A Just Culture: Accountability for Patient Safety Culture Original.pdf · A Just Culture:...
15
A Just Culture: Accountability for Patient Safety Mary Barkhymer MSN, MHA, RN, CNOR, CNO Team Lead - UPMC St. Margaret February 14, 2012
Transcript of A Just Culture: Accountability for Patient Safety Culture Original.pdf · A Just Culture:...

A Just Culture:
Accountability for Patient Safety
Mary Barkhymer MSN, MHA, RN, CNOR, CNO
Team Lead - UPMC St. Margaret
February 14, 2012

A Just Culture: Accountability for Patient Safety Today’s Presenters: Mary C. Barkhymer, MSN, MHA, RN, CNOR
Vice President, Patient Care Services
& Chief Nursing Officer
Peer Review Team Leads: Daniele Crisi-Couchenour, MHR
Human Resource Manager, Human Resources
Wendy Kastelic, MSN, RN
Advanced Practice Nurse, Nursing Education
Mary Jo Klebine, BSN, RN, CMSRN
Clinician, 5A Medical/Surgical Unit
Aimee K. Wilson, MSN, RN, ACM, CMSRN
Manager, Care Management
Karen L. Zanin, RN, CNOR
IS Specialist, Surgical Services
2

Program Objectives
• Describe the safety concept of A Just Culture.
• Introduce UPMC’s A Just Culture Algorithm as a tool
for evaluating patient-safety events.
• Highlight the use of A Just Culture principles in the frontline
staff peer-review process.
3

• UPMC fosters a ―nonpunitive response to error‖:
• Range of ―agree‖ responses: 28%-43%
• Number of hospitals surveyed: 12
– Perception is that same error is treated differently at different hospitals and/or on different units.
– We react because of the patient outcome.
– Negative perception among staff can have a ―chilling effect‖ on their reporting of errors and ―near misses.‖
– Lack of reported information decreases the organization’s ability to proactively address patient-safety issues and improve the existing work infrastructure.
UPMC Culture of Patient Safety
4
5
Blame Free or Punitive?
BLAME-FREE
CULTURE PUNITIVE
CULTURE
BLAME-FREE
CULTURE
PUNITIVE
CULTURE
A JUST CULTURE
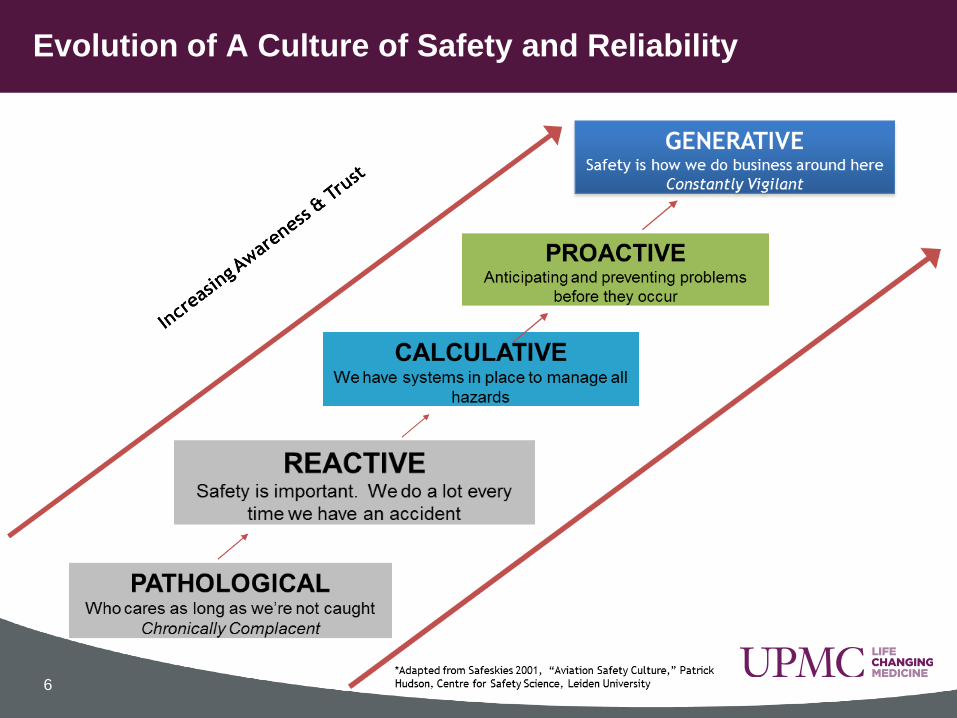
Evolution of A Culture of Safety and Reliability
6

• We all want to work in a place where patients and staff are safe and
treated with dignity and respect.
• Nobody comes to work wanting to do the wrong thing.
• We know that we have the opportunity to do better every day.
• We know that everyone has everyday workarounds that create the
potential for risk.
THEREFORE . . .
• We are going to have rules to play by where staff are accountable to try
hard and play by those rules.
• If someone plays by the rules and makes an error, they are safe.
• They are safe to tell us about the error.
• We will listen, console, and address system failures.
• We will share our learning to prevent future errors.
Our Story of “Just Culture”
7
• Supports a culture where frontline personnel feel comfortable disclosing errors—including their own—while maintaining professional accountability.
• Recognizes that individual practitioners should not be held accountable for system failings over which they have no control.
• Does not tolerate reckless behavior, conscious disregard of clear risks to patients, or gross misconduct (e.g., falsifying a record, performing professional duties while intoxicated).
• Realizes that competent professionals make errors and acknowledges development of unhealthy norms (shortcuts, ―routine rule violations‖).
• Focuses on fair, consistent, and predictable organizational responses to errors.
Definition of “Just Culture” From Agency for Healthcare Research and Quality (AHRQ)
8

Just Culture: A Piece of the Patient Safety Puzzle
Employee
AHRQ patient
safety survey
Structured
language:
• SBAR
• “I need
clarity”
Just Culture:
Accountability
for Patient
Safety
• Human error
• At-risk
behavior
• Careless
(reckless)
behavior
PILLARS OF FOCUS Leadership
Employee
rounding
Patient rounding
Patient/Family
Condition Help
Speak up
campaign
Environment
Safe work
environment
Regulatory
impact on
patient safety
LEARNING ORGANIZATION
DIGNITY & RESPECT
EXCELLENT CLINICAL OUTCOMES 9

What is Our Response to Serious Medical Error?
10
Trouble...
Trouble, trouble, trouble,
trouble
Trouble been doggin' my soul
since the day I was born
Worry...
Worry, worry, worry, worry
Worry just will not seem to
leave my mind alone….
Lyrics by Ray Lamontagne

Just Culture Algorithm
11

Behaviors Identified:
• Not an Error 2%
• Human Error 16%
• Risk 42%
• Careless 40%
Processes Addressed:
• Verbal Orders
• Handoff
Communication/Voicecare
• High Alert/Emergency
Medications
• Alert Fatigue
• Allergies
• Specimen Labeling
Peer Review Study: • 50 Peer Reviews Completed
Roles Peer Reviewed:
• RNs
• PCTs
• Pharmacy Techs
• Pharmacists
• Respiratory Therapists
• Laboratory Tech
Types of Reviews:
• Medication Errors 56%
• Mislabeled Specimens 38%
• Handoff Errors 6%
Sample Caregiver Peer Review: Magee-Womens Hospital of UPMC
12
Peer Review Process: UPMC St. Margaret Process:
• Peer review referral may be made by Patient Safety Officer,
Department Manager or Staff Member
• Peer reviews not for malicious behavior, suspected staff impairment
or Code of Conduct
• Staff and patient information are blinded
• Peer review meeting scheduled with Peer Review Team
• Behaviors are identified by review of standard algorithm questions
• Process and education recommendations reviewed
• Manager instructed to consult HR if repeated careless behavior
13

• It’s about raising your hand.
• It’s about doing the right thing.
• It’s about making the right choices.
• It’s about treating everyone fairly.
• It’s about creating a learning environment.
• It’s about prevention.
• It’s about doing something about it.
14
In Summary: What is A Just Culture All About?

California Hospital Patient Safety Organization. (2008). Just
culture. California Hospital Patient Safety Organization.
Retrieved October 18, 2011, from
http://www.chpso.org/just/index.php
Edmondson, A. (1999). Psychological safety and learning behavior
in work teams. Administrative Science Quarterly, 44(2), 350-383.
General Electric Patient Safety Organization. (2011). The second
victim. Retrieved October 18, 2011, from http://www-waa-
akam.thomson-webcast.net/us/dispatching/GE20110928
Hudson, P. (2001). Evolution of a culture of safety and reliability.
Adapted from Safeskies 2001. Centre for Safety Science, Leiden
University.
Sources
15