A New Instrument for Quantitative Analysis of Neonatal · Neonatal Neurobehavioral Examination A...
7
Neonatal Neurobehavioral Examination A New Instrument for Quantitative Analysis of Neonatal Neurological Status ANDREW M. MORGAN, VERA KOCH, VICKI LEE, and JEAN ALDAG A new neonatal neurobehavioral examination (NNE) was designed in response to the need for a more quantitative assessment of neonatal neurological status. The NNE consists of 27 items divided into three sections: 1) tone and motor patterns, 2) primitive reflexes, and 3) behavioral responses. Each section consists of 9 items scored on a three-point scale. Fifty-four healthy full-term infants were examined at 2 days of age and demonstrated total NNE scores ranging from 70 to a maximum possible score of 81 ( = 76, s = 1.03). Mean section scores for these infants ranged from 25.3 to 26.6 (s = .59-1.79). Intertester agreement was 88% by item and 95% by total score in each section. Two hundred ninety-eight high-risk infants were then examined at 37 to 40 weeks conceptional age (gestational age plus chronological age) or at discharge from the neonatal intensive care unit, whichever occurred first. Total NNE mean scores for high- risk infants fell into discrete clusters by conceptional age at the time of exami- nation (37-42 weeks, mean score = 66.5; 34-36 weeks, mean score = 60.7; <34 weeks, mean score = 51.1). Similar clustering occurred for the three section scores. Highly significant differences existed between the three conceptional age groups for total scores and section scores. No clinically significant score differences were associated with severity of illness or gestational age at birth. The results of this study suggest that the NNE easily and reliably assesses infants' neonatal neurobehavioral status at a given conceptional age. Additional studies are in progress to determine the value of the NNE in predicting subsequent developmental disabilities. Key Words: Child development; Pediatrics, evaluation; Tests and measurements, functional. The field of neonatology has changed dramatically over the past 25 years, con- tributing to a steady decline in the mor- tality and morbidity of smaller low birth-weight infants. 1,2 Despite ad- vanced technology, however, neonatal neurological deficits still occur. 3,4 The ability to assess neonatal brain function and, thereby, to predict neurological deficits remains rudimentary. Multiple risk factors associated with neurological impairment have been identified, but no method exists to determine whether a specific perinatal event has actually re- sulted in irreversible brain damage. 5,6 Cranial sonography performed at var- ious times during the neonatal course has been shown to demonstrate struc- tural abnormalities such as periventric- ular leukomalacia or cystic changes, 7 but the predictive significance of these findings in terms of irreversible injury is still uncertain. 8 Clinical examination remains the most effective way to assess neonatal neurological status. The pioneer work of Thomas et al in the 1960s focused on a more classical neurological examina- tion that emphasized active tone, pas- sive tone, and primitive reflexes. 9 Prechtl and Beintema 10 and Amiel- Tison 11 subsequently designed neuro- logical scales using the data of Thomas et al 9 to assess neonatal maturity. With the introduction of the Brazelton Neo- natal Behavioral Assessment Scale (BNBAS) in 1973, however, the focus shifted to a more behavioral orientation that emphasized sensory processing and interactive responses. 12 As interest in early identification of developmental problems grew, new neonatal assess- ment scales emerged that combined both behavioral and neurological ap- proaches. 13,14 Although many neonatal assessment scales are currently available to the cli- nician, 15 almost all of them provide a descriptive, qualitative impression of neurobehavioral function that is de- pendent on the skill and experience of the examiner. This "gestalt" approach can identify areas of concern but is of limited value in predicting develop- mental outcome or assessing the success of treatment alternatives. Some scales have been modified to allow statistical interpretation, such as the "a priori clus- ters" of BNBAS items by Als et al 16 or the "optimality" scoring of Prechtl, 17 but none of the scales offer the concise nu- A. Morgan, MD, is Chief, Section of Child De- velopment, and Assistant Professor, Department of Pediatrics, The University of Illinois College of Medicine at Peoria, 530 NE Glen Oak Ave, North Building, Peoria, IL 61637. Address correspondence to PO Box 1649, The University of Illinois College of Medicine at Peoria, Peoria, IL 61656 (USA). V. Koch, MS, is Clinical Associate, Division of Child Development, Department of Pediatrics, The University of Illinois College of Medicine at Peoria. V. Lee, BS, is Clinical Assistant, Division of Child Development, Department of Pediatrics, The University of Illinois College of Medicine at Peoria. J. Aldag, PhD, is Associate Professor of Medi- cine, Department of Medicine, The University of Illinois College of Medicine at Peoria. This article was submitted April 24, 1987; was with the authors for revision 17 weeks; and was accepted March 15, 1988. Potential Conflict of In- terest: 4. 1352 PHYSICAL THERAPY
-
Upload
trinhnguyet -
Category
Documents
-
view
221 -
download
0
Transcript of A New Instrument for Quantitative Analysis of Neonatal · Neonatal Neurobehavioral Examination A...

Neonatal Neurobehavioral Examination A New Instrument for Quantitative Analysis of Neonatal Neurological Status ANDREW M. MORGAN, VERA KOCH, VICKI LEE, and JEAN ALDAG
A new neonatal neurobehavioral examination (NNE) was designed in response to the need for a more quantitative assessment of neonatal neurological status. The NNE consists of 27 items divided into three sections: 1) tone and motor patterns, 2) primitive reflexes, and 3) behavioral responses. Each section consists of 9 items scored on a three-point scale. Fifty-four healthy full-term infants were examined at 2 days of age and demonstrated total NNE scores ranging from 70 to a maximum possible score of 81 ( = 76, s = 1.03). Mean section scores for these infants ranged from 25.3 to 26.6 (s = .59-1.79). Intertester agreement was 88% by item and 95% by total score in each section. Two hundred ninety-eight high-risk infants were then examined at 37 to 40 weeks conceptional age (gestational age plus chronological age) or at discharge from the neonatal intensive care unit, whichever occurred first. Total NNE mean scores for high-risk infants fell into discrete clusters by conceptional age at the time of examination (37-42 weeks, mean score = 66.5; 34-36 weeks, mean score = 60.7; <34 weeks, mean score = 51.1). Similar clustering occurred for the three section scores. Highly significant differences existed between the three conceptional age groups for total scores and section scores. No clinically significant score differences were associated with severity of illness or gestational age at birth. The results of this study suggest that the NNE easily and reliably assesses infants' neonatal neurobehavioral status at a given conceptional age. Additional studies are in progress to determine the value of the NNE in predicting subsequent developmental disabilities.
Key Words: Child development; Pediatrics, evaluation; Tests and measurements, functional.
The field of neonatology has changed dramatically over the past 25 years, contributing to a steady decline in the mortality and morbidity of smaller low birth-weight infants.1,2 Despite advanced technology, however, neonatal neurological deficits still occur.3,4 The ability to assess neonatal brain function and, thereby, to predict neurological
deficits remains rudimentary. Multiple risk factors associated with neurological impairment have been identified, but no method exists to determine whether a specific perinatal event has actually resulted in irreversible brain damage.5,6
Cranial sonography performed at various times during the neonatal course has been shown to demonstrate structural abnormalities such as periventricular leukomalacia or cystic changes,7
but the predictive significance of these findings in terms of irreversible injury is still uncertain.8
Clinical examination remains the most effective way to assess neonatal neurological status. The pioneer work of Thomas et al in the 1960s focused on a more classical neurological examination that emphasized active tone, passive tone, and primitive reflexes.9
Prechtl and Beintema10 and Amiel-Tison11 subsequently designed neurological scales using the data of Thomas et al9 to assess neonatal maturity. With the introduction of the Brazelton Neo
natal Behavioral Assessment Scale (BNBAS) in 1973, however, the focus shifted to a more behavioral orientation that emphasized sensory processing and interactive responses.12 As interest in early identification of developmental problems grew, new neonatal assessment scales emerged that combined both behavioral and neurological approaches.13,14
Although many neonatal assessment scales are currently available to the clinician,15 almost all of them provide a descriptive, qualitative impression of neurobehavioral function that is dependent on the skill and experience of the examiner. This "gestalt" approach can identify areas of concern but is of limited value in predicting developmental outcome or assessing the success of treatment alternatives. Some scales have been modified to allow statistical interpretation, such as the "a priori clusters" of BNBAS items by Als et al16 or the "optimality" scoring of Prechtl,17 but none of the scales offer the concise nu-
A. Morgan, MD, is Chief, Section of Child Development, and Assistant Professor, Department of Pediatrics, The University of Illinois College of Medicine at Peoria, 530 NE Glen Oak Ave, North Building, Peoria, IL 61637. Address correspondence to PO Box 1649, The University of Illinois College of Medicine at Peoria, Peoria, IL 61656 (USA).
V. Koch, MS, is Clinical Associate, Division of Child Development, Department of Pediatrics, The University of Illinois College of Medicine at Peoria.
V. Lee, BS, is Clinical Assistant, Division of Child Development, Department of Pediatrics, The University of Illinois College of Medicine at Peoria.
J. Aldag, PhD, is Associate Professor of Medicine, Department of Medicine, The University of Illinois College of Medicine at Peoria.
This article was submitted April 24, 1987; was with the authors for revision 17 weeks; and was accepted March 15, 1988. Potential Conflict of Interest: 4.
1352 PHYSICAL THERAPY

RESEARCH merical system necessary for quantitative analysis and true standardization.
We attempted to design and standardize a new assessment scale that would characterize the various aspects of neu-robehavioral fitness at a given concep-tional age (gestational age in weeks and chronological age from delivery in weeks) with objective, numerical scores. A quantitative rather than qualitative assessment of neonatal neurobehavioral status would be valuable in the identification of infants at risk for developmental disabilities and would also provide a research tool for evaluating early treatment protocols.
METHOD
Design of the Neonatal Neurobehavioral Examination
After extensive review of existing gestational age scales and neonatal examinations, we selected 27 items for use in a neonatal neurobehavioral examination (NNE) because of their ability to reflect the distinct changes in neurobehavioral function that occur with increasing maturation. Alterations in arm recoil or prone suspension, for example, emerge as the infant's muscle tone gradually increases with gestational age. Grasp, positive support, and other primitive reflexes, and behavioral responses such as alertness and consolability also change in quality and intensity as the infant approaches full term. Almost all of the assessment items were taken from the previous work of Thomas et al,9
Brazelton,12 and Dubowitz and Dubo-witz.13 Other items, such as slip-through at the shoulders, were added to include areas of function not addressed in other assessment scales. Several traditional assessment items were eliminated because they were either redundant or inappropriate when applied to a premature infant. For example, both heel-to-ear and popliteal angles are measures of hip and lower extremity tone, so only popliteal angle was included on the NNE. Because all high-risk infants are exposed to the noxious lights and sounds in the neonatal intensive care unit and must habituate to them to some degree, we believed that the BNBAS response-decrement items were of questionable value and did not include them on the NNE. The 27 assessment items were organized into three sections representing different aspects of neurobehavioral status: 1) tone and motor patterns, 2) primitive reflexes, and 3) behavioral re
sponses. Each section consisted of nine assessment items.
A three-point scoring system was then applied to each item. A four- or five-point system was rejected because we believed it would result in more subtle differences in the performance choices and produce greater scoring indecision than a three-point scale. A three-point system simplified the assessment process and allowed the examiner to choose between more obvious differences in the observed performance of each item. The longitudinal data of Thomas et al9 demonstrated that distinct changes in active tone, passive tone, and primitive reflexes occur at about 32 weeks gestational age and again at about 36 weeks gestational age. The resting posture of an infant, for example, shows absence of extremity flexion before 32 weeks gestational age, leg flexion between 32 and 36 weeks gestational age, and flexion of all extremities after 36 weeks gestational age. Similarly, grasp is weak before 32 weeks gestational age, reasonably strong between 32 and 36 weeks, and strong enough to lift the infant off the bed (traction response) after 36 weeks gestational age. The natural evolution of tone and primitive reflexes, therefore, coincides nicely with a three-point scoring system.
In the tone and motor patterns and primitive reflexes sections, a score of 3 reflected responses expected of a full-term infant (37-42 weeks gestational age), a 2 reflected responses expected at 32 to 36 weeks gestational age, and a 1 reflected responses expected at less than 32 weeks gestational age. Exaggerated responses that are generally considered to be signs of neurological injury (eg, shoulder retraction, fisting, or equinus) were included in a separate column and were assigned a score of 1. The behavioral responses section was divided into three subtests—responsiveness, temperament, and equilibration—with three items in each subtest. The three subtests represented three distinct aspects of behavioral performance. Items in the responsiveness section reflect the infant's general ability to process and respond to external stimuli, items in the temperament section reflect the level of the infant's threshold to noxious stimuli, and items in the equilibration section reflect the ability of the infant to return to an emotional baseline after the stimulation threshold has been exceeded. The original Brazelton scales12 for the selected items were modified so that a score of 3 consistently represented optimal per
formance, and a score of 1 consistently represented a deficient response. The original nine-point scoring system was condensed into a three-point system to conform to the design of the other NNE items and to reduce the likelihood of scoring indecision.
Scores of the 9 items in each section were summed to provide section scores in addition to a total score for all 27 items. The maximum total score possible was 81, and the minimum total score possible was 27. In the behavioral responses section, each subtest was also given a cluster score. The subtest was assigned a cluster score of 3 if two of the three items in the subtest were scored as 3, a score of 1 if two of the three items were scored as 1, and a score of 2 for all other combinations. This multivariate scoring system was used at the outset to improve the possibility of ultimately finding a marker or combination of markers predictive of outcome. A scoring sheet was designed with all instructions and scoring mechanisms on the front and back of a single page to simplify administration of the NNE (Appendix).
Standardization
Full-term infants. We reviewed the records of all admissions to the newborn nurseries of two local hospitals from May 1983 to September 1983. Only infants with completely normal prenatal and perinatal courses were identified as potential subjects for the full-term infant standardization of the NNE. Infants were selected who satisfied the following criteria: 1) gestational age of 38 to 40 weeks as determined by dates and Dubowitz scoring system, 2) serial prenatal care, 3) no maternal problems (eg, toxemia, diabetes, medications), 4) spontaneous vaginal delivery without complications, 5) 5- and 10-minute Apgar scores of 9 or 10, 6) no resuscitation needed, 7) normal newborn examination results, 8) normal activity and sleep pattern in the nursery, and 9) no feeding problems. These infants were examined with the NNE at 48 hours postgesta-tional age midway between feedings in a quiet, dimly lit area adjacent to the nursery. Informed consent was obtained from the infants' parents. A subgroup of subjects was examined separately by two of the authors (V.K. and V.L.) within the same hour to determine intertester agreement.
High-risk infants. The NNE was subsequently standardized on a randomly
Volume 68 / Number 9, September 1988 1353

selected group of infants in the neonatal intensive care unit at Saint Francis Medical Center (Peoria, Ill) who were considered to be at greatest risk for developmental disability. The criteria for inclusion in the standardization process were 1) birth weight less than 1,500 g, 2) respiratory difficulty requiring mechanical ventilation, or 3) any neurological complication (eg, intraventricular hemorrhage, meningitis, seizures, or prolonged hypotonia). Infants with congenital defects were excluded from the study. Infants selected to participate in the study were enrolled in a follow-up program to monitor their developmental outcome.18
Infants eligible for inclusion in the standardization process were monitored by the neonatal intensive care staff during their hospitalization. The infants were scheduled for examination by one of two therapists (V.K. or V.L.) as they approached conceptional term (37-42 weeks conceptional age) or at discharge, whichever occurred first. The examination was performed as part of routine care, but informed consent was obtained from the infants' parents whenever possible. Because the population included a combination of infants born in the hospital and infants admitted after birth, many infants were discharged or transferred back to referring hospitals before they reached conceptional term or before they could be examined. The NNE was performed at the infants' bedside midway between feedings with no special preparation. The examination was postponed if the infant was medically unstable or had recently experienced an invasive procedure.
Data Analysis
Full-term infants. Means and standard deviations of the three section scores and the total score on the NNE were determined for full-term infants. Inter-tester agreement was established both by total score and by individual item.
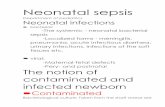
High-risk infants. Visual inspection of the mean total scores (Figure) and the three section scores for high-risk infants examined at each conceptional age demonstrated three distinct conceptional age clusters: 1) 33 weeks of age or less, 2) 34 to 36 weeks of age, and 3) 37 weeks of age or more at the time of examination. The infants, therefore, were divided into these three conceptional age groups in the subsequent data analysis. We also divided the infants into three groups by severity of illness according to the
Figure. Mean total scores of high-risk infants on the neonate neurobehavioral examination by conceptional age (in weeks) at time of examination.
amount of ventilatory support they required (<2 days, 2-7 days, or >7 days).
To study the NNE score differences associated with conceptional age and severity of illness, four two-way analyses of variance (ANOVAs) were performed for each measure (tone and motor patterns, primitive reflexes, behavioral responses, and total score). Post hoc t tests were planned if a significant interaction effect occurred to determine the nature of the mean differences. If no interaction effect existed, the main effects were tested and post hoc t tests were used to determine where the group differences occurred for any significant main effect. Because four separate primary analyses were made, an alpha level of .05 with a Bonferroni correction19 (0.5/4) yielded an acceptable level of significance of .013. The SPSS-PCplus ANOVA and t-test programs were used.20,21
We also determined correlations between conceptional age, gestational age, severity of illness, tone and motor patterns, primitive reflexes, behavioral responses, and total score. Means and standard deviations were reported by conceptional age groups for all four measures. The SPSS-PCplus CORRELATION program was used.20
RESULTS
Full-term Infants Fifty-four full-term infants satisfied
the study criteria and were available for examination. The NNE was completed and scored for each infant within 15
minutes. A scorable response was obtained for each item on each infant. Mean age of testing was 46 hours (s = 6 hours) postgestational age.
Means, ranges, and standard deviations were calculated for the three section scores and the total score (Tab. 1). Limited variability in scores existed for these presumably "normal" full-term infants. Eighty percent of the section scores were between 25 and 27, with standard deviations ranging from 0.6 to 1.8. Variability in full-term infants' performance, as reflected by the range of scores and the standard deviation, was greatest for behavioral responses and almost nonexistent for tone and motor patterns. No section scores were below 20, and no total scores were below 70. All behavioral subtests were rated 2 or 3.
Intertester agreement was established based on paired examinations of 20 children performed by two examiners (V.K. and V.L.) within an hour of each other (Tab. 2). We found an average of 88% item agreement and 95% section agreement between examiners.
High-risk Infants
Between May 1983 and June 1985, 298 high-risk infants who satisfied the inclusion criteria were examined with the NNE. As with the full-term infants, the NNE was completed and scored on all high-risk subjects within 15 minutes. A scorable response was obtained for each item on each infant examined.
The results of the two-way ANO VAs
1354 PHYSICAL THERAPY

RESEARCH
TABLE 1 Scores of Full-term Infants on the Neonatal Neurobehavioral Examination (N = 54)
Section
Tone and motor patterns Primitive reflexes Behavioral responses Total score
26.6 25.3 25.5 76.0
s
.59 1.45 1.79 1.03
Range
(25-27) (22-27) (20-27) (70-81)
TABLE 2 Intertester Agreement on the Neonatal Neurobehavioral Examination for Full-term Infants (N = 54)
Section
Tone and motor patterns Primitive reflexes Behavioral responses
Agreement (%)
Item by Item
93 88 83
Section Score
97 95 93
are reported in Table 3. No significant interactions existed for tone and motor patterns, primitive reflexes, behavioral responses, or total score. In addition, no significant differences were associated with severity of illness. For the concep-tional age groups, however, highly significant differences were found for each of the four measures. When t tests were conducted for each measure by concep-tional age group, significant differences (p < .001) existed between all three age groups for each measure. An inspection of the means by age group demonstrated that the youngest age group consistently had lower scores than the older age groups (Tab. 4).
Consistent with the findings of the two-way ANOVAs, the Pearson correlation matrix showed that the correlation of conceptional age with each of the four test measures was significant (Tab. 5). Similarly, there was no correlation of severity of illness with any of the four measures. A mild correlation of gestational age with scores on the tone and motor patterns section was found. Although this correlation was not clinically significant, it did reach statistical significance because of the large sample size. No other significant correlation of gestational age with test measures occurred.
Correlations among the three sectional scores (tone and motor patterns, primitive reflexes, and behavioral responses) varied from .498 to .630, indicating a modest amount of overlap between the scores varying from 24% to 40% (correlation squared) of the variance. These modest correlations indicate that although some overlap existed
between the section scores, a reasonable amount of variance was unique to each one. Substantial correlations existed between each section score, with the total scores varying from .804 to .862. The variance in total scores was not unexpected because the total score is a summation of the three section scores.
DISCUSSION
The results of the initial phase of standardization demonstrate that the NNE provides a quantitative representation of the multiple aspects of full-term infants' neurobehavioral status. The high numerical scores obtained indicate that the actual performance of the healthy full-term infants coincides with the theoretical design of the instrument; that is, healthy full-term infants obtained a score of 3 (the score expected of a full-term infant) on almost all of the NNE items. Behavioral responses, in general, appeared to be more diverse than the more neurological items. Very little score variability, nevertheless, was shown overall.
Analysis of the data on high-risk infants yielded similar encouraging results. The total means and section means for all high-risk groups were lower than those established for full-term infants. These results are consistent with growing evidence that even relatively healthy premature infants do not perform as well when they reach conceptional term as do their full-term counterparts.19
A very distinct pattern of distribution for the high-risk scores created three significantly different conceptional age clusters (37-42 weeks, 34-36 weeks, and <34 weeks conceptional age). These clusters approximated the design of the three-point scoring system, theoretically representing performance at greater than 36 weeks, 32 to 36 weeks, and less than 32 weeks gestational age. This finding suggests that the NNE as designed does reflect gestational maturation and is a quantitative representative of neurobehavioral status at a given conceptional age.
Additional analysis of the high-risk
infants' data demonstrated that the scores appear to depend primarily on conceptional age at the time of the examination; gestational age at birth and severity of illness do not appear to be major contributing factors to NNE score. The correlation matrix indicates a reasonable amount of variance unique to each section score and supports the importance of including all three neurobehavioral sections on the NNE. No one developmental area is representative of neonatal neurological status, and items assessing these three areas should be included in any neonatal evaluation tool.
The NNE, therefore, appears to be an efficient and accurate assessment of neurobehavioral status at the time of the infant's discharge from the nursery. The NNE is easy to administer to both full-term and premature infants and has good intertester agreement. It has an advantage over previously published scales in that it offers a numerical representation of neurobehavioral status rather than a gestalt impression. Additional studies are in progress to determine the potential clinical applications of the NNE.
CONCLUSION
The NNE was developed in response to the need for a more quantitative assessment of neonatal neurobehavioral status. The 27-item examination measuring tone and motor patterns, primitive reflexes, and behavioral responses was standardized on a sample of 54 healthy full-term infants and 298 high-risk infants. The total score and three section scores varied primarily by conceptional age at examination (gestational age and chronological age) independent of gestational age or severity of illness. Full-term infants scored higher on all measures than preterm infants examined at conceptional term.
Recent federal and state legislation has mandated that every infant at risk for possible developmental disabilities must be identified and referred for appropriate intervention services from the nursery.22 This identification process would be enhanced by an examination capable of assessing neonatal neurobehavioral status as a predictor of subsequent disabilities. The NNE has been shown to be an effective and reliable method of quantifying the neurobehavioral abilities of infants at the time of examination. Additional studies of the NNE are needed to establish its predic-
Volume 68 / Number 9, September 1988 1355

TABLE 3 Two-way Analysis of Variance by Age Group and Severity of Illness for High-risk Infants on the Neonatal Neurobehavioral Examination (N = 298)
Main effect Age group Severity of illness
Interaction Age group x sever
ity of illness
df
2 2
4
Tone and Motor Patterns
<.001 <.153
<.419
P
Primitive Reflexes
<.001 <.086
<.535
Behavioral Responses
<.001 <.229
<.264
Total Score
<.001 <.098
<.462
TABLE 4 High-risk Infants' Mean Scores and Standard Deviations by Conceptional Age Group for Each Neonatal Neurobehavioral Examination Section (N = 298)
Section
Tone and motor patterns
s Primitive reflexes
s Behavioral responses
s Total score
s
Conceptional Age (wk) at Time of Examination
<34 (n = 21)
17.43 3.25
17.38 3.53
16.33 3.94
51.14 9.49
34-36 (n = 138)
20.51 2.98
20.28 3.06
20.09 3.82
60.65 8.00
>36 (n = 139)
22.57 2.90
22.01 3.10
21.84 3.31
66.45 7.45
TABLE 5 Correlation of Conceptional Age with Neonatal Neurobehavioral Examination Section (N = 298)
Conceptional age (CA) Gestational age (GA) Tone and motor patterns
(TMP) Primitive reflexes (PR) Behavioral responses
(BEH) Total score (TS) Severity of illness (SI)
CA
1.000
GA
.427a
1.000
TMP
.413a
.161b
1.000
PR
.337a
.038
.573a
1.000
BEH
.291a
.137
.498a
.630a
1.000
TS
.412a
.139
.804a
.862a
.847a
1.000
SI
.243b
-.222a
.020
.061
-.029 .007
1.000
tive value and ability to measure change in response to intervention protocols. We currently are conducting a detailed item-by-item analysis of the NNE and a
correlation of the NNE with developmental outcome to determine the clinical value of the NNE in the follow-up of high-risk infants.
REFERENCES
1. Shapiro S, McCormick M, Crawley B, et al: Changes in infant morbidity associated with decreases in neonatal mortality. Pediatrics 72:408-415, 1983
2. Caron B, Hack M, Rivers A: The very low birthweight infant: The broader spectrum of morbidity during infancy and early childhood. J Dev Behav Pediatr 4:343-349, 1983
3. Kitchens W, Keir E, Keith C, et al: Changing outcome over 13 years of very low birthweight infants. Semin Perinatol 6:373-387, 1982
4. Ross G: Morbidity and mortality in very low birthweight infants. Pediatr Ann 12:32-44, 1983
5. Siegal L, Saigal S, Rosenbaum P: Correlates and predictors of cognitive and language development of low birthweight infants. J Pediatr Psychol 7:135-148, 1982
6. Nelson K, Ellenberg J: Neonatal signs as predictors of cerebral palsy. Pediatrics 64:225-231,1979
7. Weindling A, Rochefort M, Calvert S, et al: Development of cerebral palsy after ultrasonographic detection of periventricular cysts in the newborn. Dev Med Child Neurol 27:800-806,1985
8. Graziani L, Pasto M, Stanley C, et al: Neonatal neurosonographic correlates of cerebral palsy in the preterm infant. Pediatrics 78:88-94, 1986
9. Thomas A, Chesni Y, St. Anne Dargassies S: The Neurological Examination of the Infant. London, United Kingdom, Spastics International Medical Publications, 1960
10. Prechtl H, Beintema D: The Neurological Examination of the Full Term Newborn Infant, ed 2. Philadelphia, PA, J B Lippincott Co, 1984
11. Amiel-Tison C: Neurological evaluation of the maturity of newborn infants. Arch Dis Child 43:89-93,1968
12. Brazelton TB: Neonatal Behavioral Assessment Scale. Philadelphia, PA, J B Lippincott Co, 1984
13. Dubowitz L, Dubowitz V: Assessment of the Preterm and Full Term Infant. Philadelphia, PA, J B Lippincott Co, 1981
14. Kurtzberg D, Vaughn H, Daum C, et al: Neurobehavioral performance of low birthweight infants at 40 weeks post-conceptional age: Comparison with normal full term infants. Dev Med Child Neurol 21:590-607, 1979
15. Gorski P, Lewkowicz D, Huntington L: Advances in neonatal and infant behavioral assessment: Toward a comprehensive evaluation of early patterns of development. J Dev Behav Pediatr 8:39-53, 1986
16. Als H, Tronick E, Lester B, et al: The Brazelton Neonatal Behavioral Assessment Scale (BNBAS). Abnormal Child Psychology 5:215-231,1977
17. Prechtl H: Assessment methods for the newborn infant: A critical review. In Stratton P (ed): Psychobiology of the Human Newborn. New York, NY, John Wiley & Sons Inc, 1982, pp 21-52
18. Cohen H, Morgan A: Neonatal follow-up: A regional program. IMJ 170:23-26, 1986
19. Godfrey K: Comparing the means of several groups. N Engl J Med 313:1450-1456, 1985
20. SPSS Incorporated Staff, Norusis MJ: SPSS-PCplus. Chicago, IL, SPSS Inc, 1985
21. SPSS Incorporated Staff, Norusis MJ: SPSS-PCplus Advanced Statistics. Chicago, IL, SPSS Inc, 1985
22. Nondiscrimination on the basis of a handicap. Federal Register March 48:9630, 1983
a p < .001. b p < .01.
1356 PHYSICAL THERAPY

RESEARCH APPENDIX
Neonatal Neurobehavioral Examination Scoring Sheet
Name
Date of Birth Gestational Age
Date of Exam Chronological Age
Timing of Exam Corrected Age
1 (<32 wk.) 2 (32-36 wk.) 3 (>36 wk.)
STATES 1. Deep sleep, no movement, regular breathing 2. Light sleep, eyes shut, some movement 3. Dozing, eyes opening and closing 4. Awake, eyes open, minimal movement 5. Wide awake, vigorous movement 6. Crying
A (Abnormal)
A. TONE AND MOTOR PATTERNS
POSTURE (Predominant)
ARM RECOIL Infant supine; take arms and extend parallel to the body; hold several secs and release.
SCARF Infant supine. Head in midline. Bring arm across chest until resistance is met.
POPLITEAL ANGLE Infant supine. Approximate knee and thigh to abdomen; extend leg by gentle pressure with index finger behind ankle.
ANKLE DORSIFLEXION Infant supine. Flex foot against shin until resistance is met.
PRONE SUSPENSION Hold infant in ventral suspension; observe curvature of back and relation of head to trunk.
SLIP-THROUGH Hold infant in vertical suspension under axillae. Observe amount of support required to prevent infant from "slipping."
PULL-TO-SIT Pull infant toward sitting posture by traction on both arms.
HEAD RIGHTING Place infant in sitting position; allow head to fall forward; wait 30 sec.
total extension
no flexion within 5 sec.
no resistance
180-135°
limited 60-90°
complete
complete
complete head lag
no attempt to raise head
LE flexed, UE extended
partial flexion at elbow >100° within 4-5 sec.
limited resistance past midline
90-135°
partial 30-60°
partial
partial
partial flexion
unsuccessful attempt to raise head upright
total flexion
arms flex at elbow to <100° within 2-3 sec.
at or before midline
90-60°
complete <30°
near horizontal
none
occasional alignment
occasional alignment
opisthotonus tonic extension
difficult to extend jerky flexion
tonic flexion shoulder retraction
<60°
equinus >90°
tonic extension
shoulder retraction
tonic extension shoulder retraction
head cannot be flexed forward SC
OR
ING
1.
to
tal r
espo
nses
to th
e 9
item
s in
eac
h ar
ea;
A sc
ored
as
1 2.
be
havi
oral
sub
test
sco
red
3, if
2 o
f thr
ee it
ems
are
scor
ed 3
3.
be
havi
oral
sub
test
sco
red
1, if
2 o
f thr
ee it
ems
are
scor
ed 1
4.
be
havi
oral
sub
test
sco
red
2, if
nei
ther
of t
he a
bove
crit
eria
are
met
5.
sc
ore
num
ber o
f abn
orm
al p
atte
rns
A.
Tone
& M
otor
Pat
tern
s A
bnor
mal
Pat
tern
s B.
Pr
imiti
ve R
efle
xes
Abn
orm
al P
atte
rns
C.
Beh
avio
ral R
espo
nses
R
espo
nsiv
enes
s Te
mpe
ram
ent
Equ
ilibra
tion
Volume 68 / Number 9, September 1988 1357

APPENDIX Neonatal Neurobehavioral Examination Scoring Sheet (Continued)
1 (<32 wk.) 2 (32-36 wk.) 3 (>36 wk.) A (Abnormal)
B. PRIMITIVE REFLEXES
ROOT
SUCK
GRASP
POSITIVE SUPPORT
WALKING
CROSSED EXTENSOR
MORO
TONIC NECK
CRY
absent
weak
absent
astasia
no response
no response
no response
no response
absent
C. BEHAVIORAL RESPONSES
mouth opening, partial head turning
inconsistent, irregular
sustained flexion
inconsistent, partial
some effort but not continuous with both legs
withdrawal and flexion
abduction only
legs only
whimpering
full head turning with mouth opening
strong regular sucking in bursts of 5 or more movements
traction
full extension
at least two steps
flexion & extension
abduction & adduction
arms & legs respond
sustained cry
tongue thrust
clenching-tonic bite
thumb adduction
equinus
scissoring
tonic extension
tremor only
obligate
high-pitched
RESPONSIVENESS
ALERTNESS
ORIENTATION to face & voice
DEFENSIVE REACTION to cloth over face
TEMPERAMENT
IRRITABILITY
PEAK OF EXCITEMENT
CUDDLINESS
EQUILIBRATION
SELF-QUIETING
CONSOLABILITY
TREMORS
1
inattentive or brief responsiveness (4 or less)
does not focus or follow stimulus, brief following (4 or less)
no response: nonspecific activity with long latency
1 - flat
no cry
low level of arousal never > state 3
no molding
1
cannot self-quiet
unconsolable
tremors in all states
1 - labile
cries to 6 stimuli
insulated crying in response to stimuli
resists, arches
2
moderately sustained alertness, may use stimulation to come to alert state (5,6)
inconsistent or jerky following horizontal 30° (5,6)
rooting, head turning
2
cries to 4 or 5 stimuli
predominantly state 4, may reach state 5 with stimulation
molds with movement and handling
2
occasional success, no sustained crying
consoles with holding and rocking; consoling not needed
tremors occasionally with aversive stimuli
3
sustained and continuous attentiveness (7-9)
sustained smooth following 60° horizontally and occasionally vertically (7-9)
swipes with arms
3
cries to 1-3 stimuli
predominantly state 5, reaches state 6 with stimulation
molds and nestles spontaneously
3
quiets on two or more occasions
consoles with talking or handling in crib
no tremors or tremors only with crying C
OM
MEN
TS:
1358 PHYSICAL THERAPY