LS BMD from baseline, %
NR NR MD (95% CI): 1.10% (-0.26%, 2.46%); P=0.11
Saarto 200811 Fair
96 10 years
1600 mg/day clodronate vs standard care
Mean (SD) change in LS BMD from 3-year follow-up, %
-4.1 (7.7) -5.0 (6.7) P=0.81
Mean (SD) change in LS BMD from baseline, %
-5.5 (10.7) -10.3 (9.6) NR
Ibandronate
ARIBON23 Fair
50 1 year
150 mg/28 days ibandronate vs placebo
Mean (range) change in LS BMD, %
3.11 (-3.8, 15.1) (N=23)
-2.35 (NR) (N=25)
P<0.001
2 years
Mean (range) change in LS BMD, %
2.98 (-8.9, 19.9) (N=21)
-3.22 (NR) (N=19)
P<0.001
Pamidronate
Kristensen 200824 Fair
27a 4 years
150 mg oral pamidronate twice daily for 4 years vs standard care
Change in LS BMD
NR NR The linear mixed models analyses showed a significant decrease in the control group compared with pamidronate (P=0.0001). Additionally there was a significant interaction between time and pamidronate treatment (P=0.0092).

Systematic review of bisphosphonates in early breast cancer 53
Study ID Quality N
Follow-up
Comparison (intervention vs control) Outcome Intervention Comparator
Statistical significance
Risedronate
Hines 2009a25 Good
212b
1 year
35 mg/week risedronate vs placebo
Mean (95% CI) LS BMD at baseline, g/cm2
1.24 (1.20, 1.27)
1.19 (1.16, 1.22)
P=0.03
Mean (95% CI) LS BMD at follow-up, g/cm2
1.18 (1.15, 1.22)
1.12 (1.09, 1.15)
P=0.008
Mean (95% CI) change in LS BMD from baseline, %
-4.3 (-5.46, -3.22)
-5.4 (-6.76, -3.98)
P=0.18
Proportion with LS bone loss ≥ 5%, n/N (%)
33/106 (31.1)
38/106 (35.8)
RR (95% CI): 0.87 (0.59, 1.27); P=0.47c
REBBeCa 27 Good
87 2 years
35 mg/week risedronate vs placebo
Mean (SD) change in posteroanterior LS BMD from baseline, %
0.4 (0.8); P=0.63
-1.2 (0.7); P=0.088
P=0.082
Mean (SD) change in lateral LS BMD from baseline, %
0.1 (1.1); P=0.951
-2.4 (1.1); P=0.041
P=0.048
Mean (SE) change in posteroanterior LS BMD from baseline (women concurrently treated with AIs), %
-2.4 (1.1); P=0.04
-4.8 (0.8); P<0.001
NR
Mean (SE) change in lateral LS BMD from baseline (women concurrently treated with AIs), %
-3.6 (1.3); P=0.01
-5.2 (1.6); P=0.004
NR
Mean (SE) change in posteroanterior LS BMD from baseline (women not concurrently treated with AIs), %
2.1 (1.2); P=0.09
0.5 (0.9); P=0.57
NR
Mean (SE) change in lateral spine LS BMD from baseline (women not concurrently treated with AIs), %
3.0 (1.8); P=0.12
-1.2 (1.1); P=0.29
NR

54 Systematic review of bisphosphonates in early breast cancer
Study ID Quality N
Follow-up
Comparison (intervention vs control) Outcome Intervention Comparator
Statistical significance
SABRE3
0 Good
154d
1 year
35 mg/week risedronate vs placebo
Mean (95% CI) change from baseline in LS BMD, %
1.2 (0.22, 2.19) (N=73)
-1.2 (-2.19, -0.24) (N=65)
P<0.001
2 years
Mean (95% CI) change from baseline in LS BMD, %
2.2 (0.73, 3.76) (N=60)
-1.8 (-3.25, -0.25) (N=54)
P<0.001
Zoledronic acid
ABCSG-1232 Fair
404e
1 year
GTZ/GAZ vs GT/GA
Mean (95% CI) change in LS BMD from baseline, g/cm3
0.015 (-0.011, 0.041) P=0.260
-0.077 (-0.104, -0.049) P<0.001
NR
Mean (95% CI) change in LS BMD T-scoref from baseline
0.1 (-0.1, 0.4) P=0.295
-0.7 (-0.9, -0.4) P<0.001
NR
3 years
Mean (95% CI) change in LS BMD from baseline, g/cm3
0.004 (-0.024, 0.032) P=0.772
-0.119 (-0.146, -0.091) P<0.0001
NR
Mean (95% CI) change in LS BMD T-scoref from baseline
0.0 (-0.2, 0.3) P=0.865
-1.1 (-1.3, -0.8) P<0.001
NR
5 years
Mean (95% CI) change in LS BMD from baseline, g/cm3
0.039 (0.005, 0.075) P=0.022
-0.067 (-0.106, -0.027) P=0.001
NR
Mean (95% CI) change in LS BMD T-scoref from baseline
0.4 (0.0, 0.7) P=0.030
-0.6 (-1.0, -0.2) P=0.001
NR
Hershman 201033 Fair
114 1 year
Zoledronic acid 4 mg IV over 15 minutes every 3 months vs placebo
Mean (SE) change in LS BMD from baseline at follow-up, %
1.3 (0.58) -5.4 (0.55) P<0.001g
2 years
Mean (SE) change in LS BMD from baseline at follow-up, %
-0.6 (0.84) -6.3 (0.83)
Hines 2009b34 Fair
558 1 year
Upfront vs delayed zoledronic acid 4 mgh IV over 15 minutes every 6 months
Mean (SD) baseline LS BMD, g/cm
1.09 (NR) 1.11 (NR) P=0.35
Mean (SD) LS BMD at follow-up, g/cm
1.13 (NR) 1.09 (NR) P=0.004
Mean (SD) change in LS BMD, g/m
0.04 (NR) -0.02 (NR) P<0.001
Mean (SD) change in LS BMD, %
3.66 (NR) -1.66 (NR) P<0.001

Systematic review of bisphosphonates in early breast cancer 55
Study ID Quality N
Follow-up
Comparison (intervention vs control) Outcome Intervention Comparator
Statistical significance
Proportion with LS bone loss ≥ 5%, n/N (%)
6/279 (2.2) 41/279 (14.7)
P<0.001
2 years
Mean (SD) change in LS BMD, g/m
0.05 (NR) -0.03 P<0.001
Mean (SD) change in LS BMD, %
4.94 (NR) -2.28 (NR) P<0.001
Z-FAST38 Fair
602 1 year
Upfront vs delayed zoledronic acid 4 mg IV over 15 minutes every 6 months
LS BMD, % NR NR LSMD (95% CI): 4.3 (3.7, 5)
2 years
LS BMD, % NR NR LSMD (95% CI): 6.0 (5.1, -6.9)
3 years
LS BMD, % NR NR LSMD (95% CI): 6.7 (5.6, 7.7) Absolute difference: 6.7% (P<0.001)
Change in LS BMD from baseline, %
NR -4.5% (P<0.001) for patients who did not receive zoledronic acid 1.2% (P=0.21) for delayed patients who received zoledronic acid
NR
Mean rate of LS BMD change, g/cm2/year
0.010 -0.005
MD: 0.015 (P<0.0001)
Worsening of BMD by baseline T-score
“Fewer patients in the up-front group with a normal baseline LS T-score (> –1.0) progressed to T-scores ≤ –1.0 and ≥ –2.0 by month 36; however, more up-front patients with a T-score ≤ –1.0 and ≥ –2.0 at baseline experienced an improvement in T score to normal than the delayed-group patients. Furthermore, fewer up-front patients progressed to a T-score < –2.0 by month 36.”36
ZO-FAST14 Fair
1065
1 year
Upfront vs delayed zoledronic acid 4 mg IV over 15 minutes every 6 months
Unadjusted mean LS BMD change from baseline, %
2.1 (significantly different from zero)
-3.5 (significantly different from zero)
NR
LSMD (95% CI) in LS BMD between groups, %
- - 5.7 (5.2, 6.1); P<0.0001
Mean (95% CI) change from baseline in LS BMD (safety population), %
1.9 (1.6, 2.2) -3.1 (-3.5, -2.8)
P<0.0001

56 Systematic review of bisphosphonates in early breast cancer
Study ID Quality N
Follow-up
Comparison (intervention vs control) Outcome Intervention Comparator
Statistical significance
Mean (95% CI) change from baseline in LS BMD (recently postmenopausal women; safety population), %
-0.2 (-1.1, 0.7)
-5.5 (-6.3, -4.7)
P<0.0001
Z-FAST and ZO-FAST7
1667
1 year
Upfront vs delayed zoledronic acid 4 mg IV over 15 minutes every 6 months
Mean (SE) LS BMD at baseline, g/cm2
1.093 (0.0058)
1.092 (0.0057)
NR
Mean (SE) LS BMD at follow-up, g/cm2
1.117 (0.0062)
1.059 (0.0058)
NR
Mean (SE) change in LS BMD at baseline, %
2.0 (0.12) P<0.0001
-3.1 (0.15) P<0.0001
LSMD (95% CI): 5.2 (4.8, 5.6); P<0.0001
Mean (SE) change in LS BMD at baseline (mild-moderate osteopeniai), %
2.6 (NR) -3.4 NR
Mean (SE) change in LS BMD at baseline (normal BMDj), %
1.8 (NR) -2.5 NR
Proportion with LS BMD loss of ≥ 8%, %
0.1 9.7 NR
Other outcomes Patients in the delayed group with normal baseline BMD were significantly more likely to have BMD decreases of at least 8% compare with low baseline BMD patients.
Abbreviations: A+P, anastrozole and placebo; A+R, anastrozole and risedronate; AI, aromatase inhibitor; BMD, bone mineral density; CI, confidence interval; GA, goserelin (3.6 mg s.c. every 28 days) plus anastrozole (1 mg/day orally); GAZ, goserelin (3.6 mg s.c. every 28 days) plus anastrozole (1 mg/day orally) plus zoledronic acid (initially 8 mg IV every 4 weeks); GT, goserelin (3.6 mg s.c. every 28 days) plus tamoxifen (20 mg/day orally); GTZ, goserelin (3.6 mg s.c. every 28 days) plus tamoxifen (20 mg/day orally) plus zoledronic acid (initially 8 mg IV every 4 weeks); IV, intravenous; LS, lumbar spine; LSMD, least squares mean difference; MD, mean difference; NR, not reported; RR, risk ratio; SD, standard deviation; SE, standard error a Swedish BMD subgroup of the larger trial (N=953). b This figure reflects the patients who began the study. Two patients in each study arm withdrew before study began. c Calculated for this technical report using Review Manager 5. d Numbers of patients included those with values at baseline and the specified visit. Some patients discontinued treatment after the 24-month scan and before study completion (A+P, n=4; A+R, n=2). e BMD subgroup of larger trial (N=1803). f Defined as standard deviation units from the mean BMD of young healthy women. g P value for the comparison of the difference between treatment group means ignoring time. h The dosage of zoledronic acid was adjusted for a creatinine clearance < 60 mL/min, such that patients with a creatinine clearance of 50-60 mL/min received 3.5 mg zoledronic acid, those with a creatinine clearance of 40-49 mL/min received 3.3 mg zoledronic acid, and those with a creatinine clearance of 30-39 mL/min received 3.0 mg zoledronic acid. i T-score at baseline of -1.0 or lower and -2.0 or greater. j T-score at baseline of more than -1.0.

Systematic review of bisphosphonates in early breast cancer 57
4.7 Bone mineral density (BMD) at locations other than the spine
All of the included studies reported BMD at locations other than the spine (ie, hip, femoral neck [FN], trochanter, intertrochanter, and radius) as a clinical outcome (Table 16); this includes two studies assessing the impact of clodronate, one for ibandronate, one for pamidronate, three studies for risedronate, and five studies for zoledronic acid. In ARIBON and SABRE, the patient population was limited to osteopenic women with breast cancer.
4.7.1 Clodronate
In McCloskey 201022, participants were randomised to receive either 1600 mg/day clodronate or placebo. At two years, McCloskey 201022 found that the use of clodronate resulted in a significant improvement in TH (total hip) BMD compared with placebo (mean [95% CI] 0.52% [-0.07, 1.11] vs -0.77% (-1.24, -0.30); mean difference [95% CI] 1.29% [0.5, 2.28]; P<0.001). This was consistent for premenopausal (mean [95% CI] -0.57% [0.38] vs -1.84% [0.36]; P=0.008) but not postmenopausal women (mean [95% CI] 1.34% [0.43] vs 0.19% [0.30]; P=0.078), with no significant interaction between menopausal status and the ability of clodronate to prevent bone loss (P>0.05). At 2 years, the use of clodronate significantly reduced the loss of FN BMD (mean difference [95% CI] 1.45% [0.53, 2.38]; P=0.002), trochanter BMD (mean difference [95% CI] 1.78% [0.92, 2.64]; P<0.001), intertrochanter BMD (mean difference [95% CI] 0.88% [0.02, 1.74]; P=0.045), and Ward’s area* BMD (mean difference [95% CI] 2.13% [0.39, 3.88]; P=0.017) compared with placebo. At 5 years (ie, 3-year following cessation of therapy), the use of clodronate significantly reduced the loss of TH BMD (mean difference [95% CI] 1.40% [0.34%, 2.45%]; P=0.009), FN BMD (mean difference [95% CI] 1.70% [0.46, 2.94]; P=0.007), trochanter BMD (mean difference [95% CI] 1.78% [0.60, 2.96]; P<0.003), and Ward’s area BMD (mean difference [95% CI] 2.60% [0.66, 4.54]; P=0.0009), but not intertrochanter BMD (mean difference [95% CI] 1.00% [-0.15, 2.16]; P=0.087).
Women in the Saarto 200811 trial were randomised to receive either 1600 mg/day clodronate or standard care. The women received adjuvant chemotherapy and endocrine therapy. Reports of the Saarto 200811 trial published before 2007 determined that three-year clodronate therapy significantly reduced FN bone loss. After termination of clodronate therapy, no accelerated bone loss was found. The bone-loss rate did not differ between the groups within the next 7 years of follow-up. From 3 to 10 years, the mean change in FN BMD was -4.7% (SD 4.8) in the control group versus -4.7% (SD 5.0) in the clodronate group (P=0.56). The total FN bone loss during the 10-year period was -7.2% (SD 6.1) in the control group, and -5.2% (SD 6.3) in the clodronate group (P=NR).
4.7.2 Ibandronate
Women in the ARIBON23 trial were randomised to receive either 150 mg ibandronate every 28 days or placebo. Participants were postmenopausal women with osteopenia who all received adjuvant 1mg/day anastrozole during the study period. Ibandronate significantly reduced the loss of hip BMD compared with placebo at 1-year (mean [range] 0.98% [-4.1, 5.6] vs -2.27% [NR]; P<0.001), and 2-year follow-up (mean [range] 0.60% [-9.0, 6.9] vs -3.9% [NR]; P<0.003).
* The area in the femoral head with the lowest BMD.

58 Systematic review of bisphosphonates in early breast cancer
4.7.3 Pamidronate
Participants in the Kristensen 200824 trial were randomised to 150 mg oral pamidronate twice daily for 4 years or standard care. All participants received chemotherapy (either CMF or CEF). The linear mixed models analyses showed a non-significant tendency towards a decrease in the femur BMD in the control group compared with pamidronate. There was no significant interaction between time and pamidronate treatment.
4.7.4 Risedronate
Participants in the Hines 2009a25, REBBeCa27, and SABRE30 trials were randomised to 35 mg/week risedronate or placebo.
In Hines 2009a25, there was no significant difference between risedronate and control in the change from baseline at 1-year follow-up for either TH BMD (mean [95% CI] -2.7% [-3.98, -1.46] vs -3.4% [-4.43, -2.28]; P=0.40) or FN BMD (mean [95% CI] -2.2% [-4.11, -0.33] vs -2.4% [-5.15, 0.27]; P=0.29). At 1-year follow-up, there was no significant difference in the proportion of participants with 5% or greater FN bone loss (18.9% vs 19.8%; RR [95% CI] 0.95 [0.55, 1.65]; P=0.86) or TH bone loss (19.8% vs 17.0%; RR [95% CI] 1.17 [0.66, 2.06]; P=0.60).
The REBBeCa27 trial reported a significant difference between risedronate and placebo in the change from baseline at 2-year follow-up in TH BMD (mean [SD] 0.9% [0.6] vs -1.6% [0.4]; P<0.001), trochanter BMD (1.1% [0.8] vs -1.4% [0.4]; P<0.001), and FN BMD (-0.0% [0.6] vs -1.6% [0.8]; P=0.047), but not 1/3 distal radius BMD (-1.5% [0.7] vs -1.6% [0.5]; P=0.743) or total radius BMD (-1.7% [0.6] vs -2.1% [0.3]; P=0.533).
The SABRE30 trial included only osteopenic women. There was a significant difference between risedronate and placebo in the change from baseline in hip BMD at 1-year follow-up (mean [95% CI] 0.9% [0.12, 1.61] vs -0.4% [-1.17, 0.31]; P=0.0023) and 2-year follow-up (1.8% [0.78, 2.86] vs -1.1% [-2.14, -0.10]; P<0.001).
4.7.5 Zoledronic acid
In ABCSG-1232, participants were randomised to goserelin (3.6 mg s.c. every 28 days) plus either tamoxifen (20 mg/day) or anastrozole (1 mg/day), with or without zoledronic acid (initially 8 mg IV every 4 weeks*). There was a significant reduction in TH BMD for the patients randomised to the regimes without zoledronic acid at 1-year (mean [95% CI] -0.030 g/cm3 [-0.053, -0.007]; P=0.010), and 3-year follow-up (-0.053 g/cm3 [-0.076, -0.030]; P<0.001), but not at 5-year follow-up (-0.030 g/cm3 [-0.062, 0.001]; P=0.058). Similarly, there was a significant reduction in the TH BMD T-score for these patients at 1-year (-0.3 [-0.6, -0.1]; P=0.015), and 3-year follow-up (-0.5 [-0.7, -0.2]; P<0.001), but not 5-year follow-up (-0.2 [-0.5, 0.1]; P=0.234). For patients randomised to the treatment regimes with zoledronic acid, there was no significant reduction in TH BMD at 1-year (0.006 g/cm3 [-0.017, 0.029]; P=0.616), 3-year (0.006 g/cm3 [-0.018, 0.028]; P<0.642), and 5-year follow-up (0.028 g/cm3 [-0.003, 0.058]; P=0.73). Similarly, there was no significant reduction in TH BMD at 1-year (0.1 [-0.2, 0.3]; P=0.576) and 3-year follow-up (0.1 [-0.1, 0.4]; P=0.261). The patients randomised to the zoledronic acid containing regimens experienced a
* Protocol amendments, after 254 patients had been enrolled, reduced the dose of zoledronic acid to 4 mg every 6 months and increased the infusion time to 15 minutes.

Systematic review of bisphosphonates in early breast cancer 59
significant improvement from baseline in TH BMD T-score at 5-year follow-up (0.4 [0.1, 0.7]; P=0.017).
Hershman 201033 compared 4 mg zoledronic acid IV over 15 minutes every 3 months with placebo. Zoledronic acid significantly increased FN BMD compared with placebo at 1-year follow-up (mean [SE] 1.1% [0.42] vs -1.5% [0.61]), and 2-year follow-up (0.04% [0.84] vs -2.4% [0.71]; P=0.05*). Similarly zoledronic acid significantly increased TH BMD at 1-year follow-up (0.7% [1.06] vs -1.9% [0.66]), and 2-year follow-up (0.8% [1.07] vs -2.6% [0.84]; P<0.001†). In the placebo group, change in BMD was not correlated with type of chemotherapy, baseline BMD, hormonal therapy, or permanence of menstrual cessation.
Participants in the Hines 2009b34, Z-FAST38, and ZO-FAST14 trials were randomised to receive either upfront or delayed† zoledronic acid (4 mg IV over 15 minutes every 6 months).
The study population in Hines 2009b34 was postmenopausal women with early breast cancer starting letrozole after tamoxifen. Upfront zoledronic acid significantly reduced the loss of FN BMD compared with delayed zoledronic acid at 1-year follow-up (mean [SD] 2.08% [NR] vs -0.09% [NR]; P<0.001), and 2-year follow-up (mean [SD] 3.36% [NR] vs 0.54% [NR]; P<0.001). Similarly, upfront zoledronic acid significantly reduced the loss of TH BMD at 1-year follow-up (mean [SD] 1.02% [NR] vs -1.41% [NR]; P<0.001) and 2-year follow-up (mean [SD] 1.22% [NR] vs -3.34% [NR]; P<0.001). The proportion of subjects with 5% or greater bone loss at 1-year follow-up was significantly lower in the upfront group compared with the delayed group for both FN BMD (4.7% vs 11.9%; P=0.0057), and TH BMD (2.2% vs 10.8%; P<0.001).
In Z-FAST38, the use of upfront zoledronic acid significantly increased TH BMD compared with delayed zoledronic acid at 1-year follow-up (LSMD [95% CI] 3.2% [2.7, 3.7]; P<0.05), 2-year follow-up (LSMD [95% CI] 4.6% [4, 5.3]) and 3-year follow-up (LSMD [95% CI] 5.3% [4.4, 6.2]). Upfront zoledronic acid was significantly more effective than delayed treatment in preventing BMD loss, regardless of baseline T-score, risk factor frequency, or chemotherapy.
In the ZO-FAST14 trial, upfront zoledronic acid significantly increased TH BMD compared with delayed zoledronic acid at 1-year follow-up (LSMD [95% CI] 3.6% [3.3, -4.0]; P<0.001); this was consistent when the population of interest was restricted to postmenopausal women (mean [95% CI] 0.07% [-0.6, 0.7] vs 3.4% [-4.0, -2.8]; P<0.001).
Brufsky 20087 reported an integrated analysis of the Z-FAST and ZO-FAST trials. Upfront zoledronic acid significantly increased TH BMD compared with delayed zoledronic acid at 1-year follow-up (LSMD [95% CI] 3.5% [3.2, 3.8]; P<0.0001). Patients with mild-moderate osteopenia (T-score of -1.0 or lower and -2.0 or greater) at baseline receiving upfront zoledronic acid were found to have a greater TH BMD increase compared with patients with normal baseline BMD (1.8% vs 1%). Patients in the delayed group with normal baseline BMD experienced a greater decrease in TH BMD (-2.3% vs -1.9%) compared with patients with low baseline BMD.
4.7.6 Conclusion
Short-term use (up to four years) of clodronate, ibandronate, risedronate, and zoledronic acid all significantly reduce the hip and FN bone loss associated with the treatment of early breast * P value for the comparison of the difference between treatment group means ignoring time. † The upfront group received zoledronic acid immediately after random assignment. The delayed group received zoledronic acid when either post-baseline LS or TH T-score decreased to less than -2.0 or a non-traumatic clinical fracture occurred.

60 Systematic review of bisphosphonates in early breast cancer
cancer. Furthermore, clodronate significantly reduces bone loss at the trochanter and intertrochanter of the femur and risedronate significantly reduces bone loss at the trochanter and radius.

Systematic review of bisphosphonates in early breast cancer 61
Table 16 BMD at locations other than the spine
Study ID Quality N
Follow-up
Comparison (intervention vs control) Outcome Intervention Comparator
Statistical significance
Clodronate
McCloskey 201022 Fair
851 2 years
1600 mg/day clodronate vs placebo
Mean (95% CI) change in TH BMD from baseline, %
0.52 (-0.07, 1.11)
-0.77 (-1.24, -0.30)
MD (95% CI): 1.29% (0.5, 2.28) ; P<0.01
Mean (SD) change in TH BMD from baseline (premenopausal women), %
-0.57 (0.38) -1.84 (0.36) P=0.008
Mean (SD) change in TH BMD from baseline (postmenopausal women), %
1.34 (0.43) 0.19 (0.30) P=0.078
Mean (SD) change in FN BMD from baseline, %
0.03 (-0.67, 0.73)
-1.42 (-2.04, -0.81)
MD (95% CI): 1.45 (0.53, 2.38); P=0.002
Mean (SD) change in trochanter BMD from baseline, %
0.36 (-0.29, 1.01)
-1.43 (-1.99, -0.86)
MD (95% CI): 1.78 (0.92, 2.64) P<0.001
Mean (SD) change in intertrochanter BMD from baseline, %
0.51 (-0.18, 1.21)
-0.37 (-0.88, 0.15)
MD (95% CI): 0.88 (0.02, 1.74); P=0.045
Mean (SD) change in Ward’s area BMD from baseline, %
1.27 (-0.11, 2.66)
-0.86 (-1.95, 0.22)
MD (95% CI): 2.13 (0.39, 3.88); P=0.017
5 years
Mean (SD) change in TH BMD from baseline, %
NR NR MD (95% CI): 1.40 (0.34, 2.45); P=0.009
Mean (SD) change in FN BMD from baseline, %
-2.35 (-3.27, -1.43)
-4.05 (-4.88, -3.22)
MD (95% CI): 1.70 (0.46, 2.94); P=0.007
Mean (SD) change in trochanter BMD from baseline, %
-1.35 (-2.18, -0.51)
-3.13 (-3.97, -2.29)
MD (95% CI): 1.78 (0.60, 2.96); P<0.003
Mean (SD) change in intertrochanter BMD from baseline, %
-1.02 (-1.89, -0.15)
-2.03 (-2.79, -1.27)
MD (95% CI): 1.00 (-0.15, 2.16); P=0.087
Mean (SD) change in Ward’s area BMD from baseline, %
-1.72 (-3.15, -0.28)
-4.31 (-5.62, -3.00)
MD (95% CI): 2.60 (0.66, 4.54); P=0.009

62 Systematic review of bisphosphonates in early breast cancer
Study ID Quality N
Follow-up
Comparison (intervention vs control) Outcome Intervention Comparator
Statistical significance
Saarto 200811 Fair
96 10 years
1600 mg/day clodronate vs standard care
Mean (SD) change in FN BMD from 3-year follow-up, %
-4.7 (5.0) -4.7 (4.8) P=0.56
Mean (SD) change in FN BMD from baseline, %
-5.2 (6.3) -7.2 (6.1) NR
Ibandronate
ARIBON23 Fair
50 1 year
150 mg/28 days ibandronate vs placebo
Mean (range) change in TH BMD, %
0.98 (-4.1, 5.6) (N=23)
-2.27 (NR) (N=25)
P<0.001
2 years
Mean (range) change in hip BMD, %
0.60 (-9.0, 6.9) (N=21)
-3.90 (NR) (N=19)
P<0.003
Pamidronate
Kristensen 200824 Fair
953 4 years
150 mg oral pamidronate twice daily for 4 years vs standard care
Change in femur BMD
NR NR The linear mixed models analyses showed a tendency towards a decrease in femur BMD in the control group compared with pamidronate, however this was non-significant at all measurement locations. There was no significant interaction between time and pamidronate.
Risedronate
Hines 2009a25 Good
212a
1 year
35 mg/week risedronate vs placebo
Mean (95% CI) TH BMD at baseline, g/cm2
1.04 (1.01, 1.07)
1.02 (1.00, 1.05)
P=0.32
Mean (95% CI) TH BMD at 1-year follow-up, g/cm2
1.02 (0.98, 1.05)
1.00 (0.97, 1.03)
P=0.41
Mean (95% CI) change in TH BMD from baseline, %
-2.7 (-3.98, -1.46)
-3.4 (-4.43, -2.28)
P=0.40
Mean (95% CI) FN BMD at baseline, g/cm2
0.98 (0.94, 1.03)
0.97 (0.94, 1.00)
P=0.44
Mean (95% CI) FN BMD at 1-year follow-up, g/cm2
0.96 (0.93, 1.00)
0.94 (0.91, 0.97)
P=0.28
Mean (95% CI) change in FN BMD from baseline, %
-2.2 (-4.11, -0.33)
-2.4 (-5.15, 0.27)
P=0.29
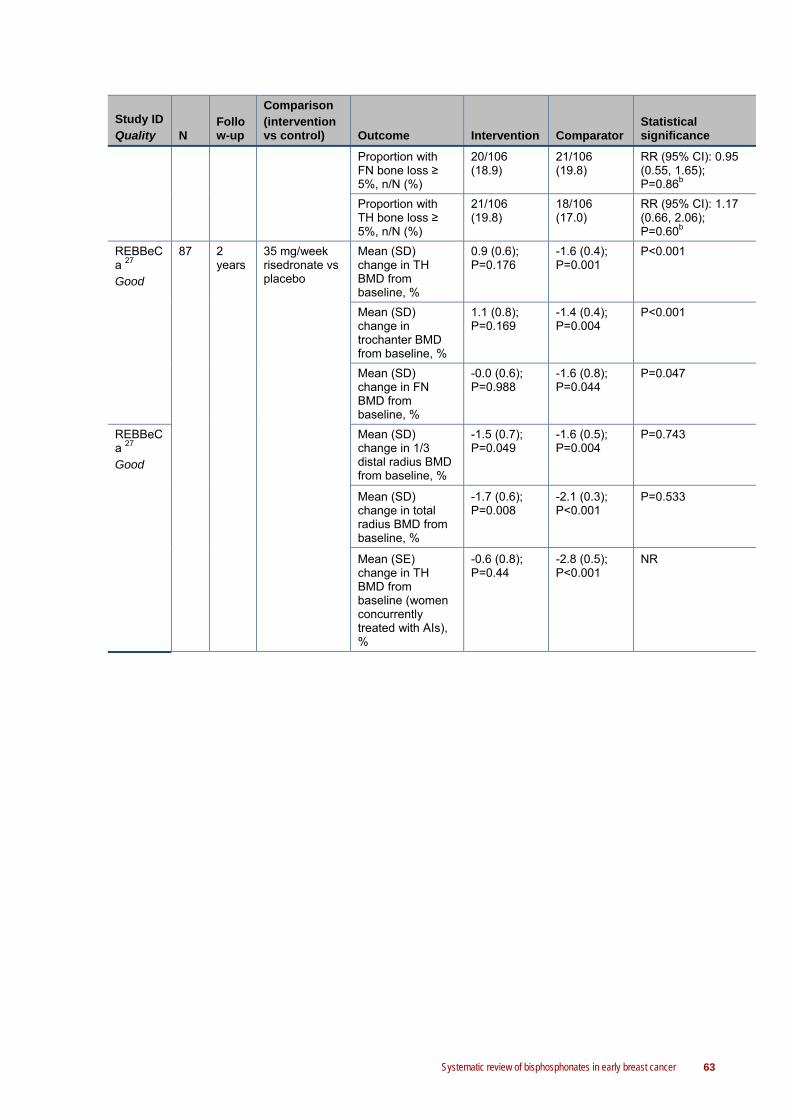
Systematic review of bisphosphonates in early breast cancer 63
Study ID Quality N
Follow-up
Comparison (intervention vs control) Outcome Intervention Comparator
Statistical significance
Proportion with FN bone loss ≥ 5%, n/N (%)
20/106 (18.9)
21/106 (19.8)
RR (95% CI): 0.95 (0.55, 1.65); P=0.86b
Proportion with TH bone loss ≥ 5%, n/N (%)
21/106 (19.8)
18/106 (17.0)
RR (95% CI): 1.17 (0.66, 2.06); P=0.60b
REBBeCa 27 Good
87 2 years
35 mg/week risedronate vs placebo
Mean (SD) change in TH BMD from baseline, %
0.9 (0.6); P=0.176
-1.6 (0.4); P=0.001
P<0.001
Mean (SD) change in trochanter BMD from baseline, %
1.1 (0.8); P=0.169
-1.4 (0.4); P=0.004
P<0.001
Mean (SD) change in FN BMD from baseline, %
-0.0 (0.6); P=0.988
-1.6 (0.8); P=0.044
P=0.047
REBBeCa 27 Good
Mean (SD) change in 1/3 distal radius BMD from baseline, %
-1.5 (0.7); P=0.049
-1.6 (0.5); P=0.004
P=0.743
Mean (SD) change in total radius BMD from baseline, %
-1.7 (0.6); P=0.008
-2.1 (0.3); P<0.001
P=0.533
Mean (SE) change in TH BMD from baseline (women concurrently treated with AIs), %
-0.6 (0.8); P=0.44
-2.8 (0.5); P<0.001
NR

64 Systematic review of bisphosphonates in early breast cancer
Study ID Quality N
Follow-up
Comparison (intervention vs control) Outcome Intervention Comparator
Statistical significance
Mean (SE) change in trochanter BMD from baseline (women concurrently treated with AIs), %
-0.8 (1.0); P=0.41
-4.2 (0.7); P<0.001
NR
Mean (SE) change in FN BMD from baseline (women concurrently treated with AIs), %
-2.5 (0.8); P=0.004
-2.4 (1.1); P=0.04
NR
Mean (SE) change in 1/3 distal radius BMD from baseline (women concurrently treated with AIs), %
-2.7 (1.1); P=0.03
-2.1 (0.6); P=0.003
NR
Mean (SE) change in total radius BMD from baseline (women concurrently treated with AIs), %
-3.3 (1.0); P=0.003
-3.0 (0.3); P<0.001
NR
Mean (SE) change in TH BMD from baseline (women not concurrently treated with AIs), %
2.2 (0.9); P=0.04
-1.2 (0.5); P=0.04
NR
Mean (SE) change in trochanter BMD from baseline (women not concurrently treated with AIs), %
2.7 (1.1); P=0.03
-0.0 (0.5); P=0.96
NR
Mean (SE) change in FN BMD from baseline (women not concurrently treated with AIs), %
1.9 (0.9); P=0.04
-1.4 (1.2); P=0.25
NR

Systematic review of bisphosphonates in early breast cancer 65
Study ID Quality N
Follow-up
Comparison (intervention vs control) Outcome Intervention Comparator
Statistical significance
Mean (SE) change in 1/3 distal radius BMD from baseline (women not concurrently treated with AIs), %
-0.6 (0.8); P=0.45
-1.2 (0.9); P=0.19
NR
Mean (SE) change in total radius BMD from baseline (women not concurrently treated with AIs), %
-0.6 (0.6); P=0.32
-1.4 (0.5); P=0.02
NR
SABRE3
0 Good
154a
1 year
35 mg/week risedronate vs placebo
Mean (95% CI) change from baseline to 12 months in hip BMD, %
0.9 (0.12, 1.61) (N=73)
-0.4 (-1.17, 0.31) (N=65)
P=0.0023
2 years
Mean (95% CI) change from baseline to 24 months in hip BMD, %
1.8 (0.78, 2.86) (N=60)
-1.1 (-2.14, -0.10) (N=54)
P<0.0001
Zoledronic acid
ABCSG-12 32 Fair
404c
1 year
GTZ/GAZ vs GT/GA
Mean (95% CI) change in TH BMD from baseline, g/cm3
0.006 (-0.017, 0.029) P=0.616
-0.030 (-0.053, -0.007) P=0.010
NR
Mean (95% CI) change in TH BMD T-scored from baseline
0.1 (-0.2, 0.3) P=0.576
-0.3 (-0.6, -0.1) P=0.015
NR
3 years
Mean (95% CI) change in TH BMD from baseline, g/cm3
0.006 (-0.018, 0.028) P=0.642
-0.053 (-0.076, -0.030 P<0.0001
NR
Mean (95% CI) change in TH BMD T-scored from baseline
0.1 (-0.1, 0.4) P=0.261
-0.5 (-0.7, -0.2) P<0.001
NR
5 years
Mean (95% CI) change in TH BMD from baseline, g/cm3
0.028 (-0.003, 0.058) P=0.073
-0.030 (-0.062, 0.001) P=0.058
NR
Mean (95% CI) change in TH BMD T-scored from baseline
0.4 (0.1, 0.7) P=0.017
-0.2 (-0.5, 0.1) P=0.234
NR
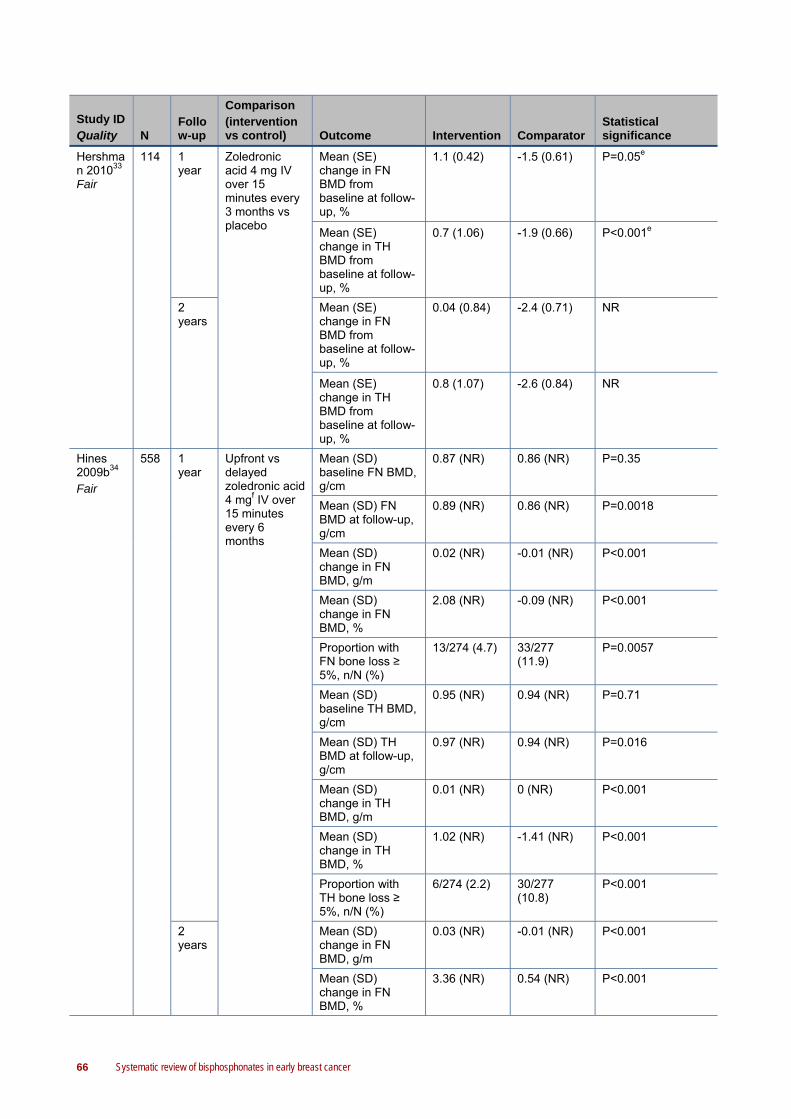
66 Systematic review of bisphosphonates in early breast cancer
Study ID Quality N
Follow-up
Comparison (intervention vs control) Outcome Intervention Comparator
Statistical significance
Hershman 201033 Fair
114 1 year
Zoledronic acid 4 mg IV over 15 minutes every 3 months vs placebo
Mean (SE) change in FN BMD from baseline at follow-up, %
1.1 (0.42) -1.5 (0.61) P=0.05e
Mean (SE) change in TH BMD from baseline at follow-up, %
0.7 (1.06) -1.9 (0.66) P<0.001e
2 years
Mean (SE) change in FN BMD from baseline at follow-up, %
0.04 (0.84) -2.4 (0.71) NR
Mean (SE) change in TH BMD from baseline at follow-up, %
0.8 (1.07) -2.6 (0.84) NR
Hines 2009b34 Fair
558 1 year
Upfront vs delayed zoledronic acid 4 mgf IV over 15 minutes every 6 months
Mean (SD) baseline FN BMD, g/cm
0.87 (NR) 0.86 (NR) P=0.35
Mean (SD) FN BMD at follow-up, g/cm
0.89 (NR) 0.86 (NR) P=0.0018
Mean (SD) change in FN BMD, g/m
0.02 (NR) -0.01 (NR) P<0.001
Mean (SD) change in FN BMD, %
2.08 (NR) -0.09 (NR) P<0.001
Proportion with FN bone loss ≥ 5%, n/N (%)
13/274 (4.7) 33/277 (11.9)
P=0.0057
Mean (SD) baseline TH BMD, g/cm
0.95 (NR) 0.94 (NR) P=0.71
Mean (SD) TH BMD at follow-up, g/cm
0.97 (NR) 0.94 (NR) P=0.016
Mean (SD) change in TH BMD, g/m
0.01 (NR) 0 (NR) P<0.001
Mean (SD) change in TH BMD, %
1.02 (NR) -1.41 (NR) P<0.001
Proportion with TH bone loss ≥ 5%, n/N (%)
6/274 (2.2) 30/277 (10.8)
P<0.001
2 years
Mean (SD) change in FN BMD, g/m
0.03 (NR) -0.01 (NR) P<0.001
Mean (SD) change in FN BMD, %
3.36 (NR) 0.54 (NR) P<0.001

Systematic review of bisphosphonates in early breast cancer 67
Study ID Quality N
Follow-up
Comparison (intervention vs control) Outcome Intervention Comparator
Statistical significance
Mean (SD) change in TH BMD, g/m
0.01 (NR) -0.01 (NR) P<0.001
Mean (SD) change in TH BMD, %
1.22 (NR) -3.34 (NR) P<0.001
Z-FAST38 Fair
602 1 year
Upfront vs delayed zoledronic acid 4 mg IV over 15 minutes every 6 months
TH BMD, % NR NR LSMD (95% CI): 3.2 (2.7, 3.7); P<0.05
2 years
TH BMD, % NR NR LSMD (95% CI): 4.6 (4, 5.3); P<0.05
3 years
TH BMD, % NR NR LSMD (95% CI): 5.3 (4.4, 6.2) Absolute difference: 5.2% (P<0.0001)
Change in TH BMD from baseline, %
NR -5.1% (P<0.001) for patients who did not receive zoledronic acid 1.0% (P=0.24) for delayed patients who received zoledronic acid
NR
Mean rate of TH BMD change, g/cm2/year
0.002 -0.009 MD: 0.011; (P<0.0001)
ZO-FAST14 Fair
1065
1 year
Upfront vs delayed zoledronic acid 4 mg IV over 15 minutes every 6 months
LSMD (95% CI) in TH BMD between groups, %
- - 3.6 (3.3, 4.0); P<0.0001
Mean (95% CI) change from baseline in TH BMD (recently postmenopausal women; safety population), %
0.07 (-0.6, 0.7)
3.4 (-4.0, -2.8)
P<0.0001
Z-FAST and ZO-FAST7
1667
1 year
Upfront vs delayed zoledronic acid 4 mg IV over 15 minutes every 6 months
Mean (SE) TH BMD at baseline, g/cm2
0.959 (0.0045)
0.956 (0.0046)
NR
Mean (SE) TH BMD at follow-up, g/cm2
0.972 (0.0046)
0.936 (0.0046)
NR
Mean (SE) change in TH BMD at baseline, %
1.2 (0.09) P<0.0001
-2.2 (0.12) P<0.0001
LSMD: 3.5 (3.2, 3.8); P<0.0001
Mean (SE) change in TH BMD at baseline (mild-moderate osteopeniag), %
1.8 -2.3 NR

68 Systematic review of bisphosphonates in early breast cancer
Study ID Quality N
Follow-up
Comparison (intervention vs control) Outcome Intervention Comparator
Statistical significance
Mean (SE) change in TH BMD at baseline (normal BMDh), %
1 -1.9 NR
Abbreviations: AI, aromatase inhibitor; BMD, bone mineral density; CI, confidence interval; FN, femoral neck; GA, goserelin (3.6 mg s.c. every 28 days) plus anastrozole (1 mg/day orally); GAZ, goserelin (3.6 mg s.c. every 28 days) plus anastrozole (1 mg/day orally) plus zoledronic acid (initially 8 mg IV every 4 weeks); GT, goserelin (3.6 mg s.c. every 28 days) plus tamoxifen (20 mg/day orally); GTZ, goserelin (3.6 mg s.c. every 28 days) plus tamoxifen (20 mg/day orally) plus zoledronic acid (initially 8 mg IV every 4 weeks); IV, intravenous; LS, lumbar spine; LSMD, least squares mean difference; MD, mean difference; NR, not reported; RR, risk ratio; SD, standard deviation; SE, standard error; TH, total hip a This figure reflects the patients who began the study. b Calculated for this technical report using Review Manager 5. c BMD subgroup of larger trial (N=1803). d Defined as standard deviation units from the mean BMD of young healthy women. e P value for the comparison of the difference between treatment group means ignoring time. f The dosage of zoledronic acid was adjusted for a creatinine clearance < 60 mL/min, such that patients with a creatinine clearance of 50-60 mL/min received 3.5 mg zoledronic acid, those with a creatinine clearance of 40-49 mL/min received 3.3 mg zoledronic acid, and those with a creatinine clearance of 30-39 mL/min received 3.0 mg zoledronic acid. g T-score at baseline of -1.0 or lower and -2.0 or greater. h T-score at baseline of more than -1.0.
4.8 Osteopenia/osteoporosis
Osteopenia is a condition where bone mineral density is lower than normal. Osteopenia may be a precursor to osteoporosis. Osteopenia is defined as a BMD T-score greater than -2.5 and less than -1.0; and osteoporosis is defined as a BMD T-score of -2.5 or lower.
Six of the included studies reported development of osteopenia or osteoporosis as a clinical outcome (Table 18); this includes studies for clodronate, ibandronate, risedronate and zoledronic acid. In ARIBON23, the patient population was limited to osteopenic women with breast cancer.
4.8.1 Clodronate
In Saarto 200811, participants receiving adjuvant chemotherapy and endocrine therapy were randomised to receive either 1600 mg/day clodronate or standard care. At 10-year follow-up there was no significant difference between the treatment arms in the proportion of participants with osteopenia (50.0% vs 44.2%; RR [95% CI] 1.13 [0.74, 1.73]; P=0.57), osteoporosis (11.4% vs 25.0%; RR [95% CI] 0.45 [0.18, 1.18]; P=0.10), or normal BMD (38.6% vs 28.8%; RR [95% CI] 1.34 [0.76, 2.36]; P=0.31). There was no significant difference between treatment arms in the proportion of women who developed LS osteoporosis (7.3% vs 22.9%; RR [95% CI] 0.32 [0.10, 1.07]; P=0.06) and the proportion who developed FN or total femoral area (TFA) osteoporosis (17.1% vs 14.6%; RR [95% CI] 1.17 [0.45, 3.06]; P=0.75). The 10-year LS osteoporosis-free survival was significantly greater in the clodronate group compared with control (92.7% vs 77.0%; P=0.035); however, there was no significant difference in the FN/TFA osteoporosis-free survival (85.4% vs 82.9%; P=0.92).
4.8.2 Ibandronate
The women in the ARIBON23 trial were randomised to receive either 150 mg ibandronate every 28 days or placebo. Participants were postmenopausal women with osteopenia who all received

Systematic review of bisphosphonates in early breast cancer 69
adjuvant 1mg/day anastrozole during the study period. There was no significant difference between treatment arms at 2-year follow-up in the proportion of osteopenic women who changed to normal BMD (24% vs 0%; RR [95% CI] 13.00 [0.77, 219.11]; P=0.08), remained with osteopenia (64% vs 80%; RR [95% CI] 0.80 [0.56, 1.14]; P=0.22), or developed osteoporosis (4% vs 20%; RR [95% CI] 0.20 [0.03, 1.59]; P=0.13).
4.8.3 Risedronate
Hines 2009a25 compared 35 mg/week risedronate against placebo. At one-year follow-up, there was no significant difference between treatment arms in the incidence of osteopenia (22.6% vs 28.3%; RR [95% CI] 0.80 [0.50, 1.27]; P=0.35) or osteoporosis (0.0% vs 1.9%; RR [95% CI] 0.20 [0.01, 4.12]; P=0.30).
4.8.4 Zoledronic acid
In ABCSG-1232, participants were randomised to goserelin (3.6 mg s.c. every 28 days) plus either tamoxifen (20 mg/day) or anastrozole (1 mg/day), with or without zoledronic acid (initially 8 mg IV every 4 weeks*). At 3-year follow-up the addition of zoledronic acid to the combination of goserelin and tamoxifen significantly reduced the incidence of osteopenia (21% vs 35%; RR [95% CI] 0.60 [0.38, 0.95]; P=0.03) but not osteoporosis (3% vs 3%; RR [95% CI] 1.03 [0.21, 4.98]) compared with therapy without zoledronic acid. Conversely, at 5-year follow-up the addition of zoledronic acid to therapy with goserelin and tamoxifen significantly reduced the incidence of osteoporosis (0% vs 11%; RR [95% CI] 0.04 [0.00, 0.75]; P=0.03) but not osteopenia (24% vs 19%; RR [95% CI] 1.24 [0.73, 2.09]; P=0.43). The addition of zoledronic acid to therapy with goserelin and anastrozole significantly reduced the incidence of osteopenia compared with therapy without zoledronic acid at 3-year follow-up (23% vs 48%; RR [95% CI] 0.48 [0.32, 0.72]; P=0.0004) and 5-year follow-up (33% vs 48%; RR [95% CI] 0.70 [0.49, 0.98]; P=0.04), but did not have a significant impact on osteoporosis at 5-year follow-up compared with goserelin and anastrozole alone (0% vs 6%; RR [95% CI] 0.07 [0.00, 1.23]; P=0.07).
The results of the ZO-FAST14 trial are presented in Table 17. Participants in the ZO-FAST trial were randomised to receive either upfront or delayed† zoledronic acid (4 mg IV over 15 minutes every 6 months). After one year, a higher percentage of patients in the delayed group with normal baseline BMD developed mild to moderate osteopenia compared with patients in the upfront group (19.1% vs 0.9%; P<0.001). In the delayed group, a higher percentage of patients progressed from mild or moderate to severe osteopenia compared with the upfront group (18.0% vs 0.6%; P<0.0001).
* Protocol amendments, after 254 patients had been enrolled, reduced the dose of zoledronic acid to 4 mg every 6 months and increased the infusion time to 15 minutes. † The upfront group received zoledronic acid immediately after random assignment. The delayed group received zoledronic acid when either post-baseline LS or TH T-score decreased to less than -2.0 or a non-traumatic clinical fracture occurred.

70 Systematic review of bisphosphonates in early breast cancer
Table 17 ZO-FAST: shift table for LS BMD measurementsa at month 1214
Baseline BMDb Month 12 BMD Upfront group patients No. (%)
Delayed group patients No. (%)
P
Normal n=342 n=341 <0.0001
Normal (T-score > -1) 304 (88.9) 245 (71.8)
Mild osteopenia (T-score ≤ -1 to ≥ -2)
3 (0.9) 65 (19.1)
Severe osteopenia (T-score < -2)
0 (0.0) 0 (0.0)
Missing data 35 (10.2) 31 (9.1)
Mild osteopenia n=162 n=150 <0.0001
Normal (T-score > -1) 39 (24.1) 7 (4.7)
Mild osteopenia (T-score ≤ -1 to ≥ -2)
110 (67.9) 103 (68.7)
Severe osteopenia (T-score < -2)
1 (0.6) 27 (18.0)
Missing data 12 (7.4) 13 (8.7)
Severe osteopenia
n=11 n=17 <0.0379
Normal (T-score > -1) 0 (0.0) 0 (0.0)
Mild osteopenia (T-score ≤ -1 to ≥ -2)
6 (54.5) 2 (11.8)
Severe osteopenia (T-score < -2)
4 (36.4) 14 (82.4)
Missing data 1 (9.1) 1 (5.9)
Abbreviations: BMD, bone mineral density; LS, lumbar spine a Based on central reading of dual-energy X-ray absorptiometry scan results. b Baseline BMD data for 17 patients in the upfront group and 24 patients in the delayed group were not transferred to or could not be read by central reader from study sites; therefore, they were not included in the analysis.
Brufsky 20087 reported an integrated analysis of the Z-FAST and ZO-FAST trials. Overall, a higher proportion of women with normal BMD in the delayed group developed osteopenia within 1 year (17% vs 1.8%) compared with women in the upfront group, and a higher proportion of women with osteopenia developed osteoporosis (17% vs 1%; P<0.0001).
4.8.5 Meta-analysis of results
Figure 5 presents a meta-analysis of the effect of bisphosphonates on the incidence of osteoporosis in women with early breast cancer. Zoledronic acid significantly reduced the incidence of osteoporosis compared with control (RR [95% CI] 0.03 [0.00, 0.46]). There were no significant differences in osteoporosis incidence between treatment arms for clodronate (RR [95% CI] 0.30 [0.09, 1.01]), ibandronate (RR [95% CI] 0.20 [0.03, 1.59]), or risedronate (RR [95% CI] 0.20 [0.01, 4.12]) compared with control.
A potential source of heterogeneity in this meta-analysis is the differences in length of follow-up. Saarto 200811 and ABCSG-1232 had follow-up lengths of 10 and 5 years respectively. The other studies had follow-up periods of two years or less.

Systematic review of bisphosphonates in early breast cancer 71
Figure 5 Meta-analysis of incidence of osteoporosis by bisphosphonate
Study or Subgroup1.2.1 Clodronate
Saarto 2008Subtotal (95% CI)
Total eventsHeterogeneity: Not applicableTest for overall effect: Z = 1.95 (P = 0.05)
1.2.2 Ibandronate
ARIBONSubtotal (95% CI)
Total eventsHeterogeneity: Not applicableTest for overall effect: Z = 1.52 (P = 0.13)
1.2.3 Risedronate
Hines 2009aSubtotal (95% CI)
Total eventsHeterogeneity: Not applicableTest for overall effect: Z = 1.04 (P = 0.30)
1.2.4 Zoledronic acid
ABCSG-12Subtotal (95% CI)
Total eventsHeterogeneity: Not applicableTest for overall effect: Z = 2.51 (P = 0.01)
Total (95% CI)
Total eventsHeterogeneity: Tau² = 0.00; Chi² = 2.91, df = 3 (P = 0.41); I² = 0%Test for overall effect: Z = 3.33 (P = 0.0009)
Events
3
3
1
1
0
0
0
0
4
Total
4242
2525
106106
205205
378
Events
12
12
5
5
2
2
17
17
36
Total
5151
2525
106106
199199
381
Weight
59.8%59.8%
19.9%19.9%
9.4%9.4%
10.9%10.9%
100.0%
M-H, Random, 95% CI
0.30 [0.09, 1.01]0.30 [0.09, 1.01]
0.20 [0.03, 1.59]0.20 [0.03, 1.59]
0.20 [0.01, 4.12]0.20 [0.01, 4.12]
0.03 [0.00, 0.46]0.03 [0.00, 0.46]
0.21 [0.08, 0.52]
Bisphosphonates Control Risk Ratio Risk RatioM-H, Random, 95% CI
0.001 0.1 1 10 1000Favours bisphosphonates Favours control
4.8.6 Conclusion
Clodronate significantly improves LS osteoporosis-free survival, but has demonstrated no significant impact as yet on FN/TFA osteoporosis-free survival. Zoledronic acid significantly reduced the incidence of osteoporosis compared with control, but there were no significant differences in osteoporosis incidence between treatment arms for clodronate, ibandronate, or risedronate. Furthermore, the Z-FAST and ZO-FAST trials found that upfront zoledronic acid as an adjunct to endocrine therapy significantly reduces the incidence of osteopenia and osteoporosis compared with delayed zoledronic acid therapy.

72 Systematic review of bisphosphonates in early breast cancer
Table 18 Osteopenia/osteoporosis
Study ID Quality N
Follow-up
Comparison (intervention vs control) Outcome Intervention Comparator
Statistical significance
Clodronate
Saarto 200811 Fair
96 10 years
1600 mg/day clodronate vs standard care
Normal BMD at baseline, n/N (%)
28/44 (63.6) 29/52 (55.8) RR (95% CI): 1.14 [0.82, 1.59]; P=0.42a
Normal BMD at 10-year follow-up, n/N (%)
17/44 (38.6) 15/52 (28.8) RR (95% CI): 1.34 (0.76, 2.36); P=0.31a
Osteopenia (T-score > -2.5 and < -1.0) at baseline, n/N (%)
14/44 (31.8) 21/52 (40.4) RR (95% CI): 0.79 (0.46, 1.36); P=0.39a
Osteopenia (T-score > -2.5 and < -1.0) at 10-year follow-up, n/N (%)
22/44 (50.0) 23/52 (44.2) RR (95% CI): 1.13 (0.74, 1.73); P=0.57a
Osteoporosis (T-score < -2.5) at baseline, n/N (%)
2/44 (4.5) 1/52 (1.9) RR (95% CI): 2.36 (0.22, 25.20); P=0.48a
Osteoporosis (T-score < -2.5) at 10-year follow-up, n/N (%)
5/44 (11.4) 13/52 (25.0) RR (95% CI): 0.45 (0.18, 1.18); P=0.10a
Incidence of osteoporosis at 10-year follow-up, n/N (%)
3/42 (7.1) 12/51 (23.5) RR (95% CI): 0.30 (0.09, 1.01); P>0.05a
Premenopausal women who developed osteoporosis (T-score < -2.5) at 10-year follow-up, n/N (%)
15/55 (27.3) NR NR
Postmenopausal women who developed osteoporosis (T-score < -2.5) at 10-year follow-up, n/N (%)
9/33 (27.3) NR NR
LS osteoporosis (T-score < -2.5) at 10-year follow-up, n/N (%)
3/41 (7.3) 11/48 (22.9) RR (95% CI): 0.32 (0.10, 1.07); P=0.06a
FN or TFA osteoporosis (T-score < -2.5) at 10-year follow-up, n/N (%)
7/41 (17.1) 7/48 (14.6) RR (95% CI): 1.17 (0.45, 3.06); P=0.75a
10-year LS OPFS, %
92.7 77.0 P=0.035
10-year FN or TFA OPFS, %
85.4 82.9 P=0.92

Systematic review of bisphosphonates in early breast cancer 73
Study ID Quality N
Follow-up
Comparison (intervention vs control) Outcome Intervention Comparator
Statistical significance
Ibandronate
ARIBON23 Fair
50 2 years
150 mg/28 days ibandronate vs placebo
Change from osteopenia (T-score > -2.5 and < -1.0) to normal BMD (T-score ≥ -1), n/N (%)
6/25 (24.0) 0/25 (0.0) RR (95% CI): 13.00 (0.77, 219.11); P=0.08a
Patients with osteopenia (T-score > -2.5 and < -1.0) who remained with osteopenia, n/N (%)
16/25 (64.0) 20/25 (80.0) RR (95% CI): 0.80 (0.56, 1.14); P=0.22a
Change from osteopenia (T-score > -2.5 and < -1.0) to osteoporosis (T-score < -2.5), n/N (%)
1/25 (4.0) 5/25 (20.0) RR (95% CI): 0.20 (0.03, 1.59); P=0.13a
Risedronate
Hines 2009a25 Good
212b
1 year
35 mg/week risedronate vs placebo
Incidence of osteopenia, n/N (%)
24/106 (22.6)
30/106 (28.3)
RR (95% CI): 0.80 (0.50, 1.27); P=0.35a
Incidence of osteoporosis, n/N (%)
0/106 (0.0) 2/106 (1.9) RR (95% CI): 0.20 (0.01, 4.12); P=0.30a
Zoledronic acid
ABCSG-12 32 Fair
404c
3 years
GTZ vs GT Incidence of osteopenia, n/N (%)
21/100 (21)
36/103 (35)
RR (95% CI): 0.60 (0.38, 0.95); P=0.03a
Incidence of osteoporosis, n/N (%)
3/100 (3)
3/103 (3) RR (95% CI): 1.03 (0.21, 4.98); P=0.97a
GAZ vs GA Incidence of osteopenia, n/N (%)
24/105 (23) 46/96 (48) RR (95% CI):0.48 (0.32, 0.72); P=0.0004a
Incidence of osteoporosis, n/N (%)
NR 16/96 (17) NR
5 years
GTZ vs GT Incidence of osteopenia, n/N (%)
24/100 (24)
20/103 (19)
RR (95% CI): 1.24 (0.73, 2.09); P=0.43a
Incidence of osteoporosis, n/N (%)
0/100 (0) 11/103 (11) RR (95% CI): 0.04 (0.00, 0.75); P=0.03a
GAZ vs GA Incidence of osteopenia, n/N (%)
35/105 (33) 46/96 (48) RR (95% CI):0.70 (0.49, 0.98); P=0.04a
Incidence of osteoporosis, n/N (%)
0/105 (0) 6/96 (6) RR (95% CI): 0.07 (0.00,1.23); P=0.07a

74 Systematic review of bisphosphonates in early breast cancer
Study ID Quality N
Follow-up
Comparison (intervention vs control) Outcome Intervention Comparator
Statistical significance
Z-FAST and ZO-FAST7
1667
1 year
Upfront vs delayed zoledronic acid 4 mg IV over 15 minutes every 6 months
Change from normal BMD at baseline to osteopenia at follow-up, %
11/587 (1.9) 99/583 (17) P<0.0001
Change from osteopenia at baseline to osteoporosis at follow-up, %
2/246 (0.8) 43/251 (17.1)
P<0.0001
Abbreviations: BMD, bone mineral density; CI, confidence interval; FN, femoral neck; GA, goserelin (3.6 mg s.c. every 28 days) plus anastrozole (1 mg/day orally); GAZ, goserelin (3.6 mg s.c. every 28 days) plus anastrozole (1 mg/day orally) plus zoledronic acid (initially 8 mg IV every 4 weeks); GT, goserelin (3.6 mg s.c. every 28 days) plus tamoxifen (20 mg/day orally); GTZ, goserelin (3.6 mg s.c. every 28 days) plus tamoxifen (20 mg/day orally) plus zoledronic acid (initially 8 mg IV every 4 weeks); IV, intravenous; LS, lumbar spine; NR, not reported; OPFS, osteoporosis-free survival; RR, risk ratio; TFA, total femoral area a Calculated for the purposes of this systematic review using Review Manager 5.
b This figure reflects the patients who began the study. Two patients in each study arm withdrew before study began. c BMD subgroup of larger trial (N=1803).
4.9 Fracture occurrence
Seven of the included studies reported fracture occurrence as a clinical outcome (Table 19); this includes one study assessing the impact of ibandronate, one studying the impact of pamidronate, two studies assessing risedronate, and three studies assessing zoledronic acid. In ARIBON and SABRE, the patient population was limited to osteopenic women with breast cancer.
4.9.1 Ibandronate
The women in the ARIBON23 trial were randomised to receive either 150 mg ibandronate every 28 days or placebo. Participants were postmenopausal women with osteopenia who all received adjuvant 1mg/day anastrozole during the study period. There were two traumatic fractures in the ibandronate group (one wrist fracture and one hip fracture) and three traumatic fractures in the placebo group (one wrist fracture, one shoulder fracture, and one rib fracture) (P=0.64). There were no fragility fractures in either study arm.
4.9.2 Pamidronate
Participants in the Kristensen 200824 trial were randomised to 150 mg oral pamidronate twice daily for 4 years or standard care. All participants received chemotherapy (either CMF or CEF). There were slightly more fractures among patients treated with pamidronate, but the difference was not significant.
4.9.3 Risedronate
REBBeCa27 and SABRE30 compared 35 mg/week risedronate against placebo. There was no significant difference in fracture occurrence between risedronate and placebo in either REBBeCa (7.0% vs 4.5%; RR [95% CI] 1.53 [0.27, 8.74]; P=0.63) or SABRE (0% vs 5.2%; RR [95% CI]
Systematic review of bisphosphonates in early breast cancer 75
0.11 [0.01, 2.03]; P>0.05). The SABRE trial included only osteopenic women.
4.9.4 Zoledronic acid
In ABCSG-1231, participants were randomised to goserelin (3.6 mg s.c. every 28 days) plus either tamoxifen (20 mg/day) or anastrozole (1 mg/day), with or without zoledronic acid (initially 8 mg IV every 4 weeks*). There was no significant difference in fracture occurrence between the treatments with and without zoledronic acid (0.1% vs 0.2%; RR [95% CI] 0.50 [0.05, 5.53]; P=0.57).
Participants in the Z-FAST38 and ZO-FAST14 trials were randomised to receive either upfront or delayed† zoledronic acid (4 mg IV over 15 minutes every 6 months). No significant difference between upfront and delayed zoledronic acid was found in either Z-FAST (4.3% vs 5.0%; RR [95% CI] 0.87 [0.42, 1.79]; P>0.05) or ZO-FAST (1.5% vs 1.7%; RR [95% CI] 0.89 [0.35, 2.29]; P=0.81).
4.9.5 Meta-analysis of results
Figure 6 presents a meta-analysis of the effect of bisphosphonates on the incidence of fracture in women with early breast cancer. There was no significant difference in the incidence of fracture for women treated with ibandronate (RR [95% CI] 0.67 [0.12, 3.65]), pamidronate (RR [95% CI] 1.52 [0.84, 2.73]), risedronate (RR [95% CI] 0.53 [0.04, 7.37]), zoledronic acid (RR [95% CI] 0.50 [0.05, 5.53]), or any bisphosphonate (RR [95% CI] 1.16 [0.63, 2.11]) compared with control.
A potential source of heterogeneity in the results of this meta-analysis is the differences in length of follow-up. Kristensen 200824 had a length of follow-up of 10 years, while the other studies had follow-up periods of less than 4 years.
* Protocol amendments, after 254 patients had been enrolled, reduced the dose of zoledronic acid to 4 mg every 6 months and increased the infusion time to 15 minutes. † The upfront group received zoledronic acid immediately after random assignment. The delayed group received zoledronic acid when either post-baseline LS or TH T-score decreased to less than -2.0 or a non-traumatic clinical fracture occurred.

76 Systematic review of bisphosphonates in early breast cancer
Figure 6 Meta-analysis of fracture incidence by bisphosphonate
Study or Subgroup1.3.1 Ibandronate
ARIBONSubtotal (95% CI)
Total eventsHeterogeneity: Not applicableTest for overall effect: Z = 0.47 (P = 0.64)
1.3.2 Pamidronate
Kristensen 2008Subtotal (95% CI)
Total eventsHeterogeneity: Not applicableTest for overall effect: Z = 1.39 (P = 0.16)
1.3.3 Risedronate
REBBeCaSABRESubtotal (95% CI)
Total eventsHeterogeneity: Tau² = 2.26; Chi² = 2.51, df = 1 (P = 0.11); I² = 60%Test for overall effect: Z = 0.47 (P = 0.64)
1.3.4 Zoledronic acid
ABCSG-12Subtotal (95% CI)
Total eventsHeterogeneity: Not applicableTest for overall effect: Z = 0.56 (P = 0.57)
Total (95% CI)
Total eventsHeterogeneity: Tau² = 0.05; Chi² = 4.32, df = 4 (P = 0.36); I² = 7%Test for overall effect: Z = 0.47 (P = 0.64)
Events
2
2
25
25
30
3
1
1
31
Total
2525
347347
4377
120
899899
1391
Events
3
3
18
18
24
6
2
2
29
Total
2525
379379
4477
121
904904
1429
Weight
11.7%11.7%
66.7%66.7%
11.3%4.2%
15.4%
6.1%6.1%
100.0%
M-H, Random, 95% CI
0.67 [0.12, 3.65]0.67 [0.12, 3.65]
1.52 [0.84, 2.73]1.52 [0.84, 2.73]
1.53 [0.27, 8.74]0.11 [0.01, 2.03]0.53 [0.04, 7.37]
0.50 [0.05, 5.53]0.50 [0.05, 5.53]
1.16 [0.63, 2.11]
Bisphosphonates Control Risk Ratio Risk RatioM-H, Random, 95% CI
0.005 0.1 1 10 200Favours bisphosphonates Favours control
4.9.6 Conclusion
None of the studies found that bisphosphonates had a significant effect on the incidence of bone fractures. The studies were not powered to detect a significant difference for this outcome.
Table 19 Fracture occurrence
Study ID Quality N
Comparison (intervention vs control)
Follow-up Outcome Intervention Comparator
Statistical significance
Ibandronate
ARIBON23 Fair
50 150 mg/28 days ibandronate vs placebo
2 years
Fragility fractures, n/N (%)
0/25 (0) 0/25 (0) NA
Traumatic fractures, n/N (%)
2/25 (8) [wrist=1, hip=1]
3/25 (12) [wrist=1, shoulder=1, rib=1]
RR (95% CI): 0.67 (0.12, 3.65); P=0.64a

Systematic review of bisphosphonates in early breast cancer 77
Study ID Quality N
Comparison (intervention vs control)
Follow-up Outcome Intervention Comparator
Statistical significance
Pamidronate
Kristensen 200824 Fair
726b
150 mg oral pamidronate twice daily for 4 years vs standard care
10 years
Fracture, n/N (%)
CMF/pamidronate 15/186 (8)c
CEF/pamidronate 10/161 (6)d
CMF 7/197 (4)e
CEF 11/182 (6)f
P>0.05
Risedronate
REBBeCa 27 Good
87 35 mg/week risedronate vs placebo
2 years
Fracture, n/N (%)
3/43 (7.0) 2/44 (4.5) RR (95% CI): 1.53 (0.27, 8.74); P=0.63
SABRE3
0 Good
154 35 mg/week risedronate vs placebo
2 years
Fracture, n/N (%)
0/77 (0.0) 4/77 (5.2) [wrist=2, foot=1, pelvis=1]
RR (95% CI): 0.11 (0.01, 2.03); P=0.14
Zoledronic acid
ABCSG-12 31 Fair
1803
GTZ vs GT Median 47.8 months
Fracture, n/N (%)
1/449 (0.2) 1/451 (0.2) RR (95% CI): 1.00 (0.06, 16.01); P=1.00
Fracture (serious event), n/N (%)
4/449 (0.9) 6/451 (1.3) RR (95% CI): 0.67 (0.19, 2.36; P=0.53
GAZ vs GA Fracture, n/N (%)
0/450 (0.0) 1/453 (0.2) RR (95% CI): 0.34 (0.01, 8.22); P=0.50
Fracture (serious event), n/N (%)
7/450 (1.6) 4/453 (0.9) RR (95% CI): 1.76 (0.52, 5.98); P=0.36
GTZ/GAZ vs GT/GA
Fracture, n/N (%)
1/899 (0.1) 2/904 (0.2) RR (95% CI): 0.50 (0.05, 5.53); P=0.57
Fracture (serious event), n/N (%)
11/899 (1.2) 10/904 (1.1) RR (95% CI): 1.11 (0.47, 2.59); P=0.82

78 Systematic review of bisphosphonates in early breast cancer
Study ID Quality N
Comparison (intervention vs control)
Follow-up Outcome Intervention Comparator
Statistical significance
Z-FAST38 Fair
602 Upfront vs delayed zoledronic acid 4 mg IV over 15 minutes every 6 months
3 years
Clinical fracture, n/N (%)
13/300 (4.3) 15/300 (5) RR (95% CI): 0.87 (0.42, 1.79); P=0.70
Significant trauma
11/300 (3.7) 12/300 (4) RR (95% CI): 0.92 (0.41, 2.04); P=0.83
Minimal trauma
2/300 (0.7) 3/300 (1) RR (95% CI): 0.67 (0.11, 3.96); P=0.66
Asymptomatic fracture, n/N (%)
2/300 (0.7) 1/300 (0.3) RR (95% CI): 2.00 (0.18, 21.94); P=0.57
Other fracture, n/N (%)
1/300 (0.3) 2/300 (0.7) RR (95% CI): 0.50 (0.05, 5.48); P=0.57
Radiologic fracture of the spineg, n/N (%)
1/300 (0.3) 1/300 (0.3) RR (95% CI): 1.00 (0.06, 15.91); P>0.99
Total fractures, n/N (%)
17/300 (5.7) 19/300 (6.3) RR (95% CI): 0.89 (0.47, 1.69); P>0.05
ZO-FAST14 Fair
1065
Upfront vs delayed zoledronic acid 4 mg IV over 15 minutes every 6 months
1 year
Fractures, n/N (%)
8/532 (1.5) 9/533 (1.7) RR (95% CI): 0.89 (0.35, 2.29); P=0.81
Abbreviations: CEF, cyclophosphamide, epirubicin, and 5-fluoracil; CI, confidence interval; CMF, cyclophosphamide, methotrexate, and 5-fluoracil; GA, goserelin (3.6 mg s.c. every 28 days) plus anastrozole (1 mg/day orally); GAZ, goserelin (3.6 mg s.c. every 28 days) plus anastrozole (1 mg/day orally) plus zoledronic acid (initially 8 mg IV every 4 weeks); GT, goserelin (3.6 mg s.c. every 28 days) plus tamoxifen (20 mg/day orally); GTZ, goserelin (3.6 mg s.c. every 28 days) plus tamoxifen (20 mg/day orally) plus zoledronic acid (initially 8 mg IV every 4 weeks); IV, intravenous; NA, not applicable; RR, risk ratio; TH, total hip
a Calculated for this technical report using Review Manager 5.
b This represents the safety population rather than the ITT population. c Rib=1; leg=3; arm=2; pelvis=1; spine=6; spine, arm, pelvis, and leg=1; unknown=1. d Rib=2; leg=1; arm=2; spine=2; spine and rib=1; spine and leg=1; unknown=1. e Rib=2; leg=2; spine=3. f Leg=1; arm=2; pelvis=1; spine=4; unknown=3. g Detected with planned 36-month X-ray.

Systematic review of bisphosphonates in early breast cancer 79
5 Clinical practice guidelines
A systematic search was undertaken to identify current recommendations, in existing guidelines, for the use of bisphosphonates in early breast cancer. Appendix D lists the guideline websites searched and the search terms used. Manual searching of reference lists was also performed. Three citations were identified.
5.1 European Society for Medical Oncology (ESMO) 2010
The 2010 ESMO guidelines4 on the diagnosis, treatment, and follow-up of primary breast cancer include the following recommendations regarding the use of bisphosphonates.
Recommendations
Bisphosphonates prevent bone loss in patients with iatrogenic premature menopause and in postmenopausal patients treated with AIs.
Preliminary adjuvant therapy with zoledronic acid and possibly other bisphosphonates may lower the risks of breast cancer recurrence in premenopausal patients treated with endocrine therapy and in postmenopausal patients treated with AIs. For patients who meet these selection criteria the use of adjuvant zoledronic acid may be justified.
There are no data supporting zoledronic acid for patients with oestrogen receptor-negative tumours following chemotherapy.
5.2 New Zealand Ministry of Health 2009
The New Zealand Ministry of Health guidelines43 for the management of early breast cancer include the following recommendations regarding the use of bisphosphonates.
Recommendation (survival)
Due to the lack of consistent evidence no recommendations were made regarding use of oral bisphosphonates for the reduction of osseous metastases in early breast cancer.
Recommendations (BMD)
Women who are osteoporotic and on adjuvant endocrine therapy which enhances loss of bone density or who have undergone premature treatment-induced menopause should receive a bisphosphonate [supported by good evidence*].
Women who are osteopenic and on adjuvant therapy which enhances loss of bone density, or who have undergone premature treatment-induced menopause should be considered for a
* Based on a number of studies that are valid, consistent, applicable and clinically relevant.

80 Systematic review of bisphosphonates in early breast cancer
bisphosphonate, especially in the presence of other risk factors: prior non-traumatic fracture, aged over 65 years, family history, tobacco use, low body weight [expert opinion].
Postmenopausal women taking aromatase inhibitors are recommended to commence treatment with bisphosphonates if the T-score is < -2.0, or < -1.0 in the presence of a vertebral fracture. Secondary causes of osteoporosis should be excluded and standard lifestyle advice on smoking and exercise, calcium supplementation and adequacy of vitamin D intake should also be provided [expert opinion].
Women with premature menopause due to chemotherapy, ovarian function suppression or oophorectomy and postmenopausal women receiving adjuvant therapy with an aromatase inhibitor should have bone density monitored at least every 2 years following a baseline DEXA (dual energy X-ray absorptiometry) scan of the spine and hip [expert opinion].
Frequency of bone mineral density monitoring should be tailored to the individual. If baseline T-score > -1.0 further monitoring of bone density may not be necessary [expert opinion].
A woman with early breast cancer at risk of bone mineral loss should be provided with appropriate advice for good bone health. This includes, but is not limited to: a healthy diet, cessation or continuing abstinence from smoking, maintenance of a healthy body mass index, regular exercise, calcium, and adequate vitamin D levels [expert opinion].
5.3 UK Expert Group* 2008
Guidance for the Management of Breast Cancer Treatment-Induced Bone Loss44 provides a bisphosphonate treatment algorithm based on BMD T-score, menopausal status and AI treatment status. Furthermore, the guidelines include the following recommendations.
Recommendations
All postmenopausal women receiving aromatase inhibitor therapy for the treatment of breast cancer should have an assessment of skeletal risk†.
Bone sparing therapy should be offered to all postmenopausal women receiving aromatase inhibitors for the treatment of breast cancer in whom the fracture risk is deemed to warrant it.
All patients receiving bone sparing therapy should receive supplemental calcium and vitamin D unless the prescribing physician is sure of adequate calcium and vitamin D status‡.
* Reviewed and supported by the National Osteoporosis Society, the National Cancer Research Institute Breast Cancer Study Group, and the International Osteoporosis Foundation. † With exceptions to patients who refuse assessment of skeletal status, patients in whom prognosis is so poor as to make bone sparing treatment unjustified, and patients already receiving bone sparing therapy. ‡ With exceptions to women with hypercalcaemia, sarcoidosis, or a history of renal failure.

Systematic review of bisphosphonates in early breast cancer 81
6 Discussion
A systematic review of the literature identified 13 clinical trials of bisphosphonates as adjuvant treatment of early breast cancer. Three of the trials assessed clodronate, one assessed ibandronate, one assessed pamidronate, three assessed risedronate, and five assessed zoledronic acid. The study populations included both pre- and post-menopausal women, women on chemotherapy, and women on endocrine therapy. In two studies, the population was limited to women with existing osteopenia (but not osteoporosis).
Two studies (Kristensen 200824, ABCSG-1231) reported either disease-free survival, recurrence-free survival, or survival without bone metastasis. The ABCSG-12 trial found that zoledronic acid improves disease-free survival (HR [95% CI] 0.64 [0.46, 0.91]) and recurrence-free survival (HR [95% CI] 0.65 [0.46, 0.92]) in women receiving adjuvant endocrine therapy for hormone-responsive breast cancer31. Kristensen 200824 found no significant difference between pamidronate and standard care in the hazard rate ratio for recurrence in the bone for women receiving either CMF or CEF chemotherapy. The meta-analysis results reported in one systematic review2 demonstrated no statistically significant difference in either bone metastasis-free survival or non-skeletal metastasis-free survival between patients treated with adjuvant clodronate therapy and those receiving no treatment.
The mortality results published in the Cochrane Review on bisphosphonates for breast cancer2 (2007 update) were updated with the results of subsequently published RCTs. The results of the updated meta-analysis indicate that bisphosphonates do not significantly reduce mortality compared with control. The studies, however, were not powered to show significant a difference for this outcome.
Ibandronate and risedronate are well tolerated compared with placebo, and have not been shown in the included studies to significantly increase the incidence of any adverse events. Zoledronic acid use in women undergoing adjuvant endocrine therapy for hormone-responsive breast cancer may increase the incidence of arthralgia, bone pain, cognitive disorder, nausea and vomiting, peripheral nerve disease, fever, and tachycardia; but may reduce the incidence of cutaneous reactions31. In women with early hormone-positive breast cancer receiving adjuvant letrozole, upfront zoledronic acid may decrease the incidence of depression and increase the incidence of fever, bone pain, and headache14,38. One systematic review16 found that zoledronic acid significantly increases the incidence of osteonecrosis of the jaw, a rare adverse event.
Meta-analyses were conducted on the effect of bisphosphonates on cancer recurrence and metastases in early breast cancer using the results of the included RCTs and previously published RCTs (as reported in Mauri 201010). The meta-analysis found that zoledronic acid may reduce the incidence of cancer recurrence. Zoledronic acid had no significant impact on the incidence of metastasis. None of the other bisphosphonates had a significant effect on cancer recurrence or metastasis.
All of the included studies reported BMD and consistently found that short-term use of bisphosphonates (up to four years) significantly reduced the bone loss associated with treatment for early breast cancer. This includes bone loss at the spine, hip, and the femur neck. Clodronate significantly improves LS osteoporosis-free survival, but has demonstrated no significant impact on FN/TFA osteoporosis-free survival11. Zoledronic acid significantly reduced the incidence of osteoporosis compared with control, but found no significant differences in osteoporosis

82 Systematic review of bisphosphonates in early breast cancer
incidence between treatment arms for clodronate, ibandronate, or risedronate. Furthermore, the Z-FAST and ZO-FAST trials found that use of upfront zoledronic acid as an adjunct to endocrine therapy significantly reduces the incidence of osteopenia and osteoporosis compared with delayed zoledronic acid treatment14,38. None of the studies found that bisphosphonates had a significant effect on the incidence of bone fractures. However, the studies were not powered to detect a significant difference for this outcome. The meta-analysis results from one systematic review17 found no significant difference between bisphosphonates and control in the incidence of fracture.
The results of this systematic review should be considered in the context of the included patient populations and their concomitant therapies, the statistical power of the studies, the bisphosphonates used as well as their mode of administration, the length of follow-up, and the pre-2007 clinical evidence.

Systematic review of bisphosphonates in early breast cancer 83
7 Conclusion
Several clinical trials investigating bisphosphonates for women with early breast cancer have been published since the last update of the Cochrane review2 in 2007. Short-term use of bisphosphonates (up to four years) can reduce lumbar spine, hip and femoral neck bone mineral density loss associated with treatment for early breast cancer at follow-up. Zoledronic acid reduces the incidence of osteoporosis; however there is insufficient evidence to demonstrate an effect in other bisphosphonates.
Zoledronic acid may lower the risk of cancer recurrence, and the addition of zoledronic acid to endocrine therapy may increase disease-free survival and recurrence-free survival in premenopausal women. There is no evidence that other bisphosphonates have an effect on cancer recurrence or disease-free survival.
Bisphosphonates are generally associated with mild and infrequent toxicity. Zoledronic acid significantly increases the incidence of osteonecrosis of the jaw; although the overall incidence is low (approximately 0.2% of women taking bisphosphonates).
A number of ongoing trials and unpublished trials are anticipated to provide further information on the efficacy and safety of bisphosphonates in early breast cancer.

84 Systematic review of bisphosphonates in early breast cancer
Abbreviations
AE adverse event
AI aromatase inhibitor
ANZBMS Australian and New Zealand Bone and Mineral Society
ASBMR American Society for Bone and Mineral Research
ASCO American Society of Clinical Oncology
BMD bone mineral density
BMI body mass index
CCO Cancer Care Ontario
CEF cyclophosphamide, epirubicin, and 5-fluoracil
CI confidence interval
CMF cyclophosphamide, methotrexate, and 5-fluoracil
DEXA dual energy X-ray absorptiometry
ECCO European CanCer Organisation
ECOG Eastern Cooperative Oncology Group
EC-TX epirubicin and cyclophosphamide followed by paclitaxel and capecitabine
ER oestrogen receptor
ESMO European Society for Medical Oncology
ETC epirubicin, paclitaxel and cyclophosphamide
FN femoral neck
GA goserelin (3.6 mg s.c. every 28 days) plus anastrozole (1 mg/day orally)
GAZ goserelin (3.6 mg s.c. every 28 days) plus anastrozole (1 mg/day orally) plus zoledronic acid (initially 8 mg IV every 4 weeks)
GIN Guidelines International Network
GT goserelin (3.6 mg s.c. every 28 days) plus tamoxifen (20 mg/day orally)
GTZ goserelin (3.6 mg s.c. every 28 days) plus tamoxifen (20 mg/day orally) plus zoledronic acid (initially 8 mg IV every 4 weeks)
HSA hip structural analysis

Systematic review of bisphosphonates in early breast cancer 85
HR hazard ratio
HRT hormone replacement therapy
ITT intention-to-treat
IU International Unit
IV intravenous
MD mean difference
LS lumbar spine
LSMD least squares mean difference
NA not applicable
NBOCC National Breast and Ovarian Cancer Centre
NCCN National Comprehensive Cancer Network
NGC National Guideline Clearinghouse
NHMRC National Health and Medical Research Council
NICE National Institute for Health and Clinical Excellence
NR not reported
NZMoH New Zealand Ministry of Health
ONJ osteonecrosis of the jaw
OR odds ratio
RCT randomised controlled trial
RR risk ratio
SAE serious adverse event
s.c. subcutaneous
SD standard deviation
SE standard error
SIGN Scottish Intercollegiate Guidelines Network
TFA total femoral area
TH total hip
UGIT upper gastrointestinal tract
UICC Union for International Cancer Control

86 Systematic review of bisphosphonates in early breast cancer
References
1. Australian Institute of Health and Welfare & Australasian Association of Cancer Registries. Cancer
in Australia: an overview, 2010. Cancer series no.60. Cat. no. CAN 56. Canberra: AIHW; 2010.
2. Pavlakis N, Schmidt RL, Stockler MR. Bisphosphonates for breast cancer. Cochrane Database of
Systematic Reviews. 2005(Issue 3. Art. No.: CD003474. DOI: 10.1002/14651858.CD003474.pub2).
3. Brufsky AM. Cancer treatment-induced bone loss: Pathophysiology and clinical perspectives.
Oncologist. 2008;13(2):187-95.
4. Aebi S, Davidson T, Gruber G, Castiglione M. Primary breast cancer: ESMO clinical practice
guidelines for diagnosis, treatment and follow-up. Annals of Oncology. 2010;21(SUPPL. 5):v9-v14.
5. National Breast Cancer Centre. Clinical practice guidelines for the management of early breast
cancer. Canberra: Commonwealth of Australia; 2001.
6. Chin SH & Vedder NB. MOC-PSSM CME article: Metacarpal fractures. Plast Reconstr Surg.
2008;121(1 Suppl):1-13.
7. Brufsky A, Bundred N, Coleman R, et al. Integrated analysis of zoledronic acid for prevention of
aromatase inhibitor-associated bone loss in postmenopausal women with early breast cancer
receiving adjuvant letrozole. Oncologist. 2008;13(5):503-14.
8. NHMRC. How to use the evidence: assessment and application of scientific evidence. Canberra:
Biotext 2000.
9. NHMRC. NHMRC additional levels of evidence and grades for recommendations for developers of
guidelines. Canberra: Biotext 2005.
10. Mauri D, Valachis A, Polyzos NP, et al. Does adjuvant bisphosphonate in early breast cancer
modify the natural course of the disease? A meta-analysis of randomized controlled trials. JNCCN
Journal of the National Comprehensive Cancer Network. 2010;8(3):279-86.
11. Saarto T, Vehmanen L, Blomqvist C, Elomaa I. Ten-year follow-up of 3 years of oral adjuvant
clodronate therapy shows significant prevention of osteoporosis in early-stage breast cancer. Journal
of Clinical Oncology. 2008;26:4289-95.
12. Diel IJ, Jaschke A, Solomayer EF, et al. Adjuvant oral clodronate improves the overall survival of
primary breast cancer patients with micrometastases to the bone marrow: a long-term follow-up.
Annals of Oncology. 2008;19:2007-11.
13. Brufsky A, Harker WG, Beck JT, et al. Zoledronic acid inhibits adjuvant letrozole-induced bone
loss in postmenopausal women with early breast cancer. Journal of Clinical Oncology. 2007;25:829-
36.
14. Bundred NJ, Campbell ID, Davidson N, et al. Effective inhibition of aromatase inhibitor-associated
bone loss by zoledronic acid in postmenopausal women with early breast cancer receiving adjuvant
letrozole: ZO-FAST study results. Cancer. 2008;112(5):1001-10.
15. Ha TC & Li H. Meta-analysis of clodronate and breast cancer survival. British Journal of Cancer.
2007;96(12):1796-801.
16. Mauri D, Valachis A, Polyzos IP, et al. Osteonecrosis of the jaw and use of bisphosphonates in
adjuvant breast cancer treatment: a meta-analysis. Breast Cancer Research and Treatment.
2009;116(3):433-9.
17. Valachis A, Polyzos NP, Georgulias V, Mavroudis D, Mauri D. Lack of evidence for fracture

Systematic review of bisphosphonates in early breast cancer 87
prevention in early breast cancer bisphosphonate trials: A meta-analysis. Gynecologic Oncology.
2010;117(1):139-45.
18. Diel IJ, Solomayer EF, Costa SD, et al. Reduction in new metastases in breast cancer with
adjuvant clodronate treatment. New England Journal of Medicine. 1998;339(6):357-63.
19. Saarto T, Blomqvist C, Virkkunen P, Elomaa I. Adjuvant clodronate treatment does not reduce the
frequency of skeletal metastases in node-positive breast cancer patients: 5-Year results of a
randomized controlled trial. Journal of Clinical Oncology. 2001;19(1):10-7.
20. Powles T, Paterson A, McCloskey E, et al. Reduction in bone relapse and improved survival with
oral clodronate for adjuvant treatment of operable breast cancer [ISRCTN83688026]. Breast Cancer
Research. 2006;8(2).
21. Coleman RE, Thorpe HC, Cameron D, et al. Adjuvant treatment with zoledronic acid in stage II/III
breast cancer. The AZURE trial (BIG 01/04). San Antonio Breast Cancer Symposium. 2010.
22. McCloskey E, Paterson A, Kanis J, Tahtela R, Powles T. Effect of oral clodronate on bone mass,
bone turnover and subsequent metastases in women with primary breast cancer. European Journal of
Cancer. 2010;46(3):558-65.
23. Lester JE, Dodwell D, Purohit OP, et al. Prevention of anastrozole-induced bone loss with monthly
oral ibandronate during adjuvant aromatase inhibitor therapy for breast cancer. Clinical Cancer
Research. 2008;14(19):6336-42.
24. Kristensen B, Ejlertsen B, Mouridsen HT, et al. Bisphosphonate treatment in primary breast
cancer: Results from a randomised comparison of oral pamidronate versus no pamidronate in patients
with primary breast cancer. Acta Oncologica. 2008;47(4):740-6.
25. Hines SL, Mincey BA, Sloan JA, et al. Phase III randomized, placebo-controlled, double-blind trial
of risedronate for the prevention of bone loss in premenopausal women undergoing chemotherapy for
primary breast cancer. Journal of Clinical Oncology. 2009;27(7):1047-53.
26. Greenspan SL, Bhattacharya RK, Sereika SM, Brufsky A, Vogel VG. Prevention of bone loss in
survivors of breast cancer: A randomized, double-blind, placebo-controlled clinical trial. Journal of
Clinical Endocrinology and Metabolism. 2007;92(1):131-6.
27. Greenspan SL, Brufsky A, Lembersky BC, et al. Risedronate prevents bone loss in breast cancer
survivors: A 2-year, randomized, double-blind, placebo-controlled clinical trial. Journal of Clinical
Oncology. 2008;26(16):2644-52.
28. van Londen GJ, Perera S, Vujevich KT, et al. Effect of risedronate on hip structural geometry: a 1-
year, double-blind trial in chemotherapy-induced postmenopausal women. Bone. 2008;43:274-8.
29. van Londen GJ, Perera S, Vujevich KT, et al. The effect of risedronate on hip structural geometry
in chemotherapy-induced postmenopausal women with or without use of aromatase inhibitors: A 2-
year trial. Bone. 2010;46(3):655-9.
30. Van Poznak C, Hannon RA, Mackey JR, et al. Prevention of aromatase inhibitor-induced bone
loss using risedronate: the SABRE trial. Journal of Clinical Oncology. 2010;28(6):967-75.
31. Gnant M, Mlineritsch B, Schippinger W, et al. Endocrine therapy plus zoledronic acid in
premenopausal breast cancer. New England Journal of Medicine. 2009;360(7):679-91.
32. Gnant M, Mlineritsch B, Luschin-Ebengreuth G, et al. Adjuvant endocrine therapy plus zoledronic
acid in premenopausal women with early-stage breast cancer: 5-year follow-up of the ABCSG-12
bone-mineral density substudy. The Lancet Oncology. 2008;9(9):840-9.
88 Systematic review of bisphosphonates in early breast cancer
33. Hershman DL, McMahon DJ, Crew KD, et al. Prevention of bone loss by zoledronic acid in
premenopausal women undergoing adjuvant chemotherapy persist up to one year following
discontinuing treatment. Journal of Clinical Endocrinology and Metabolism. 2010;95(2):559-66.
34. Hines SL, Mincey B, Dentchev T, et al. Immediate versus delayed zoledronic acid for prevention
of bone loss in postmenopausal women with breast cancer starting letrozole after tamoxifen-N03CC.
Breast Cancer Research and Treatment. 2009;117(3):603-9.
35. Powles T, Paterson S, Kanis JA, et al. Randomized, placebo-controlled trial of clodronate in
patients with primary operable breast cancer. Journal of Clinical Oncology. 2002;20(15):3219-24.
36. Powles T, Paterson A, McCloskey E, et al. Erratum: Reduction in bone relapse and improved
survival with oral clodronate for adjuvant treatment of operable breast cancer [ISRCTN83688026]
(Breast Cancer Research). Breast Cancer Research. 2006;8(3).
37. Hershman DL, McMahon DJ, Crew KD, et al. Zoledronic acid prevents bone loss in
premenopausal women undergoing adjuvant chemotherapy for early-stage breast cancer. Journal of
Clinical Oncology. 2008;26(29):4739-45.
38. Brufsky AM, Bosserman LD, Caradonna RR, et al. Zoledronic acid effectively prevents aromatase
inhibitor- associated bone loss in postmenopausal women with early breast cancer receiving adjuvant
letrozole: Z-fast study 36-month follow-up results. Clinical Breast Cancer. 2009;9(2):77-85.
39. Saarto T, Vehmanen L, Virkkunen P, Blomqvist C. Ten-year follow-up of a randomized controlled
trial of adjuvant clodronate treatment in node-positive breast cancer patients. Acta Oncologica.
2004;43(7):650-6.
40. Vehmanen L, Saarto T, Risteli J, et al. Short-term intermittent intravenous clodronate in the
prevention of bone loss related to chemotherapy-induced ovarian failure. Breast Cancer Research
and Treatment. 2004;87(2):181-8.
41. Delmas PD, Balena R, Confravreux E, et al. Bisphosphonate risedronate prevents bone loss in
women with artificial menopause due to chemotherapy of breast cancer: A double-blind, placebo-
controlled study. Journal of Clinical Oncology. 1997;15(3):955-62.
42. Eidtmann H, Bundred NJ, DeBoer R, et al. The effect of zoledronic acid on aromatase inhibitor
associated bone los in postmenopausal women with early breast cancer receiving adjuvant letrozole:
36 months follow-up of ZO-FAST. Cancer Research. 2009;69(2).
43. New Zealand Guidelines Group. Management of early breast cancer. Wellington: New Zealand
Guidelines Group; 2009.
44. Reid DM, Doughty J, Eastell R, et al. Guidance for the management of breast cancer treatment-
induced bone loss: A consensus position statement from a UK Expert Group. Cancer Treatment
Reviews. 2008;34(SUPPL. 1):S3-S18.

Systematic review of bisphosphonates in early breast cancer 89
Appendix A Contributors
Working group members
Bisphosphonates in early breast cancer: a systematic literature review was developed with input from an expert multidisciplinary Working Group with the following members:
Dr Nick Pavlakis Medical Oncologist (Chair)
Dr Peter Barry Surgeon
Ms Denice Bassanelli Consumer Representative
Ms Sholeh Boyle Specialist Breast Nurse
Dr Roslyn Drummond Radiation Oncologist
Dr Belinda Kiely Medical Oncologist
Ms Jenny Macindoe Breast Care Nurse Coordinator
Dr Katrina Moore Breast Surgeon
Ms Marlene Parsons Consumer Representative
Ms Geraldine Robertson Consumer Representative
Dr Bronwyn Stuckey Endocrinologist
National Breast and Ovarian Cancer Centre* staff
The following NBOCC staff were involved in the development of Bisphosphonates in early breast cancer: a systematic literature review:
Ms Sue Sinclair General Manager
Ms Ornella Care Program Manager
Ms Fleur Webster Program Manager
Ms Emma Lonsdale Project Officer
Dr Anne Nelson Evidence Review & Research Leader
Ms Rosemary Wade Senior Project Officer – Research
*In July 2011, National Breast and Ovarian Cancer Centre (NBOCC) amalgamated with Cancer Australia to form a single national agency, Cancer Australia, to provide leadership in cancer control and improve outcomes for Australians affected by cancer.
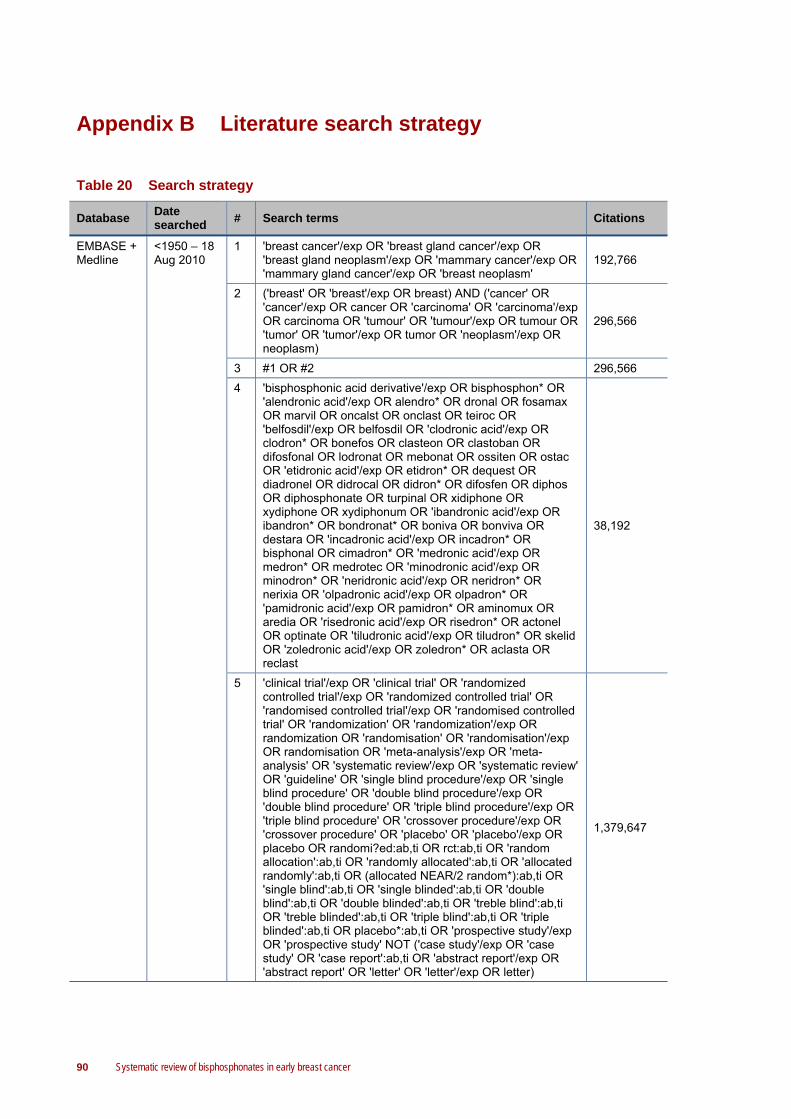
90 Systematic review of bisphosphonates in early breast cancer
Appendix B Literature search strategy
Table 20 Search strategy
Database Date searched
# Search terms Citations
EMBASE + Medline
<1950 – 18 Aug 2010
1 'breast cancer'/exp OR 'breast gland cancer'/exp OR 'breast gland neoplasm'/exp OR 'mammary cancer'/exp OR 'mammary gland cancer'/exp OR 'breast neoplasm'
192,766
2 ('breast' OR 'breast'/exp OR breast) AND ('cancer' OR 'cancer'/exp OR cancer OR 'carcinoma' OR 'carcinoma'/exp OR carcinoma OR 'tumour' OR 'tumour'/exp OR tumour OR 'tumor' OR 'tumor'/exp OR tumor OR 'neoplasm'/exp OR neoplasm)
296,566
3 #1 OR #2 296,566
4 'bisphosphonic acid derivative'/exp OR bisphosphon* OR 'alendronic acid'/exp OR alendro* OR dronal OR fosamax OR marvil OR oncalst OR onclast OR teiroc OR 'belfosdil'/exp OR belfosdil OR 'clodronic acid'/exp OR clodron* OR bonefos OR clasteon OR clastoban OR difosfonal OR lodronat OR mebonat OR ossiten OR ostac OR 'etidronic acid'/exp OR etidron* OR dequest OR diadronel OR didrocal OR didron* OR difosfen OR diphos OR diphosphonate OR turpinal OR xidiphone OR xydiphone OR xydiphonum OR 'ibandronic acid'/exp OR ibandron* OR bondronat* OR boniva OR bonviva OR destara OR 'incadronic acid'/exp OR incadron* OR bisphonal OR cimadron* OR 'medronic acid'/exp OR medron* OR medrotec OR 'minodronic acid'/exp OR minodron* OR 'neridronic acid'/exp OR neridron* OR nerixia OR 'olpadronic acid'/exp OR olpadron* OR 'pamidronic acid'/exp OR pamidron* OR aminomux OR aredia OR 'risedronic acid'/exp OR risedron* OR actonel OR optinate OR 'tiludronic acid'/exp OR tiludron* OR skelid OR 'zoledronic acid'/exp OR zoledron* OR aclasta OR reclast
38,192
5 'clinical trial'/exp OR 'clinical trial' OR 'randomized controlled trial'/exp OR 'randomized controlled trial' OR 'randomised controlled trial'/exp OR 'randomised controlled trial' OR 'randomization' OR 'randomization'/exp OR randomization OR 'randomisation' OR 'randomisation'/exp OR randomisation OR 'meta-analysis'/exp OR 'meta-analysis' OR 'systematic review'/exp OR 'systematic review' OR 'guideline' OR 'single blind procedure'/exp OR 'single blind procedure' OR 'double blind procedure'/exp OR 'double blind procedure' OR 'triple blind procedure'/exp OR 'triple blind procedure' OR 'crossover procedure'/exp OR 'crossover procedure' OR 'placebo' OR 'placebo'/exp OR placebo OR randomi?ed:ab,ti OR rct:ab,ti OR 'random allocation':ab,ti OR 'randomly allocated':ab,ti OR 'allocated randomly':ab,ti OR (allocated NEAR/2 random*):ab,ti OR 'single blind':ab,ti OR 'single blinded':ab,ti OR 'double blind':ab,ti OR 'double blinded':ab,ti OR 'treble blind':ab,ti OR 'treble blinded':ab,ti OR 'triple blind':ab,ti OR 'triple blinded':ab,ti OR placebo*:ab,ti OR 'prospective study'/exp OR 'prospective study' NOT ('case study'/exp OR 'case study' OR 'case report':ab,ti OR 'abstract report'/exp OR 'abstract report' OR 'letter' OR 'letter'/exp OR letter)
1,379,647

Systematic review of bisphosphonates in early breast cancer 91
Database Date searched
# Search terms Citations
6 'meta analysis'/exp OR 'meta analysis' OR 'systematic review'/exp OR 'systematic review' OR 'pooled analysis' OR ('review'/exp OR 'review' AND (systemat* OR pool*))
129347
7 #5 OR #6 1,413,574
8 #3 AND #4 AND #7 AND [2007-2011]/py 893
Cochrane Library
1800 –18 Aug 2010 1
"breast cancer" or "breast gland cancer" OR "breast gland neoplasm" OR mammary cancer" OR "mammary gland cancer" OR "breast neoplasm"
12,061
2 breast AND (cancer OR carcinoma OR tumour OR tumor OR neoplasm)
14,198
3
bisphosphon* OR alendro* OR dronal OR fosamax OR marvil OR oncalst OR onclast OR teiroc OR belfosdil OR clodron* OR bonefos OR clasteon OR clastoban OR difosfonal OR lodronat OR mebonat OR ossiten OR ostac OR etidron* OR dequest OR diadronel OR didrocal OR didron* OR difosfen OR diphos OR diphosphonate OR turpinal OR xidiphone OR xydiphone OR xydiphonum OR ibandron* OR bondronat* OR boniva OR bonviva OR destara OR incadron* OR bisphonal OR cimadron* OR medron* OR medrotec OR minodron* OR neridron* OR nerixia OR olpadron* OR pamidron* OR aminomux OR aredia OR risedron* OR actonel OR optinate OR tiludron* OR skelid OR zoledron* OR aclasta OR reclast
2,192
4 (#1 AND #2 AND #3), from 2007 71

92 Systematic review of bisphosphonates in early breast cancer
Appendix C Conference abstract literature search
Table 21 Conference abstract literature search
Database Date searched
Search terms Relevant citations
ASBMR
1 Jan 2009 – 7 Oct 2010
bisphosphon* OR alendro* OR dronal OR fosamax OR marvil OR oncalst OR onclast OR teiroc OR belfosdil OR clodron* OR bonefos OR clasteon OR clastoban OR difosfonal OR lodronat OR mebonat OR ossiten OR ostac OR etidron* OR dequest OR diadronel OR didrocal OR didron* OR difosfen OR diphos OR diphosphonate OR turpinal OR xidiphone OR xydiphone OR xydiphonum OR ibandron* OR bondronat* OR boniva OR bonviva OR destara OR incadron* OR bisphonal OR cimadron* OR medron* OR medrotec OR minodron* OR neridron* OR nerixia OR olpadron* OR pamidron* OR aminomux OR aredia OR risedron* OR actonel OR optinate OR tiludron* OR skelid OR zoledron* OR aclasta OR reclast
7
ASCO
Annual San Antonio Breast Cancer Symposium
ANZBMS
ECCO
ESMO
Abbreviations: ASBMR, American Society for Bone and Mineral Research; ASCO, American Society of Clinical Oncology; ANZBMS; Australian and New Zealand Bone and Mineral Society; ECCO, European CanCer Organisation; ESMO, European Society for Medical Oncology
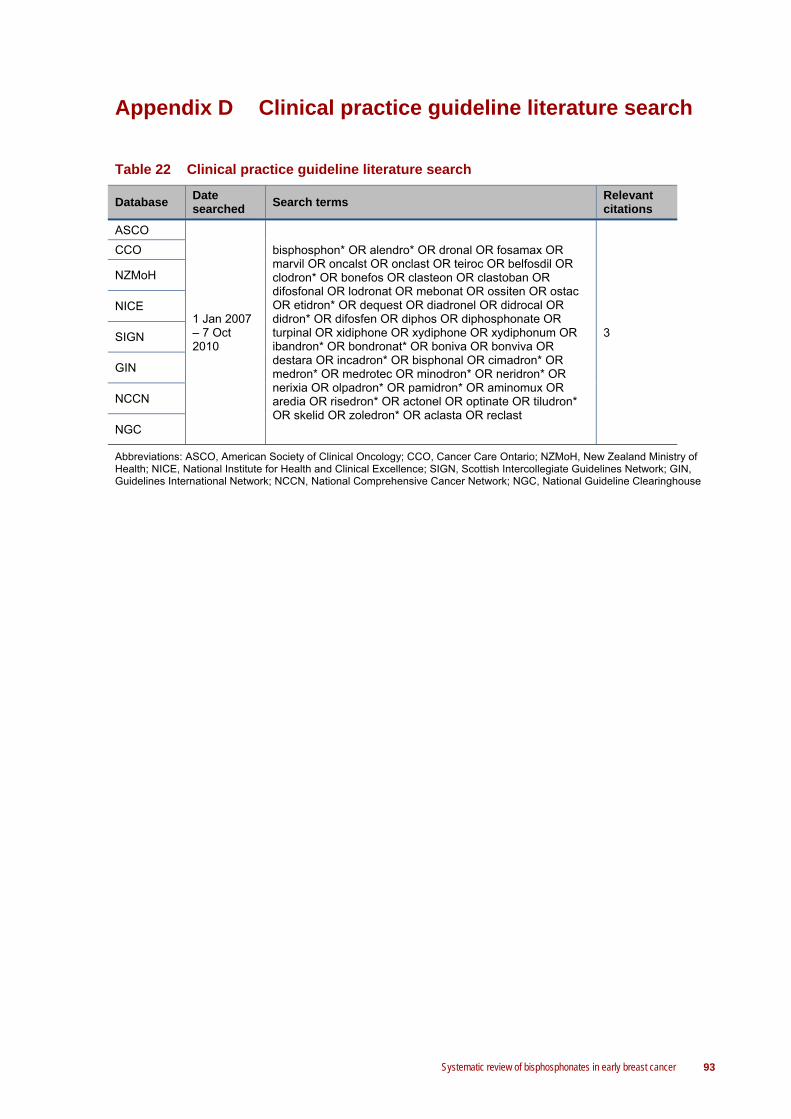
Systematic review of bisphosphonates in early breast cancer 93
Appendix D Clinical practice guideline literature search
Table 22 Clinical practice guideline literature search
Database Date searched
Search terms Relevant citations
ASCO
1 Jan 2007 – 7 Oct 2010
bisphosphon* OR alendro* OR dronal OR fosamax OR marvil OR oncalst OR onclast OR teiroc OR belfosdil OR clodron* OR bonefos OR clasteon OR clastoban OR difosfonal OR lodronat OR mebonat OR ossiten OR ostac OR etidron* OR dequest OR diadronel OR didrocal OR didron* OR difosfen OR diphos OR diphosphonate OR turpinal OR xidiphone OR xydiphone OR xydiphonum OR ibandron* OR bondronat* OR boniva OR bonviva OR destara OR incadron* OR bisphonal OR cimadron* OR medron* OR medrotec OR minodron* OR neridron* OR nerixia OR olpadron* OR pamidron* OR aminomux OR aredia OR risedron* OR actonel OR optinate OR tiludron* OR skelid OR zoledron* OR aclasta OR reclast
3
CCO
NZMoH
NICE
SIGN
GIN
NCCN
NGC
Abbreviations: ASCO, American Society of Clinical Oncology; CCO, Cancer Care Ontario; NZMoH, New Zealand Ministry of Health; NICE, National Institute for Health and Clinical Excellence; SIGN, Scottish Intercollegiate Guidelines Network; GIN, Guidelines International Network; NCCN, National Comprehensive Cancer Network; NGC, National Guideline Clearinghouse