A multi-centre phase 3 cluster randomized controlled trial of a manualized anger management...
28
A multi-centre phase 3 cluster randomized controlled trial of a manualized anger management intervention for people with mild to moderate learning disabilities A randomized controlled trial of anger management
-
Upload
alvin-barrett -
Category
Documents
-
view
221 -
download
2
Transcript of A multi-centre phase 3 cluster randomized controlled trial of a manualized anger management...

A multi-centre phase 3 cluster randomized controlled trial of a manualized anger
management intervention for people with mild to moderate learning disabilities
A randomized controlled trial of anger management

Background
• We used a Cognitive Behavioural Therapy (CBT) approach
• CBT for anger is based on teaching clients to:– Be aware of situations that evoke anger– Be aware of becoming angry– Develop skills to control and manage anger
• Physiology: Relaxation• Behaviour: Distraction, stop & think, walk away, ask for help, humour• Cognition: Cognitive restructuring, problem solving, assertiveness
• There have been 10 small controlled trials in people with intellectual disabilities (treated vs. waiting list), all showing significant, sustained effects on anger– This area of research provides the strongest support for use of CBT in
this population
• This is the first large-scale and methodologically-robust trial of any psychological therapy for people with intellectual disabilities

Limitations of earlier anger management studies Only two studies used randomized allocation to groups, and
one of those was extremely small. In some studies the groups were not well matched. There was some overlap between groups or samples: for
example, in some studies, participants in the control group were later added to the intervention group.
The relatively small size of most studies meant that they involved few centres and few therapists, and where a group format was used, very few groups.
Several studies did not include a long-term follow-up and most of those that did only followed up the intervention group.
One study only used third-party (carer) ratings to assess anger. All other studies included first-person reports from service users, but only three of them included both of these sources of information.
Some of the interventions were manualized; most were not. In those studies where the intervention was manualized, no
assessment of fidelity to the manual was reported.
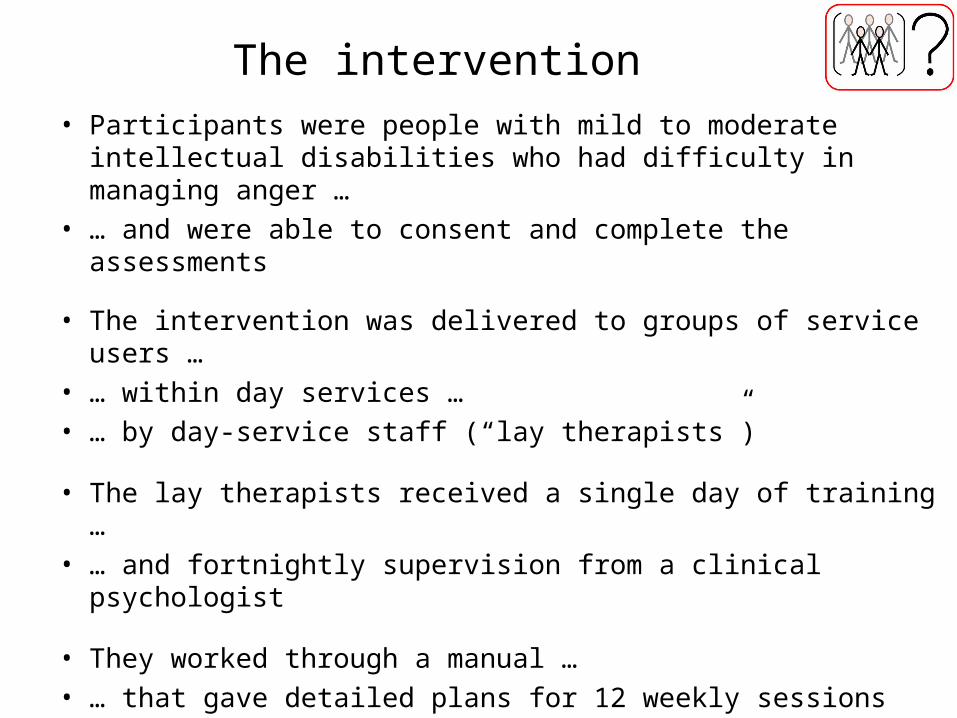
The intervention • Participants were people with mild to moderate intellectual
disabilities who had difficulty in managing anger …• … and were able to consent and complete the assessments
• The intervention was delivered to groups of service users …• … within day services …• … by day-service staff (“lay therapists”)
• The lay therapists received a single day of training …• … and fortnightly supervision from a clinical psychologist
• They worked through a manual …• … that gave detailed plans for 12 weekly sessions
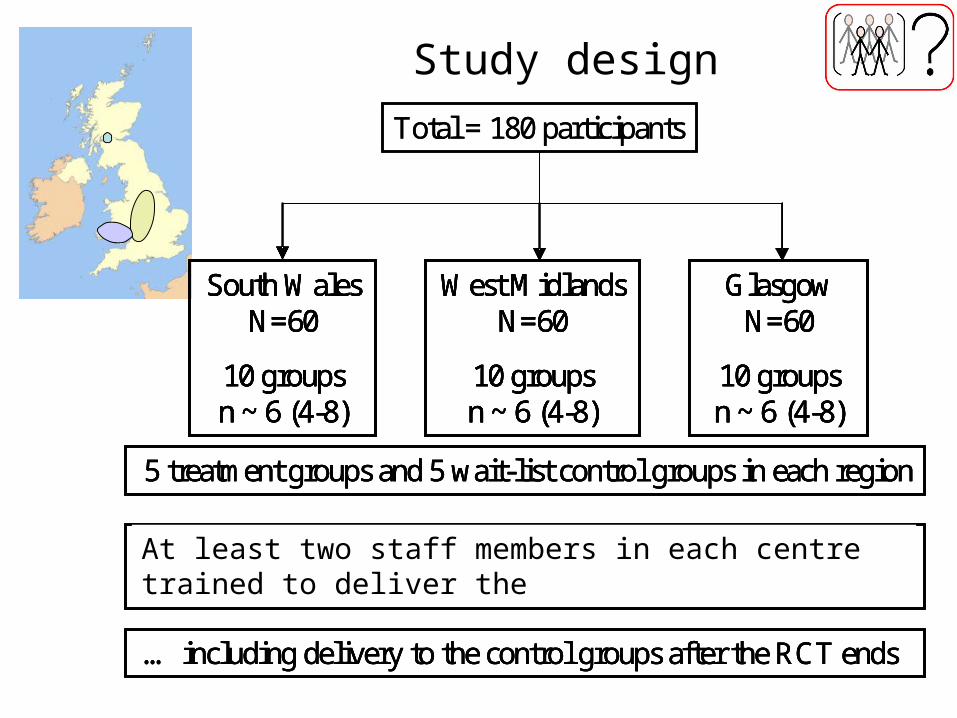
Study design
Total = 180 participants
South Wales N=60
10 groups n ~ 6 (4-8)
West Midlands N=60
10 groups n ~ 6 (4-8)
Glasgow N=60
10 groups n ~ 6 (4-8)
5 treatment groups and 5 wait-list control groups in each region
At least 2 staff members in each region trained to deliver the intervention, supervised by a clinical psychologist …
… including delivery to the control groups after the RCT ends
Total = 180 participants
South Wales N=60
10 groups n ~ 6 (4-8)
West Midlands N=60
10 groups n ~ 6 (4-8)
Glasgow N=60
10 groups n ~ 6 (4-8)
5 treatment groups and 5 wait-list control groups in each region
At least 2 staff members in each region trained to deliver the intervention, supervised by a clinical psychologist …
… including delivery to the control groups after the RCT ends
South Wales N=60
10 groups n ~ 6 (4-8)
West Midlands N=60
10 groups n ~ 6 (4-8)
Glasgow N=60
10 groups n ~ 6 (4-8)
South Wales N=60
10 groups n ~ 6 (4-8)
West Midlands N=60
10 groups n ~ 6 (4-8)
Glasgow N=60
10 groups n ~ 6 (4-8)
5 treatment groups and 5 wait-list control groups in each region
At least 2 staff members in each region trained to deliver the intervention, supervised by a clinical psychologist …
… including delivery to the control groups after the RCT ends
At least two staff members in each centre trained to deliver the

The research team
Operations
• Wales– Paul Willner
• CP: Aimee Stimpson• AP: Christopher Woodgate
• England– John Rose
• CP: Nikki Rose• AP: Jennifer Shead
• Scotland– Andrew Jahoda
• CP: Pamela MacMahon• AP: Claire Lammie
Support
• SE Wales Trials Unit– Kerry Hood
• Project manager (0.5)Julia Townson/Jacqui Nuttall
• Statistician (0.5)David Gillespie
• Qualitative analysis– Biza Stenfert Kroese
• Health economics– David Felce
• Welsh Health Economics Support Service

Service user demographics Age [median (IQR)] 38 (28 – 47) Gender 71% male Full-scale IQ [median (IQR)] 57 (53 – 62) Accommodation
o Family home 41% o Staffed group home
/supported living 38% o Other 21%
Day services attended
o Wales, Scotland: mainly local authority o England: mainly independent residential provider
Clinical level of depression 34% Clinical level of anxiety 75% Severe challenging behaviour 26% Intervention and control groups similar on all measures

Lay therapist characteristics Total trained 82 Mean age 42 Gender 37% male Years working in LD 9.3 Years in current role 5.4 Highest qualification (%)
o No qualification or NVQ/SVQ level 1 11 o NVQ/SVQ level 2 or GCSEs 7 o NVQ/SVQ level 3, highers/A-levels, or HNC 42 o NVQ/SVQ level 4, HND or irrelevant degree 20 o Relevant degree or professional qualification 21
Number with prior training in or experience of CBT 0

• Session 1: Introduction / ‘getting to know you’; group rules
• Session 2: Emotions and physiological aspects of anger
• Session 3: Responses to anger and ‘counting to ten’
• Session 4: ‘What makes us angry’; ‘What happens when we are angry’; ‘Doing something else’; ‘Thinking nice thoughts’
• Session 5: Practicing coping with anger; ‘Walking away’
• Session 6: Recap on previous sessions
• Session 7: ‘Things that make us angry’, and ‘asking for help’ are introduced, using role-plays
• Session 8: Role-plays practiced
• Session 9: ‘Rethinking the situation’
• Session 10: ‘Being assertive’ and role-plays
• Sessions 11 -12: Recap on previous sessions
Programme

• Warm-up exercise
• Recap of previous session
• “Hassle logs” (homework review)
• Role plays based on replay of real events (using knowledge of individual triggers and functional analyses from homework reports)
• Psycho-education
• Relaxation
Typical session structure

Examples of non-verbal materials
What is he doing?How might he feel? How do we know?Why might he feel like this?How could he be calmed down?

Assessments
• Quantitative evaluation – Anger/aggression and mental health/QoL measures at
baseline, post-intervention and 6-month follow up
• Interviews for qualitative analysis– Service users and lay therapists post-intervention– Service managers at baseline and 6-month follow-up
• Health economic evaluation– Costs of the intervention– Services used by both groups in the 3-months preceding
baseline and 6-month follow-up assessments
• Process evaluation– Includes monitoring of fidelity to manual, CBT, group process– Also informed by supervision notes and interview material

Outcomes
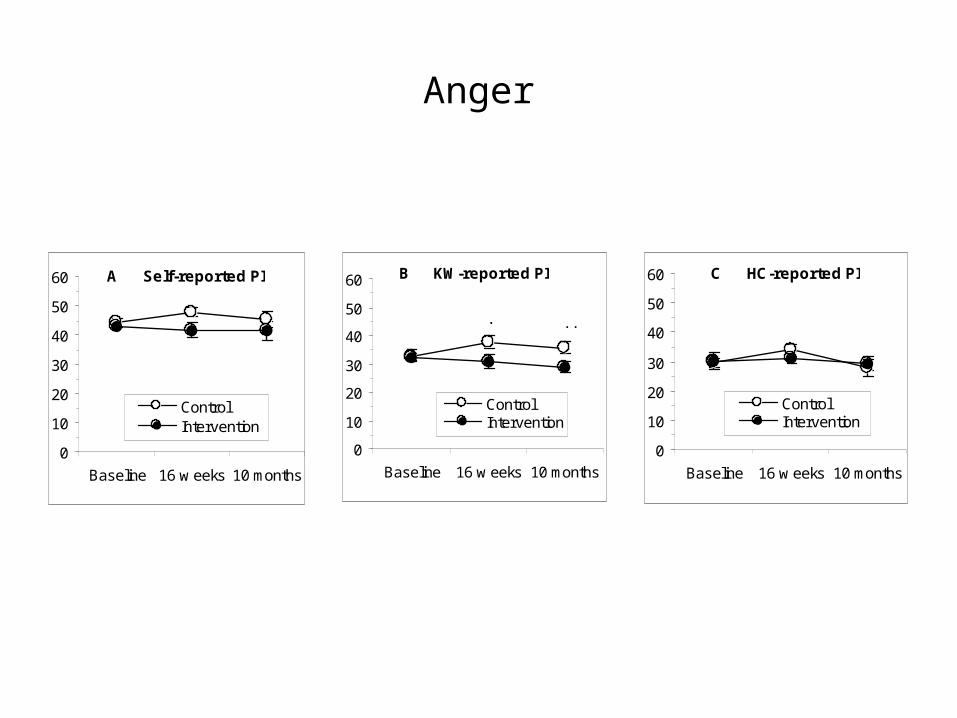
Anger
A Self-reported PI
0
10
20
30
40
50
60
Baseline 16 w eeks 10 months
ControlIntervention
B KW-reported PI
0
10
20
30
40
50
60
Baseline 16 w eeks 10 months
ControlIntervention
***
C HC-reported PI
0
10
20
30
40
50
60
Baseline 16 w eeks 10 months
ControlIntervention

Anger in personally relevant situations
How angry would you feel if X happened (25 general scenarios)
How angry do you do feel when X happens (3 personalized scenarios)
Service users report less anger in relation to strong personal triggers, but do not generalize to hypothetical situations that perhaps they rarely encounter
PI
0
20
40
60
80
100
Baseline 16 w eeks 10 months
% m
axim
um
ControlIntervention
PACS-IPT
0
20
40
60
80
100
Baseline 16 w eeks 10 months
% m
axim
um
ControlIntervention
***

Anger coping
A Self-reported PACS
0
10
20
30
40
50
Baseline 16 w eeks 10 months
ControlIntervention
*****
B KW-reported PACS
0
10
20
30
40
50
Baseline 16 w eeks 10 months
ControlIntervention
*** ***
C HC-reported PACS
0
10
20
30
40
50
Baseline 16 w eeks 10 months
ControlIntervention
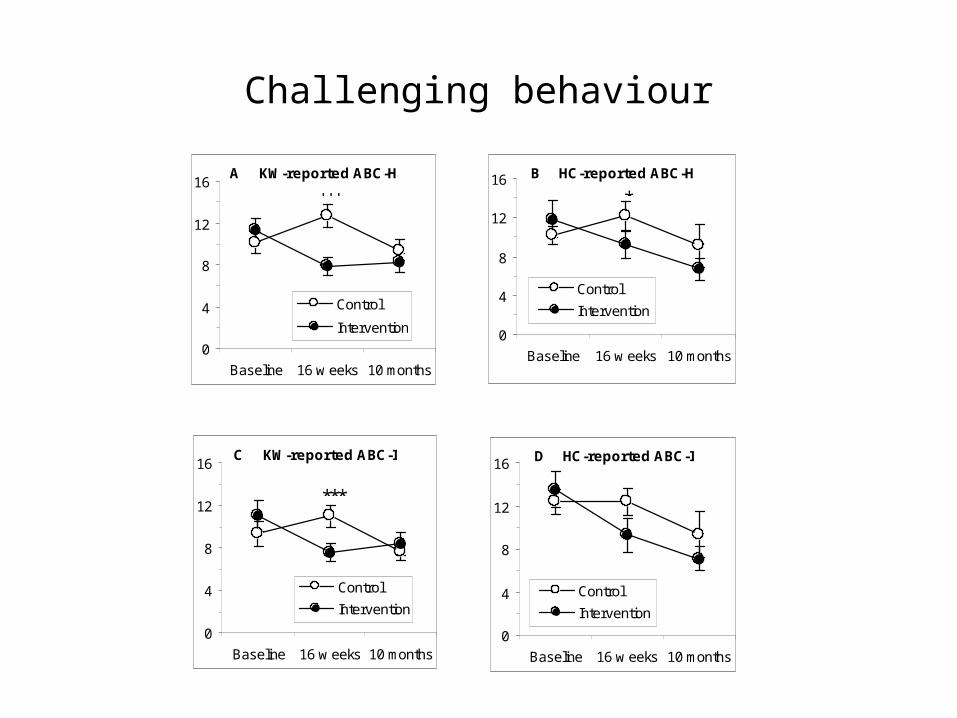
Challenging behaviour
D HC-reported ABC-I
0
4
8
12
16
Baseline 16 w eeks 10 months
Control
Intervention
C KW-reported ABC-I
0
4
8
12
16
Baseline 16 w eeks 10 months
Control
Intervention
***
B HC-reported ABC-H
0
4
8
12
16
Baseline 16 w eeks 10 months
Control
Intervention
*A KW-reported ABC-H
0
4
8
12
16
Baseline 16 w eeks 10 months
Control
Intervention
***

• Why do key-workers report larger changes in service-user’s anger than the service users themselves?
– Service users and carers use different information to rate anger• Service users rate anger according to how they feel• Carers rate anger according to what they see
– The aim was to manage anger better, not to feel less anger– Emphasis on “anger is OK; what matters is how it is expressed”
– Carer reports of decreased anger are linked to the decrease in challenging behaviour
Questions raised by these results 1

• Why are the effects smaller than in previous studies?
Variability between centres
Control groups Intervention groups
Questions raised by these results: 2
-35
-30
-25
-20
-15
-10
-5
0
5
10
15
20
25
30
35
201 302 306 203 310 204 303 102 106 105 211 307 108 109
Diff
eren
ce in
PAC
S sc
ores
(10M
-Ba
selin
e)
Centre
Difference between 10 month follow-up and baseline key worker PACS scores in control group centres
-35
-30
-25
-20
-15
-10
-5
0
5
10
15
20
25
30
35
110 101 209 305 308 207 206 301 205 309 104 107 103 311
Diff
eren
ce in
PAC
S sc
ores
(10M
-Ba
selin
e)
Centre
Difference between 10 month follow-up and baseline key worker PACS scores in intervention group centres

• What do ‘good’ lay therapists do well?
• Lay therapists who were rated as delivering the intervention well were able to create an environment where participants felt comfortable talking about their emotions
Questions raised by these results 3

What service users said about the group
• Most could describe the purpose of the group • They valued the opportunity to talk about their problems
and share experiences• They talked about the coping strategies that they had
learned and used successfully, particularly behavioural strategies such as ‘walking away’ or ‘asking for help’
• They described improved relationships with peers and staff
• They expressed a sense of pride in what they had achieved

What lay therapists said about the group
• They welcomed the opportunity to develop their professional skills
• They believed that the training, the manual and ongoing supervision equipped them well to run the groups
• They felt that they had gained had insights into what made the groups work
• They described some challenges– engaging with service users differently to their normal role
– dealing with emotive issues or disclosures of a sensitive or distressing nature

What service managers said about the group
• Before the group, managers welcomed the opportunity to develop their service and benefit from the staff training on offer
• After the group they were unanimously positive about hosting the intervention and its impact on service users and staff

Costs and consequences
• Cost of delivering the intervention = £24.68 per person per week
• Cost of supporting service users = £22.46 less per person per week in the intervention group relative to the control group
• But the difference is not statistically significant so we cannot be certain that the intervention would recoup its costs

Conclusions• Both service users and key-workers reported decreased anger as a result
of the intervention– Service users’ reports of less anger were in relation to personally-relevant
scenarios, but not to hypothetical situations
– Key-workers reported larger effects
– Service users and key-workers base their ratings on different information (feelings vs. behaviour)
• Key-workers and home carers both reported decreases in challenging behaviour
• Usage of anger coping skills increased as a result of the intervention • Most of the effects were retained at long-term follow-up• The effects observed were smaller than observed in previous studies
where the intervention was delivered by psychologists• Service users, lay therapists and service managers all gave very positive
feedback about the intervention

Overall conclusions
• The intervention was effective in increasing anger coping skills and has an impact on challenging behaviour
• Lay therapists can following a manual to deliver the intervention, after a brief training and with ongoing professional supervision
• People with mild to moderate intellectual disabilities are able to participate in interviews about their therapeutic experiences and also to report on their mental state through appropriately constructed questionnaires
• The study supports the viability of conducting randomized controlled trials of psychological interventions with people with intellectual disabilities
Recommendations for services
• The lay therapist model should be used more widely to increase the availability of psychological interventions to people with intellectual disabilities, with support from a qualified clinical psychologist.
• People with intellectual disabilities referred for problems with anger control should be offered a mental health assessment, and the outcome taken into account in the design of the anger intervention.
• Manualized psychological interventions for other common mental health problems in people with intellectual disabilities should be developed and implemented as a matter of urgency.
• Clinical psychologists should be encouraged to develop consultancy models of working to support other staff to build psychological competency within organisations and to maximise the best use of scarce resources
• Service users should usually be seen as the primary source of information concerning their psychological difficulties, with information from other sources being used to support self report