A CASE REPORT OF ORO –ANTAL FISTULA TREATED …ijhbr.com/pdf/4 2014 116-119.pdf · The oroantral...
5
International J. of Healthcare and Biomedical Research, Volume: 2, Issue: 3 , April 2014 , Pages 116-119 116 www.ijhbr.com ISSN: 2319-7072 Case Report: A CASE REPORT OF ORO –ANTAL FISTULA TREATED WITH A COMBINATION TECHNIQUE OF BUCCAL ADVANCEMENT FLAP AND BUCCAL FAT PAD 1 Dr Gopal Sharma, 2 Dr Jaya Mukherjee , 3 Dr Bhagyashree Purandare 1 Head of department, Dept of Oral medicine and Radiology, YMT Dental college , Kharghar, Navi Mumbai 2 Postgraduate studies, Dept of Oral medicine and Radiology, YMT Dental college , Kharghar, Navi Mumbai 3 Postgraduate studies, Dept of Oral medicine and Radiology, YMT Dental college , Kharghar, Navi Mumbai Corresponding author : Dr Jaya Mukherjee Abstract : The oroantral fistula (OAF) is a pathological communication between the oral cavity and the maxillary sinus; depending on the location it can be classified as alveolo-sinusal, palatal-sinusal and vestibulo-sinusal. Oro-antral communications may develop as a complication of dental extractions, but may also result from accidental or iatrogenic trauma, neoplasm or infection . An oroantral fistula which is smaller than 2 mm frequently closes spontaneously. A 28 years old healthy male reported to the outpatient department of hospital for evaluation of pus discharging fistula distal to left upper first molar. A surgery was planned for the removal of displaced root segments and closure of the fistula. A Caldwell luc approach was used to remove the roots and the closure of oro antral fistula was done by using double layer technique with buccal fat pad and a buccal advancement flap. The sutures were then placed. The treatment of oronatral fistula through the use of buccal advancement flap and buccal fat pad is a simple and complete method which enables several uses in most of cases. Keywords : Coroantral fistula Introduction : The oroantral fistula (OAF) is a pathological communication between the oral cavity and the maxillary sinus; depending on the location it can be classified as alveolo-sinusal, palatal-sinusal and vestibulo-sinusal. 1 Oro-antral communications may develop as a complication of dental extractions, but may also result from accidental or iatrogenic trauma, neoplasm or infection. 2,3 An oroantral fistula which is smaller than 2 mm frequently closes spontaneously. However, when the defect is bigger or when there is inflammation, maxillary sinus or periodontal region infection, such fistula demands surgical treatment for its complete closing. 4 This article reports a case of a oro-antral fistula successfully treated with a double layer technique using buccal fat pad and buccal advancement flap and removal of displaced roots of molar from the antrum. Case Report : A 28 years old healthy male reported to the outpatient department of hospital for evaluation of pus discharging fistula distal to left upper first molar. The patient gave history of traumatic extraction of upper left second molar 2 months back. He had discomfort in the region of the extraction socket. Soon after, expression of a yellowish foul smelling discharge followed from the socket, the patient reported for the dental check up .The patient reported that the crown was fractured while extraction. The patient also reported of foul smelling discharge from nose while drinking water. The intra oral examination revealed that the left upper second molar was absent. Purulent material from the fistula was observed distal to left maxillary first molar. A provisional diagnosis of oro-antral fistula was given based on the history and examination.
-
Upload
nguyentram -
Category
Documents
-
view
221 -
download
0
Transcript of A CASE REPORT OF ORO –ANTAL FISTULA TREATED …ijhbr.com/pdf/4 2014 116-119.pdf · The oroantral...

International J. of Healthcare and Biomedical Research, Volume: 2, Issue: 3 , April 2014 , Pages 116-119
116
www.ijhbr.com ISSN: 2319-7072
Case Report:
A CASE REPORT OF ORO –ANTAL FISTULA TREATED WITH A COMBINATION
TECHNIQUE OF BUCCAL ADVANCEMENT FLAP AND BUCCAL FAT PAD
1 Dr Gopal Sharma, 2 Dr Jaya Mukherjee , 3Dr Bhagyashree Purandare
1Head of department, Dept of Oral medicine and Radiology, YMT Dental college , Kharghar, Navi Mumbai
2Postgraduate studies, Dept of Oral medicine and Radiology, YMT Dental college , Kharghar, Navi Mumbai
3Postgraduate studies, Dept of Oral medicine and Radiology, YMT Dental college , Kharghar, Navi Mumbai
Corresponding author : Dr Jaya Mukherjee
Abstract :
The oroantral fistula (OAF) is a pathological communication between the oral cavity and the maxillary sinus; depending on
the location it can be classified as alveolo-sinusal, palatal-sinusal and vestibulo-sinusal. Oro-antral communications may
develop as a complication of dental extractions, but may also result from accidental or iatrogenic trauma, neoplasm or
infection . An oroantral fistula which is smaller than 2 mm frequently closes spontaneously. A 28 years old healthy male
reported to the outpatient department of hospital for evaluation of pus discharging fistula distal to left upper first molar. A
surgery was planned for the removal of displaced root segments and closure of the fistula. A Caldwell luc approach was used
to remove the roots and the closure of oro antral fistula was done by using double layer technique with buccal fat pad and a
buccal advancement flap. The sutures were then placed. The treatment of oronatral fistula through the use of buccal
advancement flap and buccal fat pad is a simple and complete method which enables several uses in most of cases.
Keywords : Coroantral fistula
Introduction : The oroantral fistula (OAF) is a
pathological communication between the oral
cavity and the maxillary sinus; depending on the
location it can be classified as alveolo-sinusal,
palatal-sinusal and vestibulo-sinusal.1 Oro-antral
communications may develop as a complication of
dental extractions, but may also result from
accidental or iatrogenic trauma, neoplasm or
infection.2,3 An oroantral fistula which is smaller
than 2 mm frequently closes spontaneously.
However, when the defect is bigger or when there
is inflammation, maxillary sinus or periodontal
region infection, such fistula demands surgical
treatment for its complete closing.4 This article
reports a case of a oro-antral fistula successfully
treated with a double layer technique using buccal
fat pad and buccal advancement flap and removal
of displaced roots of molar from the antrum.
Case Report : A 28 years old healthy male
reported to the outpatient department of hospital for
evaluation of pus discharging fistula distal to left
upper first molar. The patient gave history of
traumatic extraction of upper left second molar 2
months back. He had discomfort in the region of
the extraction socket. Soon after, expression of a
yellowish foul smelling discharge followed from
the socket, the patient reported for the dental check
up .The patient reported that the crown was
fractured while extraction. The patient also
reported of foul smelling discharge from nose
while drinking water. The intra oral examination
revealed that the left upper second molar was
absent. Purulent material from the fistula was
observed distal to left maxillary first molar. A
provisional diagnosis of oro-antral fistula was
given based on the history and examination.
International J. of Healthcare and Biomedical Research, Volume: 2, Issue: 3 , April 2014 , Pages 116-119
117
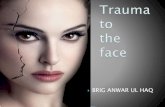
The patient was advised for a orthopantomograph
OPG and cone beam computed tomography CBCT.
The radiographs revealed oro antral communication
with displacement of two roots into maxillary
sinus.
FIG 1- PREOPERATIVE
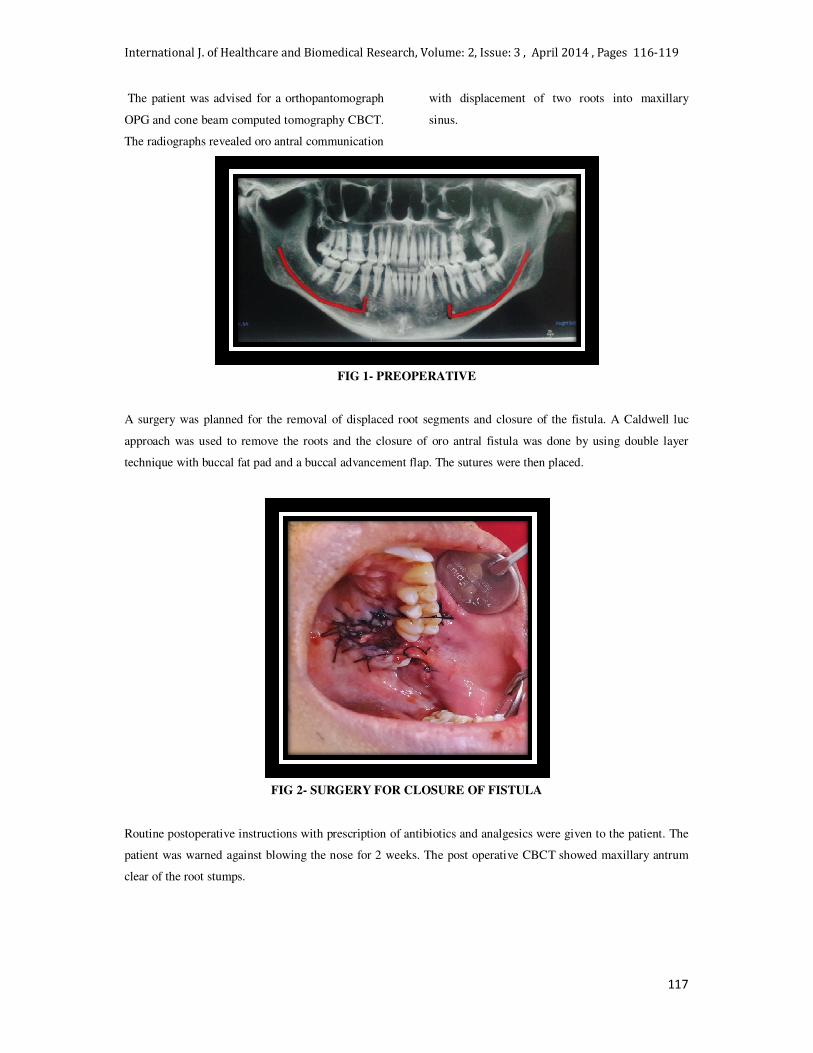
A surgery was planned for the removal of displaced root segments and closure of the fistula. A Caldwell luc
approach was used to remove the roots and the closure of oro antral fistula was done by using double layer
technique with buccal fat pad and a buccal advancement flap. The sutures were then placed.
FIG 2- SURGERY FOR CLOSURE OF FISTULA
Routine postoperative instructions with prescription of antibiotics and analgesics were given to the patient. The
patient was warned against blowing the nose for 2 weeks. The post operative CBCT showed maxillary antrum
clear of the root stumps.
International J. of Healthcare and Biomedical Research, Volume: 2, Issue: 3 , April 2014 , Pages 116-119
117
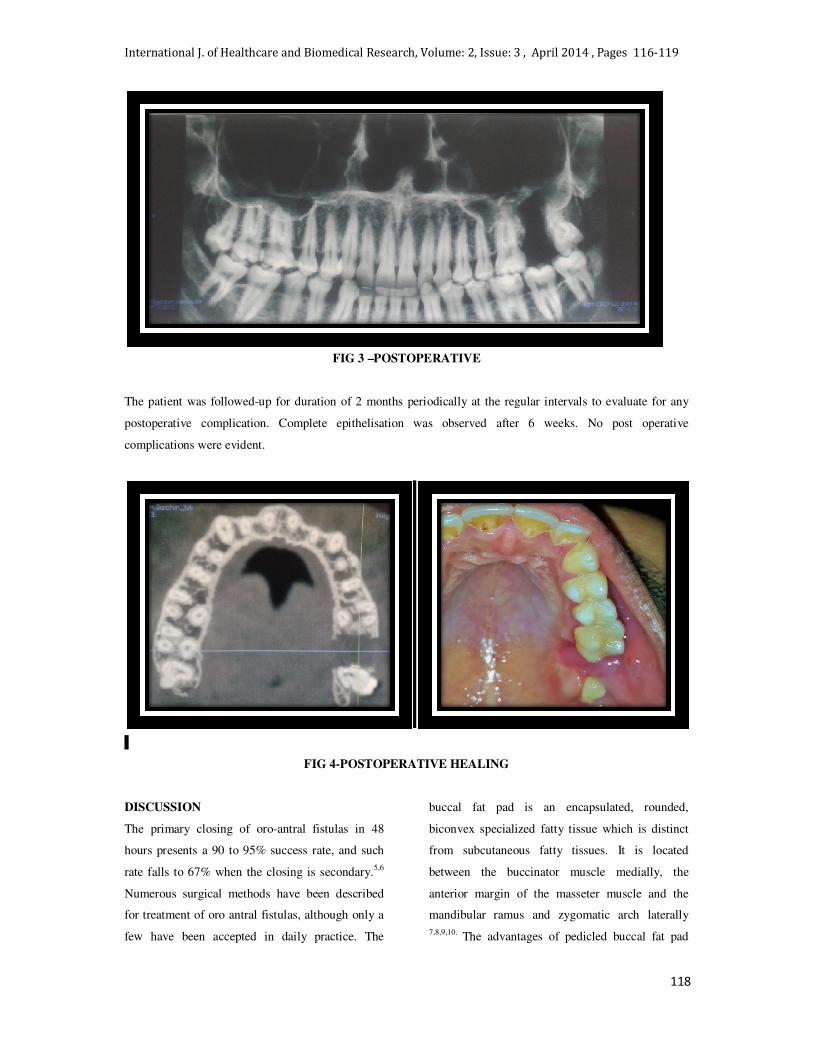
FIG 3 –POSTOPERATIVE
The patient was followed-up for duration of 2 months periodically at the regular intervals to evaluate for any
postoperative complication. Complete epithelisation was observed after 6 weeks. No post operative
complications were evident.
I
FIG 4-POSTOPERATIVE HEALING
DISCUSSION
The primary closing of oro-antral fistulas in 48
hours presents a 90 to 95% success rate, and such
rate falls to 67% when the closing is secondary.5,6
Numerous surgical methods have been described
for treatment of oro antral fistulas, although only a
few have been accepted in daily practice. The
buccal fat pad is an encapsulated, rounded,
biconvex specialized fatty tissue which is distinct
from subcutaneous fatty tissues. It is located
between the buccinator muscle medially, the
anterior margin of the masseter muscle and the
mandibular ramus and zygomatic arch laterally
7,8,9,10. The advantages of pedicled buccal fat pad
118

International J. of Healthcare and Biomedical Research, Volume: 2, Issue: 3 , April 2014 , Pages 116-119
117
www.ijhbr.com ISSN: 2319-7072
(BFP) include ease of harvesting, simplicity,
versatility, low rate of complications, and quick
surgical technique. The blood supply of the buccal
fat pad is not affected due to its displacement, once
it is gripped and replaced between the flap and the
maxillary wall. It is worth noting that the use of
BFP with buccal advancement flap (combination
technique) in the literature is scarce.11,12 It provides
more stability, can be used to cover BFP and as
additional tissue for closure where there is a
deficient BFP for closure.
CONCLUSION
The treatment of oronatral fistula through the use
of buccal advancement flap and buccal fat pad is a
simple and complete method which enables several
uses in most of cases.
REFERENES
1. Borgonovo, Andrea Enrico, Frederick Valerio Berardinelli, Marco Favale, and Carlo Maiorana.
"Surgical Options In Oroantral Fistula Treatment." The open dentistry journal 6 (2012): 94.
2. Seward GR, Harris M, McGowan DA. Killey and Kay’s Outline of oral surgery 2ed. Bristol: IOP
Publishing Ltd; 1987.
3. Yilmaz T, Suslu AE, Gursel B. Treatment of oroantral fistula: experience with 27 cases. Am J
Otolaryngol. 2003 Jul-Aug;24(4):221-3
4. . Hanazawa Y, Itoh K, Mabashi T, Sato K. Closure of oro-antral communications usig a pedicled
buccal fat pad graft. J oral Maxillof Surg. 1995, 53:771-775.
5. Eppley B, Scfaroff A. Oro-nasal fistula secondary to maxillary argumentation. Int Oral Surg. 1984,
13:535.
6. Stajcic Z. The buccal fat pad in the closure of oro-antral communications - A study of 56 cases. J
Craniomaxillofac Surg. 1992, 20:193.
7. Liversedge RL, Wong K. Use of the buccal fat pad in maxillary and sinus grafting of the severely
atrophic maxilla preparatory to implant reconstruction of the partially or completely edentulous patient:
technical note. Int J Oral Maxillofac Implants. 2002 May-Jun;17(3):424-8.
8. Martin-Granizo R, Naval L, Costas A, Goizueta C, Rodriguez F, Monje F, et al. Use of buccal fat pad
to repair intraoral defects: review of 30 cases. Br J Oral Maxillofac Surg. 1997 Apr;35(2):81-4.
9. Rapidis AD, Alexandridis CA, Eleftheriadis E, Angelopoulos AP. The use of the buccal fat pad for
reconstruction of oral defects: review of the literature and report of 15 cases. J Oral Maxillofac Surg.
2000 Feb;58(2):158-63.
10. Samman N, Cheung LK, Tideman H. The buccal fat pad in oral reconstruction. Int J Oral Maxillofac
Surg. 1993 Feb;22(1):2-6.
11. Fujimura N, Nagura H, Enomoto S. Grafting of the buccal fat pad into palatal defects. J
Craniomaxillofac Surg. 1990;18:219–22.
12. Batra H, Jindal G, Kaur S. Evaluation of different treatment modalities for closure of oro-antral
communications and formulation of a rational approach. J Maxillofac Oral Surg. 2010;9:13–8.
Date of submission: 21 January 2014, Date of provisional acceptance: 14 Feb 2013
Date of Final acceptance: 22 March 2014 Date of Publication: 07 April 2014
Source of support: Nil; Conflict of interest: Nil
119

International J. of Healthcare and Biomedical Research, Volume: 2, Issue: 3 , April 2014 , Pages 116-119
117
www.ijhbr.com ISSN: 2319-7072