
A series maxillofacial tumours Nigeria - Europe...
7
Annals of the Royal College of Surgeons of England (I977) vol 59 A series of maxillofacial tumours from Nigeria M B Edwards FDSRCS G D Roberts FDSRCS* Department of Dental Science, Royal College of Hospital, York. Introduction The Ahmadu Bello University Hospital in Kaduna, Nigeria, contains a maxillofacial unit which receives military and civilian patients referred from local hospitals within a radius of several hundred miles. Oral surgeons from Britain, usually in senior training grades at the Queen Victoria Hospital, East Grinstead, may take up a 6-month rotational appointment in Kaduna. This post provides wide-ranging ex- perience in maxillofacial surgery and post- operative management, including the treat- ment of neoplasia, which is often advanced when first seen. From time to time surgical biopsy material is made available to the De- partment of Dental Science at the Royal Col- lege of Surgeons of England for diagnosis and research. Amongst this material there are frequently rare or unusual lesions which raise basic problems of pathogenesis and differential diagnosis. A large series of tumours from a similar source in Ibadan has been described by Anand, Davey, and Cohen', whose purpose was in part to assess the relative frequency of jaw neoplasms in Nigeria. The intention of the present paper is to describe a small series of uncommon maxillofacial lesions which illustrate aspects of diagnosis in surgical patho- logy and histopathology. Case I- Orbital alveolar rhabdomyo- sarcoma A 24-year-old boy had a left suborbital swelling of uncertain duration, progressive proptosis, and up- ward displacement of the eye (Fig. ia). The tumour was not attached to skin but was fused to tissue with- in the orbit. There were no jaw lesions, but a pro- visional diagnosis of Burkitt's lymphoma was made *Formerly seconded to the Maxillofacial Unit, Ahmadu Bello University Hospital, Kaduna, Nigeria. Surgeons of Enigland, and County and treatment with intravenous cyclophosphamide started. This produced little response and in the absence of multiple primary or metastatic disease surgical removal was attempted. The suborbital mass could be dissected free, but a deep extension approached the optic nerve and was inoperable. Microscopic examination revealed the features typical of the alveolar variant of rhabdomyosarcoma (Fig. i b). Orbito-ocular tumours are more common in African than Caucasian children2, and in Ni- geria the pattern of their frequency is dominated by the high incidence of retinoblastoma and of orbital lesions in the syndrome of Burkitt's lymphoma3. In contrast to selected American populations4, in which it is the most common orbital malignancy of chilahood, rhabdomyo- sarcoma has been rarely found in this site in Nigeria3. In the early stages of the disease it may be difficult to distinguish between orbital Burkitt's lymphoma and other tumours without biopsy. Except in rare instances of involvement of the lachrynal gland the lymphoma extends from an adjacent focus within bone5, but this may not be easily demonstrated. Orbital rhabdomyosarcoma is also extraocular in origin FIG. I Case I, alveolar rhabdomyosarcoma: (a) orbital tumour composed of (b) pleomor- phic mesenchymal cells lining pseudoalveolar spaces. (Haematoxylin and eosin X 6o)
Transcript of A series maxillofacial tumours Nigeria - Europe...

Annals of the Royal College of Surgeons of England (I977) vol 59
A series of maxillofacial tumours from Nigeria
M B Edwards FDSRCS
G D Roberts FDSRCS*Department of Dental Science, Royal College ofHospital, York.
IntroductionThe Ahmadu Bello University Hospital inKaduna, Nigeria, contains a maxillofacial unitwhich receives military and civilian patientsreferred from local hospitals within a radiusof several hundred miles. Oral surgeons fromBritain, usually in senior training grades at theQueen Victoria Hospital, East Grinstead, maytake up a 6-month rotational appointment inKaduna. This post provides wide-ranging ex-perience in maxillofacial surgery and post-operative management, including the treat-ment of neoplasia, which is often advancedwhen first seen. From time to time surgicalbiopsy material is made available to the De-partment of Dental Science at the Royal Col-lege of Surgeons of England for diagnosisand research. Amongst this material there arefrequently rare or unusual lesions which raisebasic problems of pathogenesis and differentialdiagnosis.A large series of tumours from a similar
source in Ibadan has been described byAnand, Davey, and Cohen', whose purposewas in part to assess the relative frequencyof jaw neoplasms in Nigeria. The intentionof the present paper is to describe a small seriesof uncommon maxillofacial lesions whichillustrate aspects of diagnosis in surgical patho-logy and histopathology.
Case I- Orbital alveolar rhabdomyo-sarcomaA 24-year-old boy had a left suborbital swelling ofuncertain duration, progressive proptosis, and up-ward displacement of the eye (Fig. ia). The tumourwas not attached to skin but was fused to tissue with-in the orbit. There were no jaw lesions, but a pro-visional diagnosis of Burkitt's lymphoma was made
*Formerly seconded to the Maxillofacial Unit,Ahmadu Bello University Hospital, Kaduna, Nigeria.
Surgeons of Enigland, and County
and treatment with intravenous cyclophosphamidestarted. This produced little response and in theabsence of multiple primary or metastatic diseasesurgical removal was attempted. The suborbitalmass could be dissected free, but a deep extensionapproached the optic nerve and was inoperable.Microscopic examination revealed the features typicalof the alveolar variant of rhabdomyosarcoma (Fig. i b).
Orbito-ocular tumours are more common inAfrican than Caucasian children2, and in Ni-geria the pattern of their frequency is dominatedby the high incidence of retinoblastoma andof orbital lesions in the syndrome of Burkitt'slymphoma3. In contrast to selected Americanpopulations4, in which it is the most commonorbital malignancy of chilahood, rhabdomyo-sarcoma has been rarely found in this site inNigeria3. In the early stages of the disease itmay be difficult to distinguish between orbitalBurkitt's lymphoma and other tumours withoutbiopsy. Except in rare instances of involvementof the lachrynal gland the lymphoma extendsfrom an adjacent focus within bone5, but thismay not be easily demonstrated. Orbitalrhabdomyosarcoma is also extraocular in origin
FIG. I Case I, alveolar rhabdomyosarcoma:(a) orbital tumour composed of (b) pleomor-phic mesenchymal cells lining pseudoalveolarspaces. (Haematoxylin and eosin X 6o)

40 M B Edwlards and G D Roberts
and may cause similar proptosis and extrusionof the globe. The embryonal variant, whichmay not originate in striped muscle, is morecommon in the orbit and nasopharynx; thealveolar form shown here more frequentlyarises from the striped muscle of theextremities, but orbital lesions may arise inthe extraocular musculature'. A clinical dis-tinction between the twvo forms of rhabdomyo-sarcoma in the orbit is borne out by this case.Proptosis caused by the embryonal form issaid4 to be associated with downward displace-ment and that caused by the alveolar formwith upward displacement.
Case 2 - Papillary adenocarcinoma,primary or metastaticA 46-year-old man had a hard, fusiform swelling ofthe left check which elevated both buccal mucosaand skin from the ascending mandibular ramus tothe labial commissure. This had been present formany years with gradual, symptomless increase insize. Supcific al ulceration had recently occurredover the intraoral mass. Local lymph nodes werenot palpable. The tumour was dissected free froman intraoral approach; sections showed a papillaryepithelial neoplasm, parts of which had a cyst-adenomatous structure. The cytological characteristicswere uniform and there was little mitotic activity,but the lesion was not encapsulated and infiltrationapproached both skin and mucous membrane. Sali-vary tissue was not apparent in the samples. Thetumour was associated with inflammatory infiltration,but it was not distinctly within a lymph node. Oneyear later an enlarged, hard, left upper cervical lymphnode which had been noted for 2 months was re-moved. There was no evidence of recurrent intra-oral lesions. The lymph niode was overrun by aniidentical papillary neoplasm (Fig. 2) with more overtlymalignant cytological characteristics. After anotheryear a similar lymph node, infiltrated by papillaryadenocarcinoma, was found close to the excision siteagain in the absence of intraoral tumour. Ten monthslater a small semicystic lesion was founid in the leftcheek, with enlarged upper left and right cervicalnodes. Each hr.d similar histological appearances tothe previous les'ons. Over the past 2 years a largebuccal mass has recurred, further cervical nodes haveenlarged conflu ntly, and there is radiological evi-dence of lung rmetastasis.Minor salivary glands are the most obvious
site of origin for intraoral papillary cystaden-oma or adenocarcinoma. In the cheek, if thebuccinator is breached, the possibility of anorigin in sweat glands must be considered andmay be difficult to exclude on histologicalgrounds. How.ever, salivary cystadenoma, ex-
cept when arising within the lymphoid tissuetypical of Warthin's tumour, is an uncommonlesion of debatable histogenesis . The reviewby Allen, Fitz-Hugh, and Marsh' indicatesthat papillary adenocarcinoma of minor sali-vary origin is also infrequently described.
Because of the comparative rarity of thisgroup of tumours the finding of a pure papillarygrowth in oral soft tissues, unless a local origincan unequivocally be demonstrated, shouldraise the sur picion of metastatic disease. In thehead and neck the thyroid is the major site ofprimary papillary carcinoma. Characteristicallythis tumour exhibits slow growth withsequential and occasionally bilateral spread tocervical nodes; the primary lesion may be in-apparent. Regional metastasis before cervicalnode involvement is rarely reported and in theabsence of thyroid enlargement in the presentcase (scintiscan is not available) it may seemfar-fetched to suggest a thyroid origin. However,there are features which favour this view, par-ticularly the marked histological resemblance,the indolent growvth pattern, and the bilateralspread to lymph nodes. In addition, a nearidentical pattern of disease has recently beenobserved in biopsy specimens submitted fromanother source. In this case the first detectablelesion was also wvithin the cheek and enlargedlymph nodes were not found until some timelater. Subsqtuently a latent thyroid primarywas revealed by scintiscan.
FIG. 2 Case 2, part of metastatic deposit ofpapillary adenocarcinoma within cervicallymph node. (Haematoxylin and eosin X 37.5)
A series of maxillofacial tumours from Nigeria
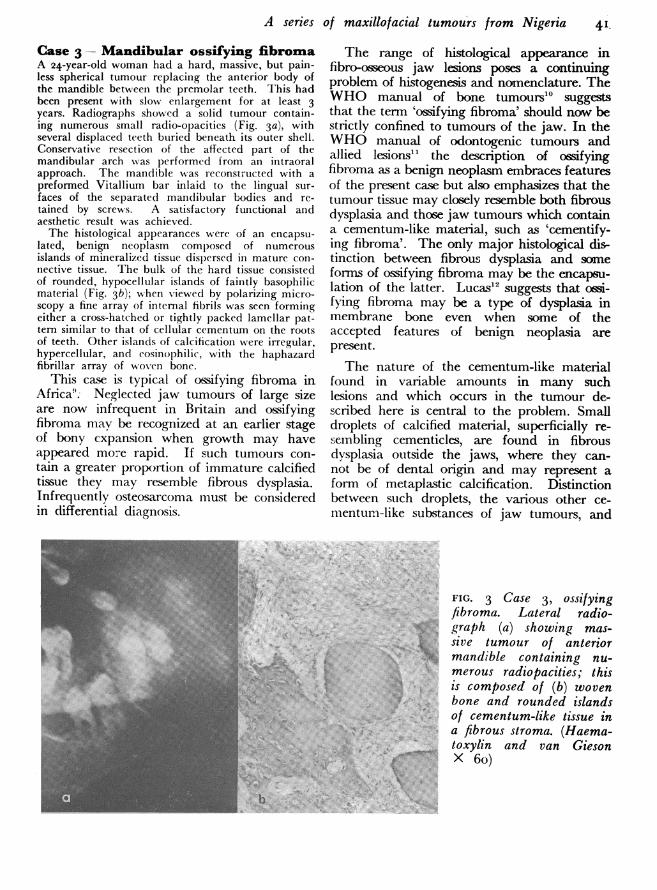
Case 3- Mandibular ossifying fibromaA 24-year-old woman had a hard, massive, but pain-less spherical tumour replacing the anterior body ofthe mandible between the premolar teeth. This hadbeen present with slow enlargement for at least 3years. Radiographs showed a solid tumour contain-ing numerous small radio-opacities (Fig. 3a), withseveral displaced teeth buried beneath its outer shell.Conservative resection of the affected part of themandibular arch w,as performed from an intraoralapproach. The mandible w as r-econstructed with apreformed Vitallium bar inlaid to the lingual sur-faces of the separated mandibular bodies and re-tained by screws. A satisfactory functional andaesthetic result was achieved.The histological appearances were of an encapsu-
lated, benign neoplasm composed of numerousislands of mineralized tissue dispersed in mature coIn-nective tissue. The bulk of the hard tissue consistedof rounded, hypocellular islands of faintly basophilicmaterial (Fig. 3b); when viewed by polarizing micro-scopy a fine array of internal fibrils was seen formingeither a cross-hatched or tightly packed lamellar pat-tern similar to that of cellular cementum on the rootsof teeth. Other islands of calcification were irregular,hypercellular, and cosinophilic, with the haphazardfibrillar array of w oven bone.
This case is typical of ossifying fibroma inAfrica9. Neglected jaw tumours of large sizeare now infrequent in Britain and ossifyingfibroma mav be recognized at an earlier stageof bony expansion when growth may haveappeared more rapid. If such tumours con-tain a greater proportion of immature calcifiedtissue they may resemble fibrous dysplasia.Infrequently osteosarcoma must be consideredin differential diagnosis.
The range of histological appearance infibro-osseous jaw lesions poses a continuingproblem of histogenesis and nomenclature. TheWHO manual of bone tumours'0 suggeststhat the term 'ossifying fibroma' should now bestrictly confined to tumours of the jaw. In theWHO manual of odontogenic tumours andallied lesions'1 the description of ossifyingfibroma as a benign neoplasm embraces featuresof the present case but also emphasizes that thetumour tissue may closely resemble both fibrousdysplasia and those jaw tumours which containa cementum-like material, such as 'cementify-ing fibroma'. The only major histological dis-tinction between fibrous dysplasia and someforms of ossifying fibroma may be the encapsu-lation of the latter. Lucas'2 suggests that ossi-fyring fibroma may be a type of dysplasia inmembrane bone even when some of theaccepted features of benign neoplasia arepresent.The nature of the cementum-like material
found in variable amounts in many suchlesions and which occurs in the tumour de-scribed here is central to the problem. Smalldroplets of calcified material, superficially re-scibling cementicles, are found in fibrousdysplasia outside the jaws, where they can-not be of dental origin and may represent aform of metaplastic calcification. Distinctionbetween such droplets, the various other ce-menturn-like substances of jaw tumours, and
FIG. Case 3, ossifyingfibroma. Lateral radio-. graph (a) showing mas-sive tumour of anteriormandible containing nu-merous radiopacities; thisis composed of (b) woven
' bone and rounded islandso.of cementum-like tissue in
10@s4e#B 'B'Am. &^ a fibrous stroma. (Haema-toxylin and van GiesonX6o)
41,
-Pi

42 AM B Edwards and G D Roberts
bone can be attempted by polarizing micro-scopy1', and such studies have endorsed theview that some benign fibro-osseous lesions ofthe jaw might evolve from the specializedtissue of the periodontal ligament. As suchthey might properly contain both dentalcementum and bone but are entirely distinctfrom fibrous dysplasia. The classification"9 oflesions based upon this hypothesis ranges fromreactive to neoplastic.The classic concept of monostotic fibrous
dysplasia as a benign, self-limiting condition ofadolescent subjects remains a valid basis forseparating it from other fibro-osseous lesions.There can be little doubt that there is a sep-arate if heterogeneous group of fibro-osseouslesions with the clinical attributes of benignneoplasia. The major point at issue is the extentto which the variety of fibro-osseous lesionsmight share a common histogenesis. Rarelyjaw lesions with histological features of fibrousdysplasia may behave as locally aggressivetumours and require radical treatment. Con-versely fibro-osseous lesions with the neoplasticattributes of ossifying fibroma may, while dis-playing continuous if slow growth, undergointernal maturation, perhaps to form the typeof tumour described here, which contains alarge amount of differentiated or inert materialresembling cementum. Amongst this group oflesions it seems unlikely that a nomenclatureof prognostic benefit will be devised from his-tology alone unless the basic problem of their
pathogenesis can be resolved.
Case 4 -Gigantiform cementomaA 28-year-old woman complained of progressiveenlargement and discomfort in the anterior mandibleover the course of 5 years. Several teeth in the in-cisor and premolar quadrants were missing and an-teriorly there was bony-hard expansion of the eden-tulous alveolar process and mucosal ulceration, re-vealing part of a yellow sequestrum-like mass. Radio-graphs showed much of the cancellous bone of the bodyof the mandible to be replaced by dense, lobulatedmasses of hard tissue, some of which fused with theroots of the remaining teeth (Fig. 4a). Similar masses,free of symptoms, were shown bilaterally in themaxilla. Surgery was undertaken as for mandibularsequestrectomy, when it was found possible to cleavethe hard tissue easily from the surrounding bone.The maxilla was left untreated. There was blood lossrequiring transfusion but a satisfactory recovery.The microscopic appearances (Fig. 4b) were of
solid, hypercalcified tissue enclosing tiny spaces filledwith delicate fibrous tissue. The hard tissue had fewentrapped cells and many lacunae were empty;there were few resting or reversal lines. There wasa resemblance to sclerotic bone or atypical cementum.The periphery of the masses was partly lobulated andadjacent connective tissue was chronically inflamedand contained new bone and cementicles. Whenviewed by polarizing microscopy the pattem ofintrinsic fibre bundles did not closely correspond tothat of bone, even when compact or sclerotic. Fibreswere arranged either in narrow, parallel lamellae(Fig. 4c) or in a random, cross-hatched fashion. Thesepattems are found in secondary or cellular cementumof the teeth'3 14The clinical features in this case conform to
those of an unusual entity described asgigantiform cementoma or familial multiple
FIG. 4 Case 4, gigantiformsrF(7 cementoma. Lateral radio-
graph (a) showing severalsclerotic masses in mandible,some fused with roots of non-carious teeth; these are com-
*.. i)'( posed of (b) sclerotic calcifiedtissue with smooth, inertmargins, few resting lines,
:- -CK * and many empty lacunae.(Haematoxylin and vanGieson X 37.5) By polarizingmicroscopy (c) intrinsic fibrebundles are shown to formnarrow lamellae of parallelfibres which resemble sec-ondary cementum.

A series of maxillofacial tumours from Nigeria
cementomas according to the classification ofPindborg, Kramer, and Torloni". A familialpattern of disease has been found only in aminority of cases. Most of the few reportedcases have been in middle-aged AmericanNegro women, but this confined incidence mayreflect both inadequate sample size anddiagnostic confusion. Many lesions of the jawspreviously decribed as sclerosing osteomyelitis'5or multiple enostosis may better fit into thecategory of gigantiform cementoma. Suchlesions are often chronic, multiple, and symp-tomless enlargements. The intervention ofosteomyelitis and sequestration is a secondaryfeature, subsequent to progressive diminutionof the blood supply to the dense tissue.As in Case 2, histological interpretation re-
quires the recognition of cementum outside itsnormal anatomical distribution on the rootsurface. In gigantiform cementoma themineralized tissue is described as fused massesof acellular, lobulated cementum bodies", saidto be distinguishable from bone by routinemicroscopy. However, as in the present case,there may be a resemblance in parts to scleroticbone and to cellular cementum'6. Discrimin-ation between bone and cementum may beattempted by polarizing microscopy, but thisprocedure is not yet accepted as definitive.Since dental cementum is a modified form ofbone it is highly probable that types of hard
tissue transitional between the two can occurin the jaws, and these may partly account forthe confusing range of appearances in fibro-osseous lesions.The diagnosis of gigantiform cementoma
rests upon the combination of clinical andhistological features. These strongly suggestthat the lesion is dysplastic rather than neo-plastic, warranting symptomatic, conservativetreatment. The danger of superimposed osteo-myelitis may be of greater clinical significancethan the disease itself. Rarely masses ofcementum-like tissue may arise in Paget'sdisease of the jaws, and appropriate biochemi-cal tests and skeletal radiographs may be em-ployed in differential diagnosis"7. Since thepathogenesis of gigantiform cementoma isobscure it could be wrong at this stage to dis-miss it as entirely unconnected with localizedPaget's disease, but it may be equally wellregarded as part of the spectrum of lesions ofperiodontal ligament origin'6.Case 5 Mandibular juxtacorticalosteosarcomaA 35-year-old man was first seen with a hard swellingof the buccal surface of his edentulous mandible fromthe left to the right first molar region. This hadbeen present for 4-5 years, causing mild discomfort.The mass was excised leaving the mandible intact;tissue was not submitted for microscopic examinationand the clinical diagnosis was 'peripheral ossifyingfibroma'. Twsro months later he retumed with a
FIG. 5 Case 5, juxtacortical osteosarcoma. Lateral radiograph (a) showing diffuse parosteal massgripping body of mandible and spreading anteriorly. The core of this mass is composed ofsclerotic bone and cartilage (b) and at the periphery (c) there is neoplastic bone in malignantmesenchyme. (Haematoxylin and eosin X 37.5)
43

44 M B Edwards and G D Roberts
painful, granulating swelling of the anterior mandiblewhich again was excised. The histological appearancewas of 'reparative and granulation tissue. Tlhreemonths later a hard, lobulated mass was palpable inthe right cheek and radiographs showed calcified tissuewithin this and a diffuse periosteal thickening overmuch of the mandible. At operation the buccal masswas found to be firmly attached to bone by a broadpedicle continuous with a thick, fibrous, and partlycalcified plaque arising from periosteum over thegreater part of the mandibular body. The underlyingbone appeared slightly resorbed but essentially corticalin character. The microscopic appearances were offocal tumour bone formation in tissue which other-wise resembled a low-grade fibrosarcoma, enclosingcentrally a complex of beam-like trabeculae of non-neoplastic bone. One year later the patient returnedwith a similar mass in the cheek which was bony-hard and firmly attached to the mandible. Themandibular body was again enlarged by a para-cortical mass of tissue with a softer consistency.Radiographs (Fig. 5a) showed a sclerotic bony massin the exophytic part of the lesion, and the normalcontour of the horizontal ramus was obscured byparosteal deposition of bone with a dense, indistinctlytrabecular structure.
Surgical removal was attempted as a 'deglovingprocedure. The. tumour could be dissected easilyfrom the mandible, leaving it intact, but the outerlimits were difficult to define because of soft-tissueinfiltration. A large sample became available forhistological examination. The deepest part of thejuxtacortical mass was the most calcified and con-sisted of sclerotic bone arranged in long, paralleltrabeculae (Fig. 5b) enclosing a fibrous stroma whichexhibited some cellular atypia. There were also fociof neoplastic cartilage and patchy endochondral ossi-fication. At the outer, infiltrative margin of thelesion cytological characteristics of malignancy weremore obvious and there were areas of fibrosarco-matous tissue in which tumour bone was formingwithin condensations of malignant mesenchyme(Fig. 5c).The clinical, radiographic, and histological
features suggest that this was an osteosarcomaof juxtacortical or parosteal origin. Typicallythese tumours occur in the femur or humerusof young adults, and mandibular lesions areeither exceedingly rare or insufficiently rec-ognized, for there are few case reports", ". Thedistinction between endosteal and juxtacorticalosteosarcoma is not academic and the exampleof this case suggests that clinical characteristics,differential diagnosis, and prognosis vary be-tween the two types in the mandible as muchas in any other bone. In distinct contrast toendosteal ogteosarcoma the known duration ofthis lesion without gross destruction or overtmetastasis was at least 6 years, during whichtime there was only local recurrence after
surgical intervention. The clinical behaviourand mnicroscopic appearances may be increas-ingly malignant in recurrent lesions. Comparedwith endosteal tumours metastasis is infrequent,but the temptation to strip the tumour frombone should be resisted. Recurrence from par-osteal residues or soft-tissue deposits is com-mnon, and adequiate resection of the earlylesion while in its most differentiated formmay be preferred.As implied in original descriptions2", the pro-
visional diagnosis is often of a benign lesion; inthe mandible benign fibro-osseous tumours,osteocartilaginous exostosis, or myositis ossificansmay be considered. The radiographic appear-ance of medullary radiolucency and the 'sun-ray' trabeculation of periosteal new bone for-mation seen in most endosteal osteosarcomascontrasts with the appearance of parosteal boneformatioln in the present lesion, which tends tosclerosis and lacks fine, radiating spicules, whileit may progressively enclose a large segment ofthe bone. The histological findings are poten-tially confusing. Sclerotic bone without neo-plastic features may predominate; in many in-stances the soft-tissue component is fibrous andexhibits atypia so that low-grade fibrosarcomamay be considered in differential diagnosis21.Neoplastic bone formation leading to the cor-rect diagnosis of osteosarcoma may be confinedto the periphery of the lesion.
Lichtenstein22 has critically reviewed theconcept of juxtacortical osteosarcoma becauseof the disparity in behaviour between manysuch lesions and endosteal sarcoma. Hesuggests that there is a broad division betweenthe rare instance of osteosarcoma arising inperiosteum, which is overtly malignant, andmalignant change in metaplastic fibro-osseous(and cartilaginous) lesions of periosteum, in-cluding myositis ossificans, which may be agradual process. Especially in the case ofmyositis ossificans the histological distinctionbetween exuberant but benign mesenchymalproliferation, with osteolgenesis, and malignantosteogenic mesenchyme may be difficult. Thepresent case falls into the second category andthe earliest changes may have been metaplastic.Evidence for malignancy is based upon therelentless local recurrence and infiltration andthe cytological interpretation of increasinglysevere atvpia within successive recurrences,

A series of maxillofacial tumours from Nigeria 45
especially associated with substantial tracts offibrosarcomatous tissue.
ConclusionThe five different conditions described in thispaper are uncommon, but they are not anec-dotal oddities and they exemplify the extra-ordinary range of neoplasms that may occurin the maxillofacial region. In each instanceboth the value and the limitation of histo-pathological diagnosis are apparent and theinfluence of the interpretation of biopsies up-on the course of future investigations andtreatment is emphasized.
We are indelted to Dr R Shamia of Kadunafor his expert clinical guidance and for permissionto describe cases under his care, to Profesor B Cohenfor his advice and constant encouragement during thepreparation of the manuscript, and to Mr E B Brainand Mr G Elia for their assistance in the preparationof illustrations.
ReferencesX Anand, S V, Davey, W W, and Cohen, B (I967)
British Journal of Surgery, 54, 901.2 Williams, A 0 (I975) Cancer, 36, 370.3 Olurin, 0, and Williams, A 0 (I972) Cancer, 30,
580.4 Porterfield, J F, and Zimmerman, L E (I962)
Virchows Archiv fur pathologische Anatomie undPhysiologie und fur klinische Medizin, 335, 329.
5 Burkitt, D, and Wright, D H (1970) Burkitt'sLymphoma, p. 9. Edinburgh and London, Living-stone.
6 Enzinger, F M, and Shiraki, M (i969) Cancer,24, I8.
7 Wilson, D F, and MacEntee, M I (I974) OralSurgery, 36, 915.
8 Allen, M S, Fitz-Hugh, G S, and March, W L(I974) Cancer, 33, 153-
9 Davey, W WV (I968) Companion to Surgery inAfrica, pp I54-157. Edinburgh and London,Livingstone.
10 Schazowicz, F, Ackerman, L V, and Sissons, H A(I972) Histological Typing of Bone Tumours.Geneva, NVorld Health Organization.
iI Pindborg, J J, Kramer, I R H, and Torloni, H(1971) hIistological Typing of OdontogenicTumours, Jaw Cysts and Allied Lesions. Geneva,World Health Organization.
12 Lucas, R B (1972) Pathology of Tumours of theOral Tissues, 2nd edn, p. 363. Edinburgh andLondon, Churchill Livingstone.
13 Waldron, C A, and Giansanti, J S (I973) OralSurgery, 35, 340-
I4 Giansanti, J S (1970) Oral Surgery, 30, 5o8.15 Leband, P F, and Leacock, A G (i967) Journal
of Oral Surgery, 25, 23.16 Waldron, C A, Giansanti, J S, and Browand, B
C (I975) Oral Surgery, 39, 590.I7 Winer, H J, Goepp, R A, and Olsen, R E (1972)
Journal of Oral Surgery, 30, 517.18 Som, M, and Peimer, R (I96I) Archives of Oto-
laryngology, 74, 532.i9 Solomon, M P, Biernacki, J, Slippen, M, and
Rosen, Y (I975) Archives of Otolaryngology, IOI.754-
20 Dwinnell, L, A, Dahlin, D C, and Ghormley, RK (I954) Journal of Bone and joint Surgery,36A, 732.
2I Heul, R 0 van der, and Ronnen, J R von (I967)Journal of Bone and Joint Surgery, 49A, 4I5.
22 Lichtenstein, L (1972) Bone Tumours, 4th edn, p.380. St Louis, Mosby.


















