
A Professor of Obstetrics & Gynecology Alexandria University
44
Diabetes in pregnancy Amr Adel Mansy, MD, MBA A Professor of Obstetrics & Gynecology Alexandria University
Transcript of A Professor of Obstetrics & Gynecology Alexandria University

Diabetes in pregnancy
Amr Adel Mansy, MD, MBA
A Professor of Obstetrics & Gynecology
Alexandria University

Definition of DM
• A Complex disease characterized byCarbohydrate intolerance with variabledegrees of severity.

Types of diabetes in pregnancy
• Type I (IDDM): absolute insulin deficiency ,usually effects children and young adults.
• Type II diabetes (NIDDM): increase insulinresistance, usually effects adults.
• Gestational diabetes: Diabetes occurring forthe first time during pregnancy.

Incidence
• Diabetes affects 2-5% of pregnancies.
• associated with maternal & fetal morbidityand mortality.
• Good antenatal care and blood sugar controlis associated with major ↓in complications.

• Pregnancy is a state of insulin resistance andglucose intolerance due to ↑anti-insulinhormones & substances:– Human Placental Lactogen (HPL)
– Estrogen and Progesterone
– Insulinase
• insulin resistance ↑with ↑ gestation.
Physiological changes

1. Mild fasting hypoglycemia
2. Postprandial hyperglycemia
3. Hyperinsulinemia
4. ↑renal threshold for glucose glucosuria
Normal pregnancy is characterized by:

• ↑Peripheral insulinresistance adequateglucose supply to fetus.
• This does not affect normalpregnancy as insulin levelswill ↑.
• Patients with glucoseintolerance gestationaldiabetes.
• Diabetics Patients
require ↑ insulin dose.

Influence of Pregnancy on Carbohydrate Metabolism
1. ↑insulin resistance ↑ production ofinsulin by pancreas (hyperplasia/ hypertrophy)
• Adequate insulin production may becomeinadequate to meet increased demand duringpregnancy gestational DM
2. Known diabetic controlled on diet may needinsulin
3. Insulin dependentmodify medication.

Effects of DM on pregnancy
• In maternal DM, fetus has hyperinsulinemia acts as growth promoting hormone fetal macrosomia
• Adverse effects are due to:
– Fetal hyperinsulinemia rather than Fetalhyperglycemia

ADVERSE FETAL EFFECT OF DM
1.Congenital Malformation:
4—10 times higher than normal.
Teratogenicity is directly related toconcentration of glucose at time oforganogenesis.
So, more risk of Congenital abnormality inpregestational diabetes

Structural abnormalities:
• Cardiac• Transposition of great
vessels
• Ventricular Septal Defects (VSD)
• Coarctation of aorta
• Patent Ductus Arteriosus(PDA)
• Atrial Septal Defects (ASD)
• Cardiomegaly
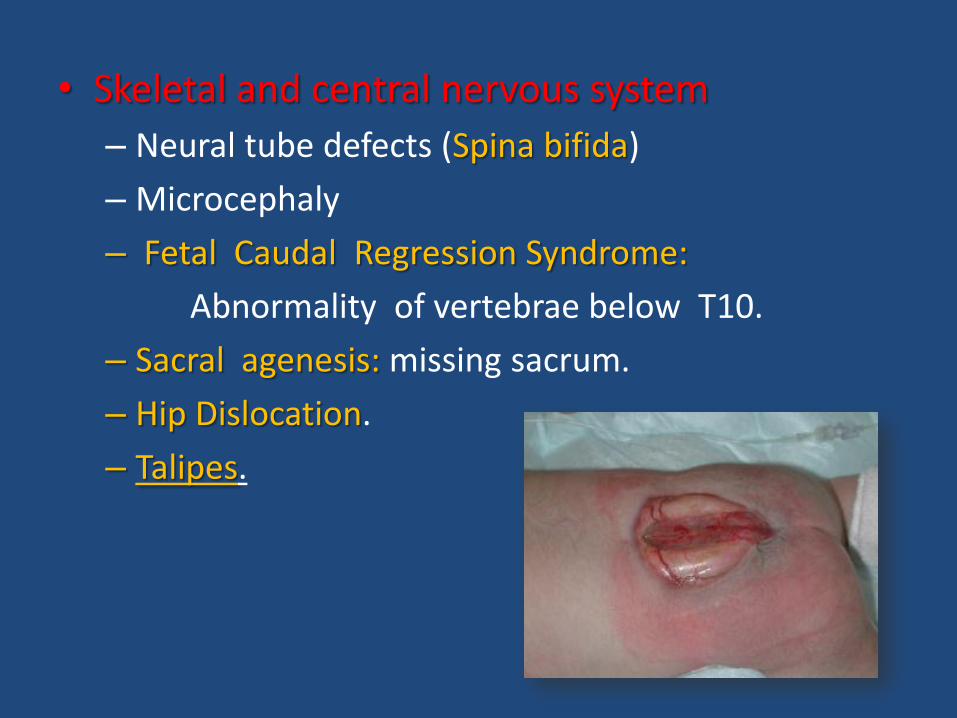
• Skeletal and central nervous system
– Neural tube defects (Spina bifida)
– Microcephaly
– Fetal Caudal Regression Syndrome:
Abnormality of vertebrae below T10.
– Sacral agenesis: missing sacrum.
– Hip Dislocation.
– Talipes.


• Renal anomalies.– Hydronephrosis– Renal agenesis
– Urinary or fecal incontinence.
• Gastrointestinal
– Duodenal atresia
– Anorectal atresia
• Other
– Single umbilical artery
2.Spontaneous miscarriage:
Due to cong. Anomalies.
3.Fetal macrosomia:
- Due to fetal hyperinsulinaemia.
Fetal body wt > 4 kg.
- fetal macrosomia - Prolonged & obstructed labour.
- Shoulder dystosia.
4.IUGR:
- due to impaired placental function.

5. Polyhydramnios:
- Preterm labour.
- malpresentation.
6.Pre-eclempsia
7. Unexplained IUFD.

9. Perinatal morbidity & mortality:
- 5 times higher.
1. RDS
2. Neonatal hypoglycemia
3. Polycythemia
4. Hyperbilirubinemia
5. Asphyxia neonatorum

Infant of diabetic mother.

Screening for diabetes in pregnancy

Risk factors for gestational diabetes
1. Previous history of diabetes.2. Positive family history.3. Age and parity.4. History of IUFD.5. History of recurrent abortion.6. History of Large size babies (> 4Kg).7. Polyhydramnios.8. Obesity.9. PCOS

Non-challenge blood glucose tests
• performed at first antenatal visit.
• Test is positive if:
– Fasting plasma glucose level >126 mg/dl
– or Random > 200 mg/dl

Screening glucose challenge testO'Sullivan test
• Done between 24–28 weeks
• No fasting is required
• drinking a solution containing 50 grams ofglucose, and measuring blood levels after 1hour.
• If > 140 mg/dl OGTT

Oral Glucose Tolerance Test
Drinking solution contains 100 gm glucose
Abnormal values by American DiabetesAssociation :
• Fasting blood glucose level ≥95 mg/dl
• 1 hour blood glucose level ≥180 mg/dl
• 2 hour blood glucose level ≥155 mg/dl
• 3 hour blood glucose level ≥140 mg/dl

Management of diabetes in pregnancy
1. Pre-pregnancy counseling.
2. Antenatal care.
3. Controlling blood sugar.
4. Management of diabetes in labour.
5. Postpartum management.

1- Pre-pregnancy counseling
1. Good diabetic control before pregnancy toprevent early complications.
2. Diabetic control is measured by glycosylatedHbA1c.
3. Folic acid to ↓NTD 3 months before.
4. If uncontrolled use contraception.
5. If on oral hypoglycemic change to insulin.
6. Advice healthy diet and life style modification.

2- Antenatal care
1. 2D & 4D Anomaly scan at 18-22 weeks.
2. Frequent antenatal follow up with U/S tomonitor fetal growth.
3. Check blood pressure and albuminuria at everyvisit.
4. Avoid delivery before 38 weeks unless othercomplications.
5. Pregnancy should not go beyond 40 weeks.

3- Controlling blood sugar
• Good control of blood sugar improvesmaternal and fetal complications.
• Good diet control “but avoid starvation”
– 3 meals and 3 snacks.
• aim to keep blood sugar near normoglycemia(<100mg/dl fasting and 140mg/dl post-prandial).

II. Further Management.
• Medical management.
• Obstetrical management.

Medical Management:
TREATMENT MODLITIES:
- diet.
- diet + insulin.
Oral hypoglycemic drugs were known to becontraindicated.

1. Diet:
• 3 meals and 3 snacks• 30-35 Kcal/Kg
– 50% of energy carbohydrates,– 30% fat– 20% proteins
• Maximum weight gain: 10-12 Kg

2.INSULIN THERAPY
• Treatment of choice
• does not cross placenta.
– Short acting.
– Long acting.

4 times daily regimen;
- short acting insulin 3 times after meal.
- long acting at night.
Biphasic regimen:
• Fixed combination of medium & short acting
insulin 70/30 is given in 2 dosage.
• One before breakfast and other before dinner
Insulin regimen:

OTHER FORMULAS
1.Maternal wt ×
0.7 in 1st trimester
0.8 in 2nd trimester
0.9 in 3rd trimester
2. Sliding scale.

Oral Hypoglycemic Drugs
• GLIBENCLAMIDE
• does not cross placentalbarrier
• Recent reports suggest no↑fetal malformation rate
• Risk of maternalhypoglycemia
• Stop as soon as patientcomes to you
• METFORMIN
• used for PCOs, infertility
• Reports suggest beneficialresults in 1st trimesterpregnancy continuation rate
• Stop as soon as pregnancy isdiagnosed/at 12 weeks

Monitoring
HbA1C (glycosylated Hb.):
Glucose irreversibly bound to Hb.
- Indicates previous 2 months glucose control
- Repeated monthly
- For good control should be <6.1%.
In pre-pregnancy counseling, HBA1C > 10% avoid pregnancy

OBSTETRICAL MANAGEMENT
1. ANTENETAL CARE:
A. -1ST trimester : - good glucose control &
- US
- 2nd trimester: - US at 18-20 wk.(cong. An.)
- US at 20-22wk.(cardiac An.)
- 3rd trimester: - Care for
. Polyhydramnios . PE
. F. macrosomia . IUFD
. Pre-term labour

2. VISIT FREQUENCY:
biweekly from 24-32 wk. followed by weekly
3. FETAL SURVEILLANCE:
a) US: good indicator of fetal wt.
AFI from 24 weeks , biweekly
b) CTG: - 2-3 times/week from 36 weeks onward
c) Doppler
d) Biophysical Profile

DELIVERY:
a) Time of Delivery:
- Well controlled DM 39-40 weeks
- Uncontrolled DM 38 weeks
b) Mode of Delivery:
- Vaginal delivery is mode of choice
- C- section

c) Management During Labour:
Insulin therapy: Give I/V insulin 1 unit/h if,
. Labour established
. Induction of labour
. Elective C-section
Measure glucose 1 hourly and manage according to sliding scale.

POST PARTUM CARECARE OF MOTHER
insulin requirement is decreased in puerperium.
CARE OF BABY1. RESPIRATORY SYSTEM
1. RDS2. TTN: Transient tachypnea of the newborn
2. HYPOGLYCAEMIA1. Blood glucose checked at 2,4,6& 12 hours of age.2. If <45 mg/dl at 4 hours I/V 10% dextrose.3. Start feeding by 2 hours & continue at 3-4 hours interval.
3. HYPERBILI RUBINAEMIA1. Vit K 1mg Inj.2. Phototherapy 3. Exchange transfusion

NEWBORN MAANAGEMENT
• Serially assess capillary glucose of the neonate especially in the first 12 hours.
• Give glucose if the glucose level is less than 45 mg/dl
• If the hematocrit value exceeds 70, exchangetransfusion
• Serially monitor bilirubin level.

CONTRACEPTION
• Estrogen containing pills: allowed with needfor tight control unless vascular disease ispresent.
• Progestin only Pills: allowed• IUCD: allowed• Barrier: allowed• Sterilization: in women with contraindications
to pregnancy (proliferative retinopathy,cardiopathy, nephropathy, gastropathy andother vascular lesions)

DON’T FORGET
• OGTT at 6 weeks to confirm disappearance of impaired glucose tolerance

THANK YOU


















