A study of optimal configuration and control of a multi-chamber balloon for intraaortic balloon...
8
Annals of Biomedical Engineering, Vol. 22, pp. 524~531, 1994 009(06964/94 $10.50 + .0t3 Printed in the USA. All rights reserved. Copyright 1994 Biomedical Engineering Society A Study of Optimal Configuration and Control of a Multi-Chamber Balloon for Intraaortic Balloon Pumping JING BAI,* HONG LIN,* ZIBIN YANG,t and XIAOQING ZHOU* *Department of Electrical Engineering, Tsinghua University, tDepartment of Biomedical Engineering, Chinese Institute of Basic Medical Sciences, Beijing, China Abstract--Balloon configuration and control scheme are impor- tant for the optimization of assistance of the failing heart with an intraaortic balloon pumping device. In this work, the configura- tion of a multi-chamber balloon and control schemes have been investigated by using a hemodynamic model and computer sim- ulation methods. Following the simulation study, physical test- ing and animal experiments were performed to demonstrate the simulation results. Results show that the optimal configuration and controlled multi-chamber balloon can provide better assis- tance to the failing heart. Based on the simulation and experi- mental results, it was found that the shape of the rear chamber of a multi-chamber balloon is critical. The optimal control scheme was to inflate the rear chamber first and deflate it last. Keywords--Mathematical modeling, Cardiovascular system, Computer simulation, Cardiac assist device. INTRODUCTION The intraaortic balloon pump is an in-series cardiac assist device. The function of this device is through a balloon placed in the descending aorta that is inflated dur- ing diastole and deflated during systole. With the opera- tion of intraaortic balloon pumping, the coronary flow is increased through the increasing of diastolic pressure in the aortic root. Intraaortic balloon pumping was first in- troduced to the clinic for the treatment of cardiogenic shock (10,11). Today, the use of the intraaortic balloon pump is widespread, and the application of such a device has been broadened to include numerous indications, such as uncomplicated myocardial infarction, prophylaxis in mild to moderate hemodynamic decompensation, postop- erative myocardial failure, unstable angina refractory to maximal medical treatment, recurrent myocardial isch- emia following acute myocardial infarction, intraoperative low cardiac output, postinfarction angina, weaning pa- tients from cardiopulmonary bypass, and ventricular irri- Acknowledgment--This work was supported by the Fok Ying Tung Education Foundation, No. F62. Address correspondence to J. Bai, Department of Electrical Engi- neering, Tsinghua University, Beijing, China, 100084. (Received 31Ju192, Revised 25Mar93, Revised 25Jun93, Accept- ed 9May94). tability resistant to medical treatment after myocardial in- farction (4). In clinical applications, significant variations in the efficacy of intraaortic balloon pumping are often observed, since the design and the operation of the present system have not been optimized. In the past, the closed-loop and optimal control scheme for intraaortic balloon pumping have been extensively studied (1,8,9,14). In respect to balloon configuration, only limited work has been carried out in an early stage (5-7). All these investigations conclude that the configu- ration of the balloon and the control scheme have signif- icant effects on the efficacy of operation. Based on early animal experimental results (5-7), the extra benefits pro- vided by using a multi-chamber balloon configuration have been observed. The purpose of this work is to study the effects of different balloon configurations and to optimize the con- trol of such new configurations. This work includes two parts: an extensive study by using modeling and simula- tion methods and a physical test of the multi-chambered balloon. COMPUTER SIMULATION Methods The model used for computer simulation was based on the canine cardiovascular model developed by Jaron et al. (1). It is a multi-element, nonlinear hemodynamic model that includes 11 aortic segments, a left ventricular part, a right ventricular part, pulmonary circulation, coronary cir- culation, and the lumped venous and peripheral segments. Two physiological feedback control mechanisms have been incorporated into the model. One is the heart rate control, and the other is the venous tone control mecha- nism. The aortic segment model was established based upon the Navier-Stokes equation. Assuming that blood is a Newtonian and incompressible fluid, the radial flow is much smaller than the longitudinal flow, the second time derivative of the longitudinal velocity is negligible, the radii of consecutive segments are related by a decreasing 524
Transcript of A study of optimal configuration and control of a multi-chamber balloon for intraaortic balloon...

Annals of Biomedical Engineering, Vol. 22, pp. 524~531, 1994 009(06964/94 $10.50 + .0t3 Printed in the USA. All rights reserved. Copyright �9 1994 Biomedical Engineering Society
A Study of Optimal Configuration and Control of a Multi-Chamber Balloon for Intraaortic Balloon Pumping
JING BAI ,* HONG LIN,* ZIBIN Y A N G , t and XIAOQING ZHOU*
*Department of Electrical Engineering, Tsinghua University, tDepartment of Biomedical Engineering, Chinese Institute of Basic Medical Sciences, Beijing, China
Abstract--Balloon configuration and control scheme are impor- tant for the optimization of assistance of the failing heart with an intraaortic balloon pumping device. In this work, the configura- tion of a multi-chamber balloon and control schemes have been investigated by using a hemodynamic model and computer sim- ulation methods. Following the simulation study, physical test- ing and animal experiments were performed to demonstrate the simulation results. Results show that the optimal configuration and controlled multi-chamber balloon can provide better assis- tance to the failing heart. Based on the simulation and experi- mental results, it was found that the shape of the rear chamber of a multi-chamber balloon is critical. The optimal control scheme was to inflate the rear chamber first and deflate it last.
Keywords--Mathematical modeling, Cardiovascular system, Computer simulation, Cardiac assist device.
INTRODUCTION
The intraaortic balloon pump is an in-series cardiac assist device. The function of this device is through a balloon placed in the descending aorta that is inflated dur- ing diastole and deflated during systole. With the opera- tion of intraaortic balloon pumping, the coronary flow is increased through the increasing of diastolic pressure in the aortic root. Intraaortic balloon pumping was first in- troduced to the clinic for the treatment of cardiogenic shock (10,11). Today, the use of the intraaortic balloon pump is widespread, and the application of such a device has been broadened to include numerous indications, such as uncomplicated myocardial infarction, prophylaxis in mild to moderate hemodynamic decompensation, postop- erative myocardial failure, unstable angina refractory to maximal medical treatment, recurrent myocardial isch- emia following acute myocardial infarction, intraoperative low cardiac output, postinfarction angina, weaning pa- tients from cardiopulmonary bypass, and ventricular irri-
Acknowledgment--This work was supported by the Fok Ying Tung Education Foundation, No. F62.
Address correspondence to J. Bai, Department of Electrical Engi- neering, Tsinghua University, Beijing, China, 100084.
(Received 31Ju192, Revised 25Mar93, Revised 25Jun93, Accept- ed 9May94).
tability resistant to medical treatment after myocardial in- farction (4). In clinical applications, significant variations in the efficacy of intraaortic balloon pumping are often observed, since the design and the operation of the present system have not been optimized.
In the past, the closed-loop and optimal control scheme for intraaortic balloon pumping have been extensively studied (1,8,9,14). In respect to balloon configuration, only limited work has been carried out in an early stage (5-7). All these investigations conclude that the configu- ration of the balloon and the control scheme have signif- icant effects on the efficacy of operation. Based on early animal experimental results (5-7), the extra benefits pro- vided by using a multi-chamber balloon configuration have been observed.
The purpose of this work is to study the effects of different balloon configurations and to optimize the con- trol of such new configurations. This work includes two parts: an extensive study by using modeling and simula- tion methods and a physical test of the multi-chambered balloon.
COMPUTER SIMULATION
Methods
The model used for computer simulation was based on the canine cardiovascular model developed by Jaron et al.
(1). It is a multi-element, nonlinear hemodynamic model that includes 11 aortic segments, a left ventricular part, a right ventricular part, pulmonary circulation, coronary cir- culation, and the lumped venous and peripheral segments. Two physiological feedback control mechanisms have been incorporated into the model. One is the heart rate control, and the other is the venous tone control mecha- nism.
The aortic segment model was established based upon the Navier-Stokes equation. Assuming that blood is a Newtonian and incompressible fluid, the radial flow is much smaller than the longitudinal flow, the second time derivative of the longitudinal velocity is negligible, the radii of consecutive segments are related by a decreasing
524

Intraaortic Balloon Pumping 525
exponential function, and the velocity profile is parabolic, the pressure-flow relation is (1):
Pn(t) - Pn--l(t) = Ln [dQn( t ) /d t ] + R n Q , ( t ) , (1)
where Pn is the pressure of the nth aortic segment, Qn is the blood flow, and R, and L, represent the effective vis- cous resistance and inertness, respectively. They are de- fined as
R n = (8 ~ /n ) / (~ rn 4) (2)
and
L n = (Pln)/(Trrn2), (3)
where l n is the length of the segment, r n is the radius, p is blood density, and ix is blood viscosity.
The simulated intraaortic balloon has been incorporated into the thoracic aorta segments in the model. To simplify the problem, the effect of the balloon catheter was ne- glected in the computer simulation. For the aortic seg- ments that included the intraaortic balloon, the effective viscous resistance and inertness were obtained from the radius of the vessel and the radius of the balloon, accord- ing to Kuklinski (11), and were defined as follows:
R n = (R0)/[1.333 r b (r n - - rb) 3 + 0.667 X (r n - - rb) 4] (4)
and
L n = (Lo) / ( rn e - rb2), (5)
where R o and L o are constants, and r b is the balloon radius. Based on the work of Suga (13) and Shroff (12), the left
ventricular model used in this work is an extended varying elastance model that includes a series viscous element rep- resenting flow-related pressure drop as follows:
Plv(t) = E ( t ) [ E D V - fred Q l v ( t ) d t - Vo] - R]v (P l v )Q jv ( t ) , (6)
where Ply represents the left ventricular pressure, Qlv rep- resents the left ventricular flow, E ( t ) represents the left ventricular elastance, and R]~ represents the viscous resis- tance. To simulate the failing heart, the maximum elastance of the left ventricle is reduced to be one-third of its normal value.
Similarly, the right ventricular model is
P~v(t) = E ( t ) [Vrv(t) -- Vo], (7)
where Vr~ represents the right ventricular volume, and V o is the volume axis intercept of the end systolic pressure- volume relation line.
The subject of our simulation was a dog with left heart failure. Its heart rate was set to be 120 bpm. The simula- tion model was programmed with PASCAL language. Values for all parameters of the model, where available, were taken from the literature (1,2). The simulation ex-
periments are performed by using an IBM PC/AT com- patible computer. To start the simulation, the initial state of the model had to be set up. Such an initial parameter set was obtained by running the model from an arbitrary ini- tial state for a while until the output of the model was periodic and stable. The model parameters obtained by this initial running were taken as the initial state of the simulation. The time steps for the calculation were chosen to be 0.001 sec of simulation time. During each time interval, the balloon pressure was updated, and a complete segment by segment computation of pressures, flows, and volumes was performed.
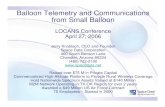
To investigate the effects of different balloon configu- rations, balloons of one chamber, two chambers, and three chambers were used for the simulation experiments. For comparison, the total volume of one, two, and three cham- bered balloon was the same (13 ml). For example, the configuration for a three chambered balloon is shown in Fig. 1. The inflation and deflation of each chamber were through a separate catheter and can be controlled sepa- rately. In the simulation, the input variables were two sets. One was the set of balloon configuration parameters, such as the volume, the diameter, and the length of each cham- ber. Another was the set of control parameters, such as the
(
FIGURE 1. Diagramatic representation of the three chamber balloon configuration.

526 J. BAI et al.
inflating and deflating times for each chamber. To evalu- ate the effectiveness of intraaortic balloon pumping with various configurations and control schemes, five physio- logical parameters were taken to be the output of the sim- ulation. They are listed as follows: mean aortic systolic pressure, MSP; mean aortic diastolic pressure, MDP; the ratio MDP/MSP; total coronary flow per beat, TCF; and end aortic diastolic pressure, EDP.
The simulation was divided into four parts: (1) simu- lation in the absence of intraaortic balloon pumping. These runs were used to validate the model and to provide a baseline for comparison of the technique's effects; (2) simulation using single chamber balloon for comparison; (3) simulation using dual chamber balloon; and (4) simu- lation using three chamber balloon.
In the multi-chamber balloon simulation parts, the op- timal division and control scheme for each balloon con- figuration were evaluated first. The comparisons between these optimized assists were then performed.
-I-
E E
co uJ Q,.
RESULTS
Figure 2 represents aortic pressure, left ventricular pressure, and left ventricular volume produced by our model for canine circulation during heart failure in the absence of intraaortic balloon pumping. When single chamber intraaortic balloon pumping was applied, as shown in Fig. 3, the typical change in aortic pressure was obtained. The aortic pressure without intraaortic balloon pumping is shown in Fig. 3 for comparison. The single chamber balloon's inflating time was adjusted so that the r ise of the balloon pressure was initiated at the dichotic
90 75
E E
GO CO W
O_
8O
7O
6O
5O
4O
3O
2O
I0 0
I" f
/ / V I v
P I v
r I I I I I ~ ] I I I I I I I , I ~ I . . . . I . . . .
0.1 0.2 0.3 0.4 0.5
7O
u J" IE 65 =,
o > >,
60
55
T I M E , sec
FIGURE 2. Computer-generated waveform of aortic pressure, left ventricular pressure, and left ventricular volume wi thout the assist device,
110
100
90
80
70
60
50
40
30
~without assistance +single chamber ~ . ~
t , , , = I , , , ~ t , , , , I , , , I I , , , , I i , = i
0 0.1 0.2 0.3 0.4 0.5 0.6
TIME, sec
FIGURE 3. Computer-generated waveform of aortic pressure with intraaortic balloon pumping using a single chamber bal- loon,
notch. This inflation time is considered to be the optimal time for single chamber balloon pumping and is used as a reference time for the multi-chamber balloon inflation tim- ing. The pumping pressure used was + 300 mm Hg for all simulations presented in this paper. The results shown in Figs. 2 and 3 are in good agreement with the results pre- sented by Jaron et al . (1,2).
For the dual chambered balloon configuration, simula- tion results show that the timing of the rear chamber is important. This is summarized in Table I. For this inves- tigation, the control scheme of the front chamber was the same with the single chamber balloon. The timing of the rear chamber was taken as the relative time to the timing of the front chamber. For example, Tin f = 0.O1 SCC means the rear chamber was inflated 0.01 sec before the inflation of front chamber, where Tin f represents the relative inflat- ing time of the rear chamber and Tde f represents the rela- tive deflating time of the rear chamber. Simulation exper- iments were performed over a range of -+0.05 sec for Tin f and Tde f. From Table 1 we can see that the mean diastolic pressure and coronary flow were increased and the mean systolic pressure and end diastolic pressure were de- creased when the rear chamber was deflated after the front one. In Fig. 4, the effects of volume division are pre- sented. Note that although the total volume was fixed, the optimal volume division occurred when the volume of the rear chamber was 35%-40% of the total volume. In Fig. 5, the effect of the diameter of the rear chamber is pre- sented and shows that the larger the rear chamber's diam- eter is the better the assistance to the failing heart, given a

Intraaortic Balloon Pumping 527
TABLE 1. Influence of the rear chamber inflation or deflation time on the effectiveness of intraaortic balloon pumping.
Inflation or MSP MDP EDP TCF Deflation Time (sec) (mm Hg) (mm Hg) (mm Hg) MDP/MSP (ml/Beat)
- 0.05 63.78 93.43 46.64 1.46 0.35 T i n f - 0.01 68.60 98.97 53.62 1.44 0.36 (sec) 0 67.32 95.71 49.91 1.42 0.35
0.01 65.98 89.96 48.24 1.36 0.33 0.05 64.71 79.41 45,63 1.22 0.28
- 0.05 68.10 93.76 57.60 1.38 0.34 Tdef -- 0.01 67.75 94,64 50.61 1.40 0.35 (sec) 0 66.46 95.64 49.11 1.43 0.35
0.01 66.44 96.66 49.43 1.45 0.36 0.05 64.74 97.84 48.65 1.51 0.36
fixed volume. The simulated diameter of the aorta was 1.6 cm for the case presented in Fig. 5.
Tables 2 and 3 represent the simulation results of the three chamber balloon configurations; the inflation was sequential from tail to tip, and the deflation was sequential from tip to tail with an interval of 0.05 sec. The effects of volume distribution to three chambers are shown in Table 2, in which V], V 2, and V 3 represent the volumes of the front, middle, and rear chambers, respectively. The re- sults suggest that mean diastolic pressure can be maxi- mized and the mean systolic pressure and end diastolic pressure can be minimized when the sum of the volume of the middle and rear chambers is about 40% of the total balloon's volume. Table 3 represents the effects of the diameters of the three chambers, with the volume of each chambers fixed; D a, D 2, and D 3 a r e the diameter of the front, middle, and rear chambers, respectively. This result suggests that a balloon with a rear chamber of large di-
100
90
Z 80 E E u3 m 70 o~
,~ 60
50
MDP ~ - - - ~ - - ~ - ~
MDP/MSP
MSP
40 1
EDP
, , , i . . . . i , j , , / , , ~ , i . . . . i . . . . l a i i i
0.1 0.2 0.3 0.4 0.5 0.6
RATIO OF REAR CHAMBER VOLUME TO TOTAL BALLOON VOLUME
1.8
1.7
1.6
1.5 o. o0 =Z
1.4
1.3
1.2
1.1
FIGURE 4. Model predictions of mean diastolic pressure (MDP), mean systolic pressure (MSP), end diastolic pressure (EDP), and the ratio of MDP to MSP versus the ratio of rear chamber volume to total balloon volume.
ameter can provide better assistance to the failing heart in the sense of increasing diastolic pressure. Simulation re- sults also show that the sequential inflation from tail to tip and sequential deflation from tip to tail constitute the op- timal control scheme for three chamber balloon pumping.
Under the optimal control and configuration, Table 4 represents the comparison of the effects of one, two, and three chamber balloon configurations. From this table, we can see that with the increasing number of balloon cham- bers, the benefits provided by intraaortic balloon pumping are increased, with the total volume of the balloon the same for each configuration.
Figure 6 represents the aortic pressure curves under the effects of two and three chamber intraaortic balloon pump- ing. Comparing the pressure curves shown in Figs. 2, 3, and 6, we can see that the multi-chamber configuration with an optimal control scheme could provide significant
o3 :E Q.
:Z
1.6
1.58
1.58
1.54
1.52
1.5
1.48
1.48 0.6
= r l , ~ , , , I . . . . . . . . . I . . . . . . . . . I . . . . . . . . . J . . . . . . . . . I . . . . . . . . . I
0.8 1 1.2 1.4 1.6 1.8
DIAMETER, cm
FIGURE 5. Model predictions of the ratio of mean diastolic pressure to mean systolic pressure versus the diameter of the rear chamber.

528 J. BAI et al.
TABLE 2. Relations between volume of each chamber of three chamber balloon and intraaortic balloon pumping effectiveness.
V 1 V 2 V 3 MDP MSP EDP V 1 + V 2 No. (ml) (ml) (ml) (mm Hg) (mm Hg) (mm Hg) MDP/MSP V~ + V 2 + V 3
1 2 8 3 89.94 63.59 50.68 1.42 84.62% 2 3 6 4 91.67 61.71 47.90 1.49 76.79% 3 4 5 4 90.76 62.16 47.30 1.46 69.23% 4 6 4 3 92.79 63.96 45.79 1.45 53.85% 5 7 3 3 97.15 61.41 39.71 1.58 46.15% 6 8 3 2 98.05 60.96 43.02 1.61 38.46% 7 9 2 2 97.37 61.64 44.44 1.58 30.76%
improvement to the efficacy of intraaortic balloon pump- ing.
PHYSICAL TESTING
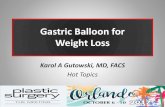
To test the pumping property of the multi-chamber bal- loon, a set of single and dual chamber balloons was pro- duced in our laboratory. Since there was only one intraaor- tic balloon pumping device available for the testing, the unidirectional pumping was realized by a catheter with holes, as illustrated by Fig. 7.
To test physically the uni-directional pumping proper- ties of different balloons, the pumping volume of the tested balloon, both cranially and caudally, was measured in a physical testing device shown in Fig. 7. The tested balloon was inserted into a glass tube of 17 mm diameter that was filled with water and fixed horizontally on the testing table. The balloon was operated by intraaortic bal- loon pumping device (Kontron Model 10; made in U.S.A.), and the pumping volumes, both cranial and cau- dal, were recorded. The data in this table indicate the following phenomena:
1. The volumes displaced in both directions by the single chamber balloon are the same.
2. The diameter of the rear chamber of the dual chamber balloon has to be close to the diameter of the tube to result in greater cranially volume displacement.
3. For those dual chamber balloons whose rear chambers' diameters are larger than the diameter of the glass tube, there is about 85%-90% volume displace cranially,
which indicates that the rear chamber is inflated earlier than the front one.
All these physical testing results agree well with the simulation results.
DISCUSSION
The results of this study suggest that balloon configu- ration and control play an important role in obtaining ben- efits from an intraaortic balloon pumping device. As in- dicated in this study and previous investigations (4), a multi-chamber balloon could provide better assistance to the failing heart. Such a benefit is subjected to the proper control of the balloon pump.
The results of our computer simulation indicate that the tail to tip sequential inflation and the tip to tail sequential deflation is the optimal control scheme for the multi- chamber balloon. With such a control scheme, the rear chamber is inflated first to occlude the down flow of blood. Thus, most of the blood displaced by the balloon has to go upward to the aortic root. Therefore, the dia- stolic aortic pressure is further increased, as well as the coronary flow, as shown in Table 1. Such a control scheme also deflates the rear chamber last, to occlude the blood flow from going to the aortic root at the end of diastole. Thus, this scheme results in a low end diastolic pressure to the left ventricular ejection, therefore, decreas- ing the working load of the failing heart further, as shown in Table 1.
Besides the control scheme, this study indicates that the
TABLE 3. Effect of balloon diameters on intraaortic balloon pumping.
D1 D2 D3 MSP MDP EDP NO. (cm) (cm) (cm) (mm Hg) (mm Hg) (mm Hg) MDP/MSP
1 0.92 0.99 1.60 59.46 94.22 44.32 1.58 2 0.96 0.96 1.60 59.56 94.60 44.34 1.59 3 0.96 1.60 0.96 56.96 85.37 39.63 1.49 4 1.12 1.03 1.18 58.56 88.13 44.34 1.50 5 0.71 1.35 1.60 62.96 93.24 49.25 1.48 6 0.87 1.03 1.60 59.63 93.67 43.89 1.57 7 0.92 1.12 1.26 61.05 91.93 44.63 1.51

Intraaortic Balloon Pumping 529
TABLE 4. Comparison of intraaortic balloon pumping effectiveness under single, dual, and three chamber balloon pumping,
MSP MDP PSP EDP TCF (mm Hg) (mm Hg) MDP/MSP (mm Hg) (mm Hg) (ml/Beat)
Before pumping 73.32 73.35 0.98 82.51 68,54 0.27 Single chamber 66.29 91.52 1.38 80,93 55,33 0.31 Dual chamber 59.83 95.05 1.59 81.98 45.50 0.33 Three chamber 60.81 103.60 1,70 81,31 44.97 0.36
volume distribution has effects on the efficacy of the in- traaortic balloon pumping device. Comparing the simula- tion results presented in Table 2, better assistance can be achieved when the front chamber is larger than the sum of the middle and rear chambers. The results shown in Table 3 tell us that the diameter of the rear chamber is an im- portant parameter for the effect of multi-chamber intraaor- tic balloon pumping. The extra benefits provided by the multi-chamber structure can be realized only when the diameter of the rear chamber is large enough to occlude the aorta.
The simulation results presented in Tables 1 to 4 sug- gest that MDP/MSP is a comprehensive parameter for evaluating the efficacy of intraaortic balloon pumping. As defined in the previous section, MDP/MSP is the ratio of mean diastolic pressure to the mean systolic pressure at the aortic root. The maximum MDP/MSP can be achieved by maximizing the mean diastolic pressure, which can be related to the oxygen supply to the heart, and minimizing the mean systolic pressure, which can be related to the oxygen consumption of the heart. From Table 4, we can
160
140
r 120
E E 100 tr-
40
~- dual chamber ~ t h r e e chamber
0 . . . . I , , h L I I I I I ] i I I [ i , f f I , f r J [
0.1 0.2 0.3 0.4 0.5 0.6
TIME, sec
FIGURE 6. Computer-generated waveform of aortic pressure with intraaortic balloon pumping using dual chamber and three chamber balloons.
see that MDP/MSP increased about 23% compared with the single chamber balloon by using a three chamber bal- loon of the same volume; the coronary flow increased 16%, and the afterload decreased about 8%.
Physical testing demonstrated part of the simulation results. As indicated by the data obtained from physical testing, the dual chamber displaces more blood volume cranially, whereas the single chamber balloon displaces the blood almost equally in both directions. The testing data presented in Table 5 also confirmed the simulation results from the investigation of the effect of the diameter of the rear chamber. The larger the diameter of the rear chamber, the more blood is pushed to the aortic root to aid the coronary circulation. Although physical testing was performed with a rigid tube, which is different from the elastic blood vessel, the results are meaningful in that they demonstrate the relation between balloon configuration and uni-directional pumping effects, since the elastance of the vessel wall is much less than that of the balloon.
Although the work presented here is limited by the facilities available, the simulation results have been par- tially confirmed by physical testing. The results of this work suggest that the optimally controlled and structured multi-chamber balloon configuration may have potential applications in the intraaortic balloon pumping treatment
, , / 1 I *~
I OSCILLOSCORE 'i]
PRESSURE TRANSDUCER
:_, -- .-._-. _ _ ~ - ' - - - '
_ - _
_ _ - - _
~._-- ~ balloon Ta Inixeoo~c Balloon : -- ._:- / Pumping Console
FIGURE 7. Block diagram of the physical testing system.

530 J. BAI et al.
TABLE 5. Physical test ing results.
No.
Diameter Diameter of Front of Rear
Chamber Chamber (mm) (ram)
Percent of Rear Fluid Volume Fluid Volume Chamber Volume Compelled to Compelled to in Total Balloon Aortic Root Distal End
Volume (%) (ml) (ml)
Percentage of Fluid Flow to Aortic Root in Total
Compelled Volume
1 13.9 16.5 2 12.8 17.5 3 13.7 16.2 4 13.2 - - 5 13.7 19.1 6 14.1 19.1 7 13.7 18.9 8 14.1 - - 9 9.7 - -
10 9.9 12.9 11 10.0 14.2 12 9.5 13.2
21.2 12.1 5.9 67.2% 32.2 13.4 3.2 81.7% 4.2 11.9 8.4 58 .6% - - 8.5 8.2 50.9%
25.0 14.2 1.9 88 .2% 42.4 15.8 1.6 90 .8% 21.3 15.3 2.6 85.5% - - 8.8 8.5 50.9% - - 6.2 6.2 50.0%
14.8 5.5 5.3 50.9% 27.1 6.0 5.9 50.4% 39.0 5.5 5.0 52.4%
in the sense of further reducing the working load and providing more energy to the failing heart.
REFERENCES
1. Barnea, O., T. W. Moore, S. E. Dubin, and D. Jaron. Car- diac energy consideration during intraaortic balloon pump- ing. 1EEE Trans. Biomed. Eng. 37:187, 1990.
2. Barnea, O., T. W. Moore, and D. Jaron. Computer simu- lation of the mechanically-assisted failing canine circula- tion. Ann. Biomed. Eng. 18:263, 1990.
3. Barnea, O. Cardiovascular dynamics and the intraaortic bal- loon pump: optimization based on cardiac oxygen balance. Ph.D. Thesis, Drexel University, Philadelphia, Pennsylva- nia, 1987.
4. Bolooki, H. Clinical Application of Intraaortic Balloon Pump. Mount Kisco, New York, Futura, 1984.
5. Bregman, D., and R. H. Goetz. Clinical experience with a new cardiac assist device: the dual-chambered intraaortic balloon assist. J. Thorac. Cardiovasc. Surg. 62:577, 1971.
6. Bregman, D., D. C. Kripke, and R. H. Goetz. The effect of synchronous unidirectional intraaortic balloon pumping on hemodynamics and coronary blood flow in cardiogenic shock. Trans. Am. Soc. Artif. Intern. Organs 16:439, 1970.
7. Buckley, M. J., J. D. Laird, P. N. Madras, R. T. Jones, A. R. Kantrowitz, and W. G. Austen. Left heart assist system: intraaortic balloon pump. Surg. Clin. North Am. 49:505, 1969.
8. Jaron, D., T. W. Moore, and P. He. Control of intraaortic balloon pumping: theory and guidelines for clinical applica- tion. Ann. Biomed. Eng. 13:155, 1985.
9. Jaron, D., T. W. Moore, and P. He. Theoretical consider- ations regarding the optimization of cardiac balloon pump- ing. 1EEE Trans. Biomed. Eng. 30:177, 1983.
10. Kantrowitz, A., F. Tjonneland, P. S. Freed, S. J. Philips, A. N. Butner, and J. F. Sherman, Jr. Initial clinical expe- rience with intraaortic balloon pumping in cardiogenic shock. J. Am. Med. Assoc. 203:135, 1968.
11. Kuklinski, W. S., D. Jaron, W. J. Ohley, and R. K. Gree- nail Jr. The intraaortic balloon pump: a non-linear digital computer mode/. Trans. ASME 106:220, 1980.
12. Shroof, S. G. Evidence and quantitation of left ventricular systolic resistance. Am. J. Physiol. 249:358, 1985.
13. Suga, H., and K. Sagawa. Instantaneous pressure-volume relationships and their ratio in the excised, supported canine left ventricle. Circ. Res. 35:117, 1974.
14. Zelano, J. A., J. K-J. Li, and W. Welkowitz. A closed- loop control scheme for intraaortic balloon pumping. IEEE Trans. Biomed. Eng. 37:170, 1990.
O 1
D 2 = D 3 = E =
E D V =
E D P =
L n =
I n = M D P =
M S P =
Plv =-
Pn =
Pry =
Qlv Q, =
Rlv =
Rn
F b
T C F
Zdef
Zinf te~ Vo
W 1
v~ v3
tx
P
NOMENCLATURE
diameter of the front chamber (cm) diameter of the middle chamber (cm) diameter of the rear chamber (cm) ventricular pressure/volume ratio (mm Hg �9 m l - 1)
ventricular end diastolic volume (ml) aortic end diastolic pressure (ram Hg) effective inertness (mm Hg sec 2 �9 m l - 1 ) length of the segment (cm) mean diastolic pressure (mm Hg) mean systolic pressure (mm Hg) left ventricular pressure (mm Hg) blood pressure (mm Hg) right ventricular pressure (mm Hg) left ventricular flow (ml �9 sec -~) blood flow (ml �9 sec -1 ) myocardial viscous forces (mm H g . m l - a . sec) effective viscous resistance (mm Hg �9 m l - 1 . sec)
radius of balloon (cm) total coronary flow (ml) time of deflation (sec) time of inflation (sec) time of end diastole (sec) volume axis intercept of end systolic pressure volume relation (ml) volume of the front chamber (ml) volume of the middle chamber (ml) volume of the rear chamber (ml) volume of right ventricle (ml) blood viscosity (dyn �9 c m - 2 . sec) blood density (Pa �9 sec)

lntraaortic Balloon Pumping 531
APPENDIX
The parameters in the computer simulation are listed in Table A and Table B, which are adopted from Barnea (3).
TABLE A. Values of the parameters for 11 aortic segments.
Segment Length R o L 0 Number (cm) (mm Hg -sec . cm) (mm Hg �9 sec 2 �9 cm 1)
1-3 2.0 0.00116 0.001075 4-6 4.5 0.00224 0.00187 7-9 4.0 0.00199 0,00166 10 6.0 0.00299 0.00249 11 4.0 0.00199 0.00166
Ro = Rnrn", Lo = /nrn 2, r n iS the radius of the aortic segments, which varies with time.
TABLE B. Values of the parameters for peripheral circulation.
R1 R 2 C Segment Name (mm Hg-sec -m1-1 ) (mm H g . s e c - m l 1) ( m l . m m Hg 1)
Right subclavian artery Cerebral circulation Left subclavian artery Hepatic and abdominal circulation Renal circulation Splanchnic circulation
10.40 41.60 0.066 5.275 16.0 0.16
10.40 41.60 0.066 5.63 22.2 0.053 3.53 11.1 0.04 3.0 12.0 0.16
R 1, C, and R 2 represent arterial resistance, compliance, and capillary resistance, respectively.