2014 Toronto Water Operating Analyst Notes - City of Toronto
E
EndocrinologyRupal Shah, AdU Shamji and Vitbika Sivabalasund.aram, chapter editors Doreen Ezeife and Nigel Tan, associate editors Steven Wong, EBM editor Dr. Alice Cheng, staff editorBasic Anatomy Review ................... 2 Major Endocrine Organs Dyslipidemias ........................... 2 Overview of Lipid Transport Hypercholesterolemia Hypertrig lyceridem ia Combined Hyperlipidemia Dyslipidemia and the Risk for CAD Treatment of Dyslipidemias Disorders of Glucose Metabolism .......... 6 Overview of Glucose Regulation Pre-Diabetes Diabetes Mellitus (OM) Treatment of Diabetes Acute Complications Macrovascular Complications Microvascular Complications Other Complications Hypoglycemia Metabolic Syndrome Obesity .............................. FM5 Pituitary Gland ......................... 16 Pituitary Hormones Growth Hormone (GH) Prolactin (PRL) Luteinizing Hormone (LH) and Follicle Stimulating Hormone (FSH) Antidiuretic Hormone (ADH) Pituitary Pathology Thyroid .............................. 20 Thyroid Hormones Tests of Thyroid Function and Structure Thyrotoxicosis Graves' Disease Subacute Thyroiditis Toxic Adenoma/Toxic Multinodular Goitre Thyrotoxic Crisis(fhyroid Storm Hypothyroidism Hashimoto's Thyroiditis Myxedema Coma Sick Euthyroid Syndrome (SES) Non-Toxic Goitre Thyroid Nodules Thyroid Malignancies Adrenal Cortex ......................... 29 Adrenocorticotropin Hormone (ACTH) Adrenocortical Hormones Tests of Adrenocortical Function Hyperaldosteronism Cushing's Syndrome Congenital Adrenal Hyperplasia Hyperandrogenism Adrenocortical Insufficiency Adrenal Medulla ........................ 35 Catecholamine Metabolism Pheochromocytoma Multiple Endocrine Neoplasm (MEN) Calcium Homeostasis .. 37 Hypercalcemia Hypocalcemia Hyperphosphatemia Hypophosphatemia Hypermagnesemia Hypomagnesemia Metabolic Bone Disease ................. 43 Osteoporosis Osteomalacia and Ricketts Renal Osteodystrophy Paget's Disease of Bone Male Reproductive Endocrinology ......... 48 Androgen Regulation Tests of Testicular Function Hypogonadism and Infertility Erectile Dysfunction Gynecomastia Common Medications ................... 51 Diabetes Medications Dyslipidemia Medications Thyroid Medications Metabolic Bone Disease Medications Adrenal Medications Landmark Endocrinology Trials ........... 55 References . . . . . . . . . . . . . . . . . . . . . . . . . . . . 56
Toronto Notes 2011
Endocrinolo8f El
E2 Endocrinology.....
Basic Anatomy Review/Dyslipidemias
Toronto Notes 2011
',
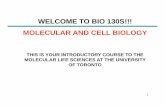
Basic Anatomy ReviewMajor Endocrine OrgansHypothalamus Corticotropin-RH (CRH) Gonadotropin-RH (GnRH) Thyrotropin-RH (TRH) Growth hormone-RH (GHRH) Antidiuretic hormone (ADH) Oxytocin Note: RH = releasing hormone Thyroid gland Triiodothyronine (T3 ) Thyroxine (T,)
ADH and oxytocin are synthesized by the hypothalamus. They are transported via neurons to the posterior pituitary and are subsequently secreted into the systemic circulation from this location.
11,GENERAL FUNCTION OF ORGANS The Hypothalamic-Pituitary Axis Information about cortical inputs, automatic function, environmental cues (light, temp) and peripheral hormonal feedback is synthesized at the coordinating centre of the endocrine system, the hypothalamus. The hypothalamus then sends signals to the pituitary to release hormones to affect the thyroid, adrenals, gonads, growth, milk production and water balance. Anatomy +-+ Function Hypothalamic hormones: small peptides, no binding protein -+ rapid degradation High [ 1in pituitary-portal blood system Low [ 1in peripheral circulation Proximity of axis preserves the pulsatile output signals from the hypothalamic neurons. Thyroid Thyroid hormone is critical to 1) brain and somatic development in fetus and infants, 2) metabolic activity in adults, and 3) function of virtually every organ system. Adrenal Each gland, 6-Sg, has 1) a cortex with 3 layers that act like independent organs (zona glomerulosa -+ aldosterone, fasciculata -+ cortisol, reticularis -+ androgen and estrogen precursors), and 2) a medulla that acts like a sympathetic ganglion to store/synthesize adrenaline and noradrenaline. Gonads Bifunctional: sex steroid synthesis and gamete production Sex steroids controls sexuality and affect metabolic and brain functions Parathyroid Synthesize and secrete PTH, a principle regulator of ECF Ca, regulated by [Ca]. [Mg1 and 1,25(0H)2D (active metabolite ofVit-D). Pancreas Endocrine islet cells produce insulin: oppose glucose production (glycogenolysis, gluconeogenesis), increase glucose uptake into muscle, liver and fat. Glucagon, epinephrine, cortisol, and GH are counter regulatory.
Pituitary gland Anterior pituitary Growth hormone (GH) Prolactin (PRL) Thyroid-stimulating hormone (TSH) Luteinizing hormone (LH) Follicle-stimulating hormone (FSH) Adrenocorticotropic hormone (ACTH)
Adrenal gland Cortex: aldosterone, cortisol. androgens Medulla:
Parathyroid glands Parathyroid hormone (PTH) Pancreas Insulin, glucagon
Figure 1. Endocrine System
DyslipidemiasDefinition metabolic disorders characterized by elevations of fasting plasma cholesterol, and/or triglycerides (TG), and/or low HDL
Overview of Lipid Transport lipoproteins are spherical complexes that consist of a lipid core surrounded by a shell of water-soluble proteins and phospholipids lipoproteins transport lipids within the body apolipoproteins serve as enzyme co-factors and stabilize the lipoprotein micelle Table 1. LipoproteinsLipoprotein Exogenous pathway Chylomicron Endogenous Pathway VLDL IDL B-48, C, E, A-1, A-11, A-IV Transports dietary TG from gut to adipose tissue and muscle Transports hepatic synthesized TG from liver to adipose tissue and muscle Product of hydrolysis of VLDL by lipoprotein lipase resulting in depletion ofTG core Enriched in cholesterol esters Formed by further removal of residual TG from IDL core by hepatic lipase resulting in greater enriched particles with cholesterol esters Transports cholesterol from liver to peripheral tissues (gonads, adrenals) Transports cholesterol from peripheral tissues to liver Acts as a reservoir for apolipoproteins Apolipoproteins Function
B-100, C, E B-100, E
LDL
B-100
HDL
A-I,A-II,C,E
'IbroDlo Nota 2011
Endocrinology E3
EXOGENOUS PATHWAY
BIDGB- PA1IIWAY
E C.ll B-4B
Chylomicron
:_;dilgtadw'lfifnla Filly Al:ids
IPE.Ptse
Mpoae TIIIUIIIld Muac:le
llC1Mitioll byApo
"lP liptQ,..,....
II
i
Figun 2.
alii! E'lld111Janoua BiDQIIItlatic Upid
HypercholesterolemiaPRIMARY HYPERCHOLESTEROLEMIA
Tlllla 2. Tha Pri..ary llyparchalllltaralamiasTn11dn11n Familial Hyparchala&t11rana (Fredlridcscln Typallll)1/!iOO in US 1' UJL Tm.Jus Xllnthomlltolis Hatarozygotal: improvement Autlls111111l cklminn Mill 1' TC (achles, patella!; 111d axl&nlar of l.lll Mill lbll combilalian high pnlnlnce ta'ldn af hand) of HMG CoA lllilctasa Defect ilthe llDil11lll Arcus com!B! iHJitors, niDI. or ble acid UJL recaptor an cell xanthelaama 8&q.l81111ntl o Heterazygotas: 11111111ura Hamorygotal: ptrtial control manmnaa CAD. SIR. risk af Ml ilman Mill pclllc:aVlll shlnt or by aga30 Llll apharais il HlllllllYIIDII!S: ITIIIIifest CAD with riacil; large lilse end ather YIICuler dileeee llorvaabllil is modallly Billy il clildhaad ll1d can be 8llilctive faml( 9.0%, initiate pharmacologic therapy immediately and consider combination oral therapy or insulin immediately see Common Medications, E51 fur details on antihyperglycemic agents Medical Treatment: Insulin (Figure 5) used fur Type 1 DM, may be used in Type 2 DM at any point in treatment routes of administration: subcutaneous injections, continuous subcutaneous insulin infusion pump, IV infusion (regular insulin only) bolus insulins: short-acting (Humulin R, Novolin Toronto), rapid-acting analogue (Apidra, Humalog, Novorapid) basal insulins: intermediate-acting (Humulin N, Novolin NPH),long-acting analogue (Lantus, Levemir) premixed insulins (%Rand %NPH) 10/90, 20/80, 30/70, 40/60, 50/50; analogues (Humalog Mix2S, Hu.malog MixSO, Novomi:x 30) estimated total daily insulin requirement: 0.5-0.7 units/kg
ffla:tatfi_..GI_ illP 2 DM: n. ACimll Trill NfJM 2008; 358:2545-51 lbldr: M.._ JllldomiNd, C411tJUiad 1rill l'lllnll: 1o,251 patients (mean age 62.2) wilh Type 2 DM. 111d Cll'dilvllailr risk flc1Drl. llllrnnlan: . . . . tlmpy llrgeting aiiJA1C laval rl laA thin 6.0'Jo or lllndlnl 111111P!' 1llgalilg 7.01D7.K. 0..-rlnorfml Ml noriml llrDkl. or dlllh flam CV CIIIIH. 11116:111t intln!M lhalpy IIIII Wlllluppad llrly (3.5"' VI. 5.6"' P8lll'lldla1D hidance rl ilcrased 1T10itllty. There WIS no dilfnlce il prim.., IIIII:Dmlfar iiiiII!Jdv IIIII. Thlrl WHisignificlnt i - in._ rnartllty, C'keUIIIII'IOIIDty. nodllll Ml, liM! all congllti8 belltfaikn in the irensive theApy PJP. There wn iiiCIIIIId IIIII rl all?jpogl'fcamic Mllll. Ill\' nonl?nogl'fcmic llrilu IIMIII Md. luid lltlnlion,ltld Wllight gain >10 ka but lower systolic ltld iludc 1m! prntiD in lha inlllllivl 1llerlpv group. There WISIII increlsed incidence rl IIIMIId ALT (>3 hiiPI* limij 111d ACE IWg Ule in the sllndllll flmpv graup. l:lli:luilll: hbmsMI lowering 1bll1py in Type 2 DM does nol in'II'M cili: M:omes 11M! IC!JJdyin-11111 rilt rillllllllllilywilh 11111111 llMnl Mllll campnd 1D llllndllll1111111!'1'. Adclilionll rasiiiiCh is rtquired to lilclm tl1ll Cllll8.
Hilda Ill. . . laad
Camalil
Tabla , D. AYIIilabla Insulin Farmulatianslnsuln Type [trade nama) Dnsat
Peak
Duration
Type 211M: D1 ACCORD Trill Nf.JM2010; 362:1575-15 .... Rtl, urllinded wilh rlflllkMrilp. . . . - : 4,733 ]lltilrGMhtype 2dillbelis, rilk 11ctors r. Clnbllcui.-ICVI sysblic
d._,
Pnndilllbal111) i1sulinsRapid-acting insulin analogues Insulin IISpllrt (NovcRapid) Insulin lispro (Humalog) Insulin glulisine (Apidra) Short-iictilg insulins Humulin R Navolin Toronto Inhaled insulinBual insulils
llllrnnlan: IIIII' control Ins 1hm120 rmiig (inlllllillel 01140 ll'rilg lllllndardl.
10-15min 10-15min 10-15min 30 min 10-20min
1-1.5 h 1-2h 1-1.5 h 2-3h 2h
J-5 h h 3-5 h 6.5h 6h
l'riniiJ DID-. MlljofCV
IIIIIIIIIIIITjOCI!dial inlldon, nodllll . . . or
(c:unP11
a....: Mlln lllrm. rimllicllin 1111 ,_, flrin1an1Mtlmy Wl53.4 (95\ Cl, 3.4-3.51Z.I Z.l-2.2) flr ltlndltd thlapv-. Thill wa 1 signiiCI!It inCII!Ise in sllious ICNerse events il 11111 inllnlivl1lllllmlllt 11111 (3.3\ VI. 1.m p= especillly bnidyca Ill anvnil {0.5\\'1. 0.13%, p=0.0211111 hypurklllllil (0.4' -vs. D.04'- p=0.01]. Tllere WISIIO signlicllll lifnlce in plinuy in111e1wv lllJdv IIIIlS, Clllklllll mmllity. Thii'IWISIIigriCIId lllllcti1111 in lillY IIUa (O.m.lr w. 0.53\fyr, p-=0.01) ltld nonfml stroka incidlncll (o.mtyr "VI. 0.471t p=0.03)in the irensiw 1berlpy .,.,, .-..........: .._..siw BP lawllilgiD lasdllll 120 11111Hgvmus140 mrnHg in pllienls wilh Type 2DM ltld CV lilt factors doe$11011'81b:1 mljor Mil risk Telllctioo mile ewniJ.
lntennediatBcting Humulin N Navolin NPH Long-ilcting basal insulin analogues Insulin detanir (l..evemir) lnaulin (Lirrtus)
1-3h
5-Bh
Upto18h
90 min
Not applicable
Up to 24 h (glargine 24 h, detemir 16-24h)
Pre-mind i1sulinsPremixed regular insulin - NPH Humulin 30/70 Navolin 30,170, 40,160, 50/50 Premixed insLJin analogues Biphasic insulin aspart {NavoMix 30) Insulin lispnV!ispro protamine Humalog Mix25 and MixSO
cv
A single vial or cartridge contains a fixed ratio of insulin (%of rapid acting or short-ilcting ilsulin to% of intermediate-acting insulin)
Ellldlll C...bmln lipid n.np, il TWIZ DM: tl1ll ACCDID Trill NUf21110; 362118):15&3-74S1udy: IICT, dwblt-bhlld trill will14.7 yan II 11111111DIIawup. 5.511plllilrdlwilhlypl2dilb8tlll. . . . . . . Sllllinwilll orwillad fhtelhellpy. Mn.yo.a:.n.: MIP' Clldi-llr tcVI Mit norfml myocllllill imtiall.lllllillll staa, 01 CV-ftiUI dellll).M:ome between 111e two anns. No dillerence il
a111'111Cri11 irillt1ion, allllakl, ar d-CIIImcmlystudyanns.
Clncbiul: The illllilion oflinla U.rapyto slllin 1berlpr in plllienls wilh Type 211M does no1TIICIJcalllljarCVMWI!rilk.
E10 Endocrinology
Diaorders of Glucose Metabolism
Toronto Notes 2011
11,DPNVInhilllbln
Regular/Toronto
Nawar antihyparglycemic agents ttlllt inhibit 1t1e degradation of endogenous incratin honnon111 tika GIP-1 Stimulate insulin ucretion. ilhibitgluciiQCin rulaa1e from the p1111Cnllll
end delay gastric emptying
Bnaekfllst
Lunch
Dinner
Bed
Figure 5. Duration of Activity of Different lnsulins Insulin Regimens 1. Oral agent+ basal insulin (NPH, detem.ir, glargine) (Type 2 only) start with 10 units qhs, titrate up until FBG 28.0 mg/mmol (women) progression over 15 years to cause hypertension, persistent proteinuria (macroalbuminuria), nephrotic syndrome, and renal failure elevated HbA 1C is an independent risk factor for progression to microalbuminuria
Treatment and Prevention tight glycemic control tight blood pressure control (60 ml/min; ARB ifCrCl ml/min consider use of non-dihydropyridine calctum channel blocker (e.g. diltiazem) in those unable to tolerate both ACE inhibitors and ARBs limit use ofnephrotoxic drugs and dyes protein restriction (controversial) renal failure may necessitate hemodialysis and renal transplant
E14 Endocrinologyar.ctlofT..-...IorSV.... rA.,._.
Disorders of Glucose Metabolism
Toronto Notes 2011
DIABETIC NEUROPATHY (see Neurololn) N30) Epidemiology approximately 50% of patients within 10 years of onset of Type 1 DM and Type 2 DM
Dilllllic Nllraplthv: Sfstlnlic llniiW BMJ 2007; 335:87 l'llpole: To evaUII81ha afllctsoflrlllmlntsfor 111e panul dillbelic neuropathy. Slldy S.lll:lial: Randomillld conlrollld trials cornplriJrJ tD!icallv ijiplied 11111 cn1t ldmililtmed dru115 with piiiCibo illdulll wi1h painful dialic
Pathophysiology mechanism poorly understood acute cranial nerve palsies and diabetic amyotrophy are thought to be due to ischemic infarction of involved peripheral nerve the more common motor and sensory neuropathies are thought to be related to metabolic or osmotic toxicity secondary to increased sorbitol and/ or decreased myoinositol (possible mechanisms include accumulation of advanced glycation endproducts (AGE), oxidative stress, protein kinase C, nerve growth factor deficiency) can have peripheral sensory neuropathy, motor neuropathy, or autonomic neuropathy
llldE 25 reporls COII1JII8d 1111i1:011Wislnts antidlpralllnll 194), opilidsl329), ion chlnl blocbrsl1731 N-malllyiIJ.aparla1a antaQonist 1141 {aJS), capsaicin lnd isosorllide dilitrlle SJ111Y 1221 wi1h plallo. n. oddllllios in llrms of 511\ pail l1ilef were 5.33 {95\ cndenc:e inteiYII1.77m 16.021 fortnlditiOI'IIIricOINUislnts,l.n 1211 m4.66Hor newergenemon llltiCOIMMrts, and 222415.83 tD84.7SIIorlri:yicridapra.nts. Tha oddsllliol in 111mB afwi1hd11WBis ralatBd 1nlvarsa 11V8n!SWitl11.51 {0.33 tD &.96llor 1lldilionallllllicorWsants, Z.!1811.751D 5.071 for newer glll!ration lllllicorWsants, and 2.3210.59 tD 9J9Ifortrit'jlic lllllidlpraSIIIIII.Insuflicilnt dic:ho1urnous dill were Milllble to cali:UI1B 1he odds llliolfor ion clllnnlil bklckln. c:.dtlian: AnticonQanls 11111 llllidlepleS11n!S 119 stilthl most com marly Ulld options tD IIIBTIIQIIIilbltic !*lropathy. Drel bicyti: antidaprlsllnts and baditionlllllticonwlllnts 119 betlar for short llnnpllin 11iaflhln nawtr gener*nanliconvulslnts. E\lid.e ofllle big linn llld of 011ll1llilllprlauds 1111 antii:OIIWUrti isitilllctiiQ. Furthir iludias 119 naadad on opilids, ionciMinnelbklclra
neiJTOllldrf.
Screening 128 Hz tuning fork or 10 g monofilament at diagnosis and annually in people with Type 2 DM and after 5 years duration of Type 1 DM
Clinical FeaturesTabla 13. Clinical Pra1entlltian af DiabBiic NeuropathiesPeripheral SIIISCIIY NeuropillllyMutor Neuropllhy Less common than S!IISOIV neuropathy Delayed motor nerve conduction end 1111scle weaknew'atrophy May involve one nerve trunk {mononeuropathyl or more (rnononauritis Some of the motor neuropathies spontaneously resolve alter 6-8 wks Reversible CN palsies: Ill (ptosi!Vophthalmoplegia), VI (inability to laterally deviate eye), and VII (Bell's palsyl Diabetic amyotrophy: refers to pain, weakness, and wasting of hip ftexors or axblnsors
Aulllnomic NeuropathyPostural hypotension, tachycardia, decreased cil'diovascLJar mponse to Valsalva maneuver Gutroparesis 111d alternating diarrhea and constipation Urinary retention end erectile dysfunction
Plreslhesias itching I, niiUI'DpCithic pain, radicular pain, numbness. decreased lllc:lile sensationBilllllrlll and symmetric with decreased pm:eption of vibration and pairv' temperature; especially true i1 the lower extremities but may also be presiJ'II in the hands Decreased ankla rdex Symptoms may fim occur in anlnlpmunt syndromes e.g. Cllplll11111el, neuropathic ulceration of fuot
Treatment and Management tight glycemic control fur neuropathic pain syndromes: tricyclic antidepressants (e.g. amitriptyline), pregabalin, anti-epileptics (e.g. carbamazepine, gabapentin), and capsaicin foot care education Jobst fitted stocking and tilting ofhead ofbed may decrease symptoms oforthostatic hypotension treat gastroparesis with domperidone and/or metoclopramide (dopamine antagonists), erythromycin (stimulates motilin receptors) medical, mechanical and surgical treatment for erectile dysfunction (see U31)
Other ComplicationsDermatologic diabetic dermopathy: atrophic brown spots commonly in pretibial region known as "shin spots': secondary to increased glycosylation of tissue proteins or vasculopathy eruptive xanthomas secondary to increased triglycerides necrobiosis lipoidica diabeticorum: rare complication characterized by thinning skin over the shins allowing visualization of subcutaneous vessels
Bone and Joint Disease juvenile cheiroarthropathy: chronic stiffness of hand caused by contracture of skin over joints secondary to glycosylated collagen and other connective tissue proteins Dupuytren's contracture bone demineralization: bone density 10-20% below normal frozen shoulder
Cataracts subcapsular and senile cataracts secondary to glycosylated lens protein or increased sorbitol causing osmotic change and fibrosis
Infections see Infectious Diseases, ID23
Toronto Notes 2011
Diardera of Glucose Metabollsm/Obesity
Endocrinology E15
HypoglycemiaEtiology and Pathophysiology hypoglycemia o=s most frequently in people: with diabc:tc:s rc:cciving insulin or certain antihyperglycemic therapies (insulin secrc:tagogues) in people without diabc:tc:s, care: must be: taken to distinguish fasting from post-prandial hypoglycemia as each invokes separate differential diagnoses
....
,..----------------. ,iniD 1he
circulation when proinsulin is a-d1o insulin.
A short peptide
Tabla , 4. Common Causal of Hypoglycamia
....Rau:tinl
Fuling Hyparilsulinil11Exogenous insulin o Sulfonylurea reaction o Autoimmune hypoglycemia (autoantibodies to ilsulin or insulin receptorl o Pentamidine o Pancreatic beta cell1umour - insulinomao
,,
Wrthaut llyparillulinism o Severe hepatic dysfunction o Ctnrlic renal insufficiencyo
u.. C-pepdde Llnll t1l DiltinguisbAlimentay Functional pancreatogenous hypoglycemic syndrome o Occult diabetes Leucine sensitivity Heredibry fructose inllllerance o Galactosemia o Newborn infant of diabetic mothero
btltwwn Exllglna aNI Endapn-
Hypocortisolism
oo
Alcohol usetumours Imam error of carbohydrate metllbolism, glycogen stomge disease, gluconeogenic enzyme deficiency
So- of ltyperinsulinllllil Increased = endogenous DecraiiSIId or nolllllll = BXDgenous
.....
o
,.. ,
Clinical Features Whipple's triad1. serum glucose 1-1.5 em
Thyroid Malignancies see OtolaqniWif OT37
Adrenal CortexAdrenocorticotropin Hormone (ACTH) a polypeptide secreted in a pulsatile fashion from the anterior pituitary with diurnal variability (peak: 0200-0400; trough: 1800-2400} part of a prohormone (pro-opiomelanocorticotropin, POMC) which contains alpha, beta and gamma melanocyte-stimulating hormones, beta-endorphin and beta-lipotropin as well as ACTH secretion of ACfH regulated by corticotropin-releasing hormone (CRH) and arginine vasopressin stimulates growth of adrenal cortex and secretion of its hormones via cAMP stimulates release of glucocorticoids, androgens and, to a limited extent, mineralocortkoids some melanocyte stimulating activity..V blood glucose, trauma. infection,emo1ion. circadian rhythm
CNS3 weeks) primary adrenocortical tumours: adenoma and carcinoma (uncommon) bilateral adrenal nodular hyperplasia major depression and alcoholism
R32 EnclocrinoloBfClinical Features
1'oroDio
2011
Olllllaparusis
Thil arms and lags
i ...::1! Q
!
li
Clinitalleabns suspicious for hyparcortisolism
Normal
No Cushing'ssynchme
24 hall' urilarv free cortiecl
I
Low clos1 DST to CGIIfirm dillgnoei8
Diatrllllis Df Cushing'seslllbliNd
AC1ll ilci'88SIId
MRI piluiay, inf1rior pelluPI-.u. sampling with CRF Slinullltion t1ISt
+ IMeasure ACTH
+
I
AC1H dacnased
CT adnmal, cdrmatury high-don DST
11 HJ118rcartisollm: Algorithm for DiagalllilTreatment
adrenal
pituitary trans-sphenoidal resection, with glucocorticoid supplement peri- and post-operatively irradiation: oDly 5096 effective, with signlfica.nt risk of hypopituitarism adenoma: unilateral adrenalectomy (curative) carcinoma: palliative (frequent metastases, poor prognosis); adjunctive chemothempy often not useful medical treatment: mitotane, ketoconazole to reduce cortisol
ectopic ACI'H tumour - usually bronchogenic cancer (paraneaplastic syndrome) chemotherapy/radiation for primary tumour agents blocldDg adrenal steroid synthesis: metyrapone or ketoconazole poor prognosis
Toronto Notes 2011
Adrenal Cortex
Endocrinology E33
Congenital Adrenal Hyperplasia see Pediatrics. P32
HyperandrogenismDefinition state of having excessive secretion of adrenal androgens (DHEA, DHEA sulfate) Etiology and PathophysiologyTable 27. Etiology of HyperandrogenismConllituliaiiii/Famililll MediCitiiiiS Andragen.mediltedOnrilll
Famiy history, predisposing ethlic backQroundPremature adrenarche Anabolic steroids, ACTH, androgens, progestational agents
PCOS (see Gvneco!ogv. GY23) Ovarian hyperthecosisTheca eel tumoursPregnancy: placental sulfatase/110matase deficiency
Adrenal
Congenital alhnal hyperplasia (CAH. late-onset CAH) Tumours (adenoma, carcinoma) CUshing's disease - high ACTH
Hyperprolactinemia
Clinical Features Hirsutism male pattern growth of androgen-dependent terminal body hair in women: back, chest, upper abdomen, face, linea alba.... ' I
Vnilization masculinization: hirsutism, temporal balding, clitoral enlargement, deepening ofvoice, acne increase in musculature Defeminization loss of female secondary sex characteristics (ie. amenorrhea, .J,.o breast size, infertility) Males minimal effects on hair, muscle mass, etc. inhibition of gonadotropin secretion may cause reduction in testicular size, testicular testosterone production and spermatogenesis
T- Conditiona that do NOT llep...-.nt True Hir.utiun 1. Androgen-indipllndent hair(u.g.lllllllllahllirl
2. Drug-induced hyp811richosis (e.g. phenytoin, diazoldde, cyclosporine, minoxidil)
Investigations increased testosterone increased LH/FSH, commonly in PCOS >2.5 DHEA-S as measure of adrenal androgen production 17-OH progesterone is elevated in CAH due to 21-0H deficiency CT/MRI of adrenals (identify tumours) Treatment discontinue causative medications oral contraceptives (e.g. cyproterone acetate - blocks androgen receptor; found in Diane 35) spironolactone - acts as peripheral androgen antagonist cosmetic therapy low dose glucocorticoid mineralocorticoid if CAH suspected surgical resection of adrenal tumour
E34 Endocrinology
Adrenal Cortn:
Toronto Notes 2011
Adrenocortical InsufficiencyPRIMARY (ADDISON'S DISEASE)
Etiology Tabla 28. Etiology of Primary AdranocorticallnsufficiancyAIIIDimiiWII (71J.811%IIsolated alhnal insufficiency autoirrmune syndrume type I &II TB (7-ZO%IImost common in developing world I Fungal: histoplasmosis, paracoccidioidomycosis HIV;CMV Syphilis African trypanosomiasis Metastatic cancer (lung>stomach>esophagus>colon>breast); inlJhoma Sarcoidosis, amyloidosis, hemochromatosis Bilateral alhnal hemoll'hage Sepsis (meningococcal, Coagulopathy in adults or Waterhouse-Friderichsen syndrome in children Thronto&is, embolism, adranal infarctionDrugs
lnfaction
lnliltmin
lmibit coritsol: ketoconazole, megestrol acetate Increase cortisol mlllabolism: rifampin, phanytuin. barbitual8s, haptlin, coumadin AdranolaukDdy&trophy Congenital adrenal hypoplasia (ill1JIIired steroidgensisl Familial glucocorticoid deficiency or resisbmce
Others
autoimmune etiology most common in developed world antibodies often directed against adrenal enzymes and 3 zones of cortexSECONDARY ADRENOCORTICAL INSUFFICIENCY inadequate pituitary ACTH secretion multiple etiologies (see Hypopituitarism, El9}, including withdrawal of exogenous steroids that suppress pituitary ACTH production
Clinical Features Table 29. Clinical Features of Primary and Secondary Adrenal Insufficiency (All Primary AI (Addison's or Aclllll All Secandary AISkin IIIII mucou
Dark (palmar crease, axtensor surface!High Low PresentPrinary hypothyroidism, type 1 diabetes, vitiligo,
Pale
I'DiaaiumSodium Mtllbolic acidosis
Normal Normal or LowAbsent Central hypogonadism or hypothyroidism, growth honnone deficiency, diabetes insipidus. haadachas, visual NO hyperpigmll'llltion NO craving Glless common Low morning plasma ACTH Low 2hour ulfight plasma renin
Altociltld di-
neurological deficits
Altociltld sympblml
Weakness, fatigues, weight loss, hypotension, cmving, postural dizzinass, myalgia, arthralgia, Gl: nausea. vomiting, abdominal pain, dianhea High morning plasma ACTH High 2hour ulfight plasma l'l!lin
Diagnllltic test
Adaldfnlm: SalmrL R.JWA 21M;294:24812488.
Treatment acute condition- can be life-threatening IVNS or D5W/NS in large volumes (2-3 L) hydrocortisone 100 mg IV q6-8h for 24h, then gradual tapering identify and correct precipitating factors maintenance hydrocortisone 15-20 mg PO qam and 5-10 mg qpm (4:00pm) Florinet- (fludrocortisone, synthetic mineralocorticoid) 0.05-0.2 mg PO daily if mineralocorticoid deficient (maintain renin between 1-3 nglml/hr) increase dose of steroids 2-3 fold for a few days during moderate-severe illness (vomiting, fever) major stress (surgery, trauma) requires 150-300 hydrocortisone IV daily divided into 3 doses medical alert bracelet and instructions for emergency hydrocortisone 1M injection
Toronto Notes 2011
Adrenal Medulla
Endocrinology E35
Adrenal MedullaCatecholamine Metabolism catecholamines are synthesized from tyrosine in postganglionic sympathetic nerves and chromaffin cells of adrenal medulla predominant adrenal catecholamine = epinephrine (adrenaline) predominant peripheral catecholamine = norepinephrine (noradrenaline)ABC Gf Adranall1111Adrenaline activatas 181&-rvceplor$, increasing Cyclic AMP
PheochromocytomaDefinition rare catecholamine secreting tumour derived from chromaffin cells of the sympathetic system Epidemiology most commonly a single tumour of adrenal medulla 10% extra-adrenal (95% of which are intra-abdominal), 10% multiple tumours, 10% malignant, 10% familial rare cause of hypertension (6.51!1D.ol/day (1.2 mg/day) plasma catecholamines >2000 pg/ml (11.8 mmol/L) diagnostic >950 pg/ml (5.6 mmol/L) suggestive; proceed to clonidine suppression test (rarely done) elevated plasma epinephrine unsuppressed by clonidine {central alpha-adrenergic) is diagnostic CTabdomen ifCT is negative, meta-iodo-benzoguanidine (MIBG) scintigraphy, Octreoscan, or MRl may be helpful Treatment adequate pre-operative preparation alpha-blockade for BP control- phenoxybenzamine (14-21 days pre-operative), IV phentolamine {peri-operative) beta-blockade for HR control- propranolol (initiate only after adequate alpha-blockade) metyrosine (catecholamine synthesis inhibitor)+ phenoxybenzamine or prazosin volume restoration with vigorous salt-loading surgical removal oftumour with careful pre-operative and post-operative ICU monitoring rescreen urine one month post-operatively
Episodic swemq
Classic TriM Gf PHbchrDmocytDma Palpitations H81ld11Cha
E36 Endocrinology
Adrenal Medulla
Toronto Notes 2011
Multiple Endocrine Neoplasm (MEN)
----------------------
neoplastic syndromes involving multiple endocrine glands tumours of neuroectodermal origin autosomal dominant inheritance with variable penetrance genetic screening for RET proto-oncogene on chromosome 10 has long-term benefit early cure and prevention of medullary thyroid cancer
T1ble 38. MEN ClusificltionType MENIMEN 1- W...mBr'l Syndrom1 Affldl 111131'11
Chnunosamelmpll:llled11
TIDUIIIIMIIVIdPituillly
Clinicll MMifeslltionsAnt pituilllry adenoma, Dillin non-saCI'IIing but may SBCI'IIa GH md PRLPrimary hyperparathyroidism from hyperplasia Pancreatic islet cell tumours Gastrinoma (peptic ulcers) lnsulinomas (hypoglycemia) VIPomas (secretory diarrhea)
Wenn11r'1 SyndromB (P'fGM gena)Pituitaryl'llllllhyroid l'llncrtlllll
Parathyroid Entero-pmcreatic endocrine
MEN II 3 Distinct Syndl'lllllel
1D
(RET pruto-oncogane)Thyroid Adrenal mellllla Parathyroid Skin Thyroid Medullary 1hyroid CIIICer (MIC) ( >911%) Pheochromocytoma (41}.511%) 1 parathyroid hyperplasia (11}.211%) Cullllaous lichen amyloidosis
1. lla Sipple's SJndromB
2. FamilialThyroid Ca. (a variall: of lla)3.11b
MTC without o1hw clinical manifastations of MEN llaorllb MTC: most common more aggressive and earlier onset than MEN llaPheochromocytoma Mucosal neuroma, intestinal ganglioneuromas Marlanoid habitus {no aortic Chrmic constipation Megacolon
Thyroid
Adrenal mellllla
NeuronsMSK
Gl
History MENI symptoms of hyperparathyroidism, gastrinoma (abdominal pain, diarrhea, peptic ulcer disease), and insulinoma MENII family history of MEN syndromes symptoms related to medullary thyroid cancer (MTC), hyperparathyroidism, or pheochromocytoma scaly skin rash (cutaneous lichen amyloidosis in MEN IIa)
Clinical Features clinical picture depends on the endocrine organs involved and the hormones secreted MENI hyperparathyroidism - nephrolithiasis, bone abnormalities, MSK complaints generalized weakness, and alterations of mental status in severe hypercalcemia gastrinoma - upper abdominal pain due to peptic ulcers and esophagitis glucagonoma - rash, anorexia, anemia, diarrhea, glossitis pituitary tumour- headache, visual-field defects, prolactinoma (erectile dysfunction, decreased libido, amenorrhea, galactorrhea), acromegaly carcinoid syndrome - flushing, diarrhea. bronchospasm MEN II - physical signs are variable and often subtle MTC - neck mass or thyroid nodule; non-tender, anterior neck lymph nodes pheochromocytoma - elevated BP and HR
Toronto Notes 2011
Adrenal MedullaJCalclwn Homeostaaia
Endocrinology E37
Investigations MENI laboratory gastrinoma- elevated serum gastrin level (>200 ng/mL) after IV injection of secretin insulinoma - reduced fasting blood glucose (hypoglycemia) glucagonoma - elevated blood glucose and glucagon levels pituitary tumours - assess GH and prolactin levels hyperparathyroidism - PTH levels; bone density scan (DEXA) imaging MRI for pituitary tumours, gastrinoma, insulinoma MENII laboratory genetic screening for RET mutations in all index patients - if a mutation is identified, screen family members who are at risk calcitonin levels, urine catecltolamines, vanillylmandelic acid and metanephrine screen (pheocltromocytoma); serum Ca and PTH levels (hyperparathyroidism) pentagastrin calcium stimulation test if calcitonin level is within reference range imaging CT or MRI for imaging of the adrenal glands metaiodobenzylguanidine (MIBG) scan for pheocltromocytoma radionuclide scanning for determining the extent of metastasis octreoscan for examining the spread of MTC FNA for thyroid nodules Treatment MENI surgery is indicated for hyperparathyroidism, insulinoma, glucagonoma, pituitary tumours (trans-sphenoidal approach with external radiation when medical treatment fails) proton pump inhibitor (PPI) for acid hypersecretion in gastrinoma bromocriptine or other dopamine agonists to suppress prolactin secretion somatostatin for symptomatic carcinoid tumours MENII surgery for MEN Ila pre-operative treatment prostaglandin inhibitors to alleviate diarrhea associated with thyroid cancer alpha-blocker for at least 2 weeks for pheocltromocytoma hydration for hypercalcemia - if remains severely hypercalcemic, consider calcitonin or bisphosphonates post-operative treatment hormone replacement following total thyroidectomy and bilateral adrenalectomy calcium supplement and/or vitamin D for post-op hypoparathyroidism
Calcium Homeostasis normal total serum Ca: 2.25-2.62 mmoVL (9.0-10.5 mg/dL) ionidfree Ca levels: 1.15-1.31 mmoVL {4.6-5.25 mg/dL) serum Ca is about 50% protein bound (mostly albumin) regulated mainly by two factors: parathyroid hormone (PTH) and vitamin D actions mainly on 3 organs: GI tract, bone, and kidney
Parathyroid Hormone (PTH) secretion increased by low serum Ca and inhibited by cltronic, low serum Mg not influenced directly by P04 (except by P04 effect on the ionic calcium levels)
E38 Endocrinology
Calcium HomeostasisCl'
Toronto Notes 2011IN light I
I
1' Pili IBona
1' Osteoclast activity 1' Resorption.. Rel81lSe of Cl and P04
.
1.
I
Mg [acute)
Cho!aca!ciferol
Kidnay
Ca and Mg reabsorption
;
+ +--------
25 [DH) vit D(liver]
.I
Diat
I
PO,axcrlllon in urine and renal tub!Jar reabsorption
.. Cllcilriol formation
24, 25 [OH,] vit D (inert!
+
o!PO,
1' Boneresorption
Bone ostaoclast
1' Gl Ca and P04absorption
1
Kidnay Cl and PO, axcration
1' Cland HP04 ra!81lSaNat Effect
1' ECF Ca, 1fd D ECF phosphate
Figura 14. Parathyroid Hormone IPTHI Regulation
Vitamin D necessary for Ca and P04 absorption from GI tract cholecalciferol formed in the skin by the action of UV light Calcitonin polypeptide secreted by thyroid C cells secretion enhanced by Ca, GI hormones, pentagastrin major actions ..V osteoclastic bone resorption (pharmacological effect) 1' renal P04 and Na clearance acute net effect: ..V serum Ca when given in pharmacologic doses Magnesium major intracellular divalent cation Ca is reabsorbed from the kidney with Mg thus Ca balance is difficult to maintain in Mg deficiency Phosphorus intracellular cation found in all tissues and necessary for most biochemical processes as well as bone formationTabla 31. Summary of EffactsNat Effect
Paraflrwroid Honnona (Pill)
....
,fonn, e.g. hyperalbuminemiadahydnnion.UVII1I
Vit DDecreased PO, Increased Ca Increased P04 Decreased Ca
VbmiiD
increased proiBin binding IHding tu an elsvation in serum total Ca without a rise in lhe from
....
Correctlld Ca {mmoK.) = musurad Ca + 0.02 {40- umln)
}-----------------, total corrected serum Ca >2.62 mmol/L (10.5 mg/dL) OR ionized Ca >1.35 mmol/L (5.4 mgldL)Approach to Hypercalcemia (Figure 15) 1. Is the patient hypercalcemic? (correct fur albumin- see sidebar) 2. Is the PTH high/normal or low? 3. If PTH is low, is phosphate high/normal or low? If phosphate is high/normal are the level of vitamin D metabolites high or low?
,
HypercalcemiaDefinition
For 8WfV' dacruM in albumin by 10, inCNIM in Ca bf O.Z llanip (less likely mlllignantl: Ca IKI ITIIJ) Gluplll t rilk ct gdl1une lormm mbined with Dtins Abnonnlll M! enzymes Pnnilus IGT
BilucidsecJieslrwits
lb!sllln' PrMiite8
2-24 Wday 5-30 ll'dar 10mWday
Used for tlJJL Use as adjunct with slllins orfilntes Used for 1' B
Compllla lillry Dllslnl:liln Pl!gnancy, lactation TG>:Dll111tdl Girdilydillllle! lf\1leBensiMty
CCIIstiJD:In Nau Ra1ulellce
Cholesterolllbsorptiorr mililol$
ld
Hepatic dysfurctiorr Donlmbinel'lilbfiln111s cr bile acichtsils
Ph.,..
ii8
SiJ.Jilis Abdomilllll pail Diant. ArdntJja
Thyroid Medicationsin1CIIM llechmill al AdiDn llecl!llses thyroid h111111D1'11 pruductilrl by inlii!iv ioclne arrd pe!Ullidase from intmc1DJ NtllSIIIR: Drq Nlllla prtVI!thilllllcil (PIU)Cnd1NI111US Nil
t ..
II.....,
IRaS1mt 100q PO til,
Pftvii.TlTjmcil" llpllDie'
......
Hypl!lttrjni:lism
Also intern with CCIMniDnliT41oTl
than adjuslacCOidiljf Thyroid sbrm: sblrt 200ll0 PO qid, then adjuslS1mt 520 11'41 PO OD, than adjuslacCO!d'Dif 0.05-2.01111tday. ilet:lerlypMis sblrt It 0.1125 mWdar
Hypenmitivity Rellli8: liJ'IIIIiliUa, Mr disease
SiiiiEII'actl Nuea.wmilirG !lash , !Wg-im:ed hepds AwallhyiDsis
methimllmle !MMI) IIMIIIr,Toxine 14hyale Syulhroid' levollroid1levalyl.
Pregnancy, lacll1iDn
lle!Jetitis Symptams oflrypartlr,U:iillll
Tlryroidllmlne
'Hypotbyroilsm
Recall
thymtaxi:Diis
tMiltnil'
Angine lfype!lhennia
a
llanbea
lnsonliia TralllDTS Muscle Wlllness
... ...
f
Metabolic Bone Disease Medicationsin1CIIillllidlllilm" Aciln
&enalc lftg
CllllllNne
us Nln llllflnll
o.q5-10q00 70 40 OD fur 6nmlls
Bisphasplnlas
Wiibits asl8ocllsl mediated bona morpliCII
alandranata
fGrrlxll
lrdCIIIianl Plwantian of poslmeTqlual asllqiorUiil TNIIment li osllopOTDis GUaJcmticcilirdJCl!d DSII!OJOOSis Paget's disease T_.llld prewntion li postrnllllpual OilaapJiulia TNIIment llld prevention li ;.r:OCOI1ic:oidinduc:ed osteopOIOSis Paget's disalse
Cllllb'lildicllia
stricbn IJacllllasia Ullllllla 1D stand ar uprijll fur >:II min lOIII) lt,1lersensitivity lfypocak:tJria H11111l inufic:imqr
Sidellln GI MSKpain Headache Osmieaasisofthej&W
J... ...C)
f
TiseDal8
AclonePI
5mgOD 35 mgooceW&Bklt 150 q CIICe :11 mwODfur2 nm11s 5-10 q/lg0Dx611Dl!hs
etilranate
DidranePI
illmlnma1epamidronale
Aralia'
2.5 mg 00 or ISO q rn:e IV
ZDielarlle
Zornell' AciiiSII1
5mg IV once yeqIV
llec:e!D
Salec:live Eflragan
Dacreues rasorplirl ci hone lhrough binding 1D es1nQ!n receplln
llloxiane
Osteoporosis disaasa PrMntilllllld trelbn!nt li helm! pic osific:aliln llfmri!DI hip replllc:ellll!lt or spinaiCI:td iiVf TNIIment llld prevention li postrnllllpual OilaapJiulia (US onlyl Hypercalcemia of mlli]nmy Paget's disalse Osteolytic 1m 1IDslllses of iRist Osteolytic lesions of multiple Rfiekml TNIIment li osllopOTDsis Hypercalcemia of mlli]nmy T_.llld prewntion lisblnl amplications r8latad 1D cancer T_.llld prewntion li ]XIStmempual OilaapJiulia (2nd line!
I lictltDD l'rlgnmy Active or past lislmy of 1M; PE or retinal 1lrontosis IICJtftubes leg cramps riskoflallll
I
sblte,wnous
Calci1Dril
Wiibits asl8ocllsl mediated hone morpliCII
&Umin
t.lalc:in'
Ona ifRY 1200 lJ) par day, allnlting
T_.lipomanopauiil asllqlorulil, tlln 5years]XIStmempiiiSe
Clini!;lllallergy ID
I'IH
oStii1JIIIesnewbone fonnation by plifarantia stindation at DIIBoblastic activityiMI'osll!oclastic activity
1a'pralide
Fno'
201111SCOD X1824 months
Trnlment li poslmenopauiil Wlli1WII with ostBoporosis IWMI ara Trnlment limen with prinary or l?jpogonadal IWM!ara
ol'lget's disease PrD axllmal baam or implut radim lhnpy iMmng the skllabm oBone metastases Metabole bone diseases all1111hen ostaoporosis
lhrornboilrriiolilm Rhinitis Episluis oSirusitis oNnal dlynea oOOoslatic hypolension Hypmtemia ollllilns leg cramps
!!!!
III>
e1
Metabolic Bone Disease Medications (continued)lkugCI&IICalcium Mechlnilm of Action Inhibits P1H secretion
Generic D11111 Nme
CIIIIIIIName
US Name flf dffnnt)
Doling 1500 IIIWdav {including diet) Divide il3 doses
Indications
CIIIIIRildicati Caution renal stones
SideEfhc:aVomiting Constipation Dry mouth Hypercalcemia Headache Nausaa, vomiting Constipation
Dsteopenia Osteoporosis Prevention Ill melllbolic bone disease
VrtaminD
Regulation Ill calciLIIl and phosphata homaostasis
cholecaldfercl {vitaminll3) argocalcnerol {vitaminll2) Ostaoforte'
BOO IU/day
Dsteopenia Ostaoporosis Prevention Ill mBIIIbolic bone disease
Caution in patients an digDXin (risk Ill hypercalcemia may pracipilllte anhythmia) Hypercalcemia Malabsorption syndrome Decreased renal function Hypercalcemia Vrtamin Dtoxicity
lii8
r
m
50000 IU
Osteoporosis in patients with liverdyslunction. reh'aelllry ricksts, hypopnthyroidism
cak:itriol {1,25{0H}z-D)
Rocllltrol1 Calcijex'
SWt 0.251!Wday Trlnlt8 up by 0.25 I!Wdey at 4-8 week intervals to0.5-1 I!Wday
Hypocalcemia and ostaodyslrophy in patient8 with chronic renal failureondiaysis
SWt 0.251!Wday Trtrate up by 0.251!Wdey at 2-4 week intervals to 0.5-2 I!Wday
Hypoplllllhyroidism
I Adrenal MedicationslkugCI&IIHydrocortisone Minalocorlicoid Generic DRill Name Potency {relative Activity to Cortillll) Yes Cortef Solu-Cortef 1.0 EA,Iivalont Dole{mg) 20 Duration of Action (t 1/2 in hour.)
DosingAd!ll!al Crisis: 100 mg IV bolus, then 100 mg q 8hr (continuous infusion x 24-48 hr) PO once stable (50 mg q Bhr x 48 hrs, 1hen taper over 14 d) 20-30 mg PO OD (213 AM, 1/3 PM) Adrenal Crisis: 25-300 m{V'd PO/IM divided q12-24 hr Adrenal Crisis: 5-60 mg/d PO qd or divided Bill/OlD
Commentl In high doses, mineralocorticoid side effects may emel'lle &Bit + water retantion, ECF volume axpansion. HTN, low K metabolic alkalosis) Pro-drug which is converted to active funn as hydrocortisone High doses can result in mileralocorticoid side effects (sae above) Pro-drug which is converted to active funn as prednisolone Used for undiagnosed adrenal insufficiency {won1 iltelfere with serum cortisol levels)
t
8
Cortisone aceblle Prednisone Dexamathasone
YesNo No
Cortone Acetate
0.83.5
25 6 0.7
oral= 8 IM=18+ 16-36 36-54
Deltasane LicJiid Pr8dDecadron AK-Dex Dexone
30
Adrenal Crisis: 4 mg IV; repeat q2-6 hr necessary
n
r... ...
f
Toronto Notes 2011
Landmark Endocrinology Trials
Endocrinology E55
Landmark Endocrinology TrialsTrilllllfii'IIICI
DIABETESDCCTUICPOS EDIC
NEJM 1993; 329:977-86I.JJncst , 998; 352:837-53
lnl!nsive blood gklcose control delayed the onset end llllllced the IJIIgression of microvascular complications (retinopathy, nephropathy and neurapathyl in Type 1 OM lnllllsiw blood gklcosa control11illces microvascular, but not macrowscular complications i1 Type 2 OM Compared with conventional therapy, intensive dabetes therapy (goal HbA1C