APGO Milestone 1 Curriculum Office Practice / Outpatient ...
date post
19-Dec-2015Category
view
219download
1
8th Edition APGO Objectives for Medical Students
Infertility
Rationale
The evaluation and management of an infertile couple requires an understanding of the processes of conception and embryogenesis, as well as sensitivity to the emotional stress that can result from the inability to conceive.
Objectives
The student will be able to cite: Definition of primary and secondary
infertility Causes of male and female infertility Evaluation and managementPsychosocial issues associated with
infertility
Definition
Primary Couple has never conceived No conception during first year without
contraception Secondary - couple has had at least one
prior conception
Scope of problem Common problem - 1 of every 12 couples or 24
million women 1990 estimated health care costs in U.S. for
infertility were $1.3 billion Conception rate - fecundability
After 1 mo. ~ 20% will conceive After 3 mo. 50% will conceive After 6 mo. 75% will conceive After 12 mo. 90% will conceive
Etiology of infertility 20-40% of couples will have multiple causes
Female - about 60% Tubal - 35% Ovulatory - 15% Cervical - 5% Other - 5%
Etiology of infertility 20-40% of couples will have multiple causes
Male - 35-40% Azoospermia Compromised spermatogenesis
Etiology of infertility 20-40% of couples will have multiple causes
Couple Age (rates vary with female age) Sexual life, i.e. frequency Cigarette smoking - delays time to
conception
Evaluation
History and physical
EvaluationMale Factor - semen analysis
Volume - 2-5cc pH: 7.5-7.8 Total count - 40 x 106 - 200 x 106
Azoospermia = no sperm <40 x 106 - Oligospermia
Concentration >20 x 106 /mL count/cc >50% motile Fructose positive
EvaluationMale Factor - semen analysis
Normal morphology (>60%) Liquefaction - 1-20 min. Possible etiologies
Genetic disorders, i.e. Klinefelter Syndrome Endocrinopathies Varicoceles Obstruction Infection Hypogonadism Idiopathic Defect in spermatogenesis
EvaluationFemale Factors
Document ovulation Basal body temperature chart (sustained rise >10 days) Day 21 serum progesterone (>5ng/mL) FSH on Day 3 of cycle - if >15 mIU/mL, abnormal and
fertilization of eggs unlikely - ovarian failure, diminished ovarian reserve
Exclude cervical factors - post-coital test (Sims-Huhner Test) - look for five or more actively motile sperm in cervical mucus
Tubal factors Hysterosalpingogram to look for tubal patency Laparoscopy to look for peritoneal factors

Therapy
Male factor Urology consult Donor sperm insemination Intrauterine insemination (IUI) In Vitro Fertilization- Embryo Transfer
(IVF-ET) IVF with ICSI (intracytoplasmic sperm
injection)
Therapy
Female factors Poor or lack of cervical mucus Consider
IUI Low-dose estrogen Tubal occlusion - corrective surgery
and/or IVF Anovulation - ovulation inducers
Therapy
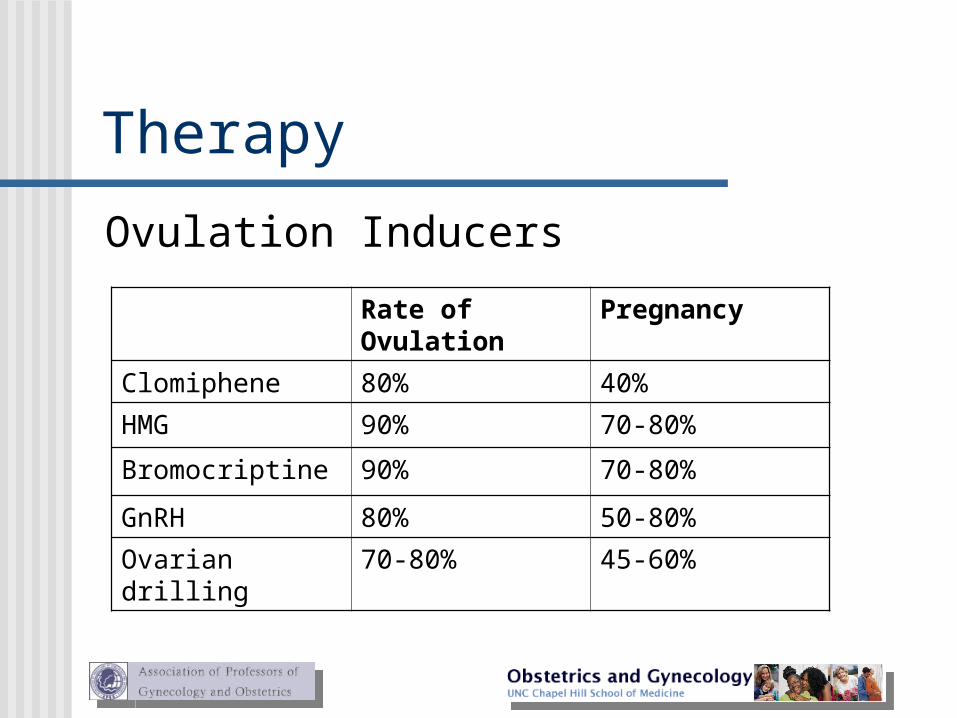
Ovulation Inducers
Rate of Ovulation
Pregnancy
Clomiphene 80% 40%
HMG 90% 70-80%
Bromocriptine 90% 70-80%
GnRH 80% 50-80%
Ovarian drilling 70-80% 45-60%
Therapy
Assisted reproductive technology Requires
Controlled ovarian hyperstimulation Retrieval of oocytes In vitro fertilization and embryo transfer
Procedures IVF-ET (In Vitro fertilization-embryo transfer) GIFT (Gamete intrafallopian transfer) ZIFT (Zygote intrafallopian transfer) ICSI (Intracytoplasmic sperm injection)
Psychological issues
Conflicting feelings about parenthood; active participation of both partners throughout
References
Speroff L, Glass RH, Kase NG. Clinical Gynecologic Endocrinology and Infertility, 5th ed., Baltimore, MD, 1994, Williams & Wilkins.
Adapted from Association of Professors of Gynecology and Obstetrics Medical Student Educational Objectives, 7th edition, copyright 1997
Clinical Case
Infertility
Patient Presentation
A 37-year-old female and her 37-year-old husband present with the complaint of a possible fertility problem. The couple has been married for 2 years. The patient has a 4-year-old daughter from a previous relationship. The patient used birth control pills until one-and-a- half-years-ago. The couple has been trying to conceive since then and report a high degree of stress related to their lack of success.
Patient PresentationThe patient reports good health and no problems in
conceiving her previous pregnancy or in the vaginal delivery of her daughter. She reports that her periods were regular on the birth control pill, but have been irregular since she discontinued taking them. She reports having periods every 5-7 weeks. Past history is remarkable only for mild depression. Imipramine 150 mg qhs for the last 8 months is her only medication. She works as a cashier, runs 12-24 miles each week for the last 2 years, and has no history of STDs, abnormal Paps, smoking, alcohol or other drugs. She has had no surgery.
Patient PresentationThe patient’s partner also reports good health and reports
no problems with erection, ejaculation or pain with intercourse. He has had no prior urogenital infections or exposure to STDs. He has had unprotected sex prior to his current relationship, but has not knowingly conceived. He has no medical problems or past surgery. He works as a long-distance truck driver and is on the road 2-3 weeks each month. He smokes a pack of cigarettes a day since age 18 and drinks 2-3 cans of beer 3-4 times a week when he’s not driving. He occasionally uses amphetamines to stay awake while driving at night. The couple has vaginal intercourse 3-5 times per week when he is at home.
Patient Presentation
Physical examThe patient is 5’9” and weighs 130 pounds. Breast exam reveals no tenderness or masses, but bilateral galactorrhea on compression of the areola. Pelvic exam reveals normal genitalia, a well-estrogenized vaginal vault mucosa and cervical mucus consistent with the proliferative phase. The uterus is anteflexed and normal in size without masses or tenderness.
Patient Presentation
LaboratoryResults Normal Values
TSH 2.1 mIU/ml 0.5-4.0 mIU/mlFree T4 1.1 ng/dl 0.8-1.8 ng/dlProlactin 60 ng/ml <20 ng/mlFSH 6 mIU/ml 5-25 mIU/mlLH 4 mIU/ml 5-25 mIU/ml
Basal body temperature chart shows a monophasic temperature graph.
Patient Presentation
PartnerSemen analysis revealed 2 cc of semen, 4 million per mL, 30% normal forms and 20% motility.
Management
The patient’s major infertility factor is anovulation; the most likely cause is hyperprolactinemia from imipramine. The prolactin level is elevated, consistent with drug-induced hyperprolactinemia. The patient was instructed, in conjunction with her therapist, to taper off the imipramine. Her follow-up basal body temperature chart was biphasic, consistent with ovulatory cycles.
Management
The patient’s partner, however, has a semen analysis that is consistent with oligospermia. The couple was given their options of: 1) In Vitro fertilization with ISCI; 2) artificial insemination with partner’s sperm; 3) artificial insemination with donor sperm; or 4) adoption.
Teaching pointes
1. Multiple causes must be considered for infertility diagnosis and treatment. Female and male reproductive anatomy and physiology should be reviewed in order to encompass the large differential diagnosis and the different factors that may contribute to infertility or subfertility.
Teaching pointes
2. Infertility is defined as one year of unprotected coitus without conception. Infertility may be primary: a woman who has never achieved pregnancy, or secondary: a woman who has achieved pregnancy in the past. Causes of infertility include tubal and pelvic pathology (35%), male problems (35%), ovulatory dysfunctional (15%), unexplained infertility (10%) and unusual problems (10%).

Teaching pointes
3. Components of an initial infertility workup include a thorough history and physical examination. Laboratory investigations include a semen analysis to assess male causes of infertility, a method to document that ovulatory cycles are occurring and, often, a hysterosalpingogram to rule out tubal disease.

Teaching pointes
4. Disorders of ovulation include polycystic ovarian syndrome (PCOS), hyperprolactinoma, thyroid dysfunction and hypothalamic causes and may be diagnosed by history, as well as laboratory tests that document the occurrence of ovulatory cycles. Basal body temperature recording, urinary LH testing, endometrial biopsy and luteal phase serum progesterone testing are all tests that may help confirm the presence or absence of ovulation.
Teaching pointes
5. Dysfunction of the hypothalamic-pituitary-ovarian axis and medical illness, including thyroid disease and pituitary tumors, can cause ovulatory disturbances. Further laboratory workup targeting these problems should be performed when history, examination, and initial laboratory evaluation indicate ovulatory dysfunction. Medication can also cause ovulatory problems.

Teaching pointes
6. Ovulatory dysfunction may sometimes be treated with correction of medical disease or change of medications. Most often, ovulatory dysfunction is treated empirically with ovulation induction agents such as clomiphene citrate. A thorough understanding of the normal physiology and pathophysiology of the menstrual cycle aids greatly in the understanding of ovulatory dysfunction.
Teaching pointes
7. Management of tubal disease is often surgical, including lysis of adhesions and removal of tubal obstruction via either laparoscopy or laparotomy, depending on the severity of the disease.
8. Male fertility problems include varicocele, duct obstruction, sperm antibodies, hypogonadism, testicular hyperthermia, drug use and industrial pollutants.