
A Report of Microtia and Ipsilateral Scalp Hemangioma
1
Poster Design & Printing by Genigraphics ® - 800.790.4001 Punam Thakkar Department of Otolaryngology SUNY Downstate Medical Center Email: [email protected] Phone: (718) 270-1638 Hemangiomas are the most common tumors of infancy. The majority of hemangiomas present in the first few weeks of life and most manifest in the head and neck region. We present a case report of an 8 month old female with a right sided grade III microtia with an ipsilateral compound hemangioma of the right occipital scalp. Exemption from formal IRB review was granted by the SUNY Downstate Institutional Review Board to present this report. The patient had a history of ulceration of the lesion and given the risk of scarring of the skin of the recipient bed for the future microtia repair, we proceeded with excision of the hemangioma with a purse-string closure. Only one other similar report of a scalp hemangioma in the presence of microtia was found in a review of the literature. Early surgical excision of a hemangioma may be warranted in such cases to provide optimal results of microtia repair. We describe possible embryological links between these two entities and also discuss the surgical treatment of an infantile hemangioma of the scalp during the proliferative phase. A Report of Microtia and Ipsilateral Scalp Hemangioma A Report of Microtia and Ipsilateral Scalp Hemangioma Punam Thakkar, MD 1 ; Jenna Lester, BA 2 ; Sydney Butts, MD 1 1 State University of New York Downstate Medical Center, Brooklyn NY, 2 Brown University School of Medicine An 8 month old female presented with right grade III microtia and hemangioma of the right scalp (Figure 1). The hemangioma was not present at birth but began to grow when the child was about 2 months of age while the ear deformity was congenital. The patient had a normal renal sonogram at birth. She had no feeding or breathing difficulties. There was no family history of congenital craniofacial anomalies or vascular anomalies and no history of teratogen exposure. Physical examination of the ears demonstrated a grade III microtia of the right ear with no definable ear canal; left external ear, canal and tympanic membrane were normal. It was imperative to rule out hemifacial microsomia (HFM) or another craniofacial syndrome in this patient. Her physical examination also suggested mild weakness of the right marginal mandibular branch of the facial nerve and mild hypoplasia of the cheek soft tissues. However, no other anomalies consistent with HFM were present. Further examination of the head demonstrated a 4 cm compound hemangioma of the right occipital scalp with superficial areas of ulceration. The patient had a normal left OAE. Sound field testing demonstrated normal hearing and Type A tympanometry in the left ear. Further work up included a cervical spine radiograph which was normal. Genetic evaluation was obtained which demonstrated a normal karyotype and chromosome mircroarray. An opthalmology evaluation revealed a normal eye exam. Cardiology examination revealed a benign heart murmur with a normal 2D ECHO. Given the large size of the hemangioma and the history of ulceration, we proceeded with excision of the lesion and purse string closure when the child was 9 months old (Figure 2). Pathology demonstrated juvenile capillary hemangioma (Figure 3). The recent description of the findings of extracutaneous malformations with certain types of hemangiomas that fall within distinct embryologically based developmental fields lead us to hypothesize that a development link might exist between the microtia and the hemangioma in this patient. A review of the literature shows 3 prior similar cases. In 1970, Krause 6 described a series of patients with Goldenhar syndrome. One patient had a temporal scalp hemangioma and type II microtia and another patient presented with bilateral preauricular skin tags and a hemangioma of the nape of the neck. Pascual-Castroviejo 7 described a female patient with right anotia and several ipsilateral cervical vascular anomalies, along with a left facial hemangioma associated with ipsilateral cerebrovascular anomalies and persistence of the stapedial artery. In that report, the hemangioma and anotia were on the opposite sides of the face but the underlying vasculophathy and persistent embryonic vessels found in the patient were believed to be pathogenetically linked. Generally, hemangiomas are not surgically managed due to their tendency to involute 1 . However, there are indications for early surgical intervention. Hemangiomas that are not responding to medical treatment or hemangiomas that could possibly be obstructing the airway or compromising vision or hearing should be managed surgically 1 . The proximity of this hemangioma to the microtic ear jeopardized the availability of adequate soft tissue coverage for the future microtia reconstruction, especially if proliferation were to continue. The known increased pliability of infant scalp soft tissues compared to adults contributed to the decision to excise this patient’s hemangioma. The purse-string closure technique decreased the size of the defect and allowed closure without the use of rotational flaps or grafting (Figure 4). INTRODUCTION 1. Beck DO, Gosain AK. The Presentation and Management of Hemangiomas. Plastic and Reconstructive Surgery. 2009; 123(6): 181e-91e. 2. Keogh, IJ, Troulis MJ, Monroy AA, Eavey RD, Kaban LB. Isolated microtia as a marker for unsuspected HFM. Arch Otolaryngol Head Neck Surg. 2007;133(10):997-1001. 3. Rahbar R, Robson CD, Mulliken JB, Schwartz L, Dicanzio J, Kenna MA, McGill TJ, Healy GB. Craniofacial, Temporal Bone, and Audiologic Abnormalities in the Spectrum of Hemifacial Microsomia. Arch Otolaryngol Head Neck Surg. 2001;127(3):265-71. 4. Pascual-Castroviejo I. Vascular and nonvascular intracranial malformations associated with external capillary hemangiomas. Neuroradiology 1978; 16:82-84. 5. Metry D, Heyer G, Hess C, Garzon M et al. Consensus statement on diagnostic criteria for PHACE syndrome. Pediatrics 2009; 124:1447-56. 6. Krause U. The Syndrome of Goldenhar affecting two siblings. Acta Opthalmologica 1970; 48:494-9. 7. Pascual-Castroviejo I, Pascual-Pascual V. Persistence of the stapedial artery associated with facial hemangioma: a case report. Neuropediatrics 2010; 41(4):186-8. CASE REPORT REFERENCES Figure 1. Right occipital scalp hemangioma and ipsilateral grade III microtia ABSTRACT CONTACT DISCUSSION Figure 2. Hemangioma was excised and purse string suture in place Figure 4. The Defect was closed in a purse string fashion. Figure 3. Capillary hemangioma admixed with skin adnexa and adipose tissue The physical findings in this patient of microtia and weakness of the marginal mandibular branch of the facial nerve are consistent with a diagnosis of hemifacial microsomia (HFM) 2 (Figure 5). Hemifacial microsomia is the second most common craniofacial abnormality after cleft lip and cleft palate 2 . HFM is the end result of developmental disruption of embryologic precursors derived from the first and second pharyngeal arches 2 . The OMENS classification is now commonly used to categorize the severity of the syndrome in affected patients 3 (Table 1). In our case, the patient’s OMENS score is O0 M0 E1 N2 S1. Some of the skeletal and soft tissue anomalies in HFM become more apparent with age, and continued follow up with possible re-scoring using the OMENS criteria is required. No findings associated with HFM outside of the head and neck were present in this patient, including results of cardiac and ophthalmologic evaluations, genetic testing, and cervical spine x-rays. Although the precise pathogenesis of HFM is incompletely understood, theories indicate that HFM may develop as a result of inadequate migration of neural crest cells to the regions of the first and second pharyngeal arches. Another leading theory suggests that a genetic defect with mesenchymal disruptions and embryonic hemorrhage could lead to HFM 2 . In 1978, Pascual-Castroviejo described a series of patients with hemangiomas of the face and cerebrovascular, cardiac and brain anomalies 4 . In 1996, the acronym PHACES was coined to describe a syndrome expanding on this original classification to define a neurocutaneous syndrome that includes posterior fossa abnormalities, hemangiomas of the face, arterial and cardiac abnormalities, coarctation of the aorta, and eye abnormalities 5 . In the majority of PHACES syndrome patients, a segmental, morphologically diffuse hemangioma of the face is seen. More recent reports indicate the diagnosis can also include scalp or neck locations. The results of ophthalmological evaluation and cardiac assessment were negative in this case. While this patient had no neurological examination findings, further neurologic imaging would be required to rule out structural brain or cerebrovascular lesions that also characterize the PHACE syndrome. OMENS Classification Orbit O0 Normal orbit size, position O1 Abnormal orbit size O2 Abnormal orbit position O3 Abnormal orbit position Mandible M0 Normal M1 Small mandible and glenoid fossa M2 Ramus short and abnormally shaped Subdivisions based on relative positions of condyle and TMJ 2A: Glenoid fossa in anatomically acceptable position 2B: TMJ inferiorly, medially, and anteriorly displaced with severely hypoplastic condyle M3 Complete absence of ramus, TMJ, and glenoid fossa Ear E0 Normal ear E1 Minor hypoplasia and cupping with all structures present E2 Absence of external auditory canal with variable hypoplasia and concha E3 Malpositioned lobule with absent auricle, lobular remnant usually inferior anteriorly displaced Facial Nerve N0 No facial nerve involvement N1 Upper facial nerve involvement (temporal or zygomatic branches) N2 Lower facial nerve involvement (buccal, mandible, or cervical) N3 All branches affected Soft Tissue S0 No obvious tissue or muscle deficiency S1 Minimal soft tissue or muscle deficiency S2 Moderate soft tissue or muscle deficiency S3 Severe soft tissue or muscle deficiency Table 1. OMENS Classiification 3 Figure 5. The patient had a mild weakness of right marginal mandibular branch of the facial nerve and mild soft tissue hypoplasia Infantile hemangiomas are the most common tumors of infancy with an incidence of 1.1 to 2.6 percent in normal weight infants 1 . The incidence is even higher in low birth weight infants with rates reported as high as 22.9 percent 1 . Microtia is less common than hemangioma occurring in approximately 1 in 10,000 live births 2 . These congenital abnormalities are rarely seen together which makes their co- presentation in this patient of particular interest. Additionally, their close anatomical proximity in this patient suggests the possibility of a link in development. Genetic, radiologic and multidisciplinary clinical evaluations were required for diagnosis and also helped to elucidate potential etiologic links between these two anomalies. The natural history of infantile hemangiomas, marked by early proliferation, was a significant factor in the management decisions in this case and emphasize the role that surgical intervention can have in the reconstructive plan.
Transcript of A Report of Microtia and Ipsilateral Scalp Hemangioma
Poster Design & Printing by Genigraphics® - 800.790.4001
Punam ThakkarDepartment of OtolaryngologySUNY Downstate Medical CenterEmail: [email protected]: (718) 270-1638
Hemangiomas are the most common tumors of infancy. The majority of hemangiomas present in the first few weeks of life and most manifest in the head and neck region. We present a case report of an 8 month old female with a right sided grade III microtia with an ipsilateral compound hemangioma of the right occipital scalp. Exemption from formal IRB review was granted by the SUNY Downstate Institutional Review Board to present this report. The patient had a history of ulceration of the lesion and given the risk of scarring of the skin of the recipient bed for the future microtia repair, we proceeded with excision of the hemangioma with a purse-string closure. Only one other similar report of a scalp hemangioma in the presence of microtia was found in a review of the literature. Early surgical excision of a hemangioma may be warranted in such cases to provide optimal results of microtia repair. We describe possible embryological links between these two entities and also discuss the surgical treatment of an infantile hemangioma of the scalp during the proliferative phase.
A Report of Microtia and Ipsilateral Scalp HemangiomaA Report of Microtia and Ipsilateral Scalp HemangiomaPunam Thakkar, MD1; Jenna Lester, BA2 ; Sydney Butts, MD1
1State University of New York Downstate Medical Center, Brooklyn NY, 2Brown University School of Medicine
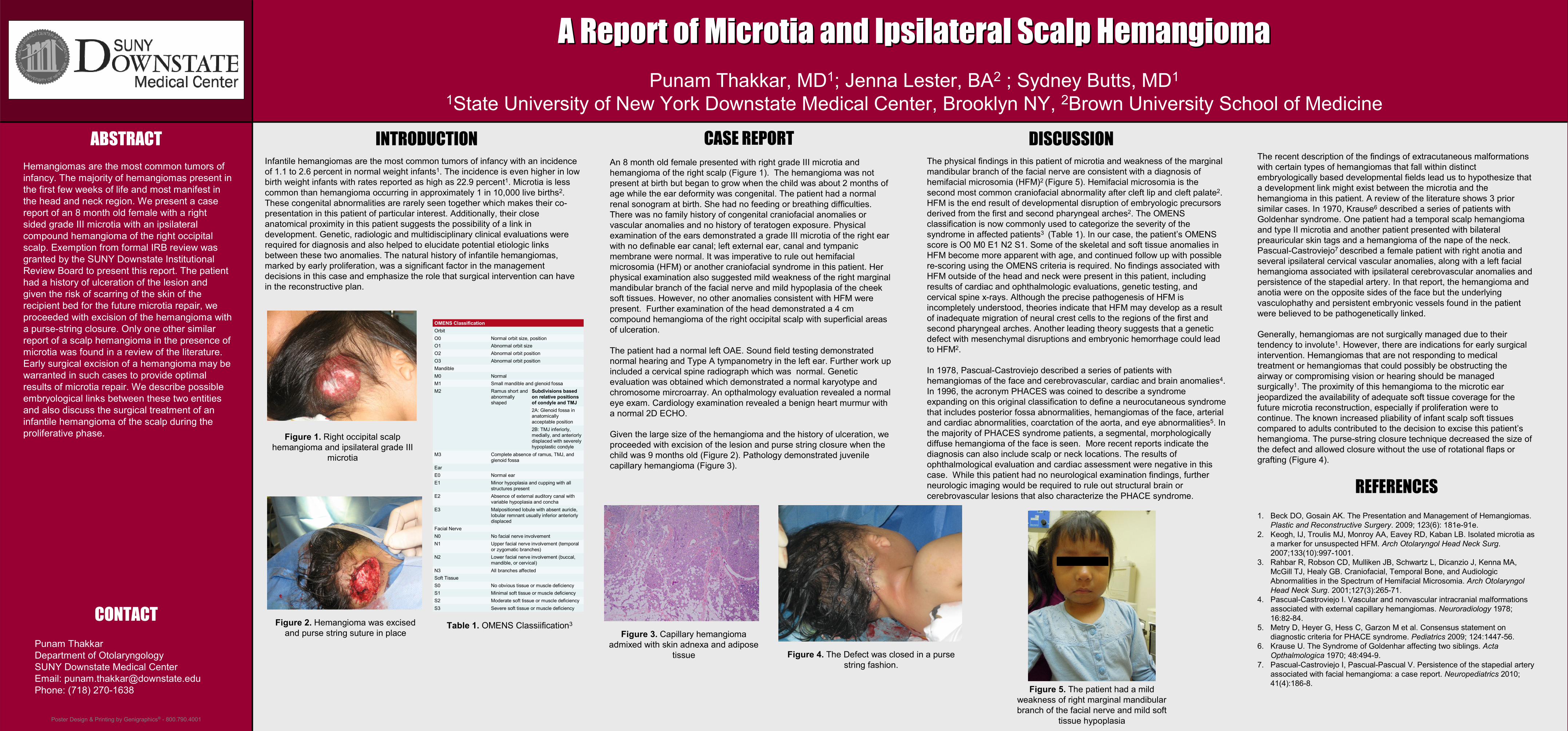
An 8 month old female presented with right grade III microtia and hemangioma of the right scalp (Figure 1). The hemangioma was not present at birth but began to grow when the child was about 2 months of age while the ear deformity was congenital. The patient had a normal renal sonogram at birth. She had no feeding or breathing difficulties. There was no family history of congenital craniofacial anomalies or vascular anomalies and no history of teratogen exposure. Physical examination of the ears demonstrated a grade III microtia of the right ear with no definable ear canal; left external ear, canal and tympanic membrane were normal. It was imperative to rule out hemifacial microsomia (HFM) or another craniofacial syndrome in this patient. Her physical examination also suggested mild weakness of the right marginal mandibular branch of the facial nerve and mild hypoplasia of the cheek soft tissues. However, no other anomalies consistent with HFM were present. Further examination of the head demonstrated a 4 cm compound hemangioma of the right occipital scalp with superficial areas of ulceration.
The patient had a normal left OAE. Sound field testing demonstrated normal hearing and Type A tympanometry in the left ear. Further work up included a cervical spine radiograph which was normal. Genetic evaluation was obtained which demonstrated a normal karyotype and chromosome mircroarray. An opthalmology evaluation revealed a normal eye exam. Cardiology examination revealed a benign heart murmur with a normal 2D ECHO.
Given the large size of the hemangioma and the history of ulceration, we proceeded with excision of the lesion and purse string closure when the child was 9 months old (Figure 2). Pathology demonstrated juvenile capillary hemangioma (Figure 3).
The recent description of the findings of extracutaneous malformations with certain types of hemangiomas that fall within distinct embryologically based developmental fields lead us to hypothesize that a development link might exist between the microtia and the hemangioma in this patient. A review of the literature shows 3 prior similar cases. In 1970, Krause6 described a series of patients with Goldenhar syndrome. One patient had a temporal scalp hemangioma and type II microtia and another patient presented with bilateral preauricular skin tags and a hemangioma of the nape of the neck.Pascual-Castroviejo7 described a female patient with right anotia and several ipsilateral cervical vascular anomalies, along with a left facial hemangioma associated with ipsilateral cerebrovascular anomalies and persistence of the stapedial artery. In that report, the hemangioma and anotia were on the opposite sides of the face but the underlyingvasculophathy and persistent embryonic vessels found in the patient were believed to be pathogenetically linked.
Generally, hemangiomas are not surgically managed due to their tendency to involute1. However, there are indications for early surgical intervention. Hemangiomas that are not responding to medical treatment or hemangiomas that could possibly be obstructing the airway or compromising vision or hearing should be managed surgically1. The proximity of this hemangioma to the microtic ear jeopardized the availability of adequate soft tissue coverage for the future microtia reconstruction, especially if proliferation were to continue. The known increased pliability of infant scalp soft tissues compared to adults contributed to the decision to excise this patient’s hemangioma. The purse-string closure technique decreased the size of the defect and allowed closure without the use of rotational flaps or grafting (Figure 4).
INTRODUCTION
1. Beck DO, Gosain AK. The Presentation and Management of Hemangiomas. Plastic and Reconstructive Surgery. 2009; 123(6): 181e-91e.
2. Keogh, IJ, Troulis MJ, Monroy AA, Eavey RD, Kaban LB. Isolated microtia as a marker for unsuspected HFM. Arch Otolaryngol Head Neck Surg. 2007;133(10):997-1001.
3. Rahbar R, Robson CD, Mulliken JB, Schwartz L, Dicanzio J, Kenna MA, McGill TJ, Healy GB. Craniofacial, Temporal Bone, and AudiologicAbnormalities in the Spectrum of Hemifacial Microsomia. Arch Otolaryngol Head Neck Surg. 2001;127(3):265-71.
4. Pascual-Castroviejo I. Vascular and nonvascular intracranial malformations associated with external capillary hemangiomas. Neuroradiology 1978; 16:82-84.
5. Metry D, Heyer G, Hess C, Garzon M et al. Consensus statement on diagnostic criteria for PHACE syndrome. Pediatrics 2009; 124:1447-56.
6. Krause U. The Syndrome of Goldenhar affecting two siblings. Acta Opthalmologica 1970; 48:494-9.
7. Pascual-Castroviejo I, Pascual-Pascual V. Persistence of the stapedial artery associated with facial hemangioma: a case report. Neuropediatrics 2010; 41(4):186-8.
CASE REPORT
REFERENCES
Figure 1. Right occipital scalp hemangioma and ipsilateral grade III
microtia
ABSTRACT
CONTACT
DISCUSSION
Figure 2. Hemangioma was excised and purse string suture in place
Figure 4. The Defect was closed in a purse string fashion.
Figure 3. Capillary hemangioma admixed with skin adnexa and adipose
tissue
The physical findings in this patient of microtia and weakness of the marginal mandibular branch of the facial nerve are consistent with a diagnosis of hemifacial microsomia (HFM)2 (Figure 5). Hemifacial microsomia is the second most common craniofacial abnormality after cleft lip and cleft palate2. HFM is the end result of developmental disruption of embryologic precursors derived from the first and second pharyngeal arches2. The OMENS classification is now commonly used to categorize the severity of the syndrome in affected patients3 (Table 1). In our case, the patient’s OMENS score is O0 M0 E1 N2 S1. Some of the skeletal and soft tissue anomalies in HFM become more apparent with age, and continued follow up with possible re-scoring using the OMENS criteria is required. No findings associated with HFM outside of the head and neck were present in this patient, including results of cardiac and ophthalmologic evaluations, genetic testing, and cervical spine x-rays. Although the precise pathogenesis of HFM is incompletely understood, theories indicate that HFM may develop as a result of inadequate migration of neural crest cells to the regions of the first and second pharyngeal arches. Another leading theory suggests that a genetic defect with mesenchymal disruptions and embryonic hemorrhage could lead to HFM2.
In 1978, Pascual-Castroviejo described a series of patients with hemangiomas of the face and cerebrovascular, cardiac and brain anomalies4. In 1996, the acronym PHACES was coined to describe a syndrome expanding on this original classification to define a neurocutaneous syndrome that includes posterior fossa abnormalities, hemangiomas of the face, arterial and cardiac abnormalities, coarctation of the aorta, and eye abnormalities5. In the majority of PHACES syndrome patients, a segmental, morphologically diffuse hemangioma of the face is seen. More recent reports indicate the diagnosis can also include scalp or neck locations. The results of ophthalmological evaluation and cardiac assessment were negative in this case. While this patient had no neurological examination findings, further neurologic imaging would be required to rule out structural brain or cerebrovascular lesions that also characterize the PHACE syndrome.
OMENS ClassificationOrbitO0 Normal orbit size, positionO1 Abnormal orbit sizeO2 Abnormal orbit positionO3 Abnormal orbit positionMandibleM0 NormalM1 Small mandible and glenoid fossaM2 Ramus short and
abnormally shaped
Subdivisions based on relative positions of condyle and TMJ 2A: Glenoid fossa in anatomically acceptable position 2B: TMJ inferiorly, medially, and anteriorly displaced with severely hypoplastic condyle
M3 Complete absence of ramus, TMJ, and glenoid fossa
EarE0 Normal earE1 Minor hypoplasia and cupping with all
structures presentE2 Absence of external auditory canal with
variable hypoplasia and conchaE3 Malpositioned lobule with absent auricle,
lobular remnant usually inferior anteriorly displaced
Facial NerveN0 No facial nerve involvement N1 Upper facial nerve involvement (temporal
or zygomatic branches) N2 Lower facial nerve involvement (buccal,
mandible, or cervical) N3 All branches affected Soft Tissue S0 No obvious tissue or muscle deficiency S1 Minimal soft tissue or muscle deficiency S2 Moderate soft tissue or muscle deficiency S3 Severe soft tissue or muscle deficiency
Table 1. OMENS Classiification3
Figure 5. The patient had a mild weakness of right marginal mandibular branch of the facial nerve and mild soft
tissue hypoplasia
Infantile hemangiomas are the most common tumors of infancy with an incidence of 1.1 to 2.6 percent in normal weight infants1. The incidence is even higher in low birth weight infants with rates reported as high as 22.9 percent1. Microtia is less common than hemangioma occurring in approximately 1 in 10,000 live births2. These congenital abnormalities are rarely seen together which makes their co-presentation in this patient of particular interest. Additionally, their close anatomical proximity in this patient suggests the possibility of a link in development. Genetic, radiologic and multidisciplinary clinical evaluations were required for diagnosis and also helped to elucidate potential etiologic links between these two anomalies. The natural history of infantile hemangiomas, marked by early proliferation, was a significant factor in the management decisions in this case and emphasize the role that surgical intervention can have in the reconstructive plan.


















