A giant staghorn calculus in the biliary tract · A giant staghorn calculus in the biliary tract...
2
Revista de Gastroenterología de México. 2014;79(3):200---201 REVISTA DE GASTROENTEROLOGIA DE MEXICO ´ ´ www.elsevier.es/rgmx CLINICAL IMAGE IN GASTROENTEROLOGY A giant staghorn calculus in the biliary tract Litiasis coraliforme gigante en la vía biliar G. Martinez-Mier ∗ , O. Avila-Mercado, S. Irisson-Mora Departamento de Cirugía General, Unidad Médica de Alta Especialidad 189 Adolfo Ruiz Cortines, Instituto Mexicano del Seguro Social, Veracruz, México Received 7 February 2014; accepted 19 February 2014 The clinical importance of biliary tract calculi is in their association with cholangitis and acute pancreatitis. Endoscopic retrograde cholangiopancreatography (ERCP) is regarded as the safest and most successful therapeutic method for extracting stones from the common bile duct. Nevertheless, large or impacted calculi that take up the entire bile duct are a therapeutic challenge. A bile duct calculus is defined as large when it is bigger than 10-15 mm. There are very few reports describing a single giant calcu- lus (> 5 cm) in the common bile duct. We describe herein a 58-year-old woman that presented with severe acute pan- creatitis. Tomography findings included a stone impacted in the bile duct, dilation of the bile ducts, and cholelithiasis (fig. 1). ERCP revealed a giant stone in the common bile duct that occupied the space up to the confluence of the hepatic ducts (fig. 2). The patient underwent a conventional cholescystectomy with bile duct exploration and a Roux- Please cite this article as: Martinez-Mier G, Avila-Mercado O, Irisson-Mora S. Litiasis coraliforme gigante en la vía biliar. Revista de Gastroenterología de México. 2014;79:200---201. ∗ Corresponding author: Corporativo San Gabriel, Alacio Pérez, 928, consultorios 313 y 314, entre Carmen Serdán y 20 de Noviem- bre. Fraccionamiento Zaragoza. Veracruz, CP 91910. Teléfono: +52(229)9327782; fax: +52(229)9232990. E-mail addresses: [email protected], [email protected] (G. Martinez-Mier). Figure 1 Abdominal CAT scan showing bile duct dilation and a calculus in its interior. en-Y hepaticojejunal anastomosis, extracting a 7 x 2 cm staghorn calculus (figs. 3 and 4). The patient was released from the hospital with no complications. She is asymp- tomatic 6 months after surgery and her liver function tests are normal. 2255-534X/© 2014 Asociación Mexicana de Gastroenterología. Published by Masson Doyma México S.A. All rights reserved.
Transcript of A giant staghorn calculus in the biliary tract · A giant staghorn calculus in the biliary tract...
-
R
C
A
L
G
DS
R
TtErmNecTl5ct(dhc
Id
9b+
g
2
evista de Gastroenterología de México. 2014;79(3):200---201
REVISTA DEGASTROENTEROLOGIA
DE MEXICO´
´
www.elsevier.es/rgmx
LINICAL IMAGE IN GASTROENTEROLOGY
giant staghorn calculus in the biliary tract�
itiasis coraliforme gigante en la vía biliar
. Martinez-Mier ∗, O. Avila-Mercado, S. Irisson-Mora
epartamento de Cirugía General, Unidad Médica de Alta Especialidad 189 Adolfo Ruiz Cortines, Instituto Mexicano del Seguroocial, Veracruz, México
eceived 7 February 2014; accepted 19 February 2014
he clinical importance of biliary tract calculi is inheir association with cholangitis and acute pancreatitis.ndoscopic retrograde cholangiopancreatography (ERCP) isegarded as the safest and most successful therapeuticethod for extracting stones from the common bile duct.evertheless, large or impacted calculi that take up thentire bile duct are a therapeutic challenge. A bile ductalculus is defined as large when it is bigger than 10-15 mm.here are very few reports describing a single giant calcu-
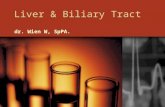
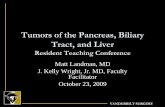
us (> 5 cm) in the common bile duct. We describe herein a8-year-old woman that presented with severe acute pan-reatitis. Tomography findings included a stone impacted inhe bile duct, dilation of the bile ducts, and cholelithiasisfig. 1). ERCP revealed a giant stone in the common bile
uct that occupied the space up to the confluence of theepatic ducts (fig. 2). The patient underwent a conventionalholescystectomy with bile duct exploration and a Roux-
� Please cite this article as: Martinez-Mier G, Avila-Mercado O,risson-Mora S. Litiasis coraliforme gigante en la vía biliar. Revistae Gastroenterología de México. 2014;79:200---201.∗ Corresponding author: Corporativo San Gabriel, Alacio Pérez,28, consultorios 313 y 314, entre Carmen Serdán y 20 de Noviem-re. Fraccionamiento Zaragoza. Veracruz, CP 91910. Teléfono:52(229)9327782; fax: +52(229)9232990.
E-mail addresses: [email protected],[email protected] (G. Martinez-Mier).
Figure 1 Abdominal CAT scan showing bile duct dilation anda
esfta
255-534X/© 2014 Asociación Mexicana de Gastroenterología. Published
calculus in its interior.
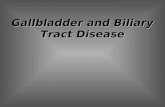
n-Y hepaticojejunal anastomosis, extracting a 7 x 2 cmtaghorn calculus (figs. 3 and 4). The patient was released
rom the hospital with no complications. She is asymp-omatic 6 months after surgery and her liver function testsre normal.
by Masson Doyma México S.A. All rights reserved.
dx.doi.org/10.1016/j.rgmxen.2014.10.006http://www.elsevier.es/rgmxhttp://crossmark.crossref.org/dialog/?doi=10.1016/j.rgmxen.2014.10.006&domain=pdfmailto:[email protected]:[email protected]
-
A giant staghorn calculus in the biliary tract 201
Figure 2 ERCP showing a 7 cm impacted calculus.
Figure 3 Staghorn calculus extracted from the bile duct.
Figure 4 The dilated hepatic duct sectioned (2 cm) and useda
F
N
C
T
s a reference point for the hepaticojejunal anastomosis.
inancial disclosure
o financial support was received in relation to this article.
onflict of interest
he authors declare that there is no conflict of interest.
A giant staghorn calculus in the biliary tractFinancial disclosureConflict of interest