A MODEL-BASED APPROACH TO LIMB APRAXIA...A Model-Based Approach to Limb Apraxia: Evidence from...
272
A MODEL-BASED APPROACH TO LIMB APRAXIA: EVIDENCE FROM STROKE AND CORTICOBASAL SYNDROME By Vessela Stamenova A thesis submitted in conformity with the requirements for the degree of Doctor of Philosophy Graduate Department of Rehabilitation Science in the University of Toronto © Copyright by Vessela Stamenova 2010
Transcript of A MODEL-BASED APPROACH TO LIMB APRAXIA...A Model-Based Approach to Limb Apraxia: Evidence from...

A MODEL-BASED APPROACH TO LIMB APRAXIA:
EVIDENCE FROM STROKE AND CORTICOBASAL SYNDROME
By
Vessela Stamenova
A thesis submitted in conformity with the requirements
for the degree of Doctor of Philosophy
Graduate Department of Rehabilitation Science
in the University of Toronto
© Copyright by Vessela Stamenova 2010

ii
ABSTRACT
A Model-Based Approach to Limb Apraxia:
Evidence from Stroke and Corticobasal Syndrome
Vessela Stamenova
Doctor of Philosophy
Graduate Department of Rehabilitation Science
University of Toronto, 2010
This thesis provides new insights about how the brain controls skilled movements,
through the study of limb apraxia in two major neurological disorders: Stroke and
Corticobasal Syndrome (CBS). Limb apraxia is a cognitive-motor deficit characterized by
impairment in the performance of skilled movement. The Conceptual-Production systems
model, used as framework in this thesis, proposes that skilled movement is under the control
of three systems: a sensory/perceptual system, a conceptual system and a production system.
Deficits in any of these systems produce limb apraxia, and depending on which system is
affected, a distinct pattern of apraxia emerges. This information processing approach was
used to evaluate performance levels, study brain asymmetries and discern patterns of deficits
in each population. In addition, longitudinal assessments in sample subsets revealed patterns
of recovery after stroke and of progression in CBS.
The first study examined acute-subacute and chronic stroke patients with left (LHD)
and right hemisphere damage (RHD) for their ability to pantomime and imitate transitive and
intransitive gestures. The results indicated that LHD and acute-subacute were more severely
impaired. Concurrent deficits in pantomime and imitation were most common, especially
after LHD. Since acute-subacute patients were more severely impaired, in the absence of any

iii
therapies, it is likely that some degree of recovery occurs over time. The second study study
examined longitudinal recovery in a series of transitive gestures tasks among stroke patients
and indicated that patients significantly recovered in all tasks, except in Action Identification,
a conceptual apraxia task which probes knowledge of actions.
Finally, two comparative studies were conducted in CBS, a neurodegenerative
disorder in which apraxia is common, making this one of the first studies that evaluated
patient performance on a complete limb apraxia battery. The first study found that patients
were often impaired on all gesture production tasks, while conceptual knowledge of gestures
and tools was usually preserved. A case series constituted the second study, which
documented the progression of apraxia in CBS demonstrating that, while deficits in gesture
production usually are present at first examination, deficits in conceptual knowledge are
infrequent and in many cases do not develop at all. Study limitations were discussed and it
was suggested that future research should expand on our findings for recovery in stroke and
progression in CBS.

iv
ACKNOWLEDGEMENTS
I would like to take this opportunity to thank all the people that have lent me a hand
in finishing my thesis.
First, I would like to thank my supervisors, Dr. Sandra Black and Dr. Eric Roy,
without whom my thesis would not have been possible. They both invested as much time as a
single supervisor would have invested and that has given me the opportunity to learn twice as
much. Their feedback has always been unique and I truly benefited from their individual
perspectives. In addition, their generosity in providing me with many opportunities to present
my work at national and international conferences has been tremendous. Finally, I would like
to thank both of them for all the advice they have given me about building my career in
academia. I would also like to thank each one of them individually.
I would like to thank Dr. Sandra Black, who made me part of her lab. I would like to
thank her for the hours she spent revising my thesis word by word and helping me with my
writing, which I hope has made me a better writer. I would also like to thank her for teaching
and guiding me in working with patients. Watching Dr. Black interact with her patients and
observing the true compassion she experiences for them have given me a model that I can
only strive to achieve one day in my clinical research work. Dr. Black is not only a clinician
but also a scientist and her guidance in the research design, methodology and data
interpretation has been extremely helpful.
I would also like to thank Dr. Eric Roy. He has been such a great support for me
throughout my studies. Even though we were at different cities, Dr. Roy has always been
there for me when I needed help. First, I would like to thank him for believing that I have
potential when I first contacted him, for agreeing to be my supervisor and for introducing me
to Dr. Black. His expertise in limb apraxia and his model-based approach to limb apraxia
have helped me shape this thesis. I am truly thankful for his critical feedback on my
theoretical interpretations. I would like to thank him for the hours we have spent together
discussing some of my findings, looking through data analyses and for taking the time to
guide me through my interpretations. He has always been caring and thoughtful and he never
said one time I was wrong, but rather always guided me in discovering myself where I was
wrong.
I would also like to thank Dr William McIlroy for taking the time to be on my
committee and for reviewing my thesis. He always provided me with a different perspective
on things and he would always challenge me in ways that made me think more deeply about
the questions at hand. I was so lucky to have him as part of my program advisory committee
and I truly appreciate all the time he devoted to my thesis work.
I would also like to express my gratitude to Dr. Richard Wolfe, who helped me so
much with my statistical analysis for Chapter 3. Without his guidance, I would not have been
able to complete the analysis for this Chapter.
My thesis would also not been possible without the participation of all the patients
who took part in my studies. They volunteered their time for nothing in return and I am
extremely thankful to them for giving me the opportunity to study how the brain works and
to understand better the disorders that have affected them. I only hope that some of my
findings could advance us even one tiny bit to a better understanding of the control of skilled
movement and to making the lives of other patients affected by the same disorders better.

v
Having two supervisors has also given me an opportunity to be part of two different
labs and this has given me the chance to make friends with people working in a hospital
setting in clinical research, as well as undergraduate and graduate students working at the
University of Waterloo. I would like to thank Naama Levy for being my friend and fellow
graduate student. She was always ready to share her experiences with me and give me advice
about my graduate work. I would like to thank her for encouraging me to keep fighting in my
own struggles to finish my thesis. I would like to thank Mark Gravely for being my fellow
lab mate, working on the apraxia project and for being my link with the lab when I am away.
Also, I would like to thank all research assistants who have worked on the apraxia project
and have collected part of the data I have used in my studies: Kira Barbour, Anish Joshi, Dr.
Quincy Almeida, Dr. Jennifer Salter, Anastasia Arvanitidis and Mark Gravely. I would also
like to express my gratitude to Dr. Mario Massellis for his support in the Corticobasal
Syndrome studies. Dr. Genevieve Desmarais has become a good friend over the last few
years and I am thankful for her help, collaboration in projects and guidance in my work and
my career. I would also like to thank Isabel Lam for her help with databases, Dr. Fuqiang
Gao for training me for some of the neuroimaging work I have been involved in outside my
thesis. Also, special thanks to Loren Kannegiesser and Tatiana Brezden for the administrative
support they have provided over the years.
Of course, I need to express my gratitude to all the funding sources I have been so
lucky to obtain and that have helped me support myself throughout graduate school. My
major scholarship was an industrial scholarship through NSERC, which would not have been
possible without the support from Winston Park Nursing Homes Ltd. I would like to thank
both of them for funding me. In addition, throughout the years, I have received support from
the Toronto Rehabilitation Institute Student Scholarship Fund, the University of Toronto
Fellowship, Ontario Graduate Scholarship in Science and Technology, Margaret & Howard
Gamble Research Grant, and Dr. Jesse Keshin Graduate Student Award.
I would like to thank my parents for being a constant support over the years while I
was working on my thesis. I truly believe that I could not have made it without them. They
have always been there for me, listening to my problems and encouraging me to continue. I
would also like to especially thank my mother, who is not only a mother but also a true
friend, for her constant support, for taking the time to listen to everything I have to say, for
her advice on my career choices and for proofreading some of my written work. I also would
like to mention the support of my sister and her husband, who have always been there to
share both my sadness and joy and to make me laugh and remember that life is not only
about work.
Last, but in no way least, I would like to thank my loving partner Andrew Pothier.
He has been such a tremendous support, going with me through all of the ups and downs I
experienced throughout the last few years of graduate school. Andrew, thank you for your
patience, support, encouragement and love.

vi
TABLE OF CONTENTS
ABSTRACT II
ACKNOWLEDGEMENTS IV
LIST OF TABLES IX
LIST OF FIGURES XI
CHAPTER 1: GENERAL INTRODUCTION 1
INTRODUCTION 1 LIMB APRAXIA-DEFINITIONS & OVERVIEW 1
THE CONCEPTUAL PRODUCTION MODEL OF APRAXIA AND PATTERNS OF DEFICITS 3
ASSESSMENT OF LIMB APRAXIA 8
OTHER GESTURE TYPES 9
LIMB APRAXIA IN STROKE 10 THE NEUROANATOMY OF THE PRAXIS SYSTEM AND ITS RELATIONSHIP TO STROKE 11
PERFORMANCE MODALITY DIFFERENCES IN STROKE: PANTOMIME, IMITATION AND OBJECT
USE 12
GESTURE TYPE DIFFERENCES IN STROKE: TRANSITIVE, INTRANSITIVE AND NON-
REPRESENTATIONAL GESTURES 14
THE CONCEPTUAL PRAXIS SYSTEM IN STROKE 16
LIMB APRAXIA RECOVERY AFTER STROKE 18
STUDY OBJECTIVES IN STROKE 20
LIMB APRAXIA IN CBS 22 THE NEUROANATOMY OF THE PRAXIS SYSTEM AND ITS RELATIONSHIP TO CBD PATHOLOGY 24
PERFORMANCE MODALITY DIFFERENCES IN CBS-PANTOMIME, IMITATION AND OBJECT USE 25
GESTURE TYPE DIFFERENCES IN CBS: TRANSITIVE, INTRANSITIVE AND NON-
REPRESENTATIONAL GESTURES 26
THE CONCEPTUAL PRAXIS SYSTEM AND CBS 27
STUDY OBJECTIVES IN CBS 28
OVERALL OBJECTIVES 30
REFERENCES 31
CHAPTER 2: PERFORMANCE ON PANTOMIME AND IMITATION OF
TRANSITIVE AND INTRANSITIVE GESTURES IN LEFT AND RIGHT
HEMISPHERE STROKE PATIENTS 43
ABSTRACT 43
INTRODUCTION 44
METHODS 46 PARTICIPANTS 46

vii
GESTURAL TASKS AND PERFORMANCE SCORING 49
ANALYSIS 49
RESULTS 50 SAMPLE CHARACTERISTICS 50
GROUP COMPARISONS 50
APRAXIA CLASSIFICATION 53
PATTERNS OF APRAXIA 55
DISCUSSION 56 PATTERNS OF APRAXIA 58
OVERALL CONCLUSION 62
REFERENCES 63
CHAPTER 3: A MODEL-BASED APPROACH TO LONG-TERM RECOVERY OF
LIMB APRAXIA AFTER STROKE 67
ABSTRACT 67
INTRODUCTION 68
METHODS 72 PARTICIPANTS 72
PROCEDURES 73
STATISTICAL ANALYSIS: HIERARCHICAL LINEAR MODELING (HLM) 76
RESULTS 80 ACTION IDENTIFICATION, TOOL NAMING BY ACTION AND TOOL NAMING (TABLE 3.5) 83
PANTOMIME TO VERBAL COMMAND, PANTOMIME BY PICTURE AND OBJECT USE 85
CONCURRENT IMITATION AND DELAYED IMITATION 87
PATTERNS OF DEFICITS ANALYSIS 89
DISCUSSION 94
APPENDIX 3A: INDIVIDUAL PATIENT PERFORMANCES 104
REFERENCES 113
CHAPTER 4: LIMB APRAXIA IN CORTICOBASAL SYNDROME (CBS) 116
ABSTRACT 116
INTRODUCTION 117
METHODS 124 PARTICIPANTS 124
TESTS AND PROCEDURES 127
RESULTS 129 GROUP COMPARISONS 129
CONCEPTUAL LIMB APRAXIA ASSESSMENT TASKS 131
DISCUSSION 149 CONCEPTUAL APRAXIA TASKS 150
APRAXIA GESTURE PRODUCTION TASKS 155
APRAXIA PATTERNS 161
REFERENCES 163

viii
CHAPTER 5: PROGRESSION OF LIMB APRAXIA IN CORTICOBASAL
SYNDROME (CBS): A SERIES OF CASE STUDIES 171
ABSTRACT 171
INTRODUCTION 173
METHODS 176 PARTICIPANTS 176
TESTS AND PROCEDURES 179
ANALYSIS 180
OTHER NEUROPSYCHOLOGICAL ASSESSMENTS 180
NEUROIMAGING REPORTS 181
RESULTS 181 PATIENT SUMMARIES: 181
TASK SUMMARIES: 193
NEUROPSYCHOLOGICAL PERFORMANCE: 197
PATTERN EVOLUTION 198
DISCUSSION 202 LIMB APRAXIA PATTERNS 208
STUDY LIMITATIONS 210
APPENDIX 5A: CASE DESCRIPTIONS. 212
APPENDIX 5B: INDIVIDUAL PERFORMANCES OF PATIENTS ACROSS TIME 219
REFERENCES 228
CHAPTER 6: GENERAL DISCUSSION 234
INTRODUCTION 234
EVIDENCE FROM STROKE 236
EVIDENCE FROM CBS 243
CONVERGING EVIDENCE FROM STUDIES IN LIMB APRAXIA IN STROKE AND
CBS 247
THESIS CONTRIBUTIONS AND CONCLUDING REMARKS 250
REFERENCES 252
APPENDIX A: THE SUNNYBROOK-WATERLOO APRAXIA BATTERY 256
GESTURE TYPES INCLUDED IN THE BATTERY 256
PART 1: CONCEPTUAL COMPONENT OF APRAXIA BATTERY 256 A. TOOL NAMING AND IDENTIFICATION TASKS: 256
B. GESTURE IDENTIFICATION TASKS 257
PART 2: GESTURE PERFORMANCE COMPONENT OF THE APRAXIA BATTERY 259

ix
LIST OF TABLES Page
Table 1.1 The eight patterns of deficits as described by Roy(1996) 7
Table 2.1: Sample Characteristics per patient group 48
Table 1.2. Right vs. Left Hemisphere Mean Percent Accuracy Scores, Z-scores and
standard deviations (SD) on each of the four task modalities 51
Table 2.3: Number of cases and frequency of occurrence in normal, borderline and
apraxia category in each hemisphere and time post-stroke. 54
Table 2.4: Number of cases and frequency of occurrence in normal, borderline and
apraxia category per hemisphere 54
Table 2.5: Patterns of Apraxia for each group in Transitive and Intransitive Gestures 56
Table 3.1: Patterns of Deficits as defined by Roy‟s Model (Roy, 1996) 69
Table 3.2: Means and Standard Deviations of Control Group per task. 74
Table 3.3: Summary of number of patients in each group for each task 75
Table 3.4: Demographic Characteristics of the patients 76
Table 3.5: Estimates of Fixed Effects for Action identification, Tool Naming by Action
and Tool Naming 84
Table 3.6: Estimates of Fixed Effects for Pantomime, Pantomime by Picture and Object
Use. 86
Table 3.7: Estimates of Fixed Effects for Delayed and Concurrent Imitation 88
Table 3.8: Estimated Variance Components (VC) for all tasks 89
Table 3.9: Pattern Evolutions 91
Table 4.1: Demographic Characteristics of each participant group 125
Table 4.2: Clinical Presentation of all patients based on neurological examination 126
Table 4.3: Group Comparisons for each task Modality. Scores are in Percentages. 130
Table 4.4 Correlations between language and conceptual tasks 135
Table 4.5. Case by case description of Impairments in Naming and Conceptual tasks..136
Table 4.6: Demographics of Subsample (n=13) used in task comparisons 138
Table 4.7. Frequencies of deficits among the sample for each task. 145
Table 4.8. Patterns of performance in Transitive Gestures 147
Table 4.9. Patterns of Performance in Intransitive Gestures 148
Table 5.1: Characteristics of the patients 178
Table 5.2. Summary of clinical presentation on initial exam. 178
Table 5.3: Summary of Patterns of apraxia performance for each patient on Transitive
and Intransitive Gestures 201
Table 5B.1: Conceptual Tasks Scores: showing percentage accuracy scores and Z-scores
for each participant across visits 220
Table 5B.2: Pantomime and Object Use Scores: showing percentage accuracy and Z-
scores for each patients across visits 221
Table 5B.3: Delayed Imitation Tasks: Summaries of percentage accuracy scores and Z-
scores per patient for each visit 222
Table 5B.4: Concurrent Imitation Tasks: Showing summaries for each patient across visits
223
Table 5B.5: Initial status and progression per patient for conceptual tasks 224
Table 5B.6: Initial status and progression per patient for Pantomime and Object Use Tasks
225

x
Table 5B.7: Initial status and progression per patient for Delayed Imitation tasks 226
Table 5B.8: Initial status and progression per patient for concurrent imitation tasks 227

xi
LIST OF FIGURES Page
Figure 1.1: The Conceptual Production Model of Apraxia Roy (1996) 3
Figure 2.1: Z-scores in each of the four tasks in each group of participants. 52
Figure 3.1: Model predicted rates of recovery for Action ID, Tool Naming by Action,
Tool Naming and Pantomime 81
Figure 3.2: Model predicted rates of recovery for Pantomime by Picture, Object Use,
Concurrent and Delayed Imitation 82
Figure 3A.1: Individual Patient Performances in Action Identification for each group. The
solid dark line in each graph represents the model- predicted slope for the
group in question 105
Figure 3A.2: Individual Patient Performances in Tool Naming by Action for each group.
106
Figure 3A.3: Individual Patient Performances in Tool Naming for each group. 107
Figure 3A.4: Individual Patient Performances in Pantomime for each group. 108
Figure 3A.5: Individual Patient Performances in Pantomime by Picture for each group. 109
Figure 3A.6: Individual Patient Performances in Object Use for each group 110
Figure 3A.7: Individual Patient Performances in Delayed Imitation for each group 111
Figure 3A.8: Individual Patient Performances in Concurrent Imitation for each group 112
Figure 4.1. Pantomime to Verbal Command, Concurrent and Delayed Imitation in
Transitive and Intransitive Gestures 139
Figure 4.2. Pantomime to Verbal Command, Concurrent Imitation and Imitation with
Verbal Cue in Transitive Gestures 140
Figure 4.3. Concurrent and Delayed Imitation of Transitive, Intransitive and Non-
Representational Gestures 142
Figure 4.4. Pantomime, Pantomime by Picture and Object Use 144
Figure 4.5 Tool Naming by Action and Action ID routes 155

1
CHAPTER 1: GENERAL INTRODUCTION 1
INTRODUCTION
The ability to make skilled, purposeful movements allows us to interact with the
world using tools in everyday activities and communicating with others. We begin our days
by using tools such as a toothbrush and a spoon to eat our breakfast and we often greet or bid
farewell to people we meet throughout the day. It is still not well understood how the brain
organizes and controls purposeful movement but the study of one neurological deficit, limb
arpraxia, has provided neuroscientists with insight into how damage to the brain affects the
control of skilled movements, which ultimately allows one to draw some inferences about
how the healthy brain controls skilled movement.
The overall objective of this thesis is to gain a better understanding of how the brain
controls purposeful skilled movement through examining apraxia. In order to meet this
objective, my goal is to examine the nature of limb apraxia in two neurological disorders,
stroke and Corticobasal Syndrome, which commonly lead to limb apraxia deficits. In the
study of both clinical populations, I have chosen the conceptual-production model of limb
apraxia (Roy, 1996) as a framework to approach this objective.
Limb Apraxia-Definitions & Overview
Limb apraxia is a neurological deficit of skilled movement that does not result from
an inability to understand or follow instructions, sensory impairment, muscle weakness,
1 This chapter contains sections that have been adapted from the following publication:
Stamenova, V, Roy, E , Black, S. (2009) A Model-Based Approach to Understanding Apraxia in
Corticobasal Syndrome. Neuropsychology Review, 19 (1), 47-63.

2
paralysis, incoordination, extrapyramidal motor signs or uncooperativeness (Geschwind,
1975). Testing for limb apraxia is usually accomplished by asking patients to pantomime
(perform gestures from memory to verbal command), imitate gestures that are visually
presented to the patient or use tools. Limb apraxia is also operationally defined as an inability
to pantomime and/or imitate gestures, or use tools (Roy, 1996). The terms “limb apraxia” as
used in this paper encompasses both “ideational apraxia” (usually described in the literature
as a conceptual deficit) and “ideomotor apraxia” (usually described in the literature as a
gesture production deficit), however, given this terminology has been used differently by
various authors and to avoid further confusion, we have chosen to side away from using these
terms and rather concentrate on the pattern of deficits presented by patients.
Attempts to carry out skilled movements in patients with apraxia are usually
characterized by spatial and temporal errors. Patients may perform the wrong sequence of
hand positions; they may incorporate an inappropriate posture (such as making a body part as
object error); they may orient their hands inappropriately; they may coordinate their joints
inappropriately; or execute a movement with the wrong amplitude (Rothi & Heilman, 1997,
Roy, Black, Blair, & Dimeck, 1998).
Hugo Liepman was the first to describe in detail limb apraxia at the beginning of the
20th
century, but the investigation of limb apraxia was largely neglected until the 1970‟s
when Norman Geschwind (1975) sparked new interest in the disorder with his account of
limb apraxia as a disconnection syndrome (Geschwind, 1975). Subsequently most research
on limb apraxia was based on examination of patients with stroke or Alzheimer‟s disease, but
in the past 20 years there has been increasing interest in studying this disorder in patients
suffering from other types of dementia (Ochipa, Rothi, & Heilman, 1992; Joshi, Roy, Black,

3
& Barbour, 2003; Buxbaum, Giovannetti, & Libon, 2000; Jacobs et al., 1999). Various
models have been proposed to explain limb apraxia (Geschwind, 1975; Heilman & Rothi,
1993; Roy, 1996; Cubelli, Marchetti, Boscolo, & Della Sala, 2000; Goldenberg & Hagmann,
1997) and while these models have their distinct features, one common feature originally
defined by Roy & Square (1985) is that two separate systems are proposed for the control of
movement: a conceptual system, which stores our knowledge of tools and gestures, and a
production system responsible for the execution of movement.
The Conceptual Production Model of Apraxia and Patterns of Deficits
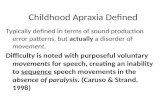
A particularly theoretically driven, information-processing approach has been
developed by Roy (1996), who proposes a conceptual-production model to explain the
deficits observed in apraxic patients (see Figure 1.1).
Figure 1.1: The Conceptual Production Model of Apraxia Roy (1996)
The Conceptual production Model suggests that skilled movement is under the control of three systems
(sensory/perceptual, conceptual and production)
Sensory/
Perceptual System
Production
System
Visual/Gestural
Info
Auditory/Verbal
Info
Visual Tool/Object
Info
Response Selection
Knowledge of
Tool/Object Function
Image Generation
Working Memory
Response
Organization/Control
Knowledge of
Action
Delayed Imitation
Route
Concurrent
Imitation Route
Pantomime
Conceptual System
Sensory/
Perceptual System
Production
System
Visual/Gestural
Info
Auditory/Verbal
Info
Visual Tool/Object
Info
Response Selection
Knowledge of
Tool/Object Function
Image Generation
Working Memory
Response
Organization/Control
Knowledge of
Action
Delayed Imitation
Route
Concurrent
Imitation Route
Pantomime
Conceptual System

4
According to the model the performance of skilled movements involves the operation
of three systems: a sensory/perceptual system, a conceptual and a production system. The
sensory/perceptual system processes information from the environment, which can be visual,
auditory or tactile information. The conceptual system stores our knowledge about tools and
actions. The production system is involved in deciding what the appropriate action is based
on the information available from the environment and in organizing a response by
transforming that information into a code that the motor system can use to control the
movement. Apraxia can arise from disruptions of any of those systems or a combination of
them. In order to be able to assess thoroughly the three systems and to be able to determine
the specific patterns of praxis deficit in a particular patient, a comprehensive assessment
examining all three systems needs to be administered. While various researchers have studied
apraxia, Roy is the first one to suggest that it is not only important to compare how limb
apraxia patients differ in their performance of various task modalities and gesture types, but
also to describe the pattern of deficits that a patient presents with (Roy, 1996).
Roy (1996) described eight patterns of praxis deficits (see Table 1.1) that, based on
the model, can be predicted to arise from disruptions of the three systems. In order to
determine the pattern of deficits the patient presents with, one needs to assess how the patient
performs on four tasks involving transitive gestures: pantomime, concurrent imitation,
delayed imitation and a task that would assess the conceptual system.
First, Roy (1996) suggests that disruptions to the sensory perceptual system may give
rise to a deficit that presents itself in an inability to imitative gestures (both concurrently and
with a delay) and an inability to recognize gestures (Pattern 1). The ability to perform
gestures on pantomime would be preserved however, because the patient would be able to

5
access the conceptual system and use his/her memory of tools and gestures to perform the
gesture correctly. The second pattern of deficits can arise from disruptions to the conceptual
system (Pattern 2). If the conceptual system is impaired the patient should be unable to
pantomime, because he would not have access to his/her knowledge of tools and gestures.
The patient would also not be able to recognize gestures, because they would have no
meaning for him/her; however, the patient would be still able to perform gestures on
imitation, because in the imitation task one does not need to know what the examiner is
demonstrating in order to be able to perform the gesture correctly. This form of apraxia has
previously been referred to as „conceptual apraxia‟ (Heilman, Maher, Greenwald, & Rothi,
1997).
According to Roy‟s model the production system consists of several processes:
response selection, image generation, working memory encoding and retrieval, and gesture
response organization and control. There are five types of gesture deficit patterns that can
result from disruptions of the various stages of the production system. First, a patient may
present with a selective impairment in pantomime with preserved ability to imitate and to
recognize gestures (Pattern 3). The preserved ability to recognize gestures in this case
indicates that the patient‟s gesture and tool knowledge is intact, however, the problem lies in
an inability to translate this knowledge into a movement. Roy suggests that this would mean
that the patient is unable to select the appropriate response. This pattern of performance has
been referred to in the past as ideomotor apraxia (Heilman, 1973).
Second, a selective impairment on imitation tasks with preserved ability to
pantomime and recognize gestures would suggest a disruption in the later stages of the
production system (Pattern 4). If a patient is unable to imitate one might be inclined to

6
conclude that the patient is unable to process visual information, however the preserved
ability to recognize tools and gestures speaks to the contrary. Therefore, such a pattern of
apraxia performance must result only from a disconnection between the centers processing
the visual/gestural information and the centers responsible for gesture production. For these
reasons, this form of apraxia has been termed conduction apraxia by some authors (Ochipa,
Rothi, & Heilman, 1994).
In Roy‟s model one of the sub-components of the production system is working
memory. Therefore, the third and fourth production system deficit patterns result from
impairments in working memory. First, a working memory encoding dysfunction would
produce a selective impairment in delayed imitation, with preservation of concurrent
imitation, pantomime and gesture recognition (Pattern 5). However, if there is an overall
working memory dysfunction, there should be impairment not only in delayed imitation, but
also in pantomime (Pattern 6). According to Roy‟s model the images generated in the early
stages of the production system (in pantomime) and those encoded from the analysis of
visual gestural information in the examiner‟s demonstration (in delayed imitation) are both
retained in working memory. Therefore, impairment of working memory would produce
deficits in both these tasks. Thus, the second type of working memory impairment would
give rise to a pattern where the patient cannot perform on pantomime and delayed imitation,
but the ability to perform gestures to concurrent imitation and to recognize gestures is spared.
The fifth production system deficit pattern results from disruptions in the final stages
of the production system (Pattern 7). At the final stages of the production system, there is a
process responsible for the response organization and control of movements. If this final
process were disrupted, the patient would not be able to pantomime or imitate, however the

7
ability to recognize gestures should be spared, because the knowledge of tools and objects, or
the conceptual system would be spared. This pattern of deficit has been referred to in the past
by the term ideomotor apraxia (Heilman, Rothi, & Valenstein, 1982).
The eighth pattern of deficit resulting from a multi-system disruption would result in
an impaired performance on all four tasks (Pattern 8). This pattern of praxis performance
should result in cases where both the production and the conceptual system are impaired and
possibly the sensory perceptual system might be impaired as well. This would most likely be
present in patients who have a more extensive damage to the cerebral cortex. Patients with
multi system disruptions would not be able to perform well on any of the four tasks.
Table 1.1 The eight patterns of deficits as described by Roy (1996).
Pattern Apraxia Performance Pattern
System
Affected Nature of Disruption
1
"Sensory/perceptual
(P+/DI-/CI-/ID-)"
Sensory/
Perceptual
Impaired ability to analyze visual
gestural and tool/object
information
2
"Conceptual
(P-/DI+/CI+/ID-)" Conceptual
Impaired knowledge of action and
tool/object function
3
"Production Response Selection
(P-/DI+/CI+/ID+)" Production
Impaired response selection
and/or image generation
4
"Production Encoding
(P+/DI-/CI+/ID+)" Production
Impaired encoding of visual
gestural information into working
memory
5
"Production Working Memory
(P-/DI-/CI+/ID+)" Production Impaired working memory
6
"Production Conduction
(P+/DI-/CI-/ID+)" Production
Impaired ability to use visual
information in the control of
movement
7
"Production Ideomotor
(P-/DI-/CI-/ID+)" Production
Impaired response organization
and control
8
"Global
(P-/DI-/CI-/ID-)"
Production +
Conceptual
Impaired knowledge of action and
tool/object function + Impaired
response organization and
control. P=Pantomime, DI= Delayed Imitation, CI=Concurrent Imitation, ID=Gesture Identification
(-) indicates impaired performance and (+) indicates normal performance.

8
Assessment of Limb Apraxia
In order to determine the specific pattern of praxis deficits, a thorough assessment of
gestural performance in various testing modalities is necessary, including pantomime,
imitation and object use. In pantomime, patients are asked to follow a verbal command, such
as: “Show me how you would use a hammer to pound a nail.” To successfully pantomime
gestures, the subject needs to know what the particular tool in question looks like, what
action is associated with it and how to transform this perception-action knowledge into an
actual movement. In the imitation condition, the examiner demonstrates a gesture to the
patient who is then required to imitate the gesture after the demonstration is complete
(delayed imitation) or while the examiner is demonstrating the gesture (concurrent imitation).
In the imitation condition, there are two routes that the patient can use to successfully
complete the task: (1) an indirect route, where the patient might recognize the gesture being
presented by retrieving the actual representation of the gesture and further transform this
representation into a motor innervatory pattern to perform the appropriate gesture, much like
it is done in the pantomime condition, or (2) a direct route, where the patient may use only
visual information to successfully complete the task (Tessari, Canessa, Ukmar, & Rumiati,
2007; Heilman et al., 1993; Roy, 1996). This route may be taken in cases where the patient
does not recognize a meaningful gesture that is presented, or when the patient recognizes the
gesture but still chooses to use this route. The direct route is always used in imitation of
nonrepresentational gestures. Finally, in the object (or tool) use condition, patients are given
the actual tools and asked to pretend they are using the tool. This condition is the most
closely related condition to real-life use of objects and therefore it is important to be included

9
to have a better understanding of the possible impact apraxia may have on performance of
daily activities.
Besides various input modalities for gesture production, no assessment of apraxia is
complete without the inclusion of tasks assessing the conceptual praxis system, such as
gesture identification and recognition tasks. For example, one could present several gestures
to patients and ask them to identify the gestures being presented. If a language disorder is
suspected and the patient has problems with gesture naming, one could ask the patient to
match a gesture with a tool (presented in a picture or as the actual tool).
Other Gesture Types
Aside from various testing modalities, it is also important to include various gesture
types. There are two main gesture categories: representational and nonrepresentational
gestures. Representational gestures are meaningful and there are two types: (1) transitive
gestures involve the use of tools, such as using a hammer to pound a nail; (2) intransitive
gestures do not involve tools but carry some symbolic meaning, such as waving goodbye.
Nonrepresentational gestures are meaningless, novel gestures and as such are useful for the
examination of pure production deficits, because they have no associated action
representations. Any apraxia assessment should have gestures that represent all three gesture
types: transitive, intransitive and non-representational gestures. While, Roy‟s model is
designed to address mainly deficits in transitive gestures, because it addresses mainly object
related tasks, it can easily be adapted to other gesture types. Assessment of all gesture types
is important because it has been suggested that the three gesture types are subserved by
different neuroanatomical brain networks (Leiguarda, 2005; Buxbaum, Kyle, Grossman, &
Coslett, 2007) and, therefore, they can be differentially affected by distinct brain pathology.

10
In addition, the different task modalities (pantomime, imitation, object use and
gesture recognition) are also subserved by different neuroanatomical brain networks.
According to the model of Roy (1996) when a patient is unable to perform a particular task,
there could be more than one reason why this was the case. For example, if a patient is
unable to pantomime, it could be either because the representation of the gesture has
degraded or because the patient is unable to select or produce the appropriate gesture.
Therefore, it is necessary to administer a combination of tasks to determine at what stage of
information processing the impairment lies. For example, in this case, including a gesture
identification task would allow the examiner to determine whether the patients‟ conceptual
knowledge is preserved and if so to infer that the patient‟s inability on pantomime was likely
due from a production deficit.
In my thesis work, all data is part of a large limb-apraxia battery, called The
Waterloo-Sunnybrook Limb Apraxia Battery. This battery contains a comprehensive
examination of three gesture types: transitive, intransitive and non-representational. In
addition, the battery contains several tasks assessing the conceptual knowledge of transitive
gestures (tool and action knowledge), as well as gesture production tasks (including
pantomime for transitive and intransitive gestures and concurrent and delayed imitation for
all three gesture types). A detailed description of the entire battery and its psychometric
characteristics is included in Appendix A.
Limb Apraxia in Stroke
While limb apraxia was first described by Liepmann in the context of a patient
suffering from syphilis, it was the study of focal neurological disorders, such as stroke, that
led Liepmann to conclude that the left hemisphere plays a dominant role in the control of

11
praxis movements (Goldenberg, 2003). The study of limb apraxia has ever since been
dominated by research in stroke patients.
The Neuroanatomy of the Praxis System and its relationship to stroke
Liepmann observed that all of his patients who presented with limb apraxia had
suffered from left hemisphere damage (LHD), whereas none with right hemisphere damaged
(RHD) patients demonstrated apraxia (Liepmann, 1988). Hence, he proposed that the motor
representations of actions were stored in the left hemisphere in right-handed individuals and
that the left hemisphere controlled gesture performance in both hands. Geschwind (1975)
later proposed a neural pathway that underlies praxis abilities that was analogous to the
language processing pathway and was previously proposed to explain gesture production in
response to verbal command. More recent studies have shown that gesture production
involves a network of structures, each subserving different stages of production. Two parieto-
frontal networks work in coordination in the control of gesture production and object use:
one for reaching (involving the superior parietal lobule and connecting to the dorsal premotor
cortex) and another involved in the other for grasping and manipulating of objects (involving
the intraparietal area and the inferior parietal lobule (IPL) and projecting to the ventral
premotor cortex) (Geyer & Zilles, 2005).Disruption in these two networks together with
impaired generation and control of independent finger movements due to disruptions of
intracortical inhibitory circuits, and a disruption of the somatosensory processing have been
suggested as the primary sources of limb-kinetic apraxia (Leiguarda et al., 2003).
In addition, the dorsal visual stream, or the so called “how” stream, is responsible for
visually-guided movements (Milner & Goodale, 2008). The dorsal stream consists of several
parallel parietofrontal networks that have been identified in primates (Mountcastle, Lynch,

12
Georgopoulos, Sakata, & Acuna, 1975) and in humans (Goodale & Milner, 2006) to be
involved in visual and somatosensory transformation for reaching, eye movements toward a
target, moving target pursuit, as well as grasping and manipulation of objects. All of these
parallel networks need to be intact in order to successfully perform a skilled movement. Once
information is passed from the parietal cortex to the frontal lobes, the dorsolateral prefrontal
regions and the supplementary motor area (SMA) contain the innervatory information
necessary for motor execution (Watson, Fleet, Gonzalez-Rothi, & Heilman, 1986; Roy,
1996). Crudely speaking, damage to frontal areas will produce motor production errors,
whereas damage to the left parietal lobe will produce gesture recognition and conceptual
errors, as well as production errors which are “downstream”. Given that the dorsal stream is
bilateral, it would equally affect left and right hemisphere patients. It is primarily the left IPL,
however, that contains the motor representations necessary for gesture production (Rothi,
Mack, & Heilman, 1986; Geschwind, 1975; Roy, 1996). Therefore, damage to the left
hemisphere would produce deficits affecting more the conceptual knowledge of tools and
actions. Buxbaum and colleagues suggest that there are two types of apraxia based on these
two anatomical networks: representational and dynamic (Buxbaum, 2001). Representational
apraxia arises from damage to the left IPL, while dynamic apraxia arises from damage to the
dorsal stream.
Performance Modality Differences in Stroke: Pantomime, Imitation and Object Use
Performance modality differences in stroke have been studied quite extensively.
While stroke patients often show impairments in both pantomime and imitation, the two
performance modalities have been shown to dissociate. There have been reports of patients
impaired only on pantomime and not imitation, as well as patients impaired on imitation but

13
not pantomime in both performance of transitive and intransitive gestures (Heath, Roy,
Black, & Westwood, 2001; Ochipa et al., 1994; Derenzi, Faglioni, & Sorgato, 1982; Roy et
al., 1998; Westwood et al., 2001). Studies of Roy and colleagues show that such selective
deficits, in either pantomime alone or imitation alone, can arise from damage to either
hemisphere, while deficits in both pantomime and imitation concurrently are more likely
after LHD. This stresses the importance of describing the actual pattern of deficits patients
present with. For example, studies comparing the performance of LHD vs. RHD on
pantomime and imitation tasks have consistently found that LHD patients are more severely
affected in their ability to perform either task modality (Kimura & Archibald, 1974; Hanna-
Pladdy et al., 2001; Haaland, Harrington, & Knight, 2000). Therefore, unless one examines
the actual pattern of limb apraxia performance on a case by case basis isolating deficits in
one or other modality or both, one may underestimate the role of the right hemisphere in the
control of praxis movements. Selective deficit in pantomime reflects a deficit in conceptual
gesture knowledge, rather than a deficit at the production stage, because imitation is spared.
Selective deficit in imitation, on the other hand, reflects possibly deficits in visual processing
or transformation of visual info into movement. Impairment in both pantomime and
imitation, however, reflects a deficit in the final stages of movement control. Therefore, Roy
et al.‟s findings suggest that both hemispheres may be equally involved in the conceptual
system and in the control of visuomotor transformations, while the left hemisphere is
dominant in the control of the final stages of the production system. (Roy et al., 1998; Heath,
Roy, Westwood, & Black, 2001). Their findings have yet to be replicated in either a different
group of stroke patients or by another group of researchers.

14
Finally, it should be noted that when both pantomime and imitation are affected,
generally, pantomime performance is usually more severely affected than imitation
(Schnider, Hanlon, Alexander, & Benson, 1997; Alexander, Baker, Naeser, Kaplan &
Palumbo, 1992; Roy et al., 2000; Heath et al., 2001).
In regard to object (or tool) use performance of stroke patients, it has been shown
quite consistently that patients improve in their performance when holding the actual tool
(Clark et al., 1994). There have been reports of cases being unable to pantomime, but able to
use objects (Graham, Zeman, Young, Patterson, & Hodges, 1999), but there has also been
cases where patients were impaired in object use, while pantomime and imitation
performance were more accurate (Motomura & Yamadori, 1994; Heath, Almeida, Roy,
Black, & Westwood, 2003). For example, Heath et al. (2003) reported on a right parietal
stroke patient, who was selectively impaired in object use (pretending to use objects when
holding them), and this deficit remained throughout the acute and chronic stages of stroke
recovery.
Gesture Type Differences in Stroke: Transitive, Intransitive and Non-Representational
Gestures
In stroke, performance of transitive gestures is often affected to a greater extent than
performance of intransitive gestures (Haaland & Flaherty, 1984; Schnider et al., 1997;
Haaland et al., 2000; Gonzalez-Rothi, Mack, Verfaellie, Brown, & Heilman, 1988). Cases of
stroke patients impaired on transitive but not intransitive gestures have been reported
(Dumont, Ska, & Schiavetto, 1999; Rapcsak, Ochipa, Beeson, & Rubens, 1993). In addition,
certain authors have suggested that the left hemisphere may control transitive gestures while
both hemispheres may be involved in intransitive gestures (Haaland et al., 1984; Buxbaum et

15
al., 2007; Rapcsak et al., 1993; Mozaz, Rothi, Anderson, Crucian, & Heilman, 2002).
Therefore, it is important to study both gesture types, because they may be subserved by
different networks (Bartolo, Cubelli, Della Sala, Drei, & Marchetti, 2001). Another reason
why the two gesture types can be affected differently by stroke is that intransitive gestures
are communicative gestures that are pantomimed more naturally in a testing situation, while
transitive gestures involve performing out of the natural context where patients must pretend
to use the tools and objects. As such, they must imagine the tool and object they are asked to
use and imagine how they would interact to complete the gesture.
Non-representational gestures are often used to examine the ability of stroke patients
to imitate gestures that carry no meaning and thus cannot be supported by the conceptual
system, storing representations of learned gestures. Therefore, imitation of non-
representational gestures can only be done through the direct route to imitation using direct
visuomotor transformations. Imitation of non-representational gestures is often affected in
stroke, but to a lesser extent when compared to transitive gestures (Kimura et al., 1974;
Haaland et al., 2000). Double dissociations between impairments of imitation of meaningful
versus imitation of meaningless gestures have been also reported after left hemisphere stroke
(Bartolo et al., 2001; Goldenberg et al., 1997). Impairment in imitation of meaningless
gestures, together with preserved ability to imitate meaningful gestures in cases of stroke
patients (Haaland et al., 1984) can easily be explained by suggesting that patients have
deficits in the direct route to imitation. Cases of patients with deficits in imitation of
meaningful gestures, but not meaningless gestures are harder to explain, given patients
should be able to use the direct route to imitate meaningful gestures in much the same way
they do in the imitation of non-representational gestures. The fact that these patients remain

16
impaired in the imitation of meaningful gestures, suggests that there is something preventing
them from using the direct route in the imitation of meaningful gestures. In addition,
imitation of non-representational gestures seems to occur after damage to either hemisphere
(Ferro, Martins, Mariano, & Caldas, 1983; Rapcsak et al., 1993; Halsband et al., 2001;
Bartolo et al., 2001), but one study suggests that imitation of finger postures may be more
affected after RHD, while imitation of hand postures may be more affected after LHD
(Goldenberg & Strauss, 2002).
Overall, the study of limb apraxia in stroke examining hemisphere effects on the
performance of the three major gesture types could benefit from further examination. While,
the role of the left hemisphere in the control of transitive gestures is relatively better
established, the role of each hemisphere in the control of intransitive gestures and non-
representational gestures needs further study.
The Conceptual Praxis System in Stroke
The conceptual system which enables one to recognize gestures and tools can often
be preserved in some cases of patients with deficits in pantomime and imitation (Heilman et
al., 1982; Halsband et al., 2001; Kimura et al., 1974), even though other studies have
suggested a relationship between imitation and pantomime recognition (Buxbaum, Kyle, &
Menon, 2005; Pazzaglia, Smania, Corato, & Aglioti, 2008). Heilman et al. (1982) suggested
that there are two forms of ideomotor apraxia: one form affects both the ability to pantomime
and imitate gestures, as well as the ability to identify gestures (i.e. affecting the conceptual
knowledge of gestures), the other form of apraxia affects only the ability to pantomime and
imitate gestures. Heilman et al. also suggested that damage to the left IPL causes deficits in
conceptual knowledge of gestures, while more anterior lesions affect the ability to

17
pantomime and imitate gestures by disconnecting the IPL from the areas of the brain
involved in motor programming.
Over 20 years later, we know that the network subserving gesture recognition is more
complex, involving frontal, parietal and temporal networks, but the IPL still remains one of
the major brain locations subserving gesture recognition. This has been supported by
neuroimaging studies showing involvement of the IPL in gesture discrimination (Villarreal et
al., 2008; Bonda, Petrides, Ostry, & Evans, 1996), as well as other studies in stroke reporting
deficits in conceptual knowledge of gestures and tools after damage to the left IPL cortex
(Rothi et al., 1986). Only one recent study examining gesture error identification in patients
with limb apraxia reported no relationship with IPL (Pazzaglia et al., 2008). Future studies
should examine if these findings can be replicated. Pazzaglia et al.‟s different findings may
be due to the fact that they asked participants to discriminate between gesture errors, while
the studies of Villareal et al. and Bonda et al. asked participants to simply observe gesture
actions. Therefore, the lack of activation in the IPL in the study of Villareal et al. may be due
to the fact that participants were detecting errors, rather than simply observing gestures.
Rothi et al. (1986) in their lesion examination of the role of IPL, also asked patients to
identify gesture errors and the patients inability to recognize the errors led them to conclude
that these patients have lost their conceptual knowledge of actions. It is equally possible,
however, that deficits in gesture error identification in this case, may have been due to an
inability to process the gesture rather than an inability to identify the error. Future studies
should attempt to differentiate between the two tasks.
Finally, deficits in the ability to recognize gestures on visual presentation with spared
ability to pantomime have been coined the term “pantomime agnosia” and have been

18
reported after damage to the occipital lobe (Rothi et al., 1986). Activation in the occipital
lobe during observation of meaningful transitive actions has also been reported in some
neuroimaging studies (Grezes & Costes, 1998).
Limb Apraxia Recovery after stroke
Even though apraxia is common in the stroke population, few studies have
investigated its pattern of recovery after stroke. Only five studies in English were found that
focus on spontaneous recovery of apraxia. First, Basso, Capitani, Della Sala, Laiacona, &
Spinnler (1987) examined the natural course of apraxia recovery in acute LHD and bilateral
stroke patient at acute stages (15-30 days) and then at 8 months post stroke. The apraxia
assessment consisted of a 24-item of meaningful and meaningless gestures that the patient
had to imitate (De Renzi, Motti, & Nichelli, 1980). The mean scores of the apraxia patients
improved significantly by the second examination; in fact, 50 % of the patients had recovered
to normal scores on the second examination. Most patients improved, but the patients who
were still apraxic at the second examination were reexamined a third time (at 16 months post
onset) and while some improvement was observed, the difference was not significant. It is
important to point out that the apraxia test included only imitation tasks and therefore the
semantic and memory dependent aspects of praxis as seen in pantomime were not examined.
In another study of long-term recovery, Basso, Burgio, Paulin, & Prandoni (2000)
used again the 24-item gesture imitation test designed by De Renzi et al. (1980) to assess the
patients. Only LHD patients were included and they were examined three times, at a mean of
1.6, 9.4 and 27.9 months after the stroke. The results showed that there was a significant
difference between the patients‟ scores on the first and second examination, but not between
the second and third examination. In accordance with other studies examining cognitive

19
recovery (Skilbeck, Wade, Hewer, & Wood, 1983) this study supported the concept that most
recovery of apraxia likely occurs within the first three months post stroke.
Foundas, Raymer, Maher, Gonzalez-Rothi, & Heilman (1993) examined recovery in
ideomotor apraxia at 6 weeks, 3 and 6 months in left-hemisphere stroke patients. They also
found that the greatest praxis recovery occurred within the first three months post stroke. The
also showed that moderately apraxic patients have the greatest potential for recovery.
Mimura, Fitzpatrick, & Albert (1996) examined 15 LHD stroke patients on
pantomime and imitation of transitive, intransitive and buccofacial gestures at 4.5 months
and 81.6 months post stroke. They showed that improvement was significant for both
pantomime and imitation.
Finally, in an abstract, Cimino-Knight et al. (2002) examined 12 patients within 6
weeks post onset and then again within 3-6 months post onset. Patients were examined on
pantomime to verbal command and gesture recognition. The authors demonstrated that the
patients‟ performance on the pantomime at first examination correlated with the patients‟
performance on the second examination, but that was not the case for gesture recognition
tasks. The authors concluded that two tasks evolved differently during recovery, which
strengthened their hypothesis that the two tasks involve different mechanisms.
All of the studies suffer from two methodological problems. First, they do not assess
patients comprehensively enough and therefore, we have evidence of recovery for only a few
task modalities. Second, they do not describe the various patterns of praxis deficits and how
these patterns evolve. Finally, none of the studies included right hemisphere stroke patients.
Given limb apraxia has been reported after both LHD and RHD stroke, it is important that
both stroke subpopulations be included in recovery studies. Given that certain apraxia

20
patterns seem to be more common after left as opposed to right hemisphere stroke (as
reported by Roy et al. (2000) and Heath et al. (2001), it is also possible that the recovery
processes may vary between the two hemispheres.
Study Objectives in Stroke
Based on the review of the literature on limb apraxia in stroke to date, together with
the overall goal of studying how the brain organizes movement, my thesis has the following
objectives with regard to examining the effects of stroke on praxis. First, given that the two
studies by Roy and colleagues (Roy et al, 2000 and Heath et al. 2001) were the first to report
that selective deficits in pantomime or imitation are equally common after damage to either
hemisphere, and that only deficits in both pantomime and imitation are more frequent after
LHD, the first study aims to replicate their findings in a new sample of stroke patients. This
study also seeks to expand their findings in the following ways: First, I will examine
concurrently transitive and intransitive gestures, which would allow me to compare directly
the performance of patients on the two gesture types. My hypothesis is that transitive
gestures will be more impaired than intransitive gestures. Second, because performance on
both gesture types will be compared within the same stroke population, which would include
both LHD and RHD patients, I will be able to directly examine brain asymmetries in each of
the two gesture types, which was not done in previous studies. Based on predictions
regarding patterns of apraxia from Roy‟s previous studies, I predict that LHD patients will be
more severely impaired than RHD patients and that transitive gestures will be more severely
affected after LHD stroke. Third, I set out to determine on a cross-sectional basis whether
patients recover from stroke. This will be done by comparing the performance of acute-
subacute and chronic patients in their pantomime and imitation of transitive and intransitive

21
gestures. The hypothesis is that chronic patients should be less severely affected by limb
apraxia than acute-subacute patients, because chronic patients would have had a chance to
recover from their initial deficits. This approach, which can only indirectly infer recovery,
however, is limited by the cross-sectional design, including the inability to determine if other
confounding variables that may affect performance are equally distributed between the two
populations. Therefore, the objective of the second study in my thesis is to examine recovery
of limb apraxia after stroke through a longitudinal study design. This study will address
previous limitations of limb apraxia recovery studies by including both LHD and RHD
patients, as well as by administering a comprehensive battery of assessments, including both
conceptual and gesture production tasks. Generally, it is expected that stroke patients will
recover in both gesture production and conceptual knowledge tasks. In addition, this study is
the first to attempt to describe how deficit patterns of limb apraxia deficits evolve post stroke
using the comprehensive approach. No studies to date have examined this, so it is difficult to
make any specific predictions. However, it is expected that if recovery of limb apraxia occurs
patients should move from patterns of impairment to patterns of no impairment. If little or no
recovery is observed, patients should remain within the same patterns over time. If only
certain systems recover, however, or they recover at significantly different rates, then
patients are expected to change their patterns, by improving only on certain pattern defining
tasks. For example, if patients recover only in conceptual tasks, we would expect them to
move from a pattern of global impairment where all patterns are impaired, to a pattern of
common impairment in pantomime and imitation, but no impairment in the knowledge of
gestures and tools.

22
Limb Apraxia in CBS
Another disorder, where limb apraxis is quite commonly observed is CBS, a
neurodegenerative process characterized by an asymmetric presentation and course. Average
age at disease onset is 63 years (±7.7) and the average duration of the disease is 7.9 (±2.6)
years (Wenning et al., 1998).
Based on the clinical diagnostic criteria summarized by Boeve, Lang, & Litvan,
(2003), the following CBS diagnostic criteria have been established: 1) Insidious onset and
progressive course of disease; 2) No identifiable cause (e.g., tumor, infarct); 3) Cortical
dysfunction as reflected by at least one of the following: focal or asymmetrical ideomotor
apraxia, alien limb phenomenon, cortical sensory loss, visual or sensory hemineglect,
constructional apraxia, focal or asymmetric myoclonus or apraxia of speech/nonfluent
aphasia, 4) Extrapyramidal dysfunction as reflected by at least one of the following: focal or
asymmetrical appendicular rigidity lacking prominent and sustained L-dopa response or focal
or asymmetrical appendicular dystonia. Boeve et al. (2003) specify the following supportive
features: 1) variable degrees of focal or lateralized cognitive dysfunction, with relative
preservation of learning and memory, on neuropsychometric testing, 2) focal or asymmetric
atrophy on computed tomography or magnetic resonance imaging, typically maximal in
parietofrontal cortex or 3) focal or asymmetric hypoperfusion on single-photon emission
computed tomography and positron emission tomography, typically maximal in
parietofrontal cortex, basal ganglia and/or thalamus. Other features that may be observed are
bradykinesia and tremor, dysarthria, postural imbalance and oculomotor problems, such as
hypometric saccades, difficulty initiating voluntary saccades (occulomotor apraxia),

23
increased saccadic latency and occasional supranuclear gaze palsy (Mendez & Cummings,
2006).
While initially it was considered that dementia symptoms are not common in the
disease, more recent studies have shown that the motor manifestation of the disease may
follow cognitive decline, and cases have been reported where the initial symptoms were
aphasia, apraxia, executive or visuospatial dysfunction (Kertesz, Martinez-Lage, Davidson,
& Munoz, 2000; Grimes, Lang, & Bergeron, 1999). In fact, several cases have been
described where patients suffering from Progressive Non-Fluent Aphasia were established to
have CBD as underlying pathology (Mimura et al., 2001; Kertesz, Davidson, & Munoz,
1999; Ioannides, Karacostas, Hatzipantazi, & Milonas, 2005).
While numerous studies have examined the characteristics of apraxia in stroke,
studies analyzing patterns of apraxic deficits in CBS are relatively scarce. This likely arises
for several reasons. First, although CBS has been recognized for almost forty years the
clinical diagnostic criteria were not completely delineated until just over a decade ago (Lang,
Riley, & Bergeron, 1994). Second, CBS is rare, comprising only about 1% of clinically
diagnosed patients with parkinsonism, and this number is probably an overestimation, given
that it is based on numbers reported from a movement disorders clinic where the likelihood
of referral of patients with atypical movement disorders is higher. Also, given that the
sensitivity of clinical diagnosis has been shown to be about 35% (Litvan et al., 1997), one
could expect that the maximum prevalence would be about 2-3% of the parkinsonian
patients. These numbers, however, relate only to cases with clear motor presentation. Recent
evidence suggests that certain cases of CBS may lack the commonly associated parkinsonism
(Grimes et al., 1999). The third reason is that limb apraxia is a neglected cognitive behavioral

24
sign, rarely looked for even in dementia clinics. Unfortunately, while some standardized
assessments of limb apraxia exist and have been used in research studies, most tests lack the
psychometric development available for other psychological assessment instruments and
have not made their way into clinical practice. This has made apraxia less likely to be
detected, unless a clinician is specifically interested in the phenomenon. The lack of readily
available assessment tools makes it difficult to study limb apraxia comprehensively and it is
problematic to compare findings across different studies due to differences in the praxis
assessments. Despite these problems in identifying patterns of apraxia in CBS the prevalence
of limb apraxia in CBS is relatively high. Estimates are between 70 to 80% of CBS cases
present with some degree of apraxia (Zadikoff & Lang, 2005; Leiguarda, Lees, Merello,
Starkstein, & Marsden, 1994). Given CBS is associated with frontal and parietal atrophy and
basal ganglia degeneration and that these regions have been associated with apraxia in stroke,
it is no surprise that the prevalence of limb apraxia would be so high in CBS.
The Neuroanatomy of the Praxis System and its relationship to CBD pathology
Frontoparietal degeneration is a hallmark finding in CBS, both by structural and
functional neuroimaging studies (Ukmar et al., 2003; Brooks, 2000), and by pathological
examination (Dickson et al., 2002). While the damage is usually greater in one hemisphere,
both sides of the brain are eventually affected by the neurodegeneration. Therefore, CBS
patients are mainly affected in the dorsal stream of visuomotor processing.
Besides degeneration in the cortex, subcortical degeneration may also contribute to
apraxia in CBS. Studies in stroke have shown some evidence that lesions to in the basal
ganglia could lead to apraxia. In a review, Pramstaller and colleagues (1996) showed that
while lesions of the thalamus sometimes have caused apraxia even if there was no apparent

25
involvement of white matter, most cases of apraxia as a result of a subcortical stroke have
involved additional capsular and periventricular or peristriatal white matter damage. Other
studies have also demonstrated the importance of white matter tracts in mediating praxis
functions. A study conducted by Roy and colleagues (1998) showed that the areas of
commonest overlap in stroke patients presenting with apraxia were the white matter tracts
deep to the parietal cortex. Also, accumulation of tau has been previously reported in the
white matter tracts deep to the affected cortical areas in CBD which may further contribute to
praxis deficits (Mackenzie, 2005). In addition, studies examining apraxia in other
neurodegenerative disorders affecting the basal ganglia, such as Parkinson‟s disease,
Progressive Supranuclear palsy and Huntington‟s disease, have occasionally reported apraxia
deficits (Goldenberg, Wimmer, Auff, & Schnaberth, 1986; Leiguarda et al., 2000).
Performance Modality Differences in CBS-Pantomime, Imitation and Object Use
In order to assess whether there is a specific pattern of deficits in CBS, it is important
to determine whether patients with CBS are impaired on pantomime or imitation tasks or
both. The differences in performance between those two modalities in CBS patients are not
as clear cut as they are in stroke patients. One study conducted by Leiguarda showed that,
while both pantomime and imitation were impaired, a sample of five CBS patients performed
better on imitation than pantomime (Leiguarda, 2001). Another study with a larger sample
(N=13), showed that imitation was better but only with the non-dominant hand (Pharr et al.,
2001). However, the study did not specify which hand was affected more by CBS and,
therefore, it is not clear whether hand dominance or the side most affected by the disease
played a role . The evidence showing imitation to be worse in CBS is somewhat more
convincing. Peigneux and colleagues (2001) showed that imitation was more impaired than

26
pantomime irrespective of the gesture type in 18 patients with CBS. Two other studies, with
smaller sample sizes provide further evidence that imitation is more impaired than
pantomime in CBS (Jacobs et al., 1999; Spatt, Bak, Bozeat, Patterson, & Hodges, 2002).
Other studies fail to provide information on both pantomime and imitation tasks and
therefore do not elucidate this issue (Monza et al., 2003; Leiguarda et al., 1994; Salter, Roy,
Black, Joshi, & Almeida, 2004).
Few studies have compared the use of objects to pantomime performance in CBS
patients. One study conducted a kinematic analysis of the movements of patients while they
used objects and showed that CBS patients showed deficits in joint coordination and the
spatiotemporal aspects of the movement (Merians et al., 1999). Leiguarda et al. (2000)
performed a similar study, examining four patients, and showed disruptions of spatial
accuracy, spatiotemporal decoupling and deficits in interjoint coordination in patients with
CBS. In addition, with the exception of the case presented by Merians et al. (1999) that
showed no improvement with object use, most studies comparing pantomime and the use of
actual objects have shown that CBS patients improve when using actual tools (Jacobs et al.,
1999; Graham et al., 1999; Spatt et al., 2002; Leiguarda et al., 2003).
Gesture Type Differences in CBS: Transitive, Intransitive and Non-Representational
Gestures
Besides differences in test modalities, it is also important to determine how the
performance is affected in different gesture types. Differences in performance between
transitive and intransitive gestures are somewhat contradictory. Some studies have suggested
that patients are equally impaired on both types of gestures (Leiguarda et al., 2003; Jacobs et
al., 1999; Peigneux et al., 2001; Buxbaum et al., 2007), while others have found more

27
impairments on transitive than intransitive gestures (Pharr et al., 2001; Salter et al., 2004;
Chainay & Humphreys, 2003).
In regard to differences between meaningful and meaningless gestures, several
studies have found no clear differences in CBS (Merians et al., 1999; Spatt et al., 2002; Salter
et al., 2004; Leiguarda et al., 2003; Buxbaum et al., 2007), with the exception of one case
study which showed non-representational gestures to be better performed than
representational gestures (Chainay et al., 2003). Most of the data suggest that CBS patients
are not able to benefit from the lexical support afforded by the semantic content associated
with meaningful gestures. This in turn suggests that the motor production centers may be
entirely disconnected from areas of visual processing, as well as areas of semantic
knowledge. The fact that CBS patients perform worse on imitation, together with the finding
that CBS patients are equally impaired in their performance of both representational and non-
representational gestures further suggests that CBS patients not only have trouble producing
gestures through the non-representational (direct) route but also through the representational
(indirect) route of action. According to Buxbaum et al. (2007), CBS patients should be less
impaired on meaningful gestures since their IPL‟s would not be as affected. Her study,
however, did not confirm this prediction and the existing literature also shows no differences
in performance between meaningful and meaningless gestures in CBS. Therefore, it is likely
that both routes of imitation are affected in CBS.
The Conceptual Praxis System and CBS
Unfortunately, as is the case with many studies in stroke patients, most studies
examining apraxia in CBS patients have failed to include such tasks and, thus, it is not
possible to determine whether the impairment is due to conceptual or production deficits. The

28
studies that have included gesture identification and recognition tasks, however, have shown
quite consistently that most patients with CBS do not have impairment in their conceptual
knowledge of actions (Leiguarda et al., 1994; Jacobs et al., 1999; Soliveri, Piacentini, &
Girotti, 2005).
Conceptual knowledge of gestures is thought to be represented in the left IPL in the
human brain (Heilman et al., 1982).Given that CBS patients do not show any conceptual
impairment, it should be the case that the IPL in CBS patients is relatively spared by
pathology. In fact, Dickson and colleagues (2002) (Dickson et al., 2002) report that it is the
superior as opposed to the inferior parietal cortex that is mainly affected by CBD pathology.
Studies examining apraxia in stroke often include patients who have suffered left middle
cerebral artery stroke (MCA), which more commonly affects the inferior parietal cortex more
than the superior parietal cortex, and thus would be more likely to produce conceptual
deficits.
Study Objectives in CBS
In conclusion, the literature has suggested that patients have an intact conceptual
system, but an impaired production system. Performance on intransitive gestures indicates
that if impaired at all, most CBS patients do not have problems pantomiming but they are
impaired on imitation. Patients with selective impairment in imitation have deficits in the
ability to transform visual gestural information into a movement. Finally, the literature has
suggested that imitation of both non-representational and representational gestures is equally
impaired. Together with evidence of impairment in pantomime of transitive gestures,
suggests that patients have problems with both the direct and indirect route of action
imitation. According to Roy‟s model this would suggest a deficit in the final stages of action

29
production (i.e. response organization and control). All of the above findings, however, are
based on a systematic review of the entire literature, rather than on a detailed comparison of
the performance of the same sample of patients on various limb apraxia tasks. There are no
group studies to date that have assessed comprehensively the performance of CBS patients
on a variety of limb apraxia tasks. In addition, no studies to date have studied the frequency
of limb apraxia patterns in CBS. Finally, no studies to date have examined the progression of
limb apraxia in CBS over time with most of the studies being conducted on patients that were
at an average of 3 years after disease onset. While this may help make the results between the
studies more comparable, cross-sectional studies provide little information about the
performance of CBS patients over time and at more advanced stages of the disease. Given
that the average disease duration is close to 8 years, we need more longitudinal studies to
understand progression patterns and gain insight into praxis abilities of CBS patients at later
stages.
My next two thesis studies, then, aim to address all of the above gaps in the literature
on limb apraxia in CBS. First, my goal is to administer a comprehensive battery of
assessments, including a variety of task modalities (pantomime, delayed and concurrent
imitation and object use) and all three gesture types (transitive, intransitive and non-
representational) in the same group of CBS patients. Based on the summarized literature, my
hypothesis is that patients will be equally impaired on pantomime and imitation, but will
have preserved conceptual knowledge of tools and gestures. Second, given the role of the left
hemisphere in the control of movement from studies in stroke, especially in transitive
gestures, and the fact that no studies to date have compared the performance of CBS patients
with a predominantly left (LHP) or right hemisphere presentation (RHP), I aim to examine

30
differences between these two CBS groups. My hypothesis is that LHP patients will be more
severely impaired than RHP patients. Third, I aim to describe the patterns of limb apraxia in
a relatively large sample of CBS patients and I expect to see a pattern of deficits with
impaired pantomime and imitation performance in transitive gestures and possibly selective
impairment in imitation in intransitive gestures. All of these predictions will be addressed in
the third study of my thesis.
Finally, in my fourth thesis study, I aim to describe the progression of limb apraxia in
CBS through a case series, each of whom will undergo again the same comprehensive limb
apraxia assessment as the one administered to the larger sample of patients. It is expected that
patients will deteriorate in gesture production performance, but it is intriguing to examine if
conceptual knowledge of tools and gestures will eventually deteriorate as well.
Overall Objectives
As described in the introduction, the overall objective of my thesis is to gain a better
understanding of how the brain controls purposeful skilled movement through the study of
limb apraxia in two clinical populations. My approach to the study of limb apraxia in both
populations, stroke and CBS, has four common subobjectives. First, I aim to examine task
modality and gesture type differences in the overall performance of patients in each of the
two disease groups. Second, I aim to examine hemispheric asymmetries in the control of
skilled movement. Third, I aim to describe the patterns of limb apraxia deficits in each of the
two clinical populations. Fourth, my aim is to examine how limb apraxia changes over time
by examining recovery in stroke and progression of deficits in CBS. Specific hypotheses for
each of these objectives will be given in the context of each study.

31
REFERENCES
Alexander, M. P., Baker, E., Naeser, M. A., Kaplan, E., & Palumbo, C. (1992).
Neuropsychological and Neuroanatomical Dimensions of Ideomotor Apraxia. Brain, 115, 87-
107.
Bartolo, A., Cubelli, R., Della Sala, S., Drei, S., & Marchetti, C. (2001). Double
dissociation between meaningful and meaningless gesture reproduction in apraxia. Cortex,
37, 696-699.
Basso, A., Burgio, F., Paulin, M., & Prandoni, P. (2000). Long-Term Follow-up of
Ideomotor apraxia. Neuropsychological Rehabilitation, 10, 1-13.
Basso, A., Capitani, E., Della Sala, S., Laiacona, M., & Spinnler, H. (1987). Recovery
from ideomotor apraxia. A study on acute stroke patients. Brain, 110, 747-760.
Boeve, B. F., Lang, A. E., & Litvan, I. (2003). Corticobasal degeneration and its
relationship to progressive supranuclear palsy and frontotemporal dementia. Annals of
Neurology., 54, S15-S19.
Bonda, E., Petrides, M., Ostry, D., & Evans, A. (1996). Specific involvement of
human parietal systems and the amygdala in the perception of biological motion. Journal of
Neuroscience, 16, 3737-3744.
Brooks, D. J. (2000). Functional Imaging Studies in Corticobasal Degeneration. In
I.Litvan, C. Goetz, & A. Lang (Eds.), Corticobasal Degeneration and Related Disorders (
Philadelphia, PA: Lippincott Williams & Wilkins.

32
Buxbaum, L. J. (2001). Ideomotor apraxia: a call to action. Neurocase, 7, 445-458.
Buxbaum, L. J., Giovannetti, T., & Libon, D. (2000). The role of the dynamic body
schema in praxis: evidence from primary progressive apraxia. Brain & Cognition, 44, 166-
191.
Buxbaum, L. J., Kyle, K., Grossman, M., & Coslett, H. B. (2007). Left inferior
parietal representations for skilled hand-object interactions: Evidence from stroke and
corticobasal degeneration. Cortex, 43, 411-423.
Buxbaum, L. J., Kyle, K. M., & Menon, R. (2005). On beyond mirror neurons:
internal representations subserving imitation and recognition of skilled object-related actions
in humans. Cognitive Brain Research, 25, 226-239.
Chainay, H. & Humphreys, G. W. (2003). Ideomotor and ideational apraxia in
corticobasal degeneration: A case study. Neurocase., 9, 177-186.
Cimino-Knight, A. M., Hollingsworth, A. L., Maher, L. M., Raymer, A. M., Foundas,
A. L., Heilman, K. M. et al. (2002). Forms of recovery in ideomotor apraxia: a preliminary
investigation. Journal of the International Neuropsychological Society, 8, 207.
Clark, M. A., Merians, A. S., Kothari, A., Poizner, H., Macauley, B., Gonzalez, R. L.
J. et al. (1994). Spatial planning deficits in limb apraxia. Brain, 117, 1093-1106.
Cubelli, R., Marchetti, C., Boscolo, C., & Della Sala, S. (2000). Cognition in action:
Testing a model of limb apraxia. Brain and cognition, 44, 144-165.

33
De Renzi, E., Motti, F., & Nichelli, P. (1980). Imitating gestures. A quantitative
approach to ideomotor apraxia. Archives of Neurology, 37, 6-10.
Derenzi, E., Faglioni, P., & Sorgato, P. (1982). Modality-Specific and Supramodal
Mechanisms of Apraxia. Brain, 105, 301-312.
Dickson, D. W., Bergeron, C., Chin, S. S., Duyckaerts, C., Horoupian, D., Ikeda, K.
et al. (2002). Office of Rare Diseases neuropathologic criteria for corticobasal degeneration.
Journal of Neuropathology & Experimental Neurology.61(11):935-46.
Dumont, C., Ska, B., & Schiavetto, A. (1999). Selective impairment of transitive
gestures: An unusual case of apraxia. Neurocase, 5, 447-458.
Ferro, J. M., Martins, I. P., Mariano, G., & Caldas, A. C. (1983). CT scan correlates
of gesture recognition. Journal of Neurology, Neurosurgery & Psychiatry, 46, 943-952.
Foundas, A. L., Raymer, A. M., Maher, L. M., Gonzalez-Rothi, L., & Heilman, K. M.
(1993). Recovery in Ideomotor Apraxia. Journal of Clinical Experimental Neuropsychology,
14, 44.
Geschwind, N. (1975). The Apraxias: Neural Mechanisms of Disorders of Learned
Movements. American Scientist, 63, 188-195.
Geyer, S. & Zilles, K. (2005). Functional Neuroanatomy of the Human Motor Cortex.
In H.J.Freund, M. Jeannerod, M. Hallett, & R. Leiguarda (Eds.), Higher-Order Motor
Disorders (pp. 3-22). Oxford: Oxford University Press.

34
Goldenberg, G. (2003). Apraxia and beyond: life and work of Hugo Liepmann.
Cortex, 39, 509-524.
Goldenberg, G. & Hagmann, S. (1997). The meaning of meaningless gestures: a
study of visuo-imitative apraxia. Neuropsychologia, 35, 333-341.
Goldenberg, G. & Strauss, S. (2002). Hemisphere asymmetries for imitation of novel
gestures. Neurology, 59, 893-897.
Goldenberg, G., Wimmer, A., Auff, E., & Schnaberth, G. (1986). Impairment of
motor planning in patients with Parkinson's disease: evidence from ideomotor apraxia
testing. Journal of Neurology, Neurosurgery & Psychiatry, 49, 1266-1272.
Gonzalez-Rothi, L., Mack, L., Verfaellie, M., Brown, P., & Heilman, K. M. (1988).
Ideomotor Apraxia: Error Pattern Analysis. Aphasiology, 2, 381-387.
Goodale, M. & Milner, D. (2006). One brain - two visual systems. Psychologist, 19,
660-663.
Graham, N. L., Zeman, A., Young, A. W., Patterson, K., & Hodges, J. R. (1999).
Dyspraxia in a patient with corticobasal degeneration: the role of visual and tactile inputs to
action. Journal of Neurology Neurosurgery and Psychiatry, 67, 334-344.
Grezes, J. & Costes, N. (1998). Top-down effect of strategy on the perception of
human biological motion: A PET investigation. Cognitive Neuropsychology, 15, 553-582.
Grimes, D. A., Lang, A. E., & Bergeron, C. B. (1999). Dementia as the most common
presentation of cortical-basal ganglionic degeneration. Neurology., 53, 1969-1974.

35
Haaland, K. Y. & Flaherty, D. (1984). The different types of limb apraxia errors made
by patients with elft vs. right hemispehre damage. Brain and cognition, 3, 370-384.
Haaland, K. Y., Harrington, D. L., & Knight, R. T. (2000). Neural representations of
skilled movement. Brain, 123, 2306-2313.
Halsband, U., Schmitt, J., Weyers, M., Binkofski, F., Grutzner, G., & Freund, H. J.
(2001). Recognition and imitation of pantomimed motor acts after unilateral parietal and
premotor lesions: a perspective on apraxia. Neuropsychologia, 39, 200-216.
Hanna-Pladdy, B., Daniels, S. K., Fieselman, M. A., Thompson, K., Vasterling, J. J.,
Heilman, K. M. et al. (2001). Praxis lateralization: errors in right and left hemisphere stroke.
Cortex, 37, 219-230.
Heath, M., Almeida, Q. J., Roy, E. A., Black, S. E., & Westwood, D. (2003).
Selective dysfunction of tool-use: a failure to integrate somatosensation and action.
Neurocase, 9, 156-163.
Heath, M., Roy, E. A., Black, S. E., & Westwood, D. A. (2001). Intransitive limb
gestures and apraxia following unilateral stroke. Journal of clinical and experimental
neuropsychology, 23, 628-642.
Heath, M., Roy, E. A., Westwood, D., & Black, S. E. (2001). Patterns of apraxia
associated with the production of intransitive limb gestures following left and right
hemisphere stroke. Brain & Cognition, 46, 165-169.
Heilman, K. M. (1973). Ideational apraxia--a re-definition. Brain, 96, 861-864.

36
Heilman, K. M., Maher, L. M., Greenwald, M. L., & Rothi, L. J. (1997). Conceptual
apraxia from lateralized lesions. Neurology, 49, 457-464.
Heilman, K. M. & Rothi, L. J. (1993). Apraxia. In Clinical Neuropsychology (pp.
141-163). New York, NY: Oxford University press Inc.
Heilman, K. M., Rothi, L. J., & Valenstein, E. (1982). Two forms of ideomotor
apraxia. Neurology, 32, 342.
Ioannides, P., Karacostas, D., Hatzipantazi, M., & Milonas, I. (2005). Primary
progressive aphasia as the initial manifestation of corticobasal degeneration. A 'three in one'
syndrome? Functional Neurology, 20, 135-137.
Jacobs, D. H., Adair, J. C., Macauley, B., Gold, M., Gonzalez, R. L. J., & Heilman,
K. M. (1999). Apraxia in corticobasal degeneration. Brain & Cognition, 40, 336-354.
Joshi, A., Roy, E. A., Black, S. E., & Barbour, K. (2003). Patterns of limb apraxia in
primary progressive aphasia. Brain & Cognition, 53, 403-407.
Kertesz, A., Davidson, W., & Munoz, D. G. (1999). Clinical and pathological overlap
between frontotemporal dementia, primary progressive aphasia and corticobasal
degeneration: the Pick complex. [Review] [33 refs]. Dementia & Geriatric Cognitive
Disorders., 10, 46-49.
Kertesz, A., Martinez-Lage, P., Davidson, W., & Munoz, D. G. (2000). The
corticobasal degeneration syndrome overlaps progressive aphasia and frontotemporal
dementia. Neurology., 55, 1368-1375.

37
Kimura, D. & Archibald, Y. (1974). Motor functions of the left hemisphere. Brain,
97, 337-350.
Lang, A., Riley, D. E., & Bergeron, C. (1994). Cortical-Basal Ganglionic
Degeneration. In D.B.Calne (Ed.), Neurodegenerative Diseases (pp. 877-894). Philadelphia:
W.B.Saunders.
Leiguarda, R. (2001). Limb apraxia: cortical or subcortical. NeuroImage, 14, S137-
S141.
Leiguarda, R. (2005). Apraxias as Traditionally Defined. In H.Freund, M. Jeannerod,
M. Hallett, & R. Leiguarda (Eds.), Higher-order motor disorders (1st ed., pp. 303-338).
Oxford: Oxford University Press.
Leiguarda, R., Lees, A. J., Merello, M., Starkstein, S., & Marsden, C. D. (1994). The
nature of apraxia in corticobasal degeneration. Journal of Neurology, Neurosurgery &
Psychiatry, 57, 455-459.
Leiguarda, R., Merello, M., Balej, J., Starkstein, S., Nogues, M., & Marsden, C. D.
(2000). Disruption of spatial organization and interjoint coordination in Parkinson's disease,
progressive supranuclear palsy, and multiple system atrophy. Movement Disorders, 15, 627-
640.
Leiguarda, R. C., Merello, M., Nouzeilles, M. I., Balej, J., Rivero, A., & Nogues, M.
(2003). Limb-kinetic apraxia in corticobasal degeneration: Clinical and kinematic features.
Movement Disorders, 18, 49-59.

38
Liepmann, H. (1988). Apraxia. In J.W.Brown (Ed.), Agnosia and Apraxia: Selected
papers of Liepmann, Lange and Pötzl (1st Ed. ed., pp. 3-42). Hillsdale, New Jersey:
Lawrence Erlbaum Associates, Publishers.
Litvan, I., Agid, Y., Goetz, C., Jankovic, J., Wenning, G. K., Brandel, J. P. et al.
(1997). Accuracy of the clinical diagnosis of corticobasal degeneration: A clinicopathologic
study. Neurology., 48, 119-125.
Mackenzie, I. R. A. (2005). Neuropathology of Atypical parkinsonian Disorders. In
I.Litvan (Ed.), Atypical parkinsonian Disorders. Clinical and Research Aspects (pp. 33-63).
Totowa, NJ: Humana Press.
Mendez, M. F. & Cummings, J. L. (2006). Frontotemporal Dementia and the
Asymmetric Cortical Atrophies. In Dementia: A Clinical Approach (3rd ed., pp. 256-260).
Butterworth-Heinemann.
Merians, A. S., Clark, M., Poizner, H., Jacobs, D. H., Adair, J. C., Macauley, B. et al.
(1999). Apraxia differs in corticobasal degeneration and left-parietal stroke: A case study.
Brain & Cognition, 40, 314-335.
Milner, A. D. & Goodale, M. A. (2008). Two visual systems re-viewed.
Neuropsychologia, 46, 774-785.
Mimura, M., Oda, T., Tsuchiya, K., Kato, M., Ikeda, K., Hori, K. et al. (2001).
Corticobasal degeneration presenting with nonfluent primary progressive aphasia: A
clinicopathological study. Journal of the Neurological Sciences.Vol.183(1)()(pp 19-26),
2001.Date of Publication: 15 JAN 2001., 19-26.

39
Mimura, M., Fitzpatrick, P. M., & Albert, M. E. (1996). Long-term recovery from
ideomotor apraxia. Neuropsychiatry, neuropsychology, and behavioral neurology, 9, 127-
132.
Monza, D., Ciano, C., Scaioli, V., Soliveri, P., Carella, F., Avanzini, G. et al. (2003).
Neurophysiological features in relation to clinical signs in clinically diagnosed corticobasal
degeneration. Neurological Sciences., 24, 16-23.
Motomura, N. & Yamadori, A. (1994). A Case of Ideational Apraxia with
Impairment of Object Use and Preservation of Object. Cortex, 30, 167-170.
Mountcastle, V. B., Lynch, J. C., Georgopoulos, A., Sakata, H., & Acuna, C. (1975).
Posterior Parietal Association Cortex of Monkey - Command Functions for Operations
Within Extrapersonal Space. Journal of neurophysiology, 38, 871-908.
Mozaz, M., Rothi, L. J., Anderson, J. M., Crucian, G. P., & Heilman, K. M. (2002).
Postural knowledge of transitive pantomimes and intransitive gestures. Journal of the
International Neuropsychological Society, 8, 958-962.
Ochipa, C., Rothi, L. J., & Heilman, K. M. (1992). Conceptual apraxia in Alzheimer's
disease. Brain, 115, 1061-1071.
Ochipa, C., Rothi, L. J., & Heilman, K. M. (1994). Conduction apraxia. Journal of
Neurology, Neurosurgery & Psychiatry, 57, 1241-1244.

40
Pazzaglia, M., Smania, N., Corato, E., & Aglioti, S. M. (2008). Neural underpinnings
of gesture discrimination in patients with limb apraxia. Journal of Neuroscience, 28, 3030-
3041.
Peigneux, P., Salmon, E., Garraux, G., Laureys, S., Willems, S., Dujardin, K. et al.
(2001). Neural and cognitive bases of upper limb apraxia in corticobasal degeneration.
Neurology, 57, 1259-1268.
Pharr, V., Uttl, B., Stark, M., Litvan, I., Fantie, B., & Grafman, J. (2001). Comparison
of apraxia in corticobasal degeneration and progressive supranuclear palsy. Neurology., 56,
957-963.
Pramstaller, P. P. & Marsden, C. D. (1996). The basal ganglia and apraxia. [Review]
[105 refs]. Brain., 119, 319-340.
Rapcsak, S. Z., Ochipa, C., Beeson, P. M., & Rubens, A. B. (1993). Praxis and the
right hemisphere. Brain & Cognition, 23, 181-202.
Rothi, L. J., Mack, L., & Heilman, K. M. (1986). Pantomime agnosia. Journal of
Neurology, Neurosurgery & Psychiatry, 49, 451-454.
Rothi, L. J. G. & Heilman, K. (1997). Apraxia: The Neuropsychology of Action.
Hove, UK: Psychology Press.
Roy, E. A. (1996). Hand Preference, Manual Assymetries, and Limb Apraxia. In
D.Elliot (Ed.), Manual Asymmetries in Motor Control (pp. 215). Boca Raton, FL: CRC Press.

41
Roy, E. A., Black, S. E., Blair, N., & Dimeck, P. T. (1998). Analyses of deficits in
gestural pantomime. Journal of clinical and experimental neuropsychology, 20, 628-643.
Roy, E. A., Heath, M., Westwood, D., Schweizer, T. A., Dixon, M. J., Black, S. E. et
al. (2000). Task demands and limb apraxia in stroke. Brain and cognition, 44, 253-279.
Roy, E. A. & Square, P. (1985). Common considerations in the study of limb, verbal
and oral apraxia. In E.A.Roy (Ed.), Advances in Psychology (pp. 111-161). Amsterdam:
North-Holland.
Salter, J. E., Roy, E. A., Black, S. E., Joshi, A., & Almeida, Q. (2004). Gestural
imitation and limb apraxia in corticobasal degeneration. Brain & Cognition, 55, 400-402.
Schnider, A., Hanlon, R. E., Alexander, D. N., & Benson, D. F. (1997). Ideomotor
apraxia: behavioral dimensions and neuroanatomical basis. Brain & Language, 58, 125-136.
Skilbeck, C. E., Wade, D. T., Hewer, R. L., & Wood, V. A. (1983). Recovery after
stroke. J Neurol Neurosurg Psychiatry, 46, 5-8.
Soliveri, P., Piacentini, S., & Girotti, F. (2005). Limb apraxia in corticobasal
degeneration and progressive supranuclear palsy. Neurology, 64, 448-453.
Spatt, J., Bak, T., Bozeat, S., Patterson, K., & Hodges, J. R. (2002). Apraxia,
mechanical problem solving and semantic knowledge: Contributions to object usage in
corticobasal degeneration. Journal of Neurology., 249, 601-608.
Tessari, A., Canessa, N., Ukmar, M., & Rumiati, R. I. (2007). Neuropsychological
evidence for a strategic control of multiple routes in imitation. Brain, 130, 1111-1126.

42
Ukmar, M., Moretti, R., Torre, P., Antonello, R. M., Longo, R., & Bava, A. (2003).
Corticobasal degeneration: Structural and functional MRI and single-photon emission
computed tomography. Neuroradiology, 45, 708-712.
Villarreal, M., Fridman, E. A., Amengual, A., Falasco, G., Gerscovich, E. R., Ulloa,
E. R. et al. (2008). The neural substrate of gesture recognition. Neuropsychologia, 46, 2371-
2382.
Watson, R. T., Fleet, W. S., Gonzalez-Rothi, L., & Heilman, K. M. (1986). Apraxia
and the supplementary motor area. Archives of Neurology, 43, 787-792.
Wenning, G. K., Litvan, I., Jankovic, J., Granata, R., Mangone, C. A., McKee, A. et
al. (1998). Natural history and survival of 14 patients with corticobasal degeneration
confirmed at postmortem examination. Journal of Neurology, Neurosurgery & Psychiatry,
64, 184-189.
Westwood, D. A., Schweizer, T. A., Heath, M. D., Roy, E. A., Dixon, M. J., & Black,
S. E. (2001). Transitive gesture production in apraxia: Visual and nonvisual sensory
contributions. Brain & Cognition., 46, 300-304.
Zadikoff, C. & Lang, A. E. (2005). Apraxia in movement disorders. Brain., 128,
1480-1497.

43
CHAPTER 2: PERFORMANCE ON PANTOMIME AND IMITATION OF
TRANSITIVE AND INTRANSITIVE GESTURES IN LEFT AND RIGHT
HEMISPHERE STROKE PATIENTS
ABSTRACT
The study investigated performance on pantomime and imitation of transitive and
intransitive gestures in 81 stroke patients, 43 with left (LHD) and 38 with right (RHD)
hemisphere damage. Patients were also categorized in two groups based on the time that has
elapsed between their stroke and the apraxia assessment: acute-subacute (n=43) and chronic
(n=38). In addition, patterns of performance in apraxia were examined. We expected that
acute-subacute patients would be more impaired than chronic patients and that LHD patients
would be more impaired than RHD patients, relative to controls. The hemisphere prediction
was confirmed, replicating previous findings. The frequency of apraxia was also higher in all
LHD time post-stroke groups. The most common impairment after LHD was impairment in
both pantomime and imitation in both transitive and intransitive gestures. Selective deficits in
imitation were more frequent after RHD for transitive gestures but for intransitive gestures
they were more frequent after LHD. Patients were more impaired on imitation than
pantomime, relative to controls. Chronic patients were also less impaired than acute-subacute
patients, even though the difference did not reach significance. A longitudinal study is
needed to examine the recovery patterns in both LHD and RHD patients.

44
INTRODUCTION
Limb apraxia is a movement disorder that expresses itself by an inability to perform
purposeful movements such as using everyday tools and/or making communicative gestures.
Unlike other motor control disorders, limb apraxia is not caused by a physical disability;
rather, it results from higher-order cognitive disruptions of the nervous system. It is often
defined by exclusion: apraxia is not caused by muscle weakness, paralysis, dystonia, tremor,
chorea, myoclonus or defects of sensory feedback. It is also not caused by cognitive deficits
such as aphasia, agnosia or inattention (Heilman & Rothi, 1993). Limb apraxia is typically
assessed by asking a patient to pantomime (perform a gesture from memory to a verbal
command) or to imitate a visually-presented gesture. Therefore, limb apraxia can also be
defined as the inability to pantomime or imitate gestures (Roy, 1996; Roy, 1996). According
to Roy‟s model of apraxia three systems are involved in the control of movement: a
sensory/perceptual system processing information from the environment, a conceptual
system stores our knowledge of gestures and tools, while the production system is
responsible for response selection and control of movement. Both pantomime and imitation
are dependent on the patient‟s preserved ability to organize and plan movements (i.e. they
require an intact production system), in order to successfully perform the gesture.
Pantomime, however, is also dependent on the patient‟s preserved knowledge of tools and
actions (i.e. it requires an intact conceptual system). When a patient is given a verbal
instruction, he/she must retrieve from memory what a particular tool looks like and what its
function is and link this with the representation of the action associated with this tool.
Imitation, on the other hand, is dependent on the preserved ability to process the visual
information in the gesture performed by the examiner and to translate this information into a

45
movement. Here a patient does not need to know what the gesture means in order to be able
to perform the movement, although meaningful gestures are often imitated more accurately
due to the support afforded through semantics (Rumiati & Tessari, 2002).
Limb apraxia is often observed in patients who have suffered a stroke. A review of
studies examining the prevalence of limb apraxia after stroke reported a prevalence of
apraxia after left hemisphere damage (LHD) ranging from 28% to 57% (median = 45%),
whereas the prevalence after right hemisphere damage (RHD) ranged from 0% to 34%
(median = 8%) (Donkervoort, Dekker, van den Ende, Stehmann-Saris, & Deelman, 2000). A
series of studies conducted by Roy and colleagues compared the performance of transitive
and intransitive gestures in pantomime and imitation in LHD and RHD stroke participants.
First, Roy et al. (2000) showed that deficits in pantomime alone or imitation alone were
equally common after damage to either hemisphere, but that deficits in pantomime and
imitation together were more common after LHD. Later, a similar study in intransitive
gestures reported that imitation alone, pantomime alone, as well as, deficits in both
pantomime and imitation were equally likely after damage to either hemisphere (Heath, Roy,
Black, & Westwood, 2001). The findings from both studies were at odds with many previous
reports showing a greater role of the left hemisphere in the control of movement (Kimura &
Archibald, 1974; Hanna-Pladdy et al., 2001; Haaland, Harrington, & Knight, 2000). Because
the studies of Roy and colleagues examined separately transitive and intransitive gestures, we
wanted to directly compare the performance of the two gesture types within the same sample.
In stroke, accuracy in the performance of transitive gestures is often lower than that of
intransitive gestures (Haaland & Flaherty, 1984; Schnider, Hanlon, Alexander, & Benson,
1997; Haaland et al., 2000; Gonzalez-Rothi, Mack, Verfaellie, Brown, & Heilman, 1988). In

46
addition, it has been suggested that the left hemisphere may control transitive gestures while
both hemispheres may be involved in the control of intransitive gestures (Haaland et al.,
1984; Buxbaum, Kyle, Grossman, & Coslett, 2007; Rapcsak, Ochipa, Beeson, & Rubens,
1993; Mozaz, Rothi, Anderson, Crucian, & Heilman, 2002). Given that the two gesture types
may be subserved by different brain networks (Bartolo, Cubelli, Della Sala, Drei, &
Marchetti, 2001), we considered it important to directly compare the performance of both
pantomime and imitation in transitive and intransitive gestures, to examine performance
differences in both hemisphere groups and to report the frequencies of the various patterns of
deficits in each group of patients for both gesture types.
Given the greater role of the left hemisphere in the performance of pantomime as
opposed to imitation and of transitive gestures as opposed to intransitive, we predicted that
pantomime tasks and transitive gestures would show greater impairment in the LHD patients.
We also hypothesized that performance on transitive gestures would be less accurate than
intransitive gestures and that pantomime would be less accurate than imitation performance.
Finally, based on Roy et al (2000) and Heath et al. (2001), we also predicted that patterns of
deficits with selective imitation in pantomime or imitation, would be equally likely after
LHD or RHD, but the pattern with deficits in both pantomime and imitation will be more
common after LHD.
METHODS
Participants
Eighty-one right-handed participants with a single unilateral hemispheric stroke, 35
women and 46 men, 43 LHD and 38 RHD, were included in the study with a mean age of 66
(SD=12.7) years. Patients were recruited from Sunnybrook Health Sciences Centre in

47
Toronto, Ontario, Canada. Consent to participate in the study was obtained from all
participants and the study was approved by the Research Ethics Board at Sunnybrook Health
Sciences Centre and at the University of Waterloo. Patients were excluded from the study if
they had a history of a neurological impairment (other than the single stroke in the case of the
stroke adults), or a history of alcohol or drug abuse, dementia, psychiatric or movement
disorders (e.g., tremor, bradykinesia or dyskinesia), or any peripheral condition (e.g.,
arthritis) which could compromise motor function. Patients were also excluded from the
study if they were over 90 years of age at the time of they were comsidered for participation
in the study or had a severe comprehension deficit that prevented them from understanding
the assessment instructions. Patients were also requires to have at least 8 years of formal
education. Because the sample consisted of patients assessed at different stages post-stroke
and given chronic patients may perform better than acute patients, based on past research
suggesting apraxia recovers somewhat over the first three months post-stroke (Basso, Burgio,
Paulin, & Prandoni, 2000; Foundas, Raymer, Maher, Gonzalez-Rothi, & Heilman, 1993), we
also categorized patients based on the time elapsed between their stroke and the apraxia
assessment. Patients assessed within 3 months post stroke were categorized as “acute-
subacute”, while patients assessed over three months post stroke were categorized as
“chronic”. This resulted in 43 patients categorized as acute-subacute and 38 patients
categorized as chronic. See Table 2.1 for a summary of the number of patients per group and
a summary of the age, years of education, MMSE scores and days since stroke onset for each
group. In the acute-subacute group, the time since stroke onset ranged from 3-84 days, while
in the chronic group the time since onset ranged from 103 to 5753 days.

48
Table 2.1: Sample Characteristics per patient group.
Western Aphasia Battery scores were available only for 20 of the LHD patients,
whose mean WAB Aphasia Quotient was 74 (SD=24). Comprehension WAB scores were
available on 21 LHD patients and the average score was 8.6 (SD=1.3), which indicates good
comprehension level (Kertesz & Poole, 1974). Unfortunately, the WAB data was not
collected consistently and, therefore, we cannot be sure that the patients who were not tested
did not have any comprehension deficits. However, all patients included in the study were at
a language comprehension level that allowed them to understand verbal instructions and their
responses on the pantomime tasks indicated that they understood what they were asked to do.
Patients were excluded from the study if they presented with multiple strokes, had a history
of any other neurological disorders, peripheral motor disorders or disorders that could affect
their ability to perform gestures such as severe arthritis.
In addition, performance of 27 age-matched [Mean Age=67.3, SD=8.7, t (1, 80)=.59,
p=.58] normal control community volunteers, with no history of neurological diseases, were
assessed on all tasks with each hand.
Acute-Subacute
Mean (SD)
Chronic
Mean (SD)
Control
Mean
(SD)
F-
Value
p-
Value
LHD RHD LHD RHD
Age 63 (15) 65 (15) 67 (9) 59 (15) 67 (9) 1.6 .19
Years of
Education 14 (3) 13 (3) 14 (3) 15 (3) 15 (3) 1.1 .36
MMSE 19(10) 25 (7) 25 (6) 27 (2) 29 (2) 6.8 <.001
Days Since
Stroke 17 (15) 23 (19) 1679 (1811) 1697 (1583) ----- 13.9 <.001

49
Gestural Tasks and Performance Scoring
Patients were asked to perform four tasks: Pantomime to Verbal Command of
Transitive Gestures, Pantomime to Verbal Command of Intransitive Gestures, Concurrent
Imitation of Transitive Gestures and Concurrent Imitation of Intransitive Gestures. The
pantomime conditions were always performed first in order to avoid giving any cues as to
how the gesture was performed. The tasks and scoring procedure are described in Appendix
A. From here on the Pantomime to Verbal Command tasks will be referred to as simply
Pantomime, while the Concurrent Imitation tasks will be referred to as Imitation.
Analysis
All patients were assessed with their ipsilesional hand. Our previous work has shown
that there were no hand differences in gesture performance in the controls (Roy, Square-
Storer, Hogg, & Adams, 1991) and, hence, ipsilesional hand performance in the stroke
groups was examined with reference to average of the hand performance of the control
group. Performance for each stroke patient was converted to a Z-score with reference to the
mean and standard deviation of the controls. This allowed us to evaluate the performance of
the patients in each task relative to controls. The two hands of the control participants were
pooled together, in order to control for differences between left versus right hand
performance in the patients, since patients used only their ipsilateral hand.
These Z-scores were used in two analyses. One was an ANOVA comparing
performance among the four groups of patients, LHD and RHD stroke in each of two
chronicity (acute-subacute vs. chronic) groups, while the other compared the frequency of
apraxia among the four groups of patients. In this analysis, Z-scores falling 2 SDs below the
mean of the controls were considered to be within the impaired or apraxic range. Z-scores

50
between 1 and 2 SDs below the mean of the controls were categorized as borderline apraxic,
while those within 1 SD of the controls were categorized as non-apraxic.
RESULTS
Sample Characteristics
In order to rule out any differences in age and education among the patient groups, a
2 (chronicity) x 2(hemisphere) MANOVA was run to compare the patients. No main effects
or interactions were observed. In addition, in order to compare the patient groups relative to
controls, an ANOVA comparison between the four patient subgroups and the controls
revealed no group differences on age or education (see Table 2.1). In addition, a
2(Chronicity) x 2(Hemisphere) MANOVA was run to compare the patients‟ performance on
the MMSE (only 20 LHD acute, 15 RHD acute, 5 LHD chronic and 19 RHD chronic had
MMSE data). The analysis showed a significant main effect of Chronicity F(1,65)=6.3, p<.05
showing acute-subacute patients obtained significantly lower MMSE scores (Mean=21,
SD=9) than chronic patients (Mean=26, SD=4). In addition, a main effect of hemisphere
showed that LHD patients performed significantly worse (Mean=21, SD=9) than RHD
patients (Mean=26, SD=5) on MMSE, [F(1.65)=6.0, p<.05)]. There was no interaction
between the hemisphere and the chronicity factor.
Group Comparisons
A 2(chronicity: acute-subacute vs. chronic) x 2 (hemisphere: LHD vs. RHD) x 2 (task
modality: pantomime vs. imitation) x 2 (gesture type: transitive vs. intransitive) mixed
multivariate analysis of variance (MANOVA) was used to compare the performance of the
stroke patients on the apraxia assessment.

51
Analyses (Figure 2.1) revealed significant main effects for hemisphere, F(1,77)=13.6,
p<.001, indicating LHD patients were more impaired (Mean=-6.7) than RHD patients
(Mean=-1.4). A significant effect for task modality was also found, F(1, 7711)=11.1, p<.1
indicating performance on imitation (Mean=-5.4) was more impaired relative to controls than
performance on pantomime (Mean=-2.7) (See Table 2.2). A main effect of gesture type was
also found F(1,77)=4.9, p<.05, showing performance of transitive gestures was more
impaired (Mean=-4.5) than performance of intransitive gestures (Mean=-3.5). While there
were no other significant main effects or interactions, several effects were in the predicted
direction. The performance of acute-subacute patients was more impaired (Mean=-5.4) than
that for chronic patients (Mean=-2.6, F(1,77)=3.9, p=.053). Finally, the two interactions that
were expected were observed but were not significant: the interactions between task modality
and hemisphere [F(1.77)=3.37, p=.07] and the interaction between gesture type and
hemisphere group [F(1.77)=3.1, p=.09], showing the main effects of gesture type and task
modality to be more pronounced in the LHD group.
Table 2.2. Right vs. Left Hemisphere Mean Percent Accuracy Scores, Z-scores and standard
deviations (SD) on each of the four task modalities.
Pantomime Transitive Pantomime Intransitive
Mean % Mean Z-score SD Mean % Mean Z-score SD
LHD 70.4 -5.9 6.3 78.7 -3.7 6.2
RHD 90.2 -0.9 1.7 90.7 -0.6 1.7
Concurrent Imitation Transitive Concurrent Imitation Intransitive
Mean % Mean Z-score SD Mean % Mean Z-score SD
LHD 82.7 -9.8 13.0 90.3 -8.5 14.4
RHD 94.5 -2.1 3.0 97.1 -1.9 3.8

52
Figure 2.1: Z-scores in each of the four tasks in each group of participants.
Pantomime of Transitive Gestures
-14
-12
-10
-8
-6
-4
-2
0
LHD RHD
Z-S
co
re
Acute-Subacute
Chronic
Pantomime of Intransitive Gestures
-14
-12
-10
-8
-6
-4
-2
0
LHD RHD
Z-S
co
re
Acute-Subacute
Chronic
Imitation of Transitive Gestures
-16
-14
-12
-10
-8
-6
-4
-2
0
LHD RHD
Z-S
co
re
Acute-Subacute
Chronic
Imtiation of Intransitive Gestures
-16
-14
-12
-10
-8
-6
-4
-2
0
LHD RHD
Z-S
co
re
Acute-Subacute
Chronic
Average performance for each of the four groups of patients for the four tasks. Acute-subacute patients obtained lower scores than
chronic patients and LHD patients were more impaired than the RHD patients relative to controls. Transitive gestures were more
impaired. Surprisingly, imitation was more severely impaired relative to the control sample than was pantomime. No interactions
were observed.

53
Apraxia Classification
A chi-square analysis was used to compare the frequency of the three levels of
apraxia (normal, borderline and apraxic) in each of the four groups of patients. A separate
chi-square analysis was run for each of the four tasks. The analysis showed that there was a
significant difference among the four groups in the number of patients falling into the three
levels of apraxia in two of the tasks: Pantomime of Transitive Gestures [χ2(6, 80)=13.4,
p<.05] and Imitation of Intransitive Gestures [χ2(6,80)=12.7, p<.05] based on their
performance in each of the four subgroups (see Table 2.3). In addition, chi-square analyses
examining the frequency of apraxia in LHD than the RHD group irrespective of whether
patients were acute-subacute or chronic revealed a higher number of apraxic patients with
LHD in each of the four tasks. These differences were significant for all four tasks, except
Pantomime of Intransitive Gestures, where the p-value was at p=.08 (See Table 2.4 for
number of cases and frequencies of apraxia categories per hemisphere group).

54
Table 2.3: Number of cases and frequency of occurrence in normal, borderline and apraxia
category in each hemisphere and time post-stroke.
Group
Normal Borderline Apraxic
Freq. % Freq. % Freq. % χ2
p-value
Pantomime Transitive
Acute-Subacute LHD 6 25 1 4 17 71 13.4 p<.05
Chronic LHD 6 32 3 16 10 53
Acute-Subacute RHD 12 63 3 16 4 21
Chronic RHD 10 53 3 16 6 32
Pantomime Intransitive
Acute-Subacute LHD 7 29 3 13 14 58 11.8 0.07
Chronic LHD 12 63 2 11 5 26
Acute-Subacute RHD 11 58 3 16 5 26
Chronic RHD 11 58 5 26 3 16
Imitation Transitive
Acute-Subacute LHD 6 25 1 4 17 71 10.3 0.12
Chronic LHD 7 37 0 0 12 63
Acute-Subacute RHD 8 42 1 5 10 53
Chronic RHD 12 63 2 11 5 26
Imitation Intransitive
Acute-Subacute LHD 5 21 1 4 18 75 12.8 p<.05
Chronic LHD 7 37 3 16 9 47
Acute-Subacute RHD 8 42 6 32 5 26
Chronic RHD 8 42 4 21 7 37
Table 2.4: Number of cases and frequency of occurrence in normal, borderline and apraxia
category per hemisphere.
Hemisphere Normal Borderline Apraxic
χ2 p-value Freq. % Freq. % Freq. %
Pantomime Transitive
LHD 12 28 4 9 27 63 10.9 p<.005
RHD 22 58 6 16 10 26
Pantomime Intransitive
LHD 19 44 5 12 19 44 5.1 0.080
RHD 22 58 8 21 8 21
Imitation Transitive
LHD 13 30 1 2 29 67 6.6 p<.05
RHD 20 53 3 8 15 39
Imitation Intransitive
LHD 12 28 4 9 27 63 8.6 p<.05
RHD 16 42 10 26 12 32

55
Patterns of Apraxia
All patients were classified as apraxic or non-apraxic across tasks. Similarly to the
classification described in Roy et al., (2000) and Heath et al., (2001), patients were
categorized into four patterns of performance for transitive gestures and four patterns of
performance for intransitive gestures based on whether they were impaired on pantomime
and/or imitation. Borderline patients were classified as non-apraxic. The patterns were both
pantomime and imitation non-apraxic (NA). (PNA INA), impaired pantomime but preserved
imitation (PA INA), impaired imitation, but preserved pantomime (PNA IA) and impaired
performance in both pantomime and imitation (PA IA). These patterns were coded for each
patient separately for transitive and for intransitive gestures. Chi-square analyses were run to
compare the frequency of each pattern in each of the four groups of participants. The
analyses were significant for both gesture types (see Table 2.5). In transitive gestures, for
LHD patients the most common pattern was that impaired in both tasks and this was the case
for both acute and chronic patients. For RHD patients, the most common pattern was no
impairment on either task in both acute and chronic patients. For intransitive gestures, in
LHD patients the most common pattern in acute patients was impairment in both pantomime
and imitation, while in chronic patients the most common pattern was „non-apraxic‟ on
either task. In RHD patients, again for both acute and chronic the most common pattern was
that of no impairment on either task. Other interesting observations were that for transitive
gestures selective impairments in either pantomime or imitation seemed to be slightly more
frequent after RHD stroke. For intransitive gestures, selective impairments in pantomime or
in imitation were equally often seen in both hemisphere stroke groups.

56
Table 2.5: Patterns of Apraxia for each group in Transitive and Intransitive Gestures.
Transitive Gestures,
χ2=18.2, p<.001
Intransitive Gestures,
χ2=9.84, p<.05
Acute Chronic Acute Chronic
LHD RHD LHD RHD LHD RHD LHD RHD
n % n % n % n % n % n % n % n %
PNA INA 5 21 8 42 7 37 10 53 4 17 11 58 8 42 11 58
PA INA 2 8 1 5 0 0 4 21 2 8 3 16 2 11 1 5
PNA IA 2 8 7 37 2 11 3 16 6 25 3 16 6 32 5 26
PA IA 15 63 3 16 10 53 2 11 12 50 2 11 3 16 2 11 P=pantome, I=imitation; NA=non-apraxic, A=apraxic
DISCUSSION
The current study aimed to examine performance differences on pantomime and
imitation of transitive and intransitive gestures in LHD vs. RHD stroke patients. The goal
was to extend the work of Roy et al., (2000) and Heath et al., (2001) by directly comparing
the performance of transitive and intransitive gestures within the same sample. In addition,
we included another variable in our comparison, that of chronicity to examine performance
differences between acute-subacute patients and chronic patients.
First, as predicted, LHD patients were more impaired than RHD patients irrespective
of gesture modality or gesture type (See Table 2.2), consistent with previous reports of Roy
and colleagues (Heath, Roy, Westwood, & Black, 2001; Roy et al., 2000), as well as, other
studies supporting a predominance of apraxia in LHD patients (De Renzi, Motti, & Nichelli,
1980; Rothi & Heilman, 1997; Roy et al., 1998).
In addition, consistent with our hypothesis, transitive gestures were significantly more
impaired than performance on intransitive gestures, a finding in support of past literature
(GoodglasS & Kaplan, 1963; Roy et al., 1993; Almeida, Black, & Roy, 2002).

57
Contrary to our expectations, imitation performance was more severely impaired than
pantomime. While this finding, at first glance, seems to be at odds with past studies showing
lower accuracy in pantomime than imitation, in fact it is not. Our analysis was based on Z-
scores that standardized the performance of patients relative to that of controls. The actual
percentage scores (See Table 2.2) for each group, reveals that patients in fact performed with
lower accuracy in pantomime than imitation; however, relative to control participants, their
imitation performance was more severely affected. While patients were less accurate on
pantomime than imitation in terms of their percentage scores, the greater negative Z-scores
for imitation reflects a greater impairment in the stroke patients due to the greater accuracy
and smaller standard deviation for imitation in the control group The lower accuracy on
pantomime concurs with the work of both Heath et al. (2001) for intransitive gestures and
Roy et al. (2000) for transitive gestures., as well as the work of other researchers (Schnider et
al., 1997; Alexander, Baker, Naeser, Kaplan & Palumbo, 1992)
In addition, while no significant interactions were observed between task modality
and hemisphere group and gesture type and hemisphere group, the effects of task modality
and gesture type as expected were somewhat more pronounced in the LHD group. This is
likely due to the more severe apraxia in the LHD group and thus these task modality and
gesture type effects were more evident in this group. In addition, a greater impairment in
LHD patients is consistent with the theory that pantomime, as well as performance of tool-
related gestures are tasks that are more dependent on the left hemisphere (Haaland et al.,
1984; Buxbaum et al., 2007; Rapcsak et al., 1993; Mozaz et al., 2002)
Unlike past studies conducted by Roy and colleagues, our study also included a
comparison between acute-subacute and chronic patients. This classification of the patients

58
was included because past studies, while relatively few and conducted only in left
hemisphere stroke, have suggested that there is a significant recovery from apraxia,
especially in the first three months post-stroke (Basso et al., 2000; Foundas et al., 1993).
Given our sample of patients included a wide range of times post-stroke, we expected that the
acute-subacute patients would perform worse than chronic patients, particularly for the LHD
patients. We expected that chronic LHD patients would have undergone some recovery of
praxis function and hence may be less severely affected than acute patients. Our expectations
were partially met. While acute patients were more impaired than chronic patients (Mean=-
5.4 for acute and Mean=-2.6 for chronic), the difference was not significantly different. It
should also be noted that both acute and chronic patients had mean Z-scores below 2SDs
(Acute LHD Mean= -9.2, while Chronic LHD patients Mean= -4.1) suggesting that both
groups were impaired relative to controls. In contrast, the RHD groups‟ mean scores (Acute
RHD Mean= -1.6 and Chronic RHD Mean=-1.2) fell in both cases above 2 SDs below the
mean of the controls suggesting a relatively preserved performance. Therefore, consistent
with past recovery studies that have examined recovery only in LHD patients, our group
comparisons support the evidence for recovery. No studies to date have examined recovery
patterns after RHD, however. Our findings of small differences between the two RHD
chronicity groups may be due to a larger number of impaired patients. Therefore, these
findings should not be taken to assume that recovery from apraxia is not observed in RHD
patients and a longitudinal study would be required to address this question.
Patterns of Apraxia
In the present study, we observed all four patterns of deficits for both transitive and
intransitive gestures proposed by Roy (1996). In most cases, all four patterns were

59
represented in each of the four groups of participants, with the exception of the selective
deficit in pantomime, which was not observed in chronic LHD patients.
First, examining the frequency of patients who did not show deficits on either
pantomime or imitation, we noted that in both transitive and intransitive gestures there is
always a greater number of RHD patients who fall in that category. Again, this confirms the
greater role of the left hemisphere in the control of pantomime and imitation tasks. In
addition, in all cases the chronic groups had a higher number of patients who were not
impaired on either task, supporting the notion that the chronic group was less affected by
apraxia, presumably because these patients have recovered to some extent.
Second, we turn to the pattern of performance representing a selective impairment in
pantomime. Such pattern of performance, according to Roy (1996), suggests that patients
have deficits in the conceptual knowledge of gestures and tools, or may have that knowledge
disconnected from the centers responsible for organizing movement. It has been widely
accepted that the conceptual knowledge related to gestures and tools is stored in the left
hemisphere and more specifically in the left IPL (Heilman, Rothi, & Valenstein, 1982;
Buxbaum, 2001). If this were the case, then we would expect that this pattern of performance
would be more frequent after LHD. However, the results in this study indicate that this
pattern is equally likely after damage to either hemisphere, and in some cases, it is even more
prevalent after right hemisphere damage (among the chronic group this pattern was not even
observed after LHD, but it was highly prevalent after RHD). Therefore, our findings are
consistent with those of Roy et al. (2000), confirming in a new sample of stroke patients, the
equal likelihood of this pattern after damage to either hemisphere. For intransitive gestures,
selective deficits in pantomime were more prevalent after RHD among acute patients, but the

60
reverse was observed among chronic patients. The sample is small, but the number of
patients presenting with this pattern is somewhat similar among the two hemisphere groups,
again supporting previous work from Roy‟s lab (Heath et al., 2001).
The third pattern of performance, selective deficit in imitation, was more frequently
observed than selective impairment in pantomime. For transitive gestures, the pattern was
more prevalent after RHD in both acute and chronic patients, which replicates Roy et al.‟s
(2000) findings. For intransitive gestures, the opposite was observed, a slightly greater
number of LHD patients, especially among acute patients, presented with this pattern of
apraxia. Selective deficits in imitation may arise from deficits in processing visuospatial
information, or from deficits translating this movement into action (Roy, 1996). It is possible,
therefore, that the acute RHD patients may have had greater deficits in visuospatial
processing, given the role of the right hemisphere in such tasks. Intransitive gestures, may be
easier to process visuospatially, given they are symbolic, which may have rendered them
easier to identify.
Finally, the fourth pattern, impairment in both pantomime and imitation, is thought to
reflect impairments in the final stages of gesture production, with or without conceptual
deficits in gesturer knowledge (Roy, 1996). This pattern was consistently more frequent after
LHD. In all cases, it was close to 4 times more frequent after LHD, except among the chronic
group‟s performance on intransitive gestures, where the frequency among LHD was 16%
while after RHD was 11%. This finding confirms the greater role of the left hemisphere in
the final stages of the control of movement and suggests that the left hemisphere is critical
for the proper functioning of the production system.

61
In summary, consistent with Roy et al.(2000), we have shown that the patterns of
apraxic deficits in transitive gestures are distinct in patients with RHD versus LHD stroke
patients and that the highest percentage of LHD patients presenting with some form of
apraxia were impaired on both pantomime and imitation, whereas the highest percentage of
RHD patients with apraxia were patients selectively impaired on imitation. For intransitive
gestures, consistent with Heath et al. (2001), we have shown that the patterns of apraxic
deficits are more similar between the two hemisphere groups, even though relative to their
findings, we had a slightly higher percent of LHD patients with deficits in both pantomime
and imitation. In addition, we report few differences in relative frequency of the patterns in
acute versus chronic patients, suggesting that if any changes in performance occur over time
they are equally likely after damage to either hemisphere.
Finally, we would like to point out one limitation of our study with regard to
examining recovery of apraxia. While we make some inferences with respect to recovery,
these conclusions were purely exploratory in nature. We believe that the only true way to
assess recovery of praxis is through a longitudinal study examining apraxia over time post
stroke within each subject. Here we took advantage of the fact that we had both acute and
chronic patients in our sample and wanted to examine any potential differences between the
two stroke groups in recovery. While we did confirm our expectations that chronic patients
with LHD performed more accurately than acute patients, the reader should remember that
these are separate samples of patients and there are many other variables that could explain
the difference in performance.

62
Overall Conclusion
The study confirmed previous findings that praxis deficits are higher among LHD
stroke patients, supporting left hemisphere specialization for praxis. In addition, consistent
with past studies impairments in transitive gestures were greater. We also observed that while
lower imitation scores were obtained in pantomime, patients were more severely affected in
imitation relative to controls. The study also provides some evidence that performance on
pantomime and imitation may be predictable based on the time that has elapsed since the
patient‟s stroke. Chronic patients performed better than acute-subacute patients, but a
longitudinal study should further examine recovery of apraxia directly in both LHD and
RHD patients. .

63
REFERENCES
Alexander, M. P., Baker, E., Naeser, M. A., Kaplan, E., & Palumbo, C. (1992).
Neuropsychological and Neuroanatomical Dimensions of Ideomotor Apraxia. Brain, 115, 87-
107.
Almeida, Q. J., Black, S. E., & Roy, E. A. (2002). Screening for apraxia: a short
assessment for stroke patients. Brain & Cognition, 48, 253-258
Bartolo, A., Cubelli, R., Della Sala, S., Drei, S., & Marchetti, C. (2001). Double
dissociation between meaningful and meaningless gesture reproduction in apraxia. Cortex,
37, 696-699.
Basso, A., Burgio, F., Paulin, M., & Prandoni, P. (2000). Long-Term Follow-up of
Ideomotor apraxia. Neuropsychological Rehabilitation, 10, 1-13.
Buxbaum, L. J. (2001). Ideomotor apraxia: a call to action. Neurocase, 7, 445-458.
Buxbaum, L. J., Kyle, K., Grossman, M., & Coslett, H. B. (2007). Left inferior
parietal representations for skilled hand-object interactions: Evidence from stroke and
corticobasal degeneration. Cortex, 43, 411-423.
De Renzi, E., Motti, F., & Nichelli, P. (1980). Imitating gestures. A quantitative
approach to ideomotor apraxia. Archives of Neurology, 37, 6-10.
Donkervoort, M., Dekker, J., van den Ende, E., Stehmann-Saris, J. C., & Deelman, B.
G. (2000). Prevalence of apraxia among patients with a first left hemisphere stroke in
rehabilitation centres and nursing homes. Clinical Rehabilitation., 14, 130-136.

64
Foundas, A. L., Raymer, A. M., Maher, L. M., Gonzalez-Rothi, L., & Heilman, K. M.
(1993). Recovery in Ideomotor Apraxia. Journal of Clinical and Experimental
Neuropsychology, 15, 44-44.
Gonzalez-Rothi, L., Mack, L., Verfaellie, M., Brown, P., & Heilman, K. M. (1988).
Ideomotor Apraxia: Error Pattern Analysis. Aphasiology, 2, 381-387.
Goodglass, H. & Kaplan, E. (1963). Disturbance of gesture and pantomime in
aphasia. Brain.86:703-20.
Haaland, K. Y. & Flaherty, D. (1984). The different types of limb apraxia errors made
by patients with elft vs. right hemispehre damage. Brain and cognition, 3, 370-384.
Haaland, K. Y., Harrington, D. L., & Knight, R. T. (2000). Neural representations of
skilled movement. Brain, 123, 2306-2313.
Hanna-Pladdy, B., Daniels, S. K., Fieselman, M. A., Thompson, K., Vasterling, J. J.,
Heilman, K. M. et al. (2001). Praxis lateralization: errors in right and left hemisphere stroke.
Cortex, 37, 219-230.
Heath, M., Roy, E. A., Black, S. E., & Westwood, D. A. (2001). Intransitive limb
gestures and apraxia following unilateral stroke. Journal of clinical and experimental
neuropsychology, 23, 628-642.
Heath, M., Roy, E. A., Westwood, D., & Black, S. E. (2001). Patterns of apraxia
associated with the production of intransitive limb gestures following left and right
hemisphere stroke. Brain & Cognition, 46, 165-169.

65
Heilman, K. M. & Rothi, L. J. (1993). Apraxia. In Clinical Neuropsychology (pp.
141-163). New York, NY: Oxford University press Inc.
Heilman, K. M., Rothi, L. J., & Valenstein, E. (1982). Two forms of ideomotor
apraxia. Neurology, 32, 342-346.
Kertesz, A. & Poole, E. (1974). The aphasia quotient: the taxonomic approach to
measurement of aphasic disability. Canadian Journal of Neurological Sciences.1(1):7-16.
Kimura, D. & Archibald, Y. (1974). Motor functions of the left hemisphere.
Brain.97(2):337-50.
Mozaz, M., Rothi, L. J., Anderson, J. M., Crucian, G. P., & Heilman, K. M. (2002).
Postural knowledge of transitive pantomimes and intransitive gestures. Journal of the
International Neuropsychological Society, 8, 958-962.
Rapcsak, S. Z., Ochipa, C., Beeson, P. M., & Rubens, A. B. (1993). Praxis and the
right hemisphere. Brain & Cognition, 23, 181-202.
Rothi, L. J. G. & Heilman, K. (1997). Apraxia: The Neuropsychology of Action.
Hove, UK: Psychology Press.
Roy, E. A. (1996). Hand Preference, Manual Assymetries, and Limb Apraxia. In
D.Elliot (Ed.), Manual Asymmetries in Motor Control (pp. 215). Boca Raton, FL: CRC Press.
Roy, E. A., Black, S. E., Blair, N., & Dimeck, P. T. (1998). Analyses of deficits in
gestural pantomime. Journal of clinical and experimental neuropsychology, 20, 628-643.

66
Roy, E. A., Brown, L., Winchester, T., Square, P., Hall, C., & Black, S. (1993).
Memory processes and gestural performance in apraxia. Adapted Physical Activity Quarterly,
10, 293-311.
Roy, E. A., Heath, M., Westwood, D., Schweizer, T. A., Dixon, M. J., Black, S. E. et
al. (2000). Task demands and limb apraxia in stroke. Brain and cognition, 44, 253-279.
Roy, E. A., Square-Storer, P., Hogg, S., & Adams, S. (1991). Analysis of task
demands in apraxia. International Journal of Neuroscience, 56, 177-186.
Rumiati, R. I. & Tessari, A. (2002). Imitation of novel and well-known actions: the
role of short-term memory. Experimental Brain Research., 142, 425-433.
Schnider, A., Hanlon, R. E., Alexander, D. N., & Benson, D. F. (1997). Ideomotor
apraxia: behavioral dimensions and neuroanatomical basis. Brain & Language, 58, 125-136.

67
CHAPTER 3: A MODEL-BASED APPROACH TO LONG-TERM RECOVERY OF
LIMB APRAXIA AFTER STROKE
ABSTRACT
Limb apraxia is a disorder affecting performance of gestures on verbal
command (pantomime), on imitation, and/or in tool and action recognition. We aimed to
examine recovery on tasks assessing both conceptual and production aspects of limb praxis
in left (n=11), right (n=18) and bilateral (n=2) stroke patients. Patients were assessed
longitudinally (average 3 times) on three conceptual (Action Identification, Tool Naming by
Action and Tool Naming) and five production tasks (Pantomime, Pantomime by Picture,
Concurrent Imitation, Delayed Imitation and Object Use). They were grouped as presenting
with impairment (Score<2 SDs of the controls‟ mean (n=27)) or not, and as acute-subacute
(first assessment within 3 months post stroke) or chronic (over 3 months post stroke).
Hierarchical linear modeling was used to analyze the data because patients were assessed at
different intervals and had variable numbers of follow-ups. Average performance of chronic
impaired patients was higher than acute impaired patients on pantomime, pantomime by
picture and concurrent imitation. While all tasks, except Action Identification, showed
evidence of recovery in both acute and chronic impaired patients, a faster rate of recovery
among acute patients was observed only in the two pantomime and two imitation tasks.
Chronic impaired patients had similar gains in performance as acute patients in object use
and the tool naming tasks.

68
INTRODUCTION
Limb apraxia is a higher-order disorder of skilled movement that could manifest itself
in deficits of gesture production or deficits in gesture and tool knowledge. Deficits in gesture
production could be manifested as an inability to pantomime (e.g., perform gestures to verbal
command), an inability to imitate gestures that are visually presented to the patient, an
inability to use tools or any combination of the above. Deficits in gesture recognition can
present themselves as an inability to recognize gestures or to identify objects or to match
objects with their functions or gestures/actions. Limb apraxia has been generally defined as
an inability to pantomime or imitate gestures or both (Roy, 1996).
An information-processing approach has been developed by Roy (1996), who
suggests that skilled movement is under the control of three systems: conceptual, production
and sensory/perceptual. The sensory/perceptual system processes visual, auditory and tactile
information from the environment. The conceptual system stores knowledge about tools and
actions. The production system consists of several subsystems serving such functions as
response selection, image generation, working memory storage of the motor plan and
response organization and control of movement. Disruptions in any of these systems produce
specific patterns of apraxia. Roy (1996) proposes eight major patterns resulting from damage
to different processes within one or more of the three systems. In order to determine the
pattern of apraxic performance three gesture production tasks (pantomime, delayed imitation
and concurrent imitation) and at least one Gesture-Tool/Object recognition task (Action
identification and/or Tool identification) need to be administered. The pattern of deficit
points to which system(s) are affected, for example by a stroke. The eight patterns are
summarized in Table 3.1 (Roy, 1996) and described in detail in Chapter 1. For example, one

69
pattern includes an inability to pantomime gestures and to identify gestures and tools with
preserved ability to imitate gestures both concurrently and with delay. This pattern suggests a
disruption in the conceptual system, that is, knowledge associated with tools, such as what
tools are used for and how they are used is lost. Imitation, however, is preserved because the
individual can process the visual gestural information demonstrated by the examiner and can
translate this into movement. Preserved imitation in the face of impaired gesture
representation suggests that access to semantics is not required to accurately imitate a
gesture. Indeed most of the patients exhibiting this pattern are able to imitate meaningless
gestures which have no representation in semantics.
Table 3.1: Patterns of Deficits as defined by Roy‟s Model (Roy, 1996)
Apraxia Performance Pattern System Affected Nature of Disruption
"Sensory/perceptual
(P+/DI-/CI-/ID-)" Sensory/Perceptual
Impaired ability to analyse visual
gestural and tool/object information
"Conceptual
(P-/DI+/CI+/ID-)" Conceptual
Impaired knowledge of action and
tool/object function
"Production Resp Selection
(P-/DI+/CI+/ID+)" Production
Impaired response selection and/or
image generation
"Production Encoding
(P+/DI-/CI+/ID+)" Production
Impaired encoding of visual gestural
information into working memory
"Production Working Memory
(P-/DI-/CI+/ID+)" Production Impaired working memory
"Production Conduction
(P+/DI-/CI-/ID+)" Production
Impaired ability to use visual
information in the control of movement
"Production Ideomotor
(P-/DI-/CI-/ID+)" Production
Impaired response organization and
control
"Global (P-/DI-/CI-/ID-)"
Production +
Conceptual
Impaired knowledge of action and
tool/object function + Impaired
response organization and control. P=Pantomime, DI= Delayed Imitation, CI=Concurrent Imitation, ID=Gesture Identification
(-) indicates impaired performance and (+) indicates normal performance.
Limb apraxia occurs commonly after stroke. A comprehensive review (Donkervoort,
Dekker, van den Ende, Stehmann-Saris, & Deelman, 2000) reported that the prevalence of
apraxia after single left hemisphere damage (LHD) ranged from 28% to 57% (median score

70
45%), whereas the prevalence of limb apraxia after single right hemisphere damage (RHD)
ranged from 0% to 34% (median score 8%). However, the literature on recovery of limb
apraxia is quite scarce, with few studies documenting spontaneous patterns of recovery. In
fact, only five studies have been published that examine the spontaneous recovery of limb
apraxia and two of those were only abstract reports. Significant performance differences
between serial examinations was demonstrated by Basso and colleagues, especially during
the first year post stroke, but patients with right hemisphere damage were excluded and the
apraxia assessment included only imitation; pantomime was not examined (Basso, Capitani,
Della Sala, Laiacona, & Spinnler, 1987; Basso, Burgio, Paulin, & Prandoni, 2000). Inclusion
of recovery studies of apraxia to pantomime is important, because pantomime can be more
severely affected than imitation (Roy et al., 2000; Heath, Roy, Black, & Westwood, 2001),
and therefore could either be more resistant to recovery or have more room for recovery and
show bigger gains. Hence, the Basso and colleagues studies provide us with limited
information on post-stroke recovery of limb apraxia. Since task modality and hemisphere
damaged can differentially elicit expression of apraxia, it is important for studies to probe
different test modalities and to test patients with damage in either hemisphere. For example,
some patients may be selectively impaired in imitation while others are only impaired in
pantomime, and frequency of apraxia is lower but not absent in RHD patients (Heath, Roy,
Westwood, & Black, 2001; Roy, Square-Storer, Hogg, & Adams, 1991).
Mimura and colleagues examined pantomime and imitation recovery in 15 LHD,
showing significant improvements in both, but only longer-term effects, assessments at 4.5
months and at 81.6 months post stroke were studied (Mimura, Fitzpatrick, & Albert, 1996).
Hence, earlier changes post stroke where recovery may be most pronounced could not be

71
determined. Furthermore, this study did not include RHD stroke patients, so the recovery
data applied only to LHD stroke patients.
Finally, an abstract reported by (Foundas, Raymer, Maher, Gonzalez-Rothi, &
Heilman, 1993) examined pantomime recovery in subacute stages (6 weeks, 3 and 6 months
post left hemisphere stroke) and reported the greatest recovery during the first three months.
None of the above-mentioned studies included any measures of conceptual
knowledge of gestures. The only such study on pantomime to verbal command and gesture
recognition was an abstract by Cimino-Knight et al., (2002) who examined 12 patients within
6 weeks post stroke onset and then at 3-6 months post onset. While no actual data were
reported, the authors indicated that the two tasks evolved differently during recovery,
suggesting that the two tasks may involve different mechanisms.
All these studies suffer from major methodological problems. First, they do not assess
patients comprehensively enough to probe various processes involved in praxis (Roy, 1996).
Second, none of the studies included RHD stroke patients and thus cannot be applied to RHD
stroke patients, some of whom do exhibit apraxia (Roy, Black, Blair, & Dimeck, 1998).
Thirdly, all of the studies assessed performance over only two time points. This approach
cannot adequately describe the time course of change (i.e. we don‟t know whether recovery
was steady or if it occurred immediately after the first assessment) (Singer & Willett, 2003).
Studies that include multiple timepoints post stroke, on the other hand, are more suitable for
tracing recovery and hierarchical linear modeling allows us to examine such data. What is
more, hierarchical linear modeling (HLM) allows patients, who have been assessed different
number of times or who have different number of assessments, to be included.

72
Therefore, the goal of the current study was to examine how performance on tasks
assessing pantomime and imitation, as well as assessments of praxis knowledge changes over
time in LHD , RHD and Bilateral Hemisphere Damage (BHD) patients. Patients not impaired
in their performance on each task served as controls. Both acute-subacute and chronic
patients were included which allowed us to examine if recovery rates differ as a function of
the chronicity of the stroke. In particular, we examined if patient groups differ in their initial
performance across assessments and if the rate of recovery differs among the groups (acute
patients with or without impairment and chronic patients with or without impairment). Our
hypothesis was that patients with impairment would have steeper slopes of recovery in all
tasks relative to patients without impairment. We also, predicted that chronic impaired
patients will perform better than acute-subacute patients at their initial assessment and that
their slope of recovery will be less steep than that of acute-suabcute impaired patients.
Finally, we also aimed to describe the patterns of limb apraxia that patients present
with and how these patterns evolve over time. While it is difficult to make specific
predictions about the evolution of patterns, given that no studies to date have described them,
if recovery occurs at a similar rate across all tasks, we expect that patients will move from
patterns of impairment to no impairment. If recovery in the three systems occurs at different
rates, then patients will improve only on some tasks, and thus they will switch from one
pattern to another.
METHODS
Participants
Eleven LHD, eighteen RHD and two BHD stroke participants participated in the
study. For all patients the index stroke was their first and only stroke. The sample of patients

73
included both acute-subacute and chronic patients. Acute-subcute patients were patients who
had their first assessment within 3 months of onset (Mean= 15 days, Range 3-31 days) and
chronic patients were first assessed over 3 months post-onset (Mean=875 days, Range 103-
3717 days).
Most patients, who met inclusion and exclusion criteria (Roy et al., 1998) and who
were willing to participate, were recruited from the Sunnybrook Health Sciences Centre
inpatient Stroke Unit or outpatient stroke clinics. Consent to participate in the study was
obtained from all participants and the study was approved by the Research Ethics Board at
Sunnybrook Health Sciences Centre and at the University of Waterloo. Chronic stroke
patients who were recruited from the Cognitive Neurology Clinic at Sunnybrook Health
Sciences Centre, a major University of Toronto academic health care institution. To be
included in the study the patient had to have suffered a single stroke and to have sufficient
comprehension to follow instructions. Exclusion criteria included a history of a neurological
impairment (other than the single stroke), a history of alcohol or drug abuse, dementia,
psychiatric or movement disorders (e.g., tremor, bradykinesia or dyskinesia), or any
peripheral condition (e.g., arthritis) which may compromise motor function. Patients were
also excluded from the study if they were over 90 years of age and had less than 8 years of
formal education.
Procedures
Only Transitive Gestures Tasks were used in this study. All patients performed three
tasks assessing their conceptual knowledge of tools and gestures: Action Identification, Tool
Naming by Action, and Tool Naming and five tasks assessing their ability to perform
transitive gestures: Pantomime to Verbal Command, Pantomime by Picture, Concurrent

74
Imitation, Delayed Imitation and Object Use. All tasks and scoring procedures are described
in Appendix A.
Some patients (N=31) could not complete all tasks. It was decided not to exclude
patients who did not complete all tasks, in order to maintain a larger sample size. Therefore,
the number of subjects varies slightly per task. Seventeen of the 31 patients were assessed
twice, seven patients were assessed three times, two patients were assessed four times and
five patients were assessed 5 times.
The assessment period varied across subjects (Mean 33 months ± 29 months). The
minimum length of participation was 52 days and the maximum was 117 months. In addition,
27 age-matched normal control participants were assessed on all tasks to establish normal
limits of performance. On tasks requiring gesture production, control participants were
assessed with each hand. There were no hand differences in performance so the average
performance of both hands of the normal controls was then calculated and used to
standardize the performance of the stroke participants. See Table 3.2 for means and standard
deviations of the control group for each task.
Table 3.2: Means and Standard Deviations of Control Group per task.
Mean Percent Accuracy SD
Pantomime 94.1 4.2
Pantomime by Picture 94.1 3.2
Object use 97.5 2.0
CI 97.8 1.6
DI 98.0 1.7
Action ID 98.7 3.6
Tool Naming by Action 95.4 7.9
Tool Naming 99.1 3.3 CI=Concurrent Imitation, DI=Delayed Imitation
Percentage scores on the first assessment for each patient were expressed as Z-scores
based on the means and standard deviations of the controls. If the Z- score was two standard

75
deviations (SDs) below the mean of the control group, the patient was categorized as
impaired on their first assessment. Patients were then grouped as impaired or not impaired at
their first assessment separately for each task (referred to below as Impaired versus Not
Impaired Group). The Z-scores were used only for classification of the patients as impaired
or not. All other analyses were done with the actual percentage accuracy scores of the
patients. The combination of acute-subacute and chronic and Impaired vs. Not Impaired
Group produced four subgroups of patients: acute-subacute not impaired, chronic not
impaired, acute-subacute impaired and chronic impaired. A summary of the number of
participants in each of the four groups is presented in Table 3.3. Data on age, education, Mini
Mental Status Examination (MMSE) for the acute-subacute, chronic and control groups are
presented in Table 3.4. An Analysis of variance (ANOVA) was performed to examine if the
three groups differed in any of these measures. The associated p-values for each measure are
also listed in Table 3.4. For categorical data, chi-square analysis was run and the associated
p-values are also listed. All patients had sufficient language comprehension to understand the
task instructions.
Table 3.3: Summary of number of patients in each group for each task
Acute-
Subacute
Not
Impaired
Chronic
Impaired
Acute-
Subacute
Impaired
Chronic
Not
Impaired
Total
Pantomime 5 11 8 7 31
Pantomime by
Picture 5 11 8 7 31
Object use 5 13 8 5 31
CI 6 11 7 7 31
DI 4 10 9 8 31
Action ID 6 3 4 13 26
Tool Naming by
Action 5 3 8 14 30
Tool Naming 4 8 9 10 31 CI=Concurrent Imitation, DI=Delayed Imitation

76
Table 3.4: Demographic Characteristics of the patients
Acute
Patients
Chronic
Patients
Controls p-Value
Age 62 (14) 64 (15) 67.3(9) .47
Years of Education 14 (6) 14 (3) 15 (3) .72
MMSE 25 (7) 27 (3) 29 (2) p<.05
Days Stroke to 1st Assessment 15 (9) 875 (1012) ----- p<.01
Handedness (R/L/Ambi) 12/0/0 14/4/0 24/2/1 .25
Sex (M/F) 8/5 10/8 10/17 .26
Hemisphere (RHD/LHD/B) 7/6/0 4/12/2 ----- .13
Statistical Analysis: Hierarchical Linear Modeling (HLM)
Hierarchical linear modeling (HLM) was used to complete the recovery rate analyses
(Raudenbush & Bryk, 2002). HLM, also called multilevel linear modeling, is an alternative
statistical technique to repeated measures univariate Analysis of Variance (ANOVA), both of
which can be used in the analysis of longitudinal data. Statistical models are mathematical
representations of population behavior that are fitted to sample data, in order to obtain a
goodness-of-fit measure that quantifies the fit between the model and the data. If the fit is
good, then the model can be used to make inferences about the population. If we were to fit a
simple regression model for performance of a person on say a measure of gesture accuracy
over time, such as yd = π0 + π1 (t) + ε, we can say that performance of an individual on a
particular day (d) is predicted by the estimated performance for an individual at time 0 (π0),
(π1(t)) is the rate of change corresponding to one time unit and the residual (ε) is the
difference between the value predicted by the model and the actual value of the particular
patient. Regression models are designed, however, for single subjects and in group studies
we are not only interested in how each patient‟s performance changes over time, but also in
how these changes vary across individuals. In HLM terms, the level-1 submodel describes
how individuals change over time, while a Level-2 submodel describes how these changes

77
across time vary across individuals. Therefore, the level-1 submodel is also known as the
individual growth model, representing the change we expect each population member to
experience for the time period under study. The level-2 submodel describes the relationship
between the interindividual differences in the change trajectories and the time-invariant
characteristics (also called predictors) of the individual. So in our example of gesture
performance, the Level-1 submodel tells us how Patient i‟s performance changes over time,
based on his gesture performance across different time points. Patient i, may also be a patient
suffering from apraxia, while Patient j may not be suffering from apraxia. Therefore, in this
case we may wonder whether patients with apraxia will change differently than patients
without apraxia and thus we may add apraxia as a predictor. In other words, we ask the
question “Do patients with apraxia have different slopes of change over time than patients
without apraxia?” If the apraxia predictor of slope turns out to be significant, then we can say
that patients, who present with apraxia, have significantly different slopes of change in
gesture accuracy performance over time than patients without apraxia. The larger the value of
the slope of one group as compared to the other the more change there is.
As mentioned above, HLM is an alternative statistical technique to repeated measures
univariate ANOVA although both can be used in the analysis of longitudinal data. The
reason we chose HLM, as opposed to ANOVA, is that HLM has several benefits over
repeated measures. Group comparisons such as ANOVA require patients to have been
assessed at similar time points post stroke, which limits the application of the analysis. If
patients were assessed once in acute stage and a second time 3 months post stroke, the
findings from such a study can only be applied to recovery expectations between acute stage
and 3 months post stroke. In other words, we would not know what kind of recovery to

78
expect after 3 months post stroke. In our study, we have more than two data points in time,
allowing us to obtain a more reliable linear estimation of the expected recovery. In addition,
we could make predictions of how patients will perform in the future, even if we have no
data on future performance. In ANOVA, time is treated at fixed points, while in HLM time is
treated as a continuous variable.
Furthermore, HLM allows us to include patients who have been assessed different
numbers of times, something that cannot be done with ANOVA. Patients, who have not been
assessed at particular time points are usually excluded from the analysis in ANOVA. HLM
allows us to use all our data, not only select the first and second assessment of the patients. In
our study if we were to keep our sample size, we would have been able to use only the first
two assessments, given seventeen of our patients were assessed only twice.
Another great advantage of HLM is that it allows us to include patients who joined
the study at different time points post stroke. Thus, we have both acute-subacute and chronic
patients included in our sample, which allowed us to directly compare recovery rates between
these two groups of patients.
Finally, the time interval between assessments varied in our sample. In repeated
measures ANOVA, patients need to be reassessed at similar intervals, because the average
performance of all patients in the group is compared to the average initial performance of all
patients. In HLM, the intervals between patients can vary, because time is not a categorical
variable. This makes this statistical methodology much more applicable to real life, where
patients sometimes miss appointments or delay appointments for various reasons.
The outcome variables in our analysis were the eight tasks (Action Identification,
Tool Naming by Action, and Tool Naming, Pantomime, Pantomime by Picture, Concurrent

79
Imitation, Delayed Imitation and Object Use). A separate HLM was run for each outcome
variable.
The following Level-1 model was used to analyze the results in each of the HLM
analyses:
y = π0 + π1 (t) + ε
where, y was the percentage score in the outcome variable, π0 was the initial status at
Time 0 (the intercept), π1 was the rate of recovery, t was the square root of the number of
days since stroke (this transformation was done to approximate linearity in the curves and to
reduce the scale of days) and ε was the Level-1 residual.
The following Level-2 model was specified:
π0 = β00 + β 01 * (Chronicity Group) + β 02 * (Impairment Group) + β 03 * (Chronicity
x Impairment Group) + ξ0
π1 = β 10 + β 11 * (Chronicity Group) + β 12 * (Impairment Group) + β 13 * (Chronicity
x Impairment Group) + ξ 1
where, β 00 is the estimated mean initial percentage score across individuals, β01 *
(Chronicity Group) is the interaction between mean percentage initial score at time 0 and the
chronicity group effect (acute vs. chronic), β 02 * (Impairment Group) is the interaction
between mean percentage initial score and Impairment group (impaired versus not impaired
on first assessment), β 03 * (Chronicity x Impairment Group) is the interaction between the
mean percentage initial score and the interaction term between the two category variables
Chronicity group (Acute vs. Chronic) and Impairment group, and ξ 0 is the residual in the
intercept, β 10 is the average recovery rate (or the average slope of the performance across
time), β 11 * (Chronicity Group) is the interaction between recovery rate and chronicity

80
group, β 12 * (Impairment Group) is the interaction between recovery rate and Impairment
group, β 13 * (Chronicity x Apraxia Group) is the interaction between recovery rate and the
interaction term (Chronicity x Impairment Group) and ξ 1is the residual in slope.
Both the intercept and the slope were modeled as having randomly varying residuals
with the assumption that the intercept and slope vary not only as a function of the two group
factors and the interaction factor but also as a function of the individual. In addition, all
predictor variables were uncentered, so that when each of the two group factors (Chronicity
and Impairment) and the interaction factor (Chronicity x Impairment) were all equal to zero,
the model predicted performance score would produce the performance of an acute-subacute
patient without impairment on the task at time 0 (or the time of stroke). Dummy variables
were created for each of the two group categories: chronicity (patients coded 0 if acute-
subacute and 1 if chronic at their first assessment), impairment (coded 0 if not impaired at
first assessment and 1 if impaired).
RESULTS
The model-predicted rates of recovery for each task are presented in Figures 3.1 and
3.2. The model-predicted rates of recovery in these graphs are produced based on the model-
predicted parameters (intercept and slope) of each of the four subgroups of patients.
Appendix 3A contains the actual individual patient performances (measures in
percent accuracy) in each group (Acute-Subacute No Impairment, Chronic No Impairment,
Acute-Subacute Impairment and Chronic Impairment) per tasks across the square root of
time.

81
Figure 3.1: Model predicted rates of recovery for Action ID, Tool Naming by Action, Tool Naming and Pantomime
0
10
20
30
40
50
60
70
80
90
100
110
0 30 75 120
165
210
255
300
345
390
435
480
525
570
615
660
Days
Ac
tio
n ID
(%
)
0
10
20
30
40
50
60
70
80
90
100
110
30 75 120
165
210
255
300
345
390
435
480
525
570
615
660
Days
Ac
tio
n N
am
e (
%)
0
10
20
30
40
50
60
70
80
90
100
110
30 75 120
165
210
255
300
345
390
435
480
525
570
615
660
Days
To
ol N
am
e (
%)
0
10
20
30
40
50
60
70
80
90
100
110
30 75 120
165
210
255
300
345
390
435
480
525
570
615
660
Days
Pa
nto
mim
e (
%)
Chronic Not Impaired Acute-Subacute Not Impaired Chronic Impaired Acute-Subacute Impaired
Evidence of recovery was seen in all of the above tasks, but Action ID. In Action naming and Tool Naming, both acute-subacute
and chronic impaired patients recovered, while in pantomime, only acute-subacute patients showed significant recovery.

82
Figure 3.2: Model predicted rates of recovery for Pantomime by Picture, Object Use, Concurrent and Delayed Imitation
0
10
20
30
40
50
60
70
80
90
100
110
30 75 120
165
210
255
300
345
390
435
480
525
570
615
660
Days
Pa
nto
mim
e b
y P
ictu
re (
%)
0
10
20
30
40
50
60
70
80
90
100
110
30 75 120
165
210
255
300
345
390
435
480
525
570
615
660
Days
Ob
jec
t U
se
(%
)
0
10
20
30
40
50
60
70
80
90
100
110
30 75 120
165
210
255
300
345
390
435
480
525
570
615
660
Days
Co
nc
urr
en
t Im
ita
tio
n (
%)
0
10
20
30
40
50
60
70
80
90
100
110
30 75 120
165
210
255
300
345
390
435
480
525
570
615
660
Days
De
lay
ed
Im
ita
tio
n (
%)
Chronic Not Impaired Acute-Subacute Not Impaired Chronic Impaired Acute-Subacute Impaired
Evidence of recovery was seen in all of the above four tasks, with recovery being larger among acute-subacute patients in all of the
above tasks, but Object Use.

83
Action Identification, Tool Naming by Action and Tool Naming (Table 3.5)
A summary of the estimated values for the intercept and slope for each task and the
interaction coefficients representing the interaction between the fixed effects and the
intercept and slope for each of the three conceptual predicted models is presented in Table
3.5. As the table indicates, the mean predicted initial performance at Time 0 across all
participants was 100% for Action Identification, 97% for Tool Naming by Action and 101%
for Tool Naming (please note that this score is above 100%, because it is an estimated score
of average performance at Time 0, based on the patients‟ performance past that Time 0
point). The recovery was 0% for Action Identification, .03% for Tool Naming by Action and
-.1% for Tool Naming. Impairment group interacted significantly with initial performance,
showing impaired patients scored significantly lower than patients who were not impaired (as
expected as per definition) (On average 13.8% lower for Action Identification, 54.8% for
Tool Naming by Action and 52.8% for Tool Naming). The Chronicity x Impairment
interaction terms were not significant and neither was the Chronicity factor suggesting that
chronic and acute-subacute patients did not differ significantly in their initial performance in
any of the tasks. In Action identification, none of the interactions between the fixed effects
and the slope were significant, i.e. the patients‟ scores did not change significantly over time.
In the two naming tasks, the interactions between Chronicity and Chronicty x
Impairment were not significant. However, the interactions between Impairment group and
the slope intercept were significant in Tool Naming (p<.05) and in Tool Naming by Action it
was right at the limit (p=.05), suggesting significantly steeper recovery rates in the impaired
groups.

84
Table 3.5: Estimates of Fixed Effects for Action identification, Tool Naming by Action and Tool Naming
Action ID Tool Naming by Action Tool Naming
Standard
Coef. T-ratio df
p-
value
Standard
Coef. T-ratio df
p-
value
Standard
Coef. T-ratio df
p-
value
Intercept β00 100 42.04 22 p<.001 97.22 39.42 26 p<.001 101.17 117.58 27 p<.001
Intercept * Chronicity, β 01 3.52 0.92 22 0.37 -5.87 -1.30 26 0.21 1.58 0.60 27 0.56
Intercept * Impairment, β 02 -13.81 -3.90 22 p<.001 -54.78 -5.17 26 p<.001 -52.80 -5.14 27 p<.001
Intercept * Chronicity *
Impairment, β 03 -7.92 -0.95 22 0.35 -12.25 -0.55 26 0.58 21.05 1.75 27 0.09
Slope, βa0 0.00 0.00 22 1.00 0.03 1.26 26 0.22 -0.09 -1.52 27 0.14
Slope * Chronicity, β 11 -0.18 -0.74 22 0.47 0.11 0.84 26 0.41 -0.04 -0.34 27 0.73
Slope * Impairment, β 12 -0.05 -0.18 22 0.86 0.95 2.05 26 p<.05 0.94 2.69 27 p<.01
Slope * Chronicity *
Impairment, β 03 0.49 1.25 22 0.23 -0.09 -0.09 26 0.93 -0.62 -1.36 27 0.19

85
Pantomime to Verbal Command, Pantomime by Picture and Object Use
A summary of the estimated values for the intercept and slope for each task and the
interaction coefficients representing the interaction between the fixed effects and the
intercept and slope for each of the three conceptual predicted models is presented in Table
3.5. As the table indicates, the average percentage performance score at Time 0 as predicted
by the model was 92.5% for Pantomime to Verbal Command, 93.4% for Pantomime by
Picture and 95.6% for Object use. Patients were recovering at a rate of -0.1 per unit of time in
both pantomime task modalities and 0.08% in Object use. A significant interaction between
the intercept and Impairment group, indicated that impaired patients had lower initial scores
than not impaired patients (on average 45.5% lower in Pantomime to Verbal Command,
46.8% in Pantomime by Picture and 24.8 in Object use). The interaction between the
Chronicity x Impairment factor for the intercept was also significant in the two pantomime
tasks, suggesting that impaired chronic patients scored significantly higher than acute-
subacute impaired patients on their first assessment (35.6% higher for Pantomime to Verbal
Command (p<.01) and 34.4% higher for Pantomime by Picture (p<.01). In Object Use, there
was no significant interaction with the Chronicity x Impairment interaction factor, suggesting
no significant difference between chronic and acute-subacute patients at Time 0.
For all three tasks, impairment group interacted significantly with the slope (i.e. the
rate of recovery), with impaired patients showing a steeper rate of recovery than patients who
were not initially impaired on the task. In the two pantomime tasks, but not Object Use, the
rate of recovery was also affected by an interaction with the Chronicity x Impairment factor,
showing that chronic apraxia patients‟ recovery slope was significantly flatter than that of
acute apraxia patients. In Object Use, this difference was not statistically significant.

86
Table 3.6: Estimates of Fixed Effects for Pantomime, Pantomime by Picture and Object Use.
Pantomime Pantomime by Picture Object use
Standard
Coef.
T-
ratio df
p-
value
Standard
Coef. T-ratio df
p-
value
Standard
Coef.
T-
ratio df
p-
value
Intercept β00 92.49 91.45 27 p<.001 93.43 57.10 27 p<.001 95.65 82.70 27 p<.001
Intercept * Chronicity, β 01 0.23 0.07 27 0.94 -1.29 -0.49 27 0.63 1.51 0.37 27 0.71
Intercept * Impairment, β 02 -45.47 -4.08 27 p<.001 -46.80 -4.30 27 p<.001 -24.82 -3.31 27 p<.001
Intercept * Chronicity *
Impairment, β 03 35.63 2.90 27 p<.01 34.41 2.97 27 p<.01 15.90 1.84 27 0.08
Slope, βa0 -0.09 -1.86 27 0.07 -0.10 -1.61 27 0.12 -0.08 -3.06 27 p<.01
Slope * Chronicity, β 11 0.06 0.54 27 0.59 0.07 0.78 27 0.44 -0.06 -0.51 27 0.62
Slope * Impairment, β 12 1.22 2.94 27 p<.01 1.30 5.89 27 p<.001 0.57 2.47 27 p<.05
Slope * Chronicity *
Impairment, β 03 -1.19 -2.65 27 p<.01 -1.24 -4.70 27 p<.001 -0.44 -1.66 27 0.11

87
Concurrent Imitation and Delayed Imitation
A summary of the estimated values for the intercept and slope for each task and the
interaction coefficients representing the interaction between the fixed effects and the
intercept and slope for each of the three conceptual predicted models is presented in Table
3.7. As the table indicates, the estimated mean performances at Time 0 for Concurrent
Imitation and Delayed Imitation were 98% and 99% and the mean recovery rate was-
0.1%.for both tasks. A significant interaction between impairment group and gesture
performance (p<.001) indicated that in concurrent and delayed imitation impaired patients
scored 23% lower in both tasks initially. The interaction between task performance and
Chronicity group were not significant in either task, however, the Chronicity x Impairment
term reached significance in Concurrent Imitation (p<.01), suggesting that chronic impaired
patients‟ level of performance was 14% higher initially than acute-subacute impaired
patients. The slope intercepts were significant in both groups, and so were the interactions
between Impairment group and the Chronicity x Impairment factor, suggesting that there was
evidence for recovery only in the acute impaired group (at a rate of 0.4% per unit of time in
both tasks), whereas the rate of recovery in chronic impaired patients was negligible 0.03%
in Concurrent Imitation and 0.02% in Delayed Imitation).

88
Table 3.7: Estimates of Fixed Effects for Delayed and Concurrent Imitation.
Concurrent Imitation Delayed Imitation
Standard
Coef T-ratio df p-value
Standard
Coef T-ratio df p-value
Intercept β00 97.91 119.83 27 p<.001 98.99 259.76 27 p<.001
Intercept x Chronicity, β
01 -0.48 -0.34 27 0.74 -1.01 -0.87 27 0.39
Intercept x Impairment, β
02 -23.20 -4.44 27 p<.001 -22.69 -3.93 27 p<.001
Intercept x Chronicity x
Impairment, β 03 14.19 2.38 27 p<.05 12.26 1.72 27 0.10
Slope, βa0 -0.07 -4.94 27 p<.001 -0.10 -7.15 27 p<.001
Slope x Chronicity, β 11 0.04 0.92 27 0.36 0.02 0.68 27 0.50
Slope x Impairment, β 12 0.46 3.65 27 p<.001 0.47 3.52 27 p<.001
Slope x Chronicity x
Impairment, β 03 -0.41 -2.87 27 p<.01 -0.37 -2.51 27 p<.05
Variance Components
The estimates of the variances for the intercept and slope for each task are listed in
Table 3.8. The intercept variance (ξ0) indicates how variable people are in their Time 0 score
within their group. The slope variance (ξ1) indicates how variable people are in their rate of
change within their group. Finally, the error term (ε) indicates the variance of performance
within person around the predicted growth curve. The standard deviation for both the
intercept and slope for each task are listed in Table 3.8 Chi-square tests were run to
determine the significance of each variance component. The variance components were
significant for both intercept and slope for Tool Naming by Action, Tool Naming,
Pantomime and Object Use suggesting that patients varied significantly in their intercepts
and slopes within their groups. The variance component in Pantomime, Concurrent Imitation
and Delayed Imitation were only significant for the intercepts, but not the slopes. Finally, in
action identification, only the variance component for slope was significant.

89
Table 3.8: Estimated Variance Components (VC) for all tasks.
SD VC df
Chi-
square
p-
value SD VC df
Chi-
square
p-
value
Action ID Action Naming
Intercept1, ξ0 0.61 0.37 17 13.73 >.500 19.11 365.30 25 82.06 0.00
√Days slope, ξ 1 0.24 0.06 17 37.74 0.00 0.53 0.28 25 45.68 0.01
level-1, ε 4.75 22.59 7.64 58.43
Tool Naming Pantomime
Intercept1, ξ0 20.46 418.49 25 67.07 0.00 16.90 285.76 24 63.29 0.00
√Days slope, ξ 1 0.60 0.36 25 41.14 0.02 0.55 0.31 24 43.19 0.01
level-1, ε 9.32 86.77 7.54 56.87
Pantomime by Picture Object use
Intercept1, ξ0 17.97 322.96 24 52.88 0.00 12.89 166.09 24 136.47 0.00
√Days slope, ξ 1 0.34 0.11 24 23.06 >.500 0.39 0.16 24 76.98 0.00
level-1, ε 5.57 31.07 4.36 19.04
Concurrent Imitation Delayed Imitation
Intercept1, ξ0 7.82 61.08 22 51.85 0.00 11.14 124.10 24 83.23 0.00
√Days slope, ξ 1 0.14 0.02 22 33.70 0.05 0.15 0.02 24 35.98 0.06
level-1, ε 5.12 26.22 5.29 27.99
Patterns of Deficits Analysis
In order to examine the performance of patients on an individual basis, rather than the
group analysis approach taken in the HLM study, we looked at the combined performance of
patients on several tasks in order to determine a pattern of deficits that they presented with.
According to Roy (1996), there are eight patterns of deficits that are predicted, based on
which praxis system is affected (See Table 3.1). The patterns are determined based on the
performance on three Gesture production Tasks (Pantomime to Verbal Command, Delayed
Imitation, Concurrent Imitation) and a composite Action Recognition Score (Tool Naming by
Action and Action Identification). Patients were considered impaired on the Action
Recognition Score only if they were impaired on both Tool Naming by Action and Action
Identification. The goal in this analysis was to see how each of the patterns evolves over
time.

90
Only 22 of the patients had enough data to be classified to one of the pre-defined
patterns by Roy (1996). Patients were included if they had at least two assessments where the
pattern of deficits could be defined. See the summary in Table 3.9. Five of the 22 patients
showed no initial deficits in any of the pattern defining tasks. The other 17 patients all
showed deficits on at least one of the four pattern defining tasks (Pantomime, Delayed
Imitation, Concurrent Imitation or Gesture Identification). Among the patients with no initial
impairment, three patients deteriorated, while two patients remained not impaired. Among
the patients who deteriorated, patients‟ accuracy decreased in either pantomime, one of the
two imitation tasks, or in some cases both pantomime and imitation together. Among the
patients who showed some deficits initially, 9 patients (2 acute-subacute and 7 chronic)
improved (their performance shifted to unimpaired ranges with one or more of the tasks,
while the rest of the task remained the same); 3 patients (1 acute-subacute and 2 chronic)
changed performance (their performance on some tasks improved while that in others
changed for the worse); 3 patients (2 acute-subcute, 1 chronic) remained within the same
pattern; 2 patients (2 chronic) deteriorated in performance (shifting to impaired ranges in
tasks they were not impaired initially).

91
Table 3.9: Pattern Evolutions
Evolution Action Name Action ID P DI CI ID.
ID # Gr. Side Pattern Z Z Z Z Z
54 1 A-S LHD N/A Same -12.1 I --- -12.4 I -16.5 I -13.1 I ---
54 2 A-S LHD Global (P-/DI-/CI-/ID-) -12.1 I -6.6 I -9.4 I -8.4 I -9.0 I I
54 3 A-S LHD Global (P-/DI-/CI-/ID-) -7.4 I -8.8 I -5.5 I -9.9 I -7.4 I I
54 4 A-S LHD Global (P-/DI-/CI-/ID-) -11.3 I -6.6 I -4.0 I -4.0 I -5.8 I I
54 5 A-S LHD N/A --- -13.5 I -1.9 NI -5.4 I -7.4 I ---
120 1 A-S LHD Global (P-/DI-/CI-/ID-) Improve -7.4 I -3.1 I -13.3 I -10.6 I -13.1 I I
120 2 A-S LHD Production Ideomotor (P-/DI-/CI-/ID+) 0.6 NI -3.1 I -3.7 I -6.2 I -5.8 I NI
120 3 A-S LHD Production Conduction (P+/DI-/CI-/ID+) 0.6 NI 0.4 NI -1.3 NI -4.7 I -5.0 I NI
28 1 A-S RHD No Impairment Worse -1.0 NI -2.7 I -1.3 NI -0.3 NI -0.2 NI NI
28 2 A-S RHD No Impairment -1.0 NI 0.4 NI -1.9 NI -0.3 NI -1.0 NI NI
28 3 A-S RHD Production Ideomotor (P-/DI-/CI-/ID+) -1.0 NI 0.4 NI -2.5 I -3.2 I -3.4 I NI
28 4 A-S RHD Production Working M. (P-/DI-/CI+/ID+) 0.6 NI 0.4 NI -2.8 I -5.4 I -1.8 NI NI
57 1 A-S RHD Production Conduction (P+/DI-/CI-/ID+) Same 0.6 NI --- -1.6 NI -4.7 I -8.2 I NI
57 2 A-S RHD Production Conduction (P+/DI-/CI-/ID+) 0.6 NI 0.4 NI 0.2 NI -4.0 I -3.4 I NI
57 3 A-S RHD Production Ideomotor (P-/DI-/CI-/ID+) 0.6 NI 0.4 NI -2.5 I -4.0 I -3.4 I NI
57 4 A-S RHD Production Conduction (P+/DI-/CI-/ID+) 0.6 NI --- -0.4 NI -4.7 I -6.6 I NI
57 5 A-S RHD Production Conduction (P+/DI-/CI-/ID+) 0.6 NI 0.4 NI -0.4 NI -3.2 I -4.2 I NI
66 1 A-S RHD Production Encoding (P+/DI-/CI+/ID+) Change -2.6 I 0.4 NI -0.4 NI -3.2 I -1.0 NI NI
66 2 A-S RHD P+/DI+/CI-/ID+ 0.6 NI 0.4 NI -0.7 NI -1.0 NI -4.2 I NI
121 1 A-S RHD Production Ideomotor (P-/DI-/CI-/ID+) Improve 0.6 NI -3.1 I -4.6 I -3.2 I -6.6 I NI
121 2 A-S RHD Production Ideomotor (P-/DI-/CI-/ID+) 0.6 NI --- -2.2 I -4.0 I -3.4 I NI
121 3 A-S RHD P-/DI+/CI-/ID+ 0.6 NI --- -3.4 I -1.8 NI -3.4 I NI
172 1 A-S RHD No Impairment Same 0.6 NI 0.4 NI 0.5 NI 1.2 NI 0.6 NI NI
172 2 A-S RHD No Impairment 0.6 NI 0.4 NI -0.7 NI 0.3 NI 1.5 NI NI
C=Chronic; A= Acute-Subacute; P=Pantomime, DI=Delayed Imitation, CI=Concurrent Imitation, ID=Action Recognition, I=Impaired, NI=Not Impaired

92
117 1 C BHD Production Resp Selection (P-/DI+/CI+/ID+) Improve -1.0 NI 0.4 NI -2.0 I -1.8 NI 0.6 NI NI
117 2 C BHD 0.00 = "No Impairment 0.6 NI 0.4 NI -0.2 NI -1.4 NI 0.2 NI NI
139 1 C BHD Production Ideomotor (P-/DI-/CI-/ID+) Improve -1.0 NI 0.4 NI -2.6 I -3.6 I -3.8 I NI
139 2 C BHD Production Conduction (P+/DI-/CI-/ID+) 0.6 NI --- 0.1 NI -2.1 I -3.0 I NI
37 1 C LHD N/A 0.6 NI --- --- --- --- NI
37 2 C LHD Production Ideomotor (P-/DI-/CI-/ID+) Same -1.0 NI 0.4 NI -5.5 I -8.4 I -15.5 I NI
37 3 C LHD Production Conduction (P+/DI-/CI-/ID+) 0.6 NI -1.4 NI -1.3 NI -17.2 I -13.9 I NI
37 4 C LHD Production Ideomotor (P-/DI-/CI-/ID+) -1.0 NI -3.1 I -3.1 I -14.3 I -5.0 I NI
37 5 C LHD Production Ideomotor (P-/DI-/CI-/ID+) 0.6 NI -6.6 I -6.4 I -5.4 I -8.2 I NI
42 1 C LHD N/A 0.6 NI --- 0.2 NI -2.2 I --- NI
42 2 C LHD P-/DI+/CI-/ID+ Improve 0.6 NI 0.4 NI -2.5 I -1.0 NI -6.6 I NI
42 3 C LHD No Impairment 0.6 NI 0.4 NI -0.7 NI -1.0 NI 0.6 NI NI
42 4 C LHD No Impairment 0.6 NI 0.4 NI -0.1 NI -1.0 NI -1.8 NI NI
50 1 C LHD Production Ideomotor (P-/DI-/CI-/ID+) Improve 0.6 NI 0.4 NI -4.6 I -2.5 I -5.0 I NI
50 2 C LHD Production Ideomotor (P-/DI-/CI-/ID+) -1.0 NI 0.4 NI -5.2 I -8.4 I -5.0 I NI
50 3 C LHD Production Encoding (P+/DI-/CI+/ID+) -1.0 NI --- -0.4 NI -7.7 I -1.0 NI NI
53 1 C LHD No Impairment Worse 0.6 NI 0.4 NI 0.8 NI -0.3 NI -1.8 NI NI
53 2 C LHD Production Conduction (P+/DI-/CI-/ID+) 0.6 NI --- 0.2 NI -2.5 I -3.4 I NI
53 3 C LHD Production Encoding (P+/DI-/CI+/ID+) 0.6 NI 0.4 NI -1.3 NI -3.2 I -0.2 NI NI
63 1 C LHD Production Ideomotor (P-/DI-/CI-/ID+) Worse --- -0.3 NI -5.8 I -13.5 I -10.6 I NI
63 2 C LHD Global (P-/DI-/CI-/ID-) -12.1 I -3.1 I -4.9 I -12.8 I -3.4 I I
63 3 C LHD Global (P-/DI-/CI-/ID-) -12.1 I -6.6 I -4.9 I -13.5 I -3.4 I I
63 4 C LHD Global (P-/DI-/CI-/ID-) -12.1 I -6.6 I -8.8 I -9.1 I -5.8 I I
63 5 C LHD 8.00 = "Global (P-/DI-/CI-/ID-)" -12.1 I -3.1 I -7.3 I -6.9 I -6.6 I I
C=Chronic; A= Acute-Subacute; P=Pantomime, DI=Delayed Imitation, CI=Concurrent Imitation, ID=Action Recognition, I=Impaired, NI=Not Impaired

93
64 1 C LHD No Impairment Worse -1.0 NI 0.4 NI -1.0 NI -1.0 NI -1.0 NI NI
64 2 C LHD Production Conduction (P+/DI-/CI-/ID+) 0.6 NI 0.4 NI -1.9 NI -5.4 I -7.4 I NI
64 3 C LHD No Impairment 0.6 NI 0.4 NI -0.4 NI 0.4 NI -1.0 NI NI
64 4 C LHD N/A -1.0 NI 0.4 NI -1.6 NI --- -1.8 NI NI
64 5 C LHD Production Conduction (P+/DI-/CI-/ID+) -1.0 NI 0.4 NI -1.0 NI -3.2 I -3.4 I NI
80 1 C LHD Global (P-/DI-/CI-/ID-) Change -5.8 I -3.1 I -2.5 I -7.7 I -7.4 I I
80 2 C LHD P+/DI+/CI+/ID- -2.6 I -3.1 I -1.0 NI -1.0 NI -1.0 NI I
80 3 C LHD Production Encoding (P+/DI-/CI+/ID+) -1.0 NI 0.4 NI -0.4 NI -4.0 I -0.2 NI NI
86 1 C LHD P-/DI+/CI-/ID+ Worse -1.0 NI 0.4 NI -4.0 I -1.8 NI -5.8 I NI
86 2 C LHD Production Ideomotor (P-/DI-/CI-/ID+) 0.6 NI 0.4 NI -3.7 I -6.9 I -4.2 I NI
129 1 C LHD Production Encoding (P+/DI-/CI+/ID+) Improve -1.0 NI 0.4 NI -1.3 NI -2.5 I -1.3 NI NI
129 2 C LHD No Impairment 0.6 NI 0.4 NI 0.5 NI -0.5 NI 0.6 NI NI
129 3 C LHD No Impairment 0.6 NI 0.4 NI 1.1 NI 0.4 NI 0.6 NI NI
138 1 C LHD Production Resp Selection (P-/DI+/CI+/ID+) Change 0.6 NI 0.4 NI -5.5 I 0.4 NI -1.0 NI NI
138 2 C LHD No Impairment -1.0 NI -3.1 I 0.2 NI -1.8 NI -1.0 NI NI
112 1 C RHD Production Ideomotor (P-/DI-/CI-/ID+) Improve -1.0 NI -3.1 I -3.4 I -10.6 I -13.9 I NI
112 2 C RHD Production Working M. (P-/DI-/CI+/ID+) -1.0 NI 0.4 NI -3.1 I -5.4 I -1.8 NI NI
112 3 C RHD Production Conduction (P+/DI-/CI-/ID+) 0.6 NI -3.1 I -1.3 NI -7.2 I -5.0 I NI
114 1 C RHD No Impairment Same 0.6 NI 0.4 NI -1.3 NI -0.3 NI -1.0 NI NI
114 2 C RHD No Impairment 0.6 NI 0.4 NI -1.3 NI -1.8 NI -0.2 NI NI
140 1 C RHD Production Ideomotor (P-/DI-/CI-/ID+) Improve -1.0 NI -3.1 I -2.2 I -4.0 I -5.0 I NI
140 2 C RHD Production Conduction (P+/DI-/CI-/ID+) 0.6 NI -3.1 I -1.6 NI -5.4 I -5.8 I NI
C=Chronic; A= Acute-Subacute; P=Pantomime, DI=Delayed Imitation, CI=Concurrent Imitation, ID=Action Recognition, I=Impaired, NI=Not Impaired

94
DISCUSSION
The main goal of the study was to examine whether patients improve spontaneously
in their performance on a number of apraxia tasks after stroke. In addition, we aimed to
determine if the recovery rate differs between acute-subacute and chronic stroke patients.
Overall, tasks were generally grouped into two categories: tasks assessing conceptual
knowledge of actions and tools and tasks assessing gesture production abilities.
Among the conceptual tasks, the only task modality that did not show evidence of
gains in performance scores over time was Action Identification. The two naming tasks, Tool
Naming by Action and Tool Naming, both showed significant gains over time in both acute-
subacute and chronic stroke patients.
Among the gesture production tasks, as expected (based on the nature of the grouping
of impaired versus not impaired patients), impaired patients obtained on average lower initial
scores than patients without impairment. Also, as predicted, chronic impaired patients
obtained, on average, higher initial scores than acute impaired patients in all gesture
production task modalities. This difference was statistically significant on all tasks except in
Object Use and Delayed Imitation, where chronic impaired patients obtained still higher
scores than acute-subacute impaired patients, but the difference was not statistically
significant. Patients showed higher gains in performance score over time if they were
impaired initially, suggesting spontaneous recovery occurred in patients who show initial
deficits. In addition, chronic patients had significantly lower rates of recovery than acute-
subacute patients in all gesture production task modalities, except Object Use.
There are three main advantages in terms of the methodological approach we have
undertaken. First, we included patients with left, right and bilateral hemisphere stroke,

95
making ours the first study that did not limit itself by including only LHD stroke patients.
Including both right, left and bilateral hemisphere patients makes our study more
generalizable. It would have been interesting to study whether the recovery patterns of left
versus right patients differ, but unfortunately we did not have enough cases in each group to
make a meaningful comparison.
Second, we included both acute-subacute and chronic patients and compared their
rate of recovery. The inclusion of both acute-subacute and chronic stroke patients makes our
contribution to recovery studies unique. Most previous studies performed the first assessment
in the acute stages (Cimino-Knight et al., 2002; Foundas et al., 1993; Basso et al., 1987;
Basso et al., 2000). While acute patients are best to capture the steep recovery rate expected
in the first 3 months post-stroke (Foundas et al., 1993), including chronic patients, allowed us
to assess recovery in more chronic stages of stroke recovery. Our study showed that chronic
patients show smaller gains in performance over time than acute-subacute patients in all tasks
but Object Use. Finally, our study is the most comprehensive with respect to the variety of
praxis tasks examined.
Third, we used a model-based approach to select the tasks included in the study, so
that both gesture production and action and tool knowledge could be followed over time. To
our knowledge, at least in studies examining recovery of apraxia deficits, our study is the
first to include various tasks of conceptual gesture and tool knowledge. We found that there
was no evidence of recovery in Action Identification, while performance on Action and Tool
Naming showed significant gains. The recovery gains in the two naming tasks did not differ
between chronic and acute-subacute patients with impairment. It is likely that the recovery in
the naming tasks reflected recovery in language production as opposed to recovery in the

96
ability to identify gestures. This is supported by the fact that both acute-subacute and chronic
patients who were impaired in Action Identification scored above 80% initially, while acute
and chronic patients impaired on Tool Naming by Action scored 42% and 24% initially;
therefore, the initial level of impairment in naming was significantly more severe than that in
action identification. This more severe impairment may be due to the fact that an inability to
name an action can be due to both an aphasia deficit and a conceptual gesture identification
deficit, while in Action Identification a deficit in conceptual gesture identification mainly
accounts for the lower score. Thus if patients recover their naming ability but not their
gesture identification, we would expect significant recovery gains in patients with
impairment in Tool Naming by Action, even if Action Identification deficits remain the
same. This is consistent with past studies showing anomia (the inability to name objects, for
example) often recovers after stroke (Kertesz, 1984) This would have to be supported with
studies looking at recovery in both aphasia and apraxia. Unfortunately, detailed aphasia
assessments were not available for the current sample of patients to examine this question.
In the two pantomime tasks, the study demonstrated evidence for recovery in
impaired patients, more so in acute-subacute than chronic patients. Acute-subacute patients
were also more severely affected, obtaining lower initial scores than chronic patients. Only
one published paper (Mimura, Fitzpatrick, & Albert, 1996) and two published abstracts
(Foundas et al., 1993; Cimino-Knight et al., 2002) have reported research on spontaneous
recovery of pantomime performance after stroke. Mimura and colleagues (1996) showed
significant recovery in chronic stroke patients (first examination at 4.5 months post-stroke
and second examination on average 82 months post-stroke). Our study suggests that, while
chronic patients continue to show some gains in performance over time that could possibly

97
lead to significant recovery gains if compared over long periods (periods comparable in
duration in those in Mimura et al.s study), the average gains over time are much smaller
compared to the average gains of acute-subacute impaired patients. This is consistent with
Foundas et al (1993) findings that the greatest recovery post-stroke occurs over the first three
months post-stroke.
The analysis of the data from concurrent imitation showed the same findings as those
in the pantomime tasks. On concurrent imitation, chronic impaired patients started out with a
significantly higher performance (on average 14% higher) than acute-subacute impaired
patients. In addition, the gain in scores over time was higher in acute-subacute impaired
patients, suggesting that most recovery occurs over the first 3 months. On delayed imitation
chronic and acute-subacute patients impaired on imitation did not significantly differ in
initial performance on the task, but acute-subacute patients still showed better recovery gains
over time.
Three studies in the past have examined imitation recovery in stroke patients. Two of
these studies administered the De Renzi‟s Imitation test, which requires patients to perform
gestures immediately after presentation, so this type of imitation is similar to our delayed
imitation task (Basso et al., 1987; Basso et al., 2000). In their first study, Basso and
colleagues showed that patients recover more between their first and second examination
(first was done 15-30 days post stroke and second around 8 months post stroke) than between
their second and third (third examination was years after the second). This finding suggests
that recovery post stroke slows down the further away the patient is from the stroke event.
This was later confirmed by another study examining long-term recovery post stroke,
showing that patients did not improve significantly between 9.4 to 28 months post stroke.

98
Our study supports their findings, but suggests that chronic patients continue to show small
gains in performance accuracy.
Mimura et al. (1996) also looked at imitation recovery among their chronic sample of
patients (initial examination at 4.5 months reexamined 83 months later). Regardless of the
late stage of initial assessment of these patients, significant improvements were observed.
This is somewhat in contradiction to our findings of little to no recovery in chronic impaired
patients. Differences may arise because of the gesture types used, as well as the
administration of the tasks. In their study, patients were asked to imitate both transitive and
intransitive gestures, and it seems patients were also provided a verbal cue in addition to
demonstrating the gesture visually and, thus, it is unclear whether patients were following the
visual presentation or if they were following the verbal cue. Also, their results were based on
both transitive and intransitive gestures, while ours are based only on transitive gestures,
making comparisons difficult.
Finally, on Object Use, impaired patients showed greater gains over time relative to
patients without impairment, suggesting patients recovered. Here, however, acute-subacute
and chronic impaired patients did not have significantly different recovery slopes. While it is
tempting to conclude that acute-subacute or chronic impaired patients recover at similar rates
in the Object Use task, we believe the lack of significance may be due to power and not to
lack of differences. Our acute-subacute impaired group starts off at 71% and recovers at a
rate of .52%, while our chronic impaired patients start off at 88% and recovers at a rate of
0.02% per unit of time. Clearly, even in Object Use, the recovery gains in chronic patients
are small and patients seem to have already achieved some recovery, as evident by the higher
initial scores in performance relative to the acute-subacute impaired patients. No studies to

99
date have examined the recovery of the ability to perform gestures when holding the actual
tool as is required in the Object Use task. It is possible that differences between the groups do
not reach significance due to high variability among scores, which in part could be due to
patients continuing to use actual objects in everyday life and thus practicing the task through
everyday activities, a situation not likely with pantomime and imitation.
Last but not least, our secondary objective was to describe the patterns of limb
apraxia deficits in stroke and their evolution. First, Roy (1996) predicted eight patterns of
performance that are likely to occur as a result of stroke. In the current study, however, we
observed some additional patterns, not anticipated in the Roy model. First, three different
patients presented with deficits in pantomime and concurrent imitation, but not in delayed
imitation. Second, we had one case where a patient had a selective deficit in action
identification. Finally, we had one case with a pattern showing selective impairment in
concurrent imitation. In some of these cases these were patterns of performance seen on
initial assessments and in others they were patterns seen at the final assessment.
Roy (1996) did not propose any patterns of deficits where patients can imitate with a
delay but not concurrently, because during concurrent imitation patients are not required to
encode the information into working memory but rather can imitate through direct
visuomotor transformations. Thus, patterns where both pantomime and concurrent imitation,
but not delayed imitation, are impaired, or patterns where only concurrent imitation is
impaired were not anticipated. The fact that we had cases presenting such patterns indicated
that concurrent imitation may be impaired without delayed imitation being impaired. We
now believe that such cases may be possible because concurrent imitation may be a task
where working memory resources are more demanding, because patients are in effect

100
performing a dual-task: they are processing visual information, while at the same time
producing an action. In delayed imitation, on the other hand, an action is observed first, then
encoded into working memory and finally this information is used to produce an action.
Dual-tasks have been shown to be impaired in stroke patients(Marshall, Grinnell, Heisel,
Newall, & Hunt, 1997), which could explain the selective deficit in concurrent imitation in
some stroke patients.
Finally, a case where only Action Identification is impaired was also not proposed
because according to Roy‟s model inability to recognize gestures, must be due either to an
inability to process visual information or a loss of conceptual knowledge. If there is a deficit
in processing visual information, the patient should also be unable to imitate; in the case of
deficits in the conceptual system, a person should be unable to pantomime. Here, however,
we had a case where all gesture production was intact and only gesture recognition was
impaired. This is similar to two patients described by (Rothi, Mack, & Heilman, 1986) who
were not able to recognize gestures but able to imitate and pantomime. They termed this
“pantomime agnosia”. According to these authors, patients with pantomime agnosia must
have disconnected visual input from the „input praxicon”. Unlike, Roy‟s model, Rothi and
Heilman‟s model of apraxia suggest that there are two independent sets of conceptual
representation, one for processing gestural input (input praxicon) and one for processing
gestural output (output praxicon). Thus, if only the representations responsible for processing
visual gestural input are damaged, then patients may not be able to visually recognize
gestures but may still be able to pantomime and imitate gestures (Heilman & Rothi, 1993)
Given the wide number of presented patterns and the small number of patients, it is
hard to draw any concrete conclusions with respect to how patterns change over time. Two

101
notable observations were made, however: 1. The largest number of patients (9 out of 15)
showed pattern changes showing improvements over time, with patients shifting from
impaired to non-impaired ranges, as was predicted by us, given the significant recovery
observed in patients through the HLM analysis. Three patients remained the same and only
three patients changed in ways that theoretically did not make sense (e.g. moving from a non-
impaired range to impaired range on some tasks while improving on others) and only two
cases deteriorated in performance. Deterioration in performance is surprising and suggests
that there may have been some underlying cognitive decline due to ongoing undiagnosed
diseases of neurodegenerative or vascular nature. 2. It is important to note that 7 out of the 9
patients who improved were chronic patients. Therefore, even though groupwise it may seem
that chronic patients recover little, it is possible for them to move from impaired to
nonimpaired performance.
Finally, the between person, within group variance of the scores at Time 0 were
significant for all tasks, but Action Identification. Overall, less variability is expected in tasks
on which the patients are performing better. Given that Action Identification was the task
performed with most accuracy by all four groups of patients, it is not surprising that this is
the case. The large variability in patient scores also suggests individual variability in the
ability to perform gestures. The participants in our study were patients with various lesion
locations. As with any neurological deficit, apraxia is more likely to result after damage to
specific brain areas (such as the left middle frontal gyrus, the left superior and inferior
parietal cortical areas) (Haaland, Harrington, & Knight, 2000). Therefore, depending on the
site of the lesion and the extent to which these brain areas are affected, patients will be

102
affected to different extents, which in turn would result in variability in performance from
patient to patient.
It should also be noted that, the between person, within group, variance of slopes was
significant among individuals as indicated by significant chi-square test of the variance
components of the slope. The only tasks where the slopes of patients did not vary to a
statistically significant degree were Pantomime by Picture and the two imitation tasks. Large
variability in recovery rates has been reported in past studies examining cognitive recovery
(Ballard, Rowan, Stephens, Kalaria, & Kenny, 2003) and specifically in aphasia (Lazar,
Speizer, Festa, Krakauer, & Marshall, 2008). Differences in recovery rates may be influenced
by lesion sites, but it should be kept in mind that patients with the same lesions often may not
show the same recovery patterns, so other variables surely play a role in this recovery, for
example, the age of the patient, the extent of the entire lesion, the gender and ethnicity, are
just a few factors that have been shown to influence recovery post stroke and hence may lead
to variable recovery rates among individual patients (Nicholas, 2005).
The lack of recovery seen in Action Identification and the evidence of such recovery
in gesture production tasks also supports the notion that the two systems are distinct and
function independently of one another. This was observed by Cimino-Knight‟s study as well
(Cimino-Knight et al., 2002) and our study supports their findings.
Overall, the following general findings can be summarized from our study. First,
Action identification was the only task, where patients with deficits did not improve over
time. Second, in the other two conceptual tasks, Tool Naming by Action and Tool Naming,
which depend on language ability, both acute-subacute and chronic patients recovered. Third,
in gesture production tasks, acute-subacute patients with deficits in pantomime and imitation

103
showed significantly higher gains in performance over time than chronic patients. Thus,
patients assessed within 3 months post stroke showed the highest gains. Finally, object use
was the only gesture production task where both chronic and acute-subacute patients did not
significantly differ in recovery rate.
Future studies should aim at examining recovery rates and correlate these rates with
specific lesion sites. Unfortunately, while it is beneficial that we included both right, left and
bilateral hemisphere stroke patients, making out findings generalizable to both these groups
of patients, due to sample size we could not compare right versus left hemisphere differences
in recovery patterns. Thus, future studies should compare the recovery patterns in left vs.
right hemisphere damaged patients, as well as examine other factors affecting recovery, as
noted above. Finally, future studies should be extended to examining gesture production of
intransitive and meaningless gestures after stroke.

104
APPENDIX 3A: INDIVIDUAL PATIENT PERFORMANCES

105
Figure 3A.1: Individual Patient Performances in Action Identification for each group. The solid dark line in each graph represents
the model- predicted slope for the group in question.
LHD=Left Hemisphere Damage; RHD=Right Hemisphere Damage; ID=Patient Identification Number

106
Figure 3A.2: Individual Patient Performances in Tool Naming by Action for each group. The solid dark line in each graph
represents the model- predicted slope for the group in question.
LHD=Left Hemisphere Damage; RHD=Right Hemisphere Damage; ID=Patient Identification Number

107
Figure 3A.3: Individual Patient Performances in Tool Naming for each group. The solid dark line in each graph represents the
model- predicted slope for the group in question.
LHD=Left Hemisphere Damage; RHD=Right Hemisphere Damage; ID=Patient Identification Number

108
Figure 3A.4: Individual Patient Performances in Pantomime for each group. The solid dark line in each graph represents the
model- predicted slope for the group in question.
LHD=Left Hemisphere Damage; RHD=Right Hemisphere Damage; ID=Patient Identification Number

109
Figure 3A.5: Individual Patient Performances in Pantomime by Picture for each group. The solid dark line in each graph represents
the model- predicted slope for the group in question.
LHD=Left Hemisphere Damage; RHD=Right Hemisphere Damage; ID=Patient Identification Number

110
Figure 3A.6: Individual Patient Performances in Object Use for each group. The solid dark line in each graph represents the
model- predicted slope for the group in question.
LHD=Left Hemisphere Damage; RHD=Right Hemisphere Damage; ID=Patient Identification Number

111
Figure 3A.7: Individual Patient Performances in Delayed Imitation for each group. The solid dark line in each graph represents the
model- predicted slope for the group in question.
LHD=Left Hemisphere Damage; RHD=Right Hemisphere Damage; ID=Patient Identification Number

112
Figure 3A.8: Individual Patient Performances in Concurrent Imitation for each group. The solid dark line in each graph represents
the model- predicted slope for the group in question.
LHD=Left Hemisphere Damage; RHD=Right Hemisphere Damage; ID=Patient Identification Number

113
REFERENCES
Ballard, C., Rowan, E., Stephens, S., Kalaria, R., & Kenny, R. A. (2003). Prospective
follow-up study between 3 and 15 months after stroke - Improvements and decline in
cognitive function among dementia-free stroke survivors > 75 years of age. Stroke, 34, 2440-
2444.
Basso, A., Burgio, F., Paulin, M., & Prandoni, P. (2000). Long-Term Follow-up of
Ideomotor apraxia. Neuropsychological Rehabilitation, 10, 1-13.
Basso, A., Capitani, E., Della Sala, S., Laiacona, M., & Spinnler, H. (1987). Recovery
from ideomotor apraxia. A study on acute stroke patients. Brain, 110, 747-760.
Cimino-Knight, A. M., Hollingsworth, A. L., Maher, L. M., Raymer, A. M., Foundas,
A. L., Heilman, K. M. et al. (2002). Forms of recovery in ideomotor apraxia: a preliminary
investigation. Journal of the International Neuropsychological Society, 8, 207.
Donkervoort, M., Dekker, J., van den Ende, E., Stehmann-Saris, J. C., & Deelman, B.
G. (2000). Prevalence of apraxia among patients with a first left hemisphere stroke in
rehabilitation centres and nursing homes. Clinical Rehabilitation., 14, 130-136.
Foundas, A. L., Raymer, A. M., Maher, L. M., Gonzalez-Rothi, L., & Heilman, K. M.
(1993). Recovery in Ideomotor Apraxia. Journal of Clinical Experimental Neuropsychology,
14, 44.
Haaland, K. Y., Harrington, D. L., & Knight, R. T. (2000). Neural representations of
skilled movement. Brain, 123, 2306-2313.

114
Heath, M., Roy, E. A., Black, S. E., & Westwood, D. A. (2001). Intransitive limb
gestures and apraxia following unilateral stroke. Journal of clinical and experimental
neuropsychology, 23, 628-642.
Heath, M., Roy, E. A., Westwood, D., & Black, S. E. (2001). Patterns of apraxia
associated with the production of intransitive limb gestures following left and right
hemisphere stroke. Brain & Cognition, 46, 165-169.
Heilman, K. M. & Rothi, L. J. (1993). Apraxia. In Clinical Neuropsychology (pp.
141-163). New York, NY: Oxford University press Inc.
Kertesz, A. (1984). Recovery from aphasia. Advances in Neurology., 42, 23-39.
Lazar, R. M., Speizer, A. E., Festa, J. R., Krakauer, J. W., & Marshall, R. S. (2008).
Variability in language recovery after first-time stroke. Journal of Neurology Neurosurgery
and Psychiatry, 79, 530-534.
Marshall, S. C., Grinnell, D., Heisel, B., Newall, A., & Hunt, L. (1997). Attentional
deficits in stroke patients: A visual dual task experiment. Archives of Physical Medicine and
Rehabilitation, 78, 7-12.
Mimura, M., Fitzpatrick, P. M., & Albert, M. E. (1996). Long-term recovery from
ideomotor apraxia. Neuropsychiatry, neuropsychology, and behavioral neurology, 9, 127-
132.

115
Nicholas, M. (2005). Aphasia and dysarthria after stroke. In M.Barnes, B. Dobkin, &
J. Bogousslavsky (Eds.), Recovery after stroke (pp. 474-502). New York: Cabridge
University Press.
Raudenbush, S. W. & Bryk, A. S. (2002). Hierarchical Linear Models: Applications
and Data Analysis Methods. (2nd ed.) Sage publications.
Rothi, L. J., Mack, L., & Heilman, K. M. (1986). Pantomime agnosia. Journal of
Neurology, Neurosurgery & Psychiatry, 49, 451-454.
Roy, E. A. (1996). Hand Preference, Manual Assymetries, and Limb Apraxia. In
D.Elliot (Ed.), Manual Asymmetries in Motor Control (pp. 215). Boca Raton, FL: CRC Press.
Roy, E. A., Black, S. E., Blair, N., & Dimeck, P. T. (1998). Analyses of deficits in
gestural pantomime. Journal of clinical and experimental neuropsychology, 20, 628-643.
Roy, E. A., Heath, M., Westwood, D., Schweizer, T. A., Dixon, M. J., Black, S. E. et
al. (2000). Task demands and limb apraxia in stroke. Brain and cognition, 44, 253-279.
Roy, E. A., Square-Storer, P., Hogg, S., & Adams, S. (1991). Analysis of task
demands in apraxia. International Journal of Neuroscience, 56, 177.
Singer, J. & Willett, J. (2003). Applied Longitudinal Data Analysis. New York:
Oxford University Press.

116
CHAPTER 4: LIMB APRAXIA IN CORTICOBASAL SYNDROME (CBS)
ABSTRACT
Corticobasal Syndrome (CBS) is a progressive neurodegenerative disorder with
asymmetric presentation and course characterized by degeneration of basal ganglia and
cortical structures. Limb apraxia is a commonly observed deficit in CBS. Few studies have
examined comprehensively the nature of deficits in limb apraxia in CBS. The goal of our
study was to investigate the severity of deficits in various conceptual and gesture production
task modalities. CBS patients were divided in two groups based on the side of brain that was
initially affected by the disease. Ten patients with Right (RHP) and seven with left (LHP)
hemisphere presentation were included. Comparisons revealed, that while LHP patients were
only impaired on tool and action naming tasks, as well as on the Western Aphasia Battery,
RHP patients were impaired on action recognition tasks requiring patients to observe a
subject performing a gesture on a video screen. Overall, performance on all conceptual tasks,
suggested a preserved conceptual knowledge of actions and tools in both patients groups. On
gesture production tasks, both groups were affected relative to controls, with LHP affected
more severely, but not significantly different than RHP patients. Performance on pantomime
and imitation of transitive gestures was less accurate than intransitive gestures. Pantomime
accuracy was lower than concurrent imitation in both transitive and intransitive gestures. The
addition of verbal cuing during Concurrent Imitation, decreased imitation accuracy, making
performance similar to pantomime. Concurrent and Delayed imitation performance were
similar in all gesture types. Imitation of non-representational gestures was least accurate and
intransitive gestures were most accurate. Patients‟ performance improved with object use and
showing pictures of tools slightly decreased their performance as compared to pantomime.

117
INTRODUCTION
Corticobasal Syndrome (CBS) is a progressive neurodegenerative disorder
characterized by degeneration of basal ganglia and cortical structures. The disorder is
characterized by an asymmetric presentation and course. Based on the clinical diagnostic
criteria summarized by Boeve, Lang, & Litvan (2003), the following CBS diagnostic criteria
have been established: 1) Insidious onset and progressive course of disease; 2) No
identifiable cause (eg, tumor, infarct); 3) Cortical dysfunction as reflected by at least one of
the following: Focal or asymmetrical ideomotor apraxia, Alien limb phenomenon, Cortical
sensory loss, Visual or sensory hemineglect, Constructional apraxia, Focal or asymmetric
myoclonus or Apraxia of speech/nonfluent aphasia, 4) Extrapyramidal dysfunction as
reflected by at least one of the following: Focal or asymmetrical appendicular rigidity lacking
prominent and sustained L-dopa response or Focal or asymmetrical appendicular dystonia.
Boeve et al. (2003) specify the following supportive features: 1) Variable degrees of focal or
lateralized cognitive dysfunction, with relative preservation of learning and memory, on
neuropsychometric testing, 2) Focal or asymmetric atrophy on computed tomography or
magnetic resonance imaging, typically maximal in parietofrontal cortex or 3) Focal or
asymmetric hypoperfusion on single-photon emission computed tomography and positron
emission tomography, typically maximal in parietofrontal cortex, basal ganglia and/or
thalamus. Recent evidence also indicates that the motor manifestation of the disease may
follow the cognitive decline, and cases have been reported where the initial symptoms were
aphasia, apraxia, executive or visuospatial dysfunction (Kertesz, Martinez-Lage, Davidson,
& Munoz, 2000; Grimes, Lang, & Bergeron, 1999).

118
Limb apraxia is one of the most commonly reported cortical features of CBS. It is a
neurobehavioral disorder characterized by an inability to perform purposeful skilled
movements, not attributable to muscle weakness, paralysis, poor comprehension,
deafferentiation or an unwillingness to perform the task (Geschwind, 1975). To assess limb
apraxia, patients are often asked to pantomime (e.g., perform from memory to verbal
command) or imitate visually presented gestures and thus limb apraxia can also be
operationally defined as an inability to pantomime and/ or imitate gestures (Roy, 1996). This
disorder is most often studied in the context of stroke and is more prevalent after left than
right hemisphere stroke (Heilman & Rothi, 1993; Donkervoort, Dekker, van den Ende,
Stehmann-Saris, & Deelman, 2000; Roy, Square-Storer, Hogg, & Adams, 1991). The
dominant role of the left hemisphere in skilled movement is largely undisputed, but studies
have reported patients with limb apraxia after right hemisphere stroke as well. The nature of
apraxia after right stroke, however, may differ from that after left hemisphere stroke (Heath,
Roy, Westwood, & Black, 2001).
Several information processing models have been proposed in the literature to explain
the specific patterns of deficits in patients suffering from apraxia (Geschwind, 1975; Heilman
et al., 1993; Goldenberg & Hagmann, 1997; Cubelli, Marchetti, Boscolo, & Della Sala,
2000). The current study uses the conceptual-production model proposed by Roy (1996) as a
framework to understand limb apraxia deficits in CBS (see Chapter 1 for detailed
description). The conceptual-production model proposes that the execution of skilled actions
is under the control of three systems: the sensory/perceptual, the conceptual and the
production system. The sensory/perceptual system processes information from the
environment (visual, auditory or tactile). The conceptual system stores knowledge about

119
tools and actions. The production system consists of several subsystems subserving such
functions as response selection, image generation, working memory storage of the motor
plan, response organization and control of movement. Roy (1996) suggests that disruptions in
any of these three systems will result in a specific pattern of praxis deficits. For example, if
the conceptual system is affected, then patients will not be able to recognize gestures or
perform gestures on pantomime, since both these tasks require patients to remember what
various gestures look like. Patients should still be able to imitate gestures, however, because
one does not need to know what a gesture means to imitate it. If the production system is
affected, on the other hand, and the conceptual system is intact, the patient should be able to
recognize gestures but can neither pantomime nor imitate gestures. Thus, Roy (1996)
suggested that if a patient presents with certain gesture production deficits, a comprehensive
assessment is needed to determine where exactly disruptions in the system lie. Tasks that
assess all three systems need to be administered to answer this question. Unfortunately, most
studies, both in stroke and CBS, include pantomime and imitation tasks, but seldom probe
the conceptual system and, thus, it is often hard to determine whether a patient who is unable
to pantomime a gesture cannot do so because of a deficit in the conceptual or the production
system or both. For this purpose, Roy and colleagues have developed a comprehensive
standardized assessment that examines all areas of praxis functioning in order to determine
which system or systems are affected.
Aside from including different task modalities in assessing apraxia, there are three
main categories of gestures that have been used in the literature to assess deficits in praxis.
Transitive gestures, the gestures most commonly used in studies of apraxia, involve the use
of tools, for example using a hammer to pound a nail. Intransitive gestures do not involve

120
tools and are usually symbolic in nature, such as waving good-bye or beckoning someone to
come. Finally, non-representational gestures are meaningless postures or actions, often used
to determine the importance of meaning (gesture semantics) in performing the gesture..
While limb apraxia is one of the most common cortical features of CBS, and often the
initial neurobehavioral feature, few studies have examined in detail the nature of the limb
praxis deficits that patients with CBS present with. The relative few studies to date suggest
the following. First, when it comes to comparing pantomime and imitation, there appears to
be greater impairment in imitation than pantomime, but overall the differences between these
two modalities are not very clear cut. Peigneux and colleagues (2001) showed in 18 CBS
patients that imitation was more impaired than pantomime, irrespective of the gesture type
and two other smaller scale studies report similar findings (Jacobs et al., 1999a; Spatt, Bak,
Bozeat, Patterson, & Hodges, 2002). Other series, however, have reported that both
pantomime and imitation were impaired, with imitation tasks sometimes performed with
more accuracy than pantomime (Leiguarda, 2001; Pharr et al., 2001). Second, when it comes
to object/tool use, studies have shown that while CBS patients improve when using actual
tools relative to pantomime, they still remain impaired on this task (Jacobs et al., 1999a;
Graham, Zeman, Young, Patterson, & Hodges, 1999; Spatt et al., 2002; Leiguarda et al.,
2003). Third, both transitive and intransitive gestures have been reported to be affected
(Leiguarda et al., 2003; Jacobs et al., 1999b; Peigneux et al., 2001; Buxbaum, Kyle,
Grossman, & Coslett, 2007), but some report greater impairments on transitive than
intransitive gestures (Pharr et al., 2001; Salter, Roy, Black, Joshi, & Almeida, 2004; Chainay
& Humphreys, 2003). Fourth, usually no clear differences between representational and non-
representational gestures are found (Merians et al., 1999; Spatt et al., 2002; Salter et al.,

121
2004; Leiguarda et al., 2003; Buxbaum et al., 2007). Finally, as mentioned before, few
studies have examined the patients‟ conceptual knowledge of tools and actions, but the
evidence to date suggests that most patients with CBS do not have impairment in their
conceptual knowledge of actions (Leiguarda, Lees, Merello, Starkstein, & Marsden, 1994;
Jacobs et al., 1999a; Salter et al., 2004; Soliveri, Piacentini, & Girotti, 2005).
While we know much more about limb apraxia in CBS than we did a decade ago,
most studies to date suffer from several methodological downfalls. First, most reports have
included very few patients. In fact, in a recent review, we reported that out of the 16 studies
examining apraxia deficits in the literature, only 6 included more than 5 CBS patients
(Stamenova, Roy, Black, 2009). In addition, most investigations assess patients only on a few
task modalities. Most studies include pantomime and imitation tasks only, as well as possibly
object use. Some, however, include only imitation tasks. Finally, many studies do not assess
the patients‟ conceptual knowledge of tools and actions, which precludes knowledge of
which system may be causing the deficits in gesture production. Even if conceptual
knowledge is evaluated, different researchers use different tasks, so it is hard to compare
findings across studies. Finally, Roy (1996) differentiates between delayed and concurrent
imitation. In concurrent imitation the examiner demonstrates an action until the patient
completes the imitation, while in delayed imitation the examiner demonstrates an action and
the patient imitates the examiner right after from memory. According to Roy (1996)
comparing the performance in these two conditions helps determine whether deficits in the
production system stem from deficits in analysis of visual gestural information (both
concurrent and delayed imitation impaired), in encoding visual gestural information into
working memory (selective impairment in delayed imitation) or in deficits of response

122
organization and control (impairments in both imitation conditions as well as in pantomime).
No studies to date have compared CBS patients‟ performance on these two tasks.
Thus, the goal of our study was to examine limb apraxia performance in 17 CBS
patients through a comprehensive standardized battery. The battery includes transitive,
intransitive and non-representational gestures. In addition, pantomime, delayed and
concurrent imitation, as well as object use are among the tasks included. Finally, the battery
includes a number of assessments examining the conceptual knowledge of tools and actions.
Based on past literature, the following predictions are made. First, if differences between
pantomime and imitation are observed, performance on imitation will be less accurate than
pantomime. Patients pantomiming when holding the tool (object/tool use) would increase
their performance accuracy relative to their pantomime performance accuracy. Performance
on transitive gestures will be less accurate than intransitive gestures. Even though past
studies have not shown significant differences between meaningful and meaningless
gestures, we predicted that non-representational gestures would be more severely affected
than meaningful gestures. This prediction was made, because meaningless gestures would
not receive support from semantics, which is often preserved in CBS and they are highly
dependent on the intact function of the dorsal parieto-frontal network, which is often
impacted by the neurodegenerative process in CBS. Finally, the conceptual knowledge of
gestures and tools will be preserved, given previous reports of lack of conceptual deficits in
CBS patients and the lack of damage to centre of conceptual knowledge storage, the left
inferior parietal lobule, (Heilman, Rothi, & Valenstein, 1982) (superior parietal damage is
more typical in CBS (Dickson et al., 2002),

123
Aside from performing a comprehensive assessment, we aimed to compare left
hemisphere presentation (LHP) vs. right hemisphere presentation (RHP) CBS patients. CBS
is a disease with an asymmetrical manifestation of extrapyramidal symptoms affecting one
side of the body more than the other early in its course. This asymmetrical presentation arises
because the neurodegenerative process starts earlier in one hemisphere, evident both in
neuroimaging studies reporting a greater hypoperfusion (Zhang et al., 2001) or
hypometabolism (Blin et al., 1992) in the hemisphere contralateral to the side of presentation,
as well as by neuropathological studies reporting asymmetrical neurodegeneration (Dickson,
Liu, Ksiezak-Reding, & Yen - SH, 2000; Rebeiz, Kolodny, & Richardson, Jr., 1968). For the
purposes of this study, by definition, LHP patients had a motor presentation affecting the
right arm or leg, and RHP patients had preferential motor impairment of the left side of their
body. Given the role of the left hemisphere in limb apraxia, we hypothesized that LHP
patients should present with greater deficits in gesture production tasks, than RHP patients.
We also hypothesized that among conceptual tasks, action and tool naming would be more
impaired in LHP patients due to naming difficulties associated with possible aphasia, which
is more prevalent in LHP patients.
Finally, we aimed to examine the patterns of deficits that patients present with. Our
hypothesis was that patients would present with patterns that reflect a common deficit in
pantomime and imitation, suggestive of a deficit in the final stages of the production system,
while knowledge of gestures should be preserved.

124
METHODS
Participants
Seventeen patients with Corticobasal Syndrome (CBS) were studied. All patients met
Boeve, Lang & Litvan (2003) diagnostic criteria. Patients were excluded from the study if
they had a history of a neurological impairment (other than the diagnosis of CBS in the case
of CBS patients), and had a history of alcohol or drug abuse, psychiatric or movement
disorders (other than the extrapyramidal features in CBS patients), or any peripheral
condition (e.g., arthritis) which could compromise motor function. Patients also had to have a
minimum of 8 years of formal education and be younger than 90 years of age at the time they
were considered for participation in the study. Ten patients had a RHP and seven patients had
LHP. In addition, 28 age-matched control participants were included. Control participants
were assessed with both their right and left hand and an average score for both hands was
used in the analysis. Past work has shown no hand differences in gesture performance in
normal age-matched control participants (Roy et al., 1991). In addition, using the average
performance between the two hands allowed us to compare more easily the two groups of
patients (who performed with their less affected limb) relative to controls. Patients performed
all tasks with their less affected limb. Consent to participate in the study was obtained from
all participants and the study was approved by the Research Ethics Board at Sunnybrook
Health Sciences Centre and at the University of Waterloo. All groups were matched on age,
sex and handedness, but the LHP group had about 4 years more education than both the
control and the RHP group (Table 4.1). The two patient groups did not differ in terms of time
from onset of the disease. Table 4.2 gives a detailed overview of the clinical presentation of
each patient.

125
Table 4.1: Demographic Characteristics of each participant group
Controls
(n=28) RHP (n=10) LHP (n=7) p-Value
Age 68 (9) 67 (9) 72 (8) 0.50
Years of Education 15 (3) 14 (2) 10 (1)* p<.001
Sex M/F 10/18 5/5 1/6 0.32
Handedness R/L 26/2 9/1 7/0 0.64
MMSE 29 (2) 25 (4)* 23 (6)* p<.001
Western Aphasia Battery 99 (2) 95 (4) 79 (15)* p<.001
Onset (Years) 4 (2) 7 (7) 0.26 * Indicates which group is significant different from controls after Bonferroni corrected post-hoc comparisons.

126
Table 4.2: Clinical Presentation of all patients based on neurological examination.
Rig
idit
y
Co
rtic
al
Sn
eso
ry L
oss
Ap
rax
ia
Ath
eto
sis
Ali
en L
imb
Ass
ym
etri
c
Rig
idit
y
Lim
b
Dy
sto
nia
My
ocl
on
us
Ea
rly
Dem
enti
a
Ap
ha
sia
Sp
eech
Vis
uo
-sp
ati
al
Ex
ecit
ive
Oth
er
Dem
enti
a
Su
pra
nu
cle
a
r P
als
y
Tre
mo
r
46-RHP + + + + Levitation + + + - + + + + - - -
49-RHP + - + n/a Possible + - - + + + + + memory loss - -
55-RHP + + + + - + - - - + + + + - - postural
58-RHP + + + + Levitation + - + + + + + + inattention - -
62-LHP + + + n/a - + - + + + + + + memory loss - -
68-RHP + + + + Levitation + + + - - - + + - - action
71-RHP + - + n/a Levitation + + - - + + + +
memory
loss/
inattention
Present; no
vertical
rest/postural/
action
73-RHP + + + + Possible + + + - - - - + - - -
76-LHP + + + n/a - + - - + + + + + - Present;
limited up
postural/
action
83-RHP + + + n/a - + - + + - + + + memory loss - -
98-RHP + - + n/a - + + - + + + - + - Present;
limited vertical -
105-LHP + - + n/a - + + + + + + + + - Present;
limited vertical -
123-LHP + - + - Levitation + + - + + + + + inattention Present;
limited vertical -
132-LHP + + + - - + + - - - - - - - - postural/
action
133-LHP + + + - - + - - - - - + + memory loss - -
153-LHP + - + n/a Levitation + + - + + + - +
memory
loss/
inattention
Present;
limited vertical -
162-RHP + + + - Levitation + - - - + + - + inattention Present;
limited vertical
postural/
action
+ Present; - Absent

127
Tests and Procedures
Limb Apraxia Assessments
Details of Tasks and Scoring Procedures are given in Appendix A. The following
tasks were included in the assessment.
Conceptual Limb Apraxia Assessment
Assessment was started with three tasks assessing naming: Tool Naming, Tool
Naming by Function and Tool Naming by Action. Two Tool Identification (ID) tasks
followed the tool naming tasks: Tool ID and Tool ID by Function. Four Gesture ID tasks:
Action ID, Action ID by Tool, Gesture Matching and Gesture Error Recognition were
administered after the gesture production tasks described below in order to avoid biasing the
patients‟ responses from observing the gesture performed on the video screen.
Gesture Production Limb Apraxia Assessment
The following tasks were administered to assess the patients‟ ability to produce
gestures: Pantomime to Verbal Command for Transitive Gestures, Pantomime to Verbal
Command for Intransitive Gestures, Pantomime by Picture, Object Use, Pantomime by
Function, Delayed Imitation of Transitive Gestures, Delayed Imitation of Intransitive
Gestures, Delayed Imitation of Non-Representational Gestures, Concurrent Imitation of
Transitive Gestures, Concurrent Imitation for Transitive Gestures with Verbal Cue,
Concurrent Imitation of Intransitive Gestures and Concurrent Imitation of Non-
Representational Gestures. The tasks were administered in the order described.
.

128
General Neuropsychological Assessments
Participants completed the Mini Mental Status Examination (MMSE) for general
cognitive level of performance (Folstein, Folstein, & Mchugh, 1975) at the time of the
apraxia assessment. In addition, the Western Aphasia Battery (WAB) was used to assess
speech-language functioning (Kertesz, 1982) and the Boston Naming Test (BNT) (30-item)
(Kaplan, 1983), as part of a longer study investigating the progression of neuropsychological
deficits in neurodegenerative disorders. The language assessment performed closest to the
apraxia assessment was included in the analysis (usually assessments performed within an
year from the apraxia assessment were chosen). The average duration between the apraxia
assessment and the language assessment was 122 days (Range 1-344). Four cases had
language assessments over 150 days away from their arpaxia assessment: in three cases the
assessments were done 293, 344 and 169 days before the apraxia assessment (Case ID 153,
162, and 55 respectively) and in one case (Case ID 49), the assessment was done 210 days
later.
In order to assess whether the timing of the WAB and BNT assessment relative to
apraxia affected findings on these measures of speech-language function two analyses were
run: 1. The WAB Naming and BNT scores were correlated with the days elapsed between the
apraxia and the language assessment. Neither the correlation with WAB Naming (r=-.21,
p=.66), nor the correlation with BNT (r=.005, p=.99) were significant. 2. We grouped
patients based on whether they have had their assessment before (N=7) or after (N=5) the
apraxia assessment and compared their WAB and BNT scores using a t-test. No Significant
difference was found between the two groups on the WAB Aphasia Quotiend scores (the
overall WAB score) (t=-.87, p=.4), the WAB Naming (t=-.4, p=.69) or the BNT score (t=-

129
.57, p=.58). Therefore, we conclude that whether the test was done before or after the apraxia
assessment was not a significant factor on how the patients performed on the language
assessment.
RESULTS
Group comparisons
A series of ANOVA‟s were run to compare the performance of each group for each
task. This approach was chosen, as opposed to a MANOVA analysis in order to maximize
the number of patients per task, because not all patients had performed all tasks. Bonferroni
corrected post-hoc t-test comparisons were run after each of the ANOVA‟s to determine
group differences. The mean percentage scores for each of the three groups (Controls, LHP
and RHP) are summarized on Table 4.3. The associated p-values are also listed.

130
Table 4.3: Group Comparisons for each task Modality. Scores are in Percentages. Control RHP LHP p-value Control RHP LHP p-value
Tool Naming
N 28 10 6 <0.001
Pantomime by Picture
N 28 10 6 <0.001
Score 99.1 91.3 83.3 Score 93.9 75.9 63.5
SD 3.3 10.3 23.3 SD 3.3 11.7 20.0
Tool Name by
Function
N 28 10 6 0.09
Object Use
N 28 10 7 <0.001
Score 97.8 93.8 89.6 Score 97.4 85.5 75.5
SD 5.9 10.6 14.6 SD 2.0 10.0 10.8
Tool Naming by
Action
N 28 10 6 <0.01
Pantomime by Function
N 28 10 5 <0.001
Score 95.1 90.0 79.2 Score 94.5 73.7 70.0
SD 7.9 14.2 20.4 SD 4.0 13.7 21.5
Tool
Identification
N 28 10 7 0.18
Delayed Imitation Transitive
N 28 10 6 <0.001
Score 100.0 98.8 100.0 Score 97.6 78.6 81.1
SD 0.0 4.0 0.0 SD 2.6 17.2 7.4
Tool
Identification by
Function
N 28 10 7 0.36
Delayed Imitation
Intransitive
N 24 9 6 <0.001
Score 99.6 100.0 98.2 Score 99.2 94.8 93.6
SD 2.4 0.0 4.7 SD 1.3 5.7 4.1
Action
Identification
N 27 8 5 <0.01
Delayed Imitation Non-
Representational
N 24 9 5 <0.001
Score 98.4 90.0 100.0 Score 96.3 69.9 74.1
SD 4.0 14.2 0.0 SD 2.9 23.2 4.4
Action
Identification by
Tool
N 27 8 4 <0.001
Concurrent Imitation
Transitive
N 28 9 5 <0.001
Score 100.0 91.3 100.0 Score 97.5 82.8 84.9
SD 0.0 11.6 0.0 SD 2.1 14.7 6.7
Gesture Matching
N 27 7 4 0.53
Concurrent Imitation
Transitive with Verbal Cue
N 28 9 5 <0.001
Score 94.1 95.4 98.1 Score 96.9 77.9 72.8
SD 7.2 6.0 3.8 SD 2.7 16.0 17.8
Gesture Error
Recognition
N 26 7 4 <0.001
Concurrent Imtiation
Intransitive
N 28 8 6 <0.001
Score 80.3 53.1 66.4 Score 99.2 93.7 93.2
SD 10.9 32.6 10.6 SD 1.1 5.8 5.1
Control RHP LHP p-value Control RHP LHP p-value
Pantomime
Transitive
N 28 10 7 <0.001
Concurrent Imitation Non-
Representational
N 28 9 7 <0.001
Score 93.8 76.8 67.6 Score 96.7 68.7 62.3
SD 4.4 13.9 16.2 SD 2.4 15.7 15.4
Pantomime
Intransitive
N 28 10 7 <0.001
Score 93.5 91.3 84.1
SD 4.2 7.9 10.2

131
Conceptual Limb Apraxia Assessment Tasks
Naming
Significant differences were observed in Tool Naming (F(2, 43)=7.4 ; p<.005) and
Tool Naming by Action (F(2, 43)= 4.76; p<.05.). Only the LHP patients performed at
significantly lower levels than the Controls, while the RHP patients were not impaired
relative to the controls. The difference in Tool Naming by Function did not reach
significance [F(2,43)=2.58; p=.088].
Tool ID
Neither Tool ID, nor Tool ID by Function showed significant differences among the
three groups, that is to say neither patient group was impaired on these tasks.
Action ID
Both Action ID and Action ID by Tool showed significant effects, [F(2, 39)=4.9;
p<.05.] [F(2, 38)= 9.23; p<..001] respectively. In this case, a post-hoc comparison indicated
that only the RHP patient group performed significantly worse than the controls.
Gesture Matching and Gesture Error Recognition
Gesture Matching did not show a significant difference among the three groups of
participants. In Gesture Error Recognition a significant effect [F(2, 36)= 7.59; p<.005]
showed that only the RHP patient group performed significantly worse than the controls .
Gesture Production Limb Apraxia Assessment Tasks
Pantomime

132
A significant main group effect was found in Pantomime to Verbal Command of
Transitive Gestures [F(2,44)=19.91; p<.001], in Pantomime to Verbal Command of
Intransitive Gestures [F(2,44)=6.71; p<.005], in Pantomime by Picture [F(2,43)=32.42;
p<.001] and in Pantomime by Function [F(2,42=21.69; p<.001]. Both LHP and RHP
patients performed significantly below normal on Pantomime to Verbal Command of
Transitive Gestures and on Pantomime by Function. The two patient groups did not differ in
performance levels. On Pantomime to Verbal Command of Intransitive Gestures, the LHP
group performed significantly lower than both the Control and the RHP groups, who in turn
did not differ from each other. On Pantomime by Picture both LHP and RHP performed
significantly lower than controls, but the LHP group also performed significantly less
accurately than the RHP group.
Object use
A significant group main effect was found in Object Use F(2,44)=29.37; p<.001]
.Both groups performed at lower levels than controls but LHP patients also obtained a
significantly lower score, scoring on an average 12% lower than RHP patients.
Delayed Imitation
A main effect of group was found significant in all Delayed Imitation tasks: Delayed
Imitation of Transitive Gestures [F (2, 43)= 20.65, p<.001], Delayed Imitation of Intransitive
Gestures [F (2, 38)= 9.91, p<.001], and Delayed Imitation of Non-Representational Gestures
[F (2, 37)= 21.35, p<.001]. Both LHP and RHP patients were significantly less accurate than
controls and the two patient groups did not differ from each other.

133
Concurrent Imitation
There was a significant main effect of group in all Concurrent Imitation tasks:
Concurrent Imitation of Transitive Gestures [F (2, 41)= 17.3, p<.001], Concurrent Imitation
of Intransitive Gestures [F (2, 40)= 23.57, p<.001], Concurrent Imitation of Transitive
Gestures with verbal Cueing [F (2, 41)= 12.19, p<.0001], and Concurrent Imitation of Non-
Representational Gestures [F (2, 43)= 49.94, p<.001]. Both LHP and RHP patients were
significantly less accurate than controls and the two patient groups did not differ.
MMSE
An ANOVA comparison showed a main group effect on MMSE scores [F(2,
32)=8.14; p<.001], the control group had a significantly higher MMSE score than both
patient groups who in turn did not differ from each other.
WAB
Unfortunately, only 8 RHP, 4 LHP and 17 Controls had completed a full WAB
assessment. An ANOVA comparison of the total WAB AQ score showed a significant main
group effect [F(2, 28)=23.6; p<.001]. The LHP group had significantly lower Aphasia
Quotient scores (Mean=78.4/100) than the RHP (Mean=94.1/100) and the control group
(Mean 98.7/100). In addition, ANOVA comparisons were also ran to compare the three
groups in the WAB naming subscore. The analysis showed that there was a significant main
effect of group [F(2, 28)=6.84; p<.001], but Bonferroni corrected posthoc comparison
showed that both the RHP and the LHP were significantly more impaired than the controls.
In addition, all patients had completed the WAB comprehension section and only one patient
scored below 7 (with a score of 6.65), which is considered impaired according to Kertesz &
Poole classification. (Kertesz & Poole, 1974). An ANOVA comparison between the three

134
groups showed a significant effect of group [F(2, 33)=4.3; p<.05]. Bonferroni corrected
posthoc t-test comparisons showed that the LHP group had a significantly lower
comprehension that the RHP group, with an average of 9.1 vs. 9.9 in both the RHP and the
control group. Finally, a t-test comparison was run between the two patient groups who also
had recorded BNT scores. 10 RHP and 6 LHP patients had BNT assessments completed. The
analysis showed that there was no significant difference between the two patient groups on
the BNT [F(1, 15)=6.84; p<.001],
In order to examine the relationship between performance on all the conceptual
components of the Limb Apraxia Assessment and the WAB AQ score, WAB Naming, WAB
Comprehension and the BNT, we ran a series of Pearson Correlations. The results indicated
that the WAB AQ was not correlated with any of the Conceptual Tasks. The BNT and WAB
Comprehension were significantly correlated only with Tool Naming by Action and Tool
Identification by Function. Finally, the WAB Naming was correlated significantly only with
Tool Naming from the Apraxia Conceptual tasks. All correlations and their associated p-
values are displayed in Table 4.4.

135
Table 4.4 Correlations between language and conceptual tasks.
Tool
Naming
Tool
Name by
Function
Tool
Name
by
Action
Tool
ID
Tool ID
by
Function
Action
ID
Action
ID by
Tool
Gesture
Recognition
Gesture
Error
Recognition
BNT .345 .128 .568* .245 .689
** .050 .099 .389 .295
WAB AQ .372 -.031 .545 -.117 .404 .000 -.017 .474 -.070
WAB
Comprehension .057 -.150 .513* -.119 .831
** -.090 -.102 .211 .026
WAB Naming .605* .256 .499 -.287 .448 .329 .203 .516 .113
Correlation is significant at the 0.05 level* and at the 0.01 level **.
In addition, Table 4.5 shows a list of all patients and whether they were impaired on
each of the conceptual apraxia tasks (impairment defined as 2 SD‟s below the performance of
the control participants), on WAB Naming (as per (Kertesz et al., 1974) a score of 9 or below
is indicative of a naming deficit), on WAB Comprehension (a score of 7 or below is
considered a deficit in comprehension Kertesz & Poole, 1974) and on the BNT (patient
scores were scaled relative to the normative data published by (Steinberg, Bieliauskas, Smith,
Langellotti, & Ivnik, 2005)) .

136
Table 4.5. Case by case description of Impairments in Naming and Conceptual tasks.
ID BNT
WAB
Compr.
WAB
Naming
Tool
Name
Tool
Name
by
Funct.
Tool
Name
by
Action
Tool
ID by
Funct.
Action
ID
Gesture
Matching
Gesture
Error
Recog.
62-LHP 1 1 1 1 0 1 1 0 0 1
76-LHP 0 0 1 1 1 1 0 ---- ---- ----
105-LHP 0 0 1 ---- ---- ---- 0 ---- ---- ----
123-LHP 0 0 1 1 0 0 0 0 ---- ----
132-LHP 0 0 ---- 0 0 0 0 0 0 0
133-LHP 0 0 ---- 0 0 0 0 0 0 0
153-LHP 0 0 ---- 1 0 1 0 0 0 0
46-RHP 0 0 0 0 0 0 0 ---- ---- ----
49-RHP 0 0 0 0 0 0 0 0 0 0
55-RHP 0 0 1 1 1 1 0 ---- ---- ----
58-RHP 0 0 0 1 0 0 0 1 0 0
68-RHP 0 0 0 0 0 0 0 0 0 0
71-RHP 0 0 1 1 0 0 0 0 0 0
73-RHP 0 0 0 0 0 1 0 0 0 1
83-RHP 0 0 ---- 1 0 0 0 1 ---- ----
98-RHP 0 0 ---- 0 0 0 0 0 0 0
162-RHP 0 0 1 1 1 1 0 1 0 1
0=Not Impaired 1= Impaired
As can be seen in the table above, nine patients were impaired on Tool Naming and
six of them were also impaired on WAB Naming. Unfortunately, for two patients we have no
data on WAB Naming and one patient was not impaired on WAB Naming. It should be noted
that the patient who was not impaired on WAB Naming but impaired on tool naming had
aphasia assessment after the apraxia assessment and therefore we know for sure that at
apraxia assessment he had no language deficits. All three patients who were impaired on
Tool Naming had preserved ability to identify Tools through other modalities and therefore
their knowledge of tools was not affected. For example, all of them were able to name tools
when the tool‟s function was given. Also, all patients except one (Case 62-LHP) were able to
identify tools when their function was described to them. In regards to gesture knowledge,
only three patients were impaired on Action ID (all RHP patients). Two of these patients

137
were able to name tools in response to gesture demonstrations and, therefore, it is unlikely
that at least those two patients had lost their knowledge of gestures.
Only one patient, 162-RHP was impaired in the ability to identify both actions and to
name tools in response to viewed actions, even though this patient successfully matched
gestures, speaking of his preserved ability to process visuogestural information. Overall,
aside from that last patient, the evidence suggests that patients had preserved knowledge of
gestures and tools.
Task Comparisons
Pantomime to Verbal Command, Concurrent and Delayed Imitation in Transitive
and Intransitive Gestures.
As already described, it is not clear whether CBS patients are more impaired on
pantomime, on imitation or if no differences exist between the two task modalities. The
examination of these two task modalities is important for our understanding of the underlying
causes of deficits in gesture production in CBS. If deficits lie at the end stages of gesture
production, few differences are expected between pantomime and imitation. If deficits arise
earlier in gesture production, such as the conversion of conceptual action knowledge into
movement, we should expect pantomime deficits to be greater. Finally, given that imitation
can involve two routes, the direct (non-semantic) and indirect (semantic) route, it is possible
that imitation performance may be better than pantomime, a condition where only semantic
performance is possible. In addition, comparisons between transitive and intransitive gestures
are also important, given the larger role of the left hemisphere in transitive movements, as
opposed to intransitive. Therefore, we aimed to examine differences between the two groups
of patients in these two gesture types.

138
To compare the performance of the patients on the three tasks common to both
transitive and intransitive gestures, a 2 (Gesture) x 3 (Task) x 3 (Group) MANOVA was run.
8 RHP, 5 LHP and 24 Control participants were included in this analysis. Similar to the
larger sample of participants, an ANOVA comparison of demographic characteristics of this
subsample showed no significant differences on any of the measures, except on years of
education (Table 4.6).
Table 4.6: Demographics of Subsample (n=13) used in task comparisons
The analysis (see Figure 4.1) revealed that, as predicted, transitive gestures were
performed with less accuracy than intransitive gestures [F(1,34)=40.8; p<.001], a difference
more pronounced in the two patient groups, as shown by a significant interaction between
gesture type and group [F(2,34)=13.11; p<.001]. A main effect of task was also found, [F(2,
33)=19.9; p<.001], opposite to prediction pantomime performance accuracy (Mean=83.6%)
was lower than performance in both Delayed Imitation (Mean=87.2%) and Concurrent
imitation (Mean=89%), but Bonferroni corrected pairwise t-test comparisons showed that the
difference was significant only between pantomime to verbal command and concurrent
imitation. A main effect of Group [F(2,34)=28.1; p<.001] showed the Control participants
performed significantly better than the patient groups, but no difference between the two
patient groups was observed, as indicated by pairwise Bonferroni corrected t-test
comparisons. No other interactions were observed.
RHP (n=8) LHP (n=5) p-value
Age 66 (8) 70 (7) 0.50
MMSE 25 (4) 26 (3) p<.001
Sex M /F 4/4 1/4 0.54
Handedness R /L 7 /1 5 /0 0.68
Education 14 (2) 9 (1) p<.01
Years from Onset 4 (2) 4 (0) 0.73

139
Figure 4.1. Pantomime to Verbal Command, Concurrent and Delayed Imitation in Transitive
and Intransitive Gestures.
0
10
20
30
40
50
60
70
80
90
100
Control RHP LHP Control RHP LHP
Transitive Gestures Intransitive Gestures
Perf
orm
an
ce A
ccu
racy (
%)
Pantomime
Delayed Imitation
Concurrent Imitation
The results indicate that performance on transitive was less accurate than intransitive gestures and pantomime
was less accurate than the two imitation tasks. No differences between the two patient groups were observed.
Control participants improved more on imitation relative to pantomime than the two patient groups did.
Pantomime to Verbal Command, Concurrent Imitation and Imitation with Verbal
Cue in Transitive Gestures
In addition, we compared the performance on Pantomime, Concurrent
Imitation and Concurrent Imitation with Verbal Cue, with the hypothesis that Verbal Cueing
should improve performance relative to both Pantomime and Imitation. This hypothesis was
made because in Imitation with Verbal Cueing, support for the patients‟ performance could
come from either route to imitation (the semantic through the verbal cueing or the visual
through the observation of examiner‟s performance). Given the lack of conceptual gesture
knowledge deficits among the patients it was expected that Imitation and Imitation with
verbal Cuing would not differ between each other, while pantomime will be relatively more
impaired than the two Imitation tasks.

140
A 3(Task) x 3 (Group) MANOVA was used to compare the performance of 9 RHP, 4
LHP and 28 Control participants. The results showed a significant effect of task,
[F(2,37)=9.6; p<.001] and Group [F(2,38)=21.6; p<.001] and a significant interaction
between the two [F(4,76)=4.2; p<.005] (See Figure 4.2). The Control group performed at
higher levels on Imitation and Imitation with Verbal Cueing relative to Pantomime, while the
two patient groups performed at a higher level only on Imitation. Their performance on
Imitation with Verbal Cuing was at a similar level to that on Pantomime. Posthoc Bonferroni
corrected multiple comparisons showed that while both patient groups were performing at
significantly lower levels than controls, they did not differ from each other (Figure 4.2).
Figure 4.2. Pantomime to Verbal Command, Concurrent Imitation and Imitation with Verbal
Cue in Transitive Gestures.
0
10
20
30
40
50
60
70
80
90
100
Control RHP LHP
Perf
orm
an
ce A
ccu
racy (
%)
Pantomime
Concurrent Imitation
Imitation with Verbal Cue
The Control group improved on Imitation and Imitation with Verbal Cueing relative to Pantomime, while the
two patient groups improved only on Imitation.
Concurrent and Delayed Imitation of Transitive, Intransitive and Non-
Representational Gestures
To examine accuracy differences between gesture types in imitation, 8 RHP, 5 LHP
patients and 24 Control Participants were included in a 3(Gesture) x 2(Task) x 3(Group)

141
MANOVA comparing the Concurrent and Delayed Imitation of the three gesture types:
Transitive, Intransitive and Non-Representational. The hypothesis was that patients would be
most impaired on non-representational gestures, since these gestures do not receive support
from semantics and also would be affected due to damage in the dorsal networks usually
associated with CBS. It was also expected that there will be no significant differences
between side of presentation, since imitation (especially of transitive and intransitive
gestures) is largely controlled by dorsal networks in both hemispheres.
The analysis showed a significant effect of Gesture Type [F(2,33)=48.1; p<.001],
Group [F(2,34)=34.3, p<.001), a significant interaction between Gesture type and Group
[F(4,68)=8.0; p<.001] and a significant 3-way interaction [F(4,38)=2.7; p<.05] (see Figure
4.3). The Gesture type by Group interaction suggests that patients were more impaired
relative to controls in transitive and non-representational gestures than in intransitive
gestures. This three-way interaction is shown in Figure 4.3. Here we can clearly see that the
difference between the controls and the two patient groups is greater for the transitive and
non-representational gestures. This effect though seems to be mitigated by the task so 3
separate 2 (Task) x 3 (Group) MANOVA‟s were run for each of the three gesture types to
compare the three groups in their performance of Delayed vs. Concurrent Imitation. The
results indicated that the group effect was significant in each of the three analyses with the
controls performing better than the two patient groups, who in turn did not differ between
each other. For all three analyses, there was no significant task effect and no significant task
by group effect. There was an almost significant group by task interaction in the non-
representational gestures, F(2,34)=2.9, P=.067, indicating very little difference between LHP
and RHP patients in Concurrent Imitation, but in Delayed Imitation the RHP group

142
performed worse (Mean=67%) than the LHP group (Mean=73%).This suggests that while
the LHP patients benefited from the introduction of a delay, the RHP patients‟ performance
not only did not benefit but slightly decreased in accuracy.
Figure 4.3. Concurrent and Delayed Imitation of Transitive, Intransitive and Non-
Representational Gestures.
60
65
70
75
80
85
90
95
100
Controls RHP LHP
Pe
rce
nt
Ac
cu
rac
y (
%)
Tran DI
Tran CI
Intran DI
Intran CI
Non-Rep DI
Non-Rep CI
A 3-way interaction is noted, with the patient groups impaired relative to controls on all tasks, but the difference
much more significant in transitive Gestures and Non_Representational Gestures. In addition, there was an
almost significant interaction between task and group within the Non-Representational Gestures, showing
delayed imitation to RHP group had lower scores on all tasks, except on concurrent imitation of non-
representational gestures where the LHP performed with less accuracy.
Pantomime, Pantomime by Picture and Object Use
Past studies have shown that holding the actual tool while pantomiming facilitates
performance in CBS patients relative to that when a tool is not available. In addition, studies
in stroke have reported cases of patients with selective impairment in pantomime to pictures
of objects with no impairment in pantomime to verbal command or object identification.
Such cases suggest the existence of a separate route to action activated in response to pictures
of objects. While apraxia is one of the commonest cortical signs of Corticobasal

143
Degeneration (CBD), no studies have directly compared performance under distinct
modalities, such as vision or touch, in this disorder.
10 RHD, 6 LHP and 28 Control participants and were compared on Pantomime to
Verbal Command, Pantomime by Picture and Object Use with a 3 (Task) x 3 (Group)
MANOVA. A significant effect of task [F (2,40) = 36.6; p<.001], group [F (2,41) = 29.0;
p<.001] and a significant interaction between the two [F (4,82) = 5.1; p<.005] (See Figure
4.4) showed that LHP patients were least accurate on pantomime by picture, followed by
pantomime to verbal command (an effect more pronounced in the LHP than the RHP group)
and most accurate on Object Use. The control participants and the RHP patients did not differ
in their performance on Pantomime and Pantomime by Picture. Bonferroni corrected
pairwise multiple comparisons showed that all three groups were significantly different from
each other, with the LHP patient group performing at lowest levels.

144
Figure 4.4. Pantomime, Pantomime by Picture and Object Use.
0
10
20
30
40
50
60
70
80
90
100
Controls RHP LHP
Perf
orm
an
ce A
ccu
racy (
%)
Pantomime
Pantomime by Picture
Object Use
LHP patients were least accurate on pantomime by picture, followed by pantomime to verbal command (an
effect more pronounced in the LHP than the RHP group). The control participants and the RHP patients did not
differ in their performance on Pantomime and Pantomime by Picture. All groups improved their performance in
Object Use.
Frequency Analysis
To determine if the frequency of apraxia deficits varies in LHP and RHP patients and
to examine how these frequencies change depending on the task, each patient‟s score per task
was converted into a Z-score relative to the performance of the control participants. If a
patient‟s score fell 2 SD‟s below the mean of the control group, the patient was considered to
be impaired on that task. Thus, the number of impaired patients and the relative percentage
could be calculated for each task for each of the two patient groups. While the percentage of
patients impaired on a task varied somewhat and usually more patients with LHP were
affected in their performance than RHP, a chi-square analysis revealed that this difference in
frequency was not significant in any of the tasks (see Table 4.7). The only tasks where more
RHP patients were affected than LHP patients were: Tool name by Function, Action

145
Identification, Gesture Error Recognition and Concurrent Imitation of Intransitive Gestures
but these differences were not significant. Interestingly, none of the RHP patients were
impaired on Tool Identification by Function or Gesture Matching, while none of the LHP
were affected in Action ID and Gesture Matching. Again, these frequencies do not include
patients who were not assessed on a task, because they were completely unable to perform it
due to reasons other than apraxia
Table 4.7. Frequencies of deficits among the sample for each task.
Normal
RHP
Impaired
RHP
Percent
RHP
Impaired
Normal
LHP
Impaired
LHP
Percent
LHP
Impaired
p-value
Tool Name 5 5 50 2 4 66.7 0.6
Tool Name by Function 8 2 20 5 1 16.7 1.0
Action Name 7 3 30 3 3 50 0.6
Action ID 5 3 37.5 5 0 0 0.2
Tool ID by Function 10 0 0 6 1 14.3 0.4
Gesture Matching 7 0 0 4 0 0
Gesture Error Recognition 5 2 28.6 3 1 25 1.0
Pantomime Transitive 5 5 50 1 6 85.7 0.2
Pantomime Intransitive 9 1 10 4 3 42.9 0.3
Pantomime by Picture 3 7 70 0 6 100 0.3
Object Use 3 7 70 0 7 100 0.5
Pantomime by Function 3 7 70 1 4 80 1.0
Delayed Imitation Transitive 3 7 70 1 5 83.3 1.0
Delayed Imitation
Intransitive 5 4 44.4 3 3 50 1.0
Delayed Imitation Non-Rep 2 7 77.8 0 5 100 0.5
Cocurrent Imitation
Transitive 3 6 66.7 0 5 100 0.3
Concurrent Imitation
Transitive with Verbal Cue 2 7 77.8 0 4 100 1.0
Concurrent Imitation
Intransitive 1 7 87.5 2 4 66.7 0.5
Concurrent Imitation Non-
Representational 1 8 88.9 0 7 100 1.0
Apraxia Pattern Analysis
Transitive Gesture Patterns.
Three Gesture production Tasks (Pantomime of Transitive gesture, Delayed Imitation
of Transitive Gestures, Concurrent Imitation of Transitive Gestures) and a composite Action

146
Recognition Score (Action Naming and Action Identification) in which a patient was
considered impaired only if they were impaired on both tasks, were used to determine the
pattern of performance for each patient.
The pattern analysis revealed that all LHP patients had at least some form of
impairment, but there were 3 patients with RHP who did not have any apraxia deficits on the
pattern defining tasks. Unfortunately, only 8 RHP and 4 LHP patients had data on all pattern
defining tasks, in order for a pattern profile to be composed. The most common pattern in all
groups was a pattern where patients were impaired on all gesture production tasks
(pantomime and the two imitation tasks) but not on the action recognition tasks, which was
consistent with out prediction. (Table 4.8)

147
Table 4.8. Patterns of performance in Transitive Gestures
Apraxia Performance
Pattern
System
Affected Nature of Disruption RHP LHP
No Impairment N/A N/A 3 0
Sensory/perceptual
(P+/DI-/CI-/ID-)
Sensory/
Perceptual
Impaired ability to analyze visual
gestural and tool/object information 0 0
Conceptual
(P-/DI+/CI+/ID-) Conceptual
Impaired knowledge of action and
tool/object function 0 0
Production Resp Selection
(P-/DI+/CI+/ID+) Production
Impaired response selection and/or
image generation 0 0
Production Encoding
(P+/DI-/CI+/ID+) Production
Impaired encoding of visual gestural
information into working memory 0 0
Production Working
Memory
(P-/DI-/CI+/ID+)
Production Impaired working memory 0 0
Production Conduction
(P+/DI-/CI-/ID+) Production
Impaired ability to use visual
information in the control of movement 1 0
Production Ideomotor
(P-/DI-/CI-/ID+) Production
Impaired response organization and
control 4 3
Global
(P-/DI-/CI-/ID-)
Production
+
Conceptual
Impaired knowledge of action and
tool/object function + Impaired
response organization and control.
1 0
Other Patterns not described by Roy (1996)
P+/DI+/CI-/ID+ Production Impaired control of attention 0 1
P-/DI+/CI-/ID+ Production
Impaired response selection and/or
image generation and impaired control
of attention
0 0
P+/DI+/CI+/ID- Conceptual Impaired input conceptual system 0 0 P=Pantomime, DI= Delayed Imitation, CI=Concurrent Imitation, ID=Gesture Identification
(-) indicates impaired performance and (+) indicates normal performance.
Intransitive Gestures Patterns.
Three Gesture production Tasks of Intransitive Gestures (Pantomime, Delayed
Imitation, Concurrent Imitation) were used to determine the pattern of performance for each
patient. Four patterns of deficits were identified: General Production Impairment; Working
memory Impairment; Impaired ability to use Visual information in the control of Movement;
Impairment in Concurrent Imitation only. Two patients (1 LHD and 1 RHP) had no
impairment in any of the three tasks. Table 4.9 describes the number of patients in each
pattern by hemisphere presentation. The most common patterns were patterns where either

148
only Concurrent imitation was Impaired, or patterns where both concurrent and delayed
imitation were impaired. The side of presentation did not have an effect on the pattern of
performance.
Table 4.9. Patterns of Performance in Intransitive Gestures
Apraxia Performance Pattern System
Affected Nature of Disruption RHP LHP
No Impairment N/A N/A 1 1
Production Resp Selection
(P-/DI+/CI+)
Production or
Conceptual
Impaired response selection
and/or image generation 0 0
Production Encoding
(P+/DI-/CI+) Production
Impaired encoding of visual
gestural information into
working memory
0 0
Production Working Memory
(P-/DI-/CI+)
Production
and/or
Conceptual
Impaired working memory 1 0
Production Conduction
(P+/DI-/CI-)
Production or
Sensory/
Perceptual
Impaired ability to use visual
information in the control of
movement
3 1
Production Ideomotor
(P-/DI-/CI-) Production
Impaired response organization
and control 0 1
Other Patterns not described by Roy (1996)
P+/DI+/CI- Production Impaired control of attention 3 2
P-/DI+/CI- Production
Impaired response selection
and/or image generation and
impaired control of attention
0 0
P=Pantomime, DI= Delayed Imitation, CI=Concurrent Imitation,
(-) indicates impaired performance and (+) indicates normal performance.
Non-Representational Gestures Patterns
Delayed and Concurrent Imitation of Non-Representational Gestures were examined
to determine if patients were selectively impaired on one task but not the other. All patients
in our sample were impaired on both Concurrent and Delayed Imitation, with the exception
of one case who was not impaired on either task and one patient who was tested only on
Delayed Imitation of Non-Representational Gestures and was not Impaired on that task.

149
DISCUSSION
With respect to conceptual apraxia tasks, the LHP group was impaired on two naming
tasks: Tool Naming and Tool Naming by Action, while the RHP group was only impaired on
Action Identification, Action Identification by Tool and Gesture Error Recognition. Overall,
however, when the performance of both naming and identification tasks of gestures and tools
is taken together, patients show preserved knowledge of gestures and tools. On gesture
production tasks, contrary to expectations, both LHP and RHP patients were impaired,
consistent with our prediction LHP patients were more severely affected. The only task not
impaired in either group of patients was the Concurrent Imitation with Verbal Cueing. The
only tasks not impaired in RHP patients alone and impaired in LHP patients were Pantomime
of Intransitive Gestures and Delayed Imitation of Transitive Gestures. Finally, significant
differences between RHP and LHP patients were seen only in Pantomime of Intransitive
Gestures (where only LHP were impaired), Pantomime by Picture and Object Use (in both
tasks both patient groups were affected but LHP patients were significantly more affected).
With respect to task modality comparisons, performance on pantomime and imitation
of transitive gestures was less accurate than intransitive gestures. Pantomime accuracy was
lower than Concurrent Imitation in both transitive and intransitive gestures (Figure 4.1). The
addition of Verbal Cuing during Concurrent Imitation decreased imitation accuracy of the
patient groups, making performance more similar to Pantomime to Verbal Command, while
in controls verbal cueing did not change Imitation performance (Figure 4.2). Performance of
Concurrent and Delayed Imitation (Figure 4.3) was similar in all gesture types among both
control and patient participants. Delayed Imitation always slightly less accurate than
Concurrent Imitation, except in Non-Representational gestures where the LHP patients

150
performed less accurately on Concurrent Imitation than Delayed Imitation. Generally,
Imitation of Non-Representational gestures was least accurate and Imitation of Intransitive
gestures was most accurate. Finally, both patient groups improved their performance with
object use. Pantomime to Pictures of tools was performed with the same accuracy to
pantomime to Verbal Command in both controls and RHP patients, while the LHP patients
decreased their performance accuracy on Pantomime to Pictures relative to Pantomime to
Verbal Command (Figure 4.4)
To our knowledge, this is the first study to directly compare performance of CBS
patients with left versus right hemisphere presentation. In addition, no studies to date have
included such a comprehensive battery of apraxia assessments as ours to examine the
performance of a relatively large sample of CBS patients. Only two studies to date have
included a sample of patients equal or larger than ours (Peigneux et al., 2001; Soliveri et al.,
2003).
Conceptual Apraxia Tasks
First, our study demonstrated that, when all conceptual tasks are taken together,
patients were not impaired in their knowledge of gestures and tools. Few studies in the past
have included tasks assessing the conceptual knowledge of tools and gestures. Most studies
are suggestive of preserved ability to identify gestures and tools (Leiguarda et al., 1994;
Graham et al., 1999; Soliveri et al., 2005). One study in a relatively large sample of patients
(n=18) showed that patients were impaired relative to controls in their ability to discriminate
between meaningful and meaningless gestures and name meaningful gestures presented on a
video screen (Peigneux et al., 2001). These authors, however, did not examine the effect of
side of presentations on these tasks. Given our study suggested that LHP patients are

151
impaired on Action Naming, while RHP patients have deficits in Action Identification, it
may be the case that the effect in each task was driven by different set of patients: deficits in
Action naming by LHP patients, while deficits in Action Identification by RHP patients. .
LHP patients were impaired on two naming tasks: Tool Naming and Tool Naming by
Action. The deficits in Tool and Tool Naming by Action seem to stem from deficits in
naming. This was supported by the findings that most patients who were impaired on Tool
Naming were also impaired on WAB Naming. In addition, the evidence suggests that
patients who were impaired on some of the tool naming tasks had preserved ability to
identify tools through other modalities and therefore their knowledge of tools was not
affected. While most patients who were impaired on Tool Naming were also impaired on
WAB Naming, surprisingly, only one patient from the entire sample was impaired on the
BNT. The WAB Naming is a composite score that includes not only object naming, but also
word fluency, sentence completion and responsive speech. Therefore, WAB Naming taps
into other cognitive functions, such as executive control (Animal Fluency) and language
comprehension (sentence completion and responsive speech). The BNT includes only
assessment of naming of pictures. These differences in the two tests may lead to different
results in the two tests and may explain why some patients are impaired on WAB Naming,
but not on the BNT.
Naming deficits were also supported by the fact that Tool Naming correlated
significantly with WAB Naming. Naming deficits in CBS, are considered quite common
(Frattali, Grafman, Patronas, Makhlouf, & Litvan, 2000; Blake, Duffy, Boeve, Ahlskog, &
Maraganore, 2003) and in fact it has recently been suggested that primary progressive non-
fluent aphasia is often a precursor of CBS (Kertesz, Davidson, & Munoz, 1999). Aside from

152
naming deficits, LHP patients were reported to have significantly lower WAB AQ than
controls. Past studies assessing aphasia deficits in LHP vs. RHP patients have not shown
significant differences in aphasia, even though they did observe that LHP patients have lower
AQ scores than RHP patients (McMonagle, Blair, & Kertesz, 2006; Frattali et al., 2000). Our
sample consists of patients with longer onset to diagnosis duration and this may have
contributed to the fact that our results indicate a significant difference in WAB AQ.
With respect to other conceptual apraxia tasks, our study suggests that RHP patients
may have more trouble with action recognition tasks. Action recognition deficits could stem
from two sources: 1. Patients may have trouble processing visuospatial information or 2.
Patients may have lost their knowledge of actions. Past studies have reported that CBS
patients in fact do present with visuospatial processing deficits (Bak, Caine, Hearn, &
Hodges, 2006). However, our study also demonstrated that neither LHP nor RHP patients
were impaired in their ability to perform the Gesture Matching task, a task highly dependent
on visuospatial processing, requiring patients to match a gesture performed on a TV screen
with a gesture performed by the examiner. Therefore, it is somewhat unlikely that the deficits
we observed in action recognition tasks in the RHP group stemmed from visuospatial
processing difficulties. This leaves the option that patients may have lost their knowledge of
actions.
How might we infer whether there is a disruption to knowledge of actions? We need
to examine the stages in processing information in the two tasks assessing this knowledge,
Action Identification and Tool Name by Action. In Tool Name by Action patients are using
visual information to retrieve the semantic representation of an action and then the semantic
representation is used to retrieve the name of the tool. According to Heilman‟s model of

153
apraxia (Rothi, Ochipa, & Heilman, 1991) this would mean that patients move from visual
analysis to the action input lexicon to semantics and then to the verbal output lexicon (See
Figure 4.5). In Action Identification, however, the patients are given a verbal question (e.g.
Is the person pretending to be using a hammer to pound a nail?), while they are observing an
action. In this case, according to Heilman‟s model again, for the verbal question, the patient
needs to perform an auditory analysis, transfer that verbal information into the phonological
input lexicon and there retrieve the semantic representation of the action. For the visual
processing of the gesture, much like in Tool Name by Action, the patient is moving from
visual analysis to the action input lexicon to semantics. At this point the patient is presumed
to perform a match between the two representations (one retrieved from auditory information
and the other from visual) and decide whether the two representations are a match or not.
Alternatively, the patients may use the representation retrieved from the visual information to
retrieve a phonological response and match that in the verbal lexicon.
Considering these processing stages how might we infer the integrity of knowledge of
action in the three patients were impaired on Action Identification. Two of those were not
impaired in Tool Name by Action. We know that if they are not impaired on Tool Name by
Action the visual route for retrieving an action representation is intact. We also know that the
semantic representation retrieved in response to the visually presented gesture can be used to
retrieve the name of a tool, so the semantics to verbal output route is intact. Then we can
conclude that, patients are making a match between the representation retrieved from
auditory input and the representation retrieved from visual input in semantics and thus these
two patients must have a disconnect between the phonological input lexicon and the semantic
representation of the gesture. If there is a disconnect between the phonological input lexicon

154
and semantics, however, then these two patients should also not be able to pantomime either
and while this was confirmed in one of the cases, the other patient was not impaired on
Pantomime of Transitive Gestures to Verbal Command. It is difficult to explain this case. It
is possible that the low score in Action Identification in this patient was due to deficit other
than limb apraxia. A more detailed analysis should be done in the future to explain this.
A disconnection between the phonological input lexicon and semantics, however,
does not imply damaged conceptual action representations and from the successful
performance of the patients on Tool Naming by Action, we know that the conceptual
representation of actions is preserved in these two cases
One patient was impaired on both Action Identification and Tool Name by Action,
but not on Gesture Matching (suggesting preserved visuospatial processing) and in this case
the patient may have in fact lost the semantic knowledge associated with gestures. This is the
only case out of all 17 patients where impairment in conceptual gesture and tool knowledge
is observed.

155
Figure 4.5 Tool Naming by Action and Action ID routes.
Auditory/Verbal Input Visual/Gestural Input
Auditory Analysis Visual Analysis
Phonological Input lexicon Action Input Lexicon
Semantics
Verbal Output Lexicon
Apraxia Gesture Production Tasks
Unlike performance on Conceptual tasks, both LHP and RHP patients were impaired
in their ability to execute gestures. Our initial prediction was that LHP patients would be
more impaired on gesture execution tasks, given the role of the left hemisphere in apraxia,
together with past reports that deficits in apraxia may be more prominent in LHP patients
(Leiguarda, Merello, & Balej, 2000). Our hypothesis was confirmed, with LHP patients
consistently obtaining lower scores than RHP patients. Interestingly, though the difference in
performance between the two patient groups was not significant in most tasks (with the
exception of two task modalities: Pantomime by Picture and Object Use). Further,
Pantomime of Intransitive Gestures and Delayed Imitation of Transitive Gestures were the
only tasks where only LHP patients were significantly impaired. It should be noted that
unlike Pantomime of Intransitive Gestures, where performance of the RHP patients was more
accurate than that for the LHP patients and comparable to that of the controls, in Delayed
Imitation of Transitive Gestures, the performance of RHP and LHP patients was similar. In
this case both patient groups were equally less accurate than controls, but only the
performance of the LHP patients was significantly less accurate than the controls. Therefore,
while in Pantomime of Intransitive gestures, the lack of effect among the RHP patients seems

156
to be due to lack of deficit in the group, the lack of effect seen in the Delayed Imitation of
Intransitive Gestures seems to be due to a lack of power. Given the progressive nature of the
disorder, it is possible that patients initially have more asymmetrical brain degeneration, but
as the disease progresses it most likely affects both hemispheres. Therefore, patients with
initial left body presentation (i.e. right hemisphere presentation) will also suffer from
degeneration in their left hemisphere, which further contributes to their deficits. In addition,
apraxia has also been reported after right hemisphere damage in stroke patients (Roy et al.,
2000; Heath, Roy, Black, & Westwood, 2001; Haaland & Flaherty, 1984). Thus, it is likely
that in some patients‟ the right hemisphere degeneration may contribute to some extent to
their gesture production deficits. Finally, it has been suggested that certain apraxia tasks,
such as imitation of non-representational gestures involve bilateral structures in the dorsal
stream and these, therefore, would be affected in both patient groups (Buxbaum et al., 2007).
This was confirmed also by our finding that in concurrent imitation of non-representational
gestures both LHP and RHP patients were equally impaired. Interestingly, while concurrent
imitation consistently was performed better than delayed imitation, in delayed imitation of
non-representational gestures the LHP patients significantly decreased their accuracy. This
may suggest that the dual task demands of processing visual information and executing a
motor response may be especially great for the left hemisphere when the direct route to
imitation is being used.
Conceptual knowledge of tools and gestures, however, has been suggested to be
stored in the left hemisphere (inferior parietal lobule) (Heilman et al., 1982; Buxbaum et al.,
2007) and therefore, even though no receptive deficits are observed, LHP patients would

157
have additional deficits affecting the ability to use that information for the performance of
meaningful gestures, which may explain their greater deficits in gesture production.
In a recent review of the literature, we suggested that while it is somewhat unclear,
the evidence weighs in on imitation being more affected in CBS patients than pantomime
(Stamenova et al, 2009). Our current analysis reveals, however, that in fact, pantomime
seems to be significantly more affected than imitation. This is consistent with stroke studies
demonstrating pantomime deficits to be larger than imitation deficits (Roy et al., 2000; Heath
et al., 2001). It is interesting to note here, however, that in stroke patients the differences seen
between pantomime and imitation are much larger than those in CBS. Better performance on
imitation of meaningful gestures, together with lower pantomime performance, which can
only be done through the semantic route, suggests that when imitating, patients may be using
the direct (non-semantic) route of imitation. If patients were imitating through the indirect
(semantic) route of imitation, i.e. observing an action recognizing that action and retrieving
an action memory that they in turn use to imitate, then their performance on imitation would
have been at a similar level to that in pantomime (Rumiati et al., 2005). In a further attempt
to determine which route of imitation is more affected in CBS, we asked patients to imitate
an action while a verbal instruction was also provided. Providing a verbal cue to patients
should facilitate access to semantics and allow patients to use the indirect route to imitation.
Deficits in imitation of meaningful gestures could stem from 1. deficits in the
sensory/perceptual system preventing them from recognizing the visually presented gesture,
2. deficits in direct visuomotor transformation, not allowing them to convert the visual
information they observe to movement, or 3. deficits in both systems. If deficits are arising
because of inability to recognize the movement and, thus, not gaining access to the semantic

158
route, then providing patients with a verbal cue would allow them to do gain access to the
semantic route. Unfortunately, this task included only transitive gestures, but it showed that
once a verbal cue was introduced during imitation, patients decreased their performance
accuracy relative to their performance on imitation only. In fact, their performance largely
resembled that of pantomime, suggesting that once the verbal cue was introduced patients
reversed back to pantomiming an action rather than visually imitating it. Thus they seemed to
be going either through the indirect route of imitation or simply to be pantomiming the action
(i.e. using the verbal cue to retrieve the memory representation of that action) rather than
direct visuomotor transformation in imitation. This is surprising given imitation seems to be
easier for these patients and may suggest that once a verbal cue is introduced patients are
forced to go through that route.
If patients have greater deficits in the indirect route to imitation, as opposed to the
direct route, we should expect that imitation of meaningful gestures to be less accurate than
imitation of meaningless gestures. While in imitation of meaningful gestures patients have
both routes to imitation to choose from, imitation of meaningless gestures can only be done
through the direct visuomotor transformation route. However, our results showed that
patients were significantly more affected in their ability to imitate meaningless gestures,
while transitive gestures were performed with higher accuracy. This suggests that CBS
affects mostly the direct route of imitation. This finding supports Buxbaums‟s proposal that
CBS patients are specifically affected in the dorsal visual stream of processing and as such
are quite deficient in gesture imitation through the direct visual route (Buxbaum et al., 2007).
The conclusion that CBS affects mostly the direct route to imitation, however, is in
contradiction to our hypothesis that imitation of transitive gestures is facilitated by access to

159
the direct route to imitation. Better imitation of meaningful gestures might suggest that
access to semantics facilitates performance rather than deters it.
Why would then imitation accuracy decrease with the introduction of verbal cueing?
If the direct route to imitation is more affected by CBS than the indirect route, then the
improvement in imitation of transitive gestures, relative to pantomime, could be facilitated by
allowing access to semantics, rather than access to the direct route. It is possible that visual
presentation of gestures facilitates access to semantics better than verbal instruction. This is
consistent with Heilman and Rothi‟s model (Heilman et al., 1993) proposing the existence of
two separate inputs to semantics: a visual input praxicon that can be used to retrieve a
semantic representation through visual input and a phonological input lexicon that can be
used to retrieve a semantic representation through verbal input. Thus, in patients with
impairments in the verbal input lexicon, performance in response to visual presentation of
gestures may simply improve by having been given access to the visual input praxicon, as
opposed to the verbal one.
In pantomime to verbal cueing, both visual and verbal instructions are available to
perform the task. The fact that in the performance on Concurrent Imitation with Verbal
Cueing was more similar to the performance on pantomime as opposed to imitation, suggests
that the patients followed the verbal cue and used the semantic route, rather than used the
visual information for direct visuomotor transformations. This is surprising, given the
patients‟ imitation performance was more accurate. It is possible that access to the semantic
route, provided by the verbal cue, blocked the response via the nonsemantic route, which
would be consistent with Chainay and Humphreys (2002) convergent-route model suggesting
the possibility that certain routes of action can block others.

160
In regard to comparisons between transitive and intransitive gesture types in
pantomime and imitation, past studies are again somewhat equivocal. Studies have reported
either equal impairment on both transitive and intransitive gestures (Leiguarda et al., 2003;
Jacobs et al., 1999a; Peigneux et al., 2001; Buxbaum et al., 2007), or greater impairments on
transitive than intransitive gestures (Pharr et al., 2001; Salter et al., 2004; Chainay et al.,
2003). Our study supports the latter finding with transitive gestures being more affected,
which is consistent with the stroke literature (Roy et al., 1991; Almeida, Black, & Roy,
2002).It has been proposed that intransitive gestures are better practiced in everyday life,
since they are used in everyday life in nonverbal communication and this practice makes
them less susceptible to deterioration (Mozaz, Rothi, Anderson, Crucian, & Heilman, 2002)
Finally, with respect to transitive gestures, patients seemed to improve significantly in
their performance when given the actual tool. This has been reported in the past in both CBS
(Jacobs et al., 1999a; Graham et al., 1999; Spatt et al., 2002; Leiguarda et al., 2003) and
stroke patients (Clark et al., 1994; Westwood et al., 2001) and it is likely that the additional
cues provided by the tactile stimulation of the object on the hand guide the movement,
leading to improved performance. Differences between Pantomime to Verbal Command and
Pantomime by Picture were not significant, even though performance accuracy decreased in
Pantomime by Picture, relative to pantomime. In fact, we had three cases of patients who
were impaired on Pantomime by Picture but not to Pantomime of Transitive Gestures. Such
performance has been reported in the past in a patient with left parietal stroke by Riddoch,
Humphreys and Price (1989) and later Rumiati and Humphreys (1998) proposed that aside
from a semantic route to transitive gesture performance, there is also a visual route to action,
that is activated in response to a visual presentation of objects and that these two systems can

161
be selectively damaged. In addition, these authors proposed that the direct visual route to
action may be mediated by the dorsal stream, whereas the semantic route to action is
mediated by the ventral stream. Therefore, the greater impairment in pantomime to picture
relative to pantomime is consistent with the dorsal stream damage reported in CBS patients.
Apraxia Patterns
Finally, we would like to discuss the patterns of deficits observed in CBS patients for
both transitive and intransitive gestures. In transitive gestures (Table 4.8), we see that most
patients present with a form of ideomotor apraxia, where both pantomime, concurrent and
delayed imitation are impaired, while conceptual knowledge of tools and actions is spared.
This is consistent with the general finding that patients were not impaired on conceptual
tasks. Such pattern of impairment suggests that most patients with CBS have deficits in
response organization and control, or the final stages of motor production. This pattern of
deficit seems to be as common in RHP and LHP patients. RHP patients, however seem to be
more likely to present with no impairment in transitive gesture. Single cases of four other
patterns were also observed, only one of which involved deficits in conceptual knowledge.
In intransitive gestures (Table 4.9), the patterns observed were somewhat different
than those in transitive gestures. The two most common deficits were cases where patients
were impaired only on concurrent and delayed imitation and not pantomime, as well as cases
where patients were impaired only on concurrent imitation. Selective impairment on
concurrent imitation was not initially proposed by Roy (1996) as a likely pattern, but recent
evidence in stroke has suggested that it does occur (see Chapter 3). We have proposed that
concurrent imitation may pose greater demands on working memory than delayed imitation,
because in concurrent imitation the participant is effectively performing a dual-task:

162
following the visual cues while executing a motor response. Dual-task deficits have been
reported in stroke (Marshall, Grinnell, Heisel, Newall, & Hunt, 1997) and thus may
contribute to deficits in concurrent imitation but not delayed imitation for some patients. In
addition, selective impairments on imitation tasks and not pantomime, suggest deficits in the
direct route of imitation, which was supported by deficits in nonrepresentational tasks.
Finally, cases with both pantomime and imitation deficits were also observed but they were
rarer. Again, in intransitive gestures, it seems like patterns are equally likely to occur in
patients with left as well as right initial presentation.
In summary, the study suggests that CBS patients rarely show deficits in conceptual
knowledge of actions and tools, as evidenced by preserved tool and action identification.
LHP patients showed deficits in action and tool naming tasks, which are possibly due to
naming deficits. RHP patients, on the other hand, showed some deficits in Action
Identification, but together with preserved Tool Naming by Action and Gesture Recognition,
may suggest selective deficits in visual gestural processing). In both cases, while selective
conceptual tasks deficits were present, the overall picture suggests preserved conceptual
representations of tools and actions. With respect to gesture production deficits, however,
both LHP and RHP patients were affected, with more severe deficits in patients with LHP.
Detailed analysis of various task modalities and gesture types, suggests that patients have
deficits in response organization and control, affecting both pantomime and imitation
performance. In addition, deficits in imitation are exacerbated when patients use the direct
route to imitation.

163
REFERENCES
Almeida, Q. J., Black, S. E., & Roy, E. A. (2002). Screening for apraxia: a short
assessment for stroke patients. Brain & Cognition, 48, 253-258.
Bak, T. H., Caine, D., Hearn, V. C., & Hodges, J. R. (2006). Visuospatial functions in
atypical parkinsonian syndromes. Journal of Neurology Neurosurgery and Psychiatry, 77,
454-456.
Blake, M. L., Duffy, J. R., Boeve, B. F., Ahlskog, J. E., & Maraganore, D. M. (2003).
Speech and language disorders associated with corticobasal degeneration. Journal of Medical
Speech-Language Pathology, 11, 131-146.
Blin, J., Vidailhet, M. J., Pillon, B., Dubois, B., Feve, J. R., & Agid, Y. (1992).
Corticobasal Degeneration - Decreased and Asymmetrical Glucose Consumption As Studied
with Pet. Movement Disorders, 7, 348-354.
Boeve, B. F., Lang, A. E., & Litvan, I. (2003). Corticobasal degeneration and its
relationship to progressive supranuclear palsy and frontotemporal dementia. Annals of
Neurology., 54, S15-S19.
Buxbaum, L. J., Kyle, K., Grossman, M., & Coslett, H. B. (2007). Left inferior
parietal representations for skilled hand-object interactions: Evidence from stroke and
corticobasal degeneration. Cortex, 43, 411-423.
Chainay, H. & Humphreys, G. W. (2002). Neuropsychological evidence for a
convergent route model for action. Cognitive Neuropsychology, 19, 67-93.

164
Chainay, H. & Humphreys, G. W. (2003). Ideomotor and ideational apraxia in
corticobasal degeneration: A case study. Neurocase., 9, 177-186.
Clark, M. A., Merians, A. S., Kothari, A., Poizner, H., Macauley, B., Gonzalez, R. L.
J. et al. (1994). Spatial planning deficits in limb apraxia. Brain, 117, 1093-1106.
Cubelli, R., Marchetti, C., Boscolo, C., & Della Sala, S. (2000). Cognition in action:
Testing a model of limb apraxia. Brain and cognition, 44, 144-165.
Dickson, D. W., Bergeron, C., Chin, S. S., Duyckaerts, C., Horoupian, D., Ikeda, K.
et al. (2002). Office of Rare Diseases neuropathologic criteria for corticobasal degeneration.
Journal of Neuropathology & Experimental Neurology, 61, 935-946.
Dickson, D. W., Liu, W.-K., Ksiezak-Reding, H., & Yen - SH. (2000).
Neuropathologic and Molecular Considerations. Litvan, I., Goetz, C., and Lang, A. E.
Corticobasal Degeneration and Related Disorders. Advances in Neurology 82[2], 9.
Ref Type: Journal (Full)
Donkervoort, M., Dekker, J., van den Ende, E., Stehmann-Saris, J. C., & Deelman, B.
G. (2000). Prevalence of apraxia among patients with a first left hemisphere stroke in
rehabilitation centres and nursing homes. Clinical Rehabilitation., 14, 130-136.
Folstein, M. F., Folstein, S. E., & Mchugh, P. R. (1975). Mini-Mental State - Practical
Method for Grading Cognitive State of Patients for Clinician. Journal of psychiatric
research, 12, 189-198.

165
Frattali, C. M., Grafman, J., Patronas, N., Makhlouf, F., & Litvan, I. (2000).
Language disturbances in corticobasal degeneration. Neurology.Vol.54(4)()(pp 990-992),
2000.Date of Publication: 22 FEB 2000., 990-992.
Geschwind, N. (1975). The Apraxias: Neural Mechanisms of Disorders of Learned
Movements. American Scientist, 63, 188-195.
Goldenberg, G. & Hagmann, S. (1997). The meaning of meaningless gestures: a
study of visuo-imitative apraxia. Neuropsychologia, 35, 333-341.
Graham, N. L., Zeman, A., Young, A. W., Patterson, K., & Hodges, J. R. (1999).
Dyspraxia in a patient with corticobasal degeneration: the role of visual and tactile inputs to
action. Journal of Neurology Neurosurgery and Psychiatry, 67, 334-344.
Grimes, D. A., Lang, A. E., & Bergeron, C. B. (1999). Dementia as the most common
presentation of cortical-basal ganglionic degeneration. Neurology., 53, 1969-1974.
Haaland, K. Y. & Flaherty, D. (1984). The different types of limb apraxia errors made
by patients with elft vs. right hemispehre damage. Brain and cognition, 3, 370-384.
Heath, M., Roy, E. A., Black, S. E., & Westwood, D. A. (2001). Intransitive limb
gestures and apraxia following unilateral stroke. Journal of clinical and experimental
neuropsychology, 23, 628-642.
Heath, M., Roy, E. A., Westwood, D., & Black, S. E. (2001). Patterns of apraxia
associated with the production of intransitive limb gestures following left and right
hemisphere stroke. Brain & Cognition, 46, 165-169.

166
Heilman, K. M. & Rothi, L. J. (1993). Apraxia. In Clinical Neuropsychology (pp.
141-163). New York, NY: Oxford University press Inc.
Heilman, K. M., Rothi, L. J., & Valenstein, E. (1982). Two forms of ideomotor
apraxia. Neurology, 32, 342-346.
Jacobs, D. H., Adair, J. C., Macauley, B., Gold, M., Gonzalez, R. L. J., & Heilman,
K. M. (1999a). Apraxia in corticobasal degeneration. Brain & Cognition, 40, 336-354.
Jacobs, D. H., Adair, J. C., Williamson, D. J., Na, D. L., Gold, M., Foundas, A. L. et
al. (1999b). Apraxia and motor-skill acquisition in Alzheimer's disease are dissociable.
Neuropsychologia, 37, 875-880.
Kaplan, E. (1983). The Boston Naming Test. (2nd ed.) Philadelphia: Lea & Febiger.
Kertesz, A. (1982). Western Aphasia Battery. San Antonio, TX: The psychological
Corporation.
Kertesz, A., Davidson, W., & Munoz, D. G. (1999). Clinical and pathological overlap
between frontotemporal dementia, primary progressive aphasia and corticobasal
degeneration: the Pick complex. Dementia & Geriatric Cognitive Disorders., 10, 46-49.
Kertesz, A., Martinez-Lage, P., Davidson, W., & Munoz, D. G. (2000). The
corticobasal degeneration syndrome overlaps progressive aphasia and frontotemporal
dementia. Neurology., 55, 1368-1375.
Kertesz, A. & Poole, E. (1974). The aphasia quotient: the taxonomic approach to
measurement of aphasic disability. Canadian Journal of Neurological Sciences, 1, 7-16.

167
Leiguarda, R. (2001). Limb apraxia: cortical or subcortical. NeuroImage, 14, S137-
S141.
Leiguarda, R., Lees, A. J., Merello, M., Starkstein, S., & Marsden, C. D. (1994). The
nature of apraxia in corticobasal degeneration. Journal of Neurology, Neurosurgery &
Psychiatry, 57, 455-459.
Leiguarda, R., Merello, M., & Balej, J. (2000). Apraxia in corticobasal degeneration.
Advances in Neurology, 82, 103.
Leiguarda, R. C., Merello, M., Nouzeilles, M. I., Balej, J., Rivero, A., & Nogues, M.
(2003). Limb-kinetic apraxia in corticobasal degeneration: Clinical and kinematic features.
Movement Disorders, 18, 49-59.
Marshall, S. C., Grinnell, D., Heisel, B., Newall, A., & Hunt, L. (1997). Attentional
deficits in stroke patients: A visual dual task experiment. Archives of Physical Medicine and
Rehabilitation, 78, 7-12.
McMonagle, P., Blair, M., & Kertesz, A. (2006). Corticobasal degeneration and
progressive aphasia. Neurology, 67, 1444-1451.
Merians, A. S., Clark, M., Poizner, H., Jacobs, D. H., Adair, J. C., Macauley, B. et al.
(1999). Apraxia differs in corticobasal degeneration and left-parietal stroke: A case study.
Brain & Cognition, 40, 314-335.

168
Mozaz, M., Rothi, L. J., Anderson, J. M., Crucian, G. P., & Heilman, K. M. (2002).
Postural knowledge of transitive pantomimes and intransitive gestures. Journal of the
International Neuropsychological Society, 8, 958-962.
Peigneux, P., Salmon, E., Garraux, G., Laureys, S., Willems, S., Dujardin, K. et al.
(2001). Neural and cognitive bases of upper limb apraxia in corticobasal degeneration.
Neurology, 57, 1259-1268.
Pharr, V., Uttl, B., Stark, M., Litvan, I., Fantie, B., & Grafman, J. (2001). Comparison
of apraxia in corticobasal degeneration and progressive supranuclear palsy. Neurology., 56,
957-963.
Rebeiz, J. J., Kolodny, E. H., & Richardson, E. P., Jr. (1968). Corticodentatonigral
degeneration with neuronal achromasia. Archives of Neurology., 18, 20-33.
Riddoch, M. J., Humphreys, G. W., & Price, C. J. (1989). Routes to Action -
Evidence from Apraxia. Cognitive Neuropsychology, 6, 437-454.
Rothi, L. J., Ochipa, C., & Heilman, K. M. (1991). A Cognitive Neuropsychological
Model of Limb Praxis. Cognitive Neuropsychology, 8, 443.
Roy, E. A. (1996). Hand Preference, Manual Assymetries, and Limb Apraxia. In
D.Elliot (Ed.), Manual Asymmetries in Motor Control (pp. 215). Boca Raton, FL: CRC Press.
Roy, E. A., Heath, M., Westwood, D., Schweizer, T. A., Dixon, M. J., Black, S. E. et
al. (2000). Task demands and limb apraxia in stroke. Brain and cognition, 44, 253-279.

169
Roy, E. A., Square-Storer, P., Hogg, S., & Adams, S. (1991). Analysis of task
demands in apraxia. International Journal of Neuroscience, 56, 177-186.
Rumiati, R. I. & Humphreys, G. W. (1998). Recognition by action: Dissociating
visual and semantic routes to action in normal observers. Journal of Experimental
Psychology-Human Perception and Performance, 24, 631-647.
Rumiati, R. I., Weiss, P. H., Tessari, A., Assmus, A., Zilles, K., Herzog, H. et al.
(2005). Common and differential neural mechanisms supporting imitation of meaningful and
meaningless actions. Journal of Cognitive Neuroscience.17(9):1420-31.
Salter, J. E., Roy, E. A., Black, S. E., Joshi, A., & Almeida, Q. (2004). Gestural
imitation and limb apraxia in corticobasal degeneration. Brain & Cognition, 55, 400-402.
Soliveri, P., Piacentini, S., & Girotti, F. (2005). Limb apraxia in corticobasal
degeneration and progressive supranuclear palsy. Neurology, 64, 448-453.
Soliveri, P., Piacentini, S., Paridi, D., Testa, D., Carella, F., & Girotti, F. (2003).
Distal-proximal differences in limb apraxia in corticobasal degeneration but not progressive
supranuclear palsy. Neurological Sciences., 24, 213-214.
Spatt, J., Bak, T., Bozeat, S., Patterson, K., & Hodges, J. R. (2002). Apraxia,
mechanical problem solving and semantic knowledge: Contributions to object usage in
corticobasal degeneration. Journal of Neurology., 249, 601-608.
Steinberg, B. A., Bieliauskas, L. A., Smith, G. E., Langellotti, C., & Ivnik, R. J.
(2005). Mayo's older Americans normative studies: Age- and IQ-adjusted norms for the

170
Boston Naming Test, the Mae Token Test, and the Judgment of Line Orientation Test.
Clinical Neuropsychologist, 19, 280-328.
Westwood, D. A., Schweizer, T. A., Heath, M. D., Roy, E. A., Dixon, M. J., & Black,
S. E. (2001). Transitive gesture production in apraxia: visual and nonvisual sensory
contributions. Brain & Cognition, 46, 300.
Zhang, L., Murata, Y., Ishida, R., Saitoh, Y., Mizusawa, H., & Shibuya, H. (2001).
Differentiating between progressive supranuclear palsy and corticobasal degeneration by
brain perfusion SPET. Nuclear Medicine Communications, 22, 767-772.

171
CHAPTER 5: PROGRESSION OF LIMB APRAXIA IN CORTICOBASAL
SYNDROME (CBS): A SERIES OF CASE STUDIES
ABSTRACT
Corticobasal Syndrome is neurodegenerative disorder characterized by asymmetrical
akinetic-rigid syndrome and cognitive decline, especially limb apraxia. Limb apraxia refers
to impaired ability to perform purposeful skilled movements. Roy (1996) proposes three
processing routes for praxis: sensory/perceptual (processes sensory information regarding
tools and gestures), conceptual (knowledge of tools and gestures), and production (execution
of hands movement). If the function of any of these routes is disrupted by disease, different
patterns of apraxia deficits emerge. Past studies of apraxia have shown that CBS patients
often have deficits in pantomime and imitation of gestures, while the conceptual knowledge
of tools and gestures is usually preserved. No studies to date have examined how the apraxia
deficits of CBS patients change over time as the disease progresses. In addition, the evolution
of apraxia patterns throughout disease progression has not been previously described.
The current study described 7 CBS cases (3 with left (LHP) and 4 with right (RHP)
hemisphere predominance, i.e. contralateral to the side of initial motor symptoms presented).
A comprehensive battery of assessments was administered, including both gesture production
tasks and tasks assessing the conceptual knowledge of gestures and tools. The study showed
that different domains of praxis may progress differently in CBS. Conceptual knowledge was
often preserved until later in the course, and in our sample over half the patients retained
their knowledge of tools and gestures at the last assessment. The patients who lost knowledge
of tools and gestures also showed a general cognitive decline as measured by a standardized
neuropsychological battery, including the MMSE, Digit Span, WAB, Boston Naming.
Performance on all gesture production tasks usually deteriorated as the disease progressed

172
and rarely remained the same or improved with time. Deficits in pantomime and imitation
developed in all seven cases. Intransitive gestures were least affected, while non-
representational gestures were affected the most.

173
INTRODUCTION
Corticobasal Syndrome is a neurological disorder, characterized by a progressive
neurodegenerative process involving the cortex and the basal ganglia (Dickson et al., 2002).
Based on the clinical diagnostic criteria summarized by Boeve, Lang, & Litvan (2003), the
following CBS diagnostic criteria have been established: 1) Insidious onset and progressive
course of disease; 2) No identifiable cause (e.g., tumor, infarct); 3) Cortical dysfunction as
reflected by at least one of the following: Focal or asymmetrical ideomotor apraxia, Alien
limb phenomenon, Cortical sensory loss, Visual or sensory hemineglect, Constructional
apraxia, Focal or asymmetric myoclonus or Apraxia of speech/nonfluent aphasia, 4)
Extrapyramidal dysfunction as reflected by at least one of the following: Focal or
asymmetrical appendicular rigidity lacking prominent and sustained L-dopa response or
Focal or asymmetrical appendicular dystonia. Boeve et al. (2003) specify the following
supportive features: 1) Variable degrees of focal or lateralized cognitive dysfunction, with
relative preservation of learning and memory, on neuropsychometric testing, 2) Focal or
asymmetric atrophy on computed tomography or magnetic resonance imaging, typically
maximal in parietofrontal cortex or 3) Focal or asymmetric hypoperfusion on single-photon
emission computed tomography and positron emission tomography, typically maximal in
parietofrontal cortex, basal ganglia and/or thalamus. While CBS is characterized by both
motor and cognitive symptoms, one can precede the other. Limb apraxia is one of the most
common cognitive symptoms in CBS and patients often complain of “clumsiness with
objects” and decreased dexterity early on in its course.
Limb apraxia is a neurological disorder characterized by an inability to perform
purposeful skilled movements (Geschwind, 1975). It is often defined by exclusion: an

174
inability to perform skillful movements not caused by weakness, dystonia, tremor,
myoclonus, deafferentiation, ataxia, inattention, poor language understanding, or
unwillingness to cooperate (Heilman & Rothi, 1993). It is also often defined as an inability to
pantomime (perform gestures from memory) or imitate gestures (Roy, 1996). Pantomime and
imitation are the two most commonly used task modalities. In addition, while apraxia
assessments most commonly involve tool related gestures (called transitive gestures), non-
tool symbolic gestures (called intransitive gestures) and meaningless gestures are also used in
more comprehensive assessments (referred to as non-representational gestures). Limb apraxia
has been most commonly studied in the context of stroke. It is a disorder that is more
common after left hemisphere stroke (Heilman et al., 1993), but it may also result from a
right hemisphere stroke (Roy et al., 2000; Heath, Roy, Westwood, & Black, 2001). Roy
(1996) proposes that there are three systems involved in the control of learned skilled
movement: the conceptual system (which stores our knowledge of tools and gestures), the
production system (responsible for response selection and action generation and control) and
the sensory/perceptual system (processes auditory and/or visual information in response to
which an action is generated) (See Chapter 1 for a detailed description of the model).
While limb apraxia is quite common in CBS, few studies have examined
comprehensively the characteristics of the limb apraxia deficits in CBS. This is partly due to
the fact that CBS is a rare neurological disorder (less than 1% of patients with parkinsonism)
(Togasaki & Tanner, 2000) first described in the 1960‟s (Rebeiz, Kolodny, & Richardson,
Jr., 1967), but also because limb apraxia is one of the few major cognitive-motor deficits (if
not the only one) that does not have a comprehensive standardized battery that is well
recognized by both clinicians and researchers. Based on evidence to date, combined with

175
some findings we recently reported (Chapter 4), the following conclusions can be drawn in
regard to the overall deficits that CBS patients manifest. First, with respect to conceptual
knowledge of tools and actions assessments, patients rarely show deficits, suggesting that the
conceptual system storing that information is intact (Leiguarda, Lees, Merello, Starkstein, &
Marsden, 1994; Salter, Roy, Black, Joshi, & Almeida, 2004; Jacobs et al., 1999; Soliveri,
Piacentini, & Girotti, 2005). My studies have demonstrated that CBS patients with right
hemisphere predominance (RHP) may have some deficits in Gesture Identification tasks ,
while left hemisphere presentation (LHP) patients have deficits in certain apraxia naming
tasks, but overall the evidence suggests that the knowledge of actions and tools of both CBS
patients is preserved (Chapter 4). Second, generally, both RHP and LHP patients are
impaired in all aspects of gesture production, with LHP patients more severely affected
(Chapter 4). Third, the evidence with respect to transitive versus intransitive gestures is
somewhat equivocal, with some studies showing transitive gestures to be more impaired
(Pharr et al., 2001; Salter et al., 2004; Chainay & Humphreys, 2003), while others suggesting
no clear differences (Leiguarda et al., 2003; Jacobs et al., 1999; Peigneux et al., 2001;
Buxbaum, Kyle, Grossman, & Coslett, 2007), our studies suggest that transitive gestures are
more affected than intransitive (Chapter 4). Fourth, imitation of non-representational
(meaningless) gestures is usually as affected as imitation of representational gestures
(Merians et al., 1999; Spatt, Bak, Bozeat, Patterson, & Hodges, 2002; Salter et al., 2004;
Leiguarda et al., 2003; Buxbaum et al., 2007), but our recent findings suggest that non-
representational gestures may be more affected (Chapter 4). Fifth, our group (Chapter 4), as
well as others (Jacobs et al., 1999; Graham, Zeman, Young, Patterson, & Hodges, 1999;
Spatt et al., 2002; Leiguarda et al., 2003), have shown that patients improve in their

176
performance when pantomiming with the actual tools, as opposed to pantomiming without
tools.
While a number of group analysis studies have been done comparing performance on
various tasks, no studies to date have examined the progression of deficits in CBS through a
case series. CBS is a neurodegenerative disorder and the severity of the apraxia deficits will
increase over time, but in the absence of progression studies, it is unclear whether all the
patients‟ abilities deteriorate in a similar fashion. That is, it is not clear whether patients‟
performance deteriorates similarly across all apraxia domains, or whether certain tasks are
affected more than others. In addition, following Roy‟s model (1996), we wanted to
determine how the patterns of deficits in CBS may change over time. To answer these
questions, the goal of the current project was to examine the progression of limb apraxia
deficits in a series of CBS patients and to track their performance in all areas of praxis
functioning across time. Given, the progressive nature of the disease it was expected that
with time, patients performance on gesture production tasks, such as pantomime and
imitation, would deteriorate. Concerning changes in conceptual task performance, it was not
as clear whether conceptual deficits in gesture and tool knowledge will evolve over time, but
given the general cognitive decline that can be seen in some patients as the disease
progresses, it was thought that eventually conceptual deficits in gesture and tool knowledge
would likely emerge.
METHODS
Participants
Seven patients with Corticobasal Syndrome (CBS) participated in the study. All
patients were recruited from the L.C. Campbell Cognitive Neurology Clinic at Sunnybrook

177
Health Sciences Centre, an academic health care facility at the University of Toronto. All
patients met Boeve et al.‟s (2003) diagnostic criteria. Patients were included in the study if
they had no history of a neurological impairment (other than the diagnosis of CBS in the case
of CBS patients), and had no history of alcohol or drug abuse, psychiatric or movement
disorders (other than the extrapyramidal features in CBS patients), or any peripheral
condition (e.g., arthritis) which may compromise motor function. All patients needed to have
a good level of comprehension, so that they could follow instructions. Patients had at least 8
years of formal education andwere younger than 90 years of age. Four patients had a right
hemisphere presentation (RHP) and three had a left hemisphere presentation (LHP). All
patients were right handed. Two patients were seen twice for assessments, three patients were
assessed 3 times and one patient was assessed four times. The length of participation ranged
from 12 months to 50 months. For detailed description of age, education, sex, number of
visits, duration of participation in the study and MMSE scores for each patient, please refer
to Table 5.1. For a summary of the initial clinical presentation of each patient see Table 5.2.
For a detailed description of the history and the presentation of each patient, please refer to
Appendix 5A. Limb apraxia was assessed in both arms if possible. Consent to participate in
the study was obtained from all participants and the study was approved by the Research
Ethics Board at Sunnybrook Health Sciences Centre and at the University of Waterloo.

178
Table 5.1: Characteristics of the patients
Patient ID Sex YOE # of
Visits
Months since
Onset at 1st
Visit
Months since
Onset at Last
Visit
Duration in the
Study (months)
MMSE
at 1st
Visit
MMSE
at Last
Visit
Age at
1st Visit
Age at
Last
Visit
58-RHP F 10 3 35 80 45 27 14 60 64
62-LHP F 12 2 65 79 14 13 10 67 69
68-RHP M 17 4 97 147 50 29 26 73 77
71-RHP F 13 2 25 37 12 19 16 72 73
73-RHP M 17 3 39 64 25 29 26 62 64
76-LHP F 8 3 52 83 31 27 22 79 82
132-LHP F 10 3 48 75 26 29 30 74 76
Table 5.2. Summary of clinical presentation on initial exam.
Rig
idit
y
Co
rtic
al S
nes
ory
Lo
ss
Ap
rax
ia
Ath
eto
sis
Ali
en L
imb
Ass
ym
etri
c
Rig
idit
y
Lim
b D
yst
on
ia
My
ocl
on
us
Ear
ly D
emen
tia
Ap
has
ia
Sp
eech
Vis
uo
spat
ial
Ex
ecit
ive
Oth
er D
emen
tia
Su
pra
nu
clea
r P
alsy
Tre
mo
r
58-RHP + + + + Levitation
only + - + + + + + + inattention - -
62-LHP + + + n/a - + - + + + + + + memory loss - -
68-RHP + + + + Levitation
only + + + - - - + + - - action only
71-RHP + - + n/a Levitation
only + + - - + + + +
memory loss/
inattention
Present; no vertical
OKNs
rest/postural/
action
73-RHP + + + + Possible + + + - - - - + - - -
76-LHP + + + n/a - + - - + + + + + - Present; limited up gaze postural/action
132-LHP + + + - - + + - - - - - - - - postural/action

179
Tests and Procedures
Limb Apraxia Assessments
Eight transitive (involving the use of tools), eight intransitive and eight non-
representational gestures were used throughout the battery. The tools for the transitive
gestures included a comb, spatula, hammer, fork, knife, watering can, toothbrush and
tweezers. The intransitive gestures included were waving good-bye, saluting, making the
okay sign, putting cream on one‟s face, beckoning, holding one‟s nose as if there were a bad
smell, scratching one‟s ear and hailing a cab. For all gesture types, half consist of movements
toward the body and half away from the body (Roy, Black, Blair, & Dimeck, 1998).
Conceptual Limb Apraxia Assessment
The Conceptual part of the Apraxia Battery included three naming tasks (Tool
Naming, Tool Naming by Function and Tool Naming by Action), two Tool Identification
(ID) tasks (Tool ID and Tool ID by Function), as well as three visuo-gestural ID tasks (
Action ID, Gesture Matching and Gesture Error Recognition) Please see Appendix A for a
description of each task.
Gesture Production Limb Apraxia Assessment
The patients performed four pantomime tasks (Pantomime of Transitive Gestures,
Pantomime of Intransitive Gestures, Pantomime by Picture, Pantomime by Function), three
delayed imitation tasks (Delayed Imitation of Transitive, Intransitive and Non-
Representational Gestures), four concurrent imitation tasks (Concurrent Imitation of
Transitive Gestures, Concurrent Imitation of Transitive Gestures with Verbal Cue,
Concurrent Imitation of Intransitive Gestures and Concurrent Imitation of Non-

180
Representational Gestures). Patients were also asked to pantomime gestures while holding
tools in the Object Use task. Each of these tasks is described in detail in Appendix A.
Analysis
Given the small sample size, a descriptive approach was used. After scoring the
performance of each patient and obtaining a composite percentage score on each task, all
scores were converted to Z-scores based on the performance of 28 age-matched control
participants. A Z-score below 2 SDs of the mean of the control group was considered
impaired, and if the score fell between 1-2 SD‟s the performance was considered borderline.
Both the percentage scores and the Z-scores were recorded for each assessment for both
hands. In addition, change scores were calculated by subtracting the score at the first visit
from the score at the last visit on which there was recorded data for the task in question.
Other Neuropsychological Assessments
Aside from the limb apraxia battery, participants also completed a detailed battery of
neuropsychological assessments, as part of a longer study investigating the progression of
neuropsychological deficits in neurodegenerative disorders. Where possible these
assessments were compared with our apraxia assessments when done within the same year in
order to gain more insight into the cognitive profiles. Detailed neuropsychological data could
be matched to all apraxia assessments, except for the second and fourth assessment of patient
68-RHP, the third assessment of patient 73-RHP and the third assessment of patient 76-LHP.
All matched neuropsychological assessments were taken during the same year as the apraxia
battery was administered, on average 113 days away from the apraxia assessment. The
following neuropsychological assessments were included: for General Function the Mini

181
Mental Status Examination (MMSE) (Folstein, Folstein, & Mchugh, 1975), Mattis Dementia
Rating Scale (DRS) (Mattis, 1976) Clock Drawing (Battersby, Bender, Pollack, & Kahn,
1956; Spreen & Strauss, 2006) and Raven’s Progressive Matrices (Raven, 1960); for
language the Western Aphasia Battery (WAB) (Kertesz, 1982) and the Boston Naming Test
(BNT ); for visuospatial Ability the Rey Complex Figure (Corwin & Bylsma, 1993) and
Judgement of Line Orientation (Benton, Hannay, & Varney, 1975); for visual memory, the
Visual Reproduction (Wechsler, 1945), for attention and working memory, Digit Span
(Forward & Backward) (Kaplan, 1991) and Trail Making Test (A & B) (Army Individual
Test Battery, 1944); for executive functions: Phonemic Fluency (FAS) (Spreen et al., 2006);
and for functional ability the Disability Assessment for Dementia (DAD) (Gelinas, Gauthier,
McIntyre, & Gauthier, 1999).
Neuroimaging Reports
Neuroimaging reports from the clinical scans of all patients were reviewed. Most
patients had MRI and SPECT scans. The clinical reports of their scans were reviewed and are
summarized in the paper. The reports were written by the staff radiologist on duty at the
hospital at the time the scan was taken. The summaries are given to provide the reader with a
general idea of the neuroanatomical regions most likely affected in each patient, but the
results should be taken with caution, given no quantitative examination was done.
RESULTS
Patient Summaries:
A summary of all percentage scores and Z-scores for each visit for each patient is
presented in Appendix 5B, Tables 5B.1-5B.4. In addition, Appendix 5B, Tables 5B.5-5B.8

182
contain a summary of each task and describe if the patient was impaired or not at first visit
vs. last visit and a summary of the change over assessments. A description of the
performance of each patient for each of the four domains of apraxia assessment is provided
below. In the discussion below, the term “affected limb” was defined as the limb where the
initial motor deficits developed, while the “nonaffected limb”, is the limb that was not
affected by the disease initially, or at least less affected, as evidenced by akinetic-rigid
syndrome. It should be kept in mind, that the “nonaffected” limb, while unaffected initially,
could still develop parkinsonian features later on in disease progression, but it normally
remains less affected throughout the disease.
Case 58-RHP
This was a 60 year-old woman, who was first assessed about 3 years after symptoms
onset. She was re-assessed at 5 years and later at 7 years since symptom onset.
Conceptual Tasks: The patient was initially impaired on all conceptual tasks except
on two: Tool naming and Action ID and then continued to deteriorate in all conceptual tasks.
Pantomime and Object Use: The patient was initially impaired on all tasks with both
hands, except on Pantomime of Intransitive Gestures; she improved on Pantomime of
Transitive Gestures with both hands, but was still within impaired ranges on her last
assessment; she deteriorated in all other tasks in both hands, with the exception of slight
improvement in Pantomime by Function for the nonaffected hand, but the patient was still
impaired. During her third visit the patients was not assessed on any of the gesture
production tasks, because she had a bilateral inability to perform any movements with her
arms or fingers due to further deterioration in her motor symptoms.

183
Delayed Imitation: The patient was impaired in both hands initially on all tasks. She
was again tested only twice on these tasks and significant deterioration was observed in all
tasks.
Concurrent Imitation: The patient was impaired quite severely on all tasks in both
hands, except in the nonaffected hand on Concurrent Imitation of Intransitive gestures. Her
affected hand was assessed only at the second visit as assessment at the third visit was not
possible; however, the deterioration in performance between the first two visits was quite
severe.
Neuropsychological Assessment: The patient‟s MMSE score at her first visit was 27
(impaired for her age) and deteriorated to 14 at the last assessment, 4 years later. She was
impaired on the DRS at her second apraxia assessment, with attention and conceptual
component preserved (which was her first DRS assessment) and by the third visit, she was
impaired on all DRS components. The patient was impaired on BNT only at the first visit;
her performance on the second visit improved to a point which moved her outside the
impaired range. No deficits in the WAB were seen, however. Few other measures were
collected except FAS, where the patient was within normal limits .
Neuroimaging Reports: A year before the first apraxia assessment, an MRI report
indicated the patient had mild diffuse cerebral atrophy. The same year, SPECT scan showed
marked decreased activity bilaterally in the posteriopariatel regions, more pronounced on the
right and extending into the right temporal and occipital regions. In addition, an associated
decreased activity in the right thalamus was noted. During the year when the patient
underwent her first apraxia assessment, a SPECT indicated a decreased activity in the

184
parietofrontal regions bilaterally, but more in the right hemisphere, where it extended to the
occipital regions. The thalami at this time appeared normal.
Two years later, the MRI was repeated and during that year the patient underwent her
second apraxia assessment. The MRI report indicated moderately severe diffuse atrophy, as
well as, two small zones of subcortical signal change in right parietal and left frontal regions.
A SPECT report the same year, suggested bilateral parietal temporal decreased activity
extending to lateral occipital lobes, more pronounced in the right hemisphere.
Case 68-RHP
This was a 73 year-old man who was first assessed at 8 years since disease onset and
was subsequently re-assessed at 10, 11 and 12 years since disease onset.
Conceptual Tasks: The patient was not impaired initially, scoring 100% on most
tasks. This patient did not show much change over time and even had some improvement in
Gesture Error Recognition.
Pantomime and Object Use: The patient was initially impaired only in the affected
hand, which could be assessed only at the first visit; the patient deteriorated throughout on all
pantomime assessments and Object Use in the nonaffected limb.
Delayed Imitation: The performance with the affected hand was assessed only at the
first visit and revealed significant impairment on all tasks. Further assessments were not
possible due to severe dystonia. Performance with the nonaffected hand was much better than
with the affected hand at the first visit and was impaired only for non-representational
gestures, while transitive gestures were borderline. Overall, performance deteriorated over
time, even if at first assessment the performance was not impaired.

185
Concurrent Imitation: In these tasks, the affected hand was impaired severely during
the initial assessment, while performance with the nonaffected hand was initially within
normal limits, except for Non-Representational Gestures. The nonaffected hand was not
assessed at the last visit for most Concurrent Imitation tasks, due to time constraints, but the
deterioration was quite severe from first to third visit.
Neuropsychological Assessment: During the first visit the patient was not impaired on
any of the general cognitive measures, such as the MMSE, Raven‟s and DRS. He also
performed well on Trails A & B, Rey Figure, JLO, BNT and WAB. A complete
neuropsychological assessment was not completed for the second apraxia assessment, but
around the third apraxia assessment, a neuropsychological assessment showed that the patient
remained unimpaired on the Raven‟s and the DRS. His MMSE score had fallen to 27
(impaired for his age), but he continued to be within normal limits on attention tests, the
FAS, JLO, BNT and WAB comprehension were all within normal limits, but the Rey figure
copying was impaired,. He was impaired on all DAD measures. Neuroimaging Reports:
In 2002, the patient underwent his first apraxia assessment. The patient‟s CT scan that year
appeared normal (an MRI could not be taken due to metal in his eye). A SPECT report the
same year indicated prominent sylvain fissures and right temporoparietal cortex decrease in
activity. Two years later, after his second apraxia assessment, the patient was again reported
to have prominent decrease around the sylvain fissures, as well as a hypoperfusion defect in
the top right parietofrontal region. In 2005, when the third apraxia assessment was
completed, the SPECT report indicated a moderate sized perfusion defect in the right frontal
parietal region, along with bilateral decreases around the sylvain fissures, no significant
changes from last SPECT visit. Finally, in 2007, a year after the last apraxia assessment was

186
completed, decreased activity was noted in the right parietal, right post temporal and right
mesial temporal region.
Case 71-RHP
This was a 72 year-old woman assessed first 2 years since symptoms onset and re-
assessed a year later.
Conceptual Tasks: The patient was initially impaired only on Tool Naming, but over
visits deteriorated on all naming tasks, except on Tool Naming (where the patient was
already impaired and remained so). The patient also deteriorated on Tool ID, but
unfortunately there was no data for Action ID and Gesture Matching.
Pantomime and Object Use: The patient was initially impaired in both hands, more so
on the affected hand. At the second assessment the nonaffected hand deteriorated further
while the affected hand could no longer be tested, due to severe progression of
extrapyramidal features.
Delayed Imitation: The patient was assessed only once on Delayed Imitation and was
found impaired in both hands in all gesture types.
Concurrent Imitation: The patient had only one assessment and was found impaired
in both hands more so in the affected side.
Unfortunately, the patient was assessed on very few tasks during the second
assessment, due to significant deterioration in both motor and cognitive functions.
Neuropsychological Assessment: The patient was impaired on MMSE, Raven‟s, DRS
Total Score (but within normal ranges on attention and conceptual sections). On attention
tasks, the patient was within normal limits on FDS and BDS, but impaired on Trails A and B.
Copying of the Rey Figure and JLO were impaired, but Visual Reproduction was normal.

187
The FAS was also normal. The BNT and WAB were normal, except for a relatively lower
performance in WAB Naming. Finally functionally, the patient was impaired on all ADL and
IADL measures at both occasions with deterioration from first to second visit. During the
second neuropsychological assessment, most tests could no longer be administered, because
the patient was found too impaired to complete the assessments.
Neuroimaging Reports: Two SPECT reports were available for this patient. Both
were done concurrently (within the same year) with the apraxia assessments. The first
SPECT report indicated that there was a moderate decreased perfusion in both frontal lobes,
extending into the medial temporal lobes bilaterally, but slightly more pronounced on the
right. In addition, a slight decreased activity was observed in the right basal ganglia. The
second SPECT report indicated no further prominent changes.
Case 73-RHP
This was 62 year-old man assessed 3 years since symptoms onset and reassessed
twice subsequently on yearly basis.
Conceptual Tasks: The patient was impaired only on Tool Name by Action, but he
subsequently deteriorated on most naming tasks. He was not impaired on Tool and Action
Identification, nor on Gesture Matching and he remained so throughout assessments. The
patient deteriorated in Gesture Error Recognition.
Pantomime and Object Use: The patient‟s affected hand could be assessed only
during the first visit and further assessment was prevented by severe parkinsonian deficits.
The nonaffected hand was not impaired at first, and remained so on many tasks at the second
visit, but deterioration to impaired ranges was observed at the third visit throughout all
pantomime tasks.

188
Delayed Imitation: The patient was severely impaired when tested with the affected
hand which was assessed only during the first visit due to motor deficits. Performance with
the nonaffected hand started off normal but deteriorated significantly to impaired ranges by
the third assessment.
Concurrent Imitation: The patient was assessed only once on transitive and
intransitive gestures with the affected limb and was found to be impaired on both tasks; the
nonaffected hand initially was not impaired, but deteriorated over time to impaired ranges in
all gesture types.
Neuropsychological Assessment: The patient was within normal limits on all
neuropsychological assessments during the first visit, except on the FAS. A year later, during
the second visit, MMSE performance had deteriorated to impaired range, but Raven‟s , DRS ,
Attention and working memoty tasks and language were still normal. Attention and
visuospatial tasks were still preserved, as was naming and language. DAD measures of ADLs
and IADLs had significantly decreased, however.
Neuroimaging Reports: Two SPECT reports were available for this patient, done
consecutively in 2002 and 2003. The patient was assessed on apraxia during the same years.
The first report indicated mild decreased perfusion in the right high parietal lobe, as well as
prominence of the interhemispheric fissure, suggestive of atrophy. The second SPECT report
indicated no significant change as compared to the scan taken in 2002.
Case 62-LHP
This was a 67 year-old woman, assessed 5 years after symptoms onset and re-
assessed two years later.

189
Conceptual Tasks: The patient was initially impaired on all but two tasks: Tool
Naming by Function and Action Identification. She deteriorated in all tasks.
Pantomime and Object Use: Both hands were initially severely affected and severe
deterioration was observed from first to second visit in all pantomime tasks.
Delayed Imitation: The patient had records for Delayed Imitation only from the
second assessment (this task was omitted from the battery at the first assessment due to time
constraints) and she was severely affected in both hands for transitive gesture and for
intransitive and non-representational gestures. The patient was assessed only with the
nonaffected limb where she was found to be impaired. No attempts were made to assess her
affected limb, due to severe motor deficits observed in the pantomime tasks and it was
thought best to discontinue further testing with that limb.
Concurrent Imitation: Due to time constraints Concurrent Imitation of Transitive
Gestures was omitted and Concurrent Imitation with Verbal Cueing was administered only at
the right hand during the first assessment. The affected hand was assessed only during the
first visit and was found to be impaired (transitive gestures were assessed only with verbal
cueing). On the non-affected hand, the patient was initially impaired on Intransitive and Non-
Representational Gestures and she deteriorated in Intransitive Gesture but slightly improved
in Non-Representational Gestures, despite remaining in the impaired range.
Neuropsychological Assessment: The patient was impaired on the MMSE and the
DRS from the beginning. There were no data on attention and visuospatial assessments.
Performance on the FAS was within normal range. The BNT was impaired and so was the
WAB, showing a profile of Wernicke‟s aphasia (comprehension was 6.65, just below 7
which is the comprehension cutoff score according to (Kertesz & Poole, 1974)) Therefore,

190
even though she was classified as impaired in her ability to understand language, she falls
just below the cutoff line and we believe she had a good understanding of what she was
asked to do in the pantomime tasks. Most neuropsychological assessments could not be re-
administered during the second visit, due to severe cognitive decline.
Neuroimaging Reports: An MRI, taken at the same year as the first apraxia
assessment, indicated mild generalized cerebral atrophy. Two SPECT assessments were
completed, both during the same years of the apraxia assessments. The first report indicated a
decreased perfusion involving the parietal temporal lobes bilaterally with extension into the
posterior frontal lobes greater in the left hemisphere. The second report indicated profound
decreased perfusion of the temporal parietal lobes bilaterally extending into the posterior
frontal lobes. The left side was still somewhat more affected.
Case 76-LHP
This was a 79 year-old woman assessed 4 years from symptom onset, reassessed
twice after that, at 6 and 7 years post symptom onset.
Conceptual Tasks: This patient was initially impaired on all naming tasks. She
improved her performance on the second assessment, but unfortunately on the third
assessment the patient was almost completely mute, so we were not able to administer most
conceptual tasks on the last assessment.
Pantomime and Object Use: The patient was initially impaired only in the
nonaffected hand in transitive and intransitive gestures, while all other pantomime tasks were
impaired in both hands. The affected hand deteriorated significantly in all tasks, except that
in Pantomime of Intransitive Gestures, where her performance remained normal. The

191
nonaffected hand deteriorated on all pantomime tasks, except Pantomime of Intransitive
Gestures and Object use.
Delayed Imitation: The patient was impaired on Transitive Gestures with both hands.
She was borderline impaired with the nonaffected hand on Delayed Imitation of Intransitive
Gestures and within normal limits with the affected limb. In Non-Representational gestures,
she was borderline with the affected hand and apraxic with the nonaffected hand. Significant
deterioration was observed in both hands over the three years she participated.
Concurrent Imitation: The patient was initially impaired on all tasks except in
Intransitive Gestures for both hands. Significant deterioration in both hands was observed on
all imitation tasks, except for improvement in the affected hand in Intransitive Gestures,
where performance remained normal .
Neuropsychological Assessment: During the first visit, the patient performed well on
most measures, except DRS Initiation, Trails B, Rey Figure Copying, and FAS. She was also
impaired on ADL and IADL at her first visit. She was impaired on WAB Naming. During the
second visit, the patient‟s DRS Initiation score had further deteriorated, causing the total
DRS score to fall within impaired limits. Additional deterioration was seen in the BDS,
which was now impaired; further decline was seen in Trails B, WAB naming and both DAD
subscores placed her now at impaired levels. Deficits in BDS were also noted.
Neuroimaging Reports: In 2002, when the first apraxia assessment was completed, an
MRI report indicated that the patient had moderate atrophy and some white matter disease
bilaterally. No abnormalities were reported in the SPECT scans initially, but by 2004, when
the second arpaxia assessment was completed, the patient had mild asymmetry in the basal
ganglia bilaterally, more pronounced on the right side.

192
Case 132-LHP
This was a 74-year-old woman assessed at 4 years post symptoms onset and
reassessed twice after that on an yearly basis.
Conceptual Tasks: The patient was initially not impaired, scoring 100% on almost all
tasks and did not change over assessments.
Pantomime and Object Use: The patient‟s affected hand was assessed only at first
visit and was impaired only on Pantomime by Picture and Object Use. Future assessment
could not be done, due to severe arm weakness. Initially, her nonaffected hand was normal
on transitive and intransitive Gestures, but deteriorated in all gesture types except intransitive
gestures. Overall, the deterioration was not as severe as in other LHP cases.
Delayed Imitation: The affected hand was tested only during the first visit and was
found significantly impaired on all gesture types, even though the Imitation of Transitive
Gestures was borderline. The nonaffected hand was impaired on all tasks, except in
Intransitive Gestures where it was borderline. Deterioration was observed in all tasks but the
patient remained borderline on Delayed Imitation of Intransitive Gestures.
Concurrent Imitation: impaired on all tasks initially with the affected hand. Again the
affected hand could only be assessed during the first visit, The nonaffected hand was
impaired initially and deteriorated further on Transitive and Intransitive Gestures, but
remained the same on Transitive Gesture with Verbal Cueing and improved on Non-
Representational Gestures, even though the patient remained quite significantly impaired on
all gesture types.

193
Neuropsychological Assessment: Aside from omitting tasks, requiring verbal
response, this patient was very high functioning, not impaired on any of the
neuropsychological measures and remaining so throughout the visits.
Neuroimaging Reports: In 2005, when the patient‟s first apraxia assessment was
completed, an MRI report indicated mild atrophy, scaterred white matter changes and an old
left pontine lacune. A SPECT in 2006, taken closer to the second apraxia assessment,
indicated mild decreased activity in the left parietal region, corresponding to focal atrophy in
this region. In 2007, when the third apraxia assessment was completed, the SPECT report
indicated no new perfusion defects.
Task Summaries:
Conceptual Tasks
Tool Naming: Four of the patients were impaired on tool naming during their first
assessment. (For detailed examination of which patients were impaired on which tasks and
their actual scores, the reader can refer to Appendix 5b). Only two of these patients
deteriorated in performance over time and another patient who started from non-impaired
ranges deteriorated to impaired ranges.
Tool Naming by Function: Only one of the seven patients was impaired on this task
initially and she actually improved her performance on the second visit. Four other patients
deteriorated to impaired ranges on subsequent assessments. One patient remained the same
and two improved over visits.
Tool Naming by Action: Three patients were impaired on this task and two of them
improved over visits, while the other impaired patient continued to deteriorate. From the

194
patients who were not initially impaired, two remained the same and one deteriorated to
impaired ranges.
Tool ID: Only one patient was initially impaired on Tool Identification and this
patient continued to deteriorate in performance over further assessments. Two patients who
were initially not impaired deteriorated to impaired ranges. All of the other patients remained
not impaired on this task on subsequent assessments.
Action ID: Only six patients had data on this task and one patient had data only at the
first assessment on which she was not impaired. Only one of the six patients was initially
impaired on this task. This patient continued to deteriorate and one other patient moved into
the impaired range over assessments.
Gesture Matching: Again only six patients had data on this task. No patients were
impaired on this task initially, and none of the five patients with follow-up data on this task
moved to impaired performance over time.
Gesture Error Recognition: Again only six patients had data on this task and only five
had follow-up assessments. Initially one patient was impaired and this patient continued to
deteriorate in performance, two other patients moved from not impaired to impaired
performance over subsequent visits and two patients remained within normal range.
Gesture Production Tasks:
Pantomime of Transitive Gestures: With the nonaffected hand, on pantomime of
transitive gestures, five out of seven patients were impaired during their first assessment and
all patients were within impaired ranges on follow-up. One patient slightly improved, but
was still within impaired ranges on follow-up. With the affected hand, five patients out of
seven were apraxic on this task and four patients were not able to have follow-up with this

195
hand due to motor deficits. Overall, everybody who could be reassessed deteriorated to
impaired performance by their last visit.
Pantomime of Intransitive Gestures: Only two of the patients initially showed deficits
in this task with their nonaffected hand and three patients with their affected hand. With their
nonaffected hand, five patients deteriorated, four of whom moved to impaired performance,
while two patients improved in performance. With their affected hand, four patients could no
longer be tested due to the severity of the motor deficits, while the other three deteriorated.
Overall, this was the one gesture production task, where patients were not as significantly
affected.
Pantomime by Picture: Only one patient was not impaired initially on this task with
their nonaffected hand and one patient was borderline, All patients deteriorated in
performance over subsequent visits and by their last visits all of them were impaired. With
the affected hand, all patients were impaired at the first assessment and only two patients
could be further tested.. In several patients this task was omitted from their assessments due
to time constraints.
Pantomime by Function: With the nonaffected hand one patient was borderline and
one was not impaired; all other patients were impaired. They all deteriorated with the
exception of one who improved slightly, but still remained impaired. Again this task was
omitted in several cases due to time contraints, requiring us to cut the assessment short. With
the affected hand, only one patient was not impaired. All patients deteriorated further in
performance if they could be reassessed.
Object Use: Here, with the nonaffected hand one patient was borderline and one
patient was impaired. Both of these patients deteriorated over time to quite impaired

196
performance. Among the rest of the patients, all deteriorated in performance even further,
except for one patient whose performance remained the same and one patient whose
performance slightly improved, but still remained quite severely affected. With the affected
limb, all patients were impaired on their initial assessment and among the three patients in
whom reassessment was possible, all deteriorated further, possibly due to both apraxia, as
well as motor deficits.
Concurrent Imitation of Transitive Gestures: With the nonaffected limb, two patients
were not impaired on this task, 5 of these patients deteriorated to impaired performance. Two
patients were not reassessed, due to motor deficits. With the affected limb, data was available
on 6 patients, all patients were impaired initially, only one was reassessed who showed
further deterioration.
Concurrent Imitation of Transitive Gestures with Verbal Cueing: The addition of
verbal cue did not seem to change the pattern of results seen in concurrent imitation of
transitive gestures. With the nonaffected hand, the same two patients were not impaired, but
eventually deteriorated to impaired performance. All tested patients deteriorated further with
the exception of one patient who did not change, but was already impaired. Again, with the
affected limb, all patients were impaired and if they were reassessed, they deteriorated
further.
Concurrent Imitation of Intransitive Gestures : In this task, with the nonaffected limb,
only two patients were impaired, three were borderline and two were not impaired.
Unfortunately, over subsequent visits all of them deteriorated in performance with all of them
becoming impaired, except one who was borderline. With the affected limb, all patients were
impaired, except two who were borderline. One of these borderline patients improved in

197
performance on a subsequent assessment, while all others could not be reassessed, due to
motor deficits.
Concurrent Imitation of Non-Representational Gestures: With the affected hand, 6
patients were assessed on this task and all were impaired, all patients who could be
reassessed deteriorated in performance. The same was true for the affected hand.
Delayed Imitation of Transitive Gestures: With the nonaffected hand, 4 out of 7
patients were impaired on their first assessment, one was borderline, one was not impaired
and one was not assessed, because a shortened battery was administered. Out of the 6
patients who had data on the affected limb, all but one (who was borderline) were impaired
initially. All patients deteriorated in performance with both hands if they could be reassessed.
Delayed Imitation of Intransitive Gestures: With the nonaffected hand, 2 patients
were not impaired, three were borderline and one was apraxic initially. With the affected
hand, only one was not impaired. All patients deteriorated with both hands in their
performance over subsequent visits, if they could be reassessed.
Delayed Imitation Non-Representational: Six patients had initial data on the
nonaffected limb and 5 on the affected limb. All were impaired in both hands, with the
exception of one patient who was borderline impaired in their performance with the affected
hand. All patients deteriorated with both limbs if they could be reassessed.
Neuropsychological Performance:
Overall, only three patients developed deficits in most of the general cognitive
function tests (58-RHP, 71-RHP and 62-LHP). Two of these patients also showed language
deficits (only one additional patient in thee entire sample had naming deficits). Patient 71-
RHP also had visospatial deficits. Unfortunately, attention and working memory and

198
functional ability assessments were not done on 58-RHP and 62-LHP. 71-RHP was impaired
on Trails A and ADL and IADL. Aside from these three patients, two other patients
eventually developed deficits in MMSE (68-RHP and 73-RHP), but the performance on the
Clock, DRS and Raven‟s remained normal. These two patients had generally preserved
language and visuospatial abilities. Patient 73-RHP had deficits in FAS. Both patients had
deficits in ADL and IADL. Finally two patients had normal performance on tests of general
cognitive function, except for some selective deficits in DRS for patient 76-LHP. MMSE,
Clock and Raven‟s were all well preserved, however. Language, visuospatial, attention and
working memory, executive function and functional abilities were generally preserved for the
most part in both cases.
Pattern Evolution
Transitive Gestures Patterns
Data needs to be available for all three gesture production tasks, (pantomime, delayed
and concurrent imitation), as well as at least one of the action identification tasks in order to
determine the pattern of performance (if data was available only for one of the action
identification tasks and the patient was impaired, the lack of information on the other task,
prevented us from determining if the patient action recognition system is intact), Therefore,
in some cases we could not define the patterns (see Table 5.3 for a summary of each pattern
across visits for each of the patients).
With the affected hand 4 of the patients started out with Pattern 7: ideomotor apraxia
with preserved conceptual system. For one patient, we had missing data. One patient
presented with conduction apraxia and remained with that pattern on second examination
(This was the only patient for whom we have pattern data on a subsequent visit for the

199
affected limb). One patient presented with selective deficit in concurrent Imitation (Pattern 9,
which was not originally defined by Roy (1996)).
With the nonaffected hand, three patients started out with pattern 7, two patients
started out not impaired, one patient presented with conduction apraxia and one patient had
missing information and the pattern could not be defined. Out of the three patients with
pattern 7, one did not have any follow-up patterns, one progressed to global apraxia (pattern
8) and one remained with pattern 7 of ideomotor apraxia, without conceptual deficits. Both
patients who started out not impaired and the patient with conduction apraxia, all progressed
eventually to pattern 7.Therefore for all patients, the final pattern of performance was usually
ideomotor apraxia with preserved ability to identify actions or global apraxia involving both
conceptual and production impairments..
Intransitive Gestures Patterns
With the affected limb, only five patients had data on pantomime and the two
imitation tasks. Of these patients 3 presented with conduction apraxia, one was not impaired
and one presented with deficits in both pantomime and imitation. Follow-up patterns were
available only for patient 76-LHP, whose last pattern was that of selective deficit in delayed
imitation, suggesting an impaired encoding of visuogestural information into working
memory.
With the affected limb, two patients started out as not impaired, one patient had
selective deficits in pantomime, one in concurrent imitation and one in delayed imitation.
Oddly, enough the patient with deficit in pantomime progressed to conduction apraxia, thus
she improved on pantomime but deteriorated in imitation. The patient with selective deficit in
concurrent imitation remained with this pattern throughout assessments. The patient with

200
selective deficits in delayed imitation, progressed to pattern 7 (ideomotor apraxia with
preserved conceptual knowledge). One of the patients who was initially not impaired,
remained not impaired on follow-up assessments, and the other one progressed to conduction
apraxia.

201
Table 5.3: Summary of Patterns of apraxia performance for each patient on Transitive and Intransitive Gestures
TRANSITIVE GESTURES PATTERNS INTRANSITIVE GESTURES
PATTERNS
Case ID Visit Nonaffected Affected Nonaffected Affected
58-R
1 Production Ideomotor (P-/DI-/CI-/ID+) Production Ideomotor (P-/DI-/CI-/ID+) P+/DI-/CI+ P+/DI-/CI-
2 Global (P-/DI-/CI-/ID-) n/a P-/DI-/CI- n/a
3 n/a n/a n/a n/a
68-R
1 No Impairment Production Ideomotor (P-/DI-/CI-/ID+) No Impairment P-/DI-/CI-
2 Production Resp Selection (P-/DI+/CI+/ID+) n/a No Impairment n/a
3 Production Conduction (P+/DI-/CI-/ID+) n/a No Impairment n/a
4 Production Ideomotor (P-/DI-/CI-/ID+) n/a n/a n/a
71-R 1 Production Ideomotor (P-/DI-/CI-/ID+) Production Ideomotor (P-/DI-/CI-/ID+) No Impairment P+/DI-/CI-
2 n/a n/a n/a n/a
73-R
1 No Impairment Production Ideomotor (P-/DI-/CI-/ID+) n/a n/a
2 No Impairment n/a No Impairment n/a
3 Production Ideomotor (P-/DI-/CI-/ID+) n/a P+/DI-/CI- n/a
62-L 1 n/a n/a n/a n/a
2 Global (P-/DI-/CI-/ID-) n/a P-/DI-/CI- n/a
76-L
1 Production Ideomotor (P-/DI-/CI-/ID+) Production Conduction (P+/DI-/CI-/ID+) P-/DI+/CI+ No Impairment
2 Production Ideomotor (P-/DI-/CI-/ID+) Production Conduction (P+/DI-/CI-/ID+) P-/DI-/CI- P-/DI-/CI+
3 n/a n/a P+/DI-/CI- P+/DI-/CI+
132-L
1 Production Conduction (P+/DI-/CI-/ID+) P+/DI+/CI-/ID+" P+/DI+/CI- P+/DI-/CI-
2 Production Conduction (P+/DI-/CI-/ID+) n/a P+/DI+/CI- n/a
3 Production Ideomotor (P-/DI-/CI-/ID+) n/a P+/DI+/CI- n/a
-Impaired (≤-2SD); +=Not Impaired (Z-score>-2);

202
DISCUSSION
Overall, the following conclusions can be made regarding the performance of patients
at their first visit. None of the patients initially had deficits in their overall conceptual
knowledge of gestures and tools. While some patients had selective deficits on certain
conceptual tasks, the overall picture suggests a preserved conceptual system, especially
during initial assessments, occurring on average about 2 years post-onset. Again, this is
consistent with previous reports of patients without deficits in the ability to identify tools and
gestures (Leiguarda et al., 1994; Salter et al., 2004; Jacobs et al., 1999; Soliveri et al., 2005;
Moreaud, Naegele, & Pellat, 1996).
With respect to the production system, most patients were initially impaired in their
ability to pantomime and imitate gestures (both with delay and concurrently). On all tasks,
deficits were more severe in their affected hand. It should be kept in mind that some of the
gesture performance in the affected limb may be affected by extrapyramidal motor features.
Attempts were made not to penalize patients for errors due to these extrapyramidal deficits.
Object Use was also affected in most patients and in all patients with their affected hand.
Intransitive gestures were generally affected less than transitive gestures in both pantomime
and imitation tasks. Non-representational gestures tended to be most affected. All these
findings have been reported in our previous paper (Chapter 4), given this is a subsample of
the group of patients examined in Chapter 4. In addition, these trends are consistent with
previous reports of deficits in object use in CBS patients (Jacobs et al., 1999; Leiguarda et
al., 2003) and of greater impairment in transitive gestures than intransitive gestures (Pharr et
al., 2001; Salter et al., 2004; Chainay et al., 2003).

203
While greater deficits in imitation of non-representational gestures have not been
found in other studies (Merians et al., 1999; Spatt et al., 2002; Leiguarda et al., 2003;
Buxbaum et al., 2007), a greater deficit in the imitation of non-representational gestures is
consistent with Buxbaum‟s theory that CBS patients suffer from dynamic apraxia, causing
deficits in body schema coding and transformation of stored representations or visual
information into movement. While she did not find a greater deficit in non-representational
gestures in her study, the smaller sample of patients or the possibility that her patients may
have been at a different stage of disease progression (it is not clear at how many years post
disease onset the patients were assessed) may have prevented her from finding this effect
(Buxbaum et al., 2007).
With respect to how patients‟ performance progressed over time, conceptual tasks
were more resistant to deterioration over time, with 4 out of 7 patients preserving gesture and
tool identification over longitudinal follow-up. Our case series suggests that the conceptual
system in praxis is relatively preserved in CBS in the early disease stage, that is, 1-2 years
after symptom onset, but it can be affected later in the disease course. It is interesting,
however, that only some patients (in our sample only half of the patients) actually show
progression of conceptual system function to the point of impairment. In fact, the patient who
started out participating in our study at the latest time point after onset (at about 8 years post-
onset) and continued to participate until 12 years post-onset was one of the patients who had
preserved tool and gesture knowledge and who showed absolutely no deterioration in this
task at all. This patient underlines the heterogeneity of this disease both in terms of praxis
pattern and rate of overall progression. In addition, in comparing the performance of patients
on some of the neuropsychological tests, it became obvious that the three patients who

204
significantly deteriorated on conceptual tasks (58-RHP, 71-RHP and 62-LHP), were also the
patients who deteriorated on various assessments of general cognitive function (such as
MMSE, DRS, Clock and Raven‟s). Patients 71-RHP and 62-LHP were also two of only three
patients with naming deficits. Unfortunately, attention and working memory, as well as
visuospatial function tests were not collected on 58-RHP and 62-LHP. Patient 71-RHP
showed deficits in Rey figure and JLO, but not on Visual Reproduction, which may have
contributed to the conceptual deficits on the apraxia tasks. Patient 71-RHP had no deficits in
digit span tasks, but showed deficits in Trails A.
Past studies have also reported that less than half of CBS patients develop generalized
cognitive decline, even though the authors of that study admit that the degree of cognitive
decline was likely underestimated (Rinne, Lee, Thompson, & Marsden, 1994). In fact, in
many of our patients who demonstrated such decline, further testing was precluded due to the
steep cognitive losses. It is not clear whether the side of presentation plays a role in
determining whether one deteriorates conceptually or not, but the current case series suggest
that this is not necessarily a fact. In our sample, the three patients who deteriorated
cognitively consisted of two patients with RHP and one patient with LHP. Given the large
number of cognitive domains affected it is likely that in these patients the disease has spread
to numerous brain areas bilaterally. This is strongly supported by the fact that the three
patients with general cognitive decline were also the only patients in whom the SPECT
reports described bilateral decrease in perfusion, while in all other patients perfusion deficits
continued to be predominantly asymmetric. Hence, it is unlikely that the side of initial
presentation plays an important role in the predisposition to cognitive decline, though this
may emerge in a larger sample. Of note is the fact that functional imaging may serve as a

205
better indicator of how patients will progress over time and whether general cognitive decline
will be observed. This finding is supported by a study by Frasson et al. (1998) showing
preserved gesture recognition in three patients (2 LHP and 1 RHP) associated with decreased
metabolism unilaterally in the hemisphere contralateral to the affected side limb.
Given the fact that this study did not include a quantitative analysis of neuroimaging,
it is hard to draw any reliable inferences of how the neuroimaging and especially the SPECT
relates to the neuropsychological assessments and the apraxia performance of the patients.
Aside from noting that bilateral perfusion defects seem to be common in patients with
generalized cognitive decline, neither the side nor the affected lobes seem at first glance to be
associated with specific deficits in neuropsychological testing. For example, aside from the
three patients with bilateral involvement (58-RHP, 71-RHP and 62-LHP), two patients had
greater perfusion defects on the right (68-RHP and 73-RHP), one patient had left perfusion
defect (132-LHP) and one patient had a normal SPECT scan (76-LHP). Patient 68-RHP had
involvement in right frontoparietal areas and patient 73-RHP had deficits in right
parietotemporal areas. Both of these patients, aside from deficits in MMSE, had an otherwise
normal performance on other neuropsychological tests. FAS impairment was also noted in
patient 73-RHP, while 68-RHP was too impaired to perform the task. Given both patients had
frontal perfusion defects, more pronounced on the right, it is likely that deficits in frontal
function are causing the deficits in the FAS. Patient 132-LHP had notable perfusion deficit in
the left parietal lobe and yet this patient remained within normal limits on all
neuropsychological tests. Patient 76-LHP, on the other hand, who had a normal SPECT scan,
had some deficits in DRS, Rey Figure, Trails B and FAS. In conclusion, overall based on
clinical SPECT reports of patients with predominantly asymmetrical perfusion defects, it

206
seems difficult to draw any general conclusions of what tests would be impaired simply
based on radiology reports.
What about the relationship between neuroimaging SPECT reports and performance
on the apraxia tasks? With respect to conceptual tasks, again the patients with bilateral
perfusion deficits were the patients with greater deficits on the conceptual arpaxia tasks. The
two LHP patients (one with normal scan, the other with parietal deficits) showed little
deficits in conceptual tasks (even though patient 76-LHP had a lot of missing data and also
showed at first assessment some deficits that were not observed on second assessment). With
respect the two patients with right perfusion defects, one had hardly any deficits in
conceptual arpaxia tasks, while the other had some deficits in tool naming and gesture error
recognition tasks, which emerged around the second visit. With respect to gesture production
tasks, all patients had deficits in pantomime and imitation tasks. The patients with bilateral
hypoperfusion, however, had lower Z-scores than patients with unilateral hypoperfusion.
This was especially the case for patients 58-RHP and 62-LHP whose Z-scores often fell
below 10 SDs of the control group and in many cases fell even below 20 SDs of the control
mean.
Overall, in conclusion, while reliable relationships can be drawn only by
quantitatively examining the relationships between test performance and neuroimaging and
by examining a larger sample of patients, a rough examination of the reports indicates that
patients with bilateral perfusion defects on SPECT seem to be more likely to show general
decline in neuropsychological measures, deficits in limb apraxia conceptual tasks (as
opposed to no deficits in other patients) and severe gesture production deficits (as opposed to
milder, but still impaired relative to controls, performance in patients with unilateral

207
perfusion defect). Future studies should examine these relationships through reliable
methods.
One should also keep in mind that the patients we are describing here are CBS
patients and, therefore, the underlying pathology of their disease can be variable within the
frontal-temporal lobar degeneration spectrum. Cases presenting with CBS have been reported
to have a variety of underlying pathologies , including classical corticobasal degeneration,
Pick Body disease, frontotemporal lobar degeneration (FTLD-U) ubiquitin positive tau
negative , motor neuron disease type inclusions (MNDI), progressive supranuclear palsy
(PSP) pathology (Kertesz, McMonagle, Blair, Davidson, & Munoz, 2005; Mizuno et al.,
2005; Grimes, Bergeron, & Lang, 1999), Alzheimer‟s Disease (Imamura, Wszolek, Lucas, &
Dickson, 2009), Dementia with Lewy Bodies (Horoupian & Wasserstein, 1999), spongiform
encephalopathy (Anschel, Simon, Llinas, & Joseph, 2002) . It is quite reasonable to consider
that the subsample of CBS patients, who deteriorate in most cognitive domains and who
develop deficits in the conceptual knowledge of tools and gestures, may represent patients
with distinct underlying pathology, different possibly than the CBS patients who remain
relatively cognitively intact over time. In fact, the only patient for whom we have a
pathological diagnosis is patient 62-L, whose pathological diagnosis was Argyrophilic
Grains, which is also a 4R tauopathy in the spectrum of FTLD. AGD also presents with
general cognitive decline and dementia, even though the clinical features of the disease can
be difficult to define (Tolnay & Clavaguera, 2004; Ferrer, Santpere, & van Leeuwen, 2008).
All patients, deteriorated in gesture production performance and the few patients who
started out without apraxia (usually with the nonaffected limb), eventually developed
apraxia. This was the case for pantomime, the two imitation tasks, as well as object use. It

208
was often the case that patient‟s affected hand could be assessed only during the first visit
because extrapyramidal features prevented further assessments of the more affected limb.
Our finding is consistent with reports of greater initial apraxia involvement in the affected
limb (Rinne et al., 1994).
Limb Apraxia Patterns
In regard to pattern presentation and evolution of patterns for transitive gestures, four
patients, all with RHP, had a presentation of deficits in both pantomime and imitation for the
affected hand, suggesting deficits in the production system, possibly in the response
organization and control of movement (Roy, 1996). Two patients with LHP had selective
deficits in imitation, without deficits in pantomime for the affected hand, but unfortunately,
further assessments with the affected hand could not be performed in most cases due to
motor deficits, so it is unclear how these cases would have developed over time with regard
to expression of apraxia.
With respect to the nonaffected hand, while some patients started out within the
normal range, all patients eventually progressed to patterns of apraxia with both pantomime
and imitation deficits evident. Two of these patients, one RHP and one LHP, developed a
more global apraxia affecting pantomime, imitation and conceptual knowledge of gestures
and tools. One patient (71-RHP) could not be reassessed on all tasks, so we were unable to
define the pattern, but the overall picture showed generalized cognitive decline, which may
have led to development of deficits in the conceptual knowledge of tools and gestures.
In regard to intransitive gestures, unfortunately the battery does not have tasks
assessing conceptual knowledge of intransitive gestures, but pantomime and imitation
deficits could be ascertained. Only 5 patients had enough data to be categorized into patterns

209
for the affected hand. Three of the patients (58-RHP, 71-RHP and 132-LHP) had selective
deficits in imitation, also called “conduction apraxia”(Ochipa, Rothi, & Heilman, 1994). One
patient (68-RHP) had both pantomime and imitation deficits, while another patient began
within the normal range and progressed to a selective deficit in delayed imitation, suggesting
difficulty encoding information into working memory (76-LHP). With respect to the
nonaffected hand, three patients began without any impairment, among whom one could no
longer be tested (71-RHP), one remained not impaired (68-RJP) and the third developed
conduction arpaxia with that hand (73-RHP). One patient had complete data for a pattern
only on the last assessment and was categorized to present with deficits in both pantomime
and imitation (62-LHP). Another patient (58-RHP) started out with selective deficit in
delayed imitation and progressed to a pattern of general apraxia affecting both pantomime
and imitation of intransitive gestures. One patient (72-LHP) began with impairment only in
imitation, and while improved in pantomime of intransitive gesture, imitation of intransitive
gestures deteriorated. Finally, one patient (132-LHP) had a selective deficit in concurrent
imitation from the beginning and did not change his pattern over time. In conclusion,
conduction apraxia, a selective deficit in imitation, seems to be a common pattern for
intransitive gestures of CBS patients in either hand and can be observed in both RHP and
LHP CBS patients.
Selective deficits in imitation with a preserved ability to pantomime may suggest a
problem with visuomotor transformations. Deficits in processing of visuogestural
information are unlikely in patients who remained intact in gesture identification tasks, but in
the three cases who eventually developed deficits in gesture identification, it is possible that
visuospatial processing deficits could have affected their imitation performance. Deficits in

210
imitation with preserved ability to recognize gestures may suggest deficits in the direct route
of imitation and suggests that patients are unable to use the indirect route even in cases where
they in fact recognize the demonstrated gestures. An intact indirect route is inferred from the
fact that patients had a preserved ability to pantomime.
Finally, the patients with deficits in both pantomime and imitation, it is likely that
patients suffered from deficits in general organization and control of movement, that may or
may not be superimposed on deficits in visuomotor transformations.
The ability of patients to imitate non-representational gestures was quite deficient
from the initial assessments and deteriorated even further over time, in both concurrent and
delayed imitation. All patients were impaired in this type of imitation from the start, with the
exception of two cases who began as borderline with the nonaffected hand. This strongly
suggests deficits in coding of body schema and supports the notion of dynamic apraxia in
CBS, as proposed by Buxbaum. (2007). It also suggests deficits in the direct, nonsemantic
route to imitation.
Study Limitations
Finally, we should address some of the limitations of the current study. First this is a
purely descriptive study examining a relatively small sample of patients. Group comparisons
were not run, because there were a variety of patients with a various number of assessments
per patient. A larger scale longitudinal study should be conducted to determine if any of the
generalizations drawn in the current paper hold in a larger sample after statistical
examination.

211
In addition, unfortunately, we had a lot of missing data. While all attempts were made
to avoid this, it was inevitable in some cases due to time constraints and patient‟s desire to
end the assessments.
Finally, the case series consisted of patients who were only clinically diagnosed with
CBS and the underlying pathology may vary from patient to patient. This variability in
underlying pathology was addressed to some extent in the discussion of our findings, but it
should be kept in mind in the interpretation of findings in future studies.
While a larger study with more structured analysis is definitely required to make any
conclusions about the progression of limb apraxia in CBS, this study is the first to attempt to
describe the progression of limb apraxia deficits in CBS. We are also the first to describe the
various apraxia patterns of CBS patients and to attempt to describe how these patterns change
over time.
In conclusion, the study supports that different domains of praxis may progress
differently in CBS. Conceptual knowledge is often preserved and in our sample more than
half the patients did not lose their knowledge of tools and gestures. The patients whose
conceptual knowledge of tools and gestures is eventually affected are also patients who
showed a general cognitive decline as measured by tests of general cognitive function.
Deficits in pantomime and imitation eventually developed with intransitive gestures being
least affected and non-representational gestures being most affected.

212
Appendix 5A: Case Descriptions.
132-LHP
The patient was a 74-year-old widowed woman, a retired switchboard operator,
referred for neurological evaluation of abnormal right upper extremity function. Medical
history included only osteoarthritis. There was no family history of neurological problems.
Her symptoms began 3 years earlier, initially presenting as numbness in the fingertips of her
right hand, which had progressed to weakness, clumsiness and general decreased dexterity in
her right hand (functional limitations include a difficulty sewing, eating, carrying a cup,
putting on a glove, putting keys in the ignition and doing up buttons). She was switching to
utilizing her left hand for most ADL‟s. She described that her hands felt like Velcro, due to
difficulty releasing objects from her grasp. She had no involvement in lower extremities or
the left hand;, difficulty walking, alien limb, hallucinations, cognitive symptoms, difficulty
initiating movements or bradykinesia. Clock drawing was intact. On motor examination she
had normal bulk and tone, except for mild increased tone in her right arm. Power was 5/5
bilaterally, symmetrically throughout, but she had reduced rapid alternating movements in
her right hand. Reflexes were 2+ bilaterally. She failed to identify objects placed in her right
hand and letters drawn on her right palm indicating cortical sensory loss. She had increased
tone with right hand , dystonic posturing of fingers, bradykinesia and corticalsensory loss in
her right hand.
58-RHP
The patient was a 58-year-old retired nurse with pain and numbness in her hands
causing her to drop objects and some speech and memory disturbances. She had
unremarkable past medical history. She presented with normal bulk and tone on motor and

213
sensory exam. A year later, the patient had clear deficits in the visual spatial, executive
function and memory domains.with limited insight After another year, she was having
trouble finding words, but was still able to communicate. She had no hallucinations,
confusion or change in level of comprehension. She was still self-sufficient with personal
care, but was unable to write well with a pen. One year later, she reported difficulty with
short-term memory, had episodes of confusion with cooking, problems with balance,
occasionally falling towards right, and slower movement. On examination, she had rigidity
with activation, right limb apraxia and to had declined in all areas of neuropsychological
testing. Her memory worsened and she started getting lost in unfamiliar places. The word
findings difficulties continued to increase and the patient continued to decline in her
cognitive and extrapyramidal features, which were worse on the left side. One year later, she
had further declined in memory and speech. At that time, she was unable to do any
housework, including cooking. Her language had deteriorated further and she needed
assistance in dressing. She became depressed, and had dystonia in both upper limbs,
increased rigidity in both arms, bradykinesia more on right and clinically showed bilateral
apraxia, her comprehension remained good. She had no falls, but needed assistance with
bathing and dressing. During her final visit, in 2006, she could not use her left hand and her
apraxia symptoms were worse. Her left arm was levitating and and her gait had deteriorated.
62-LHP
In 2001, the patient reported gradual difficulty speaking, with word finding
difficulties. She was somewhat depressed. She also had dressing apraxia and tremor in both
hands. There was no significant medical history and no family history of neurological
disorders. Written comprehension difficulties were present as well. Clock drawing was

214
impaired and her writing was illegible. In clinic, the patient was diagnosed with CBD, due to
progressive decline of apraxia and language comprehension.
The autopsy of this patient showed Alzheimer‟s Disease with Argyrophilic grain
disease..
71-RHP
The 75-year-old right handed retired homemaker, had several episodes of falling,
difficulty with balancing checkbook and reading over the previous two years. The patient had
a right foot resting tremor. She was stooped when walking, and had difficulty manipulating
objects with left arm. Over the previous 6 months, the patient had become more stiff and
bradykinetic. On examination, she was alert and oriented, except to year; her attention was
normal, with some features of perseveration; there was no evidence of neglect; she had slow
initiation of voluntary downward saccades, poor upward gaze, and absent vertical saccades.
Her muscle bulk was normal, ideomotor apraxia was reported to be more prominent on the
left with some resting tremor. The patient denied cognitive complaints, even though the
husband had noticed slow deterioration. The patient could not read anymore and was
misplacing objects.
A year later, the patient was still able to converse with friends, even though
prominent language problems were emerging. She also was walking with assistance and was
incontinent. Her verbal responses had long latency. She asked pertinent questions, had good
use of right hand, and resting tremor in right leg. Her vertical saccades were impaired. Six
months later her memory declined and that she needed help with ADL and IADL. The patient
was still generally oriented, with had memory, attention and language impairments.
73-RHP

215
This 62 year-old retired project manager for a general contractor was referred for left
sided apraxia, neglect, cortical sensory deficits and myoclonus. Three years prior to referral,
he started to notice difficulties using his left arm and leg, which initially manifested itself in
difficulty walking. The patient tended to prefer his right leg. He also noticed numbness in his
4th
and 5th
left digits, which was followed by numbness in the left elbow. Some of the initial
symptoms included difficulties tying shoes, buttoning shirts and using cutlery with his left
hand. The patient also noticed involuntary jerks of his left limbs that occurred both
spontaneously and in response to touch. The patient had history of falls. On exam the patient
was oriented to person, place and time. He was reported to have rigidity, bradykinesia,
apraxia, cortical sensory deficits, mildly increased reflexes on the left, spontaneous and
stimulus sensitive myoclonus and mild dysphagia.
Two years later, the patient had developed moderate rigidity of all limbs. He had
stimulus sensitive myoclonus in the left arm.He had choreiform movement in the left hand,
along with alien hand phenomenon. Rapid alternating movements were slow on the right, and
the left hand could not be assessed because of severe apraxia. His left leg dragged causing
him to walk slowly. A year later, there was a progression of apraxia and myoclonus on the
left and walking had become even more difficult. The left thumb was flexed into the palm,
causing pain in the left middle finger. The patient was walker dependent. He had frequent
spontaneous myoclonic jerks in the left arm and leg. The patient had no voluntary movement
in the left hand, which also showed stimulus sensitive myoclonus.
A year later, the patient had suffered an intracranial subdural bleed due to a fall and
reported about 20 falls in the last 6 months, consequently he had started using a wheelchair.
He reported often ending up doing exactly the opposite of what he intended to do, for

216
example moving backwards when he intended to move forward. He developed urinary
incontinence, was unable to control his emotions and cried very easily. There was a mild
oculomotor apraxia to the left, slowness of saccades and square-wave jerks. Rigidity in left
limbs increased, as did myoclonic jerks on left arm and hand, and his speech had become
slurred.
68-RHP
The 73-year-old retired architect presented with left arm apraxia, dystonia, rigidity,
and sensory disturbances. The patient had good health until 7 years earlier, when he was
involved in a motor vehicle accident, which resulted in a subdural hematoma, which was
evacuated at the time. CT in 2000 was normal.
The deterioration in his left arm continued, leading to difficulty buttoningshirts and
tying shoes. He reported that he knows what he wanted to do, but could not do it. There were
initially no involuntary movements. The patient was oriented to time, with normal speech
and language, memory, intellect and judgment. Affect and mood were all normal. On exam
he had left rigidity, left dystonia and left myoclonus. and bulk was normal. He had impaired
graphaesthesia and stereognosia. A year later cognitive functioning was still unchanged and
the left extrapyramidial findings were worsening. He was no longer able to walk by himself
and his left arm had become useless.
The patient was reported to have undergone further deterioration a year later, with
further decline in ambulation and decreased use of his right handThe next year, he was
reported stable but unable to perform most ADLs. Finally, during his last visit, the patient‟s
speech was much worse, mobility had decreased even more, but memory and comprehension
remained good.

217
76-LHP
This is 78- year-old retired housekeeper, who was first seen in the clinic. She reported
initially difficulty producing words, reporting that she knows what she wanted to say, but
could not produce the words. Her speech was very slow and hesitant, and occasionally
mispronounced words. She complained of slower reading and difficulty writing, as well as
difficulty with the right hand in activities such as combing her hair. She had no hallucinations
or personality changes. Insight into her cognitive deficits was good. She had no
parkinsonism, myoclonus, or alien lim. MMSE was 25/30, She had anomic non-fluent
aphasia with impaired articulation. She presented with asymmetric rigidity in the right more
than left arm. The preliminary diagnosis was primary progressive aphasia likely due to CBD.
A year later, the patient showed further decline in speaking, with relatively intact
comprehension and no problems recognizing people and objects. At this time the patient
needed help with dressing, but continued to participate in certain daily activities, such as
cooking. The following year, the patient‟s language had deteriorated greatly and she hardly
spoke anymore. She had severe dysarthria, bradykinesia and rigidity more pronounced in the
right upper and lower limbs. Six months later, she could no longer engage in any
conversation, but there was little decline in basic ADL‟s.The patient had increased rigidity in
the right arm and in legs bilaterally. A year later, she was almost essentially mute, but still
understood well. She needed help bathing, but used walker to get around. Six months later,
she presented with some further decline cognitively, but motor symptoms were relatively
stable. The following year, she was still able to answer yes/ no questions. She started to fall,
needed help bathing, but was still eating and toileting independently. A year later, she

218
followed simple commands, was still getting around with walker, but was falling a lot due to
trouble with balance.

219
Appendix 5B: Individual Performances of Patients across Time

220
Table 5B.1: Conceptual Tasks Scores: showing percentage accuracy scores and Z-scores for each participant across visits.
Tool Naming Tool Naming by Function
Tool Name by Action Tool ID Action ID
Gesture Matching
Gesture Error Recognition
Case ID Visit % Z-score % Z-
score % Z-
score % Z-
score % Z-
score % Z-score % Z-
score
58-RHP
1 87.5 -3.0 100.0 0.4 100.0 0.7 87.5 0.2 87.5 -2.8 92.5 -0.2 62.5 -1.7
2 87.5 -3.0 87.5 -1.7 50.0 -4.8 87.5 -5.3 50.0 -12.4 40.0 -7.6 12.5 -6.4
3 62.5 -9.5 50.0 -7.9 62.5 -3.4 62.5 -10.8 12.5 -22.0
Δ -25.0 -6.6 -50.0 -8.3 -37.5 -4.1 -25.0 -11.0 -75.0 -19.2 -52.5 -7.4 -50.0 -4.7
68-RHP
1 100.0 0.3 87.5 -1.7 100.0 0.7 100.0 0.2 100.0 0.4 100.0 0.8 71.8 -0.8
2 100.0 0.3 100.0 0.4 100.0 0.7 100.0 0.2 100.0 0.4 100.0 0.8 50.0 -2.9
3 100.0 0.3 100.0 0.4 100.0 0.7 100.0 0.2 100.0 0.4 100.0 0.8 75.0 -0.5
4 100.0 0.3 100.0 0.4 100.0 0.7 100.0 0.2 100.0 0.4
Δ 0.0 0.0 12.5 2.1 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 3.2 0.3
71-RHP
1 75.0 -6.2 100.0 0.4 100.0 0.7 100.0 0.2 95.0 -0.9 100.0 0.8 78.1 -0.2
2 75.0 -6.2 75.0 -3.7 50.0 -4.8 87.5 -5.3
Δ 0.0 0.0 -25.0 -4.1 -50.0 -5.5 -12.5 -5.5
73-RHP
1 100.0 0.3 100.0 0.4 75.0 -2.1 100.0 0.2 100.0 0.4 100.0 0.8 87.5 0.7
2 87.5 -3.0 87.5 -1.7 75.0 -2.1 100.0 0.2 100.0 0.4 100.0 0.8 12.5 -6.4
3 87.5 -3.0 87.5 -1.7 87.5 -0.7 100.0 0.2 100.0 0.4 100.0 0.8 50.0 -2.9
Δ -12.5 -3.3 -12.5 -2.1 12.5 1.4 0.0 0.0 0.0 0.0 0.0 0.0 -37.5 -3.5
62-LHP
1 87.5 -3.0 100.0 0.4 50.0 -4.8 100.0 -5.3 100.0 0.4 92.5 -0.2 53.1 -2.6
2 62.5 -9.5 50.0 -7.9 37.5 -6.2 75.0 -16.3 62.5 -9.2 37.5 -7.9 25.0 -5.2
Δ -25.0 -6.6 -50.0 -8.3 -12.5 -1.4 -25.0 -11.0 -37.5 -9.6 -55.0 -7.7 -28.1 -2.7
76-LHP
1 87.5 -3.0 62.5 -5.8 75.0 -2.1 100.0 0.2
2 100.0 0.3 100.0 0.4 100.0 0.7 100.0 0.2
3 75.0 0.2
Δ 12.5 3.3 37.5 6.2 25.0 2.7 100.0 11.1
132-LHP
1 100.0 0.3 100.0 0.4 100.0 0.7 100.0 0.2 100.0 0.4 100.0 0.8 75.0 -0.5
2 100.0 0.3 100.0 0.4 100.0 0.7 100.0 0.2 100.0 0.4 100.0 0.8 37.5 -4.1
3 100.0 0.3 100.0 0.4 100.0 0.7 100.0 0.2 100.0 0.4 100.0 0.8 75.0 -0.5
Δ 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0 0.0
Δ=Change from first to last visit

221
Table 5B.2: Pantomime and Object Use Scores: showing percentage accuracy and Z-scores for each patients across visits.
Pantomime Transitive Pantomime Intransitive Pantomime by Picture Pantomime by Function Object Use
NAS AS NAS AS NAS AS NAS AS NAS AS
Case ID # %
Z-score %
Z-score %
Z-score %
Z-score %
Z-score %
Z-score %
Z-score %
Z-score %
Z-score %
Z-score
58-RHP
1 53.8 -9.1 31.3 -13.1 93.5 0.1 92.3 -0.4 68.8 -7.4 52.5 -11.4 63.8 -7.2 45.0 -12.0 86.3 -5.7 71.3 -11.9
2 63.8 -6.8 45.7 -10.1 73.8 -4.1 57.8 -8.0 46.3 -14.0 18.8 -20.5 65.0 -6.9 11.3 -20.0 60.0 -18.8 27.5 -31.8
3 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
Δ 10.0 2.3 14.5 3.0 -19.8 -4.2 -
34.5 -7.7 -22.5 -6.6 -33.8 -9.1 1.3 0.3 -
33.8 -8.0 -26.3 -13.1 -
43.8 -19.9
68-RHP
1 93.8 0.0 71.3 -4.8 98.8 1.2 81.5 -2.7 92.5 -0.4 66.3 -7.7 93.8 0.0 71.3 -5.7 95.0 -1.3 48.8 -22.1
2 81.3 -2.8 --- --- 91.5 -0.3 --- --- 80.0 -4.1 --- --- 78.6 -3.7 --- --- 82.5 -7.6 --- ---
3 86.3 -1.7 --- --- 94.3 0.2 --- --- 87.5 -1.9 --- --- 86.3 -1.8 --- --- 88.8 -4.4 --- ---
4 48.8 -10.2 --- --- 78.5 -3.1 --- --- --- --- --- --- --- --- --- --- 74.3 -11.7 --- ---
Δ -45.0 -10.2 --- --- -20.3 -4.3 --- --- -5.0 -1.5 --- --- -7.5 -1.8 --- --- -20.7 -10.4 --- ---
71-RHP
1 78.8 -3.4 63.8 -6.4 95.0 0.4 88.0 -1.3 67.5 -7.8 41.3 -14.4 67.5 -6.3 70.0 -6.0 88.8 -4.4 75.0 -10.2
2 66.3 -6.2 --- --- 80.5 -2.7 --- --- 62.5 -9.2 --- --- --- --- --- --- 76.3 -10.7 --- ---
Δ -12.5 -2.8 --- --- -14.5 -3.1 --- --- -5.0 -1.5 --- --- --- --- --- --- -12.5 -6.3 --- ---
73-RHP
1 95.0 0.3 77.5 -3.5 95.0 0.4 84.8 -2.0 88.8 -1.5 77.5 -4.6 87.5 -1.5 62.5 -7.8 98.8 0.6 83.8 -6.2
2 88.8 -1.1 --- --- 88.5 -1.0 --- --- 85.0 -2.6 --- --- 88.8 -1.2 --- --- 77.5 -10.1 --- ---
3 78.8 -3.4 --- --- 88.5 -1.0 --- --- --- --- --- --- 58.8 -8.4 --- --- 88.8 -4.4 --- ---
Δ -16.3 -3.7 --- --- -6.5 -1.4 --- --- -3.8 -1.1 --- --- -28.8 -6.8 --- --- -10.0 -5.0 --- ---
62-LHP
1 32.9 -12.8 57.5 -8.2 52.3 -9.2 75.0 -3.9 25.0 -18.8 31.3 -18.4 31.3 -15.2 40.0 -12.8 45.0 -23.8 72.5 -12.6
2 0.0 -19.6 18.6 -17.1 38.0 -12.4 35.5 -12.3 --- --- --- --- 2.5 -22.1 26.3 -16.1 62.5 -15.9 45.0 -26.3
Δ -32.9 -6.8 -38.9 -8.8 -14.3 -3.2 -
39.5 -8.4 --- --- --- --- -28.8 -6.8 -
13.8 -3.3 17.5 8.0 -
27.5 -13.8
76-LHP
1 80.0 -3.0 91.3 -0.5 78.0 -3.5 93.5 0.1 68.8 -7.0 77.5 -4.8 71.3 -5.7 72.5 -5.1 80.0 -7.9 87.5 -5.1
2 70.0 -5.0 86.3 -1.7 76.0 -4.0 74.8 -3.9 68.8 -7.0 70.0 -7.0 65.0 -7.2 75.0 -4.5 73.8 -10.8 77.5 -10.1
3 61.3 -6.9 71.3 -5.1 87.1 -1.5 92.5 -0.1 58.8 -9.7 66.3 -8.1 53.8 -9.9 71.3 -5.4 80.0 -7.9 72.5 -12.6
Δ -18.8 -3.9 -20.0 -4.5 9.1 2.0 -1.0 -0.2 -10.0 -2.7 -11.3 -3.3 -17.5 -4.2 -1.3 -0.3 0.0 0.0 -
15.0 -7.5
132-LHP
1 90.0 -0.9 93.8 0.0 87.0 -1.5 86.5 -1.4 83.8 -2.9 86.3 -2.2 86.3 -2.1 90.0 -0.9 90.0 -3.4 92.5 -2.6
2 96.3 0.4 --- --- 87.5 -1.4 --- --- 86.3 -2.3 --- --- 83.8 -2.7 --- --- 91.3 -2.8 --- ---
3 83.8 -2.2 --- --- 88.8 -1.1 --- --- 81.3 -3.6 --- --- 85.0 -2.4 --- --- 87.5 -4.5 --- ---
Δ -6.3 -1.3 --- --- 1.8 0.4 --- --- -2.5 -0.7 --- --- -1.3 -0.3 --- --- -2.5 -1.1 --- ---
NAS=Nonffected Side; AS=Affected Side; Δ=Change from first to last visit

222
Table 5B.3: Delayed Imitation Tasks: Summaries of percentage accuracy scores and Z-scores per patient for each visit
Delayed Imitation Transitive Delayed Imitation Intransitive Delayed Imitation Non-
Representational
NAS AS NAS AS NAS AS
Case ID Visit % Z-score % Z-score % Z-
score % Z-
score % Z-score % Z-score
58-RHP
1 57.5 -14.9 41.3 -29.8 93.0 -6.8 78.8 -9.0 27.5 -20.3 31.3 -23.3
2 37.5 -22.3 28.8 -36.4 67.8 -33.9 46.0 -23.4 23.8 -21.4 10.0 -30.9
3 --- --- --- --- --- --- --- --- --- --- --- ---
Δ -20.0 -7.4 -12.5 -6.6 -25.3 -27.2 -32.8 -14.4 -3.8 -1.1 -21.3 -7.6
68-RHP
1 92.5 -1.9 63.8 -18.0 100.0 0.8 63.0 -15.9 85.0 -3.4 50.0 -16.5
2 96.3 -0.5 --- --- 94.8 -4.9 --- --- 78.8 -5.2 --- ---
3 88.8 -3.3 --- --- 100.0 0.8 --- --- 68.8 -8.2 --- ---
4 43.8 -20.0 --- --- 74.5 -26.7 --- --- 48.8 -14.0 --- ---
Δ -48.8 -18.1 --- --- -25.5 -27.4 --- --- -36.3 -10.7 --- ---
71-RHP
1 88.8 -3.3 71.3 -14.1 97.5 -1.9 84.8 -6.3 68.8 -8.2 27.5 -24.6
2 --- --- --- --- --- --- --- --- --- --- --- ---
Δ --- --- --- --- --- --- --- --- --- --- --- ---
73-RHP
1 97.5 -0.1 80.0 -9.5 100.0 0.8 87.8 -5.0 91.3 -1.5 68.8 -9.8
2 93.8 -1.5 --- --- 98.8 -0.6 --- --- 86.3 -3.0 --- ---
3 78.8 -7.0 --- --- 92.3 -7.6 --- --- 58.8 -11.1 --- ---
Δ -18.8 -6.9 --- --- -7.8 -8.3 --- --- -32.5 -9.6 --- ---
62-LHP
1 --- --- --- --- --- --- --- --- --- --- --- ---
2 48.0 -26.3 17.5 -29.7 67.0 -14.2 --- --- 45.0 -18.3 --- ---
Δ --- --- --- --- --- --- --- --- --- --- --- ---
76-LHP
1 75.0 -12.1 83.8 -5.2 94.8 -1.9 98.8 -0.6 73.8 -8.0 91.3 -1.5
2 58.8 -20.6 83.8 -5.2 93.0 -2.7 95.5 -4.1 63.8 -11.6 72.5 -7.1
3 66.3 -16.7 63.8 -12.6 93.8 -2.4 95.0 -4.6 68.8 -9.8 68.8 -8.2
Δ -8.8 -4.6 -20.0 -7.4 -1.0 -0.4 -3.8 -4.0 -5.0 -1.8 -22.5 -6.6
132-LHP
1 92.5 -2.9 92.5 -1.9 96.8 -1.0 94.3 -5.4 80.0 -5.7 66.3 -8.9
2 92.5 -2.9 --- --- 96.0 -1.4 --- --- 72.5 -8.4 --- ---
3 85.0 -6.8 --- --- 96.3 -1.3 --- --- 78.8 -6.2 --- ---
Δ -7.5 -3.9 --- --- -0.5 -0.2 --- --- -1.3 -0.4 --- ---
NAS=Nonaffected Side; AS=Affected Side; Δ=Change from first to last visit

223
Table 5B.4: Concurrent Imitation Tasks: Showing summaries for each patient across visits.
Concurrent Imitation Transitive Concurrent Imitation Transitive
with Verbal Cueing Concurrent Imitation Intransitive Concurrent Imitation
Non-Representational
NAS AS NAS AS NAS AS NAS AS
Case ID # % Z-score % Z-score % Z-score % Z-score % Z-score % Z-
score % Z-
score % Z-
score
58-RHP
1 58.8 -17.1 55.0 -18.3 45.0 -17.6 48.8 -24.1 95.5 -1.7 68.3 -29.3 42.5 -16.9 37.5 -23.4
2 22.5 -32.9 --- --- 35.0 -20.9 --- --- 60.5 -18.4 --- --- 26.3 -22.0 --- ---
3 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
Δ -36.3 -15.8 --- --- -10.0 -3.4 --- --- -35.0 -16.7 --- --- -16.3 -5.1 --- ---
68-RHP
1 97.5 -0.3 57.5 -17.2 96.3 -0.2 56.3 -20.4 100.0 0.4 59.5 -37.5 88.8 -2.5 43.8 -21.0
2 95.0 -1.4 --- --- 90.0 -2.3 --- --- 96.8 -1.1 --- --- 78.8 -5.6 --- ---
3 88.8 -4.1 --- --- 88.8 -2.7 --- --- 96.0 -1.5 --- --- 58.8 -11.8 --- ---
4 45.0 -23.1 --- --- --- --- --- --- --- --- --- --- --- --- --- ---
Δ -52.5 -22.8 --- --- -7.5 -2.5 --- --- -4.0 -1.9 --- --- -30.0 -9.4 --- ---
71-RHP
1 78.8 -8.4 46.3 -22.1 80.0 -5.7 41.3 -27.8 96.0 -1.5 84.8 -13.7 66.3 -9.5 30.0 -26.4
2 --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
Δ --- --- --- --- --- --- --- --- --- --- --- --- --- --- --- ---
73-RHP
1 100.0 0.8 91.3 -2.5 97.5 0.2 83.8 -6.8 --- --- --- --- --- --- --- ---
2 93.8 -1.9 --- --- 96.3 -0.2 --- --- 96.8 -1.1 --- --- 82.5 -4.4 --- ---
3 81.3 -7.4 --- --- 78.8 -6.1 --- --- 85.0 -6.7 --- --- 47.5 -15.3 --- ---
Δ -18.8 -8.2 --- --- -18.8 -6.4 --- --- -11.8 -5.6 --- --- -35.0 -10.9 --- ---
62-LHP
1 --- --- --- --- --- --- 42.5 -18.4 81.8 -16.5 87.3 -5.7 31.3 -25.9 26.3 -22.0
2 28.8 -29.7 --- --- 38.8 -29.1 --- --- 68.8 -28.8 --- --- 47.5 -19.5 --- ---
Δ --- --- --- --- --- --- --- --- -13.0 -12.3 --- --- 16.3 6.4 --- ---
76-LHP
1 76.3 -9.0 90.0 -3.6 76.3 -10.5 81.3 -5.3 98.8 -0.5 96.8 -1.1 63.3 -13.2 81.4 -4.7
2 77.5 -8.5 81.3 -7.4 66.3 -15.5 75.0 -7.4 95.0 -4.0 95.5 -1.7 76.3 -8.1 86.3 -3.2
3 72.5 -10.7 70.0 -12.2 --- --- --- --- 96.3 -2.9 98.8 -0.2 61.3 -14.0 61.3 -11.0
Δ -3.8 -1.6 -20.0 -8.7 -10.0 -5.0 -6.3 -2.1 -2.5 -2.4 2.0 1.0 -2.1 -0.8 -20.2 -6.3
132-LHP
1 91.3 -2.5 92.5 -2.5 87.5 -5.0 88.8 -2.7 96.8 -2.4 94.3 -2.3 70.0 -10.6 87.0 -3.0
2 87.5 -4.1 --- --- 87.5 -5.0 --- --- 96.6 -2.6 --- --- 78.8 -7.1 --- ---
3 88.8 -3.6 --- --- 87.5 -5.0 --- --- 90.0 -8.8 --- --- 81.3 -6.1 --- ---
Δ -2.5 -1.1 --- --- 0.0 0.0 --- --- -6.8 -6.4 --- --- 11.3 4.4 --- ---
NAS=Nonaffected Side; AS=Affected Side

224
Table 5B.5: Initial status and progression per patient for conceptual Tasks.
Case ID Visit Tool
Naming
Tool Naming
by Function
Tool Name by
Action Tool ID Action ID Gesture Matching
Gesture Error
Recognition
58-RHP
Initially I NI NI NI I NI B
Final I I I I I --- ---
Δ ↓ ↓ ↓ ↓ ↓ ↓ ↓
68-RHP
Initially NI B NI NI NI NI NI
Final NI NI NI NI NI --- ---
Δ ↔ ↑ ↔ ↔ ↔ ↔ ↑
71-RHP
Initially I NI NI NI NI NI NI
Final I I I I --- --- ---
Δ ↔ ↓ ↓ ↓ --- --- ---
73-RHP
Initially NI NI I NI NI NI NI
Final I B NI NI NI NI I
Δ ↓ ↓ ↑ ↔ ↔ ↔ ↓
62-LHP
Initially I NI I I NI NI I
Final I I I I I I I
Δ ↓ ↓ ↓ ↓ ↓ ↓ ↓
76-LHP
Initially I I I NI --- --- ---
Final NI NI NI NI --- --- ---
Δ ↑ ↑ ↑ ↑ --- --- ---
132-LHP
Initially NI NI NI NI NI NI NI
Final NI NI NI NI NI NI NI
Δ ↔ ↔ ↔ ↔ ↔ ↔ ↔
I=Impaired (≤-2SD); B=Borderline (-2< Z-score≤-1); NI=Not Impaired (Z-score>-1);
↓Deterioration ↑Improvement ↔No Change in performance from 1st to Final assessment

225
Table 5B.6: Initial status and progression per patient for Pantomime and Object Use Tasks.
Pantomime Transitive Pantomime Intransitive Pantomime by Picture
Pantomime by Function Object Use
Case ID NAS AS NAS AS NAS AS NAS AS NAS AS
58-RHP
Initial I I NI NI I I I I I I
Final I I I I I I I I I I
Δ ↑ ↑ ↓ ↓ ↓ ↓ ↑ ↓ ↓ ↓
68-RHP
Initial NI I NI I NI I NI I B I
Final I --- I --- NI --- NI --- I ---
Δ ↓ --- ↓ --- ↓ --- ↓ --- ↓ ---
71-RHP
Initial I I NI B I I I I I I
Final I --- I --- I --- --- --- I ---
Δ ↓ --- ↓ --- ↓ --- --- --- ↓ ---
73-RHP
Initial NI I NI I B I B I NI I
Final I --- NI --- I --- I --- I ---
Δ ↓ --- ↓ --- ↓ --- ↓ --- ↓ ---
62-LHP
Initial I I I I I I I I I I
Final I I I I --- --- I I I I
Δ ↓ ↓ ↓ ↓ --- --- ↓ ↓ ↑ ↓
76-LHP
Initial I NI I NI I I I I I I
Final I I B NI I I I I I I
Δ ↓ ↓ ↑ ↓ ↓ ↓ ↓ ↓ ↔ ↓
132-LHP
Initial NI NI B B I I I NI I I
Final I --- B --- I --- I --- I ---
Δ ↓ --- ↑ --- ↓ --- ↓ --- ↓ ---
I=Impaired (≤-2SD); B=Borderline (-2< Z-score≤-1); NI=Not Impaired(Z-score>-1);
↓Deterioration ↑Improvement ↔No Change inperformance from 1st to Final assessment
NAS=Nonaffected Side; AS=Affected Side

226
Table 5B.7: Initial status and progression per patient for Delayed Imitation tasks.
Delayed Imitation
Transitive Delayed Imitation
Intransitive Delayed Imitation
Non-Representational
Case ID NAS AS NAS AS NAS AS
58-RHP
Initial I I I I I I
Final I I I I I I
Δ ↓ ↓ ↓ ↓ ↓ ↓
68-RHP
Initial B I NI I I I
Final I --- I --- I ---
Δ ↓ --- ↓ --- ↓ ---
71-RHP
Initial I I B I I I
Final --- --- --- --- --- ---
Δ --- --- --- --- --- ---
73-RHP
Initial NI I NI I B I
Final I --- I --- I ---
Δ ↓ --- ↓ --- ↓ ---
62-LHP
Initial --- --- --- --- --- ---
Final I I I --- I ---
Δ --- --- --- --- --- ---
76-LHP
Initial I I B NI I B
Final I I I I I I
Δ ↓ ↓ ↓ ↓ ↓ ↓
132-LHP
Initial I B B I I I
Final I --- B --- I ---
Δ ↓ --- ↓ --- ↓ ---
I=Impaired (≤-2SD); B=Borderline (-2< Z-score≤-1); NI=Not Impaired(Z-score>-1);
↓Deterioration ↑Improvement ↔No Change inperformance from 1st to Final assessment
NAS=Nonaffected Side; AS=Affected Side

227
Table 5B.8: Initial status and progression per patient for concurrent imitation tasks.
Concurrent Imitation
Transitive
Concurrent Imitation Transitive with Verbal
Cueing Concurrent Imitation
Intransitive Concurrent Imitation
Non-Representational
Case ID NAS AS NAS AS NAS AS NAS AS
58-RHP
Initial I I I I B I I I
Final I --- I --- I --- I ---
Δ ↓ --- ↓ --- ↓ --- ↓ ---
68-RHP
Initial NI I NI I NI I I I
Final I --- I --- B --- I ---
Δ ↓ --- ↓ --- ↓ --- ↓ ---
71-RHP
Initial I I I I B I I I
Final --- --- --- --- --- --- --- ---
Δ --- --- --- --- --- --- --- ---
73-RHP
Initial NI I NI I B --- I ---
Final I --- I --- I --- I ---
Δ ↓ --- ↓ --- ↓ --- ↓ ---
62-HPL
Initial --- --- --- I I I I I
Final I --- I --- I --- I ---
Δ --- --- --- --- ↓ --- ↑ ---
76-LHP
Initial I I I I NI B I I
Final I I I I I NI I I
Δ ↓ ↓ ↓ ↓ ↓ ↑ ↓ ↓
132-LHP
Initial I I I I I I I I
Final I --- I --- I --- I ---
Δ ↓ --- ↔ --- ↓ --- ↑ ---
I=Impaired (≤-2SD); B=Borderline (-2< Z-score≤-1); NI=Not Impaired(Z-score>-1);
↓Deterioration ↑Improvement ↔No Change inperformance from 1st to Final assessment
NAS=Nonaffected Side; AS=Affected Side

228
REFERENCES
Anschel, D. J., Simon, D. K., Llinas, R., & Joseph, J. T. (2002). Spongiform
encephalopathy mimicking corticobasal degeneration. Movement Disorders, 17, 606-607.
Battersby, W. S., Bender, M. B., Pollack, M., & Kahn, R. L. (1956). Unilateral
Spatial Agnosia (Inattention) in Patients with Cerebral Lesions. Brain, 79, 68-93.
Benton, A., Hannay, J., & Varney, N. R. (1975). Visual-Perception of Line Direction
in Patients with Unilateral Brain Disease. Neurology, 25, 907-910.
Boeve, B. F., Lang, A. E., & Litvan, I. (2003). Corticobasal degeneration and its
relationship to progressive supranuclear palsy and frontotemporal dementia. Annals of
Neurology., 54, S15-S19.
Buxbaum, L. J., Kyle, K., Grossman, M., & Coslett, H. B. (2007). Left inferior
parietal representations for skilled hand-object interactions: Evidence from stroke and
corticobasal degeneration. Cortex, 43, 411-423.
Chainay, H. & Humphreys, G. W. (2003). Ideomotor and ideational apraxia in
corticobasal degeneration: A case study. Neurocase., 9, 177-186.
Corwin, J. & Bylsma, F. W. (1993). Psychological-Examination of Traumatic
Encephalopathy - the Complex Figure Copy Test. Clinical Neuropsychologist, 7, 3-21.
Dickson, D. W., Bergeron, C., Chin, S. S., Duyckaerts, C., Horoupian, D., Ikeda, K.
et al. (2002). Office of Rare Diseases neuropathologic criteria for corticobasal degeneration.
Journal of Neuropathology & Experimental Neurology, 61, 935-946.

229
Ferrer, I., Santpere, G., & van Leeuwen, F. W. (2008). Argyrophilic grain disease.
Brain, 131, 1416-1432.
Folstein, M. F., Folstein, S. E., & Mchugh, P. R. (1975). Mini-Mental State - Practical
Method for Grading Cognitive State of Patients for Clinician. Journal of psychiatric
research, 12, 189-198.
Frasson, E., Moretto, G., Beltramello, A., Smania, N., Pampanin, M., Stegagno, C. et
al. (1998). Neuropsychological and neuroimaging correlates in corticobasal degeneration.
Italian Journal of Neurological Sciences, 19, 321-328.
Gelinas, I., Gauthier, L., McIntyre, M., & Gauthier, S. (1999). Development of a
functional measure for persons with Alzheimer's disease: The disability assessment for
dementia. American Journal of Occupational Therapy, 53, 471-481.
Geschwind, N. (1975). The Apraxias: Neural Mechanisms of Disorders of Learned
Movements. American Scientist, 63, 188-195.
Graham, N. L., Zeman, A., Young, A. W., Patterson, K., & Hodges, J. R. (1999).
Dyspraxia in a patient with corticobasal degeneration: the role of visual and tactile inputs to
action. Journal of Neurology Neurosurgery and Psychiatry, 67, 334-344.
Grimes, D. A., Bergeron, C. B., & Lang, A. E. (1999). Motor neuron disease-
inclusion dementia presenting as cortical-basal ganglionic degeneration. Movement
Disorders.Vol., 14, 674-680.

230
Heath, M., Roy, E. A., Westwood, D., & Black, S. E. (2001). Patterns of apraxia
associated with the production of intransitive limb gestures following left and right
hemisphere stroke. Brain & Cognition, 46, 165-169.
Heilman, K. M. & Rothi, L. J. (1993). Apraxia. In Clinical Neuropsychology (pp.
141-163). New York, NY: Oxford University press Inc.
Horoupian, D. S. & Wasserstein, P. H. (1999). Alzheimer's disease pathology in
motor cortex in dementia with Lewy bodies clinically mimicking corticobasal degeneration.
Acta Neuropathologica, 98, 317-322.
Imamura, A., Wszolek, Z. K., Lucas, J. A., & Dickson, D. W. (2009). Corticobasal
Syndrome with Alzheimer's Disease Pathology. Movement Disorders, 24, 152-153.
Jacobs, D. H., Adair, J. C., Macauley, B., Gold, M., Gonzalez, R. L. J., & Heilman,
K. M. (1999). Apraxia in corticobasal degeneration. Brain & Cognition, 40, 336-354.
Kaplan, E. (1991). WAIS-R a neuropsychological Instrument. San Antonio, TX: The
Psychological Corporation.
Kertesz, A. (1982). Western Aphasia Battery. San Antonio, TX: The psychological
Corporation.
Kertesz, A., McMonagle, P., Blair, M., Davidson, W., & Munoz, D. G. (2005). The
evolution and pathology of frontotemporal dementia. Brain., 128, 1996-2005.
Kertesz, A. & Poole, E. (1974). The aphasia quotient: the taxonomic approach to
measurement of aphasic disability. Canadian Journal of Neurological Sciences, 1, 7-16.

231
Leiguarda, R., Lees, A. J., Merello, M., Starkstein, S., & Marsden, C. D. (1994). The
nature of apraxia in corticobasal degeneration. Journal of Neurology, Neurosurgery &
Psychiatry, 57, 455-459.
Leiguarda, R. C., Merello, M., Nouzeilles, M. I., Balej, J., Rivero, A., & Nogues, M.
(2003). Limb-kinetic apraxia in corticobasal degeneration: Clinical and kinematic features.
Movement Disorders, 18, 49-59.
Mattis, S. (1976). Mental Status examination for organic mental syndrome in the
elderly patient. In L.Bellak & T. B. Karasu (Eds.), Geriatric Psychiatry ( New York: Grune
& Stratton.
Merians, A. S., Clark, M., Poizner, H., Jacobs, D. H., Adair, J. C., Macauley, B. et al.
(1999). Apraxia differs in corticobasal degeneration and left-parietal stroke: A case study.
Brain & Cognition, 40, 314-335.
Mizuno, T., Shiga, K., Nakata, Y., Nagura, J., Nakase, T., Ueda, Y. et al. (2005).
Discrepancy between clinical and pathological diagnoses of CBD and PSP. Journal of
Neurology, 252, 687-697.
Moreaud, O., Naegele, B., & Pellat, J. (1996). The nature of apraxia in corticobasal
degeneration: A case of melokinetic apraxia. Neuropsychiatry, Neuropsychology, &
Behavioral Neurology, 9, 288-292.
Ochipa, C., Rothi, L. J., & Heilman, K. M. (1994). Conduction apraxia. Journal of
Neurology, Neurosurgery & Psychiatry, 57, 1241-1244.

232
Peigneux, P., Salmon, E., Garraux, G., Laureys, S., Willems, S., Dujardin, K. et al.
(2001). Neural and cognitive bases of upper limb apraxia in corticobasal degeneration.
Neurology, 57, 1259-1268.
Pharr, V., Uttl, B., Stark, M., Litvan, I., Fantie, B., & Grafman, J. (2001). Comparison
of apraxia in corticobasal degeneration and progressive supranuclear palsy. Neurology., 56,
957-963.
Raven, J. C. (1960). Guide to the Stanford Profressive Matrices. London: H.K Lewis.
Rebeiz, J. J., Kolodny, E. H., & Richardson, E. P., Jr. (1967). Corticodentatonigral
degeneration with neuronal achromasia: a progressive disorder of late adult life. Transactions
of the American Neurological Association, 92, 23-26.
Rinne, J. O., Lee, M. S., Thompson, P. D., & Marsden, C. D. (1994). Corticobasal
degeneration: A clinical study of 36 cases. Brain.Vol.117(5)()(pp 1183-1196), 1994., 1183-
1196.
Roy, E. A. (1996). Hand Preference, Manual Assymetries, and Limb Apraxia. In
D.Elliot (Ed.), Manual Asymmetries in Motor Control (pp. 215). Boca Raton, FL: CRC Press.
Roy, E. A., Black, S. E., Blair, N., & Dimeck, P. T. (1998). Analyses of deficits in
gestural pantomime. Journal of clinical and experimental neuropsychology, 20, 628-643.
Roy, E. A., Heath, M., Westwood, D., Schweizer, T. A., Dixon, M. J., Black, S. E. et
al. (2000). Task demands and limb apraxia in stroke. Brain and cognition, 44, 253-279.

233
Salter, J. E., Roy, E. A., Black, S. E., Joshi, A., & Almeida, Q. (2004). Gestural
imitation and limb apraxia in corticobasal degeneration. Brain & Cognition, 55, 400-402.
Soliveri, P., Piacentini, S., & Girotti, F. (2005). Limb apraxia in corticobasal
degeneration and progressive supranuclear palsy. Neurology, 64, 448-453.
Spatt, J., Bak, T., Bozeat, S., Patterson, K., & Hodges, J. R. (2002). Apraxia,
mechanical problem solving and semantic knowledge: Contributions to object usage in
corticobasal degeneration. Journal of Neurology., 249, 601-608.
Spreen, O. & Strauss, E. (2006). A compendium of neuropsychological tests. (3rd ed.)
Oxford University Press.
Togasaki, D. & Tanner, C. (2000). Epidemiologiz Aspects. In I.Litvan, C. Goetz, &
A. Lang (Eds.), Corticobasal Degeneration adn Related Disorders (pp. 53-59). Philadelphia,
PA: Lippincott Williams & Wilkins.
Tolnay, M. & Clavaguera, F. (2004). Argyrophilic grain disease: A late-onset
dementia with distinctive features among tauopathies. Neuropathology, 24, 269-283.
Wechsler, D. (1945). A standartized memorys cale for clinical use. Journal of
Psychology, 19, 87-95.

234
CHAPTER 6: GENERAL DISCUSSION
INTRODUCTION
The overall goal of my thesis was to gain a better understanding of how the brain
controls purposeful skilled movement by studying impaired performance of such movements
in two clinical populations: an acute brain damage model, stroke and a slowly progressive
neurodgeneration, Cortical Basal Syndrome (CBS). The loss of ability to perform skilled
movements due to brain damage is called limb apraxia, defined as an inability to perform
purposeful skilled movements, not due to inability to understand or follow instructions,
sensory impairment, muscle weakness, paralysis, incoordination, extrapyramidal motor signs
or uncooperativeness (Geschwind, 1975). A model-based approach was adopted as a
framework in designing the evaluation of patients‟ performance of skilled movements. More
specifically, the conceptual-production model, proposed by Roy (1996), suggests that skilled
movements are under the control of three systems: a sensory/perceptual system, processing
information from the environment, a conceptual system, storing one‟s knowledge of tools
and gestures, and a production system responsible for the response selection and organization
of the movement. In addition, Roy suggests that damage to any of these systems should
produce a specific pattern of limb apraxia deficits. Through the examination of two distinct
clinical populations, the goal of the thesis was to examine if damage to the brain due to
stroke or CBS would produce deficits in praxis and to examine whether the predicted patterns
of apraxia proposed by Roy evident in these two clinical populations. In addition, it was of
interest to examine the differential involvement of each hemisphere in limb apraxia. Finally,
in both populations, the thesis aimed to follow how limb apraxia changes over time by
examining recovery in stroke and progression of deficits in CBS.

235
One may ask why it is that after so many years that apraxia research has not gained
much attention. Geschwind himself noted in his paper in 1975 that the study of apraxia had
been widely neglected before his time, because patients often never complain about apraxia
(Geschwind, 1975). Unfortunately, this situation led some researchers and clinicians alike to
assume that apraxia had no functional implications for the performance of daily life
activities. Recent evidence has shown, however, that limb apraxia is in fact related to
decreased functional independence and for a comprehensive review of the literature on the
impact of apraxia on functional ability the reader can refer to Sunderland & Shinner (2007)
The impact of apraxia on functional independence and the high prevalence of limb
apraxia in stroke (Donkervoort, Dekker, van den Ende, Stehmann-Saris, & Deelman, 2000;
Roy et al., 2000) and Corticobasal Syndrome (CBS) (Stamenova, Roy, & Black, 2009) stress
the importance of extending the study of limb apraxia further. It is important to examine the
patterns of spontaneous recovery in stroke, as well as, to examine the progression patterns of
apraxia deficits in CBS. In stroke, an important step in designing a rehabilitation intervention
is to examine the natural course of recovery of the disorder. In CBS, in order to establish
possible prevention programs and approaches to manage the apraxic deficits and to prepare
the patient and family for what is to come, it is important to establish the natural progression
of praxis deficits. In both cases, a model-based approach to studying apraxia would enable us
to determine the relative frequency of the patterns of apraxia reflecting disruptions of
different systems in gesture production and to examine if all systems are equally susceptible
to recovery (in stroke) and deterioration (in CBS).

236
EVIDENCE FROM STROKE
The important role of the left hemisphere in the control of skilled movement has
largely been undisputed, given the numerous findings of greater deficits after left as opposed
to right hemisphere stroke (Liepmann, 1988; Kimura & Archibald, 1974; Geschwind &
Kaplan, 1962; De Renzi, Motti, & Nichelli, 1980; Haaland, Harrington, & Knight, 2000).
Most of the above-mentioned studies, however, examined relatively few task modalities
(sometimes only pantomime or only imitation) and they compare differences in patients‟
performance as groups. Two studies conducted by Roy and colleagues (Roy et al., 2000;
Heath, Roy, Black, & Westwood, 2001), however, took a somewhat different approach. They
examined the patterns of limb apraxia deficits after stroke and whether these patterns differ
after left vs. right hemisphere stroke. They found that while deficits in both pantomime and
imitation are common after left hemisphere damage (LHD), selective deficits in imitation or
pantomime alone were equally likely after LHD or right hemisphere damage (RHD). Their
findings suggest that the left hemisphere may be dominant in the final stages of production
system control, common to both pantomime and imitation, but conceptual knowledge and
visuogestural transformations may be controlled bilaterally. Replication of these novel
findings has since not been attempted. Given one of the thesis goals was to study the role of
each hemisphere in the control of movement, together with the goal to examine task modality
performance differences and to study limb arpaxia patterns, it was important to attempt to
replicate their findings in a different sample of patients. The thesis also expanded their
findings in two ways. First, the study assessed both transitive and intransitive gestures within
the same group of patients. Second, given the additional thesis goal to study changes over
time in limb apraxia post stroke, acute-subacute patients were compared in their performance

237
relative to chronic patients, with the prediction that, if recovery post stroke occurs, acute-
subacute patients should be more severely apraxic than chronic patients. The analysis
included the assessment of transitive and intransitive gestures using pantomime and imitation
in stroke patients (Chapter 2). These tasks were chosen, because past literature had shown
that, in stroke, pantomime accuracy is usually more affected than imitation (Schnider,
Hanlon, Alexander, & Benson, 1997; Roy et al., 2000; Heath et al., 2001), while transitive
gestures are usually more affected than intransitive (Haaland & Flaherty, 1984; Schnider et
al., 1997; Haaland et al., 2000). In addition to our goal of replication, given our interest in
brain asymmetries in the control of skilled movement, we wanted to examine the effect of
hemisphere in the performance of the four tasks. While pantomime is thought to be strongly
lateralized to the left, imitation has been suggested to be more bilaterally controlled (Barbieri
& Derenzi, 1988; Roy et al., 2000). In a similar vein, some transitive gestures are thought to
be under the control of the left hemisphere while intransitive gestures are thought to be more
bilaterally controlled (Buxbaum, Kyle, Grossman, & Coslett, 2007). Further studies,
however, are needed to confirm these predictions.
We had a number of hypotheses, most of which were confirmed. First, we predicted
that LHD patients would be more impaired than RHD patients and this was confirmed in
both pantomime and imitation. We also predicted that transitive gestures would be more
affected than intransitive gestures, a finding which was confirmed as well. In addition, we
expected pantomime to be more severely affected than imitation, but contrary to expectation,
imitation performance was more severely affected than pantomime. While this was
unexpected at first glance, our task comparisons reflected the patients‟ performance in Z-
scores, as standardized to the control group‟s performance. Most studies to date have

238
compared the level of performance accuracy of patients in pantomime versus imitation. In
our study, while in imitation the Z-scores were lower than pantomime (lower negative value
signifying greater impairment relative to controls), the patients‟ accuracy, as measured by a
percentage score, was lower in pantomime than imitation, signifying greater impairment for
pantomime. Thus, a lower Z-score in imitation in our study reflects a more severe deficit in
imitation than pantomime relative to the control group, rather than a lower accuracy score
relative to pantomime. This Z-score difference is also a reflection of the fact that while both
patient and control participants improved their performance in imitation relative to
pantomime, the control participants did more than the patients.
Finally, in terms of the examination of patterns of performance in each of the two
hemisphere groups, our findings largely confirmed those of Roy et al. (2000) and Heath et al.
(2001), suggesting that common deficits in pantomime and imitation are more frequent after
LHD, while selective deficits in pantomime or imitation occur after damage to either
hemisphere. The selective deficit in pantomime may result from damaged knowledge of
gestures and tools, while a selective deficit in imitation may be due to deficits in visuomotor
transformation.
What about the differences in performance in acute-subacute vs. chronic patients?
Our prediction that acute-subacute patients will perform less accurately than chronic patients
was confirmed, but the difference between the two groups failed to reach statistical
significance (p=.053). In addition, the frequency of limb apraxia was higher in acute-
subacute patients. We took these findings to be highly suggestive of recovery of apraxia post-
stroke, consistent with past studies indicating significant recovery over the first three months
post stroke (Foundas, Raymer, Maher, Gonzalez-Rothi, & Heilman, 1993; Basso, Burgio,

239
Paulin, & Prandoni, 2000). This finding, however, needed to be confirmed through a
longitudinal study (Chapter 3).
This brings us to the limitations of the study described in Chapter 2. First, given the
study was cross-sectional in nature, any conclusions drawn with respect to recovery from
limb apraxia should be taken with caution. While it is likely that the lower frequency and
severity of limb apraxia among chronic patients may be due to the fact that these patients
would have had time to recover, only a longitudinal study can definitively address the
question of recovery. Another limitation of this study is that it did not include conceptual
knowledge tasks and tasks assessing imitation of non-representational gestures. The reason
conceptual gesture knowledge tasks were not included in the study was that we were
comparing performance of transitive and intransitive gestures and we had not developed
tasks that assess the patients‟ conceptual knowledge of intransitive gestures. Future studies,
should examine how knowledge and performance of the two gesture types interact and
determine the role of each hemisphere on one‟s knowledge of the two gesture types. Finally,
future studies should include non-representational (meaningless) gesture types in order to
explore hemispheric asymmetries in imitation of gestures using the direct route involving no
access to semantics.
Roy and colleagues found that selective imitation deficits could result from damage to
either hemisphere and our findings generally confirmed theirs (even though there was some
tendency for this deficit to be more prevalent after RHD). Selective deficits in imitation
would likely result from deficits in visuomotor transformation. Visuomotor transformation
deficits should also result in deficits in imitation of non-representational gestures and thus it

240
seems likely that patients presenting with selective deficits in imitation of meaningful
gestures will also suffer from deficits in imitation of meaningless gestures.
In Chapter 3, we reported on a longitudinal study undertaken to address the question
of recovery of limb apraxia post-stroke posed in Chapter 2. In this study, we again included
both LHD and RHD patients, as well as a few bilaterally affected patients (BHD).
Unfortunately, in this study the number of patients in each hemisphere group was not
sufficiently large to allow an examination of the differences in recovery rates between
hemisphere groups. We did, however, include more measures of apraxia, including both
conceptual tasks assessing the patients‟ knowledge of gestures and tools, as well as, a larger
number of gesture performance measures of apraxia than had been used in previous recovery
studies of apraxia. As is usually the case in clinical stroke studies, the longitudinal data
collected on the patients was somewhat variable: both the number of apraxia assessments (or
visits) each patient had and the time post stroke at which patients had joined our study varied
among patients. This prompted us to use Hierarchical Linear Modeling (HLM) (Raudenbush
& Bryk, 2002) which creates a growth curve model for the performance of each patient over
time, based on all existing data points per patient and then compares how the changes over
time vary across individuals.. In Chapter 3, we again included both acute-subacute and
chronic patients, as well as patients who were apraxic and patients who were not. We
predicted that if recovery of apraxia occurs, patients presenting with deficits on the first
examination would improve significantly more in performance accuracy over time than
patients without apraxia. In addition, we predicted that chronic apraxic patients would
improve less in their performance accuracy over time than acute-subacute apraxic patients,

241
given past studies reporting greater gains of apraxia recovery over the first three months post
stroke (Foundas et al., 1993; Basso et al., 2000).
Our predictions were largely confirmed. In gesture production tasks, such as
pantomime, imitation and object use, there were significantly larger gains in performance
over time in patients who started out as impaired than patients who were not. In addition,
chronic patients gained significantly less in performance accuracy over time than acute-
subacute patients, which confirmed Foundas et al.‟s findings (1993) that recovery gains are
more significant over the first three months post stroke. In regard to conceptual measures of
apraxia, we included three tasks in the analysis: Action Identification, Action Naming and
Tool Naming. There was no evidence of recovery in Action Identification, with patients who
were initially impaired not differing from patients who were not, in terms of their gains of
performance over time. In the two naming tasks, however, both acute-subacute and chronic
impaired patients showed significantly greater gains in performance relative to unimpaired
patients. We proposed that, while gains in naming tasks accuracy may stem from recovery of
deficits in language, the lack of recovery in Action Identification which does not involve
speech-language responses might indicate that the conceptual knowledge of gestures, may be
less susceptible to recovery. In addition, we hypothesized that continued practice in naming
in everyday life may promote continued recovery even in chronic patients.
In conclusion, while the cross-sectional study (Chapter 2) could only suggest that
recovery of limb apraxia post-stroke occurs, this longitudinal study confirmed that significant
spontaneous recovery does occur in stroke patients, more so in gesture production tasks, than
conceptual tasks of apraxia. Further detailed examination of conceptual tasks, should be
undertaken to confirm and expand these findings.

242
Much like in the first study in the thesis (Chapter 2), in this second study we aimed to
examine the patterns of limb apraxia deficits that stroke patients present with and to
determine how these patterns evolve over time. Generally, deficits in conceptual knowledge
of gestures were rare, with most patients presenting with damage to pantomime and/or
imitation. In regard to how the patterns evolved, it was difficult to draw general conclusions,
but it was observed that both chronic and acute-subacute patients tended to improve in their
patterns of deficits, suggesting that while group analysis suggests that most acute-subacute
patients recover, it is possible that chronic patients can also move from impaired to
unimpaired ranges. Finally, it should be noted that there were some cases where patients
deteriorated in their performance accuracy over time, which is unexpected after stroke. It is
possible that this was due to some underlying undiagnosed neurodegenerative disease and
future studies should aim to examine more such cases.
One limitation associated with this longitudinal study is that direct comparisons
between tasks could not be made, because to maximize the number of patients, separate
analyses were run for each task. Future studies should aim to compare statistically how
recovery gains may differ between task modalities. In addition, in this study (Chapter 3) only
transitive gestures were examined; future recovery studies should be expanded to include
intransitive and non-representational gestures. Also, while we included LHD, RHD and BHD
patients, we were unfortunately unable to examine directly if the side of stroke contributed
differentially to recovery due to small number of patients in each hemisphere group. Future
studies should aim to examine such effects in larger samples. Finally, the relationship
between lesion site and recovery should closely be examined and evolution of limb apraxia
patterns should be studied more closely, in order to better guide intervention practices.

243
The limitations of the statistical approach in this study should also be kept in mind.
While the statistical model suggests that a statistically significant amount of variability in the
slopes of patients is explained by whether patients were apraxic or not, steeper slopes were
observed in patients with apraxia suggesting recovery, it also showed that there is a large
amount of variability left unexplained. Therefore, other factors that may predict changes in
performance over time, such as hemisphere effects and specific lesion sites, should be
examined in the future.
EVIDENCE FROM CBS
As a complementary strategy to achieve the goal of providing new insight into how
the brain controls skilled movement through the study of limb apraxia, this thesis also
analyzed the performance of CBS patients, a neurodegenerative disorder in which limb
apraxia is pre-eminent, on our standardized battery of limb apraxia. Performance differences,
brain asymmetries, pattern presentations and changes over time were all examined much like
they were in stroke. As far as we are aware, this is the first study to compare and contrast
apraxia in these two neurologic disorders, comprehensively and within the same theoretical
framework.
Given the different role of the two hemispheres in the control of skilled movements,
as established through stroke studies, we hypothesized that patients with predominant left
hemisphere presentation (LHP) (i.e. right arm was more affected) would perform differently
than patients with predominant right hemisphere presentation (RHP). Thus, the first goal of
the study in Chapter 4 was to establish whether there are significant differences in
performance between the two hemisphere presentation groups, with the prediction that LHP
patients would perform with less accuracy than RHP patients. Our hypothesis was generally

244
confirmed, with LHP patients consistently showing a more severe impairment than RHP
patients, but the difference between the two groups was not significant. We propose that this
might be due to disease involvement in both hemispheres, even though the hemisphere that
was initially affected often has more severe neurodegeneration. However, the limited sample
size may have been insufficient to statistically detect any hemisphere differences.
Second, we aimed to contrast the performance of patients in different task modalities
and gesture types. Transitive gestures were more impaired than intransitive gestures, which
was consistent with our stroke findings in Chapter 2, as well as with previous literature in
CBS (Pharr et al., 2001; Salter, Roy, Black, Joshi, & Almeida, 2004; Chainay & Humphreys,
2003). Pantomime accuracy was lower than concurrent imitation in both transitive and
intransitive gestures, supporting findings by Leiguarda and colleagues (Leiguarda, 2001;
Pharr et al., 2001). The addition of Verbal Cuing during Concurrent Imitation of transitive
gestures decreased imitation accuracy, making performance similar to that of pantomime.
This finding was in contradiction to our expectation that providing both visual and auditory
cues should facilitate performance. It is possible that activation of the indirect route through
the provision of the verbal cue while imitating causes interference with the direct route,
which would support Chainay and Humphrey‟s convergent route model for action. This
suggests that deficits in one route could block a response via an intact route of action
(Chainay & Humphreys, 2002). Thus, if CBS patients have deficits in the indirect route to
imitation, even if the direct route for imitation is intact, damage to the indirect route may
interfere with the normal functioning of the direct route. There is also evidence, however, of
impairment to the direct route in that imitation of non-representational gestures was also
quite impaired in CBS, even more so than in representational gestures. Hence, there may be a

245
dual deficit involving both routes to action. Finally, comparisons between Concurrent and
Delayed Imitation, especially in transitive and intransitive gestures, found no differences in
performance between the two tasks, suggesting that patient do not have deficits in encoding
visual information into working memory, but rather their deficits reside in the final stage of
the production system, that of response organization and control (Roy, 1996).
Third, with respect to the patterns of limb apraxia deficits seen in CBS patients, we
expected that patients would show patterns in which both pantomime and imitation would be
impaired, while conceptual tasks would be relatively spared. In group analysis, CBS patients
were generally not impaired on any of the conceptual tasks which was consistent with past
research (Leiguarda, Lees, Merello, Starkstein, & Marsden, 1994; Graham, Zeman, Young,
Patterson, & Hodges, 1999; Soliveri, Piacentini, & Girotti, 2005).Our prediction with respect
to limb apraxia deficits were partly supported. In transitive gestures, the limb apraxia
patterns, as predicted, reflecting preserved conceptual knowledge of gestures, but impaired
pantomime and imitation, suggested deficits in the final stages of gesture production. For
intransitive gestures on the other hand, the limb apraxia patterns reflected only selective
deficits in imitation with preserved pantomime. This finding suggests that the conceptual
knowledge related to transitive gestures, as evidenced from the preserved ability to
pantomime intransitive gestures which requires access to semantics, is differentially
represented in the brain than conceptual knowledge of intransitive gestures. This finding is
not surprising, given the different function of the two gesture types, one communicative in
nature and the other related to instrumental activities. In addition, this finding is consistent
with other studies that have suggested a dissociation in the control of the two gesture types
(Mozaz, Rothi, Anderson, Crucian, & Heilman, 2002; Buxbaum et al., 2007).

246
One major limitation of Chapter 4 is that we inferred which hemisphere was more
affected by grouping patients by the side of presentation. However, only neuroimaging
studies directly estimating the level of degeneration would be able to determine which
hemisphere is more affected by the disease. Therefore, future studies should directly link
neuroimaging findings to limb apraxia performances.
With the goal of examining changes overtime in performance accuracy, Chapter 5
examined the nature of progression of limb apraxia in CBS. Our prediction was, given the
progressive nature of CBS, that patients‟ performance would deteriorate over time. We were
unsure, however whether conceptual knowledge deficits would eventually emerge. Our
previous study (Chapter 4) demonstrated that patients are rarely impaired in their conceptual
knowledge of gestures and tools, while gesture production tasks are often quite impaired. We
wondered whether, conceptual tasks remain unimpaired or if they eventually become
impaired as do gesture production tasks. With these goals in mind, seven of the seventeen
patients included in our group analysis study (Chapter 4) were followed-up for several years.
We showed in this longitudinal case series that conceptual tasks were more resistant to
deterioration over time. Only some patients deteriorated in their performance on conceptual
tasks, while other CBS patients preserved their ability to perform on these tasks throughout
the entire disease duration. All patients, however, deteriorated in gesture production
performance and the few patients who started out without apraxia eventually developed
apraxia. In all cases, apraxia was always present at least in the affected limb. This study,
however, was purely descriptive in nature. There were a lot of missing data, partly due to the
fast progression of deficits in CBS, often rendering patients untestable. Our sample was also
quite small, including only seven patients. Future studies should aim to gather more patients

247
and determine quantitatively the patterns of progression in the various apraxia domains. In
addition, here it would be important to examine whether there are certain neuroanatomical
regions that play an important role in determining which patients deteriorate conceptually
and which patients do not.
CONVERGING EVIDENCE FROM STUDIES IN LIMB APRAXIA IN STROKE
AND CBS
What are some of the conclusions that can be drawn based on our findings from the
studies in both stroke and CBS? First, our findings in both populations suggest that the
conceptual and production system may be affected independently. Deficits in tasks assessing
gesture and tool knowledge are less frequent in both stroke and CBS as opposed to deficits in
the production system (Chapter 3 & 4). In addition, the two systems change differently over
time in both disorders. In stroke, in Chapter 3, we showed that conceptual tasks are not likely
to recover if initial deficits occur, while the production system shows significant gains in
performance accuracy over time. In CBS, while deterioration in gesture production system
stemming from deficits in the production system is quite common, many patients do not
show any deficits in tools and gesture knowledge and remain without deficits throughout the
disease progression. Therefore, all our findings support the notion that there are two separate
systems that are involved in the control of movement and they can not only be affected
differentially by disease, but they are also differentially prone to recovery in stroke and
deterioration in CBS.
While studies in stroke have taught us a tremendous amount of the role of the various
neuroanatomical regions in the control of movement, it is important to integrate findings
from stroke with findings from studies of limb apraxia in neurodegenerative disorders, such

248
as CBS. Such integration is important, because the brain regions affected by different
neurological disorders are distinct and thus can provide different insights into the role of
various brain regions in the control of movement. For example, stroke studies are limited by
cerebrovascular anatomy and they can often be quite severe affecting a large area of the
brain, which makes it sometimes difficult to draw general conclusions of the role of specific
brain subregions. In neurodegenerative disorders, the areas of the brain affected are not
limited by cerebrovascular anatomy, but by selective vulnerability to the neurodegenerative
process, which while still poorly understood gives an opportunity to examine the effects of
damage to distinct neural networks. Aside from differences, it is also important to examine
commonalities in performance of skilled movement of patients affected by distinct
neuropathology which may provide us with additional insights in the neuroanatomical basis
of skilled movement performance if common networs are affected. For example, in both
stroke and CBS, we found confirmation that the left hemisphere plays a larger role in
apraxia. In stroke, LHD stroke patients were significantly more affected than RHD patients.
In CBS, differences between the two hemisphere groups did not reach significance, but
patients with LHP were more severely affected. In addition, based on the patterns of limb
apraxia in stroke, it was suggested that the left hemisphere might be dominant in the final
stages of the control of skilled movement, while conceptual knowledge and visuomotor
transformations may be under bilateral control.
In CBS, distinct patterns were also observed depending on the gesture type being
assessed. In transitive gestures, deficits in both pantomime and imitation were observed,
while in intransitive gestures selective deficits in imitation were observed. In stroke, this was
not the case; deficits in both pantomime and imitation were most common in both transitive

249
and intransitive gestures. However, the pattern characterized by deficits in imitation alone
seemed to be somewhat more prevalent in intransitive than transitive gestures. While future
studies need to examine more closely these gesture-type differences in limb apraxia patterns,
converging evidence from stroke and CBS suggests that the control of transitive versus
intransitive gestures is differentially represented in the brain.
Limitations Common to both the Stroke and CBS Studies
There are several limitations associated with the battery used, which apply to both the stroke
and CBS studies in this thesis. First, due to the fact that the battery is scored through visual
rating, the rating of movement errors could be relatively insensitive (for example, deviations
from the normal kinematic features of a movement may not be visible to the naked eye). In
addition, visual rating is very subjective and while high inter-rater reliability has been shown
with the scoring procedures in the battery, some scores may have been influenced by rater
judgement. In addition, the full psychometric characteristics of the battery have not been
established (See Appendix A). For example, the lack of test-retest reliability studies should
be taken into consideration in the interpretation of the longitudinal studies in Stroke (Chapter
3) and CBS (Chapter 5).
Finally, in my analysis throughout, I have averaged the percentage accuracy scores between
the left and the right hand of the controls to compare with the performance of the patients. In
both stroke and CBS, one side is usually more affected than the other (due to paralysis or
weakness in stroke, or due to extrapyramidal features in CBS). Therefore, patients are usually
assessed with their less affected side, which in the case of LHP CBS patients or LHD Stroke
patients, is the non-dominant left hand. We could expect differences in performance between
hands, with the likelihood that the the dominant hand would be more accurate. Past studies in

250
our lab (Roy, Square-Storer, Hogg, & Adams, 1991), however, showed no differences
between the performances of the two hands of normal control participants.Therefore, in all
studies, we took the average of the two hands as a standardization for all performances across
patients, irrespective of the hand being used. Theoretically, this may have inflated the
average to which the left hand performance of patients was being compared, and thus LHD
stroke or LHP CBS patients may have appeared to be more impaired than they really were.
Even if this were the case, however, the results would likely not have changed dramatically,
given our past studies showing no hand differences between hands in the controls. We chose
to compare the left vs. right hand performance in the patients to a common average, which
allowed for a better comparison between the groups, but this limitation should be kept in
mind by the reader, when reading about the comparisons between left vs. right hemisphere
groups.
THESIS CONTRIBUTIONS AND CONCLUDING REMARKS
This thesis work has significantly enhanced to our understanding of limb apraxia
deficits through comparing apraxia in the two clinical populations, stroke and CBS, in
gesture performance on various task modalities, and has provided new insights into our
understanding of how each hemisphere controls skilled movement. Apart from the two
studies conducted by Roy and colleagues (Roy et al., 2000; Heath et al., 2001), one on
transitive and one on intransitive gestures, no studies to date have examined limb apraxia
patterns in stroke patients, as comprehensively within the same subjects. In CBS, no studies
have even attempted to describe apraxia patterns as completely as this work. The thesis also
examined changes over time in limb apraxia performance in both clinical populations. While
several studies in stroke have examined recovery of limb apraxia, this work has expanded on

251
previous findings by including a greater variety of tasks and by including RHD stroke
patients in the recovery analysis. In CBS, this work represents the first ever examination of
progression of limb arpaxia deficits. Finally, in regard to the study of the study of
lateralization of function related to the control of skilled movement, while numerous studies
have examined the differential role of each hemisphere in limb apraxia after stroke, this work
attempts for the first time to examine hemisphere differences in the context of CBS.

252
REFERENCES
Barbieri, C. & Derenzi, E. (1988). The executive and ideational components of
apraxia. Cortex., 24, 535-543.
Basso, A., Burgio, F., Paulin, M., & Prandoni, P. (2000). Long-Term Follow-up of
Ideomotor apraxia. Neuropsychological Rehabilitation, 10, 1-13.
Buxbaum, L. J., Kyle, K., Grossman, M., & Coslett, H. B. (2007). Left inferior
parietal representations for skilled hand-object interactions: Evidence from stroke and
corticobasal degeneration. Cortex, 43, 411-423.
Chainay, H. & Humphreys, G. W. (2002). Neuropsychological evidence for a
convergent route model for action. Cognitive Neuropsychology, 19, 67-93.
Chainay, H. & Humphreys, G. W. (2003). Ideomotor and ideational apraxia in
corticobasal degeneration: A case study. Neurocase., 9, 177-186.
De Renzi, E., Motti, F., & Nichelli, P. (1980). Imitating gestures. A quantitative
approach to ideomotor apraxia. Archives of Neurology, 37, 6-10.
Donkervoort, M., Dekker, J., van den Ende, E., Stehmann-Saris, J. C., & Deelman, B.
G. (2000). Prevalence of apraxia among patients with a first left hemisphere stroke in
rehabilitation centres and nursing homes. Clinical Rehabilitation., 14, 130-136.
Foundas, A. L., Raymer, A. M., Maher, L. M., Gonzalez-Rothi, L., & Heilman, K. M.
(1993). Recovery in Ideomotor Apraxia. Journal of Clinical Experimental Neuropsychology,
14, 44.

253
Geschwind, N. (1975). The Apraxias: Neural Mechanisms of Disorders of Learned
Movements. American Scientist, 63, 188-195.
Geschwind, N. & Kaplan, E. (1962). A human cerebral disconnection syndrome.
Neurology, 12, 675-685.
Graham, N. L., Zeman, A., Young, A. W., Patterson, K., & Hodges, J. R. (1999).
Dyspraxia in a patient with corticobasal degeneration: the role of visual and tactile inputs to
action. Journal of Neurology Neurosurgery and Psychiatry, 67, 334-344.
Haaland, K. Y. & Flaherty, D. (1984). The different types of limb apraxia errors made
by patients with elft vs. right hemispehre damage. Brain and cognition, 3, 370-384.
Haaland, K. Y., Harrington, D. L., & Knight, R. T. (2000). Neural representations of
skilled movement. Brain, 123, 2306-2313.
Heath, M., Roy, E. A., Black, S. E., & Westwood, D. A. (2001). Intransitive limb
gestures and apraxia following unilateral stroke. Journal of clinical and experimental
neuropsychology, 23, 628-642.
Kimura, D. & Archibald, Y. (1974). Motor functions of the left hemisphere. Brain,
97, 337-350.
Leiguarda, R. (2001). Limb apraxia: cortical or subcortical. NeuroImage, 14, S137-
S141.

254
Leiguarda, R., Lees, A. J., Merello, M., Starkstein, S., & Marsden, C. D. (1994). The
nature of apraxia in corticobasal degeneration. Journal of Neurology, Neurosurgery &
Psychiatry, 57, 455-459.
Liepmann, H. (1988). Apraxia. In J.W.Brown (Ed.), Agnosia and Apraxia: Selected
papers of Liepmann, Lange and P+â-¦tzl (1st Ed. ed., pp. 3-42). Hillsdale, New Jersey:
Lawrence Erlbaum Associates, Publishers.
Mozaz, M., Rothi, L. J., Anderson, J. M., Crucian, G. P., & Heilman, K. M. (2002).
Postural knowledge of transitive pantomimes and intransitive gestures. Journal of the
International Neuropsychological Society, 8, 958-962.
Pharr, V., Uttl, B., Stark, M., Litvan, I., Fantie, B., & Grafman, J. (2001). Comparison
of apraxia in corticobasal degeneration and progressive supranuclear palsy. Neurology., 56,
957-963.
Raudenbush, S. W. & Bryk, A. S. (2002). Hierarchical Linear Models: Applications
and Data Analysis Methods. (2nd ed.) Sage publications.
Roy, E. A. (1996). Hand Preference, Manual Assymetries, and Limb Apraxia. In
D.Elliot (Ed.), Manual Asymmetries in Motor Control (pp. 215). Boca Raton, FL: CRC Press.
Roy, E. A., Heath, M., Westwood, D., Schweizer, T. A., Dixon, M. J., Black, S. E. et
al. (2000). Task demands and limb apraxia in stroke. Brain and cognition, 44, 253-279.
Salter, J. E., Roy, E. A., Black, S. E., Joshi, A., & Almeida, Q. (2004). Gestural
imitation and limb apraxia in corticobasal degeneration. Brain & Cognition, 55, 400-402.

255
Schnider, A., Hanlon, R. E., Alexander, D. N., & Benson, D. F. (1997). Ideomotor
apraxia: behavioral dimensions and neuroanatomical basis. Brain & Language, 58, 125-136.
Soliveri, P., Piacentini, S., & Girotti, F. (2005). Limb apraxia in corticobasal
degeneration and progressive supranuclear palsy. Neurology, 64, 448-453.
Stamenova, V., Roy, E. A., & Black, S. E. (2009). A model-based approach to
understanding apraxia in corticobasal syndrome. Neuropsychology review, 19, 47-63.

256
APPENDIX A: THE SUNNYBROOK-WATERLOO APRAXIA BATTERY
Gesture Types Included in the Battery
List of Transitive Gestures: a comb, spatula, hammer, fork, knife, watering can,
toothbrush and tweezers.
List of Intransitive Gestures: waving good-bye, saluting, making okay sign, putting
cream on one‟s face, beckoning, holding one‟s nose as if there were a bad smell, making the
okay sign, scratching one‟s ear and hailing a cab.
Non-representational (meaningless gestures): matched with the representational gestures
with regard to static or dynamic features.
For all gesture types, half of the gestures consisted of movements toward the body and
half involved movements away from the body (Roy, Black, Blair, & Dimeck, 1998; Roy et
al., 2000).
Part 1: Conceptual Component of Apraxia Battery
A. Tool Naming and Identification Tasks:
Tool Naming: participants were asked to name the tool presented in a black and white
picture in front of them.
Tool Name by Function: participants are asked to name tools based on their function. For
example, participants are asked, “What would you use to slice a piece of bread?” and are
expected to reply “knife”.
Tool Naming by Action: the examiner pantomimes a gesture and the participants were
asked to name the tool the examiner is pretending to be using.

257
Tool Identification (ID): participants were shown four pictures: the correct picture
(knife), a semantically related foil (soup ladle), a functionally related foil (saw), and an
unrelated object (napkin) and participants are instructed to point to the object being named
(e.g. “Point to the knife).
Tool ID by Function: participants were again shown 4 pictures, much like in Tool ID, but
in this case the participants were asked to point to the tool that had the function described by
the experimenter (e.g. “Point to the object you would use to slice a piece of bread.”).
Scoring: In all of the above tasks the number of correct responses was recorded and
subsequently converted to percent accuracy score.
B. Gesture Identification Tasks
Action Identification: participants are presented with five video clips per gesture, each
showing an actor pantomiming a different correctly performed gesture taken from the set of
stimuli in this battery. One of the clips shows the actor performing the gesture in question,
two clips show correctly performed gestures towards the body and two clips show correctly
performed gestures away from the body. Patients are asked to indicate after presentation of
each video clip whether it showed an actor pretending to perform a specific gesture (e.g., “Is
the subject in the video pretending to use a knife to slice a piece of bread?” and the patient
says „Yes” or “No”).
Action ID by Tool: the task is administered in much the same way as in Action ID, but in
this case the examiner holds a tool and asks the participant: “Is the subject in the video
pretending to use the tool I am holding?” and the patient says „Yes” or “No”.
Gesture Matching: participants are shown a video clip of five correctly performed
gestures taken from the stimuli used in this battery. Two gestures are performed toward the

258
body, two are performed away from the body, and one gesture is identical to the gesture
being demonstrated by the experimenter. As each video clip is presented, the experimenter
demonstrates the gesture and asks: “Is the subject in the video doing the same thing I am
doing?”.
Gesture Error Recognition: participants are presented with four video clips per object,
one correctly performed action and three foils. One foil showed an error in the gesture
motion (action error), one showed the action being performed correctly but in an incorrect
spatial location, and one showed a body part as object error. In the case of knife, one clip
showed an actor correctly pantomiming the action of slicing a piece of bread with a knife,
one showed a slicing gesture performed with an action error (e.g. the actor performs a
circular motion rather than a slicing motion), one showed a gesture performed with a location
error (e.g., a slicing motion done to the side of the head rather than in front of the body) and
one showed a slicing gesture performed with body part as object (e.g., actor has extended his
finger to represent the knife rather than the correct posture appropriate for holding a knife in
the hand). Participants are asked each time “Is the subject in the video performing the
gesture correctly?” and they respond “Yes” or “No” following presentation of each video
clip.
Scoring: In all visual-gestural knowledge tests participants were told that there might
be more than one correct response. If a participant gives a wrong response for any one of the
series of clips per gesture, the response on that gesture is recorded as wrong. This was done,
because the gestures within each series targeted one particular gesture and therefore if a
patients fails to identify the correct gesture or accepts another gesture as the gesture being in
question, the representation of that gesture is considered to be affected.

259
Part 2: Gesture Performance Component of the Apraxia Battery
Pantomime to Verbal Command for Transitive Gestures: patients are given a verbal
instruction to perform gestures, such as “Show me how you would use a hammer to pound a
nail.” The patient is instructed to pretend to hold the object in their hand and to perform the
gesture.
Pantomime to Verbal Command for Intransitive Gestures: Same as above, except the
intransitive gestures were used.
Pantomime by Picture: the participant is presented with a picture of a tool and asked:
“Show me how you would use this”.
Pantomime by Function: the participant is given the function of the object only (e.g.
“Show me how you would slice a piece of bread?”) and asked to pantomime the gesture.
Object (Tool) Use: the participant is given the actual tool to hold and asked to pretend to
use the tool.
Delayed Imitation for Transitive Gestures: the examiner performs a gesture and the
patient is instructed to wait for the examiner to finish the gesture and the patient is then to
imitate as best as possible the gesture that was demonstrated.
Delayed Imitation for Intransitive Gestures: Same as above, except intransitive gestures
are used.
Delayed Imitation for Non-Representational Gestures: Same as above, except non-
representational gestures are used.
Concurrent Imitation of Transitive Gestures: the patient imitates the gesture presented by
the examiner. The examiner continues the gesture presentation until the patient performs the
imitation.

260
Concurrent Imitation with Verbal Cue: participants were asked to imitate concurrently
the gesture demonstrated by the examiner, while the examiner is also giving a verbal
instruction, much like the one given in pantomime. (e.g.: “Show me how you would used a
knife to slice a piece of bread”). This is done only for transitive gestures.
Concurrent Imitation of Intransitive Gestures: the patient imitates the gesture presented
by the examiner. The examiner continues the gesture presentation until the patient performs
the imitation.
Concurrent Imitation of Non-Representational Gestures: Same as above, except non-
representational gestures are used.
Scoring: The patients were videotaped while performing the gesture and were scored
on 5 performance dimensions: location, posture, action, plane and orientation. Location
referred to the location in space of the arm relative to the body. Posture was the hand posture
of the participant. Action referred to the movement characteristics of the gesture. Orientation
was the orientation of the palm. Each dimension was scored on a 3-point scale: 2 (correct),
1(distorted) and 0 (incorrect). Specific criteria have been established that need to be met for
each dimension within a gesture. If all criteria are met, the patient receives a score of 2, if
one of the criteria is not met, then the patient receives a score of 1 and if two or more of the
criteria are not met the patient receives a score of 0. Performance on each dimension was
then expressed by calculating the percentage of the maximum score achieved across the eight
gestures. A composite score for each task was calculated by taking the average of the
percentage scores of the five dimensions. Performance was scored using procedures with
high interrater reliability (Roy et al., 1998). Intra-rater reliability on a subsample of patients
has been shown to be in at least 80% agreement. Test-retest reliability has not been

261
established. Concurrent validity for the battery is difficult to establish given the lack of
generally accepted and well-recognized limb apraxia assessments with which the Waterloo-
Sunnybrook Limb Apraxia battery can be compared, but content validity is high, given the
battery contains a wide variety of tasks assessing comprehensively different aspects of limb
praxis performance. Finally, the results from the analysis of data accumulated with the
Waterloo-Sunnybrook Limb Apraxia battery in this thesis dissertation were consistent with
the Conceptual Production Model proposed by Roy (1996), which by itself strengthens the
validity of the battery in two different clinical populations: stroke and Corticobasal
Syndrome.
References
Roy, E. A., Black, S. E., Blair, N., & Dimeck, P. T. (1998). Analyses of deficits in
gestural pantomime. Journal of clinical and experimental neuropsychology, 20, 628-643.
Roy, E. A., Heath, M., Westwood, D., Schweizer, T. A., Dixon, M. J., Black, S. E. et
al. (2000). Task demands and limb apraxia in stroke. Brain and cognition, 44, 253-279.
Roy, E. A., Square-Storer, P., Hogg, S., & Adams, S. (1991). Analysis of task
demands in apraxia. International Journal of Neuroscience, 56, 177-186.