A Novel Resorbable Embolization Microsphere for Transient ... · A Novel Resorbable Embolization...
11
See discussions, stats, and author profiles for this publication at: https://www.researchgate.net/publication/265392992 A Novel Resorbable Embolization Microsphere for Transient Uterine Artery Occlusion: A Comparative Study with... Article in Journal of vascular and interventional radiology: JVIR · September 2014 DOI: 10.1016/j.jvir.2014.06.025 · Source: PubMed CITATIONS 3 READS 51 9 authors, including: Some of the authors of this publication are also working on these related projects: Drug Delivery Systems for mini-invasive treatments View project Valentin Verret French National Institute for Agricultural Res… 33 PUBLICATIONS 69 CITATIONS SEE PROFILE Mchel Wassef Hôpital Lariboisière - Fernand-Widal (Hôpita… 276 PUBLICATIONS 4,346 CITATIONS SEE PROFILE Laurent Bédouet Occlugel 58 PUBLICATIONS 692 CITATIONS SEE PROFILE Alexandre Laurent APHP - Hopital Lariboisière, 2 rue A.Paré, 750… 152 PUBLICATIONS 2,147 CITATIONS SEE PROFILE All content following this page was uploaded by Laurent Bédouet on 07 May 2015. The user has requested enhancement of the downloaded file. All in-text references underlined in blue are linked to publications on ResearchGate, letting you access and read them immediately.
Transcript of A Novel Resorbable Embolization Microsphere for Transient ... · A Novel Resorbable Embolization...
Seediscussions,stats,andauthorprofilesforthispublicationat:https://www.researchgate.net/publication/265392992
ANovelResorbableEmbolizationMicrosphereforTransientUterineArteryOcclusion:AComparativeStudywith...
ArticleinJournalofvascularandinterventionalradiology:JVIR·September2014
DOI:10.1016/j.jvir.2014.06.025·Source:PubMed
CITATIONS
3
READS
51
9authors,including:
Someoftheauthorsofthispublicationarealsoworkingontheserelatedprojects:
DrugDeliverySystemsformini-invasivetreatmentsViewproject
ValentinVerret
FrenchNationalInstituteforAgriculturalRes…
33PUBLICATIONS69CITATIONS
SEEPROFILE
MchelWassef
HôpitalLariboisière-Fernand-Widal(Hôpita…
276PUBLICATIONS4,346CITATIONS
SEEPROFILE
LaurentBédouet
Occlugel
58PUBLICATIONS692CITATIONS
SEEPROFILE
AlexandreLaurent
APHP-HopitalLariboisière,2rueA.Paré,750…
152PUBLICATIONS2,147CITATIONS
SEEPROFILE
AllcontentfollowingthispagewasuploadedbyLaurentBédoueton07May2015.
Theuserhasrequestedenhancementofthedownloadedfile.Allin-textreferencesunderlinedinblue
arelinkedtopublicationsonResearchGate,lettingyouaccessandreadthemimmediately.
XML-IS
Our reference: JVIR 3077 P-authorquery-vx
AUTHOR QUERY FORM
Journal: JVIR
Please e-mail or fax your responses and any corrections to:
Article Number: 3077
E-mail: [email protected]
Fax: 215-239-3388
Dear Author,
Please check your proof carefully and mark all corrections at the appropriate place in the proof (e.g., by using on-screen annotation in the
PDF file) or compile them in a separate list. Note: if you opt to annotate the file with software other than Adobe Reader then please also
highlight the appropriate place in the PDF file. To ensure fast publication of your paper please return your corrections within 48 hours.
For correction or revision of any artwork, please consult http://www.elsevier.com/artworkinstructions.
Any queries or remarks that have arisen during the processing of your manuscript are listed below and highlighted by flags in the proof.
Click on the Q link to go to the location in the proof.
Location in
article
Query / Remark: click on the Q link to go
Please insert your reply or correction at the corresponding line in the proof
Q1 Please confirm that given names and surnames have been identified correctly and are presented in the desired order.
Q2 Author:
� If there are any drug dosages in your article, please verify them and indicate that you have done so by initialing this
query.
� Please review and confirm the accuracy and completeness of any affiliations.
Q3 AU: Please approve shortened running head title or provide one that is �60 characters, including spaces.
Q4 AU: Are all author degrees correct as added?
Q5 AU: Please confirm all affiliations are set correctly with department and institution listed for each author. Per journal
style, street address is listed only for corresponding author. Also, please translate all French affiliations into English.
Q6 AU: Please provide Ref. 27 is not cited in the text.
Q7 AU: Editing of Purpose to conform to journal style OK?
Q8 AU: Need to explain the phrase "hormonally cycled"?
Q9 AU: Correct to add "%" to median values?
Q10 AU: Is "6 months" correct as added?
Q11 AU: Addition of the phrase "which is important for gestation" OK?
Q12 AU: Need to define or clarify the phrase "Sheep were artificially cycled"?
Q13 AU: Please add manufacturer name and location for Nesdonal.
Q14 AU: Is addition of the phrase "using a Primus workstation" correct?
Continued on next page
Original Text
AU: Please confirm all affiliations are set correctly with department and institution listed for each author. Per journal style, street address is listed only for corresponding author. Also, please translate all French affiliations into English.
XML-IS
Our reference: JVIR 3077 P-authorquery-vx
AUTHOR QUERY FORM
Journal: JVIR
Please e-mail or fax your responses and any corrections to:
Article Number: 3077
E-mail: [email protected]
Fax: 215-239-3388
Dear Author,
Please check your proof carefully and mark all corrections at the appropriate place in the proof (e.g., by using on-screen annotation in the
PDF file) or compile them in a separate list. Note: if you opt to annotate the file with software other than Adobe Reader then please also
highlight the appropriate place in the PDF file. To ensure fast publication of your paper please return your corrections within 48 hours.
For correction or revision of any artwork, please consult http://www.elsevier.com/artworkinstructions.
Any queries or remarks that have arisen during the processing of your manuscript are listed below and highlighted by flags in the proof.
Click on the Q link to go to the location in the proof.
Location in
article
Query / Remark: click on the Q link to go
Please insert your reply or correction at the corresponding line in the proof
Q15 AU: Location for Laboratoires Aguettant correct as added?
Q16 AU: Please add city, country location for Terumo?
Q17 AU: Per journal style, it is preferable to avoid subheadings in the Discussion; OK to remove all subheadings?
Q18 AU: Is change of "fibroids and uterus" to "uterine fibroids" correct?
Q19 AU: Is the sentence "Temporary clamping of the UA for 5–170 minutes generates a decrease in pH of the uterus in
association with pain, which can be attributed to anaerobic metabolism" correct as edited?
Q20 AU: Is "UFE" correctly spelled out?
Q21 AU: Please spell out IRFB here at first mention and at 2 subsequent mentions in this paragraph.
Q22 AU: Correct to add "and" before "a fibrotic reaction"?
Q23 AU: Please add a manufacturer and location for Gelfoam.
Q24 AU: Correct to add "after embolization" for fig 1b?
Q25 AU: Correct to add "after embolization" for fig 2b?
Q26 AU: Correct to expand "Med" as "median" and to add "%" in Table?
Q27 AU: Please remove bold from table body and add a footnote with asterisk to indicate the significance of this entry.
Thank you for your assistance.
Please check this box or indicate your approval
if you have no corrections to make to the PDF file
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657
Q4
Q1
Q7
Q8
Q9
LABORATORY INVESTIGATION
A Novel Resorbable Embolization Microsphere forTransient Uterine Artery Occlusion: A Comparative
Study with Trisacryl-Gelatin Microspheres in theSheep Model
Valentin Verret, Eng MSc, Jean Pierre Pelage, MD, Michel Wassef, MD,Stéphanie Louguet, PhD, Emeline Servais, PhD, Laurent Bédouet, PhD,
Thomas Beaulieu, Eng MSc, Laurence Moine, PhD, andAlexandre Laurent, MD, PhD
ABSTRACT
Purpose: To evaluate angiographic recanalization, inflammatory reaction, and uterine damage after sheep uterine artery embolization(UAE) with a novel calibrated resorbable embolization microsphere (REM) and compare the results with control nonresorbablemicrospheres.
Materials and Methods: Six hormonally cycled sheep underwent bilateral UAE until stasis with either REM or trisacryl-gelatinmicrospheres (TGMS). At 7 days, control angiograms were obtained to assess the residual vascularization at arterial and parenchymalphases. The animals were then sacrificed for analysis of the presence of microspheres, inflammatory foreign body reaction, and surfaceareas of uterine damage.
Results: Mean volume of microspheres injected per uterine artery (UA) or per animal did not differ between groups. At day 7, theflow was normal for six of six UAs that received embolization with REM versus only three of six UAs with TGMS (P ¼ .0455, χ2
test). Uterine parenchymography showed no defects in six UAs in the REM group versus five defects in six UAs in the TGMS group(P ¼ .0060, χ2 test). No REM or residual fragments of microspheres were observed on histologic analysis. TGMS were observed intissues and accompanied by a mild inflammatory response. Necrosis rates were not significantly different between the two products,either in endometrium (REM 23.5% � 28.8% [median 8.1%] vs TGMS 21.8% � 23.7% [median 14.6%]) or in myometrium (REM8.2%� 22.7% [median 0.0%] vs TGMS 8.8% � 20.8% [median 0.9%]). Endometrium alteration rate was lower with REM than withTGMS (39.7% � 25.7% [median 34%] vs 60.6% � 27.1% [median 71%]; P ¼ .0060, Mann-Whitney test). Myometrium alterationrates were not significantly different between REM (45.7% � 37.1% [median 63.0%]) and TGMS (37.8% � 34.0% [median 19.1%]).
Conclusions: At 1 week after sheep UAE with REM, the recanalization was complete, the microspheres were completely degraded,and there was no remnant inflammatory response.
ABBREVIATIONS
PEG = polyethylene glycol, PLGA = polylactic-glycolic acid, REM = resorbable embolization microsphere, TGMS = trisacryl-gelatin
microspheres, UA = uterine artery, UAE = uterine artery embolization
58596061626364656667686970
& 2014 Published by Elsevier, Inc., on behalf of the SIR.
J Vasc Interv Radiol 2014; XX:]]]–]]]
http://dx.doi.org/10.1016/j.jvir.2014.06.025
V.V., S.L., L.B., E.S., and T.B. receive salaries from Occlugel SAS. A.L., L.M.,and M.W. are shareholders in Occlugel SAS. J.P.P. is a paid consultant ofOcclugel SAS. This research work was funded by Occlugel SAS.
From Occlugel SAS (V.V., S.L., E.S., L.B., T.B.), Jouy en Josas; Service deRadiologie (J.P.P.), Centre Hospitalier Universitaire de Caen, Caen; Departe-ment de Pathologie (M.W.) and Departement de Neuroradiologie Interven-tionnelle (A.L.), APHP, Hôpital Lariboisière, 2 rue Ambroise Paré, 75010 Paris,France; UMR CNRS 8612 Institut Galien Paris-Sud (L.M.), Chatenay Malabry;Université René Diderot (M.W., A.L.), Paris; and Laboratoire MSC (A.L.), Paris,France. Received March 5, 2014; final revision received June 11, 2014;accepted June 25, 2014. Address correspondence to A.L.; E-mail: [email protected]
For uterine fibroid embolization, nonbiodegradable par-ticles are not ideal. After having played their occlusive role,they persist as remnant foreign bodies in the uterus andgenerate an inflammatory response, which sometimes maylast months (1–3). Uterine arteries (UAs) that receivedembolization may recanalize, but this is inconstant andpartial (2,4). It has been found in the sheep model thatembolization particles could constitute a durable obstacleto flow in UAs, even after a partial recanalization, reducingfertility or lowering birth weight (4).By contrast, biodegradable embolization materials are
designed to generate an inflammatory reaction that is
Original Text
givenname
Original Text
surname
Original Text
givenname
Original Text
surname
Original Text
givenname
Original Text
surname
Original Text
givenname
Original Text
surname
Original Text
givenname
Original Text
surname
Original Text
givenname
Original Text
surname
Original Text
givenname
Original Text
surname
Original Text
givenname
Original Text
surname
Original Text
givenname
Original Text
surname
Original Text
AU: Please approve shortened running head title or provide one that is 60 characters, including spaces.
Original Text
AU: Are all author degrees correct as added?
Original Text
Please confirm that given names and surnames have been identified correctly and are presented in the desired order.
Original Text
AU: Editing of Purpose to conform to journal style OK?
Original Text
AU: Need to explain the phrase "hormonally cycled"?
Original Text
AU: Correct to add "%" to median values?
Q10
Q11
Q12
Q13
Q14
Q15
7172737475767778798081828384858687888990919293949596979899
100101102103104105106107108109110111112113114115116117118119120121122123124125126127
128129130131132133134135136137138139140141142143144145146147148149150151152153154155156157158159160161162163164165166167168169170171172173174175176177178179180181182183184
Verret et al ’ JVIR2 ’ Novel REM for Transient UterineQ3 Artery Occlusion
limited to their period of resorption to insure a full andconstant recanalization of UA. The resorption time ofdegradable particles is long and associated with vasculardamage and remodeling that delay and limit recanaliza-tion. Gelatin sponge particles undergo a prolongeddegradation that lasts for weeks or months and isaccompanied by a chronic inflammatory response, vesselremodeling, and a fibrotic reaction (5,6). Collagen-coated polylactic-glycolic acid (PLGA) microspheresdegrade slowly over several months, they generate alocal inflammatory response, and the UAs remain fullyoccluded by fibrous connective tissue at 6 months (7).The persistence of particles in the vessel wall and theremodeling of the UA could act as an obstacle to bloodflow. The dilation of the UA that occurs duringpregnancy, which is important for gestation (8–10),could be compromised.To remedy these drawbacks, we have conceived
a resorbable embolization microsphere (REM) thatwould satisfy two imperatives. First, it should occludethe vessel for a short time—between a few hours and afew days—to achieve ischemia of fibroids. Second, itshould subsequently be quickly and completely elimi-nated, before the onset of a chronic inflammatoryresponse and vessel wall remodeling. We postulated thatthe UA recanalization and the absence of chronicinflammation would facilitate the healing process ofthe uterus, which could sustain collateral damage duringfibroid embolization. UA recanalization would be bene-ficial to changes in UA diameter during hormonalcycling and pregnancy.We designed the REM from a polyethylene glycol
(PEG) hydrogel cross-linked with hydrolyzable bridges(11). PEG hydrogel was chosen because it is usedin many biomedical applications for its hydrophili-city, elasticity, and biocompatibility (11). The resorptionspeed of PEG hydrogel REM can be controlled byadjusting the polymer chemistry of the hydrolyzablecross-link. The components were chosen to generate, afterhydrolysis, macromolecules that are water-soluble toavoid any accumulation in the organism leading toinflammatory reactions (12). Hydrolyzable linkages wereincorporated into the hydrogel backbone to shorten thesize of the polymer degradation products (o 50 kg/mol),facilitating renal elimination (13,14).PEG hydrogel microspheres with high water content
(� 90%) have been synthesized with sizes ranging from100–1,000 mm. Their biocompatibility was assessedin vitro by cytotoxicity tests of the microspheres andtheir degradation products on various cells in cultureand in vivo by subcutaneous implantation in rabbits (15).Degradation of the microspheres by hydrolysis inphosphate-buffered saline is achieved in o 24 hours.An in vivo study demonstrated that this REM allowedtargeted and efficient occlusion of renal arteries andangiographic recanalization at 1 week with no residualinflammation in tissue (16). The purpose of the present
study was to evaluate recanalization, inflammation, anduterine damage with REM 7 days after uterine arteryembolization (UAE) in the sheep model by comparisonwith a nonresorbable reference microsphere.
MATERIALS AND METHODS
MicrospheresREM (ResMic; Occlugel SAS, Jouy-en-Josas, France)were made by suspension polymerization of a PEGhydrogel cross-linked with PLGA-PEG-PLGA hydro-lyzable bridges (15). The formulation was adjusted toobtain a resorption time of 24 hours in phosphate-buffered saline. Hydrated REM were soft and containedabout 90% of water. After sieving at the size range of500–700 mm, REM were freeze-dried and sterilized by β-irradiation (IONISOS, Chaumesnil, France). REM werecompared with trisacryl-gelatin microspheres (TGMS)(Embosphere; Merit Medical Systems, Salt Lake City,Utah) at the nominal range 500–700 mm, which is themost common diameter used for uterine fibroid embo-lization in clinical practice.
AnimalsAll experiments were approved by the institutionalanimal care and use committee. Embolization (threeprocedures per type of embolic agent) was performedon six adult Préalpes Sheep (54 kg � 3, 48 mo � 22).For each animal, the type of embolic agent used wasrandomly assigned.
Embolization ProcedureSheep were artificially cycled 16 days before the embo-lization procedure to obtain a maximal dilation of UAs(17). Sheep were not fed for 24 hours before theprocedure. Anesthesia was induced by intramuscularinjection of 15 mg thiopental sodium (Nesdonal) perkilogram of body weight. Each animal was placed insupine position, intubated, anesthetized with a mixtureof 1.5% isoflurane (Vetflurane; Virbac, Carros, France)and 98.5% oxygen (Linde, Paris, France), and ventilatedusing a Primus workstation (Dräger Medical, Antony,France). End-tidal carbon dioxide levels were measuredcontinuously and maintained at 26–36 mm Hg with amonitor (Infinity Gamma XXL; Dräger Medical).Peripheral arterial oxygen saturation, maintained at495%, was monitored with a probe applied to the ear.Aliquots of 2 mL of embolization microspheres weresuspended in a solution of contrast agent (Telebrix35, 350 mg I/mL; Guerbet, Villepinte, France) and saline(Versol; Laboratoires Aguettant, Lyon, France) follow-ing the manufacturer’s instructions for use (REM, 12mL saline þ 6 mL contrast agent; TGMS, 8 mL saline þ10 mL contrast agent). Animals were randomly assignedto receive REM or TGMS. A 5-F vascular sheath wasplaced in the femoral artery by using the standard
Original Text
AU: Is "6 months" correct as added?
Original Text
AU: Addition of the phrase "which is important for gestation" OK?
Original Text
AU: Need to define or clarify the phrase "Sheep were artificially cycled"?
Original Text
AU: Please add manufacturer name and location for Nesdonal.
Original Text
AU: Is addition of the phrase "using a Primus workstation" correct?
Original Text
AU: Location for Laboratoires Aguettant correct as added?

Q16
F1 QF2QF3
185186187188189190191192193194195196197198199200201202203204205206207208209210211212213214215216217218219220221222223224225226227228229230231232233234235236237238239240241
242243244245246247248249250251252253254255256257258259260261262263264265266267268269270271272273274275276277278279280281282283284285286287288289290291292293294295296297298
Volume XX ’ Number X ’ Month ’ 2014 3
Seldinger technique under sterile conditions. Selectiveembolization of both internal iliac arteries was achievedusing a Cobra-type catheter, and superselective emboli-zation of both UAs was performed with a 2.7-F micro-catheter (Progreat, inner diameter 0.027 inch [0.65 mm];Terumo). The tip of the microcatheter was placed 4 cmdistally into the UA at the level of the uterine arch. Theinjection was performed slowly (1 mL/min) under fluo-roscopic control using 3-mL syringes. After injection ofthe embolic agent, the catheter was flushed with 3 mL ofsaline. Embolization was stopped when stasis of contrastmedium was observed in the UA. The stasis was assessed3 minutes later to ensure that no secondary redistrib-ution of embolization microspheres occurred. Theamount of microspheres injected to obtain stasis wasrecorded.
Follow-up and Sacrifice after EmbolizationVeterinary follow-up evaluation (behavior, appetite,complete blood count) was performed for each ewebefore sacrifice. In accordance with the protocol, ananimal with any abnormal behavior or in pain would besacrificed immediately. Otherwise, sacrifices were sched-uled at 7 days after embolization. On the day of sacrifice,bilateral control angiography of the UAs was per-formed. Sheep were sacrificed by pentobarbital injection(Dolethal; Vetoquinol, Paris, France) under anesthesia.
Angiographic ControlAngiography was performed before embolization toassess the vascular anatomy of each sheep. Embolizationwas considered successful if stasis was present in themain UA on angiography performed after embolization.Recanalization was assessed for each UA 7 days afterembolization and compared with initial angiography.The blood flow in the UA was evaluated using a three-grade scale: normal flow, reduced flow (defined ascontrast material visible during five heart beats beforedisappearing), and stasis (defined as the blockade of thecontrast column in the UA). Parenchymography wasassessed as normal (without defect of opacification), withdefects of opacification, or absent when there was noopacification of the parenchyma.Each uterus was sampled by cutting 10-mm-thick
slices in the body, in the left and right horns, and inthe ovaries. For each animal, two to three specimens ofthe body, five to six specimens of the horns, and onespecimen of each ovary were dehydrated in a series ofalcohols, set in xylene, embedded in paraffin, cut intoradial 4- to 5-mm-thick sections, and mounted on glassslides. Each section was stained with hematoxylin-eosin-saffron.
Histologic AnalysisHistologic slides were digitalized with a NanoZoomer2.0-HT slide scanner at a �20 objective (Hamamatsu,
Hamamatsu, Japan). Measurements were performedwith CaloPix (TRIBVN, Châtillon, France). Occludedvessels were analyzed on histologic sections for each typeof embolization material. The presence or absence ofrecanalization was assessed based on the presence orabsence of a vascular lumen with red blood cells orplasma in the area of the occluded vessel. Microscopicevaluation of the area of endometrial and myometriallesions was performed on each section. The two layers ofthe myometrium (ie, inner [circular muscle cells] andouter [longitudinal muscle cells]) were measured sepa-rately. Lesions were classified according to a three-gradescale: grade 0, normal tissue; grade 1, altered tissue (ie,tissues modified by fibrosis or cells with a modifiednucleus or cytoplasm); and grade 2, necrosis withdisappearance of nuclei. The percentage of normal,altered, or necrotized tissues was calculated as follows:percent of grade x in the region ¼ (sum of areas of gradex tissues in the region/total area of the region) * 100 (x is0, 1, or 2, and region is either the myometrium or theendometrium). All sections were reviewed to detectinflammatory cells such as macrophages, neutrophils,lymphocytes, and foreign body giant cells.
Statistical AnalysisStatistical analyses were performed on StatView SAS2000 (SAS Institute Inc, Cary, North Carolina). Becausethe continuous values measured mainly followed a non-Gaussian distribution, nonparametric Mann-Whitney orχ2 tests were performed for comparisons. Continuousvariables were expressed as median and mean � SD.
RESULTS
EmbolizationBilateral UAE was successful in all animals. The desiredangiographic endpoint (ie, arterial stasis) was obtainedin all cases (Figs 1a–d, 2a–d, 3a–d). There was no diffe-rence between TGMS and REM in terms of buoyancyafter mixing with contrast media and saline and no diffe-rence of injectability. For REM, a mean volume of 1.0mL � 0.5 of microspheres was injected per UA (range,0.5–2 mL) for a total of 2.1 mL � 0.8 per animal (range,1.5–3 mL). For TGMS, the mean volume was 1.6 mL �0.9 (range, 0.5–2.5 mL) for a total of 3.2 mL � 1.9 peranimal (range, 1–4.5 mL). No statistical difference bet-ween the two groups was found in terms of mean volumeof microspheres injected per UA (P ¼ .3785, Mann-Whitney) or per animal (P ¼ .5635, Mann-Whitney).During the follow-up period after embolization, therewas no abnormal behavior, no limping, and no pain. Noabnormal blood count was observed.
Angiographic RecanalizationArterial blood flow was graded normal for all UAarteries that received embolization with REM (six of
Original Text
AU: Please add city, country location for Terumo?
F4
F5
299300301302303304305306307308309310311312313314315316317318319320321322323324325326327328329330331332333334335336337338339340341342343344345346347348349350351352353354355
356357358359360361362363364365366367368369370371372373374375376377378379380381382383384385386387388389390391392393394395396397398399400401402403404405406407408409410411412
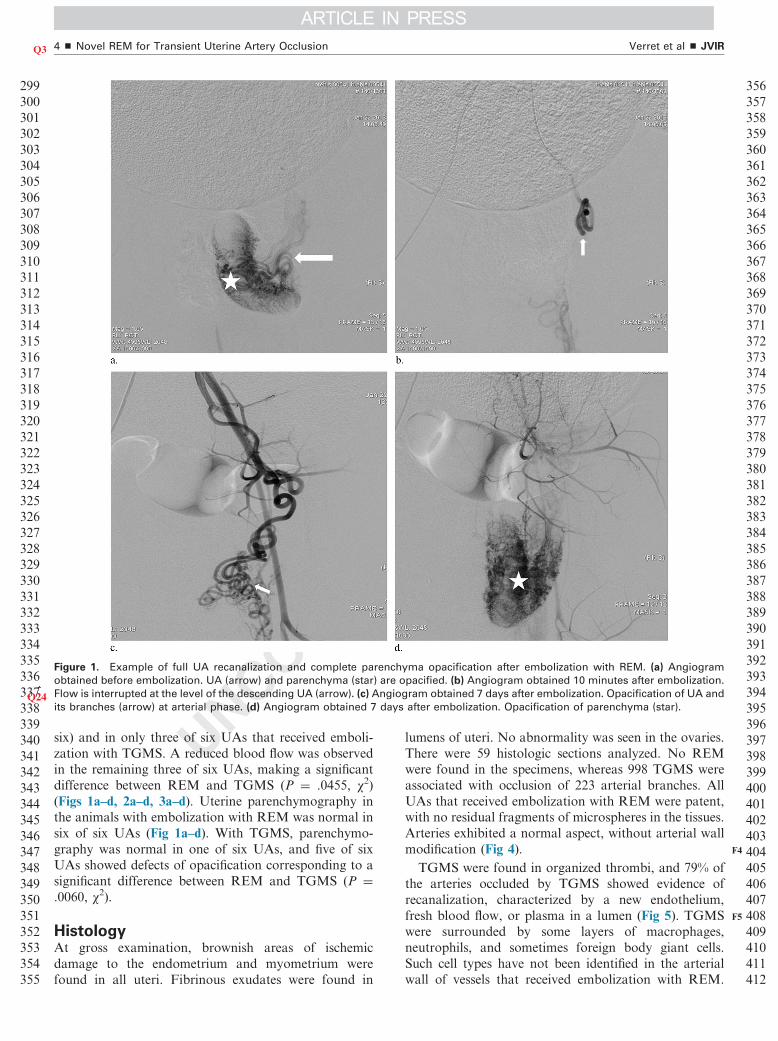
Figure 1. Example of full UA recanalization and complete parenchyma opacification after embolization with REM. (a) Angiogram
obtained before embolization. UA (arrow) and parenchyma (star) are opacified. (b) Angiogram obtained 10 minutes after embolization.
Q24 Flow is interrupted at the level of the descending UA (arrow). (c) Angiogram obtained 7 days after embolization. Opacification of UA and
its branches (arrow) at arterial phase. (d) Angiogram obtained 7 days after embolization. Opacification of parenchyma (star).
Verret et al ’ JVIR4 ’ Novel REM for Transient UterineQ3 Artery Occlusion
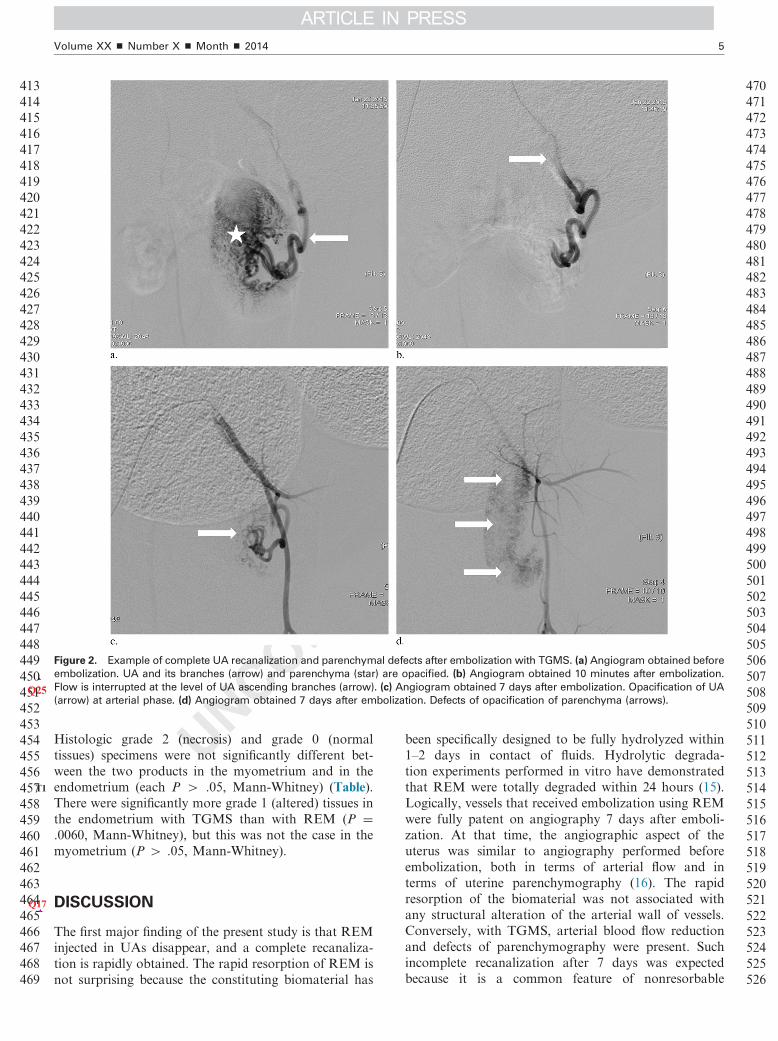
six) and in only three of six UAs that received emboli-zation with TGMS. A reduced blood flow was observedin the remaining three of six UAs, making a significantdifference between REM and TGMS (P ¼ .0455, χ2)(Figs 1a–d, 2a–d, 3a–d). Uterine parenchymography inthe animals with embolization with REM was normal insix of six UAs (Fig 1a–d). With TGMS, parenchymo-graphy was normal in one of six UAs, and five of sixUAs showed defects of opacification corresponding to asignificant difference between REM and TGMS (P ¼.0060, χ2).
HistologyAt gross examination, brownish areas of ischemicdamage to the endometrium and myometrium werefound in all uteri. Fibrinous exudates were found in
lumens of uteri. No abnormality was seen in the ovaries.There were 59 histologic sections analyzed. No REMwere found in the specimens, whereas 998 TGMS wereassociated with occlusion of 223 arterial branches. AllUAs that received embolization with REM were patent,with no residual fragments of microspheres in the tissues.Arteries exhibited a normal aspect, without arterial wallmodification (Fig 4).TGMS were found in organized thrombi, and 79% of
the arteries occluded by TGMS showed evidence ofrecanalization, characterized by a new endothelium,fresh blood flow, or plasma in a lumen (Fig 5). TGMSwere surrounded by some layers of macrophages,neutrophils, and sometimes foreign body giant cells.Such cell types have not been identified in the arterialwall of vessels that received embolization with REM.
Original Text
AU: Correct to add "after embolization" for fig 1b?
T1
Q17
413414415416417418419420421422423424425426427428429430431432433434435436437438439440441442443444445446447448449450451452453454455456457458459460461462463464465466467468469
470471472473474475476477478479480481482483484485486487488489490491492493494495496497498499500501502503504505506507508509510511512513514515516517518
Figure 2. Example of complete UA recanalization and parenchymal defects after embolization with TGMS. (a) Angiogram obtained before
embolization. UA and its branches (arrow) and parenchyma (star) are opacified. (b) Angiogram obtained 10 minutes after embolization.
Q25 Flow is interrupted at the level of UA ascending branches (arrow). (c) Angiogram obtained 7 days after embolization. Opacification of UA
(arrow) at arterial phase. (d) Angiogram obtained 7 days after embolization. Defects of opacification of parenchyma (arrows).
Volume XX ’ Number X ’ Month ’ 2014 5
Histologic grade 2 (necrosis) and grade 0 (normaltissues) specimens were not significantly different bet-ween the two products in the myometrium and in theendometrium (each P 4 .05, Mann-Whitney) (Table).There were significantly more grade 1 (altered) tissues inthe endometrium with TGMS than with REM (P ¼.0060, Mann-Whitney), but this was not the case in themyometrium (P 4 .05, Mann-Whitney).
519520521522523524525526
DISCUSSION
The first major finding of the present study is that REMinjected in UAs disappear, and a complete recanaliza-tion is rapidly obtained. The rapid resorption of REM isnot surprising because the constituting biomaterial has
been specifically designed to be fully hydrolyzed within1–2 days in contact of fluids. Hydrolytic degrada-tion experiments performed in vitro have demonstratedthat REM were totally degraded within 24 hours (15).Logically, vessels that received embolization using REMwere fully patent on angiography 7 days after emboli-zation. At that time, the angiographic aspect of theuterus was similar to angiography performed beforeembolization, both in terms of arterial flow and interms of uterine parenchymography (16). The rapidresorption of the biomaterial was not associated withany structural alteration of the arterial wall of vessels.Conversely, with TGMS, arterial blood flow reductionand defects of parenchymography were present. Suchincomplete recanalization after 7 days was expectedbecause it is a common feature of nonresorbable
Original Text
AU: Correct to add "after embolization" for fig 2b?
Original Text
AU: Per journal style, it is preferable to avoid subheadings in the Discussion; OK to remove all subheadings?
Q18
Q19
Q20
527528529530531532533534535536537538539540541542543544545546547548549550551552553554555556557558559560561562563564565566567568569570571572573574575576577578579580581582583
584585586587588589590591592593594595596597598599600601602603604605606607608609610611612613614615616617618619620621622623624625626627628629630631632633634635636637638639640
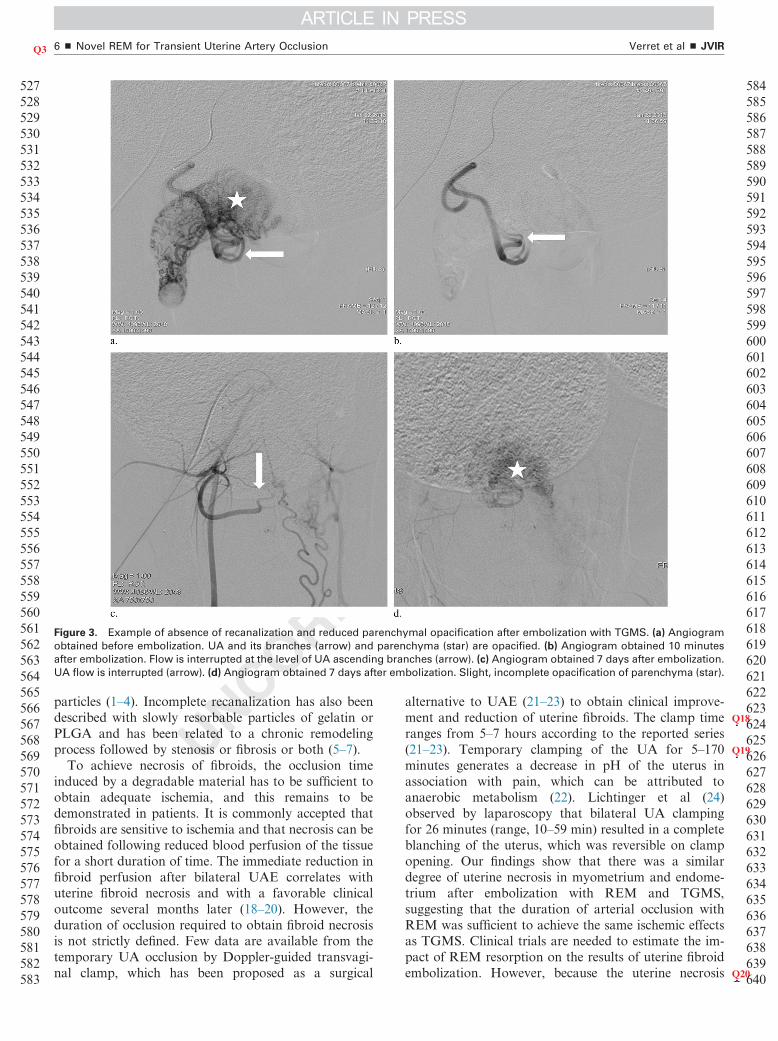
Figure 3. Example of absence of recanalization and reduced parenchymal opacification after embolization with TGMS. (a) Angiogram
obtained before embolization. UA and its branches (arrow) and parenchyma (star) are opacified. (b) Angiogram obtained 10 minutes
after embolization. Flow is interrupted at the level of UA ascending branches (arrow). (c) Angiogram obtained 7 days after embolization.
UA flow is interrupted (arrow). (d) Angiogram obtained 7 days after embolization. Slight, incomplete opacification of parenchyma (star).
Verret et al ’ JVIR6 ’ Novel REM for Transient UterineQ3 Artery Occlusion
particles (1–4). Incomplete recanalization has also beendescribed with slowly resorbable particles of gelatin orPLGA and has been related to a chronic remodelingprocess followed by stenosis or fibrosis or both (5–7).To achieve necrosis of fibroids, the occlusion time
induced by a degradable material has to be sufficient toobtain adequate ischemia, and this remains to bedemonstrated in patients. It is commonly accepted thatfibroids are sensitive to ischemia and that necrosis can beobtained following reduced blood perfusion of the tissuefor a short duration of time. The immediate reduction infibroid perfusion after bilateral UAE correlates withuterine fibroid necrosis and with a favorable clinicaloutcome several months later (18–20). However, theduration of occlusion required to obtain fibroid necrosisis not strictly defined. Few data are available from thetemporary UA occlusion by Doppler-guided transvagi-nal clamp, which has been proposed as a surgical
alternative to UAE (21–23) to obtain clinical improve-ment and reduction of uterine fibroids. The clamp timeranges from 5–7 hours according to the reported series(21–23). Temporary clamping of the UA for 5–170minutes generates a decrease in pH of the uterus inassociation with pain, which can be attributed toanaerobic metabolism (22). Lichtinger et al (24)observed by laparoscopy that bilateral UA clampingfor 26 minutes (range, 10–59 min) resulted in a completeblanching of the uterus, which was reversible on clampopening. Our findings show that there was a similardegree of uterine necrosis in myometrium and endome-trium after embolization with REM and TGMS,suggesting that the duration of arterial occlusion withREM was sufficient to achieve the same ischemic effectsas TGMS. Clinical trials are needed to estimate the im-pact of REM resorption on the results of uterine fibroidembolization. However, because the uterine necrosis
Original Text
AU: Is change of "fibroids and uterus" to "uterine fibroids" correct?
Original Text
AU: Is the sentence "Temporary clamping of the UA for 5–170 minutes generates a decrease in pH of the uterus in association with pain, which can be attributed to anaerobic metabolism" correct as edited?
Original Text
AU: Is "UFE" correctly spelled out?
641642643644645646647648649650651652653654655656657658659660661662663664665666667668669670671672673674675676677678679680681682683684685686687688689690691692693694695696697
698699700701702703704705706707708709710711712713714715716717718719720721722723724725726727728729730731732733734735736737738739740741
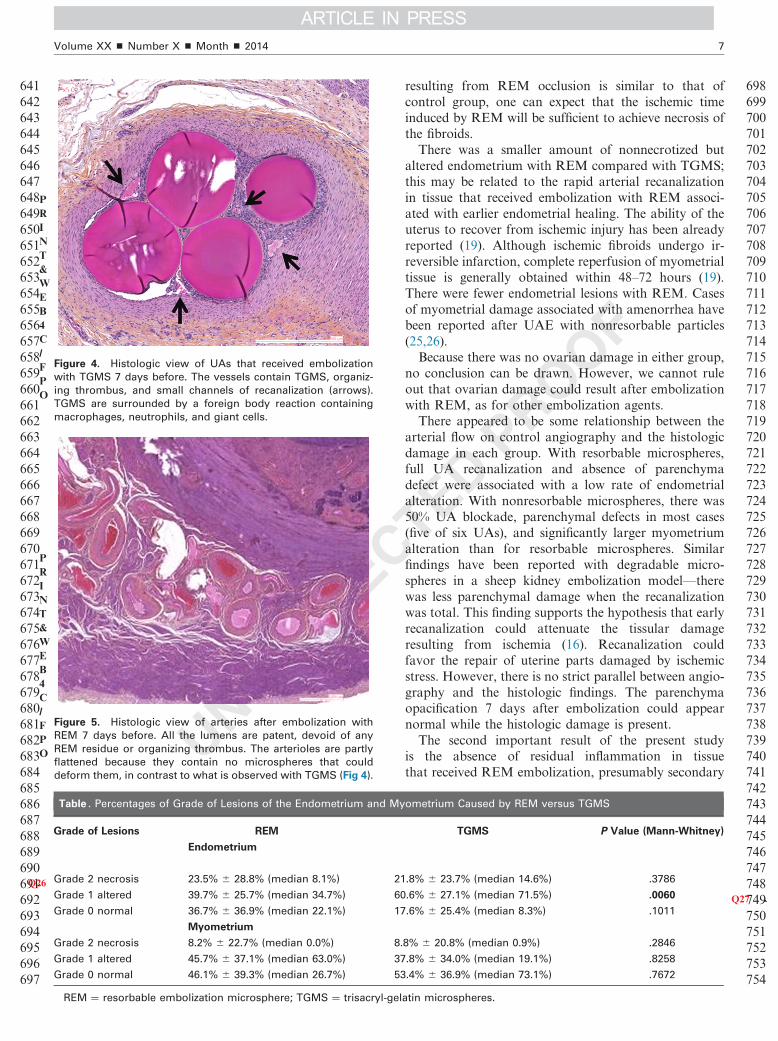
Figure 5. Histologic view of arteries after embolization with
REM 7 days before. All the lumens are patent, devoid of any
REM residue or organizing thrombus. The arterioles are partly
flattened because they contain no microspheres that could
deform them, in contrast to what is observed with TGMS (Fig 4).
PRINT&WEB4C/FPO
Figure 4. Histologic view of UAs that received embolization
with TGMS 7 days before. The vessels contain TGMS, organiz-
ing thrombus, and small channels of recanalization (arrows).
TGMS are surrounded by a foreign body reaction containing
macrophages, neutrophils, and giant cells.
PRINT&WEB4C/FPO
Table . Percentages of Grade of Lesions of the Endometrium and My
Grade of Lesions REM
Endometrium
GradeQ26 2 necrosis 23.5% � 28.8% (median 8.1%) 21
Grade 1 altered 39.7% � 25.7% (median 34.7%) 60
Grade 0 normal 36.7% � 36.9% (median 22.1%) 17
Myometrium
Grade 2 necrosis 8.2% � 22.7% (median 0.0%) 8.
Grade 1 altered 45.7% � 37.1% (median 63.0%) 37
Grade 0 normal 46.1% � 39.3% (median 26.7%) 53
REM ¼ resorbable embolization microsphere; TGMS ¼ trisacryl-gel
Volume XX ’ Number X ’ Month ’ 2014 7
resulting from REM occlusion is similar to that ofcontrol group, one can expect that the ischemic timeinduced by REM will be sufficient to achieve necrosis ofthe fibroids.There was a smaller amount of nonnecrotized but
altered endometrium with REM compared with TGMS;this may be related to the rapid arterial recanalizationin tissue that received embolization with REM associ-ated with earlier endometrial healing. The ability of theuterus to recover from ischemic injury has been alreadyreported (19). Although ischemic fibroids undergo ir-reversible infarction, complete reperfusion of myometrialtissue is generally obtained within 48–72 hours (19).There were fewer endometrial lesions with REM. Casesof myometrial damage associated with amenorrhea havebeen reported after UAE with nonresorbable particles(25,26).Because there was no ovarian damage in either group,
no conclusion can be drawn. However, we cannot ruleout that ovarian damage could result after embolizationwith REM, as for other embolization agents.There appeared to be some relationship between the
arterial flow on control angiography and the histologicdamage in each group. With resorbable microspheres,full UA recanalization and absence of parenchymadefect were associated with a low rate of endometrialalteration. With nonresorbable microspheres, there was50% UA blockade, parenchymal defects in most cases(five of six UAs), and significantly larger myometriumalteration than for resorbable microspheres. Similarfindings have been reported with degradable micro-spheres in a sheep kidney embolization model—therewas less parenchymal damage when the recanalizationwas total. This finding supports the hypothesis that earlyrecanalization could attenuate the tissular damageresulting from ischemia (16). Recanalization couldfavor the repair of uterine parts damaged by ischemicstress. However, there is no strict parallel between angio-graphy and the histologic findings. The parenchymaopacification 7 days after embolization could appearnormal while the histologic damage is present.The second important result of the present study
is the absence of residual inflammation in tissuethat received REM embolization, presumably secondary
742743744745746747748749750751752753754
ometrium Caused by REM versus TGMS
TGMS P Value (Mann-Whitney)
.8% � 23.7% (median 14.6%) .3786
.6% � 27.1% (median 71.5%) .006 Q270
.6% � 25.4% (median 8.3%) .1011
8% � 20.8% (median 0.9%) .2846
.8% � 34.0% (median 19.1%) .8258
.4% � 36.9% (median 73.1%) .7672
atin microspheres.
Original Text
AU: Correct to expand "Med" as "median" and to add "%" in Table?
Original Text
AU: Please remove bold from table body and add a footnote with asterisk to indicate the significance of this entry.
Q21
Q22
Q23
Q6
755756757758759760761762763764765766767768769770771772773774775776777778779780781782783784785786787788789790791792793794795796797798799800801802803804805806807808809810811
812813814815816817818819820821822823824825826827828829830831832833834835836837838839840841842843844845846847848849
Verret et al ’ JVIR8 ’ Novel REM for Transient UterineQ3 Artery Occlusion
to the rapid resorption of the biomaterial. No inflam-matory cells of foreign body type have been seen in theuteri that received embolization with REM, whichconfirms previous in vivo findings (15,16). The absenceof IRFB, consistent with the complete disappearance ofthe material in tissue, clearly distinguishes REM from allother embolic agents. Slowly resorbable materials areassociated with the presence of inflammatory cellsinfiltrated in the vessel wall, vessel remodeling, anda fibrotic reaction (5–7), so the functional vasculariza-tion of the organ is often limited (7). That no IRFBoccurs with REM is an improvement over existing em-bolic agents, including nondegradable and degradableagents such as absorbable gelatin sponge (Gelfoam),because the chronic inflammation that contributes to thepostembolization syndrome is circumvented. Conversely,a limited IRFB comprising macrophages, neutrophils,and sometimes foreign body giant cells was observedaround TGMS, as previously described (2,3).This study has some limitations. First, TGMS and
REM were assessed at a size range commonly used forUAE in clinical practice, but the results may not beextrapolated to other size ranges. Second, no uterinefibroid was present in our animal model, which limits theapplications of our results to the clinical situation. Third,results of angiographic recanalization were obtained 7days after embolization, and the time point for achievinga complete recanalization, presumably o 7 days, has notbeen precisely defined. Fourth, the results were obtainedon a small sample size. The present findings have to beconfirmed experimentally on larger animal cohorts andultimately in clinical trials comparing REM with otherdegradable agents used as controls.In conclusion, keeping the aforementioned limitations
in mind, it can be reasonably expected that such arapidly resorbable and calibrated material may become apromising embolization material for uterine fibroidembolization.
850851852853854
UNCITED REFERENCE
27
855856857858859860861862863864865866867
REFERENCES
1. Colgan TJ, Pron G, Mocarski EJ, et al. Pathologic features of uteri andleiomyomas following uterine artery embolization for leiomyomas. Am JSurg Pathol 2003; 27:167–177.
2. Weichert W, Denkert C, Gauruder-Burmester A, et al. Uterine arterialembolization with tris-acryl gelatin microspheres: a histopathologicevaluation. Am J Surg Pathol 2005; 29:955–961.
3. Chiesa AG, Hart WR. Uterine artery embolization of leiomyomaswith trisacryl gelatin microspheres (TGM): pathologic features andcomparison with polyvinyl alcohol emboli. Int J Gynecol Pathol 2004; 23:386–392.
4. Laurent A, Wassef M, Namur J, et al. Recanalization and particleexclusion after embolization of uterine arteries in sheep: a long-termstudy. Fertil Steril 2009; 91:884–892.
5. Ohta S, Nitta N, Sonoda A, et al. Embolization materials made of gelatin:comparison between Gelpart and gelatin microspheres. CardiovascIntervent Radiol 2010; 33:120–126.
6. Louail B, Sapoval M, Bonneau M, et al. A new porcine sponge materialfor temporary embolization: an experimental short-term pilot study inswine. Cardiovasc Intervent Radiol 2006; 29:826–831.
7. Owen RJ, Nation PN, Polakowski R, et al. A preclinical study of thesafety and efficacy of Occlusin 500 Artificial Embolization Device insheep. Cardiovasc Intervent Radiol 2012; 35:636–644.
8. Palmer SK, Zamudio S, Coffin C, Parker S, Stamm E, Moore LG.Quantitative estimation of human uterine artery blood flow and pelvicblood flow redistribution in pregnancy. Obstet Gynecol 1992; 80:1000–1006.
9. Dickey RP, Hower JF. Ultrasonographic features of uterine blood flowduring the first 16 weeks of pregnancy. Hum Reprod 1995; 10:2448–2452.
10. Konje JC, Kaufmann P, Bell SC, Taylor DJ. A longitudinal study ofquantitative uterine blood flow with the use of color power angiographyin appropriate for gestational age pregnancies. Am J Obstet Gynecol2001; 185:608–613.
11. Peppas NA, Hilt JZ, Khademhosseini A, Langer R. Hydrogels in biologyand medicine: from molecular principles to bionanotechnology. AdvMater 2006; 18:1345–1360.
12. Bergsma EJ, De Bruijn WC, Rozema FR, Bos RRM, Boering G. Latedegradation tissue response to poly (L-lactid) bone plates and screws.Biomaterials 1995; 16:25–31.
13. Yamaoka T, Tabata Y, Ikada Y. Fate of water-soluble polymers admin-istered via different routes. J Pharm Sci 1995; 84:349–354.
14. Fox ME, Szoka FC, Fréchet JM. Soluble polymer carriers for thetreatment of cancer: the importance of molecular architecture. Acc ChemRes 2009; 42:1141–1451.
15. Louguet S, Verret V, Bédouet L, et al. Poly(ethylene glycol) methacry-late hydrolyzable microspheres for transient vascular embolization. ActaBiomater 2014; 10:1194–1205.
16. Maeda N, Verret V, Moine L, et al. Targeting and recanalization afterembolization with calibrated resorbable microspheres versus handcutgelatin sponge particles in a porcine kidney model. J Vasc Interv Radiol2013; 24:1391–1398.
17. Pelage JP, Laurent A, Bonneau M, et al. Arterial blood supply to theuterus in nonpregnant sheep: a pertinent model for clinical practice?Invest Radiol 2001; 36:721–725.
18. deSouza NM, Williams AD. Uterine arterial embolization for leiomyo-mas: perfusion and volume changes at MR imaging and relation toclinical outcome. Radiology 2002; 222:367–374.
19. Scheurig-Muenkler C, Wagner M, Franiel T, Hamm B, Kroencke TJ.Effect of uterine artery embolization on uterine and leiomyoma perfusion:evidence of transient myometrial ischemia on magnetic resonanceimaging. J Vasc Interv Radiol 2010; 21:1347–1353.
20. Kroencke TJ, Scheurig C, Poellinger A, Gronewold M, Hamm B. Uterineartery embolization for leiomyomas: percentage of infarction predictsclinical outcome. Radiology 2010; 255:834–841.
21. Istre O, Hald K, Qvigstad E. Multiple myomas treated with a temporary,noninvasive, Doppler-directed, transvaginal uterine artery clamp. J AmAssoc Gynecol Laparosc 2004; 11:273–276.
22. Lichtinger M, Herbert S, Memmolo A. Temporary, transvaginal occlu-sion of the uterine arteries: a feasibility and safety study. J MinimInvasive Gynecol 2005; 12:40–42.
23. Vilos GA, Vilos EC, Abu-Rafea B, Hollett-Caines J, Romano W. Trans-vaginal Doppler-guided uterine artery occlusion for the treatment ofsymptomatic fibroids: summary results from two pilot studies. J ObstetGynaecol Can 2010; 32:149–154.
24. Lichtinger M, Burbank F, Hallson L, Herbert S, Uyeno J, Jones M. Thetime course of myometrial ischemia and reperfusion after laparoscopicuterine artery occlusion—theoretical implications. J Am Assoc GynecolLaparosc 2003; 10:554–563; quiz 564–566.
25. Davies C, Gibson M, Holt EM. Amenorrhoea secondary to endometrialablation and Asherman’s syndrome following uterine artery embolization.Clin Radiol 2002; 57:317–318.
26. Tropeano G, Litwicka K, Di Stasi C, Romano D, Mancuso S. Permanentamenorrhea associated with endometrial atrophy after uterine arteryembolization for symptomatic uterine fibroids. Fertil Steril 2003; 79:132–135.
27. Siskin GP, Dowling K, Virmani R, Jones R, Todd D. Pathologic evalua-tion of a spherical polyvinyl alcohol embolic agent in a porcine renalmodel. J Vasc Interv Radiol 2003; 14:89–98.
868
Original Text
AU: Please spell out IRFB here at first mention and at 2 subsequent mentions in this paragraph.
Original Text
AU: Correct to add "and" before "a fibrotic reaction"?
Original Text
AU: Please add a manufacturer and location for Gelfoam.
Original Text
AU: Please provide Ref. 27 is not cited in the text.