9 To void or not to void 4 FINAL - The University of …kappatau/images/9Meisterling.pdf · Heather...
12
11/16/2013 1 Sheramy Vandernat RN BSN ANM Aimee Wilson RN BSN CPAN Marilyn Evans RN CPAN Marilyn Evans RN CPAN Heather Meisterling RN BSN Objectives & Overview Scope of the problem Literature search Survey tool and algorithm Results Conclusions Conclusions References Q&A
Transcript of 9 To void or not to void 4 FINAL - The University of …kappatau/images/9Meisterling.pdf · Heather...
11/16/2013
1
Sheramy Vandernat RN BSN ANM
Aimee Wilson RN BSN CPAN
Marilyn Evans RN CPANMarilyn Evans RN CPAN
Heather Meisterling RN BSN
Objectives & Overview
Scope of the problem
Literature search
Survey tool and algorithm
Results
Conclusions Conclusions
References
Q & A

11/16/2013
2
Why POUR? Varying hospital to Posty g phospital practice
Inconsistent MD orders
Inconsistent nursing practice within our unit
PACU space is expensive and health care cost
Post
Operative
Urinaryand health care cost containment is prudent
OR flow dynamics
Patient satisfaction considerations
Urinary
Retention

11/16/2013
3
What is POUR?
Inability to void in spite of a
bladder volume > 600 mls
What were our goals?
To assess the risk factors for POUR
To develop a tool to standardize nursing care in the PACU
To evaluate the usefulness of developed tool

11/16/2013
4
Evidence Based Practice InquiryThe Johns Hopkins Nursing Evidence Based The Johns Hopkins Nursing Evidence Based
Practice Model
Methods

11/16/2013
5
6
5
Primary Literature
Randomized Controlled Trial
Quasi‐experimental
1
p
Non‐experimental
Qualitative
Non‐research
23
Quality Rating
Number of sources
High (A) 1
Good (B) 12
Low (C) 3

11/16/2013
6
Goal 1:
Influential FactorsType of Surgery History of Urinary Type of Surgery Highest Risk
Anorectal (25‐50% increased risk)
Hernia/Pelvic (5‐26% increased risk)
Urology
History of Urinary Retention POUR
Urinary hesitancy
Incontinence surgeries
Moderate Risk
GYN (4% increased risk)
Low Risk
All other surgeries
Influential Factors continuedType of Anesthesia IV FluidsType of Anesthesia
Spinal
Low dose/short acting (Chloroprocaine) vs. high dose/long acting (all others)
Intrathecal narcotic
General
IV Fluids>1200 cc intraoperative
>500 cc PACU
Increased IVF does not appear to hasten voiding, but instead increases bladder volume and
Lower risk than spinal anesthesia
> 120 minutes of GA increases risk
increases bladder volume and may make retention more likely

11/16/2013
7
Influential Factors continued
C bidi iComorbidities
Benign prostatic hypertrophy
Prostate disease
Neurological disorders
Diabetic neuropathy Pain
d h• Increased sympathetic tone increased risk of POUR
Influential Factors continuedAgeN ti Age
>50 years
Sex
M=F
Narcotics
• Escalating dosing of narcotics leads to higher likelihood of POUR
• Intrathecal narcotics

11/16/2013
8
Goal 2:
The ToolType of Surgery
4 = High Risk (anorectal, hernia/pelvic, urology)
2 = Moderate Risk (gyn)
Pain
1= Not‐tolerable
0 = Tolerable2 = Moderate Risk (gyn)0 = Low Risk
History of Urinary Retention 2 = Yes 0 = No
Spinal Administration 2 = Long acting spinal1 = Short acting spinal0 = No spinal
Fluid Administration
1= >1200cc intraop
0 = <1200 cc intraop
Comorbidities
1 = Present (BPH, DM, neuro)
0 = None present0 No spinal
Length of General Anesthesia 1 = >120 minutes0 = < 120 minutes
Age1 = >500 = <50
Narcotic Administration
2 = Escalating doses
1 = Minimal narcotics
0 = No narcotic
Total Score = 0 ‐ 15
Low Risk :score 0‐3
Void?Yes d/c
N d/c with No d/c with instructions
11/16/2013
9
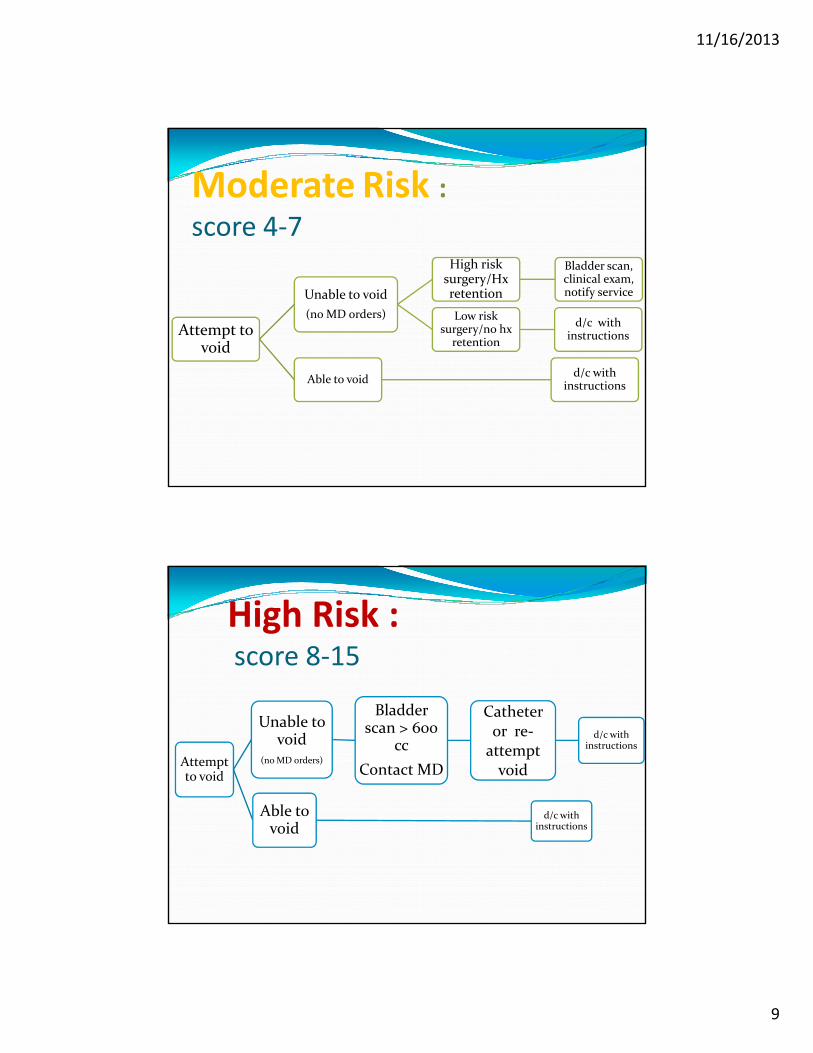
Moderate Risk :score 4‐7
Attempt to void
Unable to void
(no MD orders)
High risk surgery/Hx retention
Bladder scan, clinical exam, notify service
Low risk surgery/no hx
retention
d/c with instructions
Able to voidd/c with
instructions
High Risk :score 8‐15
Attempt to void
Unable to void
(no MD orders)
Bladder scan > 600
cc
Contact MD
Catheter or re‐attempt void
d/c with instructions
blAble to void
d/c with instructions
11/16/2013
10
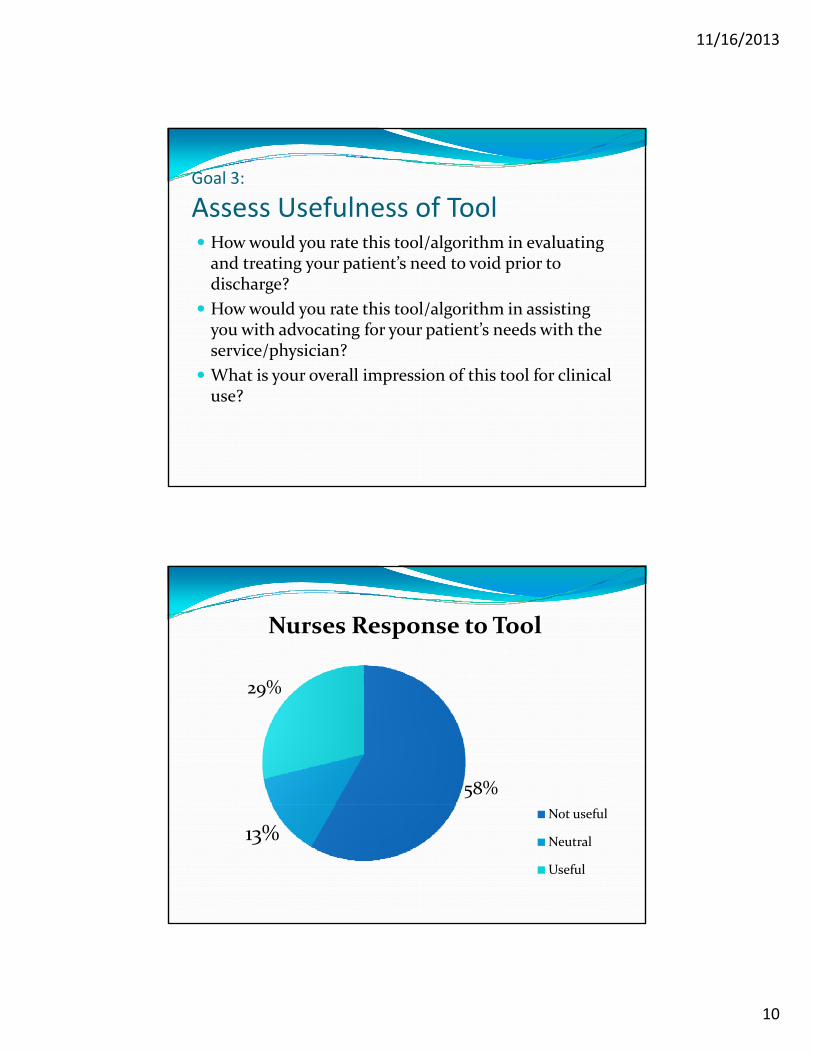
Goal 3:
Assess Usefulness of Tool How would you rate this tool/algorithm in evaluating How would you rate this tool/algorithm in evaluating and treating your patient’s need to void prior to discharge?
How would you rate this tool/algorithm in assisting you with advocating for your patient’s needs with the service/physician?
What is your overall impression of this tool for clinical use?
29%
Nurses Response to Tool
58%
29%
13%Not useful
Neutral
Useful

11/16/2013
11
How has our PACU practice evolved? Staff education
Add d h h EHR id di h Added smart phrases to the EHR to guide discharge teaching
Most of our patients are low risk for POUR
Effective screening tool to capture high risk POUR patients
W h th d d i t t (bl dd We have the recommended instrument (bladder scanner) to help diagnose POUR
Nurses empowered to advocate for patients as it relates to POUR and ambulatory surgery discharge

11/16/2013
12
ReferencesMulroy, Michael, Francis Salinas, et al. "Ambulatory patients may be discharged before voiding after short-
acting spinal and eidural anesthesia." Anesthesiology. 97.2 (2002). Print.
Pavlin, D. Janet, Edward Pavlin, et al. "Management of bladder function after outpatient surgery." Anesthesiology. 91.1 (1999): 42-51. Print.
Luger, Thomas, Ivo Garoscio, et al. "Management of temporary urinary retention after arthroscopic knee surgery in low-dose spinal anesthesia: development of a simple algorithm." Archives of Orthopedic Trauma Surgery. 128. (2008): 607-612. Print.
Orbey, B.C., Z. Alanoglu, et al. "Do we still need to restrict preoperative fluid administration in ambulatory anorectal surgery under spinal anaesthesia?." Techniques in Coloproctology. 13. (2009): 35-40. Print.
Voelckel, Wolfgang, Lukas Kirchmair, et al. "Unilateral anesthesia does not affect the incidence of urinary retention after low-dose spinal anesthesia for knee surgery." International Anesthesia Research Society. 109.3 (2009): 986-987. Print.
Gudaityte, jurate, Irena Marchertiene, et al. "Low-dose spinal hperbaric bupivicaine for adult anorectal surgery: a double-blinded, randomized, controlled study." Journa of Clinical Anesthesia. 21. (2009): 474-481. Print.
Lin, Yu-Hua, Kuang-Wen Liu, et al. "Haemorrhoidectomy: prevalence and risk factors of urine retention among post recipients." Journal of Clinical Nursing. 19. (2009): 2771-76. Print.
Toyonaga, Takayuki, Makoto Matsushima, et al. "Postoperative urinary retention after surgery for benign anorectal disease: potential risk factors and strategy for prevention." International Journal of ColorectaDisease. 21. (2006): 676-82. Print.
Wohlrab, Kyole, Elizabeth Erekson, et al. "The association between regional anesthesia and acute postoperative urinary retention in women undergoing outpatient midurethral sling procedures." American Journal of Obstetrics & Gynecology. 200.571 (2009). Print.
Ruhl, Maureen. "Postoperative voiding criteria for ambulatory surgery patients." AORN Journal. 89.5 (2009): 871-4. Print.
Darrah, Daniela, Tomas Griebling, and Jeffrey Silverstein. "Post operative urinary retention." Anesthesiology Clin. 27. (2009): 465-484. Print.
Mulroy, Michael. "Outpatients do not need to void after short neuraxial blocks." Anesthesiology. 111.6 (2009): n. page Printpage. Print.
Feliciano, Terry, Jo Montero, et al. "A retrospective, descriptive, exploratory study evaluating incidence of postoperative urinary retention after spinal anesthesia and its effect on PACU discharge." Journal of Perianesthesia Nursing. 23.6 (2008): 394-400. Print.
Shadle, Benjamin, and Casey Barbaro. "Predictors of postoperative urinary retention." Presented at the 20th Annual Scientific Meeting of the Southern CA Chapter of the American College of Surgeons. (2009):. Print.
Cetinel, Bulent, and Okaty Demirkesen. "Risk factors influencing the complication rates of tension-free vaginal tape-type procedures." Current Opinions in Obstetrics abd Gynecology. 17. (2005): 530-34. Print.
Gehrich, Alan, John Aseff, et al. "Chronic urinary retention and pelvic floor hypertonicity after surgery for endometriosis: A case series." American Journal of Obstetrics & Gynecology. 193. (2005): 2133-7. Print.
Baldini, Gabriele, Hema Bagry, et al. "Postoperative Urinary Retention, Anesthetic and PerioperativeConsiderations." Anesthesiology. 110. (2009): 1139-57. Print.
Chaney Mark "Side effects of intrathecal and epidural opioids " Canadian Journal of Anesthesiology 42 10Chaney, Mark. Side effects of intrathecal and epidural opioids. Canadian Journal of Anesthesiology. 42.10 (1995): 891-903. Print.
Malinovsky, J.M., L. Le Normand, et al. "The urodynamic effects of intravenous opioids and ketoprofen in humans." Anesthesia and Analgesia. 87. (1998): 456-61. Print.
ASPAN American Society of Perianesthesia Nurses. N.p.. Web. May 2013. <http://www.aspan.org/Clinical-Practice/FAQs>.
Rosow, CE, P Gomery, et al. "Reversal of opioid-induced bladder dysfunction by intravenous naloxone and methylnaltrexone." Clinical Pharmacology and Therapeutics. 82.1 (2007): 48-53. Print.