
A Look Model for Improvement - Video Libraryvideos.med.wisc.edu/files/Little.pdf · Model for...
63
A Look at the Model for Improvement Presented by Content Expert: Kevin Little, PhD Informing Ecological Design, LLC This presentation is part of an on‐line series, brought to you through a collaboration between the Wisconsin Office of Rural Health and the Wisconsin Hospital Association. Property of the Wisconsin Office of Rural Health.
Transcript of A Look Model for Improvement - Video Libraryvideos.med.wisc.edu/files/Little.pdf · Model for...
A Look at the Model for Improvement
Presented by Content Expert:Kevin Little, PhD
Informing Ecological Design, LLCg g g ,
This presentation is part of an on‐line series, brought to you through a collaboration between the Wisconsin Office of Rural Health and the Wisconsin Hospital Association.
Property of the Wisconsin Office of Rural Health.

DisclosureDisclosure
Kevin Little, Ph.D. has used the Model for Improvement in his work sinceModel for Improvement in his work since2000; he has served as an ImprovementAdvisor for the Institute for HealthcareAdvisor for the Institute for HealthcareImprovement since 2001. He knows several of the API consultants as colleaguesseveral of the API consultants as colleaguesand friends.
This presentation is part of an on‐line series, brought to you through a collaboration between the Wisconsin Office of Rural Health and the Wisconsin Hospital Association.
Property of the Wisconsin Office of Rural Health.

How can you get to your destination?How can you get to your destination?
This presentation is part of an on‐line series, brought to you through a collaboration between the Wisconsin Office of Rural Health and the Wisconsin Hospital Association.
Property of the Wisconsin Office of Rural Health.

Today’s SessionToday s Session
• A basic description of the Model• Brief history• When should the Model be used? • Advantages and disadvantages• Resources and sample team selection • Model Details• Lean and Six Sigma connections• Top learning resources
This presentation is part of an on‐line series, brought to you through a collaboration between the Wisconsin Office of Rural Health and the Wisconsin Hospital Association.
Property of the Wisconsin Office of Rural Health.

The Model for Improvement Basic DescriptionBasic Description
D l d bDeveloped by Associates in Process Improvement
(API)
This presentation is part of an on‐line series, brought to you through a collaboration between the Wisconsin Office of Rural Health and the Wisconsin Hospital Association.
Property of the Wisconsin Office of Rural Health.

Three Fundamental Questions for Improvement
• What are we trying to accomplish?
• How will we know that a change is an• How will we know that a change is an improvement?
• What change can we make that will result in improvement?
This presentation is part of an on‐line series, brought to you through a collaboration between the Wisconsin Office of Rural Health and the Wisconsin Hospital Association.
Property of the Wisconsin Office of Rural Health.
A Test CycleA Test Cycle
PlanAct
DoStudy

The Questions + The CycleQ y
M d l f I tWhat are we trying to
accomplish?
H ill k th t
Model for Improvement
How will we know that achange is an improvement?
What change can we make thatwill result in improvement?p
PlA PlanAct
DoStudy
© 2009 API, used by permission
DoStudy

Brief History
This presentation is part of an on‐line series, brought to you through a collaboration between the Wisconsin Office of Rural Health and the Wisconsin Hospital Association.
Property of the Wisconsin Office of Rural Health.

Roots in W.E. Deming’s ContributionsRoots in W.E. Deming s Contributions
• Plan‐Do‐Study‐Act cycle (Walter Shewhart 1939 and Deming’s courses in Japan, 1950)Deming s courses in Japan, 1950)
•Theory of Profound Knowledge (1992)( )
‐ Appreciation for a system‐ Knowledge about Variation‐ Theory of Knowledge‐ Theory of Knowledge‐ Psychology
1900-1993
This presentation is part of an on‐line series, brought to you through a collaboration between the Wisconsin Office of Rural Health and the Wisconsin Hospital Association.
Property of the Wisconsin Office of Rural Health.
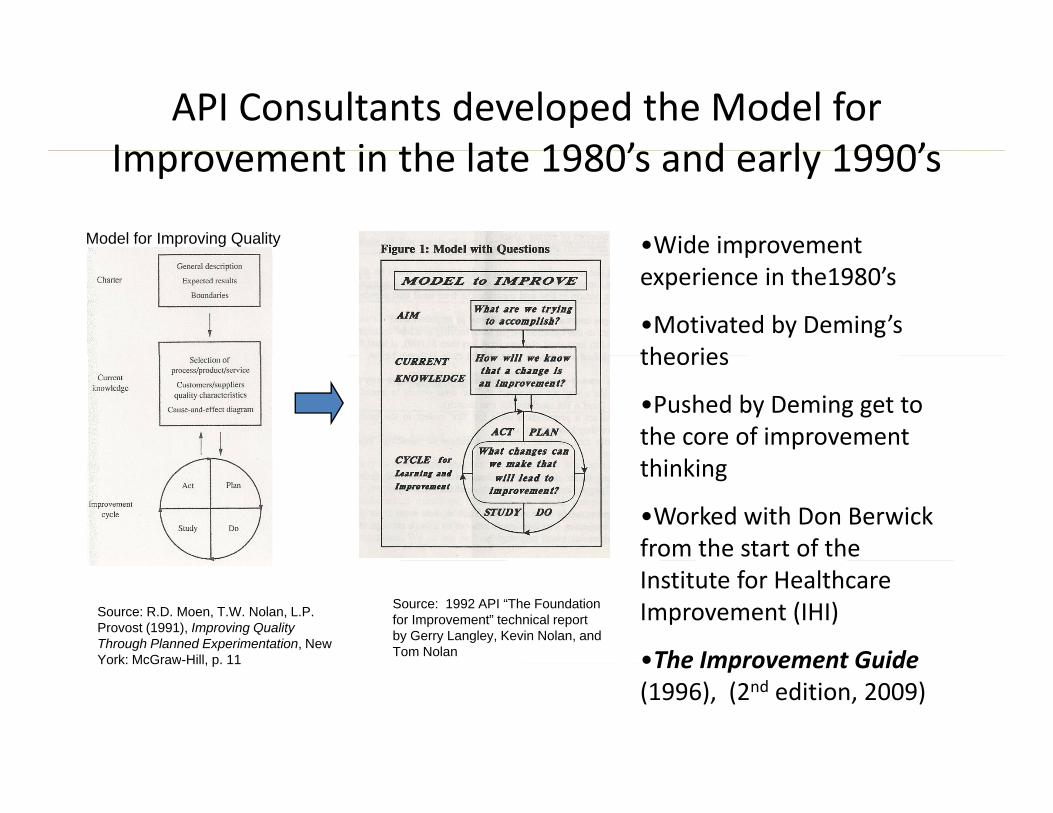
API Consultants developed the Model for I t i th l t 1980’ d l 1990’Improvement in the late 1980’s and early 1990’s
•Wide improvementModel for Improving Quality Wide improvement experience in the1980’s
•Motivated by Deming’s theoriestheories
•Pushed by Deming get to the core of improvement thinking
•Worked with Don Berwick from the start of the
Source: 1992 API “The Foundation for Improvement” technical report by Gerry Langley, Kevin Nolan, and Tom Nolan
Institute for Healthcare Improvement (IHI)
•The Improvement Guide
Source: R.D. Moen, T.W. Nolan, L.P. Provost (1991), Improving Quality Through Planned Experimentation, New York: McGraw-Hill, p. 11 •The Improvement Guide
(1996), (2nd edition, 2009)York: McGraw Hill, p. 11
Design Criteria used to create the Model for Improvement
1 It works1. It works
2. Applies to products and processes, from i l t lsimple to complex
3. Quick to apply
4. Success by a variety of users, in all environments
5. Fun to use
6. Promotes learning
G. Langley, K. Nolan, T. Nolan (1992), The Foundation of Improvement, API, p. 1

Engine for change used by IHI in…Engine for change used by IHI in…
B kth h S i C ll b ti t ti 1995• Breakthrough Series Collaboratives starting 1995• Breakthrough Series College• IMPACT Communities e gIMPACT Communities, e.g.
‐ Improving Flow through Acute Care Settings‐ Improving Outcomes for High‐Risk and Critically Ill Patients
100 000 i i• 100,000 Lives campaign• 5,000,000 Lives campaign• System interventions (VA Community Health Centers U K• System interventions (VA, Community Health Centers, U.K. National Health Service, Indian Health Service)• Etc.
This presentation is part of an on‐line series, brought to you through a collaboration between the Wisconsin Office of Rural Health and the Wisconsin Hospital Association.
Property of the Wisconsin Office of Rural Health.
When should the Model for Improvement
be used?
This presentation is part of an on‐line series, brought to you through a collaboration between the Wisconsin Office of Rural Health and the Wisconsin Hospital Association.
Property of the Wisconsin Office of Rural Health.

One‐time Journey or a Trekking Service?One time Journey or a Trekking Service?
This presentation is part of an on‐line series, brought to you through a collaboration between the Wisconsin Office of Rural Health and the Wisconsin Hospital Association.
Property of the Wisconsin Office of Rural Health.

A General Method!A General Method!
• Any improvement effort
• Individuals teams and whole organizations• Individuals, teams and whole organizations
• Formality and structure vary, not concepts
This presentation is part of an on‐line series, brought to you through a collaboration between the Wisconsin Office of Rural Health and the Wisconsin Hospital Association.
Property of the Wisconsin Office of Rural Health.

Ingredients Needed to Changeg g
Will to Change
Ideas for Change
Executiong
Nolan, T.W. A primer on leading improvement in health care. Presented at the Fifth European Forum on Quality Improvement in Health Care, Amsterdam, March 24, 2000. Used by permission.

Three Uses of the ModelThree Uses of the Model
1. Develop new knowledge
2. Test (adapt) ideas*
3 Implement (deploy) ideas*3. Implement (deploy) ideas
*Typical uses in “improvement collaboratives”Typical uses in improvement collaboratives
This presentation is part of an on‐line series, brought to you through a collaboration between the Wisconsin Office of Rural Health and the Wisconsin Hospital Association.
Property of the Wisconsin Office of Rural Health.

Scope of Improvement ProjectsScope of Improvement Projects
• Personal improvement• Test of a clinical change
small
• Reduce Hospital Acquired Infections• Improve ED flow across a set ofImprove ED flow across a set of hospitals
• Indian Health Service Primary CareIndian Health Service Primary Care System Improvement
Large
This presentation is part of an on‐line series, brought to you through a collaboration between the Wisconsin Office of Rural Health and the Wisconsin Hospital Association.
Property of the Wisconsin Office of Rural Health.
g

Example: Reducing Hospital Acquired InfectionsAcquired Infections
St. John’s Regional Health Center, Springfield, MOg , p g ,Improvement Report on IHI website
http://www.ihi.org/IHI/Topics/HealthcareAssociatedInfections/InfectionsGeneral/ImprovementStories/ReducingHealthcareAssociatedMRSAInfectionsonaSurgicalUnit htmImprovementStories/ReducingHealthcareAssociatedMRSAInfectionsonaSurgicalUnit.htm
This presentation is part of an on‐line series, brought to you through a collaboration between the Wisconsin Office of Rural Health and the Wisconsin Hospital Association.
Property of the Wisconsin Office of Rural Health.

What Are We Trying to Accomplish?y g p
i i 30 d i f i l iAim: To sustain 30 percent reduction of surgical site infections (SSIs), bloodstream infections (BSIs), and healthcare‐associated pneumonia (HAP) due to methicillin‐resistant Staphalococcus aureus (MRSA) by focusing on prevention of transmission on 7C Surgical Unit. Sustain compliance at greater than or equal to 90 percent on process measures for reliable hand hygiene, contact precaution for isolation patients, and appropriate room cleaning/disinfections on 7C Surgical Unit. Achieve 98 percent compliance obtaining admission active surveillance cultures (ASC) in adult intensive care units (ICU), pediatric ICU, and the burn unit.

How will we know that a change i i t?is an improvement?
MeasuresMeasuresProcess Measures:•% targeted patients with admission active surveillance
culture collected •% environmental cleanings completed appropriately •% patient encounters with compliance for contact % p p
precautions •% patient encounters with compliance for hand hygiene
Outcome Measures:•Days between MRSA infections •Rate of occurrence of MRSA SSI, BSI, and HAP per
1,000 patient days

What change(s) can we make that ill l d i ( )?will lead to improvement(s)?
Hand Hygiene:Hand Hygiene:• Provide alcohol‐based hand rub for patients on bedside table • Implement “hands up” campaign — the standard phrase or
ti t if b th k NOTaction to use if you observe another co‐worker NOT performing hand hygiene when appropriate
Contact Precautions:d if i l i i b l i i k i• Identify isolation patients by placing a sticker on patient menu and placing in designated area for dietary staff
• Visual aid placed on isolation holders as a reminder to h d h i i t d i PPEencourage hand hygiene prior to donning PPE
Room Cleaning and Disinfection:• Identify clean equipment with red “door knocker” tag• High touch cleaning checklist provided to workers

A Useful Idea and Data Drive ChangeA Useful Idea and Data Drive Change
The team reports:The team reports:
The project ‘tipping point’ occurred when we began to culture hands and equipment of workers [see image [ gat left depicting culture on worker's hand and culture onhand and culture on stethoscope equipment]

Performance Measures
Process Measures
Outcome Measure

Example: System‐scale improvementimprovement
Indian Health Service Primary Care InitiativeN. L. Kuchar et al., “The Indian Health Service Chronic Care Initiative: Innovations in Planned Care
for the Indian Health System”, IHS Provider, April 2009, 112‐114http://www.ihi.org/NR/rdonlyres/2B3B878A-D71F-4B9F-A718-
B0720224DF8F/0/ReidheadetalIHSChronicCareInitiative IHSProviderApr09 pdfB0720224DF8F/0/ReidheadetalIHSChronicCareInitiative_IHSProviderApr09.pdf
This presentation is part of an on‐line series, brought to you through a collaboration between the Wisconsin Office of Rural Health and the Wisconsin Hospital Association.
Property of the Wisconsin Office of Rural Health.
Aim
To improve health and promote wellness for AmericanTo improve health and promote wellness for American Indians and Alaska Natives across all ages. The redesigned system of care will be grounded in the values d l f h i d I ill fand culture of the community served. It will focus on
strengthening the positive relationships between the healthcare system/care team and the community, family, and individual. The adapted Care Model* serves as a framework to guide the creation of an efficient and accessible system of care that provides safe, timely,accessible system of care that provides safe, timely, effective, equitable, and patient‐centered care.
*http://www.improvingchroniccare.org/index.php?p=The_Chronic_Care_Model&s=2

Example Measuresp
Clinical PreventionClinical PreventionKeeping current on Preventive screeningsKeeping current on Cancer‐related screenings
Management and Prevention of Chronic ConditionsManagement and Prevention of Chronic ConditionsControl of Blood PressureControl of Lipids
CostsCostsRevenue GenerationStaff Satisfaction and other workforce measures
Patient ExperiencePatient ExperienceExperience and EfficiencyPatient ActivationPatient SatisfactionPatient SatisfactionBuilding relationships for careAccess – Primary Care and Dental

Example Change Ideasp g
•Empanelling•Empanelling•Care team•Use data to drive improvementUse data to drive improvement•Optimize use of HIT•Remove waste•Plan for every patient•Segment careR i d t•Reminders system
•Move work to appropriate licensure•Reliable follow‐upReliable follow up•Max packing
When is the Model for Improvement
not applicable?
This presentation is part of an on‐line series, brought to you through a collaboration between the Wisconsin Office of Rural Health and the Wisconsin Hospital Association.
Property of the Wisconsin Office of Rural Health.

Two Limiting SituationsTwo Limiting Situations
• Insufficient will to improve
• An alternative improvement method is already embeddedmethod is already embedded
This presentation is part of an on‐line series, brought to you through a collaboration between the Wisconsin Office of Rural Health and the Wisconsin Hospital Association.
Property of the Wisconsin Office of Rural Health.

Advantages and DisadvantagesAdvantages and Disadvantages of Using the Model for g
Improvement
This presentation is part of an on‐line series, brought to you through a collaboration between the Wisconsin Office of Rural Health and the Wisconsin Hospital Association.
Property of the Wisconsin Office of Rural Health.

Advantages of the ModelAdvantages of the Model
A li t ll l l f i ti• Applies to all levels of an organization– well‐defined, high volume processes to informal, low‐volume processes
– Executives, providers, support staff• Minimally prescriptive, maximally adaptive• Formality can vary• Formality can vary• Stresses user empowerment, learning and growth of knowledge
• Advanced skills not a requirement for use
See The Improvement Guide, 2nd edition, p. 455
This presentation is part of an on‐line series, brought to you through a collaboration between the Wisconsin Office of Rural Health and the Wisconsin Hospital Association.
Property of the Wisconsin Office of Rural Health.
p , , p

Disadvantages?Disadvantages?
• No cookbook• Expect and manage some failuresExpect and manage some failures in testing
• Data‐drivenData driven
This presentation is part of an on‐line series, brought to you through a collaboration between the Wisconsin Office of Rural Health and the Wisconsin Hospital Association.
Property of the Wisconsin Office of Rural Health.

Resources Needed to Use the M d l f I tModel for Improvement
This presentation is part of an on‐line series, brought to you through a collaboration between the Wisconsin Office of Rural Health and the Wisconsin Hospital Association.
Property of the Wisconsin Office of Rural Health.

Ingredients Needed to Changeg g
Will to Change
Ideas for Change
Executiong
Nolan, T.W. A primer on leading improvement in health care. Presented at the Fifth European Forum on Quality Improvement in Health Care, Amsterdam, March 24, 2000. Used by permission.

Education and Training TopicsEducation and Training Topics
T i ti•Team organization•Overview of the ModelD i i ki i T•Decision‐making in Teams
•Planning initial PDSA cyclesCh t d h id•Change concepts and change ideas
•Measures for a projectPl i f PDSA l•Planning a sequence of PDSA cycles
Source: The Improvement Guide, 2nd ed. p. 348-349
This presentation is part of an on‐line series, brought to you through a collaboration between the Wisconsin Office of Rural Health and the Wisconsin Hospital Association.
Property of the Wisconsin Office of Rural Health.

Sample Team RosterSample Team Roster
•Clinical champion•Day‐to‐day leaderDay to day leader•Data analyst•Team members from the areaTeam members from the area
targeted by the aim•Improvement advisorImprovement advisor
This presentation is part of an on‐line series, brought to you through a collaboration between the Wisconsin Office of Rural Health and the Wisconsin Hospital Association.
Property of the Wisconsin Office of Rural Health.

Details of the M d l f I tModel for Improvement
This presentation is part of an on‐line series, brought to you through a collaboration between the Wisconsin Office of Rural Health and the Wisconsin Hospital Association.
Property of the Wisconsin Office of Rural Health.
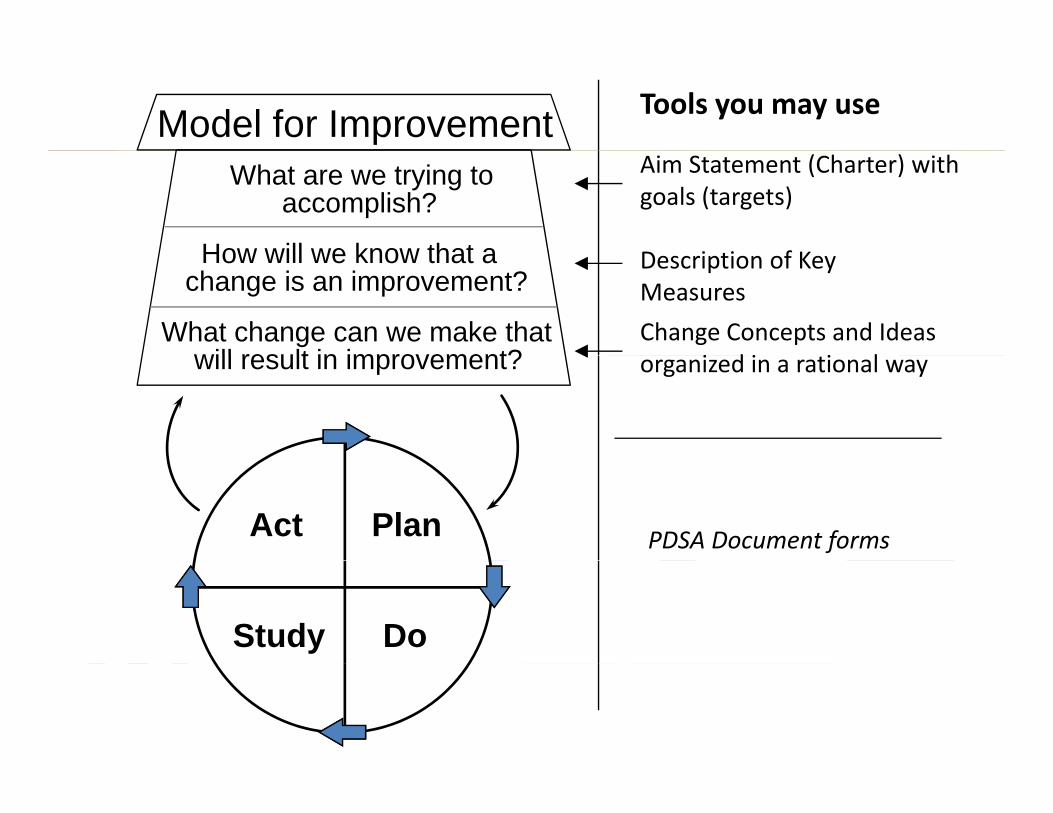
Model for Improvement Tools you may use
What are we trying toaccomplish?
How will we know that a
Aim Statement (Charter) with goals (targets)
D i ti f KHow will we know that achange is an improvement?
What change can we make thatwill result in improvement?
Description of Key Measures
Change Concepts and Ideas i d i i lwill result in improvement? organized in a rational way
Act Plan PDSA Document forms
Study Do

One page version f PDSA t l tof PDSA template

Try Before You BuyTry Before You Buy
Adapt ideas to your settingAdapt ideas to your setting by a series of test cycles
This presentation is part of an on‐line series, brought to you through a collaboration between the Wisconsin Office of Rural Health and the Wisconsin Hospital Association.
Property of the Wisconsin Office of Rural Health.

The PDSA Cycle for Learning and Improvement
Act Plan• ObjectiveQ ti d• What changes
are to be made?• Next cycle?
• Questions andpredictions (why)
• Plan to carry out the cycle (who, what, where, when)Pl f d t ll ti• Plan for data collection
Study• Complete theanalysis of the data
Do• Carry out the plan• Document problemsanalysis of the data
• Compare data topredictions• Summarize
what was
• Document problemsand unexpectedobservations
• Begin analysisof the data
learnedof the data

To Be Considered a PDSA CycleTo Be Considered a PDSA Cycle
•The test or observation was planned•The test or observation was planned(including a plan for collecting data and a prediction about results )prediction about results.)
•The plan was attempted (do the plan).
•Time was set aside to analyze the data and•Time was set aside to analyze the data and study the results.
A ti ti ll b d h t l d•Action was rationally based on what was learned.
This presentation is part of an on‐line series, brought to you through a collaboration between the Wisconsin Office of Rural Health and the Wisconsin Hospital Association.
Property of the Wisconsin Office of Rural Health.

Why Predict?Why Predict?
•Enhances learning•Forces use of test cycle measures•Forces use of test cycle measures•Adds fun to your improvement work
This presentation is part of an on‐line series, brought to you through a collaboration between the Wisconsin Office of Rural Health and the Wisconsin Hospital Association.
Property of the Wisconsin Office of Rural Health.

Use the PDSA Cycle for:Use the PDSA Cycle for:
• Testing or adapting a change idea• Implementing a change• Implementing a change• Spreading a change
This presentation is part of an on‐line series, brought to you through a collaboration between the Wisconsin Office of Rural Health and the Wisconsin Hospital Association.
Property of the Wisconsin Office of Rural Health.

Why Test?Why Test?
• Increase the belief in the change• Predict expected improvementp p• Learn how to adapt to the local environment• Evaluate costs and side effectsEvaluate costs and side effects•Minimize resistance upon implementation
This presentation is part of an on‐line series, brought to you through a collaboration between the Wisconsin Office of Rural Health and the Wisconsin Hospital Association.
Property of the Wisconsin Office of Rural Health.

Three Principles for Testing a ChangeThree Principles for Testing a Change
1. Test on a small scale2 C ll t d t ti2. Collect data over time3. Build knowledge sequentiallyg q y
This presentation is part of an on‐line series, brought to you through a collaboration between the Wisconsin Office of Rural Health and the Wisconsin Hospital Association.
Property of the Wisconsin Office of Rural Health.
Reduce RisksReduce Risks
F ibilit i b l l t• Feasibility review by local experts• Team as guinea pigs• Parallel trial: regular way and test way• Parallel trial: regular way and test way• Short test time• Rule of ONE to start (one cycle one patient• Rule of ONE to start (one cycle, one patient,
one appointment….)• Use volunteers• Simulate the change
This presentation is part of an on‐line series, brought to you through a collaboration between the Wisconsin Office of Rural Health and the Wisconsin Hospital Association.
Property of the Wisconsin Office of Rural Health.

Decrease the Time Frame for a PDSA Test Cycle
• Years• Years
• Quarters Your initial scope
• Months
• Weeks
can almost always be
• Weeks
• Daysreduced. Drop down “two
• Hours
• Minutes
levels” to plan a Test Cycle!
• Minutes
Collect Data Over TimeCollect Data Over Time
Th ‘Pl ’ t i l d l t ll t d t f hThe ‘Plan’ step includes plan to collect data for each PDSA Cycle.
• Useful data beat perfect data‐Pencil and paper system is OK!Q li i d b i i‐ Qualitative data now beats quantitative data later
•Record what went wrong during the data collection•Record what went wrong during the data collection•Sampling can reduce data burden
This presentation is part of an on‐line series, brought to you through a collaboration between the Wisconsin Office of Rural Health and the Wisconsin Hospital Association.
Property of the Wisconsin Office of Rural Health.

When tests fail to deliver predicted results…
C l b t h t l• Celebrate a chance to learn• Recognize different reasons for failed tests
1 Change was not executed well1. Change was not executed well2. Support processes inadequate3 Hypothesis/hunch wrong3. Hypothesis/hunch wrong
You need to collect data during the DoYou need to collect data during the Dophase of the Cycle to help identify which reason applies in your situation.reason applies in your situation.
This presentation is part of an on‐line series, brought to you through a collaboration between the Wisconsin Office of Rural Health and the Wisconsin Hospital Association.
Property of the Wisconsin Office of Rural Health.
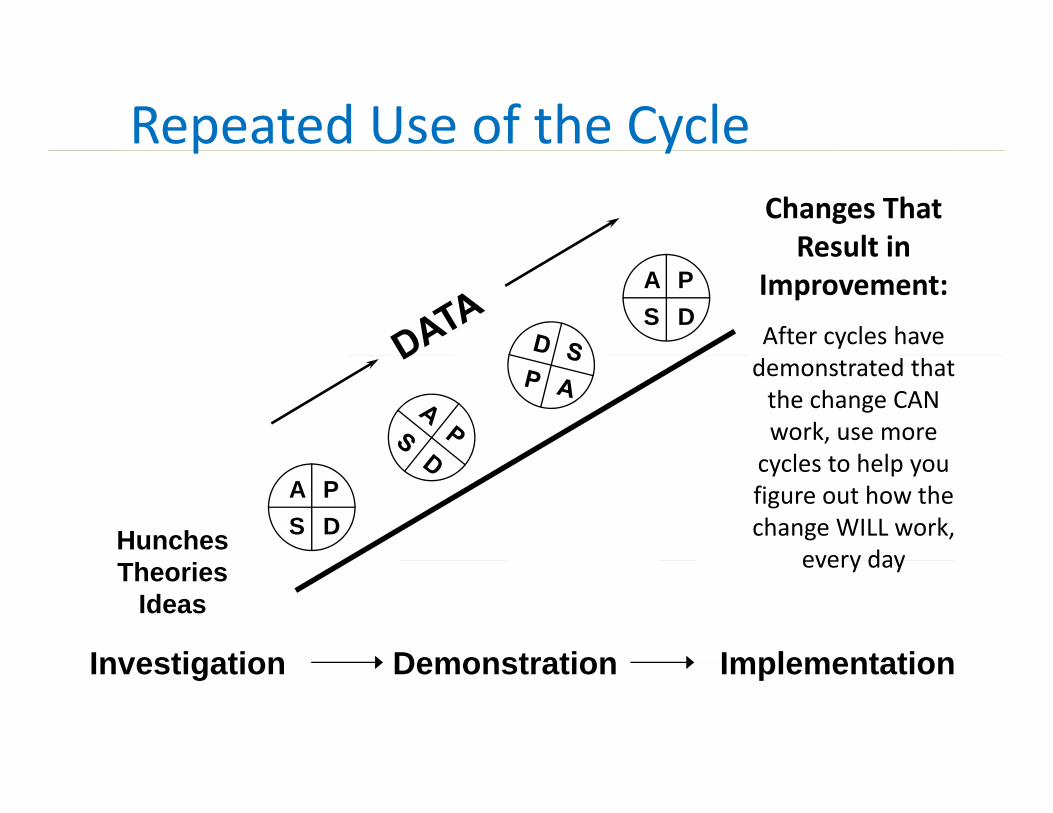
Repeated Use of the Cyclep yChanges That Result inResult in
Improvement:
After cycles have
A PS D
demonstrated that the change CAN work, use more l t h l
Hunches
cycles to help you figure out how the change WILL work,
every day
A PS D
Theories Ideas
every day
Investigation Demonstration ImplementationInvestigation Demonstration Implementation

Change Concept: Use evidence‐based guidelines in patient visits by incorporating a standard DM flow sheet
Improved care
A PCycle 1E: Implement andmonitor flow sheet use
S DCycle 1D: Use flow sheet with allof Dr B’s DM patients for a month
Use of flow sheet will catch
A PS D
Cycle 1C: Apply flow sheet to all of Dr B’s DM patients for one week
sheet will catch needed tests
Cycle 1A:Try recommended flow sheet with one of Dr Burton’s
Cycle 1B: Use edited flow sheet with all Dr. B’s DM patients on Monday.
Cycle 1A:Try recommended flow sheet with one of Dr. Burton’s patients on Thursday

Overall Aim: Improve Primary Care (IHS example)
Community Resources
Self‐Manage‐mentSupport
Delivery SystemDesign
Clinical InformationSystems
LeadershipDecision Support
SupportStrategies for Dimensions of a Primary Care Intervention

How the Model for Improvement
l t thcomplements other methodologiesmethodologies
This presentation is part of an on‐line series, brought to you through a collaboration between the Wisconsin Office of Rural Health and the Wisconsin Hospital Association.
Property of the Wisconsin Office of Rural Health.

Model for Improvement and LeanModel for Improvement and Lean
•Micro:•Micro: ‐ Lean concepts are Change Ideas (answer to Question Three)(answer to Question Three)
‐ Flow improvement projects in hospitals and clinics use Model forhospitals and clinics use Model for Improvement framework
•Macro: Use Model for Improvement pby senior managers to deploy Lean
This presentation is part of an on‐line series, brought to you through a collaboration between the Wisconsin Office of Rural Health and the Wisconsin Hospital Association.
Property of the Wisconsin Office of Rural Health.
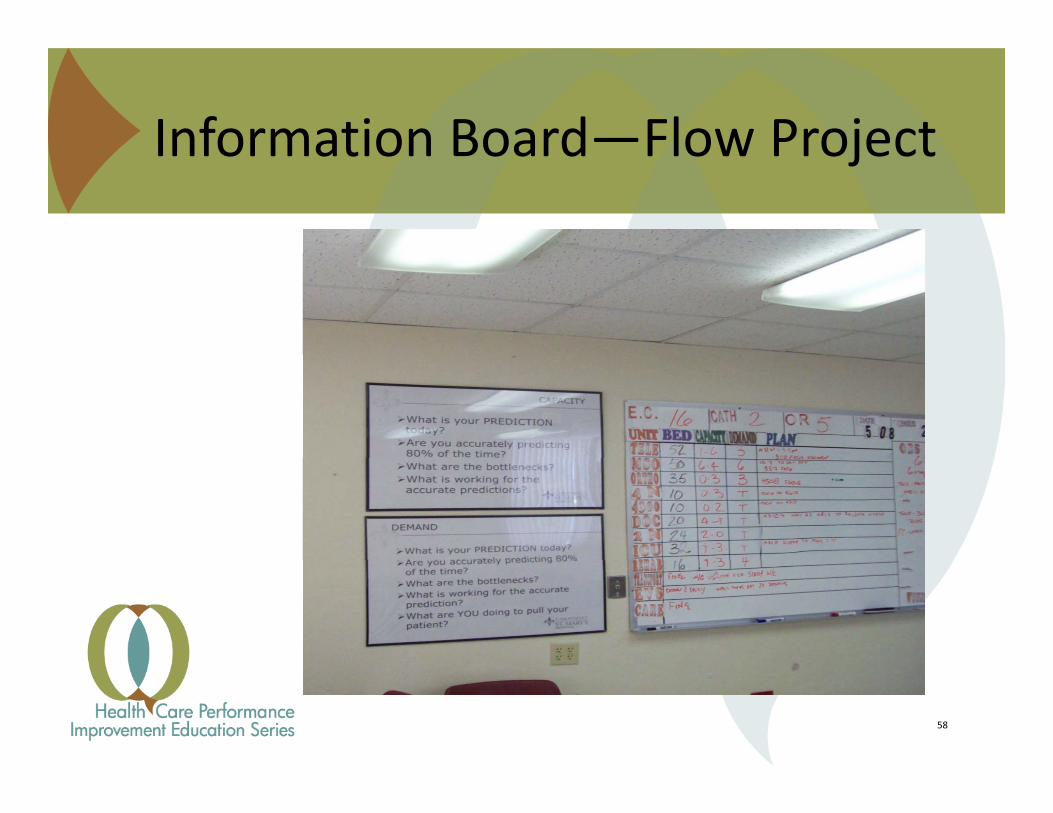
Information Board—Flow ProjectInformation Board Flow Project
58
Model for Improvement and Six SigmaModel for Improvement and Six Sigma
•Micro: I and C steps should use testing approachapproach
•Macro: Use Model for ImprovementMacro: Use Model for Improvement by senior managers to deploy Six SigmaSix Sigma
This presentation is part of an on‐line series, brought to you through a collaboration between the Wisconsin Office of Rural Health and the Wisconsin Hospital Association.
Property of the Wisconsin Office of Rural Health.
Key ReferencesKey References
G Langley et al (2009) The Improvement Guide 2ndG. Langley et al. (2009), The Improvement Guide, 2ndedition, Jossey‐Bass, San Francisco.
The IHI’s Open School courses:The IHI s Open School courses:Q101: Fundamentals of ImprovementQ102: The Model for Improvement: Your EngineQ102: The Model for Improvement: Your Engine
for ChangeQ103: Measuring for ImprovementHow to register: follow the directions on the next slide
This presentation is part of an on‐line series, brought to you through a collaboration between the Wisconsin Office of Rural Health and the Wisconsin Hospital Association.
Property of the Wisconsin Office of Rural Health.

1. Register at www.ihi.org
2 Cli k T k
1
2. Click on Take an online course
3. Click on the link to take you totake you to courses.ihi.org
4. Click on the Register button to
2
Register button to access the Open School
3
4
Additional ReferencesAdditional References
Don M. Berwick (1996), “A Primer on LeadingDon M. Berwick (1996), A Primer on Leading the Improvement of Systems,” BMJ, 312: pp 619‐622.
l d ( )T. W. Nolan and L. P. Provost (1990), “Understanding Variation”, Quality Progress, Vol. 13, No. 5.Vol. 3, No. 5.
“Accelerating the Pace of Improvement ‐ An Interview with Thomas Nolan,” Journal of Q lit I t V l 23 N 4 ThQuality Improvement, Volume 23, No. 4, The Joint Commission, April, 1997.
This presentation is part of an on‐line series, brought to you through a collaboration between the Wisconsin Office of Rural Health and the Wisconsin Hospital Association.
Property of the Wisconsin Office of Rural Health.

For More InformationFor More Information
Kevin Little PhDKevin Little, PhDInforming Ecological Design LLC, Madison, WIP: 866‐871‐7904P: 866 871 7904 E: [email protected]
Wi i Offi f R l H lth Wi i H it l A i tiWisconsin Office of Rural HealthKathryn MillerRural Hospitals & Clinics Program ManagerP: 800‐385‐0005E kmiller9@wisc edu
Wisconsin Hospital AssociationDana RichardsonVice President, Quality InitiativesP: 608‐274‐1820E drichardson@wha orgE: [email protected] E: [email protected]
This presentation is part of an on‐line series, brought to you through a collaboration between the Wisconsin Office of Rural Health and the Wisconsin Hospital Association.
Property of the Wisconsin Office of Rural Health.


















