
9 stephen mulligan
57
STEPHEN MULLIGAN, MD University of Sydney, Australia Professor, Department of Hematology, University of Sydney, Australia Dr. Mulligan is the founding Chair of the CLL Global Consortium in Australia. He is also the director of the Ruffle Pathology and Hematology Program of the Institute of Molecular Biology Science, the School of University of Sydney, and the founder and president of the Chronic Lymphocytic Leukemia Australian Research Consortium (CLLARC). Besides, he is a Fellow of the Royal Australian College of Physicians (FRACP) as well as one of the Royal College of Pathologists of Australia (FRCPA). Professor Mulligan’s research interests include the mechanism of action of purine nucleoside analogues, the ATM/p53 pathway and molecular mechanisms of resistance, signaling pathway inhibitors in CLL, the incidence and nature of small B-cell clones, and all aspects of clinical and experimental CLL.
Transcript of 9 stephen mulligan

STEPHEN MULLIGAN, MD
University of Sydney, Australia
Professor, Department of Hematology, University of Sydney,
Australia
Dr. Mulligan is the founding Chair of the CLL Global Consortium in
Australia. He is also the director of the Ruffle Pathology and
Hematology Program of the Institute of Molecular Biology
Science, the School of University of Sydney, and the founder and
president of the Chronic Lymphocytic Leukemia Australian
Research Consortium (CLLARC). Besides, he is a Fellow of the
Royal Australian College of Physicians (FRACP) as well as one of
the Royal College of Pathologists of Australia (FRCPA). Professor
Mulligan’s research interests include the mechanism of action of
purine nucleoside analogues, the ATM/p53 pathway and molecular
mechanisms of resistance, signaling pathway inhibitors in CLL, the
incidence and nature of small B-cell clones, and all aspects of
clinical and experimental CLL.
Breakthroughs in
Chronic Lymphocytic Leukaemia
2014 - 2015
Stephen Mulligan MB BS (Hons), Ph.D., FRACP, FRCPA
Royal North Shore Hospital, Sydney
Kolling Institute and University of Sydney
Laverty Pathology NSW, Sydney
CLL ARC
Australian
Research
Consortium
APHCON / BTG 2015, Beijing, 1st February, 2015

“Triple Revolution” in CLL:
1. “Immunochemotherapy [FCR] Revolution”
Median PFS extended from ~20 to 57 months
Median Time to 2nd Treatment almost a decade
- Still in progress …
2. “Molecular Revolution”
TP53, Notch-1, SF3B1, BRIC3
Key molecular lesions of CLL disease progression
3. “Non-genotoxic Novel Therapy Revolution”
B-cell receptor inhibitors, bcl-2 inhibitor, novel monoclonal antibodies

Breakthroughs in CLL 2014 (15)
1. FCR > BR
2. FCR in Fit Elderly
3. Obtinutuzumab + Cbl for comorbid CLL
4. Notch-1 – no benefit from rituximab over FC
5. Idelalisib + Rituximab in R/R CLL
6. Ibrutinib in R/R CLL
7. Ibrutinib resistance mechanisms
8. Double and triple BCR signal molecule inhibitors
9. Abt-199 / venetoclax – TLS resolved, MRD-negativity
10. PD-L1 / PD-1 in CLL
FRONTLINE CHEMOIMMUNOTHERAPY WITH
FLUDARABINE (F), CYCLOPHOSPHAMIDE (C), AND
RITUXIMAB (R) (FCR) SHOWS SUPERIOR EFFICACY IN
COMPARISON TO BENDAMUSTINE (B) AND RITUXIMAB
(BR) IN PREVIOUSLY UNTREATED AND PHYSICALLY FIT
PATIENTS (PTS) WITH ADVANCED CHRONIC
LYMPHOCYTIC LEUKEMIA (CLL):
FINAL ANALYSIS OF AN INTERNATIONAL, RANDOMIZED
STUDY OF THE GERMAN CLL STUDY GROUP (GCLLSG)
(CLL10 STUDY)
56th ASH Annual Meeting San Francisco, December, 2014
Eichhorst B, Fink A-M, Busch R, Kovac G, Maurer C, Lange E, Köppler H, Kiehl
M, Sökler M, Schlag R, Vehling-Kaiser U, Köchling G, Plöger C, Gregor M,
Plesner T, Trneny M, Fischer K, Döhner H, Kneba M, Wendtner C-M, Klapper
W, Kreuzer K-A, Stilgenbauer S, Boettcher S, Hallek M on behalf of an
international group of investigators and of the CLLSG
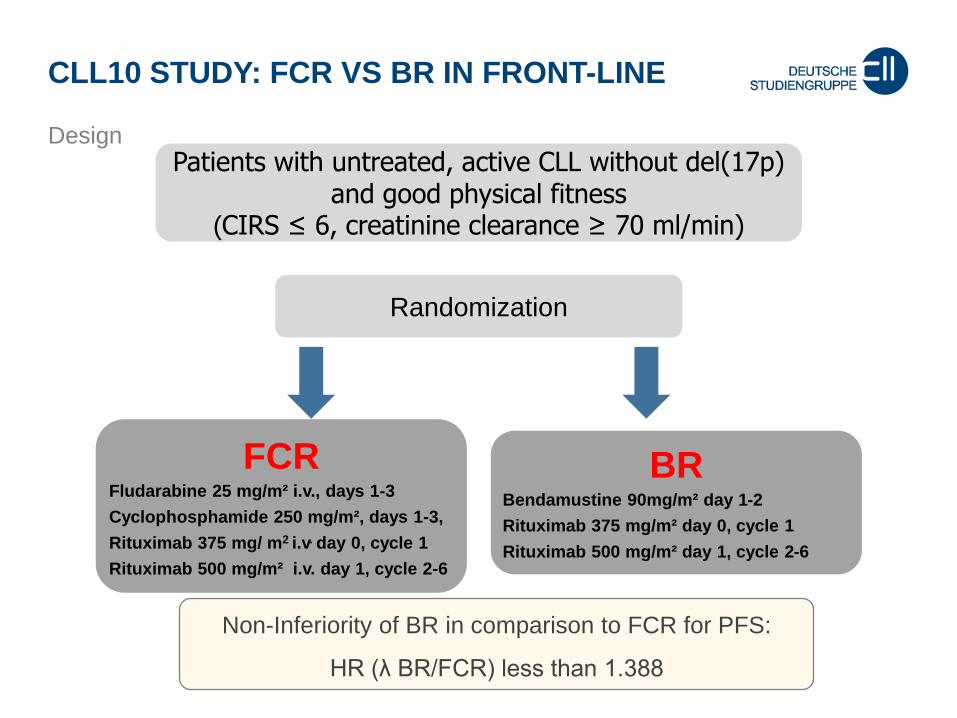
CLL10 STUDY: FCR VS BR IN FRONT-LINE
Design
Non-Inferiority of BR in comparison to FCR for PFS:
HR (λ BR/FCR) less than 1.388
Randomization
Patients with untreated, active CLL without del(17p) and good physical fitness
(CIRS ≤ 6, creatinine clearance ≥ 70 ml/min)
FCR Fludarabine 25 mg/m² i.v., days 1-3
Cyclophosphamide 250 mg/m², days 1-3,
Rituximab 375 mg/ m2 i.v. day 0, cycle 1
Rituximab 500 mg/m² i.v. day 1, cycle 2-6
BRBendamustine 90mg/m² day 1-2
Rituximab 375 mg/m² day 0, cycle 1
Rituximab 500 mg/m² day 1, cycle 2-6

CLL10 STUDY: FCR VS BR IN FRONT-LINE
Patients´ characteristics
Baseline characteristics FCR
n=282
BR
n=279
p value
Median age (y) 61.0 62.1 0.131
Age > 65 30.5% 38.7% 0.042
Male 71.3% 74.2% 0.450
Median time since
diagnosis (months)
21.6 24.6 0.846
ECOG = 0 64.1% 64.1% 0.194
CIRS, median 2 2 0.489
Mean number of cycles 5.27 5.41 0.022
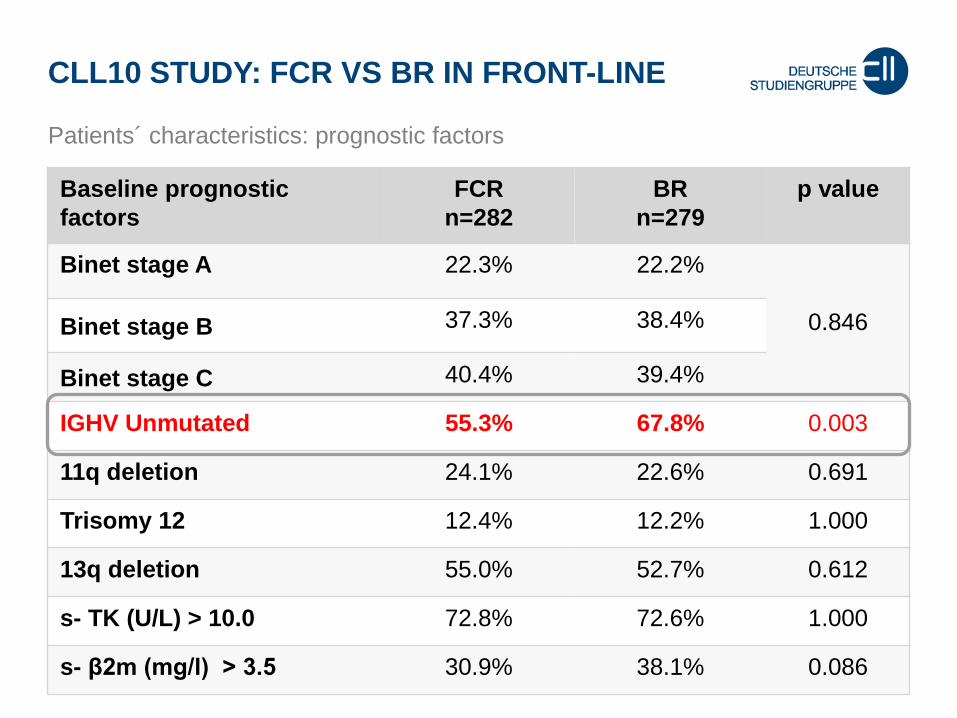
CLL10 STUDY: FCR VS BR IN FRONT-LINE
Patients´ characteristics: prognostic factors
Baseline prognostic
factors
FCR
n=282
BR
n=279
p value
Binet stage A 22.3% 22.2%
0.846Binet stage B 37.3% 38.4%
Binet stage C 40.4% 39.4%
IGHV Unmutated 55.3% 67.8% 0.003
11q deletion 24.1% 22.6% 0.691
Trisomy 12 12.4% 12.2% 1.000
13q deletion 55.0% 52.7% 0.612
s- TK (U/L) > 10.0 72.8% 72.6% 1.000
s- β2m (mg/l) > 3.5 30.9% 38.1% 0.086

CLL10 STUDY: FCR VS BR IN FRONTLINE
ITT Best Response according to IWCLL
Response FCR (%)
n=282
BR (%)
n=279
p value
CR (CR + CRi) 39.7 30.8 0.034
CR 35.1 30.4
CRi 4.6 0.4
PR 55.7 64.9
ORR 95.4 95.7 1.0
SD/PD 2.2 2.2
Missing response 2.5 2.1
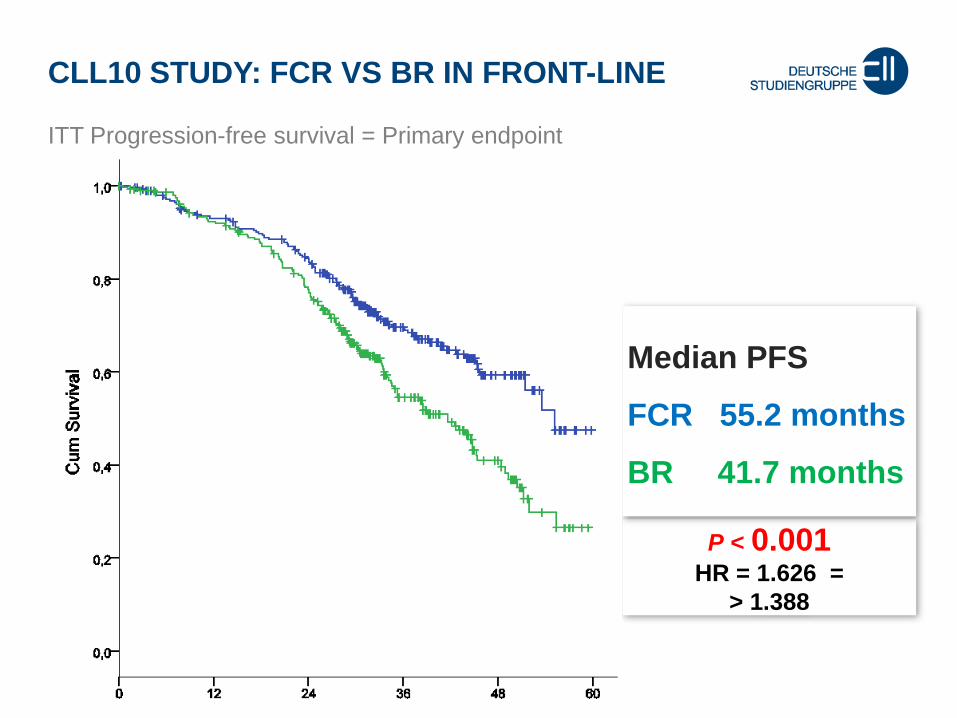
CLL10 STUDY: FCR VS BR IN FRONT-LINE
ITT Progression-free survival = Primary endpoint
P < 0.001HR = 1.626 =
> 1.388
Median PFS
FCR 55.2 months
BR 41.7 months
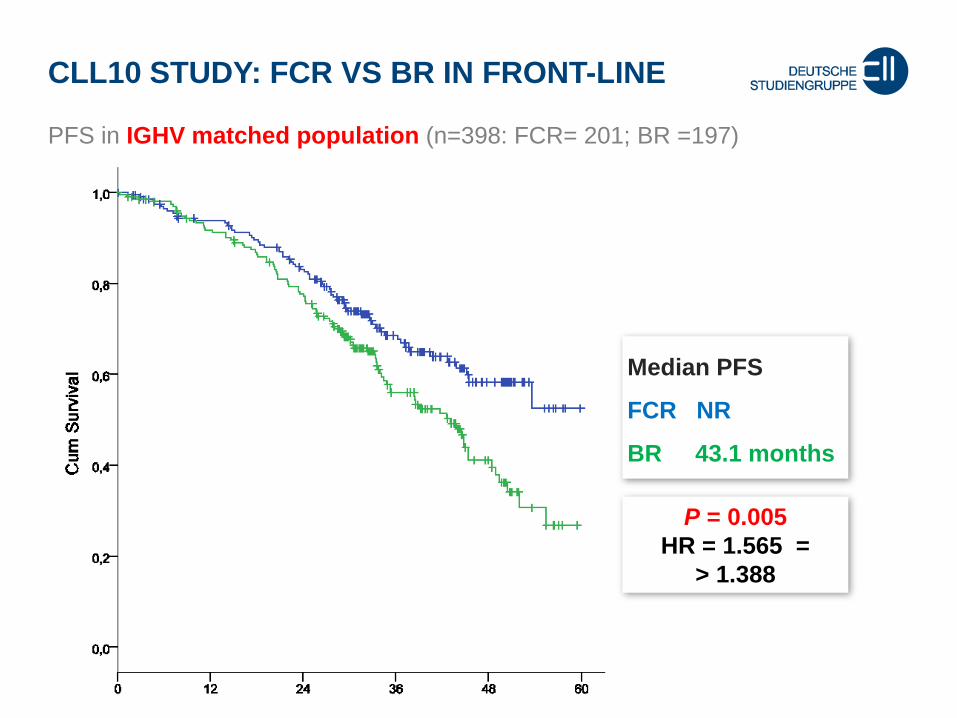
CLL10 STUDY: FCR VS BR IN FRONT-LINE
PFS in IGHV matched population (n=398: FCR= 201; BR =197)
P = 0.005
HR = 1.565 =
> 1.388
Median PFS
FCR NR
BR 43.1 months
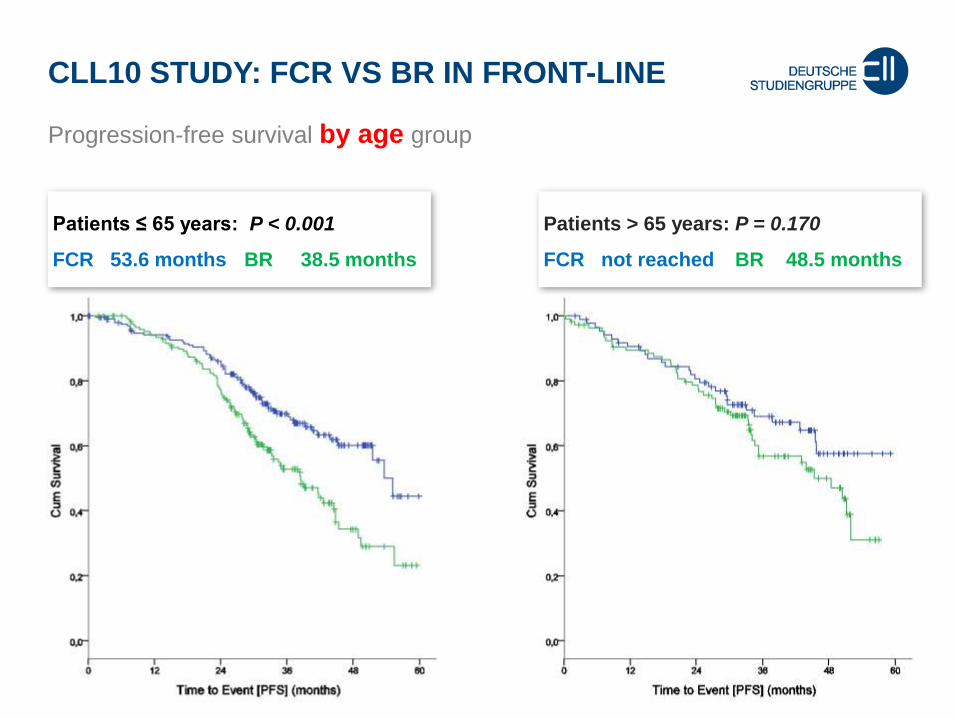
CLL10 STUDY: FCR VS BR IN FRONT-LINE
Progression-free survival by age group
Patients ≤ 65 years: P < 0.001
FCR 53.6 months BR 38.5 months
Patients > 65 years: P = 0.170
FCR not reached BR 48.5 months
CLL10 STUDY: FCR VS BR IN FRONT-LINE
Conclusion
Final analysis shows inferiority of BR versus FCR with regard to
PFS and CRR.
FCR is remains standard therapy in fit patients.
BR may be considered in fit, but elderly patients as alternative.
BR is associated with lower rates of neutropenias and severe
infections in elderly patients.

The safety and tolerability of
oral fludarabine, ± oral cyclophosphamide and
intravenous rituximab therapy in previously
untreated patients with CLL aged ≥65 years
– FINAL analysis from the
Australasian Leukaemia and Lymphoma Group (ALLG) and
CLL Australian Research Consortium (CLLARC) CLL5 Study.
Stephen P Mulligan, Devinder Gill, Paul Turner, William Renwick,
Maya Latimer, Leanne Berkahn, David Simpson, Phillip Campbell,
Rosemary Harrup, Cecily Forsyth, Melanie Sulda, Giles Best,
Bryone Kuss and Gavin Cull for the CLLARC and ALLG.
56th ASH Annual Meeting San Francisco, December, 2014
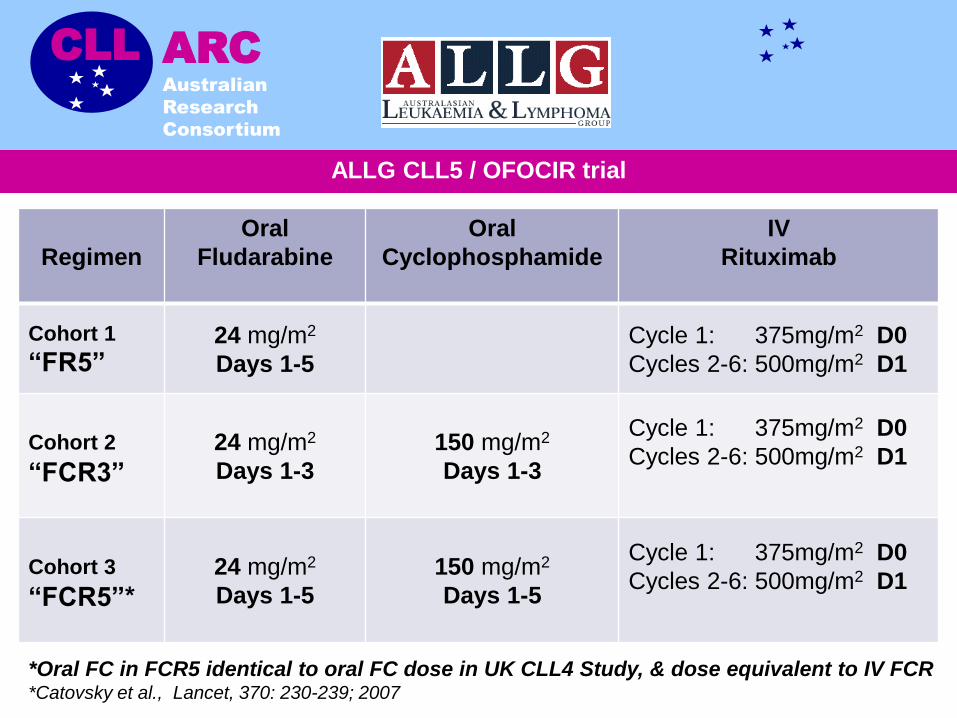
ALLG CLL5 / OFOCIR trial
CLL ARC
Australian
Research
Consortium
Regimen
Oral
Fludarabine
Oral
Cyclophosphamide
IV
Rituximab
Cohort 1
“FR5”24 mg/m2
Days 1-5
Cycle 1: 375mg/m2 D0
Cycles 2-6: 500mg/m2 D1
Cohort 2
“FCR3”
24 mg/m2
Days 1-3
150 mg/m2
Days 1-3
Cycle 1: 375mg/m2 D0
Cycles 2-6: 500mg/m2 D1
Cohort 3
“FCR5”*
24 mg/m2
Days 1-5
150 mg/m2
Days 1-5
Cycle 1: 375mg/m2 D0
Cycles 2-6: 500mg/m2 D1
*Oral FC in FCR5 identical to oral FC dose in UK CLL4 Study, & dose equivalent to IV FCR*Catovsky et al., Lancet, 370: 230-239; 2007

ALLG CLL5 / OFOCIR trial
CLL ARC
Australian
Research
Consortium
Haematologic and non-Haematologic Toxicity:
Dose delay and stopping rules
Toxicity Grade Dose Delay or Stopping Rule
Grade 1 or 2Continue Fludarabine / cyclophosphamide at prescribed dose
Supportive care per local guidelines and investigator discretion
Grade 3 or 4 Hold next cycle until RESOLVES to ≤ Grade 2
CONTINUE therapy with SAME dose (i.e. no dose reduction)
Grade 3 or 4
If FAILS TO RESOLVE to ≤ Grade 2 by 2 WEEKS,
or RECURS in subsequent cycles → OFF STUDY Then treat as per physician discretion.

End of Recruitment
120 recruited from 29 centres in Australia and New Zealand Median age Age at randomisation (in years)Mean 71.7Median 71Range 65 – 83
Age range No. %65 – 69 years 42 35.9%70 – 74 years 45 38.5%75 – 79 years 21 17.9%80 – 84 years 9 7.7%
Binet stage at registration
A 20 17.1%
B 55 47.0%
C 42 35.9%
Recruitment of 120 pts was completed in July 2012.
117 fulfilled eligibility, 1 had no treatment or follow-up with remaining
cohort to 116 patients for analysis

Responses
Final Pathological Staging 2 months Post-Rx or at Rx end
Treatment armTotal
(n=116)FR5 FCR3 FCR5
(N=37) (N=41) (N=38)
BM confirmed CR 27% 44% 45% 39%
CR 9 (24% ) 13 (32% ) 8 (21% ) 30 (26% )
CR-i 1 (3% ) 5 (12% ) 9 (24% ) 15 (13% )
Total MRD Negative(including PB MRD-neg CRu and CRi/u)
14 (38% ) 21 (51% ) 30 (79% ) 65 (56%)
nPR 11 (30% ) 13 (32% ) 3 (8% ) 27 (23% )
PR 10 (27% ) 5 (12% ) 4 (11% ) 19 (16% )
SD 1 (3% ) 1 (2% ) 0 (0% ) 2 (2% )
Progressive Disease (PD) / early death 1 (3% ) 1 (2% ) 1 (3% ) 3 (3% )
Overall Response Rate (ORR - CR, CR-i, CR-u, CR-i/u, nPR, PR)
35
(95% )
39
(95% )
37
(97% )
111
(96% )
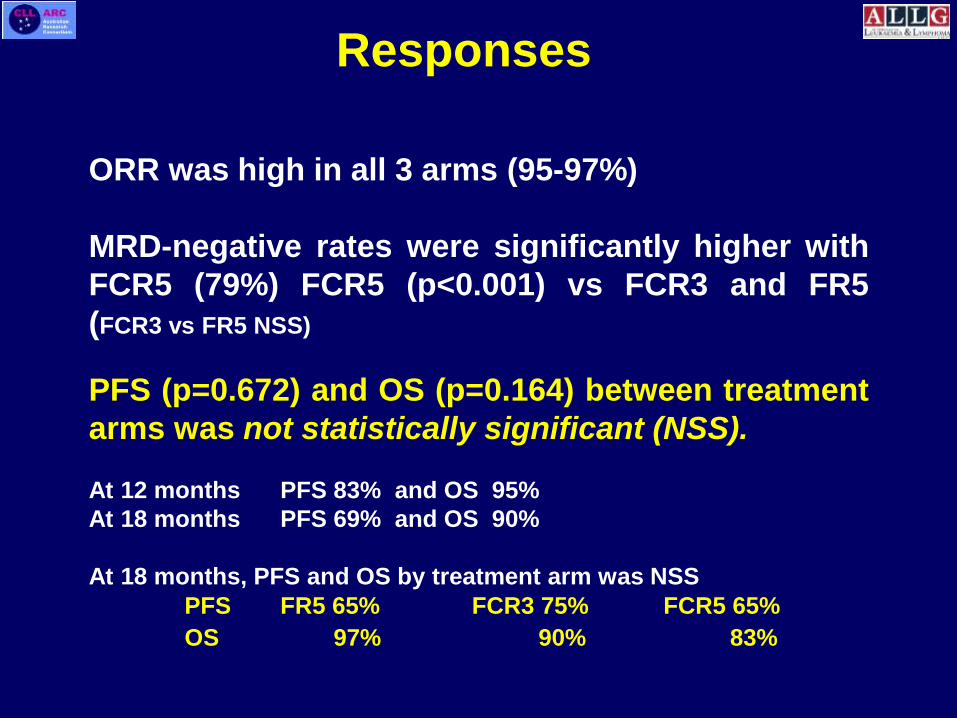
Responses
ORR was high in all 3 arms (95-97%)
MRD-negative rates were significantly higher with
FCR5 (79%) FCR5 (p<0.001) vs FCR3 and FR5
(FCR3 vs FR5 NSS)
PFS (p=0.672) and OS (p=0.164) between treatment
arms was not statistically significant (NSS).
At 12 months PFS 83% and OS 95%
At 18 months PFS 69% and OS 90%
At 18 months, PFS and OS by treatment arm was NSS
PFS FR5 65% FCR3 75% FCR5 65%
OS 97% 90% 83%

Toxicity
Grade 3+ Adverse Events
by Treatment Arm
Treatment armTotal
(n=116)FR5 FCR3 FCR5(N=37) (N=41) (N=38)
Haematological 15 (41% ) 26 (63% ) 29 (76% ) 70(60%)
Neutropenia 14 (38% ) 20 (49% ) 24 (63% ) 58 (50% )
Febrile Neutropenia / Infection 5 (14% ) 6 (15% ) 13 (34% ) 24 (21% )
Thrombocytopenia 2 (5% ) 5 (12% ) 12 (32% ) 19 (16% )
Anaemia 3 (8% ) 6 (15% ) 6 (16% ) 15 (13% )
Haemolytic Anaemia 0 (0% ) 2 (5% ) 3 (8% ) 5 (4% )
At least 1 grade 3+ AE 21 (57%) 34 (83%) 35 (92%) 90(78%)
Early cessation
due to toxicity2 (5.6%) 1 (2.4%) 13 (34%) 16 (14%)

Toxicity
Toxicity was lower with FR5 compared to FCR3 and FCR5
(p=0.004) (FCR3 vs FCR5 NSS).
Dose delay occurred in 43pts (37%):FR512 (32%), FCR3 14 (34%), FCR517 (44%) (p=0.653)
Early cessation due to toxicity more common with FCR5
(p<0.001).
11/13 pts stopping early due to toxicity received ≥3 cycles of therapy
(mean 3.5)
Cyclophosphamide with FR adds toxicity but improves CR rate

Conclusions
Oral F(C)R therapy appears safe and well tolerated in
fit CLL patients aged ≥65 years requiring 1st-line therapy
Toxicity - mostly haematological and manageable
Response rates very high - 96% ORR
No association between toxicity and CIRS 0–6 or age.
Full dose FCR is highly effective with higher cessation
due to toxicity but higher CR: ?dose intensity effect?

Novel therapies in CLL
Agent Development Phase Sponsor
CD20 mAb
Obinutuzumab Phase III Roche
BTK inhibitors
Ibrutinib
CC-292
ONO-4059
ACP-196
Registration Phase III
Phase Ib
Phase I
Pending Phase II
Pharmacyclics, Inc.
Celgene Corporation
Ono Pharmaceutical
Acerta
PI3KΥ/δ inhibitors
Idelalisib
GS-9820
IPI-145
AMG 319
TGR-1202
SAR245408 (XL147)
Registration Phase III
Phase I
Pending Phase III
Phase I
Phase I
Phase I
Gilead Sciences
Gilead Sciences
Infinity Pharmaceuticals
Amgen
TG Therapeutics
Sanofi
BCL-2 inhibitor
ABT-199 Phase Ib AbbVie/Roche
Obinutuzumab + Chlorambucil
1st line CLL with comorbidities

G-Clb (n=333)
%
R-Clb (n=329)a
%
Response rate
ORR 78 65
p <0.0001
CRb 21 7
PRc 58 58
SD 5 15
PD 4 11
Not evaluabled 13 9
CLL11 – G+Cbl End-of-treatment response
a Assessment not reached by data cut-off in 1 patient in R-Clb arm; as assessed by iwCLL criteria 3 months after end of treatmentb Confirmed by imaging and bone marrow, and includes incomplete CRc Includes nodular PRd Due to missing data or withdrawal from study treatment prior to response assessment
ORR, overall response rate; CR, complete response; PR, partial response; SD, stable disease; PD, progressive disease Slide Dr Valentin Goede

BCR SIGNAL INHIBITION IN CLL
Nat Rev Immunol 2:945
Ibrutinib
Idelalisib
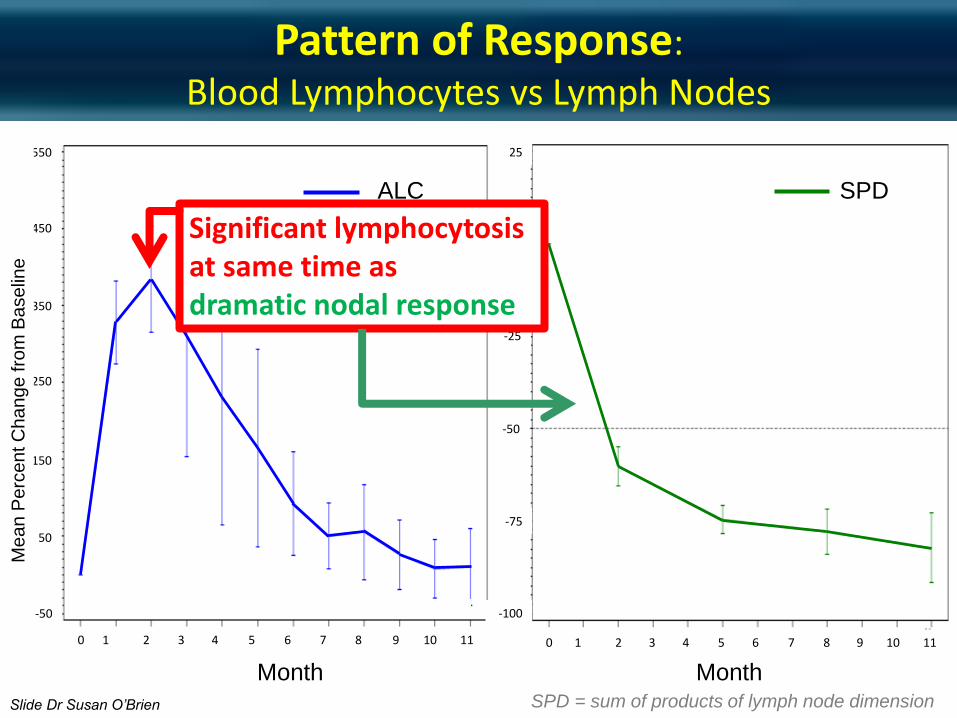
Pattern of Response:
Blood Lymphocytes vs Lymph Nodes
SPD = sum of products of lymph node dimension
SPD
0 1 2 3 4 5 6 7 8 9 10 11
550
450
350
250
150
50
-50
ALC
Month Month
-100
-75
-50
-25
0
25
Me
an
Pe
rce
nt C
ha
ng
e fro
m B
ase
line
0 1 2 3 4 5 6 7 8 9 10 11
Slide Dr Susan O’Brien
Significant lymphocytosis at same time as dramatic nodal response
American Society of Clinical Oncology 2014, PCYC 1102/1103, O’Brien et al. 28
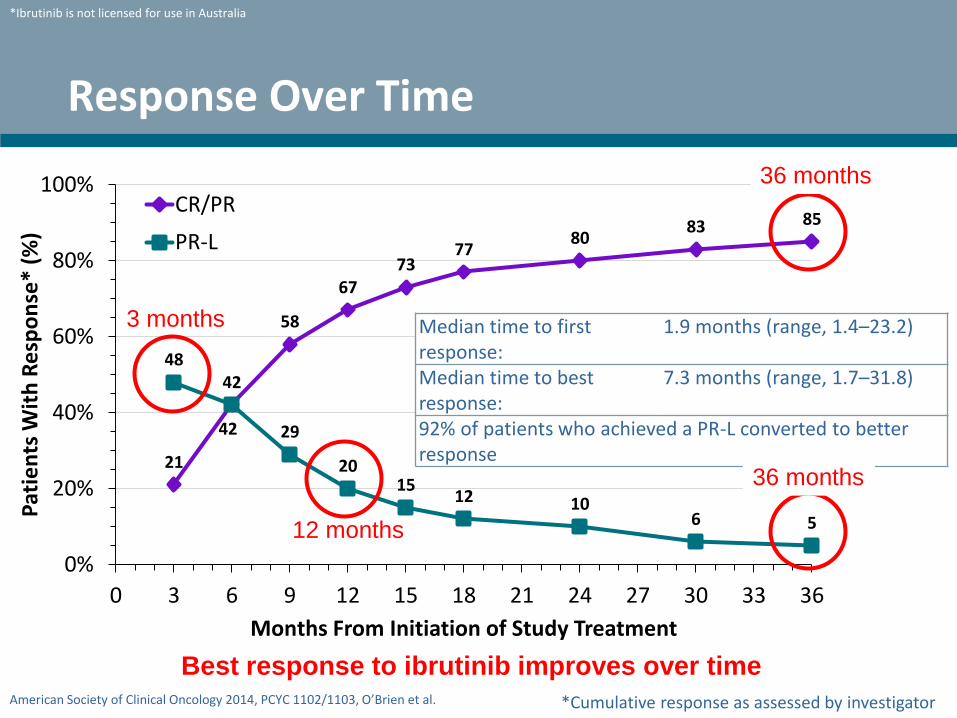
Response Over Time
21
42
58
6773
7780
83 85
4842
29
2015
12 106 5
0%
20%
40%
60%
80%
100%
0 3 6 9 12 15 18 21 24 27 30 33 36
Pat
ien
ts W
ith
Re
spo
nse
* (%
)
Months From Initiation of Study Treatment
CR/PR
PR-L
Best response to ibrutinib improves over time
Median time to first response:
1.9 months (range, 1.4–23.2)
Median time to best response:
7.3 months (range, 1.7–31.8)
92% of patients who achieved a PR-L converted to better response
*Cumulative response as assessed by investigator
*Ibrutinib is not licensed for use in Australia
3 months
12 months
36 months
36 months
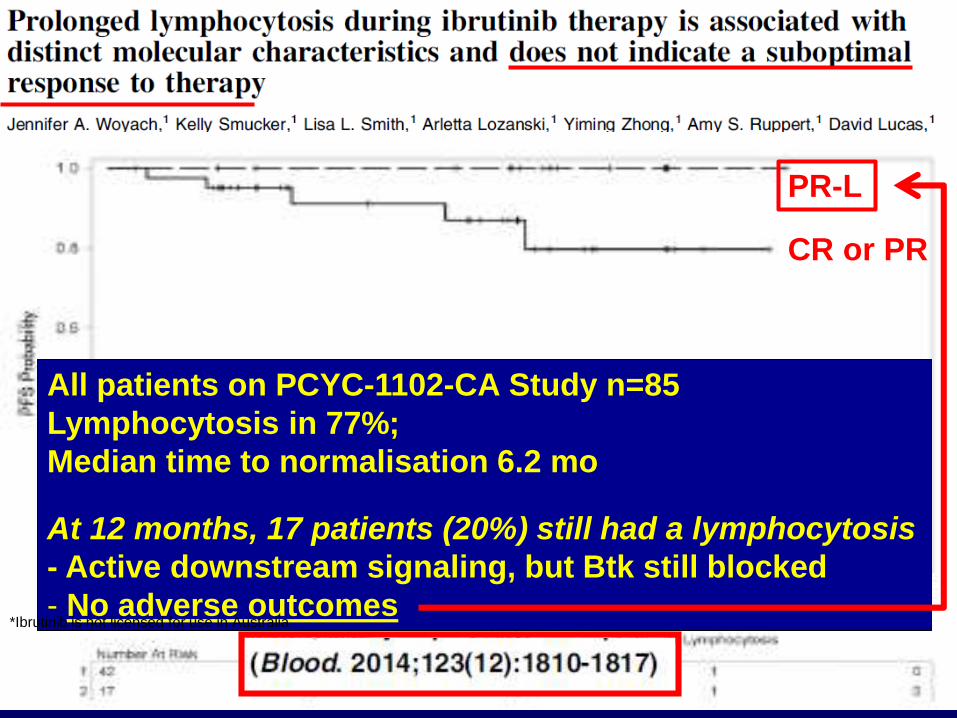
Prolonged lymphocytosis on ibrutinib
All patients on PCYC-1102-CA Study n=85
Lymphocytosis in 77%;
Median time to normalisation 6.2 mo
At 12 months, 17 patients (20%) still had a lymphocytosis
- Active downstream signaling, but Btk still blocked
- No adverse outcomes
PR-L
CR or PR
*Ibrutinib is not licensed for use in Australia

Idelalisib + Rituximab in R/R CLL
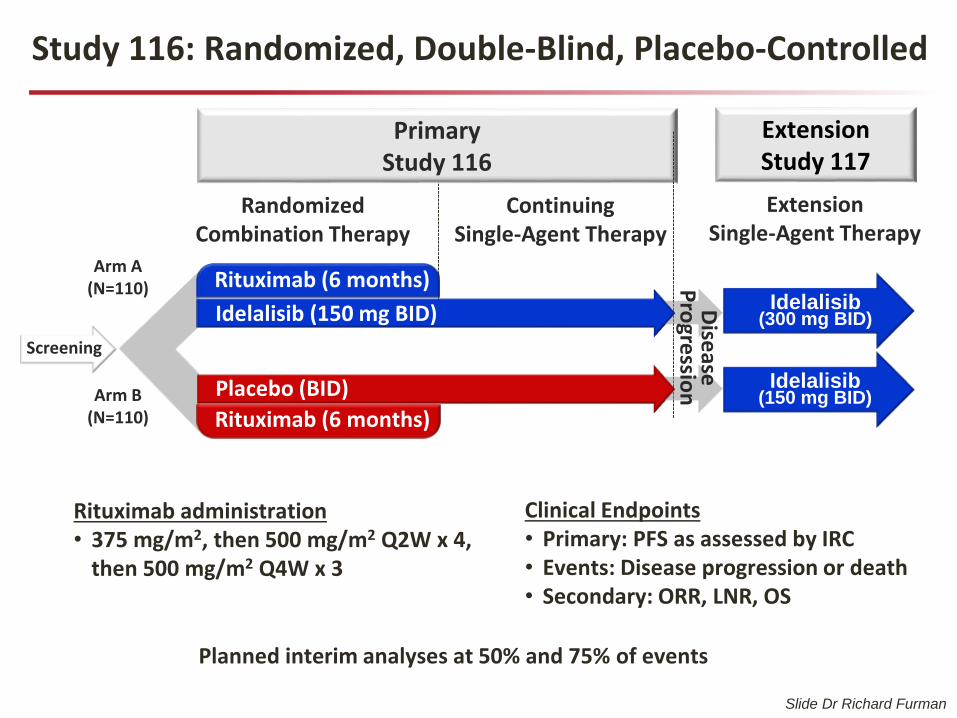
Study 116: Randomized, Double-Blind, Placebo-Controlled
Extension Single-Agent Therapy
Extension Study 117
RandomizedCombination Therapy
ContinuingSingle-Agent Therapy
Primary Study 116
Arm A(N=110)
Arm B(N=110)
Idelalisib (150 mg BID)
Placebo (BID)
Rituximab (6 months)
Rituximab (6 months)
Screening
Idelalisib (150 mg BID)
Idelalisib (300 mg BID)
Rituximab administration• 375 mg/m2, then 500 mg/m2 Q2W x 4,
then 500 mg/m2 Q4W x 3
Clinical Endpoints• Primary: PFS as assessed by IRC• Events: Disease progression or death • Secondary: ORR, LNR, OS
Dise
aseP
rogre
ssion
Planned interim analyses at 50% and 75% of events
Slide Dr Richard Furman

0 2 4 6 8 1 0 1 2 1 4 1 6
0
2 5
5 0
7 5
1 0 0
T im e (m o n th s )
Pro
gre
ss
ion
-fre
e
su
rviv
al
(%)
ID E L A + R it u x im a b
P la c e b o + R it u x im a b
M e d ia n P F S = 5 .5 m o n t h s
M e d ia n P F S : n o t r e a c h e d
H R = 0 .1 5
9 5 % C I (0 .0 8 , 0 .2 8 )
p < 0 .0 0 0 1
6 9 4 4 3 4 3 0 1 4 6 2 0ID E L A + R : 1 1 0
6 2 3 0 1 8 1 3 6 1 1 0P la c e b o + R : 1 1 0
S u b je c ts a t r is k , n
Primary Endpoint: Progression-Free Survival
Slide Dr Richard Furman

Ibrutinib vs Ofatumumab in R/R CLL
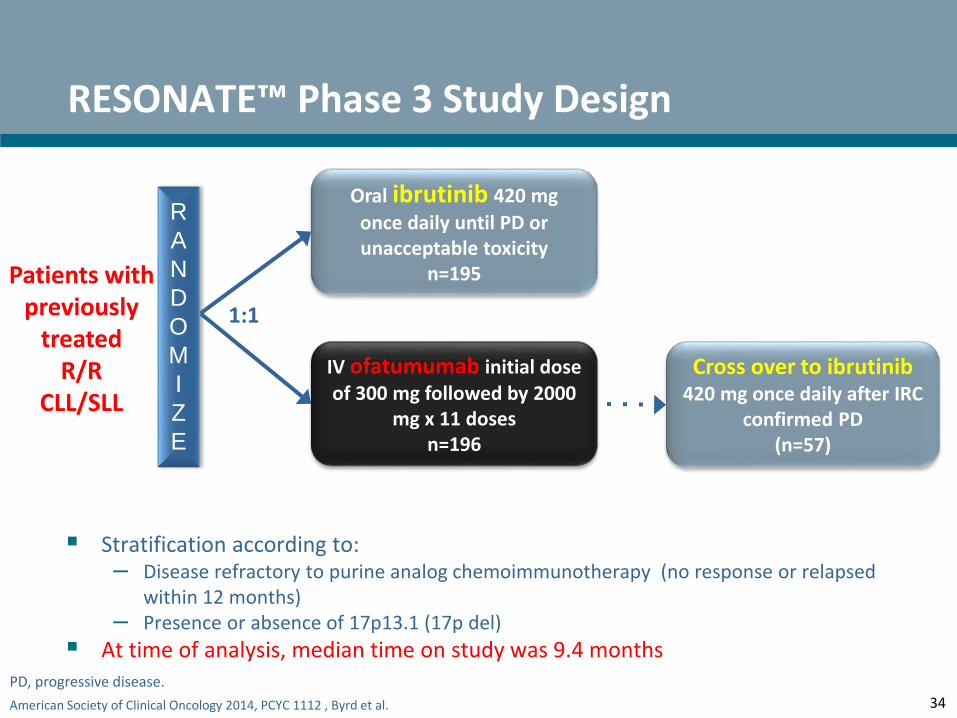
American Society of Clinical Oncology 2014, PCYC 1112 , Byrd et al.
Stratification according to:– Disease refractory to purine analog chemoimmunotherapy (no response or relapsed
within 12 months)– Presence or absence of 17p13.1 (17p del)
At time of analysis, median time on study was 9.4 months
34
RESONATE™ Phase 3 Study Design
R
A
N
D
O
M
I
Z
E
Oral ibrutinib 420 mg
once daily until PD or unacceptable toxicity
n=195
IV ofatumumab initial dose of 300 mg followed by 2000
mg x 11 dosesn=196
1:1
Patients with previously
treatedR/R
CLL/SLL
PD, progressive disease.
Cross over to ibrutinib 420 mg once daily after IRC
confirmed PD (n=57)
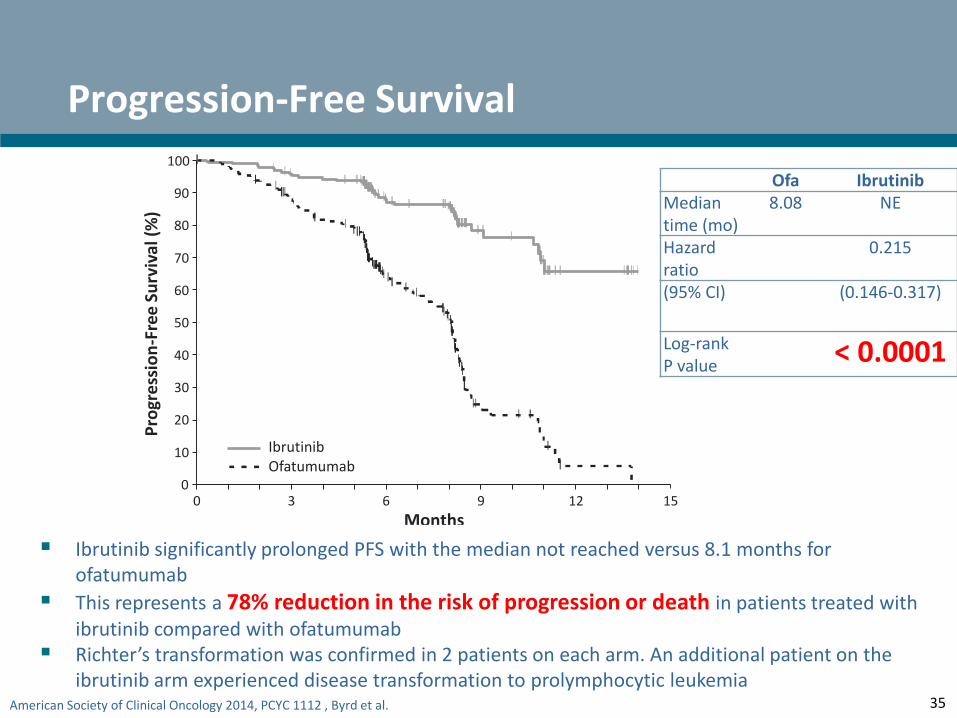
American Society of Clinical Oncology 2014, PCYC 1112 , Byrd et al. 35
Progression-Free Survival
0 3 6 9 12
195 183 116 38 7196 161 83 15 1 0
150
10
20
30
40
50
60
70
80
90
100P
rogr
ess
ion
-Fre
e S
urv
ival
(%
)
No. at riskIbrutinib:
Ofatumumab:
Months
IbrutinibOfatumumab
Ofa IbrutinibMedian time (mo)
8.08 NE
Hazard ratio
0.215
(95% CI) (0.146-0.317)
Log-rank P value
< 0.0001
Ibrutinib significantly prolonged PFS with the median not reached versus 8.1 months for ofatumumab
This represents a 78% reduction in the risk of progression or death in patients treated with ibrutinib compared with ofatumumab
Richter’s transformation was confirmed in 2 patients on each arm. An additional patient on the ibrutinib arm experienced disease transformation to prolymphocytic leukemia

American Society of Clinical Oncology 2014, PCYC 1112 , Byrd et al.
0
0.2
0.4
0.6
0.8
1.0
Pro
gre
ssio
n-F
ree
Su
rviv
al (
Pro
po
rtio
n)
0 6 12 18 24 30 36 42
Months From Initiation of Study Treatment
36
Progression-Free Survival by Cytogenetics (FISH) in Relapsed/Refractory Population
Del17p Del11q No del17p/11q
30-monthPFS 45.9% 74.2% 89.0%
(95% CI) (25.0–64.6) (53.3–86.8) (69.0–96.4)
Median PFS 28.1 months Not reached Not reached
del17p
del11q
No del17p or del11q
+ Censored

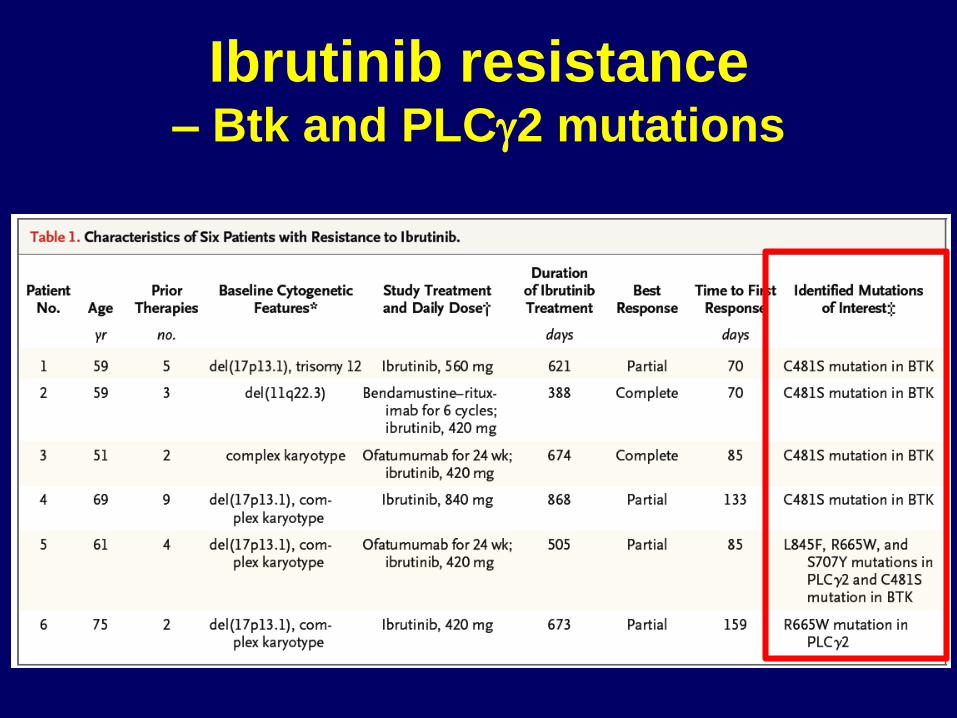
Ibrutinib resistance – Btk and PLCg2 mutations
Andrew J SteeleSouthampton, UK
The dual PI3K/mTOR inhibitor PF-04691502 induces substantial apoptosis in chronic lymphocytic
leukaemia cells in vitro and prolongs survival in the Eµ-TCL1 mouse model
56th ASH Annual Meeting San Francisco, December, 2014
DUAL AND MULTIPLE MOLECULAR
BCR INHIBITORS
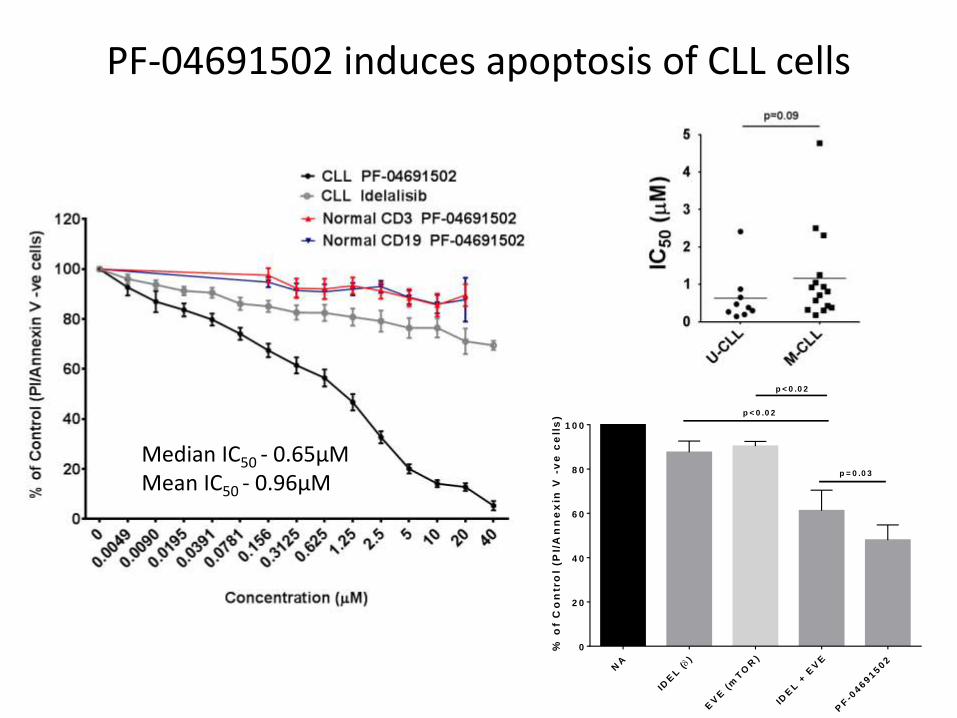
PF-04691502 induces apoptosis of CLL cells
Median IC50 - 0.65µMMean IC50 - 0.96µM
NA
IDE
L ()
EV
E (
mT
OR
)
IDE
L +
EV
E
PF
-04691502
0
2 0
4 0
6 0
8 0
1 0 0
% o
f C
on
tro
l (P
I/A
nn
ex
in V
-v
e c
ell
s)
p = 0 .0 3
p < 0 .0 2
p < 0 .0 2
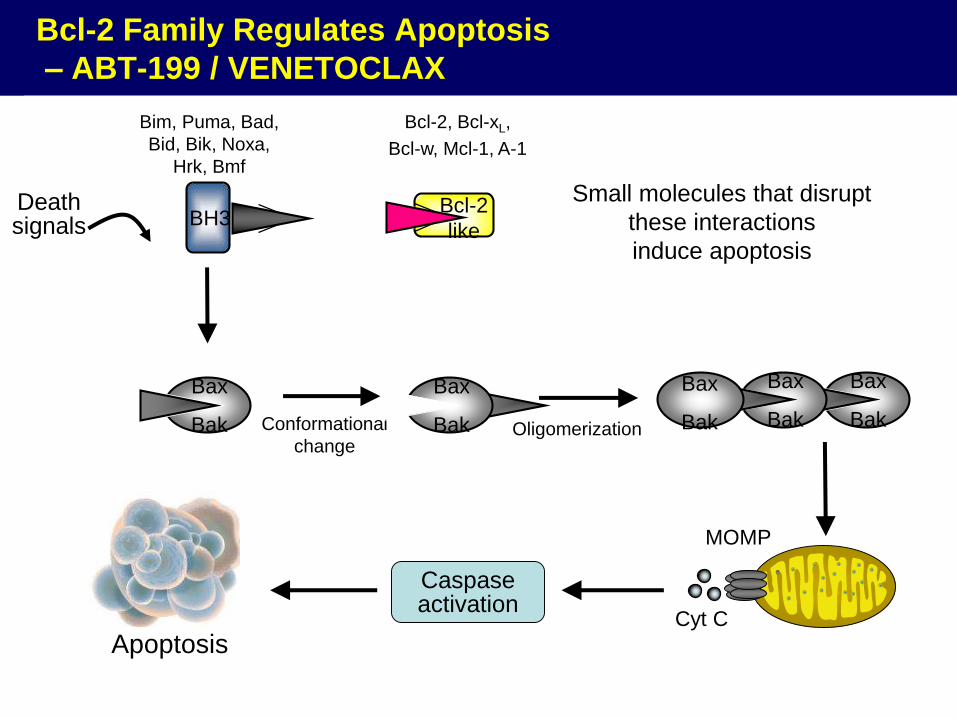
Bcl-2 Family Regulates Apoptosis
– ABT-199 / VENETOCLAX
Conformational
changeOligomerization
Small molecules that disrupt
these interactions
induce apoptosis
BH3
Bax
Bak
Bax
Bak
Bax
Bak
Bax
Bak
Apoptosis
MOMP
Cyt C
Bax
Bak
Death signals
Bim, Puma, Bad,
Bid, Bik, Noxa,
Hrk, Bmf
Bcl-2, Bcl-xL,
Bcl-w, Mcl-1, A-1
Caspaseactivation
Bcl-2
like
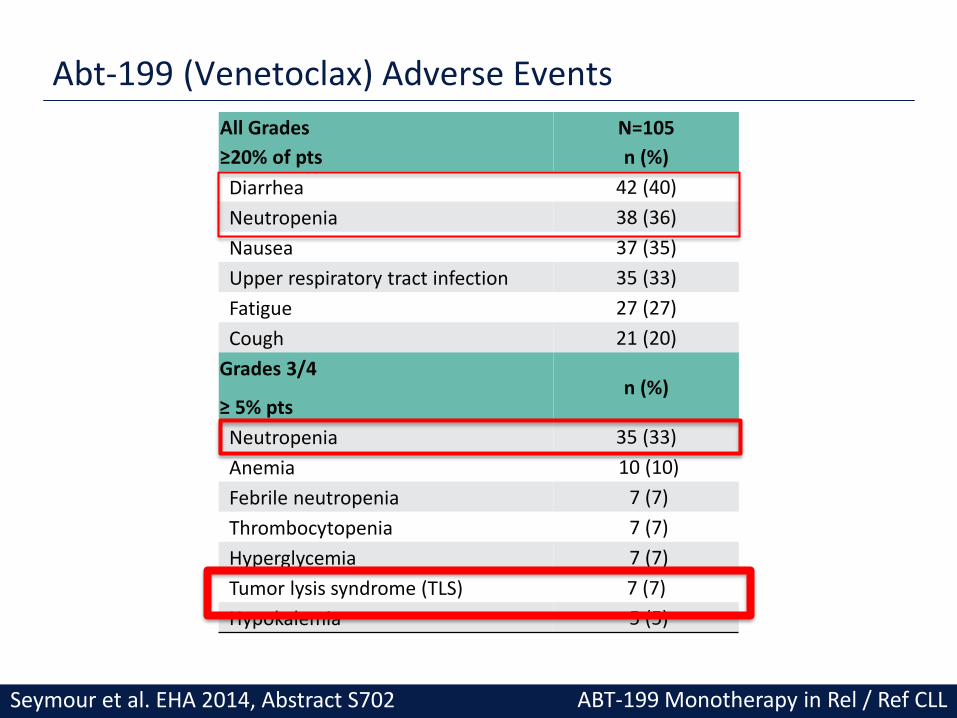
Abt-199 (Venetoclax) Adverse Events
All Grades
≥20% of pts
N=105
n (%)
Diarrhea 42 (40)
Neutropenia 38 (36)
Nausea 37 (35)
Upper respiratory tract infection 35 (33)
Fatigue 27 (27)
Cough 21 (20)
Grades 3/4
≥ 5% ptsn (%)
Neutropenia 35 (33)
Anemia 10 (10)
Febrile neutropenia 7 (7)
Thrombocytopenia 7 (7)
Hyperglycemia 7 (7)
Tumor lysis syndrome (TLS) 7 (7)
Hypokalemia 5 (5)
ABT-199 Monotherapy in Rel / Ref CLL Seymour et al. EHA 2014, Abstract S702
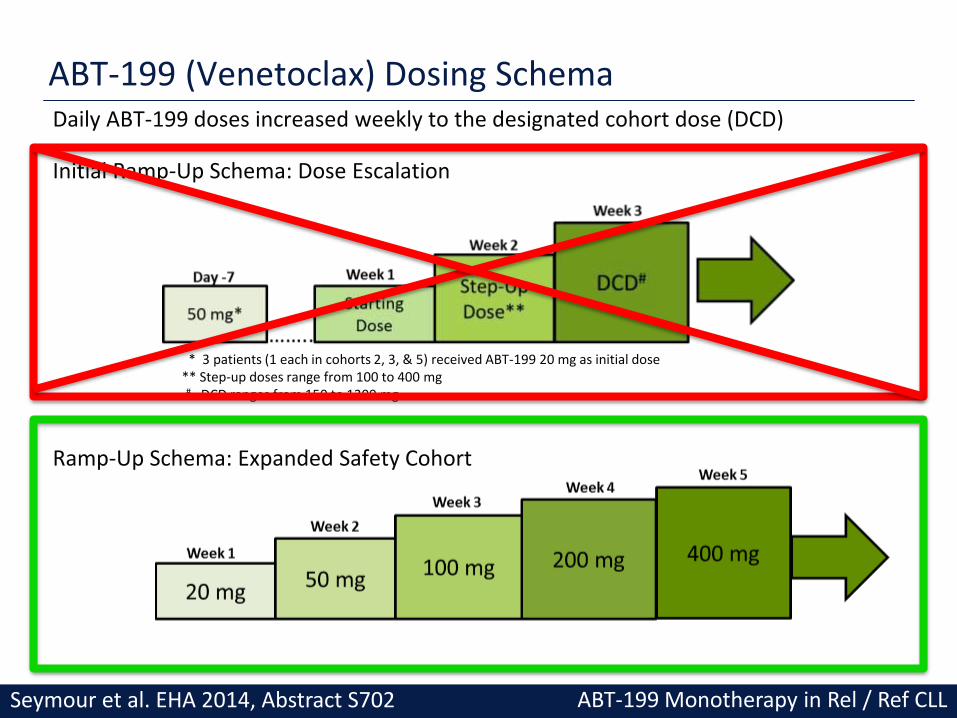
ABT-199 (Venetoclax) Dosing SchemaDaily ABT-199 doses increased weekly to the designated cohort dose (DCD)
Initial Ramp-Up Schema: Dose Escalation
Ramp-Up Schema: Expanded Safety Cohort
* 3 patients (1 each in cohorts 2, 3, & 5) received ABT-199 20 mg as initial dose** Step-up doses range from 100 to 400 mg# DCD ranges from 150 to 1200 mg
ABT-199 Monotherapy in Rel / Ref CLL Seymour et al. EHA 2014, Abstract S702

Objective Responses of ABT-199 (Venetoclax)
ResponsesAll
n (%), n = 78del (17p)
n (%), n = 19F-Refractoryn (%), n = 41
IGHV Unmutatedn (%), n = 24
Overall response 60 (77) 15 (79) 31 (76) 18 (75)
Complete response (CR/CRi)# 18 (23) 5 (26) 9 (22) 7 (29)
Partial response* 42 (54) 10 (53) 22 (54) 11 (46)
Stable disease 10 (13) 2 (11) 7 (17) 2 (8)
Disease progression 2 (3) 1 (5) 1 (3) 2 (8)
D/C Prior to assessment+ 6 (8) 1 (5) 2 (5) 2 (8)Some patients may have more than one high risk marker. #4 patients have CRi; +D/C = discontinued, first assessment at 6 weeks*3 patients had confirmatory CT imaging assessments at less than an 8 week interval (5, 6, and 7 weeks)
• As of April 9, evaluable patients (n=78) had 2 CT scans, performed approximately 8 weeks apart, n=55 from dose escalation and n=23 from the safety expansion cohort
• A total of 26 patients are not yet evaluable in the SE cohort (12 patients had a PR at their first scan, 14 patients have not yet reached their first assessment)
• The median duration of response has not yet been reached based on current patient enrollment numbers.
ABT-199 Monotherapy in Rel / Ref CLL Seymour et al. EHA 2014, Abstract S702
Some patients MRD-negative

Progression Free Survival (PFS) at 400 mg or Higher
• Median PFS for patients treated at or above 400 mg has not yet been reached,(median follow-up of 5.3 months, range [0.03 – 22])
• As of April 9, 2014, the median PFS for all patients is approximately 18 months
ABT-199 Monotherapy in Rel / Ref CLL Seymour et al. EHA 2014, Abstract S702

Genetics from CLL8 trial
Stilgenbauer, Blood, 22nd May, 2014, 123: 3247
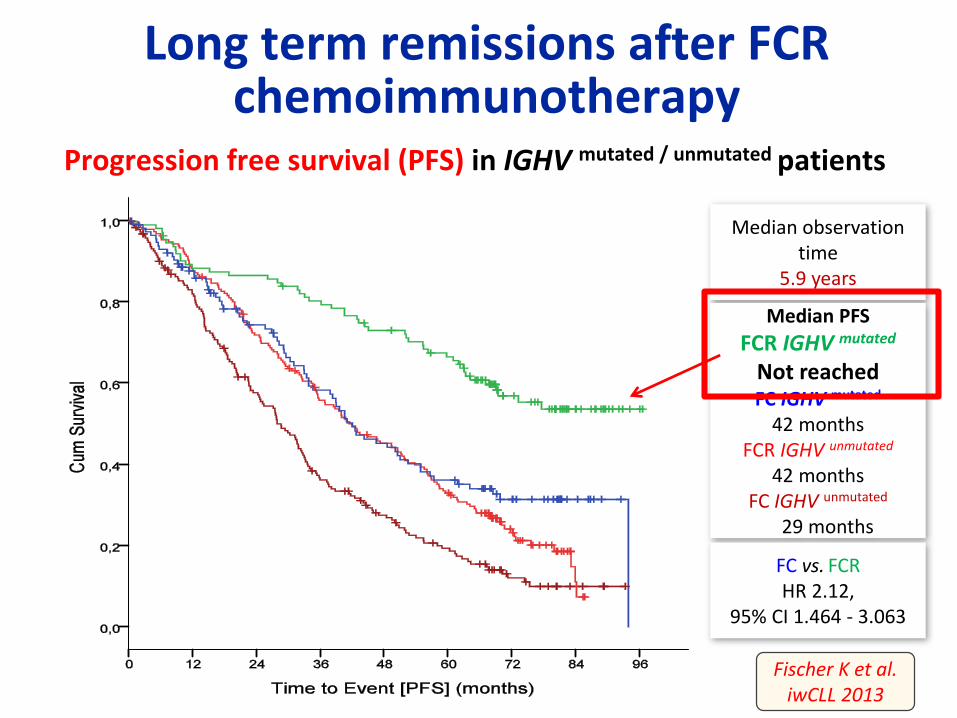
Long term remissions after FCR chemoimmunotherapy
Progression free survival (PFS) in IGHV mutated / unmutated patients
Fischer K et al. iwCLL 2013
Median observationtime
5.9 years
Median PFS
FCR IGHV mutated
Not reachedFC IGHV mutated
42 monthsFCR IGHV unmutated
42 monthsFC IGHV unmutated
29 months
FC vs. FCRHR 2.12,
95% CI 1.464 - 3.063

Novel Genetic Markers in CLL8
1. TP53 and SF3B1 strongest predictive markers
2. Notch1 – FC with rituximab fails to improve
response and survival
Stilgenbauer et al., Blood, 2014, 123: 3247
PD-L1 Immune Checkpoint Blockade Prevents
Immune Dysfunction and Leukemia Development in
a Mouse Model of Chronic Lymphocytic Leukemia
Bola Hanna
PhD student
German Cancer Research Center
December 8th 2014
56th ASH Annual Meeting San Francisco, December, 2014

PAge5025.02.2014 |
Author
Division
Myeloid
cells PD-L1
PD-L1
PD-1
Inhibitory ligands(Ramsay et al. Blood 2012)
Chronic activation(Riches et al. Blood 2013,
Brusa et al. Haematologica 2013)
MDSCs and TAMs(Jitschinet al. Blood 2014,
Hanna et al. manuscript in preparation)
PD-1/PD-L1 axis as key inducer of
CLL-associated immune defects
CLL
cells
T cells
(Topalian at al. NEJM, 2012)
Significant anti-tumor response of PD-1
blocking antibodies in solid tumors

PAge5125.02.2014 |
Author
Division
PD-L1 blockade controls disease in
blood and secondary lymphoid organs
isotype
aPD-L1
all graphs show median with IQR, *** p<.0001, ** p<.001, * p<.05
Spleen weight and tumor load
Tumor load in PB and other lymphoid organs
Prevents
T-cell subset changes
CD4:CD8 ratioRestores T-cell cytokine production
and proliferation levels
Prevents “exhaustion” phenotype
and restores T-cell functions
??Therapy for immune failure and autoimmunity in CLL??
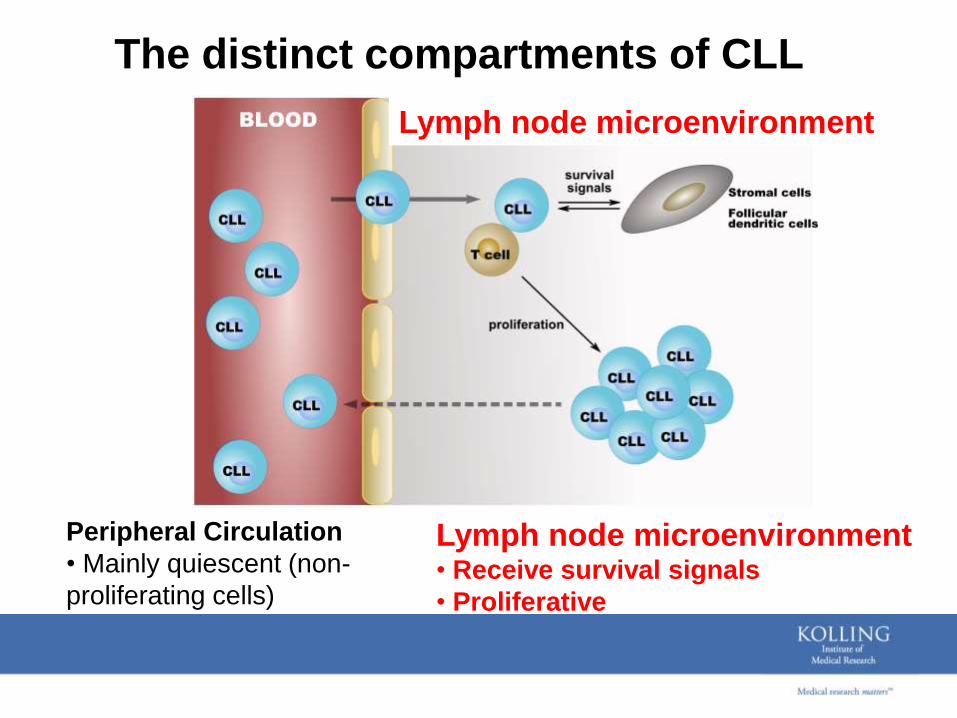
The distinct compartments of CLL
Peripheral Circulation
• Mainly quiescent (non-
proliferating cells)
Lymph node microenvironment• Receive survival signals
• Proliferative
Lymph node microenvironment
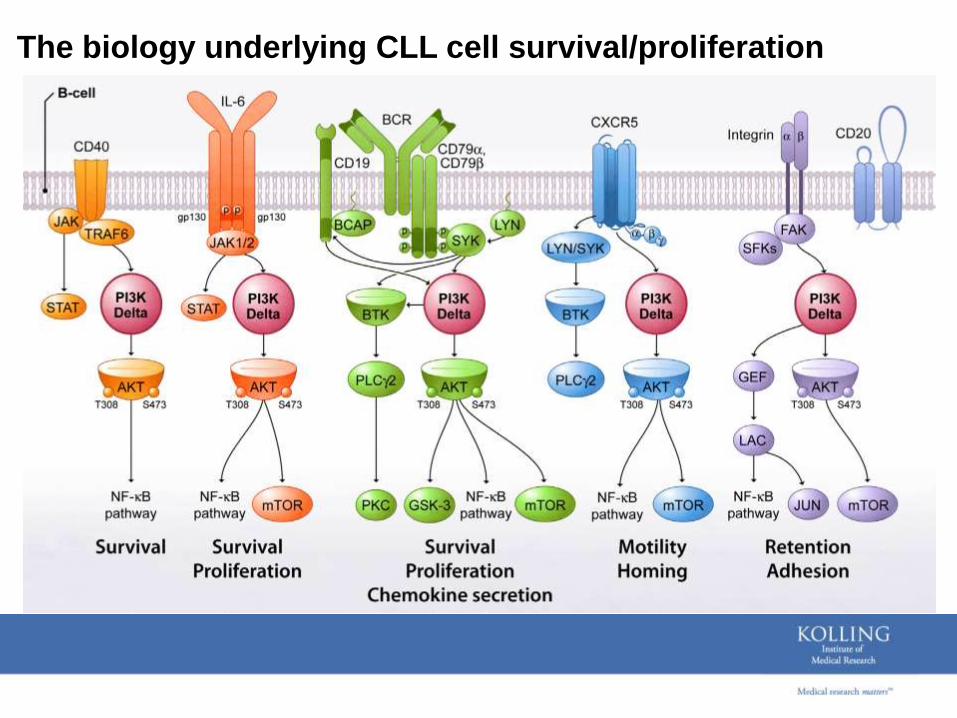
The biology underlying CLL cell survival/proliferation
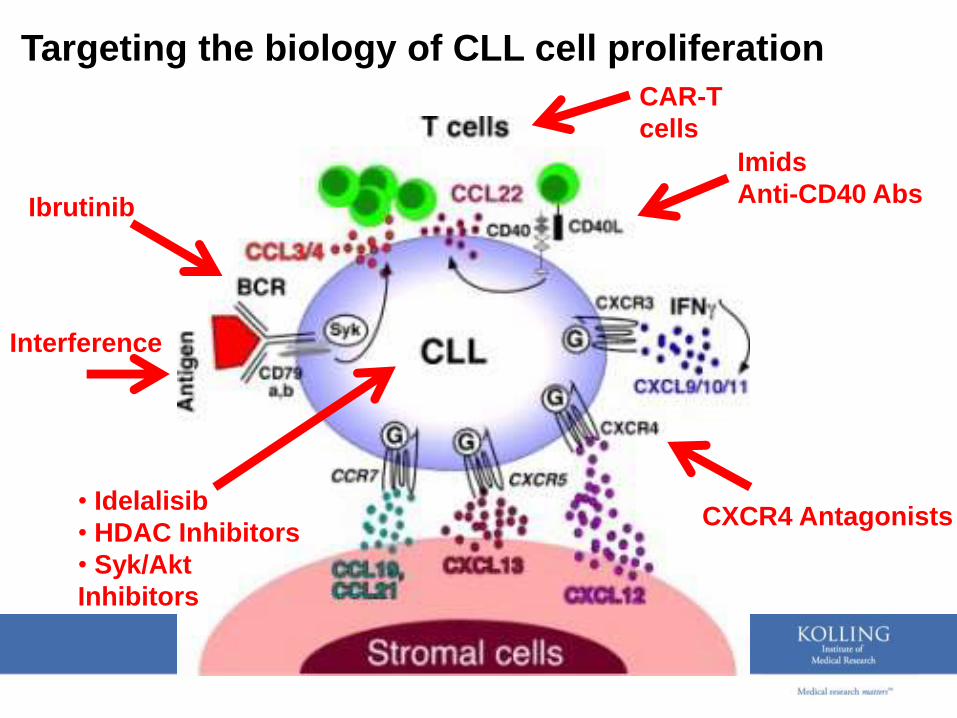
Targeting the biology of CLL cell proliferation
• Idelalisib
• HDAC Inhibitors
• Syk/Akt
Inhibitors
Ibrutinib
CAR-T
cells
Interference
Imids
Anti-CD40 Abs
CXCR4 Antagonists

Invitation to Sydneyiw CLL 2015
6-9th September, 2015

iwCLL Sydney 2015
6th September Young Investigator Meeting
6th September CLL Education Forum
7-9th September iwCLL Program
Day 1 The B-Cell Receptor
Day 2 Patient related issues
Day 3 CLL cell related issues
CLL in Asia Session

Invitation to Sydneyiw CLL 2015
6-9th September, 2015














![9. Stephen Cheung(update)[2]](https://static.fdocuments.net/doc/165x107/577d2d411a28ab4e1ead4307/9-stephen-cheungupdate2.jpg)



