A Centralized Clinical Outcome Measurement of Eating Disorders in
47
Clinical Outcome Measurement of Eating Disorders 1 The Provincial Centre of Excellence for Child and Youth Mental Health at CHEO Le centre d’excellence provincial au CHEO en santé mentale des enfants et des ados Evaluation Implementation Grant EIG 1208 Final Report March 31 st , 2011 A Centralized Clinical Outcome Measurement of Eating Disorders in Youth across Ontario: A Multi-Site Partnership Written by: Dr. Katherine Henderson, PhD, C.Psych and Nicole Obeid, MA Co-Principal Investigators: Dr. Katherine Henderson and Dr. Annick Buchholz Co-Investigators: Dr. Wendy Spettigue, Dr. Mark Norris, Dr. Nick Barrowman, Dr. Margus Heinmaa, Dr. Leora Pinhas, Dr. Debra Katzman, Dr. Melissa Lieberman, Dr. Karin Jasper, Dr. Ahmed Boachie, Dr. Adele Lafrance
Transcript of A Centralized Clinical Outcome Measurement of Eating Disorders in

Clinical Outcome Measurement of Eating Disorders
1
The Provincial Centre of Excellence for Child and Youth Mental Health at CHEO
Le centre d’excellence provincial au CHEO en santé mentale des enfants et des ados
Evaluation Implementation Grant EIG 1208
Final Report March 31st, 2011
A Centralized Clinical Outcome
Measurement of Eating Disorders in Youth across Ontario:
A Multi-Site Partnership
Written by: Dr. Katherine Henderson, PhD, C.Psych and Nicole Obeid, MA
Co-Principal Investigators:
Dr. Katherine Henderson and Dr. Annick Buchholz
Co-Investigators: Dr. Wendy Spettigue, Dr. Mark Norris, Dr. Nick Barrowman, Dr. Margus Heinmaa, Dr. Leora Pinhas, Dr. Debra Katzman,
Dr. Melissa Lieberman, Dr. Karin Jasper, Dr. Ahmed Boachie, Dr. Adele Lafrance

Clinical Outcome Measurement of Eating Disorders
2
Table of Contents Page Contents
3 Executive Summary
6 Introduction
12 Results and Lessons Learned
23 Conclusion and Recommendations/Next Steps
24 Knowledge Exchange
27 References
28 Appendices

Clinical Outcome Measurement of Eating Disorders
3
Executive Summary
Eating disorders are chronic and life threatening illnesses. Despite the morbidity and
mortality of this condition, these disorders remain understudied and underserved, and there
is an absolute paucity of research examining outcomes in pediatric clinical populations.
Three pediatric eating disorder programs located in tertiary care hospitals in Ontario worked
collaboratively together to create a multisite research partnership that would allow for the
creation of knowledge about the children and youth served in Ontario and an evaluation of
the services provided to our children and youth.
In Ontario, three specialized pediatric eating disorder teams; the Children’s Hospital of
Eastern Ontario (CHEO), Southlake Regional Health Centre (SHRC), and the Hospital for
Sick Children (HSC), made a commitment to take action to address the lack of research
available for this vulnerable population. The vision for this multi-site partnership was
conceptualized by members from all sites and with the leadership of Dr. Henderson and
Buchholz from CHEO, the members were able to successfully implement the vision. The
three centres created an interdisciplinary, multi-institutional partnership with the goals of
greater research collaboration, shared resources, and shared data to attempt to close the
knowledge gap in research on outcomes and treatment in children and youth suffering from
eating disorders. This multi-institutional partnership received a Provincial Centre of
Excellence Program Implementation Grant in June of 2010 to formally develop a Centralized
Multisite Database Partnership (CMDP) and to develop capacity for research with the
creation of a multisite database.
Over the course of the granting period, the partnership met monthly via teleconference,
as well as in-person on three separate occasions. Through these meetings this team has
accomplished four main goals: 1) the establishment of a solid partnership across the three
sites with one representative from each site acting as a Steering Committee member, 2) the
creation and approval of all relevant authorship and ownership documents necessary to

Clinical Outcome Measurement of Eating Disorders
4
operate a multi-site partnership, 3) the establishment of a web-based database and data
definition dictionary which explicitly lists and defines all variables that are to be part of the
multi-site database, and 4) has contributed to knowledge translation at both a provincial and
national level.
A strong partnership is the cornerstone to the success of any longitudinal multisite
research program. Drs. Henderson and Buchholz, with Ms. Obeid as a research coordinator
worked within a collaborative participatory framework to establish a formal partnership that
was inclusive and sustainable. Interdisciplinary representatives from each site were invited
to join the research partnership. Interdisciplinary and inter-site relationships were fostered
and strengthened through bi-monthly teleconferences and 3 full day in-person meetings.
These meetings provided a forum for an exchange of knowledge and expertise and the
development and refinement of our common vision for the partnership. During these
meetings the detailed authorship agreement, methodology for the study, data dictionary, and
future knowledge dissemination and research plans were developed, discussed, and agreed
upon by all involved. Furthermore, the web-based database structure was successfully
designed and developed over the course of the grant. Unfortunately there was a significant
delay in moving the data base to the secure server at CHEO. This delay resulted in an
inability to enter and store data in the centralized web-based database, which prevented any
outcomes analyses of the data.
Through the funding for this grant, Dr. Henderson and Dr. Buchholz with their co-
investigators were successful in creating a formal multisite partnership for outcomes
research on pediatric eating disorders with clear terms of agreement on the use of the data
and authorship, developing a centralized web-based data-base, and in successfully
engaging in knowledge translation and exchange. The development of this multisite
partnership is extremely important. Through this partnership the CMDP will finally be able to
start to address the paucity of research examining outcomes in pediatric eating disorders.

Clinical Outcome Measurement of Eating Disorders
5
The knowledge generated over the upcoming years from this partnership and centralized
database will provide missing evidence to better guide the prevention and treatment of this
serious and chronic mental health illness affecting many children and youth in Ontario. This
knowledge will also be essential to our national and international partners who work hard to
provide excellent care and treatment to youth suffering from eating disorders.
The CMDP has learned from the challenges faced in implementing this grant and
continues to work to build upon the successes achieved. The delay in being able to
implement the web-based data base, was turned into an opportunity to apply for further
funding to pilot test the data and the feasibility of data collection once the data base has
been established. The team was successful in receiving funds from the Sick Kids Psychiatry
Endowment Fund ($25,000). The team further used the strength of the partnership to apply
for a CIHR grant to hold a national meeting (CIHR meetings and plannings grant, $9,999).
The partnership has set a goal of building on the results and success of the Centre of
Excellence Grant and the Hospital of Sick Children grant. To this end we are committed to
submitting a grant to CIHR in January in 2012 to provide funds for an extensive 3 year
evaluation of programs in Ontario and possibly across Canada.

Clinical Outcome Measurement of Eating Disorders
6
Introduction
Eating disorders are chronic and life threatening illnesses. Despite the morbidity and
mortality of this condition, these disorders remain understudied and underserved, and there
is an absolute paucity of research examining outcomes in pediatric clinical populations. The
shared vision of the current project was to create a forum in which to conduct a quasi-
experimental, multi-site, repeated measures design to examine recovery trajectories of
medical and psychological outcome variables across a number of organizations within
Ontario. Initially, four pediatric eating disorder programs located in tertiary care hospitals
worked collaboratively to address the shared goals of creating a centralized web-based
database to examine the clinical profiles of patients, 6-month recovery trajectories, as well
as predictors of clinical outcome.
Throughout the course of the granting period, numerous tasks related to the
formation of a solid partnership were established, as was the creation of a secure web-
based database that has the capacity to store, disseminate, and retrieve data from various
sources was created. Due to unexpected challenges and delays in the Children’s Hospital of
Eastern Ontario (CHEO) IS department, the timely establishment of an operational and
secure centralized database was not possible. A thorough explanation of the challenges and
delays encountered will be described later in this report. Without the secure operational
centralized database it has not been possible to complete any analyses. It is anticipated that
with ongoing support of the current partnership and an ongoing commitment to finalize the
secure centralized database, that the data that each site has gathered, will be entered into
the centralized database as soon as possible, and that analysis of this data will provide
valuable information on clinical outcomes from services that are provided by eating disorder
programs within Ontario. The data base and partnership will also provide a measurement
framework upon which to build a larger, potentially national, partnership among programs
offering treatment to children and youth struggling with eating disorders.

Clinical Outcome Measurement of Eating Disorders
7
This final report will focus the four main objectives that were accomplished during the
granting period and will discuss how the principal investigators addressed the challenges
presented by the delays in the technology. While discussing each of the objectives in turn,
this report will highlight the accomplishments and lessons learned. Although it is recognized
that a multisite evaluation of clinical populations of youth with eating disorders was not
successfully completed, the solid partnership that has grown and evolved from this ongoing
collaboration has been paramount in securing a platform in which multisite outcomes
research is now possible. The four main achievements of this project were: 1) the creation of
a formal a provincial inter-disciplinary multi-site partnership, 2) researching and creating
authorship and ownership guidelines to direct the partnership 3) consensus on common
outcome indicators including a data definition dictionary that would be placed in a
centralized database to be developed and maintained at CHEO, and 4) contribution to
knowledge translation.
Background
Physical and emotional development is profoundly affected in children and youth
suffering from eating disorders. Physical complications of the illness include bradycardia,
hypotension, hypothermia, cardiac arrhythmias, heart failure, amenorrhea, osteopenia,
neurological impairments, hormonal imbalances, growth deceleration, and impaired bone
density and fertility (Katzman, 1999). Psychological sequelae of an eating disorder include
depression, suicidality, mood lability, social withdrawal, cognitive impairment, insomnia,
irritability, agitation, and marked deterioration in family relationships (Neiderman, 2000).
Sullivan (Sullivan, 1995) reported mortality rates in individuals with eating disorders that
exceeded the expected incidence of death from all causes in women 15 to 24 years of age
by twelve-fold. In short, eating disorders in youth are associated with potentially devastating
psychosocial and medical outcomes, impaired quality of life, premature mortality, and
exorbitant costs to the health care system (Nielson & Bara-Carrill, 2003). Many youth

Clinical Outcome Measurement of Eating Disorders
8
diagnosed with a severe eating disorder are no longer capable of functioning at school or
with their peers and may require intensive interventions such as hospitalization.
Current treatment for an eating disorder typically involves a multidisciplinary
approach including medical and nutritional rehabilitation as well as psychological
interventions (Wilson & Shafran, 2005). More recently, rehabilitation centers for eating
disorders have adopted a treatment approach which has come out of the Maudsley Hospital
in England, and which has been expanded, modified, and systematically detailed by Lock
and LeGrange (Lock & le Grange, 2005). In this approach, family therapy is provided to
empower and support parents in the refeeding process of their child, as well as to address
underlying psychosocial issues. In parallel to the emergence of the Maudsley family-based
therapeutic approach, relatively new pediatric day treatment programs for the treatment of
eating disorders in youth have emerged in many provinces. Both family-based outpatient
therapies and day treatment programs have been developed, in part, to address historically
lengthy hospital stays and repeat admissions for youth struggling with an eating disorder.
However, to date, there has been no long-term outcome measurement examining the
effectiveness of these approaches, or predications of best outcome based on types of eating
disorders. There is also a lack of research on clinical pathway management, even though it
is acknowledged that there is a wide range of eating disorders requiring different levels of
intervention.
The paucity of research on treatment outcomes in eating disorders is partly related to
the prohibitive expense of creating a randomized control trial to compare one intensive and
comprehensive treatment approach to another. Single site studies do not have the power to
complete the research and the generalizability of the results would be limited. The current
study was acknowledged to be limited by its lack of randomization; however, it was
established to overcome the issues concerning power and generalizability that is afforded by
use of a multi-site study. Data from the participating sites is thought to provide results to help

Clinical Outcome Measurement of Eating Disorders
9
researchers understand the profile of patients presenting to tertiary care hospitals, 6 month
recovery trajectories, and predictors of outcome.
Existing Partnerships
At the beginning of this grant informal partnerships were being developed between
the Children’s Hospital of Eastern Ontario’s (CHEO) eating disorder program, and the
pediatric eating disorders programs located at McMaster Children’s Hospital (MCH),
Southlake Regional Health Centre (SRHC), and the Hospital for Sick Children (HSC), to
explore how to become a multisite team to allow for the examination of clinical profiles and
recovery trajectories of youth suffering from eating disorders. When this grant was
developed, all four pediatric centers provided outpatient services in the form of
comprehensive assessments, medical management, psychopharmacology, nutritional
counseling, family therapy, individual therapy, and group therapies. All four tertiary care
centers also had specialized interdisciplinary teams to care for patients who are medically
unstable and must be admitted to hospital. In addition, CHEO, SRHC and HSC eating
disorder programs offer intensive day treatment programs for youth suffering from severe
eating disorders. Although the particular range and nature of services available for youth
differ within each program, the programs treat the same population (youth younger than
age18), and the family/team based treatment model and philosophy of each program are
similar. The four partners had already demonstrated a capacity for single site program
evaluation activities and each had established databases with common measures across
sites. The following provides a brief description of the single site program activities that each
site was engaged in at the time of the grant application:
1) CHEO EDP had been actively collecting and evaluating clinical outcomes from their Day
Treatment Program since the program began in January 2000; clinical outcome findings had
been presented at provincial, national, and international conferences. Similarly, all
assessment, outpatient, and tracking data had also been collected and managed in a

Clinical Outcome Measurement of Eating Disorders
10
database since the opening of the program, providing further evidence of this site’s abilities
to participate in program evaluation and outcomes management. In January 2007, CHEO
received funding for a provincial inpatient eating disorder program and implemented a
program evaluation component to this service in April 2008; since that time, a steering
committee for ED program evaluation activities met on a weekly basis to discuss
implementation successes, challenges and changes. Similarly, the Mental Health Patient
Service Unit (MHPSU) at CHEO is strongly committed to program evaluation and had
developed a steering committee for outcomes measurement for which a representative from
each of the service units (including eating disorders) met on a monthly basis for the
purposes of knowledge exchange and the development of a common database. The
MHPSU had prioritized program evaluation activities across the full continuum of its
services. The Eating Disorders Team had taken a leadership role in the capacity building of
its program evaluation activities since January 2000.
2) SRHC EDP had been formally measuring outcomes since September 2008 for all
patients presenting to the Program for an assessment. Other evaluation activities also
ongoing included the evaluation of new adjunct therapies (emotion-focused therapy; multi-
family therapy and reflecting team family therapy) and an assessment of needs identified by
family physicians and psychologists in the community.
3) HSC EDP had recognized the importance of maintaining consistent and ongoing program
evaluation activities and had been evaluating outcome from all components of their
program. The EDP employed psychologists and a psychometrist for ongoing program
evaluation activities, and had the program evaluation infrastructure necessary for this study.
4) MCH Pediatric EDP highly valued clinically relevant research such as program
evaluation. Staff members of the EDP all actively participated in program evaluation work
through assisting with data collection, providing suggestions and feedback regarding

Clinical Outcome Measurement of Eating Disorders
11
specific evaluation questions. MCH has had considerable success to date with implementing
program evaluation practices.
The initial four participating organizations also created strong ties with the Ontario
Community Outreach Program for Eating Disorders. It was anticipated that through the
partnership and the resulting multi-site centralized database, a framework for the
amalgamation of data with others sites in Ontario would be possible. The director of the
Ontario Community Outreach program for Eating Disorders, Dr. Gail McVey, was fully
supportive of this initiative, and was invited to provide consultation to the partnership
regarding the broader needs of the province. It was anticipated that this liaison would lead to
excellent knowledge exchange opportunities within the province.
Recognizing that a centralized multi-site database requires expertise in technology,
privacy legislation, and ethics, the principal investigators had been in consultation with
experts on behalf of the partnership group. Mr. Tyson Roffey the Director of Information
Services and the Privacy Officer at CHEO and Dr. Khaled El-Emam, principal investigator
for the Electronic Health Information Laboratory at the University of Ottawa and CHEO
Research Institute had been consulted to ensure that the database could be created with
the appropriate security dimensions, with enough sophistication to handle at least four
separate sites, to be able to be enhanced over the years, and that all privacy legislation
could be considered. Finally, Dr. Carole Gentile, chair of the Research Ethics Board at
CHEO was a key consultation partner providing expert ethical guidance.
The proposed evaluation activities (see Appendix A and B for the Program Logic
Model and the Evaluation Plan) resulting from the development of this multi-site partnership
will have direct impact on child and youth mental health, with a focus on eating disorder
programs for children and youth at hospitals in Ontario. Eating disorders continue to be
chronic and life threatening illnesses for the children and youth of Ontario, with an ongoing
paucity of research examining clinical outcomes. This study was designed to build on the

Clinical Outcome Measurement of Eating Disorders
12
existing capacity for strong outcomes research in youth with eating disorders, by creating a
partnership in outcomes management between four provincial organizations who provide
intensive interdisciplinary treatment for eating disorders.
Results and Lessons Learned
In Ontario, four specialized pediatric eating disorder teams; the Children’s Hospital of
Eastern Ontario (CHEO), Southlake Regional Health Centre (SHRC), McMaster Children’s
Hospital (MCH) and the Hospital for Sick Children (HSC), made a commitment to take action
to address the lack of research available for this vulnerable population. The vision of this
multi-site partnership was conceptualized by members from all sites and with the leadership
of Dr. Katherine Henderson and Dr. Annick Buchholz at CHEO this vision has been realized.
At this time, only Dr. Katherine Henderson remains as the principal lead on this project, as
Dr. Buchholz has taken a leave of absence from her role on the Eating Disorder Team.
These initial four centres created an interdisciplinary, multi-institutional partnership with the
goals of greater research collaboration, shared resources, and shared data to attempt to
close the knowledge gap in research on outcomes and treatment in children and youth
suffering from eating disorders. This multi-institutional partnership received this Provincial
Centre of Excellence Program Implementation Grant in June of 2010 to formally develop a
Centralized Multisite Database Partnership (CMDP) and develop capacity for research with
the creation of a multisite database.
Over the course of the granting period, the partnership met monthly via
teleconference, as well as met in-person on four separate occasions. Through these
meetings this team has accomplished four major goals: 1) the establishment of a solid
partnership across the three sites with one representative from each site acting as a
Steering Committee member, 2) the creation and approval of all relevant authorship and
ownership documents necessary to operate a multi-site partnership, 3) the establishment of

Clinical Outcome Measurement of Eating Disorders
13
a web-based database and data definition dictionary which explicitly lists and defines all
variables that are to be part of the multi-site database, and 4) has contributed to knowledge
translation both provincially and nationally.
1) Evolution of the Partnership
A strong partnership is the cornerstone to the success of any longitudinal multisite
research program. Thus, a primary objective of this project was to formalize a multisite
partnership between the four interested pediatric eating disorder programs in Ontario. Prior
to being granted funding from the Centre of Excellence, colleagues from the initial four sites
discussed informally over the phone and met once face-to-face (during an annual provincial
network meeting) in order to establish interest in forming this partnership. With confirmed
interest, the four sites worked together to draft the proposal for the current grant. It was
agreed that CHEO would lead this research initiative with Dr. Henderson and Dr. Buchholz
as principal investigators.
Drs. Henderson and Buchholz, with Ms. Obeid as a research co-ordinator worked
within a collaborative participatory framework to establish a formal partnership that was
inclusive and sustainable. Interdisciplinary representatives from each site were invited to
join the research partnership. Interdisciplinary and inter-site relationships were fostered and
strengthened through bi-monthly teleconferences and 3 full-day in-person meetings. These
meetings provided a forum for an exchange of knowledge and expertise and the
development and refinement of our common vision for the partnership. During these
meetings the detailed authorship agreement, methodology for the study, data dictionary, and
future knowledge dissemination and research plans were developed, discussed, and agreed
upon (this will be reviewed in more detail in later sections).
Through their participation in the regular meetings and the development of the
structure of the partnership and the research program, the MCH representatives had to
make the very difficult decision that due to a lack of protected time and financial resources,

Clinical Outcome Measurement of Eating Disorders
14
they would not be able to collect the minimum data required to be part of the partnership.
They continue to be committed to joining the partnership should they or the partnership be
successful in securing more funds to provide the resources required.
The CMDP partnership currently consists of 3 pediatric eating disorder programs in
Ontario with a strong interdisciplinary representation. The CHEO program has 4 co-
investigators involved: 2 psychologists, 1 psychiatrist, 1 adolescent health physician, and
the support of 1 research coordinator and 1 software consultant. HSC has 4 co-investigators
including 2 psychologists, 1 psychiatrist, 1 adolescent health physician, and the support of a
psychometrist. SRHC has 2 co-investigators 1 Clinical Mental Health Specialist and 1
psychiatrist, and the support of a PhD student who helps with data entry and database
maintenance. A further partner to this collaboration is Dr. Adele Lafrance who originally held
the lead at SRHC, but in September 2010 she accepted a position at Laurentian University.
She has remained a co-investigator on the project, and has become an academic partner
(see Appendix C for a list of study partners).
In addition to the direct partners involved in the partnership, the CHEO site
investigators have also fostered important relationships with staff members with a breadth of
expertise within CHEO who have an ongoing central role in the maintenance and
sustainability of this partnership. The MHPSU Operations Director and the Chief Information
Officer at CHEO have committed to the development and on-going maintenance of the
provincial database for eating disorders beyond the timelines of this initiative. Although
funding from the current grant was sought to support software development and consultation
fees, CHEO has committed to supporting this proposal with in-kind funds for the
development and sustainability of this database (to be housed at CHEO). For example,
CHEO currently pays the $2000 fee for annual maintenance of the website server. Given
that the multi-site data collection process developed for this study has been designed to be
sustained beyond the terms of the current grant (i.e., resource infrastructures and web-

Clinical Outcome Measurement of Eating Disorders
15
based database), the partnering sites have also agreed to collect the common data set at
12-months post-assessment, speaking to the long-term collaboration created by this grant.
Furthermore, the Software Consultant, provided by Dr. Khaled El-Emam’s E Health
Information lab, has agreed to continue to provide in-kind support for the maintenance of the
web-based database.
The work and time dedicated to ensuring a strong, formal partnership between the
three sites will provide the foundation for a larger provincial and national partnership
between pediatric eating disorder programs. Following the presentation provided by Dr.
Henderson and Dr. Buchholz at the November 2010 annual provincial network meeting for
eating disorders in Ontario, the London Health Sciences Centre has contacted the CMDP to
express an interest in joining the partnership.
2) Creation of the authorship and ownership guidelines
Over the course of the grant the multi-site team focused on developing a solid
partnership, and an important component of formalizing the partnership was the creation of
authorship and ownership agreements. These agreements are complex and have been
designed to address the time frame of the current grant from the Centre of Excellence and
the long term vision for the database, which includes the current research proposal and the
possibility of the partnerships and database thriving for many years. Each site has
demonstrated incredible commitment to ensuring the success of this research project, and
with this level of commitment also comes a need to ensure that ownership and credit are
attributed fairly to all involved. Through the early stages of this partnership, it came to the
attention of the collaborators that the need for formalized agreements was necessary. The
process of establishing these agreements was lengthy and complicated. CMDP members
invested time in researching and consulting with other multi-site projects and teams, to
determine all of the important components to address when developing an authorship
agreement for a longitudinal multisite research program. Each site dedicated some time to

Clinical Outcome Measurement of Eating Disorders
16
this initiative, and together several relevant documents were shared with the partnership.
Through research and many lengthy discussions and debates, the CMDP was able to
establish the guidelines through consensus and collaboration. The formalization of the
authorship agreement represents a significant accomplishment of this partnership, and
forms the foundation for the ongoing success of the partnership.
The following documents were drafted and approved by the CMDP partnership (see
Appendix D):
1. Authorship, Acknowledgements, and Manuscripts Agreement
2. General Authorship and Manuscripts
3. Single Site versus Central Shared Dataset
4. Requesting Secondary Use of Data
5. Ancillary Studies
6. Designating a New Partner on the CMDP of PEDP of Ontario
7. Maintaining the Integrity of the Database
8. Intellectual Property and Data Sharing Agreement
Furthermore, the CMDP partners collaboratively prioritized the top 9 research papers that
would address the overall goals of the research program. It was agreed that each site would
take the lead on 3 separate projects that would follow from either the assessment data or
the follow-up data. The assignment of site and title of the 9 projects are available in
Appendix E.
3) Centralized Database
The third central objective that was achieved over the course of the grant was the
development of the web-based centralized database. This objective was achieved through
three steps: (a) achieving consensus on the central indicators to be evaluated, (b)
development of a detailed data definition dictionary, and (c) the software development of a
web-based database.

Clinical Outcome Measurement of Eating Disorders
17
Common Indicators
During the in-person meetings, the CMDP partners had extensive discussions and
engaged in knowledge exchange about which indicators were most appropriate for this
research initiative (based on research and clinical expertise) and how to best measure these
indicators. The common outcome indicators that were selected to be part of this centralized
database were agreed upon by all participating sites. Specifically, medical indicators include
body mass index and percent of healthy weight, including items to define how these are
calculated for each child and youth. Eating disorder behaviour and attitudes indicators are
measured using an internationally recognized and standardized self-report measure of
eating disorders and a relatively new clinician-report measure validated by CHEO
investigators (EDS3). Psychological indicators have been chosen to reflect the two most
common comorbidities in patients with eating disorders and include internationally
recognized and standardized self-report measures of depression (CDI) and anxiety (MASC)
in youth. Parents are also asked to complete a validated measure of self-efficacy in their
ability to support their child through recovery. Other predictor variables agreed upon include
demographic information (age, gender, region) and clinical variables (e.g., diagnosis,
chronicity of illness). Data collection is well underway at all three remaining sites, and is
currently being collected at the time of the initial assessment (a patient’s first presentation to
the treatment program, Time 1) and identical medical, eating disorder and psychological
outcome data is also currently being collected at six months post-assessment (Time 2).
Further, this study is also measuring whether the programs are providing family- and youth-
friendly services, by assessing parent and youth satisfaction with the treatment they receive
(Time 2 only). Finally, the feasibility of the data collection process is to be evaluated by all
those involved in the data collection process using a feasibility questionnaire (via web-based
survey-monkey). This feasibility survey will be distributed once the web-based data base is
operational.

Clinical Outcome Measurement of Eating Disorders
18
All programs have the resource infrastructure available to collect the data through
medical/dietetic appointments and/or follow-up appointments with therapists. Trained
therapists and psychometrists are administering and scoring the psychological measures,
and physicians/nurses/dieticians are collecting the medical data. The psychological
measures take approximately 20 minutes for patients to complete. The medical and
psychological data are also being used clinically to track the patient’s progress. Research
assistants (an existing resource at each site) at the respective sites have been involved in
scoring and entering the data into each site’s database, while waiting for the instalment of
the shared web-based statistical database. Raw data remains secured in psychology and
medical files at the respective sites.
Data Definition Dictionary
Once the common indicators were decided upon, a very detailed data definition
dictionary was created. This consisted of detailing the name of the variable as it appeared in
SPSS, the data type, the descriptive variable label, the value number, and the value labels.
This dictionary was created in Excel and describes all 835 variables contained in the
database. An excerpt of the data definition dictionary is provided in Appendix F. Generating
the data definition dictionary required collaboration across sites about each sites existing
data base and the best definition for the new multi-site data base that would still be feasible
for each site.
Web-based database
The centralized database and web application has been developed by the IT
professionals from the E-health Information Lab at CHEO’s Research Institute led by Dr.
Khaled El Emam at CHEO’s Research Institute and supported by Tyson Roffey, Chief
Information and Privacy Officer at CHEO. It has been designed so that each partner is able
to log into the web application through a web browser and then upload and enter all of their

Clinical Outcome Measurement of Eating Disorders
19
data into the centralized database. Data may be viewed and retrieved from the database,
via the web application, by those with the correct privileges. Data will be anonymized at the
user end as necessary and sent to the centralized database via a secure channel (i.e. using
128-bit SSL encryption). The database itself will be stored on a server within CHEO. The
server will have the appropriate security, monitoring, and backup systems in place. This set
up will ensure that only the study partners will be able to read and modify the database. The
IT professionals from the E-health Information lab have committed to continuing to provide
support during the pilot testing of the database to ensure that it is stable, user friendly and
secure. Given that the web-based database is maintained at CHEO, credentials and access
will be provided by CHEO researchers to the appropriate people (i.e., study investigators
and trained research assistants), and the CMDP partnership has agreed that CHEO will act
as a gatekeeper to this database. Data within the database will be identified by coded IDs
that correspond to participants at the respective sites. There will be no names or identifying
information stored within the centralized database. Privacy specialists from the E-Health
Information Lab at CHEO have been consulted to ensure that the data stored within the
database meets all privacy standards.
While the data base structure was successfully designed and developed over the
course of the grant, there was a significant delay in moving the data base to the secure
server at CHEO. We have been waiting for 12 months for the implementation of a secure
server that is to house the web-based database. This delay was due to the launch of an
electronic documentation (eclin Doc) system at CHEO which took priority of CHEO IS
resources. IS was unable to provide any personnel due to the time commitment required for
the launch of eClin Doc, resulting in a fairly significant delay in the installation of a secure
server devoted to this project. At this point in the time, the secure server has been
configured, passwords and access have been provided to our software developer, so it
appears reasonable to expect that the web-based database will be secured on the CHEO

Clinical Outcome Measurement of Eating Disorders
20
server by the end of April 2011. Once the secure server is established, data from each
respective site will be uploaded into the multi-site database in order for analyses to start.
Outcomes Evaluation
Although unique challenges arose throughout the course of the granting period that
delayed the acquisition of a secure multi-site database to be populated with data that would
allow for evaluative analyses, the vision and objectives for the partnership are still clear and
pressing. The paucity of research on pediatric treatment outcomes in eating disorders has
been noted by researchers over the last decade, and in order to optimize the power and
generalizability of outcomes data, the partnership agreed to work collaboratively to address
three shared objectives.
Data collection commenced at all sites in January of 2010, and ongoing collection is
still underway. Once the web-based database is secured on the CHEO server (expected
date: April 2011), data from each respective site will be uploaded into the multi-site
database in order for analyses to start.
The specific goals of this study were:
(1) To examine the clinical profiles of youth presenting for an eating disorder
assessment in tertiary care hospitals in Ontario;
(2) To examine recovery trajectories of medical and psychological outcome markers of
youth struggling with an eating disorder for six months following their initial
assessment;
(3) To evaluate predictors of outcome based on clinical profiles and treatment services
received over six months.
It is anticipated, that with the ongoing multisite partnership and the dedication of the
remaining sites that are currently committed to the partnership, that the above objectives will
be met in the upcoming months. At the current time, the establishment of the web-based
database on a secure server should be completed by the end of April 2011, and data from

Clinical Outcome Measurement of Eating Disorders
21
the respective sites will be imported into the database within the month of May 2011.
Analyses on the data, once available, are set to commence over the summer of 2011.
Feasibility of data collection
In addition to the communal indicators that are collected at each site, the partnership
is also committed to learning about the feasibility of this data collection. Specifically, the
CMDP is interested in knowing the estimation of the rates for patient/parent participation,
enrolment, and adherence/compliance at each of the three sites. In order to collect this
information, a mixed methods survey created through a participatory approach with all co-
investigators was created. Quantitative data will be collected on the number of participants
invited, the number who choose to participate, the number who decline, and the number lost
to attrition at the six-month follow-up time. Qualitative data regarding types of barriers and
facilitators that were felt by each member of the partnership will also be collected, as well as
a rank-ordering of which were felt to be the top 3 barriers or facilitators. Each site will be
asked to complete open-ended questions regarding suggestions to overcome any barriers
and how they felt the facilitators were helpful. This data will be analyzed to determine any
common or site specific themes. All feasibility surveys will be administered by the research
coordinator once the web-based database goes live. In order to evaluate the user-friendly
interface, security, and sustainability of the centralized database over time, as well as
assessing the feasibility of uploading the data in a timely manner, a survey will be
administered to all end-users and investigators at each site. Further, the survey will be
designed to collect the following information about the centralized web-based data base: a)
number of times unable to access the server; b) median time to upload data to the server;
and c) number of mistakes encountered at each site in the uploads. Any ongoing issues
detected from these feasibility surveys will be followed-up by our IT consultant.

Clinical Outcome Measurement of Eating Disorders
22
4) Contribution to KT
One of the final objectives of this project was to promote and contribute to knowledge
translation in this field. Thus, the interdisciplinary, multi-institutional provincial partnership of
the CMDP proposed, secured funding for, and executed a national meeting for specialized
pediatric eating disorder teams in tertiary care hospitals across Canada, with the goals of
connecting, collaborating, and ultimately creating a national outcomes research agenda in
pediatric eating disorders. The meeting, which was CIHR funded, directly addressed child
and youth mental health, with a focus on outcomes research on the treatment of eating
disorders in children and youth. Building on lessons learned and the strength of the
provincial partnership, the CMDP proposed a day that focused on knowledge sharing and
exchange, catalyzing new research initiatives, and creating a national consensus on the
research needs, gaps and opportunities in outcomes management of eating disorders in
children and youth. One of the aims of the meeting was that it would act as a catalyst for the
development of a national interdisciplinary, multi-institutional partnership that will work
toward a national research agenda on outcomes research in the treatment of pediatric
eating disorders. Using the lessons learned from the already formed provincial multi-site
partnership, it was felt that the knowledge gained through a multi-institute national research
initiative would create crucial evidence for the provincial, national, and international
communities regarding the effectiveness of the current standards of care for youth with
eating disorders, and enhance eating disorder treatment for children and youth in Canada
and the international community. Paramount to this initiative was the leadership that the
CMDP Steering Committee provided for the full-day meeting, and the vision that the
provincial partnership held to solidify and create firm stepping stones and guidelines for a
provincial partnership that could then be applied to a larger national platform.

Clinical Outcome Measurement of Eating Disorders
23
Conclusion and Recommendations/Next Steps
In conclusion, through the funding for this grant, Dr. Henderson and Dr. Buchholz
with their co-investigators were successful in creating a formal multisite partnership for
outcomes research on pediatric eating disorders with clear terms of agreement on the use of
the data and authorship, in developing a centralized web-based database, and in
successfully engaging in knowledge translation and exchange.
The development of this multisite partnership is extremely important. Through this
partnership the CMDP will finally be able to start to address the paucity of research
examining outcomes in pediatric eating disorders. The knowledge generated over the
upcoming years from this partnership and centralized database will provide missing
evidence to better guide the prevention and treatment of this serious and chronic mental
health illness affecting many children and youth in Ontario. This knowledge will also be
essential to our national and international partners who work hard to provide excellent care
and treatment to youth suffering from eating disorders.
As noted earlier, the success of the CMDP has allowed the partnership to be
successful in receiving a CIHR grant to hold a national meeting on outcomes research in
pediatric eating disorders. This meeting will help generate much needed interdisciplinary
and inter-site collaborations to enhance outcomes research in pediatric eating disorders
across Canada. The next steps from this meeting include regular working groups and a bi-
annual national meeting to continue to maintain and improve on a national research agenda
for outcomes research in pediatric eating disorders.
The CMDP has learned from the challenges faced in implementing this grant. The
delay in being able to implement the web-based database, was turned into an opportunity to
apply for further funding to pilot test the data and the feasibility of data collection once the
database was established. The team was successful in receiving funds from the Sick Kids
Psychiatry Endowment Fund ($25,000, January 2011- January 2012). The partnership also

Clinical Outcome Measurement of Eating Disorders
24
worked to strengthen the relationship and formal agreement with the CHEO IS department
to ensure the long term sustainability of the web-based database and to prevent future
challenges (as much as possible). The partnership has set the goal of building on the
results and successes of the Centre of Excellence Grant and the Hospital of Sick Children
grant. To this end we are committed to submitting a grant to CIHR in January of 2012 to
provide funds for an extensive 3 year evaluation of programs in Ontario and possibly across
Canada.
Knowledge Exchange
Knowledge exchange and dissemination from this project has focused on ensuring
the success of this centralized multi-site database, with the long term vision that its
successes will be the seed for the development of a province wide centralized multi-site
database for all pediatric eating disorder programs, greatly enhancing knowledge exchange
across the province. Knowledge gained through the process of creating a collaborative
network and a web-based centralized multi-site database has been shared between the
partnering agencies, within their hospitals, with the full Ontario network for eating disorder
providers, and at regional, provincial, and national meetings. It is anticipated that knowledge
and skills gained as a result of the data within this program evaluation project will be used to
better understand the presentation and treatment trajectories of youth with eating disorders
at specialized interdisciplinary eating disorder programs in the province. Having the large
multi-site sample size will allow important questions to be asked and answered regarding
the prognosis of different patients and how to best match treatment to youth at assessment
and throughout their treatment journey, to ensure the best success for each individual and
youth with an eating disorder. The expectation is that the innovative knowledge gained
through these research activities will be shared in the form of presentations, discussions,
face-to-face meetings, publications, etc, and may also lead to the creation of a community of
practice focused on pediatric eating disorders.

Clinical Outcome Measurement of Eating Disorders
25
Also, the partnering agencies and the director of the outreach program, Dr. McVey,
have been engaged in regular knowledge exchange over the course of the granting period,
and she has been kept abreast of the progress and outcomes of this partnership.
Knowledge exchange has occurred through regular teleconference calls and face-to-face
meetings. Further, the multisite partners have and will continue to share knowledge and
anecdotal experiences with one another regarding the process of creating and starting a
multi-site database, by means of regular conference calls which have allowed for the
exchange of new and creative ideas and ensure that each site learns from the experience of
the other sites. These opportunities for exchange have ensured the success of the
centralized database and the longevity of the partnership.
Knowledge and skills gained as a result of this project has been disseminated
through formal and informal presentations and written documents:
• Findings regarding the ongoing multi-site program evaluation project have been
shared with members of the eating disorder teams at each organization, during
weekly/monthly research meetings and bi-annual/annual team retreats.
• Acquired knowledge and skills related to program evaluation generally, the creation
of a multi-site partnership, and of the programs specifically, have been presented to
key hospital staff across the country during a national meeting of all eating disorder
programs. It has also been presented to all pediatric and adult eating disorder
programs at the Annual Provincial Outreach Conference in November 2010.
• It is also anticipated that information will be disseminated through The Provincial
Centre for Excellence’s required Final Outcomes Report and Plain Language
Summary of project outcomes.

Clinical Outcome Measurement of Eating Disorders
26
• As the results of the outcomes evaluation become available, further knowledge
exchange will occur in the form of manuscripts in applied scholarly journals and
presentations at provincial, national, and international conferences.
• Teams at London Health Sciences Centre, the Central West Eating Disorder
Program and an eating disorder team in Newfoundland have consulted the CMDP
principal investigators on outcomes research for children and youth with eating
disorders.

Clinical Outcome Measurement of Eating Disorders
27
References
Katzman, D. K. (1999). Preventing Eating Disorders: A handbook of interventions and
special challenges. Philidelphia, PA: Taylor & Francis Group.
Lock, J. & le Grange, D. (2005). Family-based treatment of eating disorders. Int.J
Eat.Disord., 37 Suppl, S64-S67.
Neiderman, M. (2000). Anorexia Nervosa and Related Eating Disorders in Childhood and
Adolescence. (2nd edition ed.) East Sussex, UK: Psychology Press.
Nielson, S. & Bara-Carrill, N. (2003). Family, Burden of Care and Social Consequences. In
J.Treasure, U. Schmidt, & E. van Furth (Eds.), Handbook of Eating Disorders (2nd
ed., West Sussex: John Wiley & Sons.
Sullivan, P. F. (1995). Mortality in Anorexia Nervosa. American Journal of Psychiatry, 152,
1073-1076.
Wilson, G. T. & Shafran, R. (2005). Eating Disorder guidelines from NICE. The Lancet, 365,
79-81.

Clinical Outcome Measurement of Eating Disorders
28
APPENDIX A
___________________________________
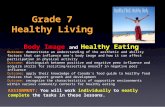
Program Logic Model

Clinical Outcome Measurement of Eating Disorders
29
Evaluation Outcomes ► Medical
stabilization
► Reduction in eating disorder symptoms
► Improved psychological functioning: reduced depression
► Improved psychological functioning: reduced anxiety
► Increase in parent’s self-efficacy in ability to support child/youth
Process Outcomes ► Demographics/
patient profile
► Satisfaction
► Feasibility of outcomes measurement
I N P U T S O U T C O M E S
► Resources specific to program evaluation activities within overall fiscal resources:
○ Children’s Hospital of Eastern Ontario
(CHEO): 0.2 FTE psychologist/psychiatrist; 0.2 FTE psychometrist
○ Hospital for Sick Children (HSK): 0.2 FTE psychologist/psychiatrist; 0.4 FTE psychometrist
○ Southlake Regional Health Centre (SRHC): 0.4 FTE psychologist
► Human Resources:
○ Specialized interdisciplinary team at each of the four sites. Core clinical disciplines include:
- Psychologists - Nurses - Psychiatrists - Dietitians - Pediatricians/Adolescent Health Specialists - CYCs
Program Goals: Improved medical and mental health through specialized pediatric family-based services across the continuum of care for eating disorders
Program Logic Model An evaluation of pediatric eating disorder programs in Ontario:
A multisite approach
• Regular
appointments for nutritional & medical monitoring
• Individual &
group therapy provided in intensive (inpatient & day hospital) and outpatient settings
• Parents/ caregivers & family therapy & education groups
O U T P U T S
Activities Target Group
• Children/
Youth under 18 years of age
• Children/
Youth under 18 years of age
• Parents/
caregivers & families
CO
MPO
NEN
TS
▪ Men
tal h
ealth
ser
vice
s
▪ M
edic
al in
terv
entio
n an
d
n
utrit
iona
l man
agem
ent

Clinical Outcome Measurement of Eating Disorders
30
APPENDIX B
____________________________________
Evaluation Plan

Clinical Outcome Measurement of Eating Disorders
31
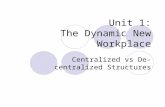
Evaluation Plan
● Outcome indicators: Focus on medical stabilization, reduction in eating disorder symptoms, mental health improvement, and increase in parental feelings of self-efficacy toward recovery from eating disorders.
Outcomes Indicator(s) Source of data
Method to collect data
Who collects data
When collects data
E V A L U A T I O N O U T C O M E S
Medical stabilization
Movement toward targeted ideal BMI
Scale & stadiometer
Weight and Height
Team nurse, physician or
team clinician
Assessment and 6 months post-
assessment
Reduction in eating disorder symptoms
Decrease in scores on a self-report &
clinician measures of eating disorder
symptoms
EDI 3 (child/youth)
EDS3 (clinician)
Validated self-report
questionnaire EDS3:
validated clinician rating
scale
Team clinician, psychometrist;
or research assistant
Assessment and 6 months post-
assessment
Improved psychological functioning: Reduced Depression
Decrease in scores on a validated self-report measure of child & adolescent
depression
CDI (child/youth)
Validated self-report
questionnaire
Team clinician, psychometrist,
or research assistant
Assessment and 6 months post-
assessment
Improved psychological functioning: Reduced Anxiety
Decrease in scores on a validated self-report measure of child & adolescent
anxiety
MASC (child/youth)
Validated self-report
questionnaire
Team clinician, psychometrist,
or research assistant
Assessment and 6 months post-
assessment
Increase in parent’s self-efficacy in ability to support child/youth
Increase in scores on a measure of self-efficacy for
parents/caregivers
PVA (parent/
caregiver)
Validated self-report
questionnaire
Team clinician, psychometrist,
or research assistant
Assessment and 6-months post-
assessment
P R O C E S S O U T C O M E S
Demographics/patient profile
Demographic & clinical patient
profiles
Interview checklist
Clinician completes intake form
Team clinician Assessment
Satisfaction Scores on
Satisfaction Measure: CSQ
CSQ (youth & parents)
Validated self-report
questionnaire
Team clinician, psychometrist,
or research assistant
6 months post-assessment

Clinical Outcome Measurement of Eating Disorders
32
APPENDIX C ____________________________________
Centralized Multi-site Database Partners

Clinical Outcome Measurement of Eating Disorders
33
Partners
Site Partner Title
Children’s Hospital of Eastern Ontario
Dr. Katherine Henderson Psychologist Dr. Annick Buchholz Psychologist Dr. Mark Norris Pediatrician Dr. Wendy Spettigue Psychiatrist Dr. Nick Barrowman Senior Statistician
Southlake Regional Health Centre
Dr. Karin Jasper Clinical Mental Health Specialist
Dr. Ahmed Boachie Psychiatrist
Hospital for Sick Children
Dr. Leora Pinhas Psychiatrist Dr. Margus Heinmaa Psychologist Dr. Melissa Lieberman Psychologist Dr. Debra Katzman Adolescent Health Physician
Laurentian University Dr. Adele Lafrance Psychologist

Clinical Outcome Measurement of Eating Disorders
34
APPENDIX D
____________________________________
CMDP Partnership Agreements

Clinical Outcome Measurement of Eating Disorders
35
CENTRALIZED MULTI-SITE PARTNERSHIP OF PEDIATRIC EATING DISORDERS PROGRAM’S IN ONTARIO
- AUTHORSHIP GUIDELINES, ROLE DEFINITIONS AND PROCEDURES MANUAL -
Background/Reference Material Regarding Authorship
The Committee on Public Ethics Report on Authorship Disputes recommends that authorship issues should be discussed right at the start. “Start gathering views of all team members and if possible discuss authorship at a face-to-face meeting. Even before a study is finished, you should have some idea of the publications that might come out of it, such as a conference abstract, the full paper, then some supplementary papers, and who is likely to be most involved in these. Continue to discuss ideas about authorship as the project evolves, and especially if new people get involved. Keep a written record of your decisions.” Decide authorship before you start each article. Many authorship difficulties arise because of misplaced expectations and poor communication. So it is important that, before you start to write up your project, you confirm in writing who will be doing what and by when. Ideally you should do this face to face, though this may not always be possible. Keep everyone informed of any changes with a written note. (http://publicationethics.org/files/u2/2003pdf12.pdf) According to the International Committee of Medical Journal Editors (ICMJE) (www.icmje.org), “…an author is generally considered to be someone who has made substantive intellectual contributions to a published study”. Authorship applies to all publications, abstracts and presentations and any other published or presented material (will be referred to as papers throughout this agreement). As detailed in the ICMJE’s Uniform Requirements for Manuscripts Submitted to Biomedical Journals: Writing and Editing for Biomedical Publication (2008):
• Authorship credit should be based on 1. substantial contributions to conception and design, acquisition of data, or
analysis and interpretation of data; 2. drafting the article or revising it critically for important intellectual content;
and 3. final approval of the version to be published.
Authors should meet conditions 1, 2, and 3. • When a large, multi-center group has conducted the work, the group should
identify the individuals who accept direct responsibility for the manuscript. • Acquisition of funding, collection of data, or general supervision of the research
group alone does not constitute authorship. • All persons designated as authors should qualify for authorship, and all those
who qualify should be listed. • Each author should have participated sufficiently in the work to take public
responsibility for appropriate portions of the content.
According to Tri Council Policy on Integrity in Research and Scholarship (www.nserc-crsng.gc.ca)
• All papers will recognize the substantive contributions of collaborators and students.

Clinical Outcome Measurement of Eating Disorders
36
• All papers will ensure that authorship of published work includes all those who have materially contributed to, and share responsibility for, the contents of the publication, and only those people.
Background/Reference Material Regarding Contributors Listed in
Acknowledgments All contributors who do not meet the criteria for authorship should be listed in an acknowledgment section. Examples of those who might be acknowledged include a person who provided purely technical help, writing assistance, or a department chair that provided only general support. Corresponding authors should declare whether they had assistance with study design, data collection, data analysis, or manuscript preparation. If such assistance was available, the authors should disclose the identity of the individuals who provided this assistance and the entity that supported it in the published article. Financial and material support should also be acknowledged. Groups of persons who have contributed materially to the paper but whose contributions do not justify authorship may be listed under such headings as “clinical investigators” or “participating investigators,” and their function or contribution should be described—for example, “served as scientific advisors,” “critically reviewed the study proposal,” “collected data,” or “provided and cared for study patients.” Because readers may infer their endorsement of the data and conclusions, these persons must give written permission to be acknowledged. As recommended by the Council of Science Editors’ Recommendations for Group Author Articles in Scientific Journals and Bibliometric Databases, the CMDP team will use the following byline style when the number of contributing authors exceeds that requested by a specific journal. Byline: Steven Q Smith, MD, Yoko Suzuki, MD, J T Mann, PhD, Klaus T Schulze, MD, Christine DeAngelo, MD, Charles Davis, MD, PhD, Katherine J Jones, MD, and CMDP of PEDP in Ontario.

Clinical Outcome Measurement of Eating Disorders
37
Centralized Multi-Site Partnership of Pediatric Eating Disorders Program’s in Ontario’s
Additional Processes Regarding Authorship, Acknowledgements, and Manuscripts Agreement
Our approach to authorship is inclusive in that all partners/investigators will have the opportunity to be co-authors on papers and presentations. Decisions about lead authorship on papers that address primary research questions are/were discussed when the CMDP group met/meets on XXX and are documented in the “People & Projects” document. Any changes to the documented decisions will be made by the research team by 100% consensus. Decisions about lead authorship on papers that address secondary research questions will also be made by the research team by consensus. The CMDP investigators will establish a PI lead group. The investigators will each choose ____ from each site to sit on the PI lead group committee. This committee will meet regularly to review research proposals, authorship, and timelines for research papers.
• The investigator team will prepare and approve a list of potential manuscripts and presentations, lead authors and timeframes that will be approved by all investigators.
• The list of proposed manuscripts will identify a corresponding “lead” author who will meet the criteria above and will hold responsibility for drafting the first version, managing input from other authors, manuscript submission and editorial process.
• Investigators who take a key role in the writing of any paper of the full study findings will be listed according to their contribution following the lead author. If contributions are equal, authors will be listed alphabetically.
• Site Investigators will have the first option to be the lead author on papers that report results from an individual site.
• All authors have the right to opt-out of any paper where they feel they have not contributed by informing the lead author in writing at the time of the first manuscript review.
• The lead author should inform any co-authors who have not participated or contributed to the paper or to the review process following the designated review timeline that they will be removed from the author list and included in the Acknowledgments.
• The PI Lead Group and all co-investigators will be informed of any proposed manuscripts or presentations stemming from the CMDP’s database that have not already been vetted by the team. All proposed papers will be submitted to the PI Lead Group with a title, proposed list of authors, short abstract, intended journal and timeframe for submission. This will be circulated to the investigator team for review and approval. The PI Lead Group will provide written permission via email to the investigative team to proceed with manuscript submission, after an in-person or conference call discussion. Manuscripts will be prepared and submitted in a 12 month period from the time of outline approval, unless otherwise indicated in the Application for Requesting Secondary Use of Data.
• All authors involved with a paper will be responsible for reviewing and making

Clinical Outcome Measurement of Eating Disorders
38
contributions within a timely manner including: o 2 weeks for manuscripts o 1 week for abstracts
Students and Learners
• All students and other learners who have contributed to the project will be acknowledged in the Acknowledgement section.
• If a student or learner assumes a major role in a secondary project associated with the CMSP database, under the supervision of a Partner, the student or learner may request to co-lead authorship. Under this circumstance, the student or learner would have to play a major role in the initial draft.
Any concerns regarding authorship decisions should be discussed with the PI Lead Group.
Designating a New Partner on the CMDP of PEDP of Ontario To be considered as a partner the candidate must meet the following criteria:
• Be nominated by a partner of the CMDP • Be a clinician/treatment provider with one of the partnering organizations
Decision making regarding the designation of a new partner will include the following;
• Information is presented to the PI Lead Group for discussion and a recommendation.
• If the PI Lead Group agrees on a recommendation, the information and PI Lead Group’s recommendation is shared with all partners via email and feedback is requested (options: agree with recommendation or prefer to discuss with all partners).
• If the PI Lead Group do not agree on a recommendation, the information is shared with the all partners and is discussed during a teleconference or in-person meeting.
Formalizing the designation of a new partner will include the following;
• A member of the PI Lead Group will invite the candidate to join the partnership via email and outline anticipated contributions and collaborations, and send the candidate relevant documents (e.g. this manual, Research Projects & People, and Application for Requesting Secondary Use of Data).
• Once the candidate confirms this agreement to join the partnership, a member of the PI Lead Group will ensure that the candidate completes the Partnership Letter of Agreement.
• The Research Projects & People document will be updated.

Clinical Outcome Measurement of Eating Disorders
39
Background/Reference Material Regarding Intellectual Property and Data Sharing According to Tri Council Policy Statement: Ethical Conduct for Research Involving Humans 1998(TCPS) www.pre.ethics.gc.ca, the following principles will be followed. Article 11.11 With respect to research findings:
(a) Institutions and research ethics boards should take necessary measures to ensure that researchers and institutions share research results and publish or otherwise disseminate the analysis and interpretation of research findings in a timely manner without undue restriction.
Article 11.11 further states: 4. Provide that all confidentiality and publication clauses: (a) Are consistent with the researcher’s duty to share new information from
clinical trials with REBs and trial participants in a timely manner (Section D [“Sharing New Information”]);
(b) Are reasonable in terms of any limitations or restrictions on the publication or other dissemination or communication of information; and
(c) Permit researchers to access study data.
Centralized Multi-Site Partnership of Pediatric Eating Disorders Program’s in Ontario’s
Intellectual Property and Data Sharing Agreement All data will be shared with co-investigators through remote access to the centralized
multi-site database. Note that this does not permit an investigator to publish from this data unless agreed upon in the process detailed in this document.
Each site will send a copy of raw data to the research team lead at the Children’s Hospital of Eastern Ontario’s Eating Disorders Program.

Clinical Outcome Measurement of Eating Disorders
40
Application for Requesting Secondary Use of Data Compiled by the
Centralized Multi-Site Partnership of Pediatric Eating Disorders Program’s in Ontario
The Centralized Multi-Site Partnership (CMSP) of Pediatric Eating Disorders Program’s in Ontario fosters a collaborative atmosphere. This self-governing group makes decisions based on 100% consensus. While the group operates on an honor system, there are requirements and conditions of participation that have evolved and which must be met if the privileges of access to CMSP data sets are to be granted. These conditions are outlined in this document, the Partnership Letter of Agreement, and the Authorship Guidelines, Role Definitions, and Procedures Manual, each of which must be read before signing this Application. Partner use of data from the CMSP database is contingent upon adherence to the following stipulations: 1. A brief research proposal outlining the title, proposed list of authors, a short abstract (detailing the research question(s), relevant hypotheses, sub-sample or groups, variables, and proposed statistical methods), intended journal for submission, and a timeframe must be submitted to the CMSP PI Lead Group for approval. The PI Lead Group may work to refine the research topic and questions to prevent duplication or overlap with existing projects. 2. The proposal must also identify how this study adheres to the purposes of CMSP and might be of benefit to youth struggling with an eating disorder. 3. Ethics review must be obtained from an accredited Research Ethics Board at the partner’s institution, prior to submission to the Research Ethics Board at the Children’s Hospital of Eastern Ontario. 4. All data analyses must be conducted by remote access to the Centralized Multi-Site Database housed by the Children’s Hospital of Eastern Ontario. No dataset or subset may be copied or removed. 5. Partners agree to hold all data as confidential, and will neither conduct analyses nor report data in such a way that individual participants could be identified or identifiable. 6. Any reports, manuscripts, presentations, or posters must be approved in writing by the PI Lead Group of the CMSP prior to submission; requests for review and approval must be made at least 3 weeks before the submission deadline. 7. Acknowledgment of the CMSP as the source of the data must be made in any reports, manuscripts, presentations, or posters. 8. Approval is for a particular purpose and research question(s) and cannot be transferred to another person or extended to include other uses. If you wish to expand the scope of the project to include other questions, you must first discuss this with the PI Lead Group, have the approval of all partners, and have approval in writing from the CMSP Lead. 9. CMSP encourages the dissemination of research to the wider community. It is expected that each project will conclude with a brief fact sheet or abstract of results for general audiences that the CMSP can distribute to policymakers, professionals who work with this population, and youth themselves.

Clinical Outcome Measurement of Eating Disorders
41
10. Permission for the use of data is given for a specified period of time. If the project is not completed during this time period, the permission is rescinded, unless an extension has been approved by the CMSP. The specific time period will be discussed and agreed on by all partners of the CMSP. 11. In order to promote timely reporting of research, if a partner contracts to submit a manuscript for publication from their project, and such a manuscript is not submitted within the approved timeline, the PI Lead Group reserves the right to approve/assign a new lead to that particular project who will prepare this manuscript for publication on the partners behalf. In such a circumstance, author order may need to be renegotiated to reflect the efforts of the CMSP partner who assumes the lead role on this project. 12. A copy of any reports, manuscripts, presentations, posters, or fact sheets must be given to all CMSP partners.
The Centralized Multi-Site Partnership of Pediatric Eating Disorders Program’s in Ontario gives permission to:
Name ______________________________________________________________________ To use the following variable(s) from the data set _____________________________________ For the proposed project entitled: _____________________________________________________________________________________________________________________________ which has been submitted to the Centralized Multi-Site Partnership (see attached) and has been approved by all partners of the Centralized Multi-Site Partnership on (date) ________________ The permission is given for the time period of __________ to _____________________ I have read all the requirements in this contract and I agree to adhere to them. Signature ________________________________ Date _________________________ Name ___________________________________ Title _________________________ Partnering Site __________________________________

Clinical Outcome Measurement of Eating Disorders
42
As a member of the PI Lead Group, my signature below indicates that I have agreed to allow the data from my site to be included in the data analyses conducted by the above stated partner, for the above stated purpose(s). Signature _______________________________ Date _________________________ Dr. Annick Buchholz, Children’s Hospital of Eastern Ontario, Eating Disorders Program Signature ________________________________ Date _________________________ Dr. Sherry Van Blyderveen, McMaster Children’s Hospital, Pediatric Eating Disorders Program Signature ________________________________ Date _________________________ xxx Signature ________________________________ Date _________________________ xxx

Clinical Outcome Measurement of Eating Disorders
43
APPENDIX E
____________________________________
Assignment of Research Studies

Clinical Outcome Measurement of Eating Disorders
44
Research Projects
Project Lead Site Brief Description Publications
Assessment Data
CHEO
Clinical profile by diagnostic category (AN-R, AN-BP, etc.) of youth presenting for an eating disorder assessment at a tertiary care hospital in Ontario.
CHEO Examining parent variables at assessment.
Southlake Satisfaction with assessment services provided.
Southlake Presence of abuse at assessment.
HSK Using assessment data for the purposes of improving the system of diagnostic classification, using latent class analysis.
Follow-up Data
CHEO Trajectory of different diagnostic category (psychological focus).
Southlake
Exploration of how assessment results relate to treatment recommendations and how recommendations map onto services offered and accepted.
HSK Predictors of short term medical outcomes.
HSK Determination of ideal body weight.

Clinical Outcome Measurement of Eating Disorders
45
APPENDIX F
____________________________________
Excerpt from Data Definition Dictionary

Clinical Outcome Measurement of Eating Disorders
46