A Collaborative Approach to Development and Implementation of Inpatient Code Stroke Protocol
19
A Collaborative Approach to Development and Implementation of Code Stroke Protocol February-18-16 1 Beena Parappilly St. Paul’s Hospital, Vancouver, BC, Canada Feb 26, 2016
-
Upload
bcpsqc -
Category
Healthcare
-
view
240 -
download
0
Transcript of A Collaborative Approach to Development and Implementation of Inpatient Code Stroke Protocol
A Collaborative Approach to Development and Implementation of Code Stroke Protocol
February-18-16 1
Beena Parappilly
St. Paul’s Hospital, Vancouver, BC, Canada
Feb 26, 2016

Disclosure
February-18-16 2
I have no potential conflict of interest

Background
February-18-16 3
There is a need to facilitate early identification and treatment of the in-hospital patients experiencing a new stroke in Canada.
Consistent with stroke best practices, hospital inpatients who have a new stroke should have timely access to assessment and appropriate care. (www.strokebestpractices.ca)2015

Background, continued…
February-18-16 4
Literature reviews indicated:
• A poorer outcome for patients who developed stroke in the hospital compared to the community (Saltman et
al., 2014)
• A need for a standardized approach for the in-hospital stroke patients
Critical incident reviews of inpatient strokes found:
• Communication breakdowns
• A need for a standardized approach

Objectives
February-18-16 5
To design and implement an evidence-based, standardized protocol to manage in-hospital new stroke to:
Reduce:
• time from assessment to CT scan
• time from diagnosis to intravenous tissue
plasminogen activator (IV tPA)
• mortality
• length of stay
Increase:
• IV tPA administration rate
• staff satisfaction
Methods
February-18-16 6
• Collaborate with an interdisciplinary team of physicians, leaders from various programs, and patient and family member, to develop the Inpatient Code Stroke Protocol.
• Computerize the code stroke order entry.
• Refine the Protocol with ongoing feedback.

Protocol / Algorithm
February-18-16 7

Protocol / Algorithm
February-18-16 8
Code Stroke Protocol for SPH – Cont.

February-18-16 9
Pre-printed Orders
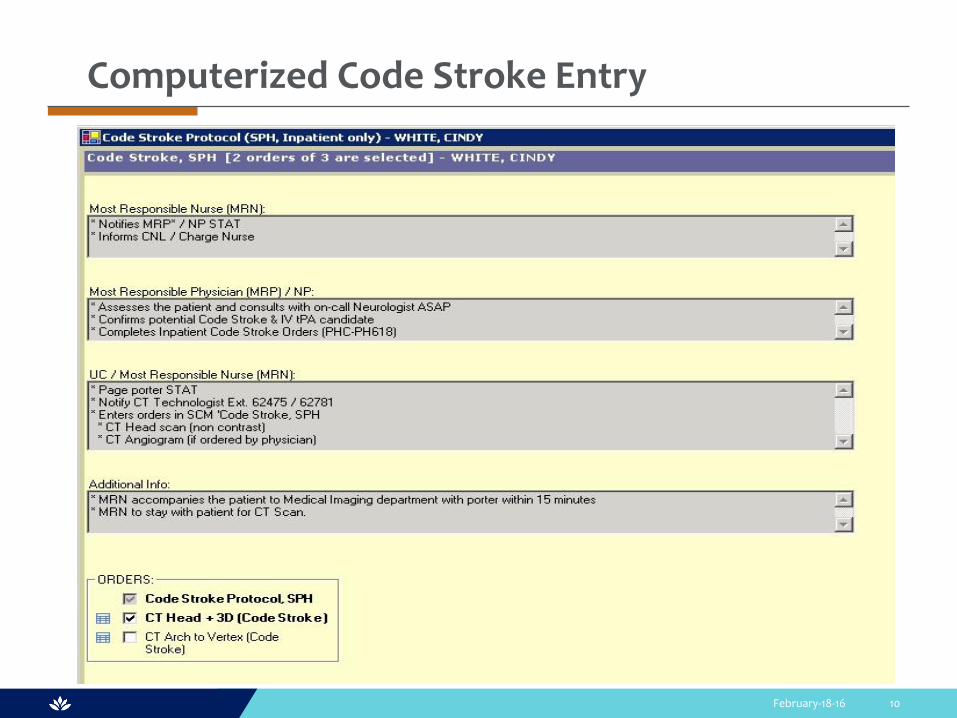
February-18-16 10
Computerized Code Stroke Entry
Implementation
February-18-16 11
•Communication to all program leaders
• Education to nurses, physicians and unit coordinators
•Auto notification of every code stroke to CNS and stroke educator
•Real time follow up and mentoring of nurse leaders, nurses, physicians and unit coordinators for each code stroke case

Evaluation
February-18-16 12
•Seek feedback from front line staff and leaders after each code stroke case
•Data extracted from every code stroke activations
•Stroke champion follows up on every code stroke to ensure protocol is followed appropriately
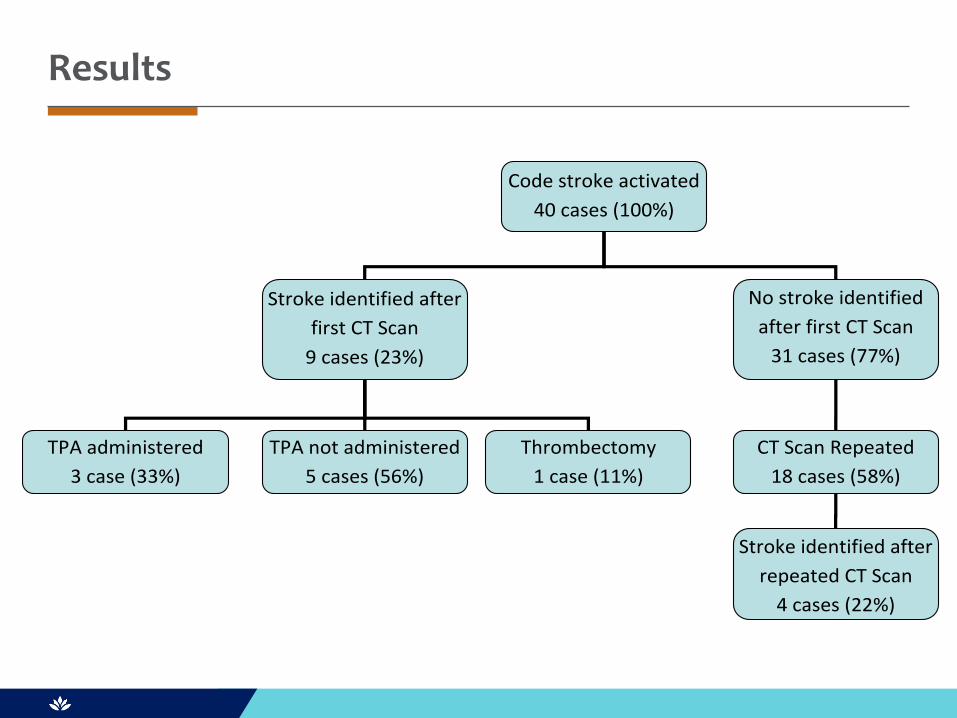
Results
Code stroke activated
40 cases (100%)
Stroke identified after
first CT Scan
9 cases (23%)
No stroke identified
after first CT Scan
31 cases (77%)
TPA administered
3 case (33%)
TPA not administered
5 cases (56%)
Thrombectomy
1 case (11%)
CT Scan Repeated
18 cases (58%)
Stroke identified after
repeated CT Scan
4 cases (22%)
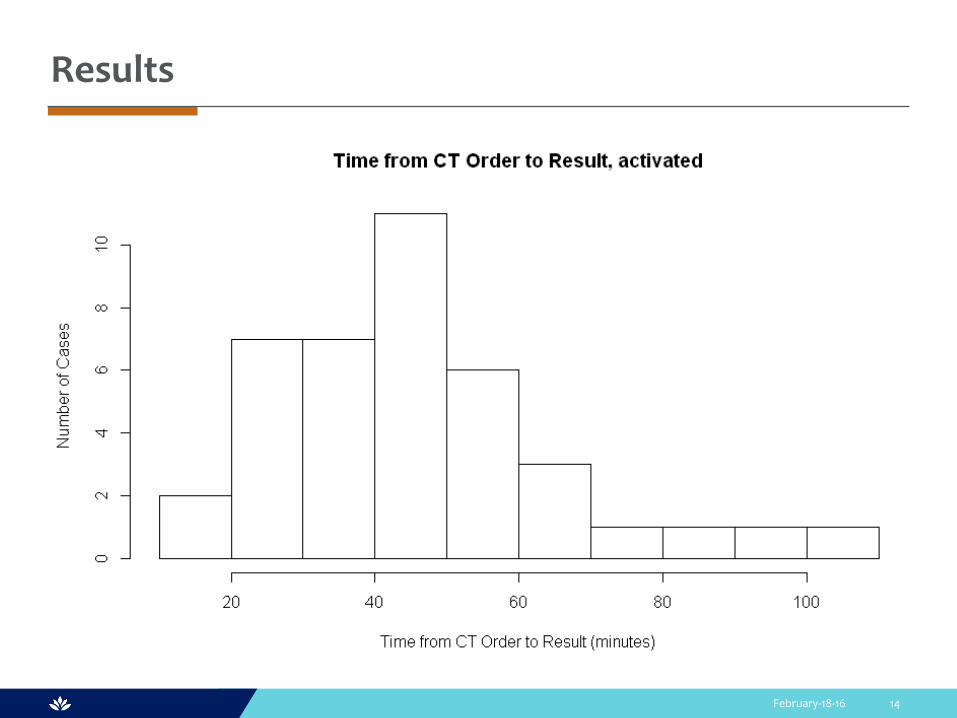
Results
February-18-16 14

Feedback
February-18-16 15
“the code stroke is simple, practical and facilitates rapid and coordinated assessment of strokes and potential strokes”
“Patient safety is enhanced… by making sure the right tests and treatment are done at the appropriate time”
“The step by step orders provide clear instruction”

Sustainability
February-18-16 16
• Part of Resident Orientation and Nursing orientation
• On-going in services on the units
• Computerized Protocol and order entry
• Real time follow up on all cases and ongoing mentoring by stroke champions

Key success factors
February-18-16 17
• An interdisciplinary and collaborative approach
•Ongoing education and communication
• Real time follow up
•Mentoring of staff and physicians by stroke champions
•Revisions based on the user’s feedback

References
February-18-16 18
www.strokebestpractices.ca
Saltman AP, Fang J, Silver FL, Kapral MK (2014). Code Stroke on the Ward-Care and Outcomes of Patients with In-Hospital Stroke. University of Toronto, Faculty of Medicine, Toronto, ON.
Vancouver Island Health Authority. Inpatient “Hot stroke” Guideline. BC, Canada.

Contact information
February-18-16 19
Beena Parappilly
St. Paul’s Hospital
Providence Health Care
Vancouver, BC
Email: [email protected]
Phone: 604 682 2344 Ext 66768