A, B, Cs of Arterial Studies - St. Joseph Mercy Ann Arbor
33
St. Joseph Mercy Health System endorses the Essentials and Standards of the Accreditation Council for Continuing Medical Education: Faculty are expected to disclose to the audience all relationships with pharmaceutical companies, biomedical device manufacturers, and other healthcare- related for-profit entities... Michalene McPharlin has nothing to disclose DISCLOSURE
Transcript of A, B, Cs of Arterial Studies - St. Joseph Mercy Ann Arbor

St. Joseph Mercy Health System endorses the Essentials and Standards of the Accreditation Council for Continuing Medical Education: Faculty are expected to disclose to the audience all relationships with pharmaceutical companies, biomedical device manufacturers, and other healthcare-related for-profit entities...
Michalene McPharlin has nothing to disclose
DISCLOSURE

‘A’ is for ANATOMY
Aortic Arch &Major Vessels ofUpper Extremity

Aorta and Major Vessels of Abdomen
Major Vessels of Aorto-iliac Segment

Major Vesselsof LowerExtremity
Example of Normal AngiogramExample of Normal Angiogramof Lower Extremity (AP)of Lower Extremity (AP)
SG: Supreme SG: Supreme geniculargenicular
SLG: Superior SLG: Superior lateral genicularlateral genicular
SMG: Superior SMG: Superior medial genicular medial genicular

Example of Normal AngiogramExample of Normal Angiogramof Lower Extremity (AP) of Lower Extremity (AP)
SMG: Superior SMG: Superior medial genicular medial genicular
SLG: Superior SLG: Superior lateral genicularlateral genicular
SU: SuralSU: Sural
ILG: Inferior lateral ILG: Inferior lateral geniculargenicular
Longitudinal & Longitudinal & Transverse Transverse
views obtainedviews obtained
Anatomy Anatomy represented on represented on transverse views transverse views related to related to transducer transducer placementplacement

Vessel Size
The following factors effect size of vessels:Body sizeAgeB/PGender (identified in some studies)
1.5 – 2 times normal adjacent vessel: Ectatic> 2 times: Aneurysmal
Mean Arterial Diameter and PSV
Artery Diameter + SD (cm) Velocity + SD (cm/sec)
Aorta 1.90* (Suprarenal)1.57* (Infrarenal)
80 + 25
Celiac 0.8 + 0.3 160 + 90
SMA 0.6 + 0.15 160 + 60
Renal 0.59 + 1.2* 80 + 20
CIA 0.91 + 1.38* 119.3 + 21.7
(*Journal of Texas Heart Institute, 2006; 33[4]:463-468)

Mean Arterial Diameter and PSV
Artery Diameter + SD (cm) Velocity + SD (c/sec)
EIA 0.79 + 0.13 119.3 + 21.7
CFA 0.82 + 0.14 114.0 + 24.9
Prox SFA 0.60 + 0.12 90.8 + 13.6
Distal SFA 0.54 + 0.11 93.6 + 14.1
Popliteal 0.52 + 0.11 68.8 + 13.5
(Zierler RE, Zierler BK: Duplex sonography of lower extremity arteries)
Arterial Variants: Upper extremity
Common origin of Rt innominate & Lt CCA: Common origin of Rt innominate & Lt CCA:
22%22%
Radial A originates from Axillary Artery: 1Radial A originates from Axillary Artery: 1--3%3%
Ulnar A originates from Axillary A: 2Ulnar A originates from Axillary A: 2--3%3%
Early division of Brachial Artery: 19%Early division of Brachial Artery: 19%

Arterial Variants: Lower extremity
High bifurcation of the popliteal artery: 4%
High bifurcation of the popliteal artery w/
peroneal arising from the ATA: 2%
Absent PTA (may have distal reconstruction
at ankle from peroneal): 1-5%
Arterial Variants: Lower extremity
Hypoplasia or aplasia of ATA (with
resultant absence of DPA pulse): 4-12%
Anomalous location of DPA: 8%

Some of the more common Collateral Routes of Lower
Extremity…
Lower extremity
SFA or PopA obstruction:SFA or PopA obstruction:
DFA TO distal SFA or PopA DFA TO distal SFA or PopA
Distal SFA TO PopA or proximal Distal SFA TO PopA or proximal
trifurcation vessels in calftrifurcation vessels in calf
Genicular and/or sural arteries TO Pop Genicular and/or sural arteries TO Pop
or infrapop arteries dto or infrapop arteries dto

Example of Example of Collateralization:Collateralization:
Occluded Popliteal Occluded Popliteal Artery Artery
SU: SuralSU: Sural
rAT: Recurrent ATrAT: Recurrent AT
Lower extremity
Obstruction of AT/PT/Peroneal:
Non-obstructed proximal calf branches
TO distal arteries in the lower leg or
ankle
Distal peroneal branches TO distal ATA
or PTA

‘B’ means BY THE BOOK
Society for Vascular Ultrasound
4601 Presidents Drive, Suite 260, Lanham, MD 20706-4831 Toll-free: 800-788-8346
Telephone: 301-459-7550 Fax: 301-459-5651
svunet.org

Professional Performance Guidelines
Screening For Abdominal Aortic Aneurysms (AAA)(2/5/13)Mesenteric/Splanchnic Artery Duplex Imaging (2/5/13)Renal Artery Duplex Imaging (11/15/12)Lower Extremity Arterial Duplex Evaluation (8/10/12)Upper Extremity Vein Mapping for Creation of a Dialysis Access or Peripheral Vascular Bypass Graft (8/10/12)Transcranial Doppler in Pediatric Patients with Sickle Cell Anemia: (Non-Imaging) (04/11/12)Evaluation of Dialysis Access (04/11/12)Lower Extremity Arterial Segmental Physiologic Evaluation (04/11/12)
Professional Performance Guidelines
Radial Artery Assessment for Coronary Artery Bypass(04/11/12)Intracranial Cerebrovascular Evaluation Transcranial Doppler (Non-Imaging) and Transcranial Duplex Imaging (TCDI) (04/11/12)Quality Assurance Guidelines for Accuracy of Examinations in the Vascular Laboratory (3/13/12)Upper Extremity Arterial Segmental Physiologic Evaluation (Arterial, TOS, Cold) (revised 12/22/11)Upper Extremity Arterial Duplex Evaluation (revised 11/11)Abdominal Aortoiliac Duplex Evaluation (revised 11/11)Extracranial Cerebrovascular Duplex Ultrasound Evaluation (revised 06/11)
Scope of Practice
Diagnostic Ultrasound Professionals…Perform patient assessmentsAcquire and analyze data obtained using
ultrasound and related diagnostic technologiesProvide a summary of findings to the physician to
aid in patient diagnosis and managementUse independent judgment and systematic
problem solving methods to produce high quality diagnostic information and optimize patient care.
Intersocietal Commission on the Accreditation of Vascular Laboratories
(ICAVL)
6021 University Blvd, Suite 500, Ellicott, MD 21043
Toll-free: 800-838-2110 Fax: 866-663-5663
Intersocietal.org/vascular

3.6.3B Duplex ultrasound of lower extremity arteries (if performed) must include:
3.6.3.1B Grayscale and/or color Doppler images must be documented as required by the protocol and must include at a minimum:
i. common femoral artery; ii. superficial femoral artery; iii. proximal deep femoral artery; iv. popliteal artery; and v. aorta, common and external iliac arteries and tibial
arteries (when appropriate); vi. bypass graft(s) when present including anastomoses.
3.6.3B Duplex ultrasound of lower extremity arteries (if performed) must include:
3.6.3.2B Spectral Doppler waveforms and velocity measurements must be documented as required by the protocol and must include at a minimum waveforms from:
i. common femoral artery; ii. superficial femoral artery; iii. proximal deep femoral artery; iv. popliteal artery; v. tibial arteries; vi. aorta, common and external iliac arteries (when
appropriate); and vii. bypass graft when present, including proximal and
distal anastomoses, inflow and outflow arteries.

Remember to ‘Think Outside the Box’…
Protocols are guidelines that represent ‘best practice’ in the majority of patient situations.
Thinking Outside the Box…
Atypical signs/symptoms or unusual findings compel you to obtain additional information, e.g., more anatomic images and/or flow patterns than stated in protocol.Innovative surgical procedures may require additional documentation in post-op or surveillance studies.Our goal should be to help answer the clinical question whether it follows a ‘protocol’ or not.

‘C’ COMPLETES THE PROCESS
Did you help answer the clinical question/s?
“Listen to your patients, at least 90% of your diagnosis is based on the history and physical examination. The other 10% depends on diagnostic tests”
D. Eugene Strandness, Jr., M.D.

A Critical Component of All Noninvasive Evaluations…
Requires thinking outside the box: Truly listening to the patientA willingness to do more than what is stated in the protocol
Diagnostic Tests: Noninvasive Evaluations…
Serves to refine the clinical evaluation by providing objective information about anatomy and physiologyRequires knowledge of:
Differential diagnosesNormal anatomy & anatomic variantsNormal & abnormal blood flow patterns
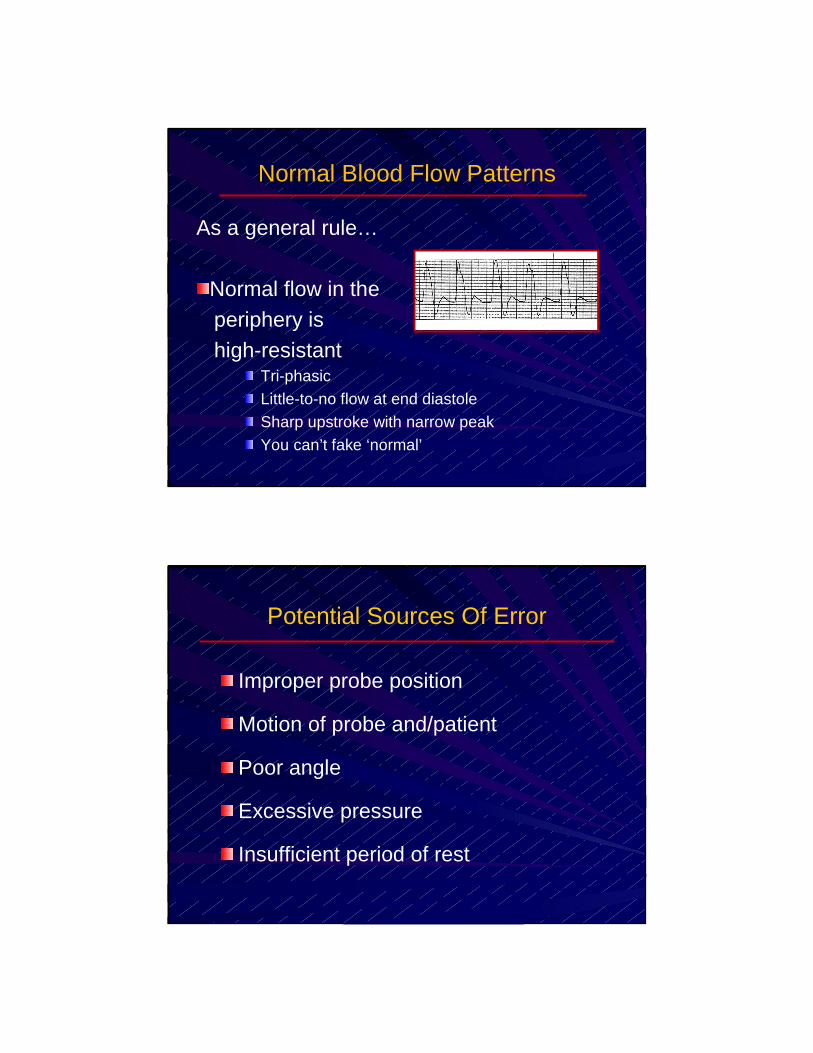
Normal Blood Flow Patterns
As a general rule…
Normal flow in theperiphery is high-resistant
Tri-phasicLittle-to-no flow at end diastoleSharp upstroke with narrow peakYou can’t fake ‘normal’
Potential Sources Of Error
Improper probe position
Motion of probe and/patient
Poor angle
Excessive pressure
Insufficient period of rest

Normal Blood Flow Patterns
As a general rule…
Flow to organs islow-resistance (Fasting SMA is an exception)
High metabolic needsBlood required throughout cardiac cycle Sharp upstroke expected
Blood Flow Patterns
Diastolic flow documents the status of the distal vascular bedIf diastolic flow different from expected,
ask why…Normal physiologic response? Reflective of a diseased state?

Altered Diastolic Flow Patterns
A peripheral vessel may have low resistance flowfor a variety of reasons, e,g,
StenosisHyperemia related to healingHyperemia secondary to cellulitisDistal arteriovenous fistulaExercise
Altered Diastolic Flow Patterns
A normally low-resistantvessel may have high-resistance flow for avariety of reasons, e,g,
Distal occlusionOrgan failureNonfunctioning dialysis accessVasospasm/vasoconstriction

Blood Flow Patterns
Systolic flow represents the status of the proximal vesselsIf systolic flow different from expected,
ask why…Unilateral change probably attributed
to proximal arterial diseaseBilateral alterations may be related to
vessels and/or cardiac status
Altered Systolic Flow Patterns
Objective measurements:Pulsatility indexAcceleration time /Rise time
> 133 msec in CFA consistent with inflow disease> 100 msec in Kidney consistent with
renal artery disease
Subjectively applied to most vessels in the body

Remember…
Systolic upstroke provides information about where the blood came fromDiastolic flow patterns provide informationabout where the blood is going to
Velocity

Physical Principles
Calculating for Velocity V = c Df 2Fo Cos Ø
– V = Calculated value– C = Speed of US in soft tissue– Df = Known value, measured by duplex;
Proportional to velocity of source– Fo = Carrier frequency/transducer frequency
– Cos Ø = Angle determined from image
Effects of Stenosis
Stenosis Profile
Pre-stenosis: Reduced velocities with alteration in diastolic flow
Stenosis: Elevated velocities with severe spectral broadening
Post-stenosis: Turbulence (e.g., flow reversals, eddy currents, vortices)

General Guidelines: Peripheral Vessels
Abnormal: (Compare stenotic to pre-stenotic)
– 2:1 ratio = > 50% DR– 4:1 ratio = > 75% DR– PSV >400 cm/s = > 75% DR
– Never accept value of numbers alone; should see post-stenotic turbulence
General Guidelines: Renal Artery
RAR: Highest Renal A PSVAorta PSV
Normal: < 3.5
Abnormal: bnormal: > 3.5 ( > 60% DR)
Cannot use RAR if AAA detected
Cannot use RAR if aortic PSV >90 or <40 cm/s
Renal A PSV: >180 - 200 cm/sec = > 60% (“Stenosis profile”)

General Guidelines: Kidney
� EDR: End Diastolic V Normal = > 0.2PSV Abnormal = < 0.2
� RI: PSV - EDV Normal = < 0.8PSV Abnormal = > 0.8
General Guidelines: Mesenteric Arteries
SMA CeliacNormal PSV: 110-177 cm/s 50-160 cm/s
Stenosis >275 cm/s >200 cm/sCriteria: predicts predicts
> 70% DR > 70% DR
(DR = Diameter Reduction)

General Guidelines: ICA(University of Washington)
% Stenosis PSF EDF PSV EDV
0-15% <4 NA < 125 NA
16-49% <4 NA < 125 NA
50-79% >4 <4 > 125 < 140
80-99% >4 >4 > 125 > 140
Carotid Duplex Consensus Conference
Suggested Criteria For Doppler Diagnosis of ICA Ste nosis
Additional Parameters

Stented VesselsStented Vessels
Elevated velocities are expectedElevated velocities are expected
However, greatly elevated However, greatly elevated velocities are abnormalvelocities are abnormal
Image and velocity measurements Image and velocity measurements are critical in the evaluation of are critical in the evaluation of stented vesselsstented vessels
Additional Data Obtained…
Pressure Measurements

Four cuff method
Three cuff method
Interpretation: LE Pressures
Ankle/brachial Index (ABI): divide ankle BP by higher brachial BP
> 1.0 = Normal
>0.9 - 1.0 = May be within normal limits
0.8 - 0.9 = Mild arterial disease
0.5 - 0.8 = Claudication (moderate disease)
< 0.5 = Rest pain (severe disease)(Incompressible vessels can cause falsely elevated BP)

Additional Guidelines:
Segmental P drops of >30 mmHg between 2 adjacent levels is significant
Horizontal P difference of >20-30 mmHg suggests obstructive disease
Interpretation: UE Pressures
15-20 mmHg difference from arm - arm
>15-20 mmHg drop from upper arm to forearm suggests…– Brachial A obstruction distal to upper cuff– Obstruction in both radial and ulnar A– Obstruction in single forearm A
>20 mmHg between radial and ulnar
Interpretation: Digits
UE digits : Finger/brachial indices 0.8-0.9
LE digits :Toe/brachial indices 0.6-0.8
Interpretation: Penile Pressures
Normal = > 0.75
Marginal = 0.65 – 0.74
Abnormal = < 0.65

Completing the Process Includes…
Generating waveforms, gray-scale images, color-flow Doppler, and variouscalculations Knowing when additional information is needed to help answer the clinical question
The Process isn’t Complete Until the Paperwork is Done…
Storing/processing the diagnostic information obtainedProviding preliminary reportCompleting billing documentsSubmitting data for final report
In conclusion...In conclusion...
Know the A, B, Cs of arterial testingKnow the A, B, Cs of arterial testing …It will help you provide important diagnostic information critical to the medical and/or surgical management of your patient.However, the value of that information is directly related to your knowledge, skill, and willingness to sometimes ‘think outside the box’ in order to answer the clinical question.
YOU make the Difference...YOU make the Difference...
Between an adequate study and an exceptional oneDetermining whether additional diagnostic information is neededAssisting with possible treatment optionsEvaluating the success of traditionaland/or non-traditional treatment

YOU make the Difference...YOU make the Difference...
Did you help the patient?
That’s the real reason we’re here!